Radiology Lecture CXR.ppt [Read-Only] · 2018. 4. 3. · • Right lung lobes – Upper – Middle...
25
10/2/2014 1 Chest Radiology: A Systematic Approach Brian Wetzel ACNP Senior Instructor OHSU School of Medicine Department of Emergency Medicine Objectives •A systematic approach to evaluating CXRs •Identifying common pathology •Accurately identifying several “can’t miss” findings Basic Principles • Plain‐film radiographs – Depends on differences in radiographic density • Air • fat • Tissue (water) • Metal (bone) – Border sharp & well defined
Transcript of Radiology Lecture CXR.ppt [Read-Only] · 2018. 4. 3. · • Right lung lobes – Upper – Middle...
-
10/2/2014
1
Chest Radiology:A Systematic Approach
Brian Wetzel ACNPSenior Instructor
OHSU School of MedicineDepartment of Emergency Medicine
Objectives
•A systematic approach to evaluating CXRs
•Identifying common pathology
•Accurately identifying several “can’t miss” findings
Basic Principles
• Plain‐film radiographs– Depends on differences in radiographic density
• Air• fat• Tissue (water) • Metal (bone)
– Border sharp & well defined
-
10/2/2014
2
CXR: why get one?
• CXR is helpful in selected patients– Dyspnea– Cough– Hemoptysis – Fever– Chest pain– Thoracic trauma
CXR: why get one?
• Clinical decision rules developed to predict positive predictors
• Absence of fever, tachycardia, tachypnea, adventitious breath sounds decrease the likelihood of infiltrate to
-
10/2/2014
3
Chest X‐ray
• Standard view is Posterior‐anterior (PA) view and
• LEFT lateral view• Anterior‐posterior (AP) view used if pt too sick to stand– Heart is further away (distorted)
Systematic Approach
Generally least to most interesting1.Adequacy of the film2.Upper abdomen3.Thoracic cage (soft tissue and bones)4.Mediastinal structures5.Lungs
a. each individuallyb. comparison of both
-
10/2/2014
4
X‐ray Quality
1. Penetration – thoracic spine is just visible
2. Alignment – clavicles should be equal
3. Nothing is cut off – entire chest visualized
4. Sufficient Inspiration – 9 or 10 ribs seen
Upper abdomen
1. Right hemi‐diaphragm slightly elevated
2. Gastric bubble
3. No free sub‐diaphragmatic air
-
10/2/2014
5
Subdiaphramatic air
Thoracic Cage
• Scapula • Humerus• Shoulder joint• Clavicle • Ribs • Sternum• Thoracic spine
-
10/2/2014
6
Mediastinal Structures
• Mediastinum & heart
– Trachea (including carina) – Mediastinal widening (> 8cm = pathology)– Cardiac borders– Cardiothoracic ratio (> ½ the width of the thorax = cardiomegaly)
• Hila
Left ventricle
Aortic knob
Right atrium
-
10/2/2014
7
Cardiothoracic ratio
Lungs
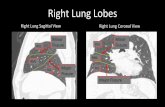
• Right lung lobes– Upper– Middle– Lower
• Left lung– Upper– Lingula (lower portion of upper lobe)– Lower
Lungs
• Lung markings well defined• Compare for symmetry• Various shades of Opacities
– Alveolar or interstitial process• Volume loss• Hyperinflation • Pleural surfaces
– Effusion, pneumothorax
-
10/2/2014
8
Left ventricle
Aortic knob
Right atrium
Normal Chest X‐Ray
-
10/2/2014
9
Case #1
– 53 y/o female c/o fever, productive cough, DOE, right sided pleuritic chest pain.
– No Pmhx, – Soc. Hx smokes
– 38.5, 102, 20, 94%, 120/71– Scattered rales heard on the right
-
10/2/2014
10
Case #2
– 60 y/o male c/o fevers, productive cough (no blood), pleuritic chest pain for 2 weeks. Alcohol binge; 14 pound weight loss
– Soc Hx: alcoholic, homeless– PMHx: HIV not on ART– VS 112/78 HR 110 RR 20 T 38 O2 sat 93%
-
10/2/2014
11
Case #3
– 72 y/o male right sided CP worse over last several months, new onset dry, hacking cough, sputum blood streaked, (+) malaise
– Denies SOB, fever, recent URI symptoms – 2 pack cigarettes per day for 40 years– VS 37.2, HR 72, R 12, 135/85 92%– Crackles right upper lung
-
10/2/2014
12
Case #4
– 62 y/o female presents to clinic with c/o SOB at rest x 1 week. Productive cough. No hemoptysis.
– Recent URI. No fevers.– Long smoking hx – Exam: T 37, HR 105, BP 150/85, RR 24, O2 89%– Expiratory wheezes with poor air movement
-
10/2/2014
13
Case #5
– 29 y/o male left sided CP worse over last several days, no known trauma or overuse injury
– Denies SOB, fever, fatigue – 1 pack cigarettes per day for 15 years– VS 37.2, HR 105, R 12, 135/85 92%– Diminished breath sounds left upper lung
-
10/2/2014
14
Case #6
– 66 y/o female c/o progressively worsening SOB and cough over last several days with DOE, PND, and bilateral lower leg swelling
– Denies fever or recent illness– Pmhx: MI 2 yrs ago– VS 37.2, HR 105, R 18, 135/85 92%– Bibasilar rales
-
10/2/2014
15
Plain abdominal radiography
• Suspected perforation• Obstruction• Foreign body
Plain abdominal radiography
• Abdominal series– Supine & upright abdominal films
• Air‐fluid levels• Dilated loops of bowel
– Upright chest• Free air under the diaphragm • Abdominal pain may have intrathoracic disorder
Case Study
• Mrs. Obstruction– 72 y/o female c/o 3 day hx of constipation, diffuse abdominal discomfort, “bloating”, and nausea
– Pmhx: recently tx’d with vicodin s/p fall with foot fx
– VS 37.2, HR 90, R 18, 135/85 99%– Mildly distended, diffusely tender abdomen
-
10/2/2014
16
Extremity Films
Trauma• Fractures and dislocations
Foreign Bodies• Metal easily seen• Glass +/‐ visualized• Wood rarely seen
Standard and Supplementary Views
Standard View Supplement View
Shoulder AP views:Internal & Ext rotation
Y view of scapulaAxillary view
Elbow APLateral
Oblique views (2)Olecranon view
Wrist PA; LateralOblique
Scaphoid
Finger PA; LateralOblique
Thumb PA; Lateral True AP
-
10/2/2014
17
Upper Extremity Films
• Wrist and hand
1. Colles (distal radius)
2. Scaphoid
3. Boxer’s (5th metacarpal)
Colles Fracture
Scaphoid Fracture
• Common wrist injury
• Fall onto outstretched hand (typical)
• If missed, high risk of avascular necrosis
-
10/2/2014
18
Boxer’s Fracture
• Fracture of the 5th metacarpal
• Maximal acceptable angulation is 40 degrees
• Suspect “fight bite” with any break in skin
-
10/2/2014
19
Lower Extremity Fractures
• Ankle or Foot fractures
1. Jones fracture (transverse 5th metatarsal)2. Pseudojones (avulsion of 5th MT)3. Distal tibia/fibula fx’s4. Maisonneuve fractures5. Lisfranc fractures
Standard and Supplementary Views
Standard View Supplement View
Pelvis AP JudetInlet & outlet
Hip AP (pelvis)“frog leg”
Cross-table lateralOblique view
Knee APLateral
“Sunrise”Notch view
Ankle AP; LateralMortise
Oblique
Foot AP; LateralOblique
Calcaneal views
Ottawa Knee Rules
• Patient’s age 55 years or older• Tenderness at head of the fibula• Tenderness of the patella• Inability to flex to 90 degrees• Inability to bear weight for four steps both immediately and in the ED
(Stiell IG, et al., Prospective validation of a decision rule for the use of radiography in acute knee injuries. JAMA, 1996)
-
10/2/2014
20
Ottawa Ankle Rules
• Bone tenderness– Posterior edge of either lateral or medial malleolus
• Tenderness at the anterior aspect of the distal fibula – common in ankle sprains
– Midfoot• Navicular• Base of 5th metatarsal
• Inability to bear weight– Both immediately or in the ED– Defined as ability to take 4 steps (even w/ limp)
(Stiell, IG, et al., Decision rules for use of radiography in acuteankle injuries: Refinement and prospective validation. JAMA, 1993).
Evaluating Ankle Films
1. AP View2. Lateral View3. Mortis 4. +/‐ Oblique
-
10/2/2014
21
Metaphyseal‐Diaphyseal Junction (Jones) Fracture
• Fracture extends across 5th metatarsal
• Mechanism: side to side motion (i.e. soccer/basketball players)
• High risk of nonunion due to blood supply
-
10/2/2014
22
-
10/2/2014
23
Salter‐Harris Classification
How to present your case
Describing a fracture
1. Clinical descriptors: age, gender, mechanism of injury, anatomic location, soft tissue involvement
2. Key physical exam findings: radiologic descriptors, type of imaging, anatomic location
3. Fracture pattern: relationship of fragments, physeal involvement, apophyseal disruption, joint involvement, soft tissue involvement
-
10/2/2014
24
References
•Goodman, L.R. Felson’s Principles of Chest Roentgenology. (2007) Third ed. W. B. Saunders Co.
•Google images
Disseminated bronchioloalveolar cell carcinoma
Cardiomyopathy
-
10/2/2014
25
Pulmonary edema
Community Acquired PNA