
Prosthetic rehabilitation of a patient with a unilateral ... · Prosthetic rehabilitation of a...
4
Prosthetic rehabilitation of a patient with a unilateral cleft palate: A clinical report Mehmet Cudi Balkaya, DMD, PhD, a Huseyin Sultan, b Seda Erdem, c and Deniz Mutlu d Faculty of Dentistry, Istanbul University, Istanbul, Turkey Cleft palate is a congenital disorder characterized by maxillary growth defect and dental anomalies. Its correction requires an interdisciplinary approach, which includes surgical, orthodontic, and prosthetic treatments. This clinical report describes the prosthetic management of a 19-year-old woman with a unilateral cleft palate defect that had not been closed completely with surgical repair. The deficient maxillary residual anterior ridge was restored with a tooth-supported overdenture that improved her facial appearance, speech, and masticatory functions. (J Prosthet Dent 2014;111:269-272) Cleft palate with or without cleft lip is the most common malformation of the orofacial region that results from delayed cell migration during palate develop- ment. 1,2 The etiology of cleft palate is thought to include endogenous factors such as genetic disorders and exogenous factors such as environmental teratogens that can cause congenital defects. The environmental factors include cigarette smoke, systemic corticosteroid treat- ment, drug and lead pollution, viral ef- fects, and maternal malnutrition. 3-5 Increasing maternal age may increase the risk for cleft palate. 6 Contemporary treatment concepts for cleft palate correction require early surgery at birth or in childhood. Speech and hearing functions can be improved by cleft closure before 2 years of age, because speech development in children from birth to 5 years of age is more rapid than that in any other phase of life. 7-9 However, surgical treatment dur- ing the maxillary growth phase may result in residual ridge collapse followed by midface growth inhibition. 7,10 Although mandibular growth is generally normal in patients with a cleft palate, adolescent or adult patients who are not treated for cleft closure at the optimal time experience posterior reverse articulation, resulting from the collapse of the maxillary arch due to palatal muscle strain and scar retrac- tion. 11 The occlusal vertical dimension of these patients is consistent with that of individuals without clefts. 12 However, the maxillary length decreases slightly because of anteroposterior growth defect, leaving the patients with insufficient facial support and a concave maxillary lip. 13 Treatment options are arch expansion after residual ridge augmentation with autogenous graft from the iliac crest or tooth-supported or implant-supported partial fixed dental prostheses. 14,15 However, the closure of a cleft palate is more difficult in adults than in infants because of the wide cleft and irregular palate surface around the suture and the higher incidence of postoperative complications. 16 If the cleft area is not closed completely with surgery, partial remov- able dental prostheses can be used to replace missing teeth and to compensate for tissue deficiencies that interrupt the continuity of the dental arch 17 ; however, they rest on soft tissue and may cause irritation. 15 In this instance, an over- denture supported entirely by the teeth may be a reasonable method of avoiding soft tissue injury in the cleft area. This 1 Intraoral view. a Associate Professor, Department of Prosthetics. b Doctoral student, Department of Prosthetics. c Doctoral student, Department of Prosthetics. d Doctoral student, Department of Prosthetics. Balkaya et al
-
Upload
nguyenphuc -
Category
Documents
-
view
216 -
download
1
Transcript of Prosthetic rehabilitation of a patient with a unilateral ... · Prosthetic rehabilitation of a...

Proa un
Mehmet Cudi Ba
aAssociate Professor, Department ofbDoctoral student, Department of PcDoctoral student, Department of PdDoctoral student, Department of P
Balkaya et al
sthetic rehabilitation of a patient withilateral cleft palate: A clinical report
lkaya, DMD, PhD,a Huseyin Sultan,b Seda Erdem,c
and Deniz Mutlud
Faculty of Dentistry, Istanbul University, Istanbul, Turkey
Cleft palate is a congenital disorder characterized by maxillary growth defect and dental anomalies. Its correction requires aninterdisciplinary approach, which includes surgical, orthodontic, and prosthetic treatments. This clinical report describes theprosthetic management of a 19-year-old woman with a unilateral cleft palate defect that had not been closed completely withsurgical repair. The deficient maxillary residual anterior ridge was restored with a tooth-supported overdenture that improvedher facial appearance, speech, and masticatory functions. (J Prosthet Dent 2014;111:269-272)
1 Intraoral view.
Cleft palate with or without cleft lip isthe most common malformation of theorofacial region that results from delayedcell migration during palate develop-ment.1,2 The etiology of cleft palate isthought to include endogenous factorssuch as genetic disorders and exogenousfactors such as environmental teratogensthat can cause congenital defects. Theenvironmental factors include cigarettesmoke, systemic corticosteroid treat-ment, drug and lead pollution, viral ef-fects, and maternal malnutrition.3-5
Increasing maternal age may increasethe risk for cleft palate.6
Contemporary treatment conceptsfor cleft palate correction require earlysurgery at birth or in childhood. Speechand hearing functions can be improvedby cleft closure before 2 years of age,because speech development in childrenfrom birth to 5 years of age is morerapid than that in any other phase oflife.7-9 However, surgical treatment dur-ing the maxillary growth phase mayresult in residual ridge collapse followedby midface growth inhibition.7,10
Although mandibular growth isgenerally normal in patients with a cleftpalate, adolescent or adult patients whoare not treated for cleft closure at theoptimal time experience posterior
Prostheticrosthetics.rosthetics.rosthetics.
reverse articulation, resulting from thecollapse of the maxillary arch due topalatal muscle strain and scar retrac-tion.11 The occlusal vertical dimensionof these patients is consistent with thatof individuals without clefts.12 However,the maxillary length decreases slightlybecause of anteroposterior growthdefect,leaving the patientswith insufficient facialsupport and a concave maxillary lip.13
Treatment options are arch expansionafter residual ridge augmentation withautogenous graft from the iliac crest ortooth-supported or implant-supportedpartial fixed dental prostheses.14,15
However, the closure of a cleft palate is
s.
more difficult in adults than in infantsbecause of the wide cleft and irregularpalate surface around the suture andthe higher incidence of postoperativecomplications.16
If the cleft area is not closedcompletely with surgery, partial remov-able dental prostheses can be used toreplace missing teeth and to compensatefor tissue deficiencies that interrupt thecontinuity of the dental arch17; however,they rest on soft tissue and may causeirritation.15 In this instance, an over-denture supported entirely by the teethmay be a reasonable method of avoidingsoft tissue injury in the cleft area. This
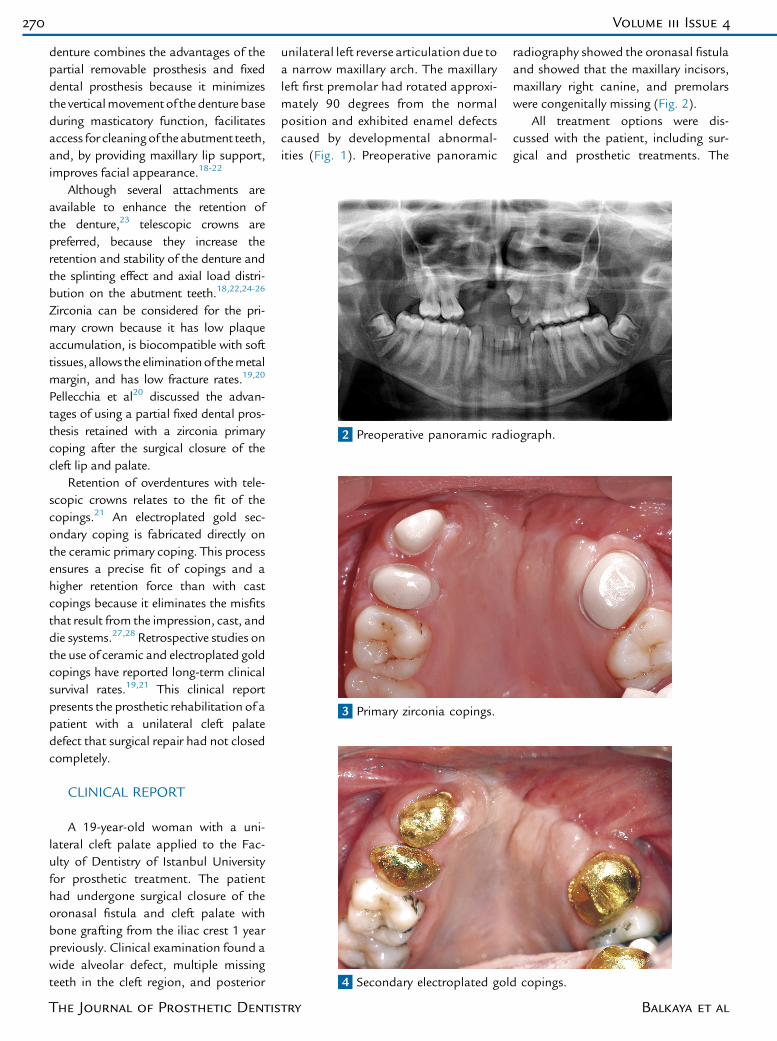
2 Preoperative panoramic radiograph.
4 Secondary electroplated gold copings.
3 Primary zirconia copings.
270 Volume 111 Issue 4
denture combines the advantages of thepartial removable prosthesis and fixeddental prosthesis because it minimizesthe verticalmovementof thedenturebaseduring masticatory function, facilitatesaccess for cleaningof the abutment teeth,and, by providing maxillary lip support,improves facial appearance.18-22
Although several attachments areavailable to enhance the retention ofthe denture,23 telescopic crowns arepreferred, because they increase theretention and stability of the denture andthe splinting effect and axial load distri-bution on the abutment teeth.18,22,24-26
Zirconia can be considered for the pri-mary crown because it has low plaqueaccumulation, is biocompatible with softtissues, allows the eliminationof themetalmargin, and has low fracture rates.19,20
Pellecchia et al20 discussed the advan-tages of using a partial fixed dental pros-thesis retained with a zirconia primarycoping after the surgical closure of thecleft lip and palate.
Retention of overdentures with tele-scopic crowns relates to the fit of thecopings.21 An electroplated gold sec-ondary coping is fabricated directly onthe ceramic primary coping. This processensures a precise fit of copings and ahigher retention force than with castcopings because it eliminates the misfitsthat result from the impression, cast, anddie systems.27,28 Retrospective studies onthe use of ceramic and electroplated goldcopings have reported long-term clinicalsurvival rates.19,21 This clinical reportpresents the prosthetic rehabilitation of apatient with a unilateral cleft palatedefect that surgical repair had not closedcompletely.
CLINICAL REPORT
A 19-year-old woman with a uni-lateral cleft palate applied to the Fac-ulty of Dentistry of Istanbul Universityfor prosthetic treatment. The patienthad undergone surgical closure of theoronasal fistula and cleft palate withbone grafting from the iliac crest 1 yearpreviously. Clinical examination found awide alveolar defect, multiple missingteeth in the cleft region, and posterior
The Journal of Prosthetic Dentis
unilateral left reverse articulation due toa narrow maxillary arch. The maxillaryleft first premolar had rotated approxi-mately 90 degrees from the normalposition and exhibited enamel defectscaused by developmental abnormal-ities (Fig. 1). Preoperative panoramic
try
radiography showed the oronasal fistulaand showed that the maxillary incisors,maxillary right canine, and premolarswere congenitally missing (Fig. 2).
All treatment options were dis-cussed with the patient, including sur-gical and prosthetic treatments. The
Balkaya et al
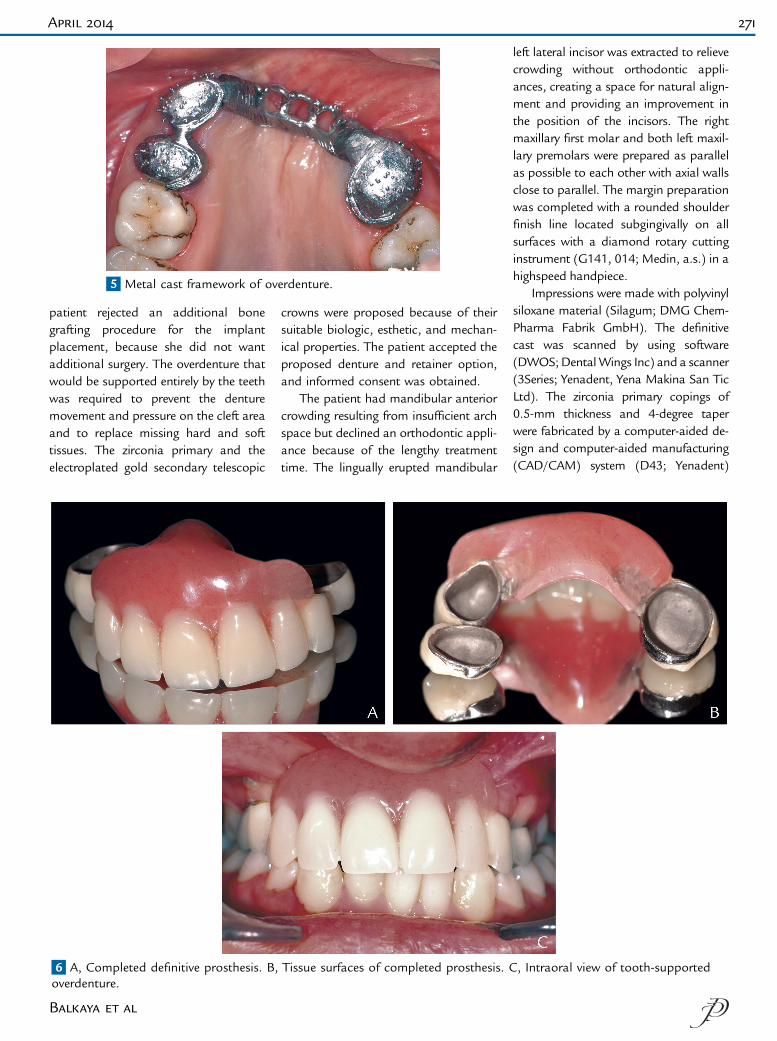
5 Metal cast framework of overdenture.
April 2014 271
patient rejected an additional bonegrafting procedure for the implantplacement, because she did not wantadditional surgery. The overdenture thatwould be supported entirely by the teethwas required to prevent the denturemovement and pressure on the cleft areaand to replace missing hard and softtissues. The zirconia primary and theelectroplated gold secondary telescopic
6 A, Completed definitive prosthesis. B,overdenture.
Balkaya et al
crowns were proposed because of theirsuitable biologic, esthetic, and mechan-ical properties. The patient accepted theproposed denture and retainer option,and informed consent was obtained.
The patient had mandibular anteriorcrowding resulting from insufficient archspace but declined an orthodontic appli-ance because of the lengthy treatmenttime. The lingually erupted mandibular
Tissue surfaces of completed prosthesis. C
left lateral incisor was extracted to relievecrowding without orthodontic appli-ances, creating a space for natural align-ment and providing an improvement inthe position of the incisors. The rightmaxillary first molar and both left maxil-lary premolars were prepared as parallelas possible to each other with axial wallsclose to parallel. The margin preparationwas completed with a rounded shoulderfinish line located subgingivally on allsurfaces with a diamond rotary cuttinginstrument (G141, 014; Medin, a.s.) in ahighspeed handpiece.
Impressions were made with polyvinylsiloxane material (Silagum; DMG Chem-Pharma Fabrik GmbH). The definitivecast was scanned by using software(DWOS;DentalWings Inc) and a scanner(3Series; Yenadent, Yena Makina San TicLtd). The zirconia primary copings of0.5-mm thickness and 4-degree taperwere fabricated by a computer-aided de-sign and computer-aided manufacturing(CAD/CAM) system (D43; Yenadent)
, Intraoral view of tooth-supported

272 Volume 111 Issue 4
fromapresintered zirconia block (VITA In-Ceram YZ; VITA Zahnfabrik) and wereevaluated for fit intraorally (Fig. 3). Puregold (DeguDent GmbH) secondary cop-ings of 0.25-mm thicknesswere fabricatedon the zirconia copings by direct electro-plating with the Solaris system (DeguDentGmbH).
The zirconia primary copings werecemented to the abutment teeth withdual-polymerized self-adhesive resin(BisCem; Bisco Inc). The gold copingswere placed on the zirconia copings(Fig. 4), and the denture frameworkcast with a Co-Cr alloy (Wironium;Bego, Herbst GmbH & Co KG) wasevaluated for fit on the copings (Fig. 5).The framework was bonded intraorallyto the gold copings with autopolyme-rizing adhesive resin (C&B Cement;Bisco). The definitive frameworkimpression was made with the polyvinylsiloxane material (Silagum; DMGChem-Pharma Fabrik GmbH) to fabri-cate a new definitive cast. The prosthesiswas completed with veneering material(Solidex; Shofu Dental GmbH), acrylicresin denture teeth (Vitapan; VITAZahnfabrik), and a heat-polymerizedacrylic resin (Rapid Simplified; VertexDental) (Fig. 6A-C).
The polished denture was insertedintraorally and evaluated for occlusion,retention, and stability. After oral hy-giene instructions, the patient wasrecalled after 24 hours, 1 week, 1month,3 months, and 6 months for examina-tion and cleaning of the denture. Duringthe patient recall periods, no soft tissueinjury, periodontal disease, or estheticfailures were observed, and the dentureretention was satisfactory.
SUMMARY
This clinical report describes theprosthetic rehabilitation of a patientwith a unilateral cleft palate that hadnot been closed completely with surgicalrepair. The tissue deficiencies that hadinterrupted the continuity of the ma-xillary dental arch were restored withthe entirely tooth-supported overdenture.
The Journal of Prosthetic Dentis
This denture improved the patient’s facialappearance, speech, and masticatoryfunctions.
REFERENCES
1. Kummer AW. Cleft palate and craniofacialanomalies: effect on speech and resonance.2nd ed. New York: Thomson DelmarLearning; 2008. p. 36-64.
2. Menezes R, Vieira AR. Dental anomalies aspart of the cleft spectrum. Cleft Palate Cra-niofac J 2008;45:414-9.
3. Honein MA, Paulozzi LJ, Watkins ML.Maternal smoking and birth defects: validityof birth certificate data for effect estimation.Public Health Rep 2001;116:327-35.
4. Edwards MJ, Agho K, Attia J, Diaz P, Hayes T,Illingworth A, et al. Case-control study ofcleft lip or palate after maternal use oftopical corticosteroids during pregnancy. AmJ Med Genet A 2003;120A:459-63.
5. Vinceti M, Rovesti S, Bergomi M, Calzolari E,Candela S, Campagna A, et al. Risk of birthdefects in a population exposed to environ-mental lead pollution. Sci Total Environ2001;278:23-30.
6. Bille C, Skytthe A, Vach W, Knudsen LB,Andersen AM, Murray JC, et al. Parent’s ageand the risk of oral clefts. Epidemiology2005;16:311-6.
7. Haapanen ML, Rantala SL. Correlation be-tween the age at repair and speech outcome inpatients with isolated cleft palate. Scand J PlastReconstr Surg Hand Surg 1992;26:71-8.
8. Zhao S, Xu Y, Yin H, Zheng Q, Wang Y,Zhong T, et al. Incidence of postoperativevelopharyngeal insufficiency in late palaterepair. J Craniofac Surg 2012;23:1602-6.
9. Rohrich RJ, Love EJ, Byrd HS, Johns DF.Optimal timing of cleft palate closure. PlastReconstr Surg 2000;106:413-21.
10. Denk MJ, Magee WP Jr. Cleft palate closurein the neonate: preliminary report. Cleft Pal-ate Craniofac J 1996;33:57-61.
11. Oberoi S, Chigurupati R, Vargervik K.Morphologic and management characteris-tics of individuals with unilateral cleft lip andpalate who required maxillary advancement.Cleft Palate Craniofac J 2008;45:42-9.
12. Will LA. Growth and development in patientswith untreated clefts [review]. Cleft PalateCraniofac J 2000;37:523-6.
13. Daskalogiannakis J, Mercado A, Russell K,Hathaway R, Dugas G, Long RE Jr, et al. TheAmericleft study: an inter-center study of treat-ment outcomes for patients with unilateral cleftlip and palate part 3. Analysis of craniofacialform. Cleft Palate Craniofac J 2011;48:252-8.
14. Yang CJ, Pan XG, Qian YF, Wang GM. Impactof rapid maxillary expansion in unilateral cleftlip and palate patients after secondary alve-olar bone grafting: review and case report.Oral Surg Oral Med Oral Pathol Oral Radiol2012;114:e25-30.
15. Reisberg DJ. Dental and prosthodontic care forpatients with cleft or craniofacial conditions[review].Cleft PalateCraniofac J 2000;37:534-7.
try
16. Morioka D, Yoshimoto S, Udagawa A,Ohkubo F, Yoshikawa A. Primary repair inadult patients with untreated cleft lip-cleftpalate. Plast Reconstr Surg 2007;120:1981-8.
17. Hickey AJ, Salter M. Prosthodontic and psy-chological factors in treating patients withcongenital and craniofacial defects.J Prosthet Dent 2006;95:392-6.
18. Langer Y, Langer A. Tooth-supported tele-scopic prostheses in compromised denti-tions: a clinical report. J Prosthet Dent2000;84:129-32.
19. Zafiropoulos GG, Rebbe J, Thielen U, Deli G,Beaumont C, Hoffmann O. Zirconia remov-able telescopic dentures retained on teeth orimplants for maxilla rehabilitation. Three-year observation of three cases. J OralImplantol 2010;36:455-65.
20. Pellecchia R, Kang KH, Hirayama H. Fixedpartial denture supported by all-ceramiccopings: a clinical report. J Prosthet Dent2004;92:220-3.
21. Weigl P, Lauer HC. Advanced biomaterialsused for a new telescopic retainer forremovable dentures. J Biomed Mater Res2000;53:337-47.
22. Mañes Ferrer JF, Martínez González A, OteizaGaldón B, Bouazza Juanes K, Benet Iranzo F,Candel Tomás A. Telescopic crowns in adultcase with lip and palate cleft: update on theetiology and management. Med Oral PatolOral Cir Bucal 2006;11:E358-62.
23. Rosenstiel SF, Land MF, Fujimoto J.Contemporary fixed prosthodontics. 4th ed.St Louis: Elsevier; 2006. p. 649-80.
24. Weaver JD. Telescopic copings in restor-ative dentistry. J Prosthet Dent 1989;61:429-33.
25. Akagawa Y, Seo T, Ohkawa S, Tsuru H.A new telescopic crown system using asoldered horizontal pin for removablepartial dentures. J Prosthet Dent 1993;69:228-31.
26. Ohkawa S, Okana H, Nagasawa T, Tsuru H.Changes in retention of various telescopecrown assemblies over long-term use.J Prosthet Dent 1990;64:153-8.
27. Bayer S, Kraus D, Keilig L, Gölz L, Stark H,Enkling N. Wear of double crown systems:electroplated vs. casted female part. J ApplOral Sci 2012;20:384-91.
28. Castilho AA, Kojima AN, Pereira SM,Vasconcellos DK, Itinoche MK, Faria R, et al.In vitro evaluation of the precision of workingcasts for implant-supported restoration withmultiple abutments. J Appl Oral Sci 2007;15:241-6.
Corresponding author:Dr Mehmet Cudi BalkayaDepartment of Prosthetics, Faculty of DentistryIstanbul UniversityMillet St34390 IstanbulTURKEYE-mail: [email protected]
Copyright ª 2014 by the Editorial Council forThe Journal of Prosthetic Dentistry.
Balkaya et al


















