PROJECT REPORT - WA Health · PROJECT REPORT Nicole Beattie Ivan Lin ... A Catalogue of Relevant...
42
PROJECT REPORT Nicole Beattie Ivan Lin Suzanne Spitz Alex Ellis
Transcript of PROJECT REPORT - WA Health · PROJECT REPORT Nicole Beattie Ivan Lin ... A Catalogue of Relevant...

�
������������� ���������������
���� ���������������������������
��
��
�
PROJECT REPORT
Nicole Beattie Ivan Lin
Suzanne Spitz Alex Ellis

Table of Content 1. Introduction / Background..................................................................................... p. 1
1.1 Project Context............................................................................................... p. 2 1.2 Project Scope.................................................................................................. p. 3 1.3 Project Aims and Activity............................................................................... p. 4
2. Project Reference Group........................................................................................ p. 5 3. Ethics......................................................................................................................... p. 6 4. Literature Review.................................................................................................... p. 6
4.1 Search Strategy.............................................................................................. p. 6 4.2 Search Results................................................................................................ p. 7 4.3 Key Findings.................................................................................................. p. 9
5. Development of Draft Competencies.................................................................... p. 10 6. Delphi review…………........................................................................................... p. 10
6.1 First Round: Ranking Exercise...................................................................... p. 11 6.2 Second Round: Focus Groups....................................................................... p. 13 6.3 Third Round: WACHS review......................................................................... p. 16
7. Organisation within a Developmental Framework…………………………….. p. 16 8. Conclusion…………………………........................................................................ p. 17 9. Bibliography............................................................................................................ p. 18 10. Appendices………………………………………………………………………... p. 20
A Catalogue of Relevant Competency Frameworks…………………….......... p. 20 B WACHS Senior Allied Health Competencies Developmental Framework… p. 26 C Developing Rural and Remote Senior Allied Health Competencies Final
Draft………………………………………………………………………… p. 27
List of Tables and Figures Figure 1 Map of WACHS Health Regions………………………………………… p. 2 Figure 2 Elements of senior allied health staff role………………………………. p. 4 Figure 3 Summary of Search Strategy…………………………………………….. p. 8 Table 1 Ranking Exercise responses by discipline……………………….............. p. 11 Table 2 Ranking Exercise responses by WACHS region…………………………. p. 12 Table 3 Focus group Participation……………………………………………….. p. 15

Acknowledgements The Combined Universities Centre for Rural Health (CUCRH) project team and the WA Country Health Service (WACHS) would like to acknowledge Project Reference Group, including: Alex Ellis, Aasta Abbot, Dawn Logan and Suzanne Spitz, who were invaluable in guiding the development and ongoing review of the senior competency framework. Additionally, the project team would like to recognize the contribution of all WACHS staff who participated in survey and focus groups. List of Abbreviations and Acronyms AHP Allied health professional AHRG Allied Health Reference Group HSOA Hospital Salaried Officers Association CUCRH Combined Universities Centre for Rural Health DRRAHC-EP Developing Rural and Remote Allied Health Competencies – Entry to Practice�DRRSAHC Developing Rural and Remote Senior Allied Health Competencies�WACHS WA Country Health Service

1
1. Introduction / Background High quality health services require health professionals who have up-to-date skills and expertise and are trained to be ‘fit for purpose’. Allied health professionals (AHPs) working in rural and remote areas require skills unique to country practice. Establishing clear competencies is one way of ensuring health care delivered by AHPs in rural and remote areas meets the high demands of their work. To date however there has been a limited delineation of allied health competencies and a dearth of information relating to competencies for AHPs in the rural Australian context. The use of competency frameworks in the workplace became popular in the 1980’s (Hartley and Hinksman 2003, p. 18) and has since come to feature strongly in healthcare and related fields both in Australia and internationally. While the exact definition and usage of the term is contested, competency can be broadly defined as ‘the knowledge, skills, ability and behaviours that a person possesses in order to perform tasks correctly and skilfully’ (Whelan, p. 198). As an extension of this definition, competency assessment refers to an ‘ongoing process of initial development, maintenance of knowledge and skills, educational consultation, remediation, and redevelopment’ (Whelan, p. 198). In practice healthcare leadership and management competencies ‘provides a framework and a language for identifying the leadership knowledge and skills required for high quality healthcare’ (Baker 2003, p. 49). Competencies and related frameworks serve many purposes in the delivery of quality health care. They are frequently employed as a tool during recruitment to compare staff skills against the requirements of a position. Additionally, they are used to facilitate individual performance reviews and to identify ongoing professional development needs of individual employees (Baker 2003, p. 50). At the organisational or institutional level competency frameworks allow for the identification of leadership skills and knowledge necessary to achieve an organizations strategic agenda (Baker 2003, p. 50). In terms of health management and leadership, Baker (2003) suggests, most importantly competency frameworks ‘provides a language for talking more precisely about leadership knowledge and skills… [they] offer a way to deepen current conversations about the specific knowledge and skills necessary for leaders’ (p. 55), and provide a mechanism for measuring these. This project has seen the development of a competency framework for WA Country Health Service (WACHS) senior allied health professionals. It follows the development of ‘Developing Rural and Remote Allied Health Competencies – Entry to Practice’ (DRRAHC - EP) in 2004. Like the DRRAHP-EP, and inline with the roles of competency frameworks outlined above, it is intended that the senior competency framework will be used to identify learning and developmental needs, and areas of strength and proficiency for WACHS senior level AHPs. These frameworks may be used by individual allied health professionals for self-assessment, with peers or with allied health managers in the performance development process. Previous to the commencement of this project, a bank of competencies were identified by senior allied health staff within the WACHS Allied Health Reference Group (AHRG). This project has

2
overseen the ongoing development of these competencies ensuring their congruence with demonstrated workplace need, and readiness for implementation within WACHS.
1.1 Project Context WACHS is the state government provider of health services to rural and remote Western Australia. Geographically, WACHS covers in excess of 2.5 million square kilometres and has a combined regional population of nearly half a million people (representing almost a third of the state’s population), and includes approximately 44,900 Aboriginal people (Department of Health Western Australia, 2006). It is divided into seven health regions across the state including Kimberley, Pilbara Gascoyne, Midwest Murchison, Wheatbelt, Goldfields South East, South West and Great Southern (Department of Health Western Australia, 2006). Figure 1: WACHS Health Regions

3
WACHS is charged with the delivery of acute and primary health services to regional WA and delivers these services through 70 hospitals and a large number of smaller health services and nursing posts, including: aged care facilities; health centres; child, community, dental, alcohol & drug, mental and public health facilities (Department of Health Western Australia, 2006). Within this portfolio, WACHS provides the majority of the allied health services to rural and remote Western Australia, including physiotherapy, speech pathology, occupational therapy, social work, dietetics, audiology, podiatry and pharmacy (Department of Health Western Australia, 2006). Senior staff within each of these disciplines are employed by WACHS under the Hospital Salaried Officers Association (HSOA) generally as Level 7 staff. These senior staff members are charged with higher duties than general allied health professionals, which may include a clinical role, the management and planning of service delivery, staff management and various other context specific duties.
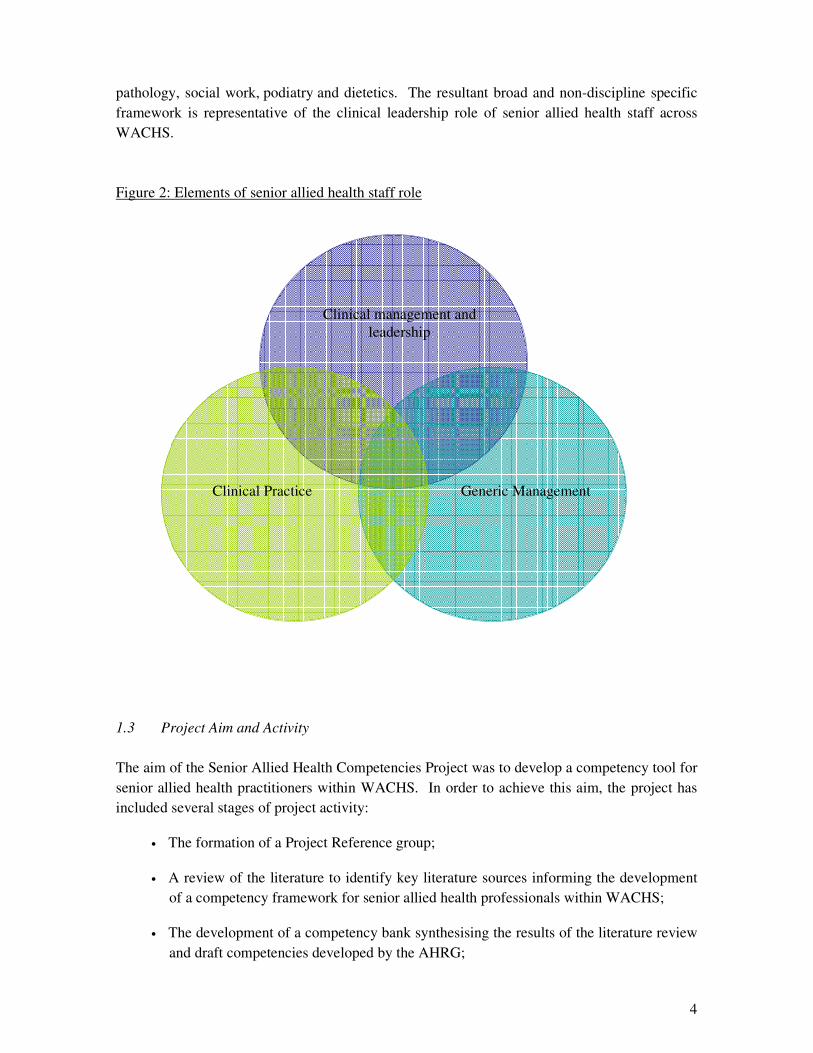
1.2 Project Scope We view competencies for senior staff in a rural and remote context as a combination of skills across three broad domains (Figure 2):
a. clinical skills; b. generic management; and c. clinical management and leadership.
Clinical skills are those that apply to a specific discipline or programs in which senior AHPs deliver services. Competency frameworks for these skills are provided on a discipline specific basis by professional associations, governing boards, or program leadership organisations. By generic management skills, we refer to competencies which have applications in a range of contexts, and are not specific to the allied health environment. These include communication skills, conflict resolution, teamwork, staff development etc. Whilst alluding broadly to the first two domains, our focus in developing a senior competency framework is on clinical management and leadership in the rural and remote context. By clinical management and leadership we refer to those skills required to manage and lead service delivery in the rural environment. This includes skills specific to people management in the health environment, and service management and leadership (including planning, delivery, and evaluation of health services), with view to enhanced community health, better client care and improved practice. In focusing on this group of skills this competency framework aims to best support senior allied health staff in their work practice. The precise role of senior AHPs is highly variable, contingent on discipline, service organisation, local management structures, local AHP staff numbers and classification, and the presence of local senior management staff. Given this variability, the scope of the competencies has been limited to ensure its manageability and relevance to senior allied health staff as a generic group. Additionally, the identified competencies focus on skill areas common to a core group of disciplines, including audiology, occupational therapy, physiotherapy, speech
4
pathology, social work, podiatry and dietetics. The resultant broad and non-discipline specific framework is representative of the clinical leadership role of senior allied health staff across WACHS. Figure 2: Elements of senior allied health staff role
1.3 Project Aim and Activity The aim of the Senior Allied Health Competencies Project was to develop a competency tool for senior allied health practitioners within WACHS. In order to achieve this aim, the project has included several stages of project activity:
• The formation of a Project Reference group;
• A review of the literature to identify key literature sources informing the development of a competency framework for senior allied health professionals within WACHS;
• The development of a competency bank synthesising the results of the literature review and draft competencies developed by the AHRG;
Clinical Practice
Generic Management
Clinical management and leadership
5
• Broad consultation with senior allied staff and management across WACHS through a Delphi Review process. This review included several phases:
o An initial round, targeted at allied health managers and senior allied health staff from occupational therapy, physiotherapy, speech pathology, social work and dietetics, in each of the WACHS regions; and
o Targeted focus groups with senior staff and management across the WACHS regions.
o A final broad review with the dissemination of draft the framework for comment and feedback from a broad audience, including the AHRG, Population Health Directors, and all Senior AHP within WACHS.
• The ongoing development of draft competencies based on consultation;
• The reorganisation of the draft competencies within a developmental framework;
• The finalisation and dissemination of the competency framework for senior allied health staff within the WACHS.
2. Project Reference Group A project reference group was established to advise and support the CUCRH Project Officer on aspects of project development and management. The Project Officer consulted with the Reference Group on a regular basis for the duration of the project. Additionally, group members reviewed project progress, promoted the project within their networks, and recruited participants for focus group participation.
Membership of the project reference group included: Alex Ellis (nee Mattson) Senior Physiotherapist WACHS Goldfields (Chair) Aasta Abbot Regional Coordinator Speech Pathology & Audiology WACHS
Midwest Dawn Logan Allied Health Coordinator & Senior Social Worker WACHS Pilbara Suzanne Spitz WA Country Health Service Ivan Lin Combined Universities Centre for Rural Health Nicole Beattie Project Officer - Combined Universities Centre for Rural Health

6
3. Ethics An exemption from formal ethics review for the development of the senior competencies was sought, and endorsed, by the Human Research Ethics Committee at the University of WA. This exemption was granted on the basis that the project met the National Health and Medical Research Council guidelines for quality assurance activities rather than pure research. 4. Literature Review A review of the available literature was undertaken looking at competencies and the use of competency frameworks in health management, with particular reference to the use of these tools in the allied health field. The literature review was driven by the following aims:
• To identify existing competency frameworks for senior rural and remote allied health professionals, in the absence of these, to identify other competency frameworks with applicability to senior rural and remote allied health professionals; and
• To catalogue a bibliography of pertinent literature in this area. 4.1 Search Strategy Several peer reviewed and non-peer reviewed databases were searched to identify literature and project activity in this area. These included: Cinahl; Cochrane Library; Medline; Pubmed; ProQuest; and Google Scholar. A Google web-search was also undertaken to identify non-published material available on the World Wide Web.
Search restrictions were used to confine results to those most relevant to the research topic. These included materials published in the last 17 years (since 1990). A series of key words were used to direct searches, these were searched in combination to retrieve the most relevant resources. As per the Senior Allied Health Competencies Project Plan, searches were focused on the terms: rural and remote; allied health; senior; management; and clinical leadership. Additional terms were also included based on initial search results, these included: competence truncated; self assessment; standards; professional practice; skills frameworks; leadership; performance management; and guidelines. Several additional exclusion criteria were employed to sort results, as detailed in Section 4.2: Search Results.
The reference lists of each of the relevant publications retrieved in the review process were also reviewed. Web based searches were expanded to look at specific projects identified within the initial literature base. These strategies allowed for the identification of additional publications and project materials. Additional strategies were employed to highlight gaps in existing literature and the most relevant resources from within the literature base. Specifically, this
7
included the review of WACHS Job Description Forms (JDFs) for senior allied health positions and professional standards available on Australian allied professional association websites.
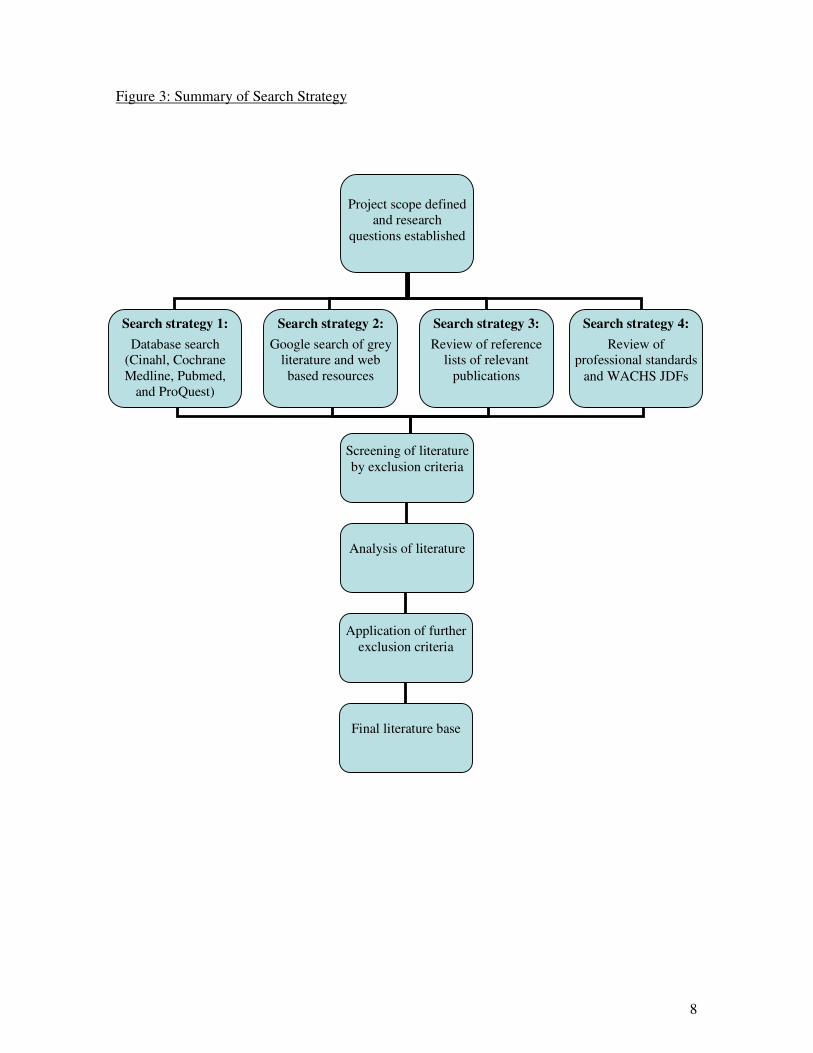
4.2 Search Results The literature review yielded two different categories of literature. The first included publications, primarily journal articles and book chapters, around competencies and competency frameworks broadly. These focused on the value, application and applicability of competency frameworks to the health, allied health, specific disciplines, management or education. With the exception of those that included or made reference to a relevant existing competency frameworks (Adamson, Lincoln et al. 2000; Baker 2003; Pruitt and Epping-Jordan 2005; Verma, Paterson et al. 2006), publications of this nature were discarded as too broad, lacking in depth, or failing to articulate with the prescribed project aims. The second category of literature emerging from the review included specific competency frameworks. A vast number of existing competency frameworks were retrieved principally from project reports and online resources. While all addressed competencies of health service delivery, they varied in focus and complexity to include: reviews and comparisons of existing standards, and suggested holistic frameworks; broad frameworks oriented towards specific service delivery models and aimed at a multi-skilled staff base; those that focused at different institutional levels, including the organisations level, management, specific disciplines, and entry level; those aimed at the clinical management of specific chronic conditions, such as stroke; and those with a specific area of practice, such as rural and remote or a non-Australian context. Much of the literature, specifically competency standards targeted at: entry level practitioners; the management of specific conditions; clinical skills only; and very broad models, were discarded to ensure an adherence of the literature to the aims outlined in the project proposal. Retained resources were directly relevant to clinical management competencies of senior allied health professionals. These references are summarised in the Bibliography of this report
8
Figure 3: Summary of Search Strategy
Project scope defined
and research questions established
Search strategy 1: Database search
(Cinahl, Cochrane Medline, Pubmed,
and ProQuest)
Search strategy 2: Google search of grey
literature and web based resources
Search strategy 3: Review of reference
lists of relevant publications
Search strategy 4: Review of
professional standards and WACHS JDFs
Screening of literature by exclusion criteria
Analysis of literature
Application of further exclusion criteria
Final literature base

9
4.3 Key Findings The competency frameworks identified in the literature were catalogued by overarching competency areas (see Appendix A). While aspects of several of the identified competency standards articulated with clinical management and leadership competencies of senior AHPs working with the WACHS none independently captured the roles and responsibilities of senior allied health professionals working within WACHS (see Skills for Health; Family Planning Management Development Technical Unit 1998; Pew Health Professions Commission 1998; The Accreditation Council of Graduate Medical Education 1999; National Centre for Healthcare Leadership 2003 ; Agenda for Change Project Team 2004; Prime R&D Ltd and Skills for Health 2004; Skills for Health 2004; Australian Council for Safety and Quality in Health Care 2005; Department of Human Services Victoria 2005; National Centre for Healthcare Leadership 2005; Pruitt and Epping-Jordan 2005; Queensland Health and Griffith University 2006; Skills for Health 2003; Skills for Health 2006; American Association of Colleges of Nursing 2007 for those competencies that had limited articulation). Despite the growing prevalence of competency frameworks and assessment in health, very little of the available literature focuses on the skills and knowledge required of senior allied health staff specifically (Gardner and Boucher 2000). While a vast quantity of competencies can be identified within the ‘scattered and fragmented’ (Gardner and Boucher 2000, p. 3) body of literature ‘so far there has been little attempt to present a comprehensive competency framework’ (Gardner and Boucher 2000, p. 3) for allied health. Further, the small existing literature body in this area is drawn mainly from the United States and United Kingdom. It is not representative of an Australian context, much less allied health service delivery in rural and remote Western Australia. Despite this lack of relevant competency frameworks, there is a clear and established need for the development of such competencies. The literature recognises a clear role for competencies, and frameworks articulating these, in health practice (Gardner and Boucher 2000; Department of Human Services Victoria 2005; Pruitt and Epping-Jordan 2005; Rosing and Gassiot 2005; Glasgow, Wells et al. 2006; Skills for Health 2006; Verma, Paterson et al. 2006), thus validating this project. While not directly transferable for a senior allied practitioner competency model working within WACHS, a thematic analysis of the competencies and domain areas in existing models identified within the literature reflected a series of reoccurring key themes, which contributed to the development of a WACHS senior competency model. These included: • Management skills • Human recourses • Leadership skills • Health and safety • Clinical practice • Ethics and professional practice • Policy • Workforce planning • Strategic planning / governance • Education and professional development • Technology • Cultural awareness • Research and evaluation • Financial and physical resource management

10
In addition to the identification of reoccurring themes, the literature review also saw the development of a bibliography of pertinent literature in this area, catalogued in an Endnote library of relevant resources and existing competency frameworks.
5. Development of Draft Competencies In the formative stages of this project, the New Graduate, Management Support and Development Team within the AHRG developed a bank of draft competencies in consultation with WACHS allied health managers and senior staff. This consultation included two phases. During the first phase, HSU Level 8 allied health staff and above, including regional discipline coordinators and allied health managers, were emailed and asked to identify competencies relevant to the generic practice of senior allied health staff. Six email responses providing feedback were received.
Managers and seniors were invited to participate in the second phase of consultation. Two focus groups sessions were conducted: One face-to-face meeting with a single participant; and one teleconference attended by three senior staff. Both sessions ran for approximately one hour and were used to further develop the responses received during the first phase of consultation.
The resulting body of competencies were then compiled by a member of the New Graduate and Management Support and Development team, with the assistance of a therapy assistant and grouped under headings contained within the EQuIP 3 framework. At the commencement of the current project (some time after its initial compilation), this competency bank was then reviewed by the CUCRH Project Officer and refined to identify competencies related only to clinical management and leadership, increase clarity, reduce repetition, and to reorganise the competencies under the recently released EQuIP 4 guidelines.
6. Delphi Review In order to ensure the validity and appropriateness of the competency framework a Delphi Review was undertaken with relevant stakeholders. Broadly, Delphi is a technique employed to gain consensus on a particular subject or problem from a large number of an often geographically dispersed group (Turnoff and Linstone 2002). In order to gain this consensus, stakeholders are asked provide to feedback on the particular subject or problem. In response to this feedback the original subject or problem is reviewed and further developed, then returned to stakeholders for further feedback. This review process is repeated several times until consensus is reached.

11
According to Turnoff & Linstone (2002), a variety of methods may be employed within a Delphi Review, and may include: surveys or questionnaires; teleconference or videoconference; one on one face to face meetings; group interactions; and other interactions. Turnoff and Linstone (2002) suggest that ‘there are instances where it is desirable to use a mix of these approaches’. In line with Turnoff & Linstone, the Delphi Review employed in this project included several Delphi methods, including: a ranking exercise; focus groups; and a WACHS review, utilised over a total of three rounds of Delphi.
6.1 First Round: Ranking Exercise
The first round of the Delphi Review consisted of a ranking exercise in which AH seniors were required to rank each competency outlined within the draft framework on a 3 point scale for appropriateness for seniors (1; Realistic expectation, 2; Should be developing, 3; Not relevant or expected), and importance in practice [High Priority (essential for practice), Medium Priority (Important for practice), Low Priority]. Additionally, two open-ended questions prompted participants to identify areas in need of further development and provide additional comments.
The ranking exercise, with the draft competency bank, was distributed to primary health managers and allied health managers across all WACHS regions. The draft bank was then disseminated by managers to allied health seniors within the targeted disciplines, including occupational therapy, physiotherapy, speech pathology, social work, audiology and dietetics. A reminder email was sent directly to seniors by the CUCRH Project Officer one week after the specified due date for feedback.
A total of 34 responses were received. These represented all targeted disciplines, and included: four allied health managers, seven physiotherapists, four social workers, four speech pathologists, eight occupational therapists, three dieticians, and four responses from three other allied health disciplines, including podiatry, health promotion and audiology. These responses came from across the WACHS regions, and included three from the Kimberley, four from the Pilbara, two from the Midwest, eight from the Wheatbelt, seven from the Great Southern, six from the South West, three from the Goldfields and one unspecified.
Table 1: Ranking Exercise responses by discipline
Discipline Number Allied health Management 4 Physiotherapist 7 Social Worker 4 Speech Pathologist 4 Occupational Therapist 8 Dieticians 3 Other discipline 4 Total 34

12
Table 2: Ranking Exercise responses by WACHS region
WACHS Region Number Kimberley 3 Pilbara 4 Midwest 2 Wheatbelt 8 Great Southern 7 South West 6 Goldfields 3 Unspecified 1 Total 34
Of the 34 responses received, 18 provided only written feedback and 26 provided both written and numeric feedback. Written feedback was used to identify gaps, and additional areas of interest within the draft. Numeric responses were tabulated and analysed to assess the relevance and appropriateness competencies within the draft bank.
Analysis of numeric responses reflected a high correlation between the appropriateness and importance of competencies. All but one competencies of the 109 within the early draft framework (Possesses and employs financial monitoring skills, with an average rating of 2.2), had an average rating of between one and two on both scales (that is: realistic expectation or should be developing; or high priority or medium priority), suggesting all competencies1 were considered both important to appropriate. While still considered important and relevant within senior allied health practice, some competency areas outlined within the draft framework were rated more poorly than others. Of particular note:
• Competencies relating to consumer involvement, such as ‘facilitates consumer consultation in health service planning and development’, and ‘facilitates consumer engagement in health service planning and development’ had an average rating of 1.8 and a mode of 2 for appropriateness, and an average of 1.95 and a mode of 2 for importance.
• Competencies within the domain of research and evaluation, namely ‘researches and evaluates allied health activities’ and ‘investigates and evaluates innovative service delivery methods’, had an average rating of 1.75 and a mode of 2 for appropriateness, and an average of 1.95 and a mode of 2 for importance.
• Competencies pertaining to financial skills, including ‘possesses and employs financial monitoring skills’ and ‘is able to effectively manage resource planning and allocation’,
1 With the exception of the afore mentioned financial competency.

13
had an average rating of 1.9 and a mode of 2 for appropriateness, and an average and mode of 2 importance.
• Additionally, some competencies relating to quality improvement, facilities and resources, human resources systems, staffing, information management, policies and guidelines and strategic planning were considered to be of limited appropriateness and importance.
Based on written and numeric responses, the draft competency document was reviewed and restructured by the CUCRH Project Officer. The review focused on re-ordering competencies to reflect the hierarchy (of both relevance and appropriateness) identified in the analysis of feedback provided, the development of additional competencies to include competence areas identified by respondents, further refining existing competencies, particularly increasing clarity and further reducing repetition.
6.2 Second Round: Focus Groups The second round of the Delphi Review included two sets of two focus groups, conducted with participants from across the WACHS regions and from all allied health disciplines across the scope of the competency framework. Initially two groups were run. All those that had participated in the ranking exercise were contacted by emailed and invited to participate in focus groups. An additional email was sent one week later to those who had not responded, again inviting participation in the focus groups. Of the 34 people contacted, eight people from two regions agreed to participate, four declined, 20 failed to respond to either email, and two were on leave at the time when focus groups were scheduled and subsequently could not attend. Following the first round of focus groups, the CUCRH Project Officer consulted with the Project Reference Group regarding subsequent groups. It was determined that two additional focus groups should be conducted. Owing to the limited response from AHP’s in the coordination on the first round, participants for the two additional sessions were recruited by two members of the AHRG within their respective regions. The majority of these participants had not participated in the ranking exercise. For each of the four groups, participants were provided with the draft competency framework, and a supporting document outlining the project background and the intended use and scope of the competency framework, one week prior to the focus group. Participants were asked to reflect on their own practice, and that of their colleagues in reviewing the document. At the commencement of focus groups participants were again provided with a brief summary of the project, and the intended use and scope of the competency framework was reiterated. Again participants were asked to reflect on their own practice, and that of their colleagues in their comments. Focus groups lasted between 60 and 90 minutes, and followed the schedule outlined below:

14
• First, participants were asked to discuss, and provide feedback on, the competency framework at macro level. This included a discussion of the overall format of the document, the length, structure, and potential usefulness and relevance of the tool.
• Second, the facilitator (the CUCRH Project Officer) led participants through the competency framework on a domain by domain basis. Participants were asked to revisit each domain in turn and comment on: the relevance of the domain; the validity and appropriateness of each competency within the domain; and any additional competencies that fell within that domain in their practice and that of their senior level colleagues.
• Finally, participants were asked to again comment on the overall competency framework. Discussion was directed towards: the representativeness of the clinical leadership and management role of senior AH staff in the document; the relevance, usefulness and appropriateness of the competency document; gaps in the framework; the organisation and structure of the framework. Participants were then asked for any additional comments and feedback.
The first set of focus groups included both a face to face meeting and a videoconference session. The face to face meeting included 3 participants, including the regional coordinators for speech pathology and audiology, and occupational therapy and a senior dietician. The video conference included three sites, including the host site, and was attended by four participants, including an allied health team leader and seniors from physiotherapy, speech therapy and occupational therapy. Based on the feedback provided in these sessions the draft competency document was refined further, again focusing on re-ordering competencies according to hierarchy, developing additional competencies to include competence areas identified by respondents, further refining existing competencies, particularly increasing clarity, and further reducing repetition. The second set of focus groups again included a face to face meeting and a videoconference session. The face to face meeting was attended by four participants, including: the regional physiotherapy coordinator; a senior audiologist; the drug and alcohol coordinator; and a Level 4/6 occupational therapist (acting in a senior position). The videoconference was conducted with a single site, and included five participants, including: two senior physiotherapists; one social worker, a speech therapist; and a podiatrist. The feedback provided was used to finalise the hierarchy of the competencies within the draft document, to further refine existing competencies, and to increase the clarity of the document.

15
Table 3: Focus group Participation
Regional speech pathology and audiology coordinator Regional occupational therapy coordinator Face to Face
Senior dietician Allied health team leader Senior Physiotherapist Senior Speech Therapist
Round 1
Videoconference
Senior Occupational Therapist Regional physiotherapy coordinator Senior audiologist Regional drug and alcohol coordinator
Face to Face
Level 4/6 occupational therapist Senior Physiotherapist Senior Physiotherapist Senior social worker Senior speech therapist
Round 2
Videoconference
Podiatrist
Based on focus groups both the first and second set of focus groups, the draft competency document was further reviewed by the CUCRH Project Officer and members of the Project Reference Group. The review focused on sorting competencies, developing additional competencies to include competence areas identified by focus group participants, the further refining existing competencies, particularly increasing clarity and further reducing repetition. In addition to refinements to the draft framework, focus groups allowed participants to express thoughts on a number of related issues. Several themes were identified on numerous occasions:
• The specific role of rural and remote allied health staff: Participants consistently identified the divergence in role of metropolitan allied health practitioners and those working in a rural and remote context. Participants suggested that the competency document must capture these differences in order to be useful.
• The diverse role of allied health seniors: Participants were quick to identify the diverse role of allied health seniors across the targeted disciplines and that in each of the WACHS regions, dependant on the local context. In order for the competency document to be meaningful, participants suggested the framework must adequately capture this multiplicity.
• The availability of training: Several participants identified the current limited availability of training for allied health seniors to support staff development in the competencies

16
within the framework. In the absence of appropriate training the capacity of allied health seniors to acquire the competencies was seen to be constrained.
• Implementation: While the value of the competency document was recognised by participants, concerns were raised as to its implementation. Specific concerns centred on where responsibility for implementation would fall; that is to seniors, supervisors, managers, or others. Several participants suggested that without a clear and monitored implementation strategy, the uptake of the competency framework would likely be limited. Further, the current capacity of allied health managers and seniors to take on this role was minimal.
6.3 Third Round: WACHS Review The final round of the Delphi Review consisted of a WACHS wide allied health review. The draft competency framework was circulated via email to all WACHS allied health senior staff and managers by the Chair of the reference group. Staff were asked to review the document as a final draft and invited to provide comment. A total of 14 staff responded. Feedback was consistently positive and included comment on language, wording, grammar, and clarity. Comments such as: ‘the competencies are looking really good, I wouldn’t have anything to add or change at this stage’ typical. Based on the final round of feedback minor changes relating to grammar, spelling, language, and format were incorporated into the final draft document. 7. Organisation within a Developmental Framework
While the senior competency framework was initially organised under the EQuIP guidelines, the final stage of the project saw the reorganisation of the framework within a developmental model. The aim of this project was to create a tool for staff development, not solely self assessment. That is, the tool was designed to be used to guide and support staff in identifying learning and development needs. While the EQuIP guidelines proved useful in the formative stage of the project they lacked the necessary developmental focus for their ongoing application and use. As such, competencies structured under these guidelines were difficult clearly link to developmental goals and outcomes.
In order to maximise the usefulness of the framework, the final draft document was restructured under a developmental model. The model used was adapted from one recently developed in WACHS nursing, and is also in-line with Australian Curriculum Framework for Junior Doctors (Confederation of Postgraduate Medical Education Councils, 2003).
17
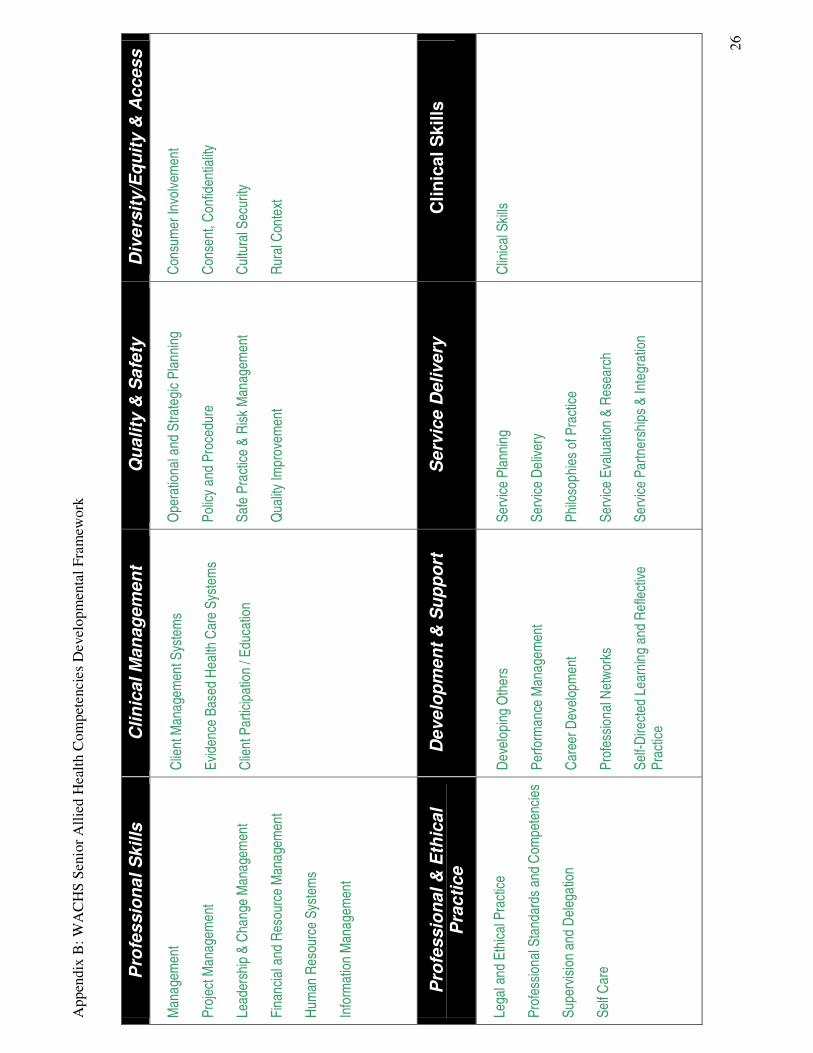
The developmental framework adopted as an organising framework for the senior competencies is comprised of eight domains:
• Service Planning • Clinical Management • Quality and Safety • Development and Support • Professional Skills • Clinical Skills • Equity, Access and Diversity • Professional & Ethical Practice
The sixty four competencies within the framework have been organised into these domain categories (see Appendix B for further detail), providing a clear links between individual competencies, and boarder competence areas, and skill development domains. The final draft of the DRRSAHC document is including in this document as Appendix C.
In addition in increasing the useability of the document for senior allied health staff, this developmental orientation allows for greater identification of skill sets and training needs common across the professional groups of allied health, nursing and medicine. Potentially this allows for greater inter-professional learning and increases the capacity for shared training between professional groups, particularly benefiting allied health staff in rural and regional areas. 8. Conclusion This project has seen the development of a competency framework for WACHS senior AHPs. Together with the DRRAHC – EP framework, this document is intended to better equip and support the rural and remote AHP workforce within WACHS. Like the DRRAHP-EP, the senior competency framework will be used to identify learning and developmental needs and areas of strength and proficiency for WACHS senior AHPs. In order to ensure the successful implementation of the senior competency framework a multifaceted strategy targeting both AH management and senior AH staff should be employed, with sufficient support for AH staff during this process. A broad dissemination of the senior competency framework has been planned (project launch, email, presentations at meetings, conference presentations, inclusion on intranet) to inform key stakeholders across WACHS. Finally, it will be important to evaluate the senior competency framework six to twelve months following implementation. An evaluation should measure the effectiveness of the implementation itself, the uptake of the tool, and relevance and utility for senior AHPs within WACHS.
18
9. Bibliography Adamson, B., M. Lincoln, et al. (2000). "An analysis of managerial skills for the current and future health care environment" in Journal of Allied Health 29(4): 203-213.
Agenda for Change Project Team (2004). The NHS Knowledge and Skills Framework (NHS KSF) and the Development Review Process. UK Department of Health. Retrieved July 2007, from: www.dh.gov.uk/PolicyAndGuidance/HumanResourcesAndTraining/ModernisingPay/ AgendaForChange/fs/en
American Association of Colleges of Nursing (2007). White Paper on the Education and Role of Clinical Nurse Leader. American Association of Colleges of Nursing. Retrieved August 2007, from: http://www.aacn.nche.edu/Publications/WhitePapers/ClinicalNurseLeader.htm.
Australian Council for Safety and Quality in Health Care (2005). National Patient Safety Education Framework, Canberra. Commonwealth of Australia.
Baker, R. (2003). "Identifying and Assessing Competencies: A Strategy to Improve Healthcare Leadership", in Healthcare Papers 4(1): 49-58.
Confederation of Postgraduate Medical Education Councils (2003). “Australian Curriculum Framework for Junior Doctors”, Retrieved 1st February 2008, from http://www.cpmec.org.au/curriculum/welcome.cfm.
Department of Health Western Australia. (2006). "WA Country Health Service", Retrieved 24th July 2007, from http://www.wacountry.health.wa.gov.au/.
Department of Human Services Victoria (2005). Competency standards for health and allied health professionals in Australia, Department of Human Services, Victoria, Australia. Retrieved July 2007, from: http://health.vic.gov.au/workforce/downloads/core_clinical_ skills_ mapping. pdf.
Family Planning Management Development Technical Unit (1998). The Health and Family Planning Manager's Toolkit: Supervisor Competency Self-Assessment Inventory, Family Planning Management Development Technical Unit. Retrieved August 2007, from: http://erc.msh.org/newpages/english/toolkit/supervis.pdf.
Gardner, I. and C. Boucher (2000). Reflective Practice as a Meta-competency for Australian Allied Health Managers. RMIT Business Working Paper Series.
Glasgow. N, Wells. R, Butler. J, Gear. A, Lyons. S & Rubiano. D, (2006). Using Competency-Based Education to Equip the Primary Health Care Workforce to Manage Chronic Disease, Australian Primary Health Care Research Institute, ANU College of Medicine & Health Sciences Hartley, J. and B. Hinksman (2003). Leadership Development: A Systematic Review of the Literature. A report for the NHS Leadership Centre, Warwick Business School. National Centre for Healthcare Leadership (2003). Allied Health Professionals Self-Assessment Tool, National Primary and Care Trust Development Programme. Retrieved August 2007, from: http://www.natpact.nhs.uk/uploads/aph_framework.pdf.

19
National Centre for Healthcare Leadership (2005). Health Leadership Competency Model: Summary, National Centre for Healthcare Leadership. Retrieved August 2007, from: http://www.nchl.org/ns/documents/CompetencyModel-short.pdf. Pew Health Professions Commission (1998). Recreating Health Professional Practice for a New Century, The Fourth Report of the Pew Health Professions Commission. San Francisco. Pew Health Professions Commission. Retrieved August 2007, from http://www.futurehealth. ucsf.edu/pdf_files/recreate.pdf. Prime R&D Ltd and Skills for Health (2004). Map of Competences for Remote and Rural Healthcare. Skills in Health. Retrieved August 2007, from http://www.skillsforhealth.org.uk /uploads/remote_and_rural_healthcare_competences.pdf.
Pruitt, S. D. and J. E. Epping-Jordan (2005). "Preparing the 21st century global healthcare workforce" In British Medical Journal 330(7492): 637-639.
Queensland Health and Griffith University (2006). Audit of the Training and Education Needs of Staff Working in Community Based Rehabilitation in Queensland, Queensland Health & Griffith University. Retrieved August 2007, from: http://www.health.qld.gov.au/qhcrwp/.
Rosing, J. J. and C. C. A. Gassiot (2005). AHP Competencies: A Method for Effective Assessment, HCPro.
Skills for Health. Learning and Development Competencies, Retrieved 21 June, 2007, from http://www.skillsforhealth.org.uk/tools/view_framework.php?id=83.
Skills for Health. (2003). Allied health professions project: Demonstrating competence through continuing professional Development (CPD). Retrieved July 2007, from: http://www.dh.gov.uk/en/Consultations/Closedconsultations/DH_4071458. "Skills for Health. (2004). "Workforce Planning Competencies", Retrieved 21 June 2007, from http://www.skillsforhealth.org.uk/tools/view_framework.php?id=105. Skills for Health (2006). Allied Health Professions Competence Project: National Reference Group Workshop Report.
Turoff, M. and H. Linstone (2002). The Delphi Method: Techniques and Applications M. Turoff and H. Linstone, New Jersey Institute of Technology. Online book, retrieved Septemberr 2007, from http://is.njit.edu/pubs/delphibook/.
Verma, S., M. Paterson, et al. (2006). "Core competencies for health care professionals: what medicine, nursing, occupational therapy, and physiotherapy share" in Journal of Allied Health 35(2): 109.
Whelan, L. "Competency assessment of nursing staff." in Orthopedic Nursing 2006 May; 25(3): 198-204.

20
10. Appendices Appendix A: Catalogue of Relevant Competency Frameworks Author Title Competencies / Domains Skills for Health
Management and Leadership Competencies
• Manage your own resources and professional development • Develop your personal networks • Develop and implement operational plans for your area of responsibility • Map the environment in which your organisation operates • Develop and action a strategic business plan for your organisation and put into
action • Provide leadership for your team, in your area of responsibility and for your
organisation • Ensure compliance with legal, regulatory, ethical and social requirements. • Develop the culture of your organisation • Manage risk • Promote equality of opportunity and diversity in your area of responsibility and in
your organisation • Encourage innovation in your team, your area of responsibility and in your
organisation • Plan, implement and lead change • Develop productive working relationships with colleagues and stakeholders • Recruit, select and keep colleagues • Plan the workforce • Allocate and check work in your team • Allocate and monitor the progress and quality of work in your area of
responsibility • Providing learning opportunities for colleagues • Manage a budget and finance for your area of responsibility • Obtain additional finance for the organisation • Promote the use of technology within your organisation • Ensure your own actions reduce risks to health and safety • Ensure health and safety requirements are met in your area of responsibility • Ensure an effective organisational approach to health and safety • Manage a project • Develop and review a framework for marketing • Resolve customer service problems • Monitor and solve customer service problems • Support customer service improvements • Work with others to improve customer service • Build your organisation's understanding of its market and customers • Develop a customer focussed organisation • Manage the achievement of customer satisfaction • Improve organisational performance
Skills for Health
Workforce Planning competencies
• Identify the purpose and scope of a workforce plan • Identify and evaluate forces for change that may impact on the workforce • Contribute to preparing for workforce planning based on service needs • Assess workforce demand and supply • Develop a workforce plan • Implement and review a workforce plan • Contribute to developing and implementing a workforce plan

21
Skills for Health
Learning and Development competencies
• Assess candidates using a range of methods • Develop a strategy and plan for learning and development • Identify individual learning aims and programmes • Design learning programmes • Develop training sessions • Prepare and develop resources to support learning • Manage the contribution of other people to the learning process • Create a climate that promotes learning • Enable learning through presentations, demonstrations, instruction and coaching • Enable group learning • Support learners by mentoring in the workplace • Monitor and review progress with learners • Evaluate and improve learning and development programmes • Respond to changes in learning and development • Support competence achieved in the workplace • Plan how to provide basic skills in the workplace • Introduce training for basic skills in the workplace • Support how basic skills are delivered in the workplace • Support people learning basic skills in the workplace • Conduct internal and internal quality assurance of the assessment process
Queensland Health, 2006 and Griffith University
Competencies for CR in Queensland for allied health, nursing and support staff
• Frameworks of understanding • Consumer engagement • Holistic focus • Service continuity • Networks • Cultural awareness • Community engagement • Boundaries and safety • Reflective practice
Family Planning Management Development Technical Unit
Supervisors competency self assessment inventory
• Gain acceptance as a supervisor • Develop individual work plans • Maintain a high level ff performance • Conduct formal performance review meetings • Deal with performance problems • Manage conflict between employees • Counsel troubled employees • Time management
American Association of Colleges of Nursing
White Paper on Education and Role of the Clinical Nurse Leader
• Critical thinking • Communication • Assessment • Technology and resource management • Health promotion, risk reduction and disease prevention • Illness and disease management • Information and health care technologies • Ethics • Human diversity • Global health care • Health care systems and policy • Provider and manager of care • Designer / Manager / Coordinator of Care • Member of Profession

22
Prime & Skills for Heath (UK)
Map of competencies for remote and rural health care – community practice based health care
Core areas • Foundations of ethical and effective practice • Leading and developing individuals and teams • Evaluation and Research Organisational / Management areas • Health needs assessment – population level • Working with and for communities to improve health and wellbeing and address
related needs • Development of organisational and area policies, strategies and plans to improve
health and wellbeing and address needs • Development of quality programs and services • Resource acquisition, management and coordination Front line health and healthcare areas • Promotion of health and wellbeing and prevention from adverse effects on health
and wellbeing • Protection of the population form harm • Diagnosis, treatment and management of undifferentiated illness of individuals
who are ill or believe that they are ill • Assessment, treatment and care of individuals with health and wellbeing needs • Management of long-term conditions • Provision of palliative care • Management of accidents and emergencies • Procurement and dispensing of medication
Skills for Health
Allied Health Professions Competences Project
• Assessment and Investigation of health • Planning for and addressing health requirement s • Promotion and protection of health • Support of health care through technology • Provision of facilities and estates for health care • Development and sharing of information and knowledge on health • Management of the provision of health care • Education and learning around health
ACT Health Standards of Practice for ACT Allied Health Professionals
• Standards pertaining to interaction with the client • Standards pertaining to the health professional • Standards pertaining to the environment • Standards pertaining to professional colleges • Standards pertaining to the community
NHS NHS Knowledge and Skills Framework
Core • Communication • Personal and people development • Health, safety and security • Service improvement • Quality • Equality and diversity Specific • Health and wellbeing • Estates and facilities • Information and knowledge • General

23
NHS NHS Leadership Qualities Framework
Personal Qualities • Self belief • Self awareness • Self management • Drive for improvement • Personal integrity Setting direction • Seizing the future • Intellectual flexibility • Broad scanning • Political astuteness • Drive for results Delivering the service • Leading change through people • Holding to account • Empowering others • Effective and strategic influencing • Collaborative working
Skills for Health
AHP – consultant AHP competences
• Expert clinical practice • Professional leadership • Practice and service development, research and evaluation • Education and professional development
National Centre for Healthcare Leadership
Allied Health Professionals Self-Assessment Tool
• Leadership • Workforce • Corporate governance • Clinical governance • Commissioning and service development • Performance management • Access and choice • Partnership
National Centre for Healthcare Leadership
Health Leadership Competency Model: Summary
Transformation • Achievement Orientation • Analytical thinking • Communication orientation • Financial skills • Information seeking • Innovative thinking • Strategic orientation Execution • Accountability • Change Leadership • Collaboration • Communication skills • Impact and influence • Initiative • Information technology management • Organisational awareness • Performance management • Process management / organisational design • Project management People • Human resources management • Interpersonal understanding • Professionalism • Relationship building • Self confidence • Self development • Talent development • Team Leadership

24
The Accreditation Council for Graduate Medical Education
ACGME General Competencies
• Patient Care • Medical Knowledge • Practice Based Learning and Improvement • Interpersonal and communication skills • Professionalism • System based practice
Pew Health Professions Commission
• Embrace a personal ethic of social responsibility and service. • Exhibit ethical behavior in all professional activities. • Provide evidence-based, clinically competent care. • Incorporate the multiple determinants of health in clinical care. • Apply knowledge of the new sciences. • Demonstrate critical thinking, reflection and problem-solving skills. • Understand the role of primary care. • Rigorously practice preventive health care. • Integrate population-based care and services into practice. • Improve access to health care for those with unmet health needs. • Practice relationship-centered care with individuals and families. • Provide culturally sensitive care to a diverse society. • Partner with communities in health care decisions. • Use communication and information technology effectively and appropriately. • Work in interdisciplinary teams. • Ensure care that balances individual, professional, system and societal needs. • Practice leadership. • Take responsibility for quality of care and health outcomes at all levels. • Contribute to continuous improvement of the health care system. • Advocate for public policy that promotes and protects the health of the public.
Verma, Sarita Paterson, Margo Medves, Jennifer
Core Competencies for Health Care Professionals
• Communication • Consultation • Cooperation • Coordination • Collaboration • Collaborative practice
Pruitt, Sherri Epping-Jordon, Joanne (WHO)
Preparing a health care workforce for the 21st century
• Patient centred care • Partnering • Quality improvement • Information and communication technology • Public health perspective
The Australian Council for Safety and Quality in Health Care
The National Patient Safety Education Framework
• Communicating Effectively • Identifying, preventing and managing adverse events and near misses • Using evidence and information • Working safely • Being ethical • Continuing learning • Specific issues
Department of Human Services Victoria
Competency standards for health and allied health professional in Australia
Client service • Philosophy of care • Service delivery • Occupational body of knowledge Professionalism • Ethics • Equity • Performance improvement Workplace • Management • Team player • Occupational health and safety Communication
25
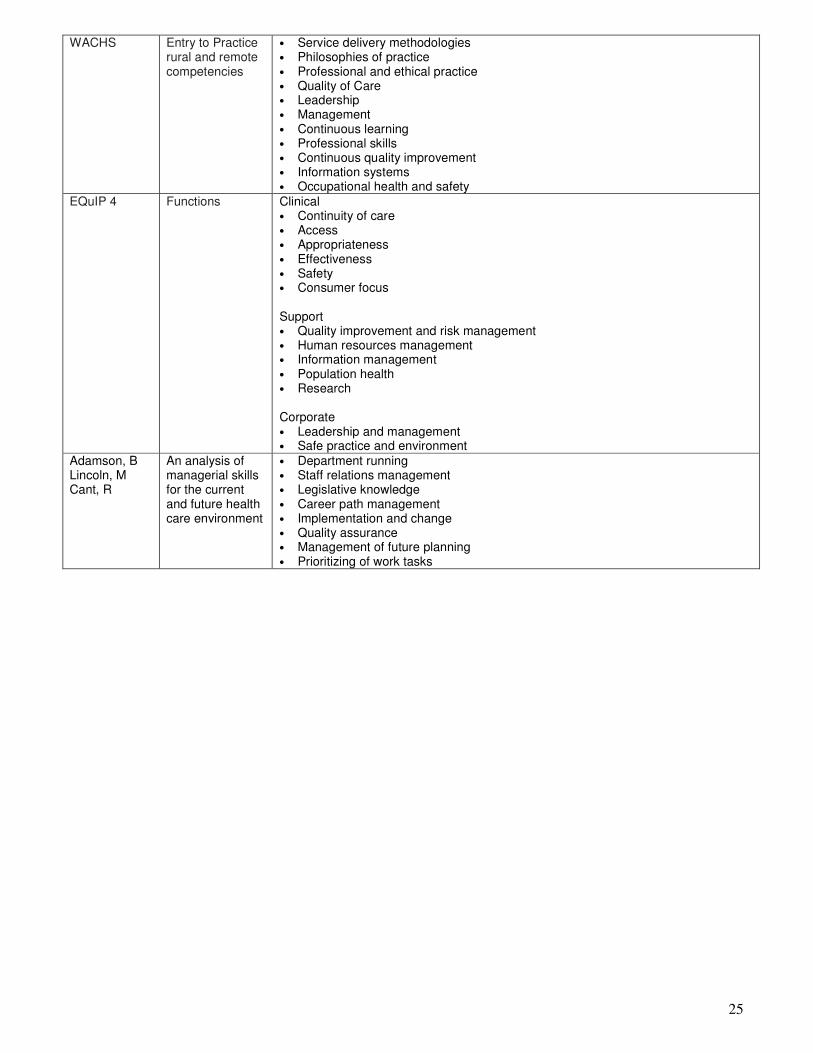
WACHS Entry to Practice rural and remote competencies
• Service delivery methodologies • Philosophies of practice • Professional and ethical practice • Quality of Care • Leadership • Management • Continuous learning • Professional skills • Continuous quality improvement • Information systems • Occupational health and safety
EQuIP 4 Functions Clinical • Continuity of care • Access • Appropriateness • Effectiveness • Safety • Consumer focus Support • Quality improvement and risk management • Human resources management • Information management • Population health • Research Corporate • Leadership and management • Safe practice and environment
Adamson, B Lincoln, M Cant, R
An analysis of managerial skills for the current and future health care environment
• Department running • Staff relations management • Legislative knowledge • Career path management • Implementation and change • Quality assurance • Management of future planning • Prioritizing of work tasks
26
App
endi
x B
: WA
CH
S Se
nior
Alli
ed H
ealth
Com
pete
ncie
s D
evel
opm
enta
l Fra
mew
ork
Pro
fess
iona
l Ski
lls
Clin
ical
Man
agem
ent
Qua
lity
& S
afet
y D
iver
sity
/Equ
ity &
Acc
ess
Man
agem
ent
Proj
ect M
anag
emen
t Le
ader
ship
& C
hang
e M
anag
emen
t Fi
nanc
ial a
nd R
esou
rce
Man
agem
ent
Hum
an R
esou
rce
Syst
ems
Info
rmat
ion
Man
agem
ent
�
Clie
nt M
anag
emen
t Sys
tem
s
Evid
ence
Bas
ed H
ealth
Car
e Sy
stem
s
Clie
nt P
artic
ipat
ion
/ Edu
catio
n
O
pera
tiona
l and
Stra
tegi
c Pl
anni
ng
Polic
y an
d Pr
oced
ure
Safe
Pra
ctice
& R
isk M
anag
emen
t Q
uality
Impr
ovem
ent
�
Cons
umer
Invo
lvem
ent
Cons
ent,
Conf
iden
tiality
Cu
ltura
l Sec
urity
Ru
ral C
onte
xt
Pro
fess
iona
l & E
thic
al
Pra
ctic
e D
evel
opm
ent &
Sup
port
S
ervi
ce D
eliv
ery
Clin
ical
Ski
lls
Lega
l and
Eth
ical P
ract
ice
Prof
essio
nal S
tand
ards
and
Com
pete
ncie
s
Supe
rvisi
on a
nd D
eleg
atio
n Se
lf Ca
re
Deve
lopi
ng O
ther
s
Perfo
rman
ce M
anag
emen
t Ca
reer
Dev
elop
men
t Pr
ofes
siona
l Net
work
s
Self-
Dire
cted
Lea
rnin
g an
d Re
flect
ive
Prac
tice
Serv
ice P
lann
ing
Serv
ice D
elive
ry
Philo
soph
ies
of P
ract
ice
Serv
ice E
valu
atio
n &
Rese
arch
Se
rvice
Par
tner
ship
s &
Inte
grat
ion
�
Clin
ical S
kills

27
Appendix C: Developing Rural and Remote Senior Allied Health Competencies Final Draft
�
������������� ���������������
��������������������������
����
��
�
�
Senior Allied Health Practitioners
Draft Jan 2008
A tool for developing
Senior Allied Health Competencies in rural
and remote practice
28
��
������������� ���������������
�������������������������� Developing Rural and Remote Allied Health Competencies – Senior Allied Health Practitioner
(DRRAHC - SAHP) is a framework and tool for facilitating continuing learning, development and planning
for senior allied health professionals. DRRAHC-SAHP is designed for use as a self-assessment tool to
assist in identifying individual learning and developmental needs and areas of strength and proficiency of
senior allied health staff working within the WA Country Health Service (WACHS).
DRRAHC-SAHP reflects a collation of identified clinical management and leadership competencies
developed relevant to a rural and remote context. It is not presumed that senior Allied Health Professional
(AHPs) require proficiency in all the identified competencies when working in the rural and remote context.
Neither is it presumed that this document reflects all competencies required and demonstrated when
working in the rural and remote context. The precise role of senior AHPs is dependent on several factors,
including discipline, health region, local management and staffing levels. As such workplace competency
will vary from region to region, site to site, and individual to individual. The DRRAHC-SAHP should not be
seen as absolute, rather as a resource and tool for senior AHPs, and their managers, to:
• Confirm individual areas of strengths.
• Identify learning opportunities to improve skills and practice.
• Identify and prioritise skills and competencies for growth and development.
• Build a plan for learning and development.
Whilst the task of attempting to define core senior allied health competencies in the rural and remote
context has been a challenge, the reward of a common framework that encompasses the skills necessary
for senior rural and remote practice is significant. This list of competencies, which transcends discipline
specific boundaries, is but the first step towards a comprehensive competency framework to guide senior
allied health workforce skill and development requirements in the rural and remote context. The tool
should be considered a dynamic document, which evolves and adapts to new learning and insight
regarding senior allied health competencies.

29
�������������������������������������
��������������������
A range of structures exist to support the life long learning of allied health professionals. These include
� Performance Management
� Clinical Supervision
� Contining Professional Development
� Mentoring and Coaching (to name a few)
The DRRAHC-SAHP is an important tool for application in a range of development contexts, and can be
easily applied in each of the above. The tool should form part of every senior allied health professional’s
resources for life-long learning and career development.
A simple framework for utilising the DRRAHC-SAHP as a self-assessment tool is detailed below. Self-
assessment involves learners in making judgements and reflections about their own practice, behaviour
and development. However to ensure that maximum benefit is obtained from the process it is suggested
that senior allied health professionals engage their manager, supervisor, peers, or mentor in all steps to
obtain additional feedback and support regarding appropriate competency assessment and learning plan
development.
This mix of self-assessment and assessment by others is referred to as co-assessment. Strengths in
using co-assessment can include (1) foster a feeling of ownership for learning, (2) motivate and encourage
active involvement in learning, (3) encourage autonomy in learning, and (4) create a shared learning
environment with exchange of ideas.
Step One. Identify the competency areas most relevant to current work role.
This tool identifies a range of competency areas that form part of senior rural and remote allied health
practice. This framework aims to provide a range of competencies generic to senior allied health practice
in rural settings. Some competencies may not be relevant to current work role. Read through the
document carefully and identify the competency areas that are of the most relevance to the current work
role. Where appropriate tick the box that denotes workplace relevance. If unsure, discussion with a
manager or with peers may assist. Additional space has been provided at the conclusion of the document
for competencies that are not identified on the document, but are of significant work role relevance.

30
Step Two. Assess competency in the areas of most relevance to the workplace.
The tool provides a framework to assess your competency in a range of areas. Assessment is carried out
by studying the evidence and matching it against criteria. A range of methods can be used to determine
your competency levels:
1. Self-reflection
2. Visual observation by a manager, peer or expert
3. Examining outcomes of practice
4. Written or oral supporting evidence
5. Questioning (to determine underpinning knowledge of the task or function)
6. Work related simulations or projects.
Step Three. Review the self-assessment and identify priority competency areas that require
development.
Step Four. Prepare a development plan.
Step Five. Put the development plan into practice.
Step Six. Reflect on progress.
Step Seven. Repeat the process regularly to identify changing professional development
requirements.
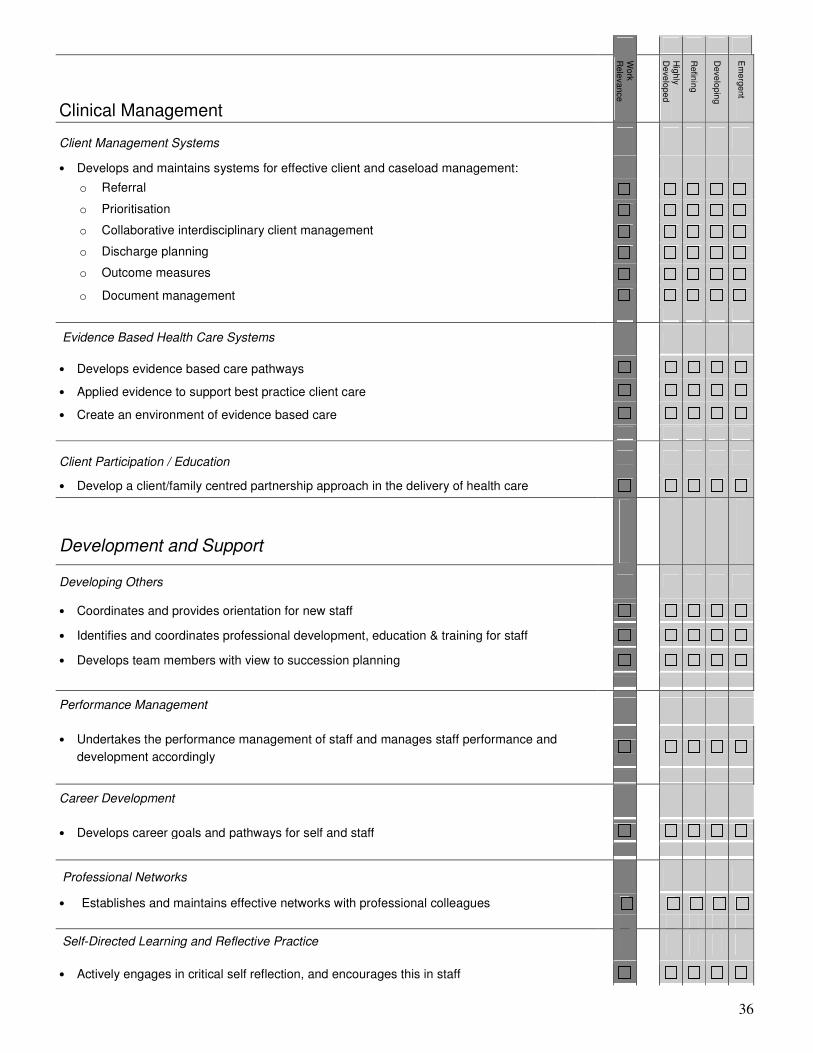
Consider level of proficiency and skill in the specific competencies relevant to the current
work role. Think about work practices and assess competence via the scale outlined
below. Select the descriptor that most reflects ability in this competency.
Hig
hly Developed
Refining
Develo
ping
Em
ergent
EMERGENT A skill or practice that you are do not currently perform, but that you feel
should be included in your role
DEVELOPING A skill or practice in which you occasional undertake, but see room for
further development
REFINING A skill or practice in which you are confident and competent
HIGHLY DEVELOPED A skill or practice in which you are very confident and feel you excel in

31
����������� ���������������
��������������������������
��
����
��
��
�������
������������� ������������� �������������
��������������������������
�������
����������������������������������������������������������������������������������������� �����
�������������������� ��������������������������������������
• � �������
• �����������
• ���������
• ��������������
�������
����������������� �������������������������� ������������� ���������������������������������������
����� �
��������������� ������������������������!����"�
� ��� ��������������������������������������� ������������
�����!�
����������������� �������������������������� ������������"����� �����

32
Discipline Specific Competencies
• Demonstrates professional (discipline specific) competency in the provision of health care services.
This tool focuses on competencies shared across allied health professionals. Discipline specific competencies are an essential part of rural and remote practice, and should form an integral part of any competency and learning framework. Please refer to discipline specific competencies provided by the relevant professional associations.
Service Delivery
Work
Relevance
Highly
Developed
Refining
Developing
Em
ergent
Service Planning • Plans services considering
o Population and community need
o Evidence and best practice
o Organisational direction/priorities
o Sustainability
o Service prioritisation
o Resources available
• Understands the interrelationships among access, quality, cost, resource allocation, sustainability, accountability, and community in service planning
Service Delivery
• Understands the system of healthcare delivery locally, regionally and state wide
• Develops and implements health programs and services consistent with service planning
• Oversees the delivery of local, outreach and region wide services
• Demonstrates service initiation and encourages innovation in service delivery
• Employs and supports a range of service delivery methodologies
Philosophies of Practice • Applies contemporary principles of practice to service planning and delivery, including:
o Primary health care
o Client/family centred practice
o Best practice and evidence-based practice
o Community development
Service Evaluation & Research
• Evaluates allied health activities/programs and service delivery methodologies
• Works collaboratively to set and achieve performance measurements for service delivery.
• Understands and applies the fundamental concepts and methods of research to review and improve services

33
Service Delivery (cont)
Work
Relevance
Highly
Developed
Refining
Developing
Em
ergent
Service Partnerships & Integration
• Develops and facilitates collaborative relationships with:
o Service stakeholders (eg other AH services, private providers, Metropolitan AHPs, Disability Service Commission, Aboriginal Medical Services, Divisions of General Practice)
o Community stakeholders (community groups, clients)
o Educational stakeholders (including those coordinating student placements and support, post graduate studies, research, etc.)
• Works within these partnerships to source funding, plan, deliver and evaluate services
Quality and Safety
Operational and Strategic Planning
• Understands and translates the organisational vision, structure, and strategic intent into operational practice
• Contributes to, and integrates AH programs into, organisational planning (strategic, operational, service planning)
Policy and Procedure
• Understands, complies with and contributes to the development of organisational policy and procedure
• Develops and monitors clinical and operational AH guidelines as they relate to work area
Safe Practice & Risk Management
• Understands and manages the safety and quality of clinical practice (including application of the Australian Incident Monitoring System (AIMS) protocol)
• Understands and manages non-clinical risk (staff, visitors and environment)
• Promote a positive Occupational Health & Safety culture within the team.
Quality Improvement
• Leads the development, implementation and evaluation of quality and safety plans, systems and activities, relevant to the work area.
• Contributes to quality and safety activities in other relevant work areas.
• Works to develop a quality improvement culture within the AH team
• Demonstrates a sound understanding of EQuIP, and is responsible for ensuring the department meets EQuIP standards

34
Professional Skills
Work
Relevance
Highly
Developed
Refining
Developing
Em
ergent
Management
• Effectively manages others, including:
o Communicates effectively
o Provides feedback
o Negotiates and resolves conflict
o Promotes teamwork
o Mentors & coaches others
o Promotes professional autonomy and responsibility
• Maintains communication with relevant managers and health leaders.
Project Management
• Plan and manage projects, incorporate scope definition, scheduling, budget, quality processes, project team management, communication and risk assessment.
Leadership & Change Management
• Utilises change management principles to lead and manage change
• Demonstrates leadership, including:
o Develops a shared vision and mission for the work area
o Thinks and acts strategically (organisational awareness)
o Promotes team work and coalition building
o Empowers people to act
o Influences others through advocacy and effective communication, and
o Develops others (mentoring, coaching, building competence)
Financial and Resource Management
• Demonstrates a sound understanding of financial procedures and controls
• Effectively manages financial and departmental resources (planning, prioritisation, allocation and budgeting)
Human Resource Systems
• Has sound knowledge of relevant industry awards and agreements including Health Service Union (HSU) award
• Has sound knowledge of formal Human Resources processes (HR), including selection and recruitment process, workforce planning, succession planning, grievance processes
• Where appropriate authorise various types of leave (including annual leave, TOIL, Professional Development and Study Days) for staff
• Demonstrates an ability to coordinate staff rosters and timetabling
• Has a sound working knowledge of Health Corporate Network (HCN)

35
Professional Skills (cont)
Work
Relevance
Highly
Developed
Refining
Developing
Em
ergent
Information Management
• Employs, and supports the use of, relevant information management strategies to guide service delivery, including:
o Promotes the collection and collation of statistical data
o Undertakes analysis and reporting of statistical data.
o Develops improved client record systems
o Has a sound understanding of available resources (eg. Clinical Information Access Online (CIAO))
Equity, Access and Diversity
Consumer Involvement
• Engages, consults and advocates for consumers and the community in health service planning, development and evaluation
• Actively promotes available services within the community
Consent, Confidentiality
• Supports staff to apply principles of informed consent, and to ensure confidentiality in service provision.
• Demonstrates effective communication and negotiation skills to manage conflict and complaints
Cultural Security
• Develop and provide culturally secure services to meet the needs of people from culturally and linguistically diverse (CALD) backgrounds
• Provides culturally secure health services to Indigenous people:
o Applies principles of the WA Cultural Respect Framework and works within the organization to ensure culturally secure services to Indigenous people and cultural respect is maintained
o Coordinates opportunities for staff orientation and ongoing education in cultural awareness/safety/security
o Develops and maintains partnerships with key local Indigenous organisations and individuals for service planning, delivery, and review
o Undertakes periodical reviews of the cultural appropriateness of services •
o Personally, and facilitates staff, to undertake self-assessment of health service delivery to Aboriginal people
o Ensures AH staff and departments work effectively with Indigenous staff
Rural Context
• Understands the rural context in the planning and delivery of health services.
36
Clinical Management
Work
Relevance
Highly
Developed
Refining
Developing
Em
ergent
Client Management Systems • Develops and maintains systems for effective client and caseload management:
o Referral
o Prioritisation
o Collaborative interdisciplinary client management
o Discharge planning
o Outcome measures
o Document management
Evidence Based Health Care Systems
• Develops evidence based care pathways
• Applied evidence to support best practice client care
• Create an environment of evidence based care
Client Participation / Education
• Develop a client/family centred partnership approach in the delivery of health care
Development and Support
Developing Others
• Coordinates and provides orientation for new staff
• Identifies and coordinates professional development, education & training for staff
• Develops team members with view to succession planning
Performance Management
• Undertakes the performance management of staff and manages staff performance and development accordingly
Career Development
• Develops career goals and pathways for self and staff
Professional Networks
• Establishes and maintains effective networks with professional colleagues •
Self-Directed Learning and Reflective Practice
• Actively engages in critical self reflection, and encourages this in staff

37
• Demonstrates the capacity to give and receive feedback effectively
• Support self-directed learning for staff and self.
Clinical Skills
• Demonstrates, and continues to develop, advanced professional competency
Professional & Ethical Practice
Legal and Ethical Practice
• Has a sound knowledge of relevant legal and legislative requirements as they relate to the work area (including Freedom of Information Act, Occupational Health and Safety, Equal Opportunities Act)
• Provides ethical leadership and demonstrates an adherence to ethical guidelines for the relevant discipline and the organisation
Professional Standards and Competencies
• Ensures staff competence and professional credentials
Supervision and Delegation
• Demonstrates supervisory skills, including:
o Supervision of staff
o Peer supervision
o Develops supervision and delegation skills in others
Self Care
• Works to ensure the well-being of self and others
Additional Competencies
Work
Relevance
Highly
Developed
Refining
Developing
Em
ergent
38
Summary of Priority Competencies
Work
Relevance
Highly
Developed
Refining
Developing
Em
ergent
39
Notes