Protective role of folic acid in thyroxine-induced cardiac hypertrophy in hyperthyroid rat
7
Biomedicine & Aging Pathology 3 (2013) 89–95 Available online at www.sciencedirect.com Original article Protective role of folic acid in thyroxine-induced cardiac hypertrophy in hyperthyroid rat Ehab Tousson ∗ , Ezar Hafez , Ahmed A. Massoud , Osama Sweef , Nermin Atta Department of Zoology, Faculty of Science, Tanta University, Damanhour, Egypt a r t i c l e i n f o Article history: Received 5 February 2013 Accepted 8 March 2013 Available online 4 June 2013 Keywords: Hyperthyroidism Thyroxine Heart Myocardial hyperatrophy PCNA Immunohistochemistry a b s t r a c t Hyperthyroidism is a common metabolic disorder with prominent cardiovascular manifestation. It causes a hyperdynamic circulatory state because of a marked reduction in peripheral vascular resistance and an increased total blood volume and heart rate. We studied the changes in the heart structure of hyperthy- roid rat at the post-pubertal stage, in addition to the role of folic acid in treatment. Thirty male Wistar rats were equally divided into six groups; the first and second groups were the control and folic acid groups respectively while the third group was the hyperthyroid rat group; the fourth and fifth groups were co- and post-treated hyperthyroid rat with folic acid respectively and the sixth group was self-treated hyperthyroid rat group. Serum T 3 andT 4 levels were significantly increased while TSH levels were signifi- cantly depressed in rats receiving thyroxine indicating the induction of hyperthyroid state. Left ventricle section in the heart of hyperthyroid rats showed many abnormalities such as myocardial hyperatrophy, hydrophobic changes of myofibrillar structure with striations, and focal haemorrhage when compared with that in control. The PCNA label index in cardiac tissues was significantly increased in hyperthyroid rat (grade 4) and their levels were significantly decreased in co- and post-treated hyperthyroid rats with folic acid (grades 3 and 2 respectively) when compared with control (grade 0). Treatment of hyperthyroid rats with folic acid improves the histopathological alternation and the intensity of PCNA immunoreactive cells demonstrating the recovery of some injury. In conclusion, our results indicated that folic acid had ameliorative effect against cardiac hypertrophy induced by thyroxine and the best results were found in case of using the folic acid as an adjuvant therapy after returning to the euthyroid state. © 2013 Elsevier Masson SAS. All rights reserved. 1. Introduction Thyroid hormones have marked effects on the growth, devel- opment, and metabolic function of virtually all organs and tissues [1–12]. The action of thyroid hormone on the heart is mediated through a dual mechanism. The main mode of action is a direct effect on the transcription of specific and non-specific cardiac genes [13]. The second is a non-genomic action on plasma membranes, mitochondria, and the sarcoplasmic reticulum [14]. The heart is an organ sensitive to the action of thyroid hormone, and measurable changes in cardiac performance are detected with small variations in thyroid hormone serum con- centrations [10]. Hyperthyroidism is a disease in which tissues are exposed to high levels of thyroid hormones. Usually hyper- thyroidism will increase the thyroid hormones and decrease thyrotropin in serum is detectable [15]. Hyperthyroidism is present in 1.3% of the United States population (overt in 0.5% ∗ Corresponding author. Tel.: +201093905527. E-mail address: [email protected] (E. Tousson). and subclinical in 0.7%), and hypothyroidism in 4.6% of the population (overt in 0.3% and subclinical in 4.3%). Heart fail- ure occurs in 6% of hyperthyroid patients. Nonetheless, only half of those with hyperthyroidism-related heart failure have impaired left ventricular systolic function [16]. Hyperthyroidism is a common metabolic disorder with prominent cardiovascu- lar manifestations [17–19]. It causes a hyperdynamic circulatory state because of a marked reduction in peripheral vascular resistance and an increased total blood volume and heart rate [20]. Most patients with hyperthyroidism experience cardiovascular manifestations, and the most serious complications of hyperthy- roidism occur as a result of cardiac involvement. Recent studies provide important insights into the molecular pathways that medi- ate the action of thyroid hormone on the heart and allow a better understanding of the mechanisms that underlie the hemo- dynamic and clinical manifestations of hyperthyroidism. Several cardiovascular conditions and drugs can interfere with thyroid hormone levels and may pose a difficulty in the interpreta- tion of laboratory data in patients with suspected thyroid heart disease. 2210-5220/$ – see front matter © 2013 Elsevier Masson SAS. All rights reserved. http://dx.doi.org/10.1016/j.biomag.2013.03.001
Transcript of Protective role of folic acid in thyroxine-induced cardiac hypertrophy in hyperthyroid rat

O
Ph
ED
ARAA
KHTHMPI
1
o[te[m
hdcattp
2h
Biomedicine & Aging Pathology 3 (2013) 89–95
Available online at
www.sciencedirect.com
riginal article
rotective role of folic acid in thyroxine-induced cardiac hypertrophy inyperthyroid rat
hab Tousson ∗, Ezar Hafez , Ahmed A. Massoud , Osama Sweef , Nermin Attaepartment of Zoology, Faculty of Science, Tanta University, Damanhour, Egypt
a r t i c l e i n f o
rticle history:eceived 5 February 2013ccepted 8 March 2013vailable online 4 June 2013
eywords:yperthyroidismhyroxineeartyocardial hyperatrophy
CNAmmunohistochemistry
a b s t r a c t
Hyperthyroidism is a common metabolic disorder with prominent cardiovascular manifestation. It causesa hyperdynamic circulatory state because of a marked reduction in peripheral vascular resistance and anincreased total blood volume and heart rate. We studied the changes in the heart structure of hyperthy-roid rat at the post-pubertal stage, in addition to the role of folic acid in treatment. Thirty male Wistar ratswere equally divided into six groups; the first and second groups were the control and folic acid groupsrespectively while the third group was the hyperthyroid rat group; the fourth and fifth groups wereco- and post-treated hyperthyroid rat with folic acid respectively and the sixth group was self-treatedhyperthyroid rat group. Serum T3 andT4 levels were significantly increased while TSH levels were signifi-cantly depressed in rats receiving thyroxine indicating the induction of hyperthyroid state. Left ventriclesection in the heart of hyperthyroid rats showed many abnormalities such as myocardial hyperatrophy,hydrophobic changes of myofibrillar structure with striations, and focal haemorrhage when comparedwith that in control. The PCNA label index in cardiac tissues was significantly increased in hyperthyroid
rat (grade 4) and their levels were significantly decreased in co- and post-treated hyperthyroid rats withfolic acid (grades 3 and 2 respectively) when compared with control (grade 0). Treatment of hyperthyroidrats with folic acid improves the histopathological alternation and the intensity of PCNA immunoreactivecells demonstrating the recovery of some injury. In conclusion, our results indicated that folic acid hadameliorative effect against cardiac hypertrophy induced by thyroxine and the best results were found incase of using the folic acid as an adjuvant therapy after returning to the euthyroid state.© 2013 Elsevier Masson SAS. All rights reserved.
. Introduction
Thyroid hormones have marked effects on the growth, devel-pment, and metabolic function of virtually all organs and tissues1–12]. The action of thyroid hormone on the heart is mediatedhrough a dual mechanism. The main mode of action is a directffect on the transcription of specific and non-specific cardiac genes13]. The second is a non-genomic action on plasma membranes,
itochondria, and the sarcoplasmic reticulum [14].The heart is an organ sensitive to the action of thyroid
ormone, and measurable changes in cardiac performance areetected with small variations in thyroid hormone serum con-entrations [10]. Hyperthyroidism is a disease in which tissuesre exposed to high levels of thyroid hormones. Usually hyper-
hyroidism will increase the thyroid hormones and decreasehyrotropin in serum is detectable [15]. Hyperthyroidism isresent in 1.3% of the United States population (overt in 0.5%∗ Corresponding author. Tel.: +201093905527.E-mail address: [email protected] (E. Tousson).
210-5220/$ – see front matter © 2013 Elsevier Masson SAS. All rights reserved.ttp://dx.doi.org/10.1016/j.biomag.2013.03.001
and subclinical in 0.7%), and hypothyroidism in 4.6% of thepopulation (overt in 0.3% and subclinical in 4.3%). Heart fail-ure occurs in 6% of hyperthyroid patients. Nonetheless, onlyhalf of those with hyperthyroidism-related heart failure haveimpaired left ventricular systolic function [16]. Hyperthyroidismis a common metabolic disorder with prominent cardiovascu-lar manifestations [17–19]. It causes a hyperdynamic circulatorystate because of a marked reduction in peripheral vascularresistance and an increased total blood volume and heart rate[20].
Most patients with hyperthyroidism experience cardiovascularmanifestations, and the most serious complications of hyperthy-roidism occur as a result of cardiac involvement. Recent studiesprovide important insights into the molecular pathways that medi-ate the action of thyroid hormone on the heart and allow abetter understanding of the mechanisms that underlie the hemo-dynamic and clinical manifestations of hyperthyroidism. Several
cardiovascular conditions and drugs can interfere with thyroidhormone levels and may pose a difficulty in the interpreta-tion of laboratory data in patients with suspected thyroid heartdisease.
9 & Agi
lcdsvbafieirtsfdatatibigpa
2
twFim5tamware
••
•
•
•
•
it
0 E. Tousson et al. / Biomedicine
Folic acid is water-soluble vitamins, which are essential in ourife. Numerous clinical trials using folic acid for prevention ofardiovascular disease, stroke, cognitive decline, and neural tubeefects have been completed or are underway [21]. Folic acidtatus is also affected by hypothyroidism [3–9,11]. In healthy indi-iduals, folic acid is converted to L-methyl folate, which is theiologically active form of the vitamin. Hypothyroidism causes
decrease in the activity of the enzyme methylenetetrahydro-olate reductase, which is responsible for producing L-methyl folaten the liver. Low levels of L-methyl folate result in excess lev-ls of homocysteine. This indirect relationship could be causativen increasing cardiovascular disease risk in people with hypothy-oidism [21,22]. Yet, all functions of folate are performed byetrahydrofolate and its one-carbon derivatives. Folic acid is aynthetic oxidized form not significantly found in fresh naturaloods; to be used it must be converted to tetrahydrofolate byihydrofolate reductase [23]. Hyperthyroidism in man is associ-ted with depletion of folate stores and subclinical deficiency ofhis vitamin. This is attributed to an increased demand for foliccid in the hypermetabolic state [24]. There is little informa-ion about the relation between hyperthyroidism and the changesn heart structure. So, the present study represents a contri-ution to declare the alternation on the histopathological and
mmunohistochemical detection of proliferating cell nuclear anti-en (PCNA) in the cardiac tissues of hyperthyroid rat at theost-pubertal stage, in addition to the ameliorating role of foliccid.
. Materials and methods
The experiments were performed on 30 male albino rats (Rat-us norvigicus) weighing 125 ± 10 g and of 7–8 week’s age. Theyere obtained from our laboratory farms, Zoology Department,
aculty of Science, Tanta University, Egypt. The rats were keptn the laboratory for 1 week before the experimental work and
aintained on a standard rodent diet (20% casein, 15% corn oil,5% corn starch, 5% salt mixture and 5% vitaminzed starch; Egyp-ian Company of Oils and Soap Kafr-Elzayat, Egypt) and watervailable ad libitum. The temperature in the animal room wasaintained at 23 ± 2 ◦C with a relative humidity of 55 ± 5%. Lightas on a 12:12-h light-dark cycle. The experimental protocol was
pproved by Local Ethics Committee and Animals Research. Theats were randomly and equally divided into six groups (10 animalsach).
G1: control group in which animals did not receive any treatment;G2: folic acid group in which animals received folic acid daily (ElNasr Pharmaceutical Chemicals Co.; at 8 mg/kg of body weight)for 4 weeks from second to sixth week [8];G3: hyperthyroid rats group in which rats received L-thyroxinsodium administration (100 �g/kg, 4 weeks) as a chewable labchow [25];G4: co-treated group in which animals received L-thyroxinsodium daily in drinking water and folic acid simultaneouslyaccording to Tousson et al. [8];G5: post-treated group in which animals received L-thyroxinsodium daily in drinking water and folic acid simultaneouslyaccording to Tousson et al. [8];G6: hyperthyroid rats self-recovered group.
At the end of the experimental period, rats were euthanized withntraperitoneal injection with sodium pentobarbital and subjectedo a complete necropsy.
ng Pathology 3 (2013) 89–95
2.1. Biochemical assays
Blood samples were individually collected from the inferior venacava of each rat in heparinized and non-heparinized glass tubes toestimate biochemical parameters. The non-heparinized blood wasused to obtain blood serum while the heparinized blood was usedto obtain blood plasma.
2.2. Blood serum
Serum was separated from non-heparinized blood by centrifu-gation at 3000 rpm for 15 min. The collected serum was storedat −18 ◦C until analysis. Determination of serum T3, T4 and TSHwas performed using Biocheck Kits Inc (Los Angeles, USA) catalogNo. BC-1005, BC-1008 and BC-1001 respectively (using monoclonalantibody).
2.3. Histological investigation
Immediately after decapitation, animals were dissected, heart(left ventricle) were removed from different groups and were fixedin 10% neutral buffered formalin. After fixation, specimens weredehydrated in an ascending series of alcohol, cleared in two changesof xylene and embedded in molten paraffin (mp. 50–58 ◦C). Sec-tions of 5 microns thickness were cut using rotary microtome andmounted on clean slides. For histopathological examination, sec-tions were stained with Ehrlich’s haematoxylin and counterstainedwith eosin as a routine method after Bancroft and Stevens [26] andthe rest were used for immunohistochemical studies.
2.4. Immunohistochemical detection of proliferating cell nuclearantigen (PCNA)
Paraffin sections (5 �m thick) from ventricle were mountedon positive gelatin chromalum-coated glass slides for PCNAimmunohistochemical staining method [7]. The distribution ofPCNA receptor subunits in left ventricle sections from differ-ent groups was examined in deparaffinized sections (5 �m)using an Avidin-Biotin-Peroxidase immunohistochemical method(Elite–ABC, Vector Laboratories, CA, USA) against PCNA (dilu-tion 1:100, DAKO Japan Co, Ltd, Tokyo, Japan) were employed.Briefly, sections were deparaffinized, rehydrated, washed in phos-phate buffered saline (PBS) (3 × 5 min) and peroxidase activity wasquenched using 0.3% H2O2 in methanol for 30 min. Subsequently,samples were washed in PBS and incubated with blocking solutionat room temperature for 10 min. After rinsing with PBS, sectionswere incubated with biotinylated mouse anti-PCNA primary anti-body in moist chamber for 30–60 min and then rinsed with PBS.Samples were incubated with Streptavidin Peroxidase at room tem-perature for 10 min and washed with PBS. The antibody-peroxidasecomplex was developed using DAB chromogen at 18–24 ◦C for2–5 min. Finally, the sections were washed with PBS, counter-stained with methyl blue for 1 min, washed with tap water thenPBS for 30”, dehydrated through ascending grades of alcohol,delipidated in xylene, and cover-slipped with Mount-Quick (DaidoSangyo, Tokyo). All stained slides were viewed by using Olympusmicroscope and images were captured by a digital camera (Cannon620).
2.5. Statistical analysis
Data were expressed as mean values ± SE and statistical anal-
ysis was performed using one-way analysis of variance (ANOVA)followed by the Least Significant Difference (LSD) tests to assesssignificant differences among treatment groups. The criterion forstatistical significance was set at P < 0.05. All statistical analyses
E. Tousson et al. / Biomedicine & Agi
Table 1Assessment of T3 (ng/dL), T4 (ng/dL) and TSH (ng/dL) levels in different groups understudy.
Group T3 T4 TSH
G1 31.23 ± 2.23 3.05 ± 0.78 1.34 ± 0.10G2 30.61 ± 2.09 3.11 ± 0.10 1.33 ± 0.11G3 93.52 ± 6.56* 5.91 ± 0.27* 0.04 ± 0.02*G4 73.76 ± 5.91* 4.45 ± 0.47 0.06 ± 0.02*G5 49.60 ± 3.79* 2.65 ± 0.36 0.11 ± 0.01*G6 82.51 ± 6.43* 4.45 ± 0.97 0.08 ± 0.02*
Di
w(
3
ihcadgfcsrshtsah
tb(vmsbhffpctmc(gv
3
(wsa4crc
ata are expressed as mean ± SE of five observations. Stars mean statistically signif-cant at P ≤ 0.05.
ere performed using SPSS statistical version 16 software packageSPSS® Inc., USA).
. Results
Serum T3, T4 and TSH concentrations in the control and exper-mental groups are given in Table 1. Serum T3 and T4 levels inyperthyroid rats were significantly increased compared with theontrol and self-treated hyperthyroid groups. Serum T3 levels in co-nd post-treated hypothyroid rats with folic acid were significantlyecreased when compared with the hyperthyroid and self-treatedroups and significantly increased compared with the control andolic acid groups. T3 and T4 levels in self-treated were signifi-antly decreased when compared with hyperthyroid group andignificantly increased when compared with post-treated hypothy-oid rats with folic acid group (Table 1). Serum TSH levels wereignificantly decreased in hyperthyroid, self-treated and treatedypothyroid rats with folic acid when compared with the con-rol and folic acid groups (Table 1). TSH levels in self-treated wereignificantly increased when compared with hyperthyroid groupnd significantly decreased when compared with post-treatedypothyroid rats with folic acid group.
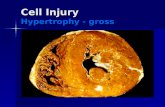
Light microscopy of the rat left ventricle sections in con-rol group showed normal myofibrillar structure with striations,ranched appearance and continuity with adjacent myofibrilsFig. 1A). Also, normal blood vessels were also observed in the leftentricle. Rat ventricle sections in folic group revealed a normalyofibrillar structure with striations (Fig. 1B). Histopathological
tudies of the ventricle in hyperthyroid rats revealed hydropho-ic changes of myofibrillar structure with striations, myocardialypertrophy, nuclear pyknosis, cytoplasmic vacuoles, edema and
ocal hemorrhage (Fig. 1C, D). Co-treated hyperthyroid rats witholic acid showed mild tissue injury with myocardial hypertro-hy and cytoplasmic vacuoles with increase in the collection ofardiac nuclei were observed (Fig. 1E). Left ventricle sections ofhe post-treated hyperthyroid rat with folic acid revealed a few
yofibrillar structures with striations, branched appearance andontinuity with adjacent myofibrils and mild cytoplasmic vacuolesFig. 1F, G). Left ventricle sections in self-treated hyperthyroid ratroup revealed myocardial hypertrophy with severe cytoplasmicacuoles, edema, and focal hemorrhage (Fig. 1H).
.1. PCNA immunoreactivity in left ventricular
The detection and distribution of PCNA immunoreactivityPCNA-ir) in the left ventricular in the different groups under studyere revealed in Fig. 2. Myocardium in control and folic acid groups
howed negative reaction for PCNA-ir (grade 0) in both sarcoplasmnd nuclei (Fig. 2A, B). Severe positive reactions for PCNA-ir (grade
) were detected in the sarcoplasm and sarcolema of the ventri-ular sections in hyperthyroid rat group (Fig. 2C, D). Mid positiveeactions for PCNA-ir (grade 3) in sarcoplasm of myocardium ino-treated hyperthyroid rats with folic acid (Fig. 2E, F) while theng Pathology 3 (2013) 89–95 91
intensity of PCNA-ir were significantly decreased (grade 2) in post-treated hypothyroid rats with folic acid (Fig. 2G) when comparedwith hyperthyroid and co-treated hyperthyroid rats with folic acidgroups. Self-treated hyperthyroid rats groups showed a signifi-cant decrease in PCNA-ir (grade 2) in sarcoplasm of myocardium(Fig. 2H) when compared with hyperthyroid group (Fig. 2C, D).
4. Discussion
Thyroid status is also an important determinant of cardiovas-cular function [5,11,21,27,28]. Thyroid hormone lowers systemicvascular resistance, increases blood volume, and has inotropic andchronotropic effects on cardiac function [29,30]. The combinationof these effects on both the circulation and the heart itself results inincreased cardiac output. The present study was designed to inves-tigate the role of thyroid hormone on rat cardiac muscle structures.In order to ensure the hyperthyroid state, we regularly determinedthe serum T3, T4 and TSH through the dose period where serum T3and T4 levels are increased and serum TSH levels is depressed inrats receiving thyroxine indicating the induction of hyperthyroidstate. In the present study, the effect of thyroxine on T3, T4 and TSHseems to be reversed in adult rats when the treatment was with-drawn after 4 weeks as the levels of the T3, T4 and TSH tend to benearing normal levels. Also, serum T3 and T4 levels in self-treatedco- and post-treated hypothyroid rats with folic acid were signif-icantly decreased when compared with the hyperthyroid group.This increase in TSH can be explained by decreased production ofT3 from the thyroid gland that minimizes TSH feedback inhibitionresulting in an increase in its secretion by the anterior pituitarygland; this result coincides with studies of Shibutani et al. [31].
Triiodothyronine hormone (T3)-induced changes in cardiacfunction can result from direct or indirect T3 effects. Direct effectsresult from T3 action in the heart itself and are mediated by nuclearor extranuclear mechanisms. Extranuclear T3 effects, that occurindependently of nuclear T3 receptor binding and increases in pro-tein synthesis, influence primarily the transport of amino acids,sugars, and calcium across the cell membrane [20]. Nuclear T3effects are mediated by the binding of T3 to specific nuclear receptorproteins, which results in increased transcription of T3-responsivecardiac genes. T3 also leads to an increase in the speed of dia-stolic relaxation, which is caused by the more efficient pumpingof the calcium ATPase of the sarcoplasmic reticulum. This T3 effectresults from T3-induced increases in the level of the mRNA cod-ing for the sarcoplasmic reticulum calcium ATPase protein, leadingto an increased number of calcium ATPase pump units in the sar-coplasmic reticulum [32].
Thyroid hormones exert important effects on the cardiovascularsystem, including effects on cardiac systolic and diastolic func-tion, peripheral vascular resistance, and arrhythmogenesis. Thyroidhormone is very important for normal cardiovascular function, sowhen not enough thyroid hormone is present neither the heart northe blood vessels function normally [28,29]. Fazio et al. [33] andStanescu et al. [30] reported that in hypothyroidism the heart mus-cle is weakened in both its contraction phase, and also its relaxationphase. This means that the heart cannot pump as vigorously as itshould and the amount of blood it ejects with each heartbeat isreduced [28]. Owen et al. [34] and Tousson et al. [10] reported thatthe decrease of thyroid hormone can cause an increase in levels oftotal cholesterol and low-density lipoprotein cholesterol and a pos-sible change in high-density lipoprotein cholesterol due to a changein metabolic clearance.
Our histopathological results revealed that left ventricle tis-sues in the hyperthyroid rats showed many abnormalities suchas myocardial hypertrophy, hydrophobic changes of myofibrillarstructure with striations, and focal hemorrhage when compared

92 E. Tousson et al. / Biomedicine & Aging Pathology 3 (2013) 89–95
Fig. 1. A–H. Photomicrographs of the cardiac myocytes of rat left ventricle stained by HE. A. Micrograph from control group of the cardiac myocytes displays normalmyofibrillar structure with striations, branched appearance and continuity with adjacent myofibrils. B. Micrograph from folic acid group of the cardiac myocytes displaysnormal myofibrillar structure with striations. C and D. Micrographs of the cardiac myocytes in hyperthyroid rats revealed myocardial hypertrophy, nuclear pyknosis (blackstars), cytoplasmic vacuoles (white arrows), edema and focal hemorrhage (white stars) and collections of nuclei (arrow heads). E. Left ventricle section in the co-treatedhyperthyroid rat with folic acid revealed severe tissue injury with mild myocardial hypertrophy, cytoplasmic vacuoles (white arrows), focal hemorrhage (white stars) andcollections of nuclei (arrow heads). F and G. Left ventricle section in the post-treated hyperthyroid rat with folic acid revealed a few myofibrillar structures with striations,branched appearance and continuity with adjacent myofibrils, nuclear pyknosis (black stars) and mild cytoplasmic vacuoles (white arrows). H. Left ventricle sections inself-treated hyperthyroid rat group revealed myocardial hypertrophy with severe cytoplasmic vacuoles (white arrows) and focal hemorrhage with collections of nuclei(arrow heads).

E. Tousson et al. / Biomedicine & Aging Pathology 3 (2013) 89–95 93
Fig. 2. A–H. Photomicrographs of the cardiac myocytes of rat left ventricle showed the detection and distribution of PCNA immunoreactivity (PCNA-ir) in the different groupsunder study. A and B. Negative reaction for PCNA-ir (grade 0) in the cardiac myocytes of rat left ventricle in control and folic acid groups. C and D. Strong positive reaction forPCNA-ir (grade 4) in the cardiac myocytes of rat left ventricle in hyperthyroid rats. E. Mild positive reaction for PCNA-ir (grade 2) in the cardiac myocytes of rat left ventriclein the co-treated hyperthyroid rat with folic acid. F and G. Finite negative reactions for PCNA-ir (grade 1) in the cardiac myocytes of rat left ventricle in the post-treatedhyperthyroid rat with folic acid. H. Mild positive reaction for PCNA-ir (grade 2) in the cardiac myocytes of rat left ventricle in self-treated hyperthyroid rat group.

9 & Agi
wf[due
bsPlicdmigasPcPr((rtfatr
caoietalidmaopldcri
D
i
R
[
[
[
[
[
[[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
4 E. Tousson et al. / Biomedicine
ith that in control. Also, the treatment of hyperthyroid rats witholic acid improves the histopathological alternation. Massoud et al.21] reported that folic acid had ameliorative effect against cardiacamage induced by PTU and the best results were found in case ofsing the folic acid as an adjuvant therapy after returning to theuthyroid state.
Recently, the use of immunocytochemical assays, based on anti-odies to cell proliferation-related antigens as PCNA, has beenhown to be effective in the assessment of cell proliferation [7,35].roliferating cell nuclear antigen expression and synthesis areinked to cell proliferation [36] and its presence subsequent tommunohistochemical processing can be observed microscopi-ally. This technique may be used for the purpose of providingirect visual evidence of cell proliferation under various experi-ental conditions [7,37]. The detection and distribution of PCNA
mmunoreactivity (PCNA-ir) in the left ventricular in the differentroups under study were revealed. Myocardium in control and foliccid groups showed negative reaction for PCNA-ir (grade 0) in botharcoplasm and nuclei. Unexpectedly, severe positive reactions forCNA-ir (grade 4) were detected in the sarcoplasm of the ventri-ular sections in hyperthyroid rat group. No marked increasing inCNA-ir in sarcoplasm of myocardiumin co-treated hyperthyroidats with folic acid while the intensity of PCNA-ir was decreasedgrade 1) in post-treated hypothyroid rats with folic acid decreasedgrade 2) in self-treated hypothyroid rats group. Abou-Harga [38]eported that cardiac muscles also have severe PCNA positive reac-ion in hypothyroid rats. Co-treatment of hyperthyroid rats witholic acid or self-treatment mild decreased the positive reactiongainst PCNA immunoreactivity in cardiac rat tissues, while post-reatment of hyperthyroid rats with folic acid showed a negativeeaction against PCNA immunoreactivity.
So, our immunohistochemical results supported the biochemi-al and histopathological results and therefore the folic acid playss a coenzyme factor for both hypo- and hyperthyroidism. Thebservation that methylenetetrahydrofolate reductase is increasedn hyperthyroidism and decreased in hypothyroidism may be rel-vant for the relation between plasma homocysteine levels andhyroid status [39]. Osman et al. [40] reported that hyperthyroidismnd hypothyroidism often cause opposing effects on cardiovascu-ar physiology and the majority of cardiac adaptations to changesn thyroid function are physiologic; however, certain patients doemonstrate clinical evidence of cardiac disease. Atrial arrhyth-ias, limitations in exercise tolerance and congestive heart failure
re reported to occur as a result of hyperthyroidism. The morphol-gy of cardiac muscle fibers was relatively well preserved in theost-treated hypothyroid rats with folic acid. We believe that the
oss of regularly arranged contractile proteins, degradation of bun-le structures and disarrayed muscle fibers all contribute to thehanges of birefringence effect in myocardium. Also, the presentesults revealed that folic acid treatment was better if it is admin-stered as an adjuvant after returning to the euthyroid state.
isclosure of interest
The authors have not supplied their declaration of conflict ofnterest.
eferences
[1] Ahmed OM, El-Gareib AW, El-bakry AM, El-Tawab SA, Ahmed RG. Thyroidhormones states and brain development interactions. Int J Dev Neurosci2008;26:147–209.
[2] Toshihiro I. Thyroid hormone and atherosclerosis. Vascul Pharmacol2010;52:151–6.
[3] Ibrahim W, Tousson E, Ali EM, Mansour MA. Folic acid alleviates oxidative stressand hyperhomocysteinemia involved in testicular dysfunction of hypothyroidrats. Gen Comp Endocrinol 2011;174:143–9.
[
[
ng Pathology 3 (2013) 89–95
[4] Ibrahim W, Abo Gazia M, El-Atrash A, Massoud A, Tousson E, Abou-HargaH. Ameliorative effect of folic acid on propylthiouracil-induced histologi-cal and immunohistochemical alterations in aorta of albino rats. J Am Sci2012;8:155–9.
[5] Ibrahim W, Tousson E, El-Masery T, Arafa N, Akela M. The effect of folic acid asan antioxidant on the hypothalamic monoamines in experimentally inducedhypothyroid rat. Toxicol Ind Health 2012;28:253–61.
[6] Salama AF, Tousson E, Ibrahim W, Hussein MW. Biochemical and histopatho-logical studies in the PTU-induced hypothyroid rat kidney with refer-ence to the ameliorating role of folic acid. Toxicol Ind Health 2012,http://dx.doi.org/10.1177/0748233711432577.
[7] Tousson E, Ali EM, Ibrahim W, Mansour MA. Proliferating cell nuclear antigenas a molecular biomarker for spermatogenesis in PTU-induced hypothyroidismof rats. Reprod Sci 2011;18:679–86.
[8] Tousson E, El-Gerbed MSA, Shaleby S. Effects of maturity on histopathologicalalteration after a growth promoter boldenone injection in rabbits. J Am Sci2011;7:1074–80.
[9] Tousson E, Ali EM, Ibrahim W, Mansour MA. Treatment with folic acid ame-liorated the histopathological alterations caused by propylthiouracil-inducedhypothyroid rat testes. Toxicol Ind Health 2012;28:566–76.
10] Tousson E, Ali EM, Ibrahim W, Ashraf RM. Histopathological and immuno-histochemical alterations in rat heart after thyroidectomy and the roleof hemin and ketoconazole in treatment. Biomed Pharmacother 2012;66:627–32.
11] Tousson E, Ibrahim W, Nadia A, Akela MA. Histopathological changes in rathypothalamus after propylthiouracil induced hypothyroidism and the protec-tive role of folic acid. J Neurol Sci 2012;29:705–13.
12] Tousson E, Ibrahim W, Arafa N, Akela MA. Monoamine concentrations changesin the PTU induced hypothyroid rat brain and the ameliorating role of folic acid.Hum Exp Toxicol 2012;31:282–9.
13] Tsai MJ, O’Malley BW. Molecular mechanisms of action of steroid thyroid recep-tor superfamily members. Annu Rev Biochem 1994;63:451–86.
14] Davis PJ, Davis FB. Nongenomic actions of thyroid hormone. Thyroid1996;6:497–504.
15] Cooper DS. Hyperthyroidism. Lancet 2003;362:459–68.16] Fadel BM, Ellahham MD, Ringel MD, Lindsay Jr MD, et al. Hyperthyroid heart
disease. Clin Cardiol 2000;23:402–8.17] Siu CW, Yeung CY, Lau CP, et al. Incidence, clinical characteristics and outcome
of congestive heart failure as the initial presentation in patients with primaryhyperthyroidism. Heart 2007;93:483–7.
18] Siu CW, Pong V, Zhang X, et al. Risk of ischemic stroke after new-onsetatrial fibrillation in patients with hyperthyroidism. Heart Rhythm J 2009;6:169–73.
19] Siu CW, Jim MH, Zhang X, et al. Comparison of atrial fibrillation recurrence ratesafter successful electrical cardioversion in patients with hyperthyroidism-induced versus non-hyperthyroidism-induced persistent atrial fibrillation. AmJ Cardiol 2009;103:540–3.
20] Kahaly GJ, Kampmann C, Mohr-Kahaly S. Cardiovascular hemodynamics andexercise tolerance in thyroid disease. Thyroid 2002;12:473–81.
21] Massoud A, El-Atrash A, Tousson E, Ibrahim W, Abou-Harga H. Lightand ultrastructural study in the propylthiouracil-induced hypothyroid ratheart ventricles and the ameliorating role of folic acid. Toxicol Ind Health2012;28:262–70.
22] Chan MMS, Stokstad ELR. Metabolic responses of folic acid and related com-pounds to thyroxine in rats. Biochim Biophys Acta 1980;632:244–53.
23] Bailey SW, Ayling JE. The extremely slow and variable activity of dihydrofolatereductase in human liver and its implications for high folic acid intake. ProcNatl Acad Sci U S A 2009;106:15424–9.
24] Lindenbaum J, Klipstein F. Folic acid clearances and basal serum folate levels inpatients with thyroid disease. J Clin Pathol 1964;17:666–70.
25] Caminos JE, Seoane LM, Tovar SA, Casanueva FF, Dieguez C. Influence ofthyroid status and growth hormone deficiency on ghrelin. Eur J Endocrinol2002;147:159–63.
26] Bancroft JD, Stevens A. Theory and practice of histological technique. 3rd edEdinburgh, London: Churchill Livingstone; 1990.
27] Duntas LH, Wartofsky L. Cardiovascular risk and subclinical hypothyroidism:focus on lipids and new emerging risk factors. What is the evidence? Thyroid2007;17:1075–84.
28] Toruner F, Altinova AE, Karakoc A, Yetkin I, Ayvaz G, Cakir N, et al. Risk factors forcardiovascular disease in patients with subclinical hypothyroidism. Adv Ther2008;25(5):430–7.
29] Neves C, Alves M, Medina JL, Delgado JL. Thyroid diseases, dyslipidemia andcardiovascular pathology. Rev Port Cardiol 2008;27:1211–36.
30] Stanescu C, Branidou K, Ranetti EA. Heart failure and dilated cardiomyopathyassociated with severe longstanding untreated hypothyroidism. Rom J InternMed 2007;45:77–83.
31] Shibutani M, Woo GH, Fujimoto H, Saegusa Y, Takahashi M, Inoue K,et al. Assessment of developmental effects of hypothyroidism in rats fromin utero and lactation exposure to anti-thyroid agents. Reprod Toxicol2009;28:297–307.
32] Kahaly GJ, Dillmann WH. Thyroid hormone action in the heart. Endocr Rev
2005;26:704–28.33] Fazio S, Palmieri EA, Lombardi G, Biondi B. Effects of thyroid hormone on thecardiovascular system. Recent Prog Horm Res 2004;59:31–50.
34] Owen PJ, Sabit R, Lazarus JH. Thyroid disease and vascular function. Thyroid2007;17:519–24.

& Agi
[
[
[
[
[
E. Tousson et al. / Biomedicine
35] Abdel-Dayem M. Histological and immunohistochemical changes in the adultrat testes after left experimental varicocele and possible protective effects ofresveratrol. Egypt J Histol 2009;32:81–90.
36] Kurki P, Ogata K, Tan EM. Monoclonal antibodies to proliferating cell nuclearantigen (PCNA)/cyclin as probes for proliferating cells by immunofluo-
rescence microscopy and flow cytometry. J Immunol Methods 1988;109:49–59.37] Tousson E, El-Moghazy M, Massoud A, Akel A. Histopathological and immuno-histochemical changes in the testes of rabbits after injection with the growthpromoter boldenone. Reprod Sci 2012;19:253–9.
[
ng Pathology 3 (2013) 89–95 95
38] Abou-Harga H. Impact of folic acid on endothelial dysfunction in experimen-tally induced hypothyroidism. PhD Thesis, Department of Zoology, Faculty ofScience, Tanta University, Egypt; 2012.
39] Lindeman RD, Romero LJ, Schade DS, Wayne S, Baumgartner RN, Garry PJ.Impact of subclinical hypothyroidism on serum total homocysteine concen-
trations, the prevalence of coronary heart disease (CHD), and CHD risk factorsin the New Mexico Elder Health Survey. Thyroid 2003;13:595–600.40] Osman F, Gammage MD, Franklyn JA. Thyroid disease and its treatment:short-term and long-term cardiovascular consequences. Curr Opin Pharmacol2001;1:626–31.