Resectional Anatomy of Pancreas
34
Resectional Anatomy of Pancreas Dr Happy D Kagathara 4 th January, 2015 CME – Management of Pancreatic Neoplasms Ahmedabad Surgeon’s Association
-
Upload
happy-kagathara -
Category
Health & Medicine
-
view
43 -
download
4
Transcript of Resectional Anatomy of Pancreas

Resectional Anatomy of Pancreas
Dr Happy D Kagathara4th January, 2015
CME – Management of Pancreatic Neoplasms
Ahmedabad Surgeon’s Association

Outline
• Gross anatomy– Gland– Vascular anatomy– Lymphatic drainage– Ductal anatomy
• Approach for resection– Pancreatico-duodenectomy– Distal pancreatectomy

Introduction
• Pancreatic surgery– Complicated and technically challenging– Requirement of detailed understanding of anatomy and relation to
adjacent structures• Casual observer assumed that pancreas played an insignificant role
– First discovery • By Herophilus• Referred to as the “finger of the liver”, between 200 BC and 200
AD– 400 years later, Ruphos, gave the name “pancreas” (“all flesh” In
Greek)– Grey’s Anatomy (1901 edition) – “Pancreas presents but little of
surgical importance– Whipple, surgery for pancreatic neoplasm in 1930

Gross anatomy
• Soft, elongated, flattened• Length – 4 to 6 inches• Weight – 92 gm (41 to 182 gm)• Oblique location
– Epigastric & left hypochondriac regions– T12/L-1 to L-3
• No true capsule, covering of fine connective tissue • Arbitrary division

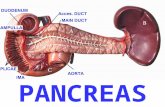
Gross anatomy: Head
Lies within the C-shaped concavity of the duodenum2 surfaces: anterior and posterior
The anterior surface is adjacent to the pylorus, the first part of
the duodenum, and the transverse colon and crossed by the attachment of the root of the transverse mesocolon. The posterior surface
abuts the right kidney, the inferior vena cava and the right renal vessels, and the right crus of the diaphragm.

Gross anatomy: Uncinate Process
• Projection from the lower part of the head• Extending upward and to the left• Lies posterior to SMA and SMV• Lies anterior to aorta and the inferior vena cava• Variable size• SMA give branches into and SMV receive tributaries from the uncinate
process

Gross anatomy: Neck
Constricted part1.5 to 2.0 cm long and 3.0 to 4.0 cm wideFrom the head toward the leftExtends to the right as far as the ASPDA
Anterior surfaceLesser sac cavityPyloro-duodenal junctionGastroduodenal artery
Posterior surfaceconfluence of the SMV and SV, forming PVThe IMV is related to the inferior border and may pass behind it to enter the SV or turn medially to enter the SMV

Gross anatomy: Body
Prismoid shapeRuns toward the left sideAnterior surface abuts
The antrum and body of the stomach and the transverse mesocolonSuperior border related to
Coeliac trunk (runs forwards above)Splenic artery (runs to the left along this border)
Anterior border gives attachment to the transverse mesocolon.
Posteriorly related toThe aorta, origin of the SMA, the left crus of
the diaphragm, the left kidney and its vessels, the left adrenal gland, and the SVInferior surface
Covered by peritoneum of the greater sacDuodenum-jejunal flexureCoils of the jejunumLeft colic flexure
The middle part of the body overlies the lumbar spine, which makes this area of the pancreas most vulnerable to abdominal trauma

Gross anatomy: Tail
Relatively mobile, tapering endAbuts hilus of spleenRests on splenic flexurelies in the lineorenal ligament accompanied by the splenic vessels and lymphatics

Gross anatomy: Peritoneal Covering
• *Posterior 2 layers of the greater omentum divergeon the anterior surface of the head and the body– Anterior layer passes upwards and covers the
anterior surface– Posterior layer passes downwards and covers
the inferior surface• End of the tail within lienorenal ligament• Posterior surface is devoid of peritoneum
Vascular relations to IVC, left renal vein, aorta, celiac axis and branches, SMA, PV, SMV, SV make the pancreas prone for invasion by malignant pancreatic disease

Arterial circulation
• *The head and uncinate process – Supplied by the pancreatico-duodenal arcade
• On the anterior and posterior surface of the pancreas next to the duodenum
• Anterior arcade – closer to the duodenum• From the SPDA (branch of GDA) and IPDA (branch of the SMA)
• The second system from the SA– gives three arteries on the dorsal surface of the gland– The dorsal pancreatic artery
• Most medially• Right branch supplies the head and usually joins the posterior
arcade in the neck• one or two left branches make connections with branches of the
SA and the left gastroepiploic artery• In 1/3rd cases, tail of pancreas receives supply from left gastro-epiploic
artery
Two arterial systemFor head and uncinate processFor body and tailThe neck is a watershed between these two

Arterial circulation
The coeliac artery Rises vertically, close to the superior edge of the pancreasGives off the CHA-GDA and the SA
The splenic artery Run posterior to the body and tail
The SMA Rises posterior to the junction of the neck and body

Arterial circulation
• Inferior pancreatic artery*– 22% - absent IPA– 25% - body and tail supplied only by branches of IPA, increases risk of
pancreatic infarction if IPA thrombosed.• Inferior pancreaticoduodenal artery*
Continuation of dorsal pancreatic artery, within the pancreas, towards inferior margin
Landmark for pancreatic head resectionLigation of IPDA opens up plane for dissection for SMA, posterio-medial margin of resection

Venous drainage
• *The veins of the body and tail of the pancreas – Short and fragile– Drain into the SV
• The veins of head and uncinate process– The pancreaticoduodenal veins lie close to their corresponding
arteries– Drain into the SMV and PV– Invariable tributary entering the PV at the level of superior margin of
head• The veins from Uncinate process
– Drain into a large first jejunal vein, • abuts the uncinate process
– Empty into the SMV
Follows arterial supply

Venous drainage
• Splenic vein*– Because of the close anatomic relationship, inflammatory or
neoplastic diseases involving the body and tail can lead to SV occlusion resulting in retrograde venous drainage toward the splenic hilum and then, through the short gastric veins, can create gastric varicesOriginates at the hilum of the
spleen and run to the right along the posterior surface of the pancreas, partly embedded in the back of the pancreas

Venous drainage
• Inferior mesenteric vein– Normally not drain the pancreas*– If the termination of the SV is surgically occluded during a resection,
IMV may become a draining vein of the pancreas• Only when it drains into the SV
Related to the inferior border of the neck and may pass behind it to enter the SV or turn medially to enter the SMV or into the confluence

Lymphatic drainage
• *Standard node dissection during Whipple’s procedure– Removes all N1 nodes unless there is direct lymphatic drainage to the
left side of the SMA or to nodes around the coeliac artery• Anterior and posterior lymphatic system
– Run near the pancreaticoduodenal vessels. – Each drainage system has superior and inferior sub-systems
Understanding of drainage is important for accurately staging the disease and for achieving clearance to reduce risk of loco-regional recurrenceRing of nodes around the pancreas that drain the adjacent sections of the gland (N1). These nodes drain into nodes along the SMA, coeliac artery and aorta (N2, axial nodes).Axial nodes are also N1 for portions of the head, body and uncinate process that lie close to the aorta

Lymphatic drainage
• Head of the pancreas and duodenum– Upper head drains into subpyloric nodes– Inferiorly drains into retropancreatic and antepancreatic nodes– Into the celiac and superior mesenteric groups of pancreatic nodes
and into the cisterna chyli• Body of pancreas
– Drain into the pancreaticosplenic nodes • Lying along the superior border• Drain into celiac nodes
• Tail of the pancreas – drain into splenic hilar nodes

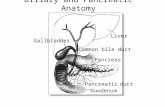
Ductal anatomy: PD
• The main pancreatic duct (of Wirsung)*– 3.1 - 4.8 mm in the head, tapers to 0.9 - 2.4 mm in the tail
• The uncinate process is served by its own duct– joins the main pancreatic duct 1–2 cm from its entry into the
duodenum.
Begins near the tail of the pancreas, courses left to rightFormed from anastomosing ductules draining the lobules of the gland

Ductal anatomy: PD
• The accessory pancreatic duct (of Santorini)– Present in 70%*– Drains into the minor papilla
• 2cm proximal to the ampulla of Vater in the second duodenum
Runs upwardsReceives ductules from the lower part of the headUsually communicates with the main duct

Ductal anatomy: PD
– No connection between the accessory duct and the main duct in 10%, Pancreatic divisum
– Only duct of Santorini in 2%

Ductal anatomy: Intrapancreatic CBD
• As CBD descends behind 1st part of duodenum, it becomes enclosed by (80%) or grooves (20%) the pancreas as it passes to exit at papilla.
Each duct and the common channel have their own sphincters

Ductal anatomy: Sphincter mechanism
– PD Joins CBD within the sphincter segment in 70% - 85%*• In sphincteroplasty, open the common channel superiorly (10–12 o’clock
position in the mobilised duodenum) to avoid the orifice of the pancreatic duct (4 o’clock)
– PD Enters the duodenum independently in 10% - 13%• Pancreatic duct more inferiorly
The length of the common channel 4.5 mm (1 to 12 mm)

Innervation
• Splanchnic nerve – sympathetic innervation• Vagus nerve – parasympathatic innervation• Both has efferent vasomotor fibers to the pancreatic acini, ducts and
blood vessels and afferent pain fiber
• Afferent pain fibers pass through the celiac plexus to cell bodies in dorsal root ganglia within the splanchnic nerves

Innervation
• Sympathetic efferent fibers– Pre-ganglionic fibers run through greater (T5-T10), lesser (T9-T11) and
least splanchnic nerves– To celiac and SMA ganglia– Post ganglionic nerve fibers reach pancreas by accompanying
branches of arteries• Parasympathetic efferent fibers
– Pre-ganglionic nerves from celiac division of the posterior vagal trunk– ganglia within pancreas– Postganglionic fibers terminates at pancreatic islet cells

Approach to pancreas (PD)
• Right subcostal incision with Midline extension• Entering the lesser sac
– Approach• Divide of the greater omentum below the gastroepiploic arcade,
or• Release of the greater omentum from its attachment to the
transverse colon– The anterior surface of the neck, body and tail are often visible but
may be obscured by congenital flimsy adhesions to the posterior wall of the stomach

Approach to pancreas (PD)
• Exposure of head– Mobilization of the right side of the transverse colon and hepatic
flexure inferiorly– Kocher maneuver (2nd part of duodenum)

Approach to pancreas (PD)
• Exposure of the neck– Division of the right gastroepiploic vein*– Division of anterior branch of IPDV at inferior border of body
– Normally no veins enter the SMV or PV from the posterior surface of the neck of the pancreas*
Crosses the inferior border of the pancreas to join with the middle colic vein to form the gastrocolic trunk, which then enters the SMV.
Most common site for venous bleeding in pancreatic surgery
Neck can be separated from the anterior surface of the SMV/PV in this avascular plane

Approach to pancreas (PD)
• Celiac axis stenosis– Important vascular consideration in pancreatic head resection– Liver more reliant on supply via GDA or anomalous HA– Temporarily occlude GDA before division to test that HA pulsation in
the porta is not lost*• Right gastric artery division and ligation
GDA or IPDA stumps are common sites for arterial bleeding in pancreatic surgery

Approach to pancreas (PD)
• Division of First two- three jejunal veins• Uncinate process dissection from above to below
– The veins from Uncinate process divided
• A soft pancreas + MPD with normal diameter– high risk for P-J anastomotic leakage
• Relatively high output of pancreatic juice

Approach to pancreas (DP)
• Exposure of body and tail– Splenic flexure mobilisation to expose lower pole of spleen, hilum and
pancreatic tail– Peritoneal incision along inferior border of body the pancreas

Access to pancreas (DP)
– Infereior mesenteric vein ligation (Try to preserve)– Division of splenic vessels along superior border of pancreas

Take home message
• Retroperitoneal organ divided into Head, uncinate process, neck, body, tail
• Detailed knowledge of anatomy and relation to surrounding visceral structures are important for better oncological outcome in pancreatic cancer surgery
• Understanding of lymphatic drainage is Important– For accurately staging– For achieving clearance to reduce risk of loco-regional recurrence

Take home message
• Arterial supply– Head and uncinate process
• Supplied by the pancreatico-duodenal arcade– Body and tail
• The second system arises from the splenic artery• Venous drainage
– Head and uncinate process• The pancreaticoduodenal veins lie close to their corresponding
arteries• Drain into the superior mesenteric vein (SMV) and portal vein (PV)
– Body and tail of the pancreas• Drain into the splenic vein