Sad Ha Sivam 2012

of 22
Transcript of Sad Ha Sivam 2012
-
8/17/2019 Sad Ha Sivam 2012
1/22
1719
REVIEW
ISSN 1462-241610.2217/PGS.12.152 © 2012 Future Medicine Ltd Pharmacogenomics (2012) 13(15), 1719–1740
Pharmacogenomics of opioids and perioperative
pain management
One of the fundamental perioperative goals is tooptimize pain management with better controlof pain without signicant adverse effects frompain medications for all patients. Unfortunately,safe and effective analgesia is an importantunmet critical medical need [1] and its contin-
ued existence is an important clinical, economicand societal problem. This is mainly because ofhuge and unpredictable interpatient variabilityand narrow therapeutic indices of currently usedperioperative opioids. Each year, in the USAalone, more than 30 million children and adultsundergo painful surgical procedures [2]; world- wide more than 250 mil lion patients undergopainful surgery annually. Many patients experi-ence inadequate pain relief [3] and serious sideeffects with opioids, the most commonly usedperioperative analgesics [4]. Inadequate pain
relief and serious side effects from perioperative
opioids occur frequently in approximately 50%of patients [4,5].
The goal of personalized analgesia is an appro-priate and individualized balance at which apatient experiences maximum desirable anal-gesic relief and minimal undesirable adverse
effects. The current clinical considerations for variability are inadequate: age, weight, gender,race, anxiety and type of surgery. To achieve thegoal of personalized analgesia, a better under-standing of the genetic contribution to interindi- vidual variability with perioperative analgesics isneeded. Recently, a number of small adult studieshave shown association of SNPs in genes in thepain pathway with altered pain sensitivity andaltered responses to perioperative analgesics. Thisarticle is a comprehensive review of the availableevidence on improving and personalizing pain
management with further focus on the need for
Inadequate pain relief and adverse effects from analgesics remain common in children and adults duringthe perioperative period. Opioids are the most commonly used analgesics in children and adults to treatperioperative pain. Narrow therapeutic index and a large interpatient variability in response to opioidsare clinically significant, with inadequate pain relief at one end of the spectrum and serious side effects,such as respiratory depression and excessive sedation due to relative overdosing, at the other end.Personalizing analgesia during the perioperative period attempts to maximize pain relief while minimizingadverse events from therapy. While various factors influence response to treatment among surgicalpatients, age, sex, race and pharmacogenetic differences appear to play major roles in predicting outcome.Genetic factors include a subset of genes that modulate the proteins involved in pain perception, pain
pathway, analgesic metabolism (pharmacokinetics), transport and receptor signaling (pharmacodynamics).While results from adult genetic studies can provide direction for pediatric studies, they have limited directapplicability, as children’s genetic predispositions to analgesic response may be influenced by developmentaland behavioral components, altered sensitivity to analgesics and variation in gene-expression patterns.We have reviewed the available evidence on improving and personalizing pain management with opioidsand the significance of individualizing analgesia, in order to maximize analgesic effect with minimaladverse effects with opioids. While the early evidence on individual genotype associations with pain,analgesia and opioid adverse outcome are promising, the large amount of conflicting data in the literaturesuggests that there is a need for larger and more robust studies with appropriate population stratificationand consideration of nongenetic and other genetic risk factors. Although the clinical evidence and theprospect of being able to provide point-of-care genotyping to enable clinicians to deliver personalizedanalgesia for individual patients is still not available, positioning our research to identify all possible majorgenetic and nongenetic risk factors of an individual patient, advancing less expensive point-of-caregenotyping technology and developing easy-to-use personalized clinical decision algorithms will help usto improve current clinical and economic outcomes associated with pain and opioid pain management.
KEYWORDS: analgesia n genetics n opioids n personalized medicinen pharmacogenetics n pharmacogenomics n surgical pain
Senthilkumar
Sadhasivam*1,2,3
& Vidya Chidambaran1,2,3
1Department of Anesthesiology,
Cincinna Children’s Hospital Medical
Center, 3333 Burnet Avenue,
MLC 2001, Cincinna, OH 45229, USA 2Department of Pediatrics, Cincinna
Children’s Hospital Medical Center,
Cincinna, OH, USA3University of Cincinna College of
Medicine, Cincinna, OH, USA *Author for correspondence:
Tel.: +1 513 636 4408
Fax: +1 513 636 7337
part of
-
8/17/2019 Sad Ha Sivam 2012
2/22
Pharmacogenomics (2012) 13(15)1720 future science group
REVIEW Sadhasivam & Chidambaran
pediatric pharmacogenetic studies to maximizeanalgesia while minimizing adverse effects.
Since its discovery and use in the third cen-tury BC, as described by Theophrastus, opiumhas remained the principal treatment for painthrough administration of its many derivatives
[6]. Today opioid analgesics remain the primarytreatment for pain during the intraoperative andimmediate postoperative period among whichmorphine is the most widely used opioid acrossall age groups [7]. Morphine, along with theother opioids, have narrow therapeutic indicesand high interpatient variability, which oftenresults in inadequate pain relief at one end of theoutcome spectrum and adverse effects, includ-ing respiratory depression, sedation, dizziness,postoperative nausea and vomiting, pruritus,constipation, physical dependence and tolerance
at the other end[8–16]
. Adverse events related tomorphine in adults were found to signicantlyincrease median total hospital costs by 7.4% andmedian length of stay by 10.3% [17]. Thus, thereis a need for a ne balance aiming to maximizeanalgesic efcacy without compromising safety.
The clinical practice of perioperative painmanagement has evolved as an art and a science,but is far from perfect due to the unpredict-ability and heterogeneity of individual patientresponses [18]. These differences lead to unpre-dictable responses or toxic effects in individualsor subgroups, and can ultimately affect patient
outcomes. A priori identication of susceptibleindividuals could lead to modication of drugdosage or use of an alternate drug, which mightprevent serious adverse drug reactions. More-over, inadequate pain management is also associ-ated with major clinical, nancial and societalconsequences [19,20]. Recent advances in genomictechniques and molecular biology have enabledresearchers to identify associations betweenan individual’s genotype and drug response. Although there have been review articles pertain-ing to pharmacogenetic effects on analgesia in
the past [18,21–23], evolving genomic technology,identication of newer genotype–phenotypeassociations, and emerging elds, such as epi-genetics and functional genomics, have furtherexpanded the knowledge base. The necessity torecapitulate this knowledge for clinicians can-not be overemphasized as they face an increasedlikelihood of implementing pharmacogenetics indaily clinical care in the near future.
History of pharmacogeneticsThe last couple of decades have been revolution-
ized by the implementation of the US Human
Genome Project. This was a 13-year effort coor-dinated by the US Department of Energy andthe NIH. The project was originally planned tolast 15 years, but rapid technological advancesaccelerated the completion date to 2003, result-ing in elucidation of the 2.85 billion nucleotides
that make up the human genome, and encodeapproximately 25,000 genes [24]. Presently, theUS FDA has approved pharmacogenetic/genomicinformation/warnings in the labels of over100 drugs, which include analgesics such ascodeine and tramadol [25].
Pharmacogenomics basic concepts‘Pharmacogenomics’ is a broader application ofgenomic technologies to drug discovery, phar-macokinetics, pharmacodynamics and thera-peutic outcomes, while ‘pharmacogenetics’ is
the study of genetic variations affecting drugresponse though the terms are sometimes usedinterchangeably. The genes and DNA determinethe structure and function of proteins. Varia-tions in the genetic makeup can understandablyalter the structures and functions of proteins andplay a major role in the pharmacokinetics andpharmacodynamics of drugs such as opioids[26]. The most common genetic variation is theSNP, which occurs at an appreciable frequency,>1% [27]. Other variations are called mutations(incidence G which is the SNPof the OPRM1 at base pair 118, which codesfor change of adenine to guanine); alternatively,alteration of amino acid sequence induced bythe SNP (e.g., A118G of OPRM1 can be abbre- viated as Asn40Asp, which indicates change ofamino acid at position 40 from asparagine toaspartate); or changes at the allele level (e.g., thesecond variant of the wild-type CYP450 enzyme
CYP2C9*1 is CYP2C9*3 ). SNPs can have pro-found impact on the function of the proteinsor associated genes, even if they are located at asignicant distance from the transcription ini-tiation site of the gene. Hence, it is clear thatidentication of an individual SNP may not besufcient to explain the variation in phenotype.Genetic linkage is the phenomenon wherebyalleles at loci close together on the same chromo-some tend to be inherited together, because it israre for crossover to occur between the loci dur-ing meiotic division of the chromosomes. SNPs
that are linked together are said to be in linkage
-
8/17/2019 Sad Ha Sivam 2012
3/22
www.futuremedicine.com 1721future science group
Perioperative pain & pharmacogenomics of opioids REVIEW
disequilibrium because they are not randomlyinherited and hence have not reached equilib-rium within a population. A haplotype is a setof closely linked alleles or polymorphisms thatare inherited together. The number of uniqueproteins (millions) in human are signicantly
more than the number of genes (approximately25,000), thus the study of proteins ‘proteomics’is often more informative. Moreover, differentcells and tissues have different expression of thesame genes, thus resulting in different proteinexpressions [28]. This evolving science is broadlytermed ‘functional genomics’. ‘Epigenetics’ is thestudy of the mechanisms of temporal and spatialcontrol of gene activity during the developmentof complex organisms [29].
Genetics of pain & pain management
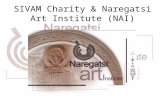
It has been hypothesized in previous studies thatup to two-thirds of the interindividual variabil-ity in response to morphine results from genetic variations [30]. Pharmacogenetics of opioids willbe discussed under two major sections, ‘Per-sistent postoperative pain’ and ‘Pharmacoge-nomics of opioid analgesia & opioid-relatedadverse effects’. Under these headings, geneticinuences on opioid receptors and signaling,opioid metabolism and opioid transport will bereviewed (FIGURE 1).
n Pain perception & genetics
Pain is a complex neurophysiological conditioninvolving multiple components and their inter-actions, which is perceived differently amongindividuals. Endogenous opioids, includingthe enkephalins, endorphins and dynorphins,along with neurotransmitters such as the cat-echolamines (epinephrine, norepinephrine anddopamine), are vital components in the pain per-ception pathway as indicated in disease states [31–36]. Increase in catecholamines can be elicited byphysiological stress resulting from physiologicalconditions such as emotional stress in addition to
that elicited by pain stimuli itself [37,38]. COMTis the enzyme responsible for metabolizing andinactivating catecholamines by transfer of amethyl group from the coenzyme S -adenosyl-l-methionine to one of the hydroxyls of the cat-echols in the presence of magnesium. Therefore,COMT serves as a pivotal regulator of dopa-mine, epinephrine and norepinephrine concen-trations in the pain perception pathway [39,40].
Important differences have been found in thegene encoding COMT among patients experi-encing painful conditions. The main and well-
studied COMT SNPs are rs6269, rs4633, rs4818
and rs4680 [41,42]. The SNP rs4680 is a commonpolymorphism of the COMT gene on chromo-some 22q11 coded by 472G>A, which causes thesubstitution of valine by methionine at aminoacid position 158 (Val158Met). The valine formethionine substitution in the COMT enzyme
reduces the activity of the enzyme three- to four-fold and leads to high pain sensitivity [34,39,43].The Val158Met substitution also affects ther-mostability, although some studies have indi-cated no association of the SNP and hot–coldsensitivity [44]. Clinically, adult cancer patients with the Met/Met genotype of COMT SNPrs4680 were found to have the greatest sensitiv-ity to pain, while those with the Val/Val geno-type the least pain sensitivity [34]. This ndingseems contradictory, but may be related to othergenes. In cancer patients, when analyzing both
the OPRM1 and COMT genes, OPRM1 AA at118 position and COMT Met/Met required theleast morphine and those without either of theserequired higher morphine [45]. Patients withMet/Met were found to have decreased opioidresponses to pain compared to the Met/Val as well as higher sensitivities to pain [40]. Furtherinvestigation into relationships among the dif-ferent genes known to affect analgesic outcomeare necessary to determine their effects upon oneanother, and verify which have greater impact inthe perioperative period.
Different combinations of these COMT SNPsat these alleles dene distinct haplotypes (low[LPS], average [APS] and high [HPS] painsensitivity haplotypes) that have been found tobe predictive of specic levels of pain response. Although SNPs can result in variation in COMTactivity, results have been conicting. Hence, ithas been proposed that haplotypes serve as betterexplanation and account for approximately 11%of variation in pain sensitivity [42,44].
The LPS haplotype codes for the shortest andleast stable structure and the HPS the longestmost stable in the Val158 region [46]. The more
stable COMT enzyme was found to be less activeand does not metabolize the catecholamines aseffectively, resulting in increased levels of thesespecic pain contributing factors [46]. Furtherinvestigations indicated that LPS/LPS homo-zygotes had the least, APS/APS average, and APS/HPS the greatest pain sensitivity [42].
Low COMT activity, resulting in elevated lev-els of the catecholamines, has been indicated toincrease pain sensitivity through the b2 and b3adrenergic receptors [33,46]. As the primary targetfor epinephrine, the B2 receptor (ADRB2) vari-
ants are signicant in pain response. The two
-
8/17/2019 Sad Ha Sivam 2012
4/22
Pharmacogenomics (2012) 13(15)1722 future science group
REVIEW Sadhasivam & Chidambaran
most common haplotypes of ADRB2 based oneight SNPs (G-7127A, rs11958940, rs1432622,rs1432623, rs2400707, rs1042713, rs1042714and rs1042717) with >20% frequency of poly-morphisms in humans were found to have spe-cic psychological traits such as depression andanxiety, and high arterial pressure, and were
ten-times less likely to develop temporo-man-dibular joint disorder [47]. Therefore, differenthaplotypes of ADRB2 can result in differentlevels of the B2 receptor expression and vari-ability in the likelihood of developing painfulconditions such as temporo-mandibular jointdisorder. An ‘emotional personality’ has alsobeen implicated in subjective perception of painin head pain patients [48]. These reports furtherindicate the implication of catecholamines andthe autonomic nervous system in the perceptionof pain.
Genes encoding metabolic factors have sig-nicant variation among ethnic populations. Forthe COMT enzyme, differences in the gene existat the Val158Met polymorphism among differ-ent ethnic groups with Hispanic individualshaving the highest proportion of Met/Met and African–Americans Val/Val. Val/Met are thehighest proportion in all of these ethnic groups[44]. Therefore, Hispanic populations are likely tohave the greatest sensitivity to pain and requireless opioid for analgesia, while African–Ameri-cans are expected to have the lowest sensitivity to
pain and require more opioid for analgesia [44].
In our relatively large prospective clinical studyof a homogeneous pediatric population undergo-ing adenotonsillectomy (n = 275), we observedthat rs4818 COMT polymorphisms had strongassociations with intravenous analgesic interven-tions in African–American children in the post-anesthesia recovery unit (PACU; odds ratio: 14.8;
p = 0.0034) as well as COMT SNP rs6269 asso-ciations with opioid related adverse effects leadingto prolonged stay in the PACU especially in Afri-can–American children (p = 0.031). In addition,a genetic variant of GCH1 was associated withhigher incidences of clinical respiratory depres-sion (odds ratio: 6.6; p = 0.0057) and highersubjective postoperative numerical pain scores(p = 0.0434) especially in African–Americanchildren in our tonsillectomy study [SS, U D]. These genetic factors couldat least partly explain why African–American
children experience relatively more postoperativepain than Caucasian children undergoing similarsurgery [49].
n Persistent postoperative painIn human acute and surgical pain studies, certainCOMT genotypes and low COMT activity havebeen associated with increased sensitivity to acuteand postoperative pain [50–53] and a trend towardspersistent pain after mastectomy [54]. A lowCOMT activity also increases availability of opi-oid receptors and may enhance opioid analgesia
and adverse effects at least in cancer pains [41].
Pharmacokinetics(volume of distribution,
clearance)
Metabolizing
enzymes
G e n e t i c
f a c t o r s
N o n g e n e t i c f a c t o r s
w i t h
g e n e t i c l i n k s Drug interactions
Opioid analgesia and side effects
Physiological(Age, sex)
Ethnicity/race
Psychological
(anxiety, stress)
CYP2D6,
UGT2B7
ABCB1 OPRM1, COMT,
MC1R
Transporters Opioid
receptorsSignal
transduction
Genetic factors
Pharmacodynamics(pain sensitivity,
efficacy)
Figure 1. Interindividual variations of opioid effects. Illustrates clinically relevant genetic andnongenetic factors influencing analgesic responses and side effects of opioids. Possible links betweengenetic and nongenetic factors are highlighted with dotted lines.
-
8/17/2019 Sad Ha Sivam 2012
5/22
www.futuremedicine.com 1723future science group
Perioperative pain & pharmacogenomics of opioids REVIEW
GCH1, the gene encoding the rate-limitingenzyme in tetrahydrobiopterin (BH4) synthesis,has been strongly implicated as a determinantof pain experience. BH4 is an essential cofac-tor in the synthesis of serotonin, dopamine,epinephrine, norepinephrine and nitric oxide
and levels increase pathologically in the injuredsomatosensory system. Following peripheralnerve damage, levels of BH4 are dramaticallyincreased in sensory neurons principally due tothe upregulation of the rate-limiting enzyme forBH4 synthesis, GCH1, causing increased activ-ity and pain hypersensitivity. A human GCH1 gene pain protective haplotype had been associ-ated with less BH4 and less pain, especially fol-lowing nerve injury where BH4 production ispathologically augmented [55]. A small study ofadults undergoing spine surgery for degenerative
disk disease suggests that the T allele at rs998259of GCH1 may be associated with improved dis-ability outcomes 1 year following surgery [25].It was recently proposed that sulfasalazine, anFDA-approved anti-inammatory agent, couldbe antineuropathic pain medicine by inhibitingsepiapterin reductase and reducing BH4 levels[56]. Prospective human studies are needed to validate the benets of BH4-blocking drugs.
Inflammatory components alter anal-gesic responseGenetic variation also affects a human’s individ-
ual response to pain-causing stimuli. Systemicinammation is a common response to tissuestress and damage following surgery, traumaand infection [57–62]. During inflammatoryresponses proinammatory cytokines such asTNF-a and TNF-b, and interleukins, includ-ing the studied IL-1b and IL-6, are released intocirculation. TNF-a serves as an early modula-tor of the inammatory response while IL-6stimulates endothelial activation, smooth mus-cle cell proliferation, leukocyte recruitment andeventually plaque growth [63,64]. TNF-a is also
believed to be the central cytokine responsiblefor the development of septic shock, the primarycause of death in intensive care units in the USA[65]. As a major response to surgery, the inam-matory response and its components are likelyto have a signicant impact upon patients’ painexperiences. For instance, polymorphisms in thepromoter region of the IL-6 gene were foundto have an effect upon peak IL-6 levels follow-ing coronary artery bypass surgery [63]. Amonganother group of patients undergoing cardiacsurgery with cardiopulmonary bypass, differ-
ences in peak levels of IL-6 postoperatively also
reected differences in other cytokines includingserum levels of TNF-a and IL-1b. Those patients with elevated IL-6 levels had increases in othercytokine levels [64]. In addition to IL-1, the che-mokines and other spinal proinammatory cyto-kines have been found to be endogenous regula-
tors of analgesia as they decrease analgesic out-come and increase pain sensitivity [66,67]. As IL-6increases, the concentration of IL-1b will also riseand decrease the analgesic effects of opioid treat-ment. IL-1 plays a critical role in the developmentand maintenance of incisional pain [62]. A recentstudy showed that the variable number of tandemrepeats in intron 2 of IL-1 receptor antagonistgene, IL1RN, contribute to interindividual varia-tions in opioid consumption in the rst 24 h afternephrectomy [68]. Patients homozygous for theIL1RN*1 allele have lower concentrations of IL-1
receptor antagonist and require higher doses ofopioids postoperatively than patients carrying atleast one IL1RN*2 allele [68].
Role of sex in pain & analgesiaInvestigations of the genetic and environmen-tal factors related to pain perception and anal-gesia have recently indicated the importance ofgenetic and physiological differences among sexesas well as the cultural impact upon pain experi-ence and analgesic outcome. Sex is dened byan individual ’s biological sex and gender as one’sidentication as a male or female [69]. Therefore
while gender often relates to one’s psychologi-cal experience of pain, sex dif ferences have beenreported in species other than humans, suggest-ing that underlying inherent differences existthat are distinct from sociocultural inuences[70]. Consistently, females are found to experi-ence more painful situations, higher levels ofpain during these times and have a decreasedthreshold for various forms of painful stimuli.Still differences exist between types of stimuli with mechanical having the greatest thresholddecrease and blunt pressure the least [71]. How-
ever, after the age of 40 these sex differences inthermal and mechanical threshold stimuli appearto become less signicant suggesting that age andcorresponding hormone levels are also importantfactors in pain perception and analgesia [71]. Hor-mone expression in females may alter their experi-ence of pain through their effect upon peripheralmechanisms. A recent study suggests that tempo-ral processing of pain differs between males andfemales with females experiencing more pain atthe outset of exposure to multiple painful stimulibut then experienced less pain than males as the
stimulus was sustained [72].
-
8/17/2019 Sad Ha Sivam 2012
6/22
Pharmacogenomics (2012) 13(15)1724 future science group
REVIEW Sadhasivam & Chidambaran
Women compared with men have higher inci-dences of adverse effects such as nausea, vomit-ing, respiratory depression and bradycardia withµ-opioid agonists [73]. However, treatment withk-opioid analgesics has been indicated to pro-duce more intense and longer lasting analgesia in
women than men [71,73]. In females, MC1R wasfound to impact the k-opioid receptor and anal-gesic outcome when activated [74]. Discrepanciesexist as studies have indicated greater morphinepotency but slower speed of onset and offset in women [73,75].
Different coping strategies have also beenfound to affect painful experiences among women and men. In a study of males and femalesexperiencing cold pressor task, men were foundto benet from sensory focusing techniques while women were not [76]. Studies have indicated that
women benet from emotional focusing tech-niques but did not if using negative emotionalfocusing, which involves labeling one’s emotionsin a negative manner [76].
Role of race on pain & analgesiaPain sensitivity appears to differ among differentraces/ethnicities. There is considerable evidenceto suggest that African–American and Hispanicpatients report lower tolerance for experimen-tally induced pain compared with Caucasians[77–79]. Moreover, there are reports of racial dis-parities in the prescription of opioid analgesics
in the management of postoperative pain [80].Recently, we have demonstrated that race isassociated with an unequal burden of periop-erative pain and opioid adverse effects in chil-dren. Specically, African–American childrenhad higher postoperative pain and Caucasianchildren had higher incidences of opioid-relatedadverse effects following tonsillectomy [49].
It is important to stratify populations basedon ancestry before correlating high-risk genes with clinical outcomes. Among different eth-nic groups many genetic differences are part
of the underlying cause of different responsesand experiences of pain. For example, polymor-phisms in OPRM1’s exon 1 C17T and A118G,and in the promoter region at t-1793A, -1699T,and A-1320G are statistically different among African–American and Caucasian populations[81]. The frequency of the A118G polymor-phism is estimated to be approximately 46% in Asian populations, while between 5 and 25%in European and African–Americans popula -tions, which are also signicantly different fromeach other [82–85]. Similarly, differences exist
at the OPRM1 Ala6Val and Asp40Asn alleles
in exon 1 among European–American and African–American populations [85].
Psycho-emotional factors& perioperative pain A recent cross-sectional Tromsø study strength-
ens the strong association between psychologicaldistress and surgica l pain and its persistence [86].Psychological factors, including anxiety, fear ofsurgery [87] and catastrophizing [88], are associ-ated with increased pain after surgery. The levelof preoperative anxiety is determined by a com-plex interplay of various factors including geneticmakeup [89]. In addition to pain and analgesia,COMT is believed to be an important compo-nent in the expression of mood as well as cogni-tive function [42]. Catecholamines are known toincrease during both emotional and physiologi-
cal stress. The COMT gene has been shown tomoderate pathways of pain-related cognition andmaladaptive coping with pain [90]. Pain catastro-phizing and COMT genotypes have been shownto inuence postoperative pain ratings [51]. Inthe operating room, children are likely to have adifferent experience both emotionally and physi-cally compared with adults corresponding witha specic level of stress. Studies have indicatedthat pediatric patients with increased levels ofpreoperative anxiety and stress are more likelyto experience greater postoperative behavioraldisturbances and pain [91,92]. As catecholamines
are likely to play a signicant role in periop-erative stress, developing a better understand-ing of the regulation of the COMT gene andthe corresponding catecholamine metabolism will provide insight into optimizing analgesictherapy.
Persistent postoperative pain A recent cross-sectional survey reports that theincidence of persistent postoperative pain (PPP)is as high as 40% with 18.3% of patients report-ing moderate or severe pain [86]. Persistent pain
after surgery is not only an important and expen-sive clinical problem, but also a model for explor-ing the mechanisms underlying the change fromacute to chronic pain. Pain and general physicalfunctioning before surgery have been associated with persistent postsurgical pain [87]. Evidenceindicates that psychological factors, includinganxiety, depression, fear of surgery [87] and cat-astrophizing [88], are associated with increasedrisk for PPP. Out of the risk factors leading toPPP, nerve injury from surgery leading to centralsensitization is emerging consistently conrming
a strong neuropathic component to persistent
-
8/17/2019 Sad Ha Sivam 2012
7/22
www.futuremedicine.com 1725future science group
Perioperative pain & pharmacogenomics of opioids REVIEW
postsurgical pain [93,94]. More research focus-ing on preventive strategies is needed. In humanacute and surgical pain studies, certain COMT genotypes and low COMT activity have beenassociated with increased sensitivity to acute andpostoperative pain [50–53] and a trend towards
persistent pain after mastectomy [54].
n Pharmacogenomics of opioid anal-gesia & opioid-related adverse effectsOpioid receptors & clinical effects
Opioids are commonly employed analgesics formanaging postoperative pain [4,95–99]. Despitetheir analgesic strength, opioids have a narrowtherapeutic index and several adverse effectsincluding respiratory depression, miosis, drowsi-ness, nausea, vomiting and constipation. In arecent opioid pharmacogenetic twin study of
114 monozygotic and dizygotic twin pairs who were given either an infusion of short-actingopioid, alfentanil or saline placebo, the authorsconcluded that genetic effects accounted forapproximately 60% of the response variancein nausea, 30% of the variance in respiratorydepression and 36% of variations in opioid dis-liking; genetic, environmental and demographicfactors together influence opioid responses with varying contributions to specic opioidresponses [100].
Opioids exert their pain relieving effects byacting as agonists at the µ-opioid receptor, a
seven-transmembrane spanning protein codedfor by the OPRM1 gene located on chromosome6q24-q25 [30,101]. OPRM1 is an essential com-ponent inuencing analgesic outcome [96,102,103].One of the most widely studied genetic varia-tions in the OPRM1 gene is the SNP at basepair 118 in exon 1. In this SNP, an adenine isreplaced by a guanine, resulting in the aminoacid exchange of aspartate replacing asparagineon the µ-opioid receptor protein at position 40of its extracellular terminal. This change resultsin the loss of N-linked glycosylation [96]. The
allelic frequency of this polymorphism hasbeen estimated between 10.5 and 18.8% [83,96].In vitro , one study has indicated that the A118Gpolymorphism increased the µ-opioid receptor’safnity for the endogenous opioid, b-endorphinby 300% compared with the wild-type allele [83].
Clinically, patients homozygous for the118GG allele have been found to requireincreased morphine dosages while demonstrat-ing resistance to the opioid’s adverse effects. Among 147 adults treated with postoperativemorphine following total knee arthroplasty,
patients homozygous for the 118GG allele
consumed signicantly higher doses of mor-phine during the rst 48 h postoperatively toachieve analgesia compared with those homo-zygous for 118AA and heterozygous for 118AG[101]. Similarly, among women undergoing totalabdominal hysterectomy the 118GG homozy-
gotes required signicantly more morphine dur-ing the rst 24-h period than the AA homozy -gotes and the heterozygotes, although not duringthe entire 48-h postoperative period [104].
However, in a study of American adults, nosignicant association was observed between thepresence of A118G polymorphism and postop-erative pain score or morphine doses used in theimmediate postoperative period [105]. Followingcolorectal surgery in adults, different alleliccomposition at OPRM1 A118G SNP were notfound to affect morphine dose requirements or
side effects, although the GG did require a largerdosage, which may not have been statisticallysignicant due to sample size [106]. It merits men-tion that a meta-analysis of pain phenotypes byOPRM1 genotype found no consistent associa-tion between OPRM1 118A>G genotypes andmost of the phenotypes. An analysis of eightdifferent heterogeneous clinical studies demon-strated only weak association between OPRM1 GG genotype and less nausea and of increasedopioid dosage requirements [107]. Mergingmany studies with different population intoa meta-analysis without appropriate consider-
ation of population stratication, other knownimportant genetic and nongenetic risk factorsassociated with outcomes and gene–gene inter-actions may not result in clinically meaningfulinformation.
Morphine-6-glucoronide (M6G) is a metab-olite of the opioid morphine, and like its par-ent compound also serves as a potent analgesic[103]. In patients heterozygous for the OPRM1 118 allele, an increased amount of M6G wasneeded to achieve comparable analgesic out-come as in the 118AA homozygotes. However,
no differences were found in respiratory depres-sion relating to the different alleles [103]. Furtherstudy with the analgesic alfentanil indicated thatalthough the heterozygous condition decreasesthe analgesic effect of alfentanil at a specic opi-oid dosage, only the respiratory depressive effects were signicantly decreased in the homozygous118GG patients [98]. While heterozygous patientsdemonstrate an increased dosage requirement foropioids, they do not have any increased protec-tion against the adverse effects, possibly makingthem the most susceptible to opioid side effects
[98]. Therefore, the need for an increased dosage
-
8/17/2019 Sad Ha Sivam 2012
8/22
Pharmacogenomics (2012) 13(15)1726 future science group
REVIEW Sadhasivam & Chidambaran
of opioid for analgesia does not indicate resis-tance to opioid adverse effects. A recent study inadults from Israel demonstrated that the G118SNP impairs the analgesic response to opioids byreporting increased opioid requirement for alfen-tanil in patients with the G118 SNP (GG and
AG genotypes), who self-administered a higherdose, achieved higher plasma concentration, andyet complained of more severe postoperativepain (T ABLE S 1 & 2) [108].
Recently, previously unpublished and newhaplotypes of the OPRM1 gene have been shownto predict increased pain after thoracotomy [109].This promising association needs validation in alarger postoperative pain population and mecha-nistic studies. Finding altered function based onthe new genetic variations would help us under-stand the pain–opioid pathway better and allow
clinicians to tailor opioid management.
Other genetic variations affectingthe µ-receptor signalingIn addition to a diversity of OPRM1 alleles, othergenes can affect the µ-opioid receptor’s prop-erties. Genetic variations extrinsic to OPRM1 have also been found to interact with and affectthe µ-opioid receptor. For instance, the MC1R gene encodes for MC1R, which serves a role inskin and hair pigmentation and immunomodu-lation. Genetic differences in the MC1R genehave recently been found to impact the µ-opioid
receptor through possible effects upon the phar-macodynamics of morphine’s metabolite, M6G[74,110]. Additionally, MC1R has been suggestedto affect analgesic response at the k-opioidreceptor in females. MC1R is believed to inu-ence basal pain sensitivity more so than alter-ing receptor function at the µ-opioid receptor[74,110]. Further research is required to explorethe mechanisms involved. Another gene, Stat6 ,is a transcription factor that causes an increase inOPRM1 expression [30]. Serotonin (5-hydroxy-tryptamine) receptor agonists are suggested to
have an important role in reducing opioid sideeffects. Some 5-HT4 variants have been associ-ated with less adverse events without decreasinganalgesic outcome [111]. Such genetic compo-nents could provide us with a better understand-ing of how to optimize analgesic outcomes whiledecreasing adverse effects. Similarly, insight intothe relationships among distinct alleles of differ-ent genes could provide us with a better under-standing of the regulation of OPRM1 expressionand µ-opioid receptor phenotype.
Opioid ligands bind to opioid receptors, and
the signal is transmitted to a variety of effectors
such as G-protein-activated inwardly rectify-ing potassium channels, thereby resulting inanalgesic effects. G-protein-activated inwardlyrectifying potassium channel gene polymor-phisms, especially those of the KCNJ6 genehad been associated with increased postopera-
tive pain [112]. A small clinical study in Japaneseadults undergoing major open abdominal sur-gery reported that AA homogeneous genotypeof A1032G SNP or 1250G/1032A haplotyperequired higher doses of rescue analgesics,especially in women, compared with carriersof other genotypes or haplotypes, respectively(T ABLE 2) [112]. Interpretation of results is limitedby the study sample size, but raises interestingavenues for future research in this area.
Opioid metabolism
Smith published an extensive review of opi-oid metabolism [113]. Major hepatic enzymesinvolved in opioid metabolism include CYP2D6and UGT2B7 .
CYP450 systemThe process of opioid metabolism, includingits rate and mechanisms, directly impacts itsanalgesic potency and duration of action. TheCYP450 enzyme, CYP2D6, has a signicantrole in analgesia as it is known to catalyze theO -demethylation of codeine to morphine.Codeine is a prodrug with no intrinsic analge-
sic effect. Nearly all of the analgesic activity ofcodeine occurs through its morphine derivative[114–116]. Codeine is frequently used to achievepostoperative analgesia in children because ofthe belief that it is a weak opioid analgesic andit is safe [117,118].
The CYP2D6 gene is highly polymorphic with over 100 different alleles many of whichhave been shown to inuence enzyme activ -ity [119,201]. CYP2D6*1 and *2 are the mostcommon fully functional alleles [120,121]. Thehomozygous or compound heterozygous
states with these two alleles lead to an exten-sive metabolizer phenotype [122]. Up to 10%of children prescribed codeine in USA arehomozygous or compound heterozygous forCYP2D6 alleles leading to a nonexistent ornonfunctional CYP2D6 isozyme [123]. Thesechildren, described as CYP2D6 poor metabo-lizers (PMs), are unable to convert codeine tomorphine and hence incapable of experiencingthe intended analgesic effect of codeine due tolack of active metabolite, morphine’s effect, butremain susceptible to codeine’s side effects from
codeine and nor-codeine [124,125]. The ultrarapid
-
8/17/2019 Sad Ha Sivam 2012
9/22
www.futuremedicine.com 1727future science group
Perioperative pain & pharmacogenomics of opioids REVIEW
metabolizer (UM) phenotype commonly results
from at least one duplicated functional allele onone chromosome combined with a functionalallele on the other chromosome [120,122,126,127].CYP2D6 UMs are at increased risk for excessivemorphine-related side effects from codeine asa greater percentage of codeine is converted tomorphine. The prevalence of CYP2D6 PMs inthe USA is between 5 and 10% in non-Hispanic whites and African–Americans. The prevalenceof CYP2D6 UMs varies across populations:1–4% of American whites and blacks, 8–10%of Turks and Spaniards, 20% of Saudi Arabians
and 29% of Ethiopians (T ABLE 3) [128].
There are multiple deaths related to opioids
in children [129–131], especially with codeine inyoung children following tonsillectomy due torelative overdose and/or CYP2D6 UM status[132–135]. Three recent deaths in children dueto codeine [136] highlight the importance ofCYP2D6 genetic tests and potentially avoidingcodeine and other opioids metabolized by theCYP2D6 pathway, in UMs and even extensivemetabolizers, especially in young children withhistory of sleep apnea or respiratory illness inunmonitored home environment [137]. While amother who was an UM took the commonly pre-
scribed codeine, delivered a larger than expected
Table 1. Pharmacogenetics and perioperative opioid analgesia.
Opioid Gene SNP Study population Result Ref.
Morphine OPRM1 A118G (74AA,33AG, 13GG)
120 Taiwanese adults following
knee arthroplasty
GG more morphine consumption (40 mg vs
25 mg in 48 h)
[101]
A118G (43AA,
19AG, 18GG)
80 Taiwan females following
abdominal hysterectomy
GG had significantly higher postoperative
day 1 morphine requirements
[104]
A118G Caucasians:
66 = AA, 29AG;
Africans: 1 = AA,
1 = AG; Hispanic:
3 = AA, 1 = AG
101 (23/78) adults with acute
pain following laparoscopy
(Caucasian 90%, African–
Americans 2%, Hispanic 5%)
and 127 adults with chronic pain
(95% Caucasian)
No significant difference noted in analgesic
requirement
[105]
A118G 588 healthy Asian females had
spinal morphine post-cesarean
section: 46% AA, 40% AG and
14% GG
AA had lowest pain scores and highest
incidence of nausea. Age and paying status
influenced morphine use
[176]
OPRM1 ABCB1
UGT2
OPRM1 -A118G ABCB1 -C3435T,
G2677T/AUGT2B7 -T802C
74 (30/44)
70 white, one black,
three biracial followingabdominal surgery
Age, psychotropic agents and creatinine
clearance were found to be associated with
postoperative morphine requirements. ABCB1 GG–CC diplotype only borderlinesignificant for fewer side effects such as
nausea
[106]
UGT2B7 161C/T802C/T
99 (36/63): 68 white, 27 black,
two Hispanic, two Asian gastric
bypass/joint replacement
M6G/M in T/T>C/T>C/C. CC low
glucuronidators. Less significant in
African–Americans
[148]
Fentanyl OPRM1 rs1799971 (A118G)and rs9384179
280 Japanese females following
orofacial cosmetic surgery
Patients with minor G allele of A118G had
less effect of fentanyl, minor G allele of
rs9384179 needed less fentanyl in 24 h
postoperative period
[177]
ABCB1 C1236T, G2677T/A,C3435T
126 (89/37) Korean patients
undergoing spinal anesthesia
with iv. fentanyl
1236TT, 2677TT, 3435TT: early and
profound respiratory depression after iv.
fentanyl
[165]
Codeine CYP2D6 PM, IM, EM 96 pediatric (age 3–12 years old),Caucasian 38%, Asian 22%,
African 17%, Turkish 8%, others
15% following
adenotonsillectomy
47% had genotypes associated with
reduced enzyme activity. Morphine and its
metabolite were not detected in 36% of
children given codeine
[118]
Alfentanil OPRM1 A118G 99 Israeli adults followingextracorporeal shock wave
lithotripsy
AG/GG genotype had more pain, higher
alfentanil needs despite higher plasma
concentration
[108]
EM: Extensive metabolizers; IM: Intermediate metabolizers; iv.: Intravenous; PM: Poor metabolizers.
-
8/17/2019 Sad Ha Sivam 2012
10/22
Pharmacogenomics (2012) 13(15)1728 future science group
REVIEW Sadhasivam & Chidambaran
T a b l e 2 . E f f e c t s o f g e n e t i c v a r i a n t s o n p e r i o p e r a t i v e p a i n a n d r e s p
o n s e s t o o p i o i d s .
G e n e / s y s t e m
V a r i a n t
A u t h o r
S t u d y g r o u p a n d m e t h o d s
i n b r i e f
E x a m p l e s
o f c l i n i c a l c o n s e q u e n c e s
R e f .
C a t e c h o l - O -
m e t h y l t r a n s f e r a s e
( C O M T )
C O M T S N P s a n d
h a p l o t y p e s
H e n k e r e t a l . ( 2 0 1 2 )
O r t h o
p e d i c t r a u m a s u r g e r y
G e n e t i c v a r i a t i o n s i n C O M T g e n e ( r s 4 8 1 8 , r s 4 6 8 0 a n d
h a p l o t y p e ‘ G C G G ’ ) c o n t r i b u t e t o t h e a c u t e p o s t o p e r a t i v e p a i n
a n d a n a l g e s i a a n d o p i o i d c o n s u m p t i o n
[ 5 3 ]
H i c k e y e t a l . ( 2 0 1 1 )
M a s t e
c t o m y w i t h r e c o n s t r u c t i o n
A t r e n d t o w
a r d s a n a s s o c i a t i o n b e t w e e n C O M T V a l 1
5 8 M e t a n d
p e r s i s t e n t p
o s t o p e r a t i v e p a i n
[ 5 4 ]
D a i e t a l . ( 2 0 1 0 )
S p i n e
s u r g e r y f o r d e g e n e r a t i v e
d i s k d
i s e a s e
T T a l l e l e o f S N P r s 4 6 3 3 a l o n g w i t h a c o m m o n h a p l o
t y p e ‘ A T C A ’
w e r e a s s o c i a t e d w i t h g r e a t e r 1 - y e a r p o s t o p e r a t i v e O
s w e s t r y
D i s a b i l i t y I n d e x s c o r e s
[ 5 2 ]
L e e e t a l . ( 2 0 1 1 )
T h i r d m o l a r e x t r a c t i o n
A d e q u a t e p
o s t o p e r a t i v e a n a l g e s i a w a s g r e a t e r a m o n
g s t t h o s e
w i t h t h e G G
g e n o t y p e f o r e i t h e r r s 4 8 1 8 o r r s 6 2 6 9
[ 5 0 ]
G e o r g e e t a l . ( 2 0 0 8 )
S h o u l d e r s u r g e r y
P a i n c a t a s t r o p h i z i n g a n d C O M T d i p l o t y p e w e r e a s s o
c i a t e d w i t h
h i g h e r p o s t o p e r a t i v e p a i n r a t i n g s
[ 5 1 ]
µ - o p i o i d r e c e p t o r
g e n e ( O P R M 1 )
A 1 1 8 G
C h o u e t a l . ( 2 0 0 6 )
J a n i c k i e t a l . ( 2 0 0 6 )
S i a e t a l . ( 2 0 0 8 )
F u k u d a e t a l . ( 2 0 0 9 )
S e e T A B L E
1
[ 1 0 4 , 1
0 5 ,
1 7 6 , 1
7 7 ]
2 0 S N P s i n c l u d i n g
r s 6 3 4 4 7 9 ,
r s 4 9 9 7 9 6 , r s 5 4 8 6 4 6
r s 6 7 9 9 8 7 a n d h a p l o t y p e s
O c h r o c h e t a l . ( 2 0 1 1 )
P o s t - t h o r a c o t o m y p a i n
O P R M 1 S N P
s r s 6 3 4 4 7 9 , r s 4 9 9 7 9 6 , r s 5 4 8 6 4 6 a n d
r s 6 7 9 9 8 7 w
e r e a s s o c i a t e d w i t h p o s t o p e r a t i v e p a i n
[ 1 0 9 ]
3 0 4 A > G
L a n d a u e t a l . ( 2 0 0 8 )
A n a l g
e s i a a f t e r i n t r a t h e c a l
f e n t a n
y l i n l a b o r i n g w o m e n
G v a r i a n t f o
u n d m o r e r e s p o n s i v e t o o p i o i d s
[ 1 7 8 ]
G T P c y c l o h y d r o l a s e
( G C H 1 )
G C H S N P s
K i m e t a l . ( 2 0 1 0 )
F u n c t i o n a l o u t c o m e a f t e r s p i n e
s u r g e r y
T a l l e l e a t r s
9 9 8 2 5 9 o f G C H 1 w a s a s s o c i a t e d w i t h i m
p r o v e d
1 - y e a r p o s t o p e r a t i v e O s w e s t r y D i s a b i l i t y I n d e x s c o r e s
[ 2 5 ]
M e l a n o c o r t i n
r e c e p t o r ( M C 1 R )
R 1 5 1 C
R 1 6 0 W
D 2 9 4 H
M o g i l e t a l . ( 2 0 0 3 )
R e s p o
n s e t o p e n t a z o c i n e w a s
e v a l u a
t e d a m o n g f e m a l e s
W o m e n w i t
h M C 1 R v a r i a n t s h a d g r e a t e r a n a l g e s i a f r o m
k - a g o n i s t , p
e n t a z o c i n e
[ 7 4 ]
M o n o a m i n e o x i d a s e
( M A O )
M A O B ( i n t r o n 1 3 A > G )
M A O A ( e i g h t S N P s ) ,
M A O B ( t h r e e S N P s )
S e r y e t a l . ( 2 0 0 6 )
P o s t - t o n s i l l e c t o m y p a i n
G a l l e l e i n m
a l e s a s s o c i a t e d w i t h h i g h e r p a i n s c o r e s
[ 1 7 9 ]
K i m e t a l . ( 2 0 0 6 )
P o s t o p e r a t i v e p a i n a f t e r o r a l
s u r g e r y i n E u r o p e a n A m e r i c a n s
N o s i g n i fi c a
n t a s s o c i a t i o n w i t h a c u t e p a i n r e s p o n s e
[ 1 8 0 ]
G I R K : G - p r o t e i n - a c t i v a t e d i n w a r d l y r e c t i f y i n g p o t a s s i u m c u r r e n t ; K C N : P o t a s s i u m c h a n n e l ; R A : R e
c e p t o r a n t a g o n i s t .
-
8/17/2019 Sad Ha Sivam 2012
11/22
www.futuremedicine.com 1729future science group
Perioperative pain & pharmacogenomics of opioids REVIEW
T a b l e 2 . E f f e c t s o f g e n e t i c v a r i a n t s o n p e r i o p e r a t i v e p a i n a n d r e s p
o n s e s t o o p i o i d s ( c o n t . ) .
G e n e / s y s t e m
V a r i a n t
A u t h o r
S t u d y g r o u p a n d m e t h o d s
i n b r i e f
E x a m p l e s
o f c l i n i c a l c o n s e q u e n c e s
R e f .
I n t e r l e u k i n s o r I L - R A
I L - 1 b
- 5 1 1 C > T , I L - 1 R A
8 6 b p V N T R
B e s s l e r e t a l . ( 2 0 0 6 )
P a i n s c o r e s a n d m o r p h i n e
c o n s u m p t i o n a f t e r h y s t e r e c t o m y
i n J e w
i s h p a t i e n t s
I L - 1 R A S N P m a y c o n t r i b u t e t o v a r i a t i o n i n p o s t o p e r a t i v e
m o r p h i n e c o n s u m p t i o n
[ 1 8 1 ]
C a n d i o t t i e t a l . ( 2 0 1 1 )
O p i o i d c o n s u m p t i o n a n d p a i n
s c o r e s
i n 9 6 p a t i e n t s u n d e r g o i n g
n e p h r
e c t o m y
P a t i e n t s h o m o z y g o u s f o r t h e I L 1 R N * 1 a l l e l e h a v e l o w
e r
c o n c e n t r a t i o n s o f I L - 1 R A a n d r e q u i r e h i g h e r d o s e s o f o p i o i d s
p o s t o p e r a t i v e l y t h a n p a t i e n t s c a r r y i n g a t l e a s t o n e I L
1 R N * 2
a l l e l e
[ 6 8 ]
S o l u t e c a r r i e r o r g a n i c
a n i o n t r a n s p o r t e r
( S L C )
S L C 6 A 2
( n o r e p i n e p h r i n e )
S L C 6 A 3
( d o p a m i n e )
S L C 6 A 4
( s e r o t o n i n )
K i m e t a l . ( 2 0 0 6 )
P a i n s c o r e s , a n a l g e s i c n e e d p o s t -
o r a l s u r g e r y i n C a u c a s i a n s
W e a k a s s o c
i a t i o n s o f r s 4 0 4 3 4 i n S L C 6 A 2 a n d r s 2 0 6 6 7 1 3 i n
S L C 6 A 4 w i t h p a i n r e s p o n s e
[ 1 8 0 ]
G e n e c o d i n g G I R K
( K C N J 6 )
N i n e S N P s
N i s h i z a w a e t a l . ( 2 0 0 9 ) A n a l g
e s i c r e q u i r e m e n t a f t e r
a b d o m
i n a l s u r g e r y
T h e A / A g e n o t y p e i n t h e A 1 0 3 2 G S N P a n d - 1 2 5 0 G / 1
0 3 2 A
h a p l o t y p e h
a d s i g n i fi c a n t l y i n c r e a s e d p o s t o p e r a t i v e o p i o i d
r e q u i r e m e n t s
[ 1 1 2 ]
G I R K : G - p r o t e i n - a c t i v a t e d i n w a r d l y r e c t i f y i n g p o t a s s i u m c u r r e n t ; K C N : P o t a s s i u m c h a n n e l ; R A : R e
c e p t o r a n t a g o n i s t .
-
8/17/2019 Sad Ha Sivam 2012
12/22
Pharmacogenomics (2012) 13(15)1730 future science group
REVIEW Sadhasivam & Chidambaran
dose of morphine to her newborn through herbreast milk (70 ng/ml of morphine compared with a typical morphine range of 0.2.2 ng/ml in
breast milk), which resulted in death of theneonate [138]. The FDA provided a warning oncodeine following the death of a breastfed neo-nate of an UM mother [202]. Recently, the FDAprovided another warning that codeine use incertain children after tonsillectomy and/or ade-noidectomy may lead to rare, but life-threaten-ing adverse events or deaths related to CYP2D6 genetic variations [203]. Although cost prohibitivefor routine use, these fatal cases emphasize theimportance of CYP2D6 testing before adminis-tering drugs such as codeine. Tramadol, a semi-
synthetic codeine derivative [139], hydrocodone[140,141] and oxycodone [116,142] are also convertedto their more potent analgesic metabolites byCYP2D6. Tramadol is converted into O -des-methytramadol by CYP2D6, which has higherµ-agonist effects [143]. In PMs, even though tra-madol’s analgesic effect is not fully abolished,patients require two-times more rescue analge-sia [144]. Zwisler et al. proposed a hypoalgesiceffect of oxycodone in human experimental painmodels based on CYP2D6 phenotypes [142] butin a later study of 217 patients undergoing thy-
roid surgery, the authors found no difference in
postoperative oxycodone requirement amongUM and PM CYP2D6 phenotypes and con-cluded that this gene does not signicantly affect
oxycodone effects [145].Despite increasing evidence for the clini-
cal value of CYP2D6 genetic tests for codeine,pharmacogenetic tests such as CYP2D6 are notreadily being adopted into clinical practice dueto inconsistent evidence, cost, limited access togenetic testing and absence of peer-reviewed andstandard guidelines to facilitate personalizedcare. The Clinical Pharmacogenetics Implemen-tation Consortium (CPIC), which was devel-oped to create peer-reviewed, evidence-based,freely accessible guidelines, recently published
codeine-related guidelines, which will help clini-cians to select appropriate opioid and avoid sub-optimal opioids for given CYP2D6 metabolizerstatus [146].
UDP-glucuronosyltransferaseMorphine is metabolized in the liver to activemetabolites morphine-6-glucoronide and mor-phine 3-glucoronide by UGT2B7. UDP-gluc-uronosyltransferases are glycoproteins, local-ized in the endoplasmic reticulum and nuclearmembranes and the 2B7 isoform participates in
the glucuronidation of steroid hormones, bile
Table 3. Ethnicity and allele frequencies of genetic polymorphisms influencing opioids.
Ethnicity OPRM1A118G [85]
COMT
Val158Met [44]UGT2B7
161C/T and802C/T [150]
ABCB1
C3435T [163]CYP2D6
UM (%) [128]
European–American/
Caucasian
0.154 Val/Val: 0.226
Val/Met: 0.566
Met/Met: 0.208
C: 0.511, T: 0.489
C: 0.463, T: 0.537
C/C: 0.24
C/T: 0.48
T/T: 0.28
1–4
African–Americans 0.047 Val/Val: 0.358
Val/Met: 0.567
Met/Met 0.075
C: 0.68, T: 0.32 C/C: 0.68
C/T: 0.31
T/T: 0.01
1–4
Hispanic 0.14 Val/Val: 0.316
Val/Met: 0.447
Met/Met: 0.237
NA NA NA
Japanese 0.485 NA C: 0.732, T: 0.268 NA NA
Ashkenazi Jewish 0.210 NA NA NA NA
Saudi NA NA NA C/C: 0.37
C/T: 0.38
T/T: 0.26
20
Ethiopian 0.17 NA NA NA 29
Asian NA Val/Val: 0.395
Val/Met: 0.526
Met/Met: 0.079
C: 0.734
T: 0.266(southwest Asians)
C/C: 0.15, C/T: 0.38,
T/T: 0.47
NA
Chinese NA NA NA C/C: 0.32, C/T: 0.42,
T/T: 0.26
NA
Frequency of UMs is expressed as a percentage. Allelic frequencies of other polymorphisms are expressed as fractions between 0 and 1.NA: Not available; UM: Ultrarapid metabolizers.
-
8/17/2019 Sad Ha Sivam 2012
13/22
www.futuremedicine.com 1731future science group
Perioperative pain & pharmacogenomics of opioids REVIEW
acids, retinoids, fatty acids, in addition to itsrole in metabolizing opioids and nonsteroidalanti-inammatory drugs. Among a populationof 239 Norwegian cancer patients, 12 SNPs inthe UGT2B7 gene were investigated and foundto have no signicant impact upon the patients’
morphine glucuronide to morphine serum ratios[147]. However, in patients receiving morphinethrough patient-controlled analgesia, variationsin the UGT2B7 gene correlated with morphineand its metabolite concentrations in serum.The -161C/T promoter variant was found tobe in complete linkage disequilibrium with the802C/T variant and was noticeably more fre-quent in low glucuronidators. M6G:morphineratios were studied and morphine levels wereincreased in the T/T group when compared withC/T and C/C groups suggesting greater metabo-
lism in the T/T patients. M6G and morphine-3-glucuronide were signicantly lower in C/Cpatients compared with C/T and T/T patients[148]. The frequency of nausea was found to behigher in patients without UGT2B7*2 allelein a recent study of morphine side effects incancer patients [149]. Haplotype analysis of theUGT2B7 gene in Japanese patients suggestsdifferences with other ethnic groups [150].
In our own clinical research in childrenreceiving morphine perioperatively, we observedthat African–Americans had higher morphineclearance than Caucasians and that common
UGT2B7 genetic variations (-161C>T and802C>T) were not associated with observedracial differences in morphine’s clearancealthough the wild-type of the UGT2B7 isozymeis more prevalent in the African–Americans [151].
Ancestry & opioid managementGiven the common origins of all members of ourspecies [152], the denition of ancestry is oftenequated with geographic regions, race (basedon physical characteristics) or sociocultural fac-tors dening ethnicity [153,154]. Interethnic dif-
ferences in polymorphisms of genes encodingdrug-metabolizing enzymes, transporters andreceptors have been observed [155]. Genetic epide-miologists interested in identifying genetic asso-ciations with diseases or drug responses oftenseek to employ methods of ancestry inferencefor specic analytical reasons: either to con-trol for statistical biases related to populationstratication among study subjects or to mapsusceptibility variants better among recentlyadmixed groups. Ancestry information markers(AIMs) are a set of haploid markers (mtDNA
or Y-chromosome haplotypes) or multiple
unlinked autosomal markers that are diploidand exhibit substantially different frequenciesbetween populations from different geographi-cal regions. This is important for opioids. Forexample, A118G is the most commonly testedOPRM1 SNP. The allelic frequency of 118G is
close to 50% in Asians compared with 10–15%in Caucasians and Africans (T ABLE 3 ). SimilarlyCYP2D6 UMs are very frequent in north Afri-cans (>25%) compared with Caucasians (3–5%)as drug toxicities such as codeine-related respi-ratory depression and death are expected to bemore frequent in UMs. In our own research, we observed the origin of ancestry (African orEuropean) or race was associated with differentrates of morphine clearance, postoperative painand opioid-related adverse effects in childrenundergoing surgery [49,151]. By using a number of
AIMs, one can estimate the geographical originsof the ancestors of an individual and ascertain what proportion of ancestry is derived from eachgeographical region.
Opioid transport n MDR1 gene codes for analgesic
efflux transportMDR1 (or ABCB1) is located on chromo-some 7 and includes 28 exons consisting of3843 bp [156]. This gene codes for P-glycoprotein(P-gp), an important efux transporter at theblood–brain barrier [157]. Variations in ABCB1 gene can affect the efux transporter functionat the blood–brain barrier and signicantly altercerebral pharmacokinetics of substrate opioidsby restricting their uptake or enhancing theirclearance from the brain into the blood. P-gphas been one of the most highly studied drugtransport proteins and is believed to be a majorregulator of drug transport, especially in causingmultidrug resistance to cancer therapies [156,158–160]. Genetic variability in ABCB1 also inuencesdaily methadone dosage, further indicating itsimportant role in opioid drug transport and cor-
responding drug actions and adverse effects [161].The 1236C>T, 2677G>T/A and 3435C>T
SNPs, the most common variants in the cod-ing region of ABCB1, are in strong linkage dis-equilibrium. The CGC haplotype ( ABCB1*1)and TTT ( ABCB1*13) haplotypes show dif-ferent mRNA stability, but only the 3435C>T was found to have signicantly higher mRNAexpression encoding for P-gp resulting in morethan fourfold lower P-gp expression than theCC [162,163]. ABCB1 GG–CC diplotype at the3435 and 2677 SNPs was the only borderline
signicant indicator of morphine side effects as it
-
8/17/2019 Sad Ha Sivam 2012
14/22
Pharmacogenomics (2012) 13(15)1732 future science group
REVIEW Sadhasivam & Chidambaran
decreased the need for ondansetron for postoper-ative nausea or vomiting [106]. Among 145 adultpatients of Italian descent treated with mor-phine, those with the polymorphisms C3435T
of ABCB1 and A80G of OPRM1 were associated with signicant pain relief variability [164]. Thestudy authors reported that on combining theextreme genotypes of both genes, the associa-tion between patient polymorphism and painrelief improved with allocation of patients intothree groups: strong responders, responders andnonresponders, with sensitivity close to 100%and specicity of more than 70% [164]. Simi-larly, among 146 adult Korean patients treated with fentanyl, ABCB1 1236T and 3435T allelesshowed a signicant difference in the level of
respiratory suppression [165]. In another clinicalstudy investigating morphine-related adverseevents in 32 Japanese cancer patients receivingoral controlled release morphine tablets, theT/T genotype at 1236 or TT/TT diplotype at2677 and 3435 in ABCB1 was found to be asso-ciated with signicantly lower fatigue and thefrequency of vomiting [149].
Various ethnic differences have been foundto exist in the ABCB1 gene (T ABLE 3 ). Compar-ing Europeans and African–Americans, tenSNPs with different frequencies were iden-
tified. Two synonymous SNPs C1236T in
exon 12 and C3435T in exon 26 and one non-synonymous SNP G2677T in exon 21 werefound to be linked as ABCB1*2 , occurring in62% of European–Americans but only 13%of African–Americans. The *1/*1 genotypeexpresses decreased P-gp activity compared with
the ABCB1*2/*2 or *1/*2 alleles [166]. Hence, the African population is more likely to have greaterP-gp expression and thereby reduced responseto analgesic drugs due to increased efux acrossthe blood–brain barrier. Ashkenazi Jewish indi- viduals were more likely to have more T allelesthan Caucasians [167] suggesting that the lowerP-gp expression may cause adverse effects andincreased analgesic response from drug therapy.Many of the P-gp substrates are also substratesof the drug-metabolizing enzyme CYP4503A4and are found in lymphocytes. Therefore, other
drugs acting as substrates and the immune sys-tem’s regulation of lymphocytes are likely tohave an effect upon analgesics that are absorbedby the P-gp [158].
In our prospective clinical study of childrenundergoing adenotonsillectomy, we observedthat the ABCB1 gene had strong associations with opioid-induced central side effects, respi-ratory depression and postoperative nausea and
vomiting; the odds of having respiratory depres-sion and postoperative nausea and vomiting withTT genotype of the ABCB1 SNP, rs1045642 wastwo- to ten-times higher compared with TC and
CC genotypes [S S, U D].
Gene–gene interactions & opioideffectsThere are not many reports assessing mul-tiple gene effects and gene–gene interactionson opioid effects. Reyes-Gibby et al. studiedthe combined effects of OPRM1 and COMT variations in patients with chronic cancer painand found that carriers of the OPRM1 A118G and COMT Met/Met genotype required thelowest morphine dose [45]. A study of surgical
pain in 102 patients undergoing abdominalsurgery showed that the heterozygous patientsof OPRM1 A118G and COMT Val/Met SNPsrequired signicantly less morphine compared with homozygous patients [168]. Nausea andsedation scores were also signicantly lower dur-ing the postoperative period for heterozygouspatients [168]. Zwisler et al. studied antinocicep-tion and adverse drug reactions with oxycodoneafter experimental pain in 33 human volunteersand found reduced antinociception in OPRM1 118G carriers and less side effects in the com-
bined wild-type genotype 3435CC–2677GG for
Less opioid-associated
side effects
Excellent pain relief
from opioids
COMT, OPRM1, ABCB1and exploratory SNPs
Age, sex, race andother predictive factors
G e n e C h i p
G e n e C h i p
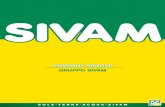
Figure 2. Personalized opioid pain management. Taking into account clinicallyrelevant genetic factors along with nongenetic factors in pain management withopioids may help optimize analgesia and minimize serious adverse effects ofopioids.
-
8/17/2019 Sad Ha Sivam 2012
15/22
www.futuremedicine.com 1733future science group
Perioperative pain & pharmacogenomics of opioids REVIEW
ABCB1 [169]. When they tried to replicate theirresults in 268 patients who received intravenousoxycodone analgesia for postoperative pain, they were unable to conrm similar associations [170]. Although this study had drawbacks associated with the surgical pain being low intensity and
no control for comedications, which could affectP-gp function, it points to the inconclusivenessof available research data.
ConclusionPain and analgesia are complex, dynamic andmultifactorial phenomena, further complicatedin children due to associated physiological,developmental and emotional factors. Pharma-cogenetics of opioids and genetics of pain per-ception offer new insights into the mechanismsof pain and differences in an individual patient’s
responses to pain medications, such as opioids,used in the perioperative setting. However, theuse of genetic approaches to studying clinicallymeaningful outcomes are complicated and lim-ited by many factors, including lack of large sam-ple sizes needed, population stratication, publi-cation bias, expense of genetic testing in a large
sample, statistical and bioinformatics analyticalchallenges, gene and environmental interactions, validation of genetic associations by mechanis-tic studies and independent research groups andnally incorporation of genetic information topersonalize clinical care.
In the setting of ethical and other challenges with surgica l pain related to pharmacogeneticstudies in healthy volunteers, relatively healthychildren (with less interferences from epigeneticsand environmental factors than adults) undergo-ing surgery offer unique opportunities to studythe roles of genetic factors. In our ongoing largepediatric surgical pain and opioid pharmaco-genetic research, we were able to identify novelgenetic and nongenetic risk factors (e.g., race)for opioid-related analgesia and serious adverseeffects, which are important steps towards
personalizing perioperative care. Appropriategenetic tests in childhood might be useful life-long for genotype-based clinical outcome predic-tions and appropriate interventions. In addition,the study of developmental pharmacogeneticspertaining to analgesics/pain response andinheritance of genetic characteristics/phenotypes
Engaging physicians and medical community
E n g a g i n g p a t i e n t s a n d p u b l i c
Engaging policy-makers
Publications
resource informationand education
E d u c a t i o n a n d
s o c i a l m a r k e t i n g
E n g a gi n g
p a y er s , p er s on al i z e d m e d i c i n e an d ph ar m
a c e u t i c al i n d u s t r y
Personalizedanalgesia
Personalized healthoutcome improving
economic and societalimpact
E v i d en c e s of o u t c om e
i m pr ov em en t
I n t el l e c t u al pr o p er t y
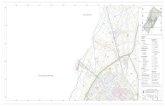
Figure 3. Personalized analgesia: making the connection. To personalize pain managementeffectively, prediction based on genetic and nongenetic factors and their interactions are theimportant first step. Making the connection with other important players such as pharmacy,pharmaceutical industry and healthcare payers are equally essential to make personalized analgesiaeasily adaptable in clinical practice.
-
8/17/2019 Sad Ha Sivam 2012
16/22
Pharmacogenomics (2012) 13(15)1734 future science group
REVIEW Sadhasivam & Chidambaran
may be easier to conrm by recruitment ofchildren and their parents.
Genetic and pharmacogenetic studies alsoneed to incorporate the integration of proteomic,transcriptomic and metabolomic information when appropriate to improved personalized care
and outcomes. Large studies with appropriatepopulation stratication accounting for multiplegenes, their interactions along with nongeneticrisk factors associated outcomes are needed tomove towards personalized care and pain man-agement. Merging many studies with differentpopulations into a meta-analysis to get a largesample size without paying consideration to thestudy populations’ ethnic/racial and geographi-cal background, other known important geneticand nongenetic risk factors associated with out-comes, and gene–gene interactions may not
result in clinically meaningful information.In the eld of pain and pain management,genetic variations seem to play a major role indetermining clinical and economic outcomes.In addition, genetic-association studies willhelp identify patients at risk of PPP. The knowl-edge gained could help develop new and tar-geted therapies to optimize postoperative pain
management and reduce the burden due to pain. We have made a good start in identifying someof the genetic determinants relevant to periop-erative pain management in children and more work needs to be done to translate the promiseof personalized pain management to clinical
practice.
Future perspective of personalizedanalgesia research: promise topracticeSimilar to the Global Positioning System weoften use to navigate roads, a Genomic Prescrib-ing System (GPS) to guide therapy and person-alize care had been suggested [171]. Pre-emptiveprediction and identication of patients at higherrisk of inadequate pain control and opioid-relatedadverse effects is essential in tailoring pain man-
agement(FIGURE 2)
. To give an example of clinicaltranslation of genotype-directed therapy, Lötschet al. have suggested a simple genotype-based per-sonalized dosage based on OPRM1, COMT andMCR1 genotypes [172], though these have neitherbeen validated nor clinically practiced [173]. Inorder to reach the goal of incorporating phar-macogenetic ndings into clinical practice, there
Genomics
Pharmacy
Public
healthpolicy
Clinical riskfactors
Medical
informatics
Pharmaceutical
industry
Personalizedanalgesia
Payers andinsuranceindustry
Figure 4. Personalized opioid analgesia: promise to practice and policy. Personalized analgesiais realizable with continuous high-quality research. Patients and clinicians need to be engaged asearly adaptors to build additional evidence of clinical and economic outcome improvements, whichwill help engage the pharmaceutical industry, third party payers and policy-makers to bring thepromise of personalized analgesia to day-to-day clinical practice.
-
8/17/2019 Sad Ha Sivam 2012
17/22
www.futuremedicine.com 1735future science group
Perioperative pain & pharmacogenomics of opioids REVIEW
Executive summary
Pain perception & genetics
Pain is a complex neurophysiological condition involving endogenous opioids and various neurotransmitters such as epinephrine,
norepinephrine and dopamine. Pain management in children is fur ther complicated due to associated physiological, developmental
and emotional factors affecting pediatric pain perception and response to opioids.
Low COMT activity results in elevated levels of catecholamines and increased pain sensitivity, and may play a role in persistent pain
after surgery. Different combinations of COMT SNPs (rs6269, rs4633, rs4818 and rs4680) define distinct haplotypes that have beenfound to be predictive of specific levels of pain response.
Genetic variations of proinflammatory cy tokines such as IL-1 receptor antagonist and IL-6 have been shown to affect pain
sensitivity.
Pain sensitivity appears to differ among the genders (women tend to have higher pain sensitivity with different coping mechanisms
compared with men), races (African–American children have higher postoperative pain compared with Caucasians) and ethnicity
(the frequency of OPRM1 polymorphisms is approximately 46% among Asians, but only 5 and 25% in European and African–Americans populations, respectively). Ancestry information markers could be used to identify differences in allele frequency
between populations from different geographical regions.
Pharmacogenetics of opioid analgesia & opioid-related adverse effects
There is a significant genetic variation effect on opioid-related respiratory depression, nausea and drug disliking.
The most studied genetic variation in the OPRM1 receptor gene is the A118G SNP, with increased postoperative opioid
requirements and reduced side effects reported in the GG homozygotes compared with the AA genotypes, although the
observation has not been consistent. Deaths in children due to codeine highlight the importance of CYP2D6 genetic tests and avoidance of opioids metabolized by theCYP2D6 pathway in ultrarapid and extensive metabolizing children. Responses to tramadol and possibly oxycodone and
hydrocodone may also be affected by CYP2D6 genotypes though studies are not consistent and therefore more evidence is needed.
P-glycoprotein (P-gp) is an important efflux transporter for opioids such as morphine and methadone, and is regulated by the
ABCB1 gene. The 1236C>T, 2677G>T/A and 3435C>T SNPs, the most common variants in the coding region of ABCB1, have beenimplicated in variations in opioid analgesia and side effects such as vomiting and respiratory depression.
Multiple genetic effects require a detailed analysis of gene–gene interactions, a holistic approach integrating genetic, proteomic,
transcriptomic and metabolomic information, robus