
I CAN Prevent Diabetes! Individuals and Communities Acting Now to Prevent Diabetes

Prevent Emphysema
Now!Information for Physicians on the
Diagnosis and Treatment of COPD
Thomas L. Petty, M.D.Dennis E. Doherty, M.D.
National Lung Health Education Programwww.NLHEP.org

TESTYOUR LUNGS-KNOWYOUR NUMBERS
FEV1
FEV6
What is your FEV1?
What is your FEV6?
(FVC)
Forced Vital Capacity in
six seconds
NationalLungHealth Education Program(NLHEP)

One of the greatest challenges facing primary care physicians as well as medical specialists today isthe growing problem of chronic obstructive pulmonary disease (COPD).
The National Lung Health Education Program (NLHEP) healthcare initiative is designed to identifyand to treat patients in the early stages of emphysema and related chronic bronchitis. Together,emphysema and chronic bronchitis are known as chronic obstructive pulmonary disease (COPD).Approximately 120,000 Americans die of COPD each year! In 2000, more women than men diedof COPD. COPD is now the fourth most common cause of death in the U.S.A. It is the onlydisease among the top five killers in America that continues to rise in the number of annual sickdays and deaths.
By contrast, great progress has been made in reducing the number of people who become sickor who die from major diseases, such as heart attack, stroke, and many cancers, largely becauseof early identification and treatment programs.
The NLHEP initiative is directed to both primary care physicians and to patients. Manymedical societies and governmental agencies within the United States sponsor the NLHEP.Financial support for the NLHEP comes from unrestricted grants from the pharmaceutical andmedical equipment industries. The NLHEP enjoys a partnership with the AmericanAssociation for Respiratory Care (AARC), a professional organization representing 130,000respiratory care professionals.
Together, the NLHEP and the AARC are attacking COPD, a common disease tat results insuffering and early death. Please learn how you can help prevent emphysema! We aim toreduce the social and the economic impact of this important problem. We believe thatthrough education to the public by professional and governmental agencies, the problem ofCOPD can finally be prevented and solved. Please visit our web sites (nlhep.org, aarc.org,and nepp.org) for current information.
Thomas L. Petty, M.D.Dennis E. Doherty, M.D.Co-Chairs, National Lung Health Education Program (NLHEP)
Introduction
1

Undiagnosed COPD
A recent large population-based study, thethird National Health and NutritionExamination Survey (NHANES III), foundthat a large proportion of patients withCOPD have not been diagnosed. This istrue despite these patients manifestingsymptoms of cough, excess mucus, dyspneaon exertion, or wheeze — the cardinal signsand symptoms of COPD. Even patients withmoderate to advanced stages of diseasemay not be diagnosed, and accordingly, donot receive treatment. Today we have apowerful armamentarium to use for patientsfound to have early-stage COPD. Thesetherapies can prevent progression intoadvanced stages of the disease. Thecatastrophe of developing emphysema withits life threatening implications, the need foroxygen and possibly surgery, and itstremendous impact on healthcare costs,make early diagnosis and interventionimperative.
We now recognize that spirometry is asimple expression of a complex process. Like blood pressure, spirometry has manydeterminates, as summarized in Table 1.
Who Should be Tested?
A consensus report of the National LungHealth Education Program (NLHEP)Spirometry Committee recommends simple spirometric testing for all smokersage 45 years or older. Testing should alsobe done in anyone with chronic cough,excess mucus, dyspnea on exertion, orwheeze. These are the major symptoms ofCOPD, which includes a spectrum ofdiseases: asthmatic bronchitis, chronicbronchitis, and emphysema. It is theemphysema component of this spectrumthat leads to the greatest impairment anddisability. In addition, anyone with a familyhistory of emphysema or chronic bronchitisshould have a spirometric test as a part oftheir initial evaluation. Knowing simple lungfunction values provides a baseline by whichsubsequent changes can be evaluated.
2
Making the Diagnosis of COPD
Table 1
BLOOD PRESSURE (Sphygmomanometry) LUNG FUNCTION (Spirometry)
120/80 3.0 FEV1/4.0 FVCCardiac output Elastic recoilPeripheral vascular resistance Small airways resistanceBlood volume Large airways resistanceBlood viscosity InterdependenceRenin-angiotensin axis Muscular effort and coordination

Spirometry measures airflow over time. It ismost commonly expressed as two numbersthat represent volume expired from thelungs. The forced vital capacity (FVC), is theamount of air that can be blown out of fullyinflated lungs. This is the volume test. Theforced expiratory volume in one second(FEV1) is the amount of air blown out in thefirst second of the forced vital capacity. The FEV1 is the flow test. The ratio betweenthe two (FEV1/FVC), should be more than70%. lf the FEV1/FVC ratio is less than70%, this is a strong indicator of earlyairflow obstruction. It is a harbinger offurther rapid decline often leading todisabling emphysema.
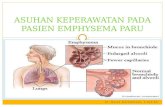
The determinants of expiratory airflow areillustrated in Figure 1. Expiratory airflow is afunction of pressure against resistance. Thepressure is generated by elastic recoil and
How to Test?
Factors Associated with Expiratory Airflow
Flow or Pressure ResistanceIn Respiratory Function
Loss of Elastic Recoil(pressure)
as in Emphysema
Airway Narrowingas in Asthma or
Chronic Bronchitis.Dynamic
Airway Collapsein Emphysema
Figure 1 Figure 2
Simple hand-held spirometers areinexpensive, accurate, and easy to use.
the resistance of the conducting airways.Spirometry is an effort-dependent test. lttakes effort by the patient to fill the lungscompletely and a complete uninterruptedeffort to empty the lungs. Normal lungsempty in about six seconds.
It is now known that the forced expiratoryvolume in six seconds (FEV6), is an excellentsurrogate for FVC. Thus, doing a six-secondexpiratory maneuver is more pleasant forthe patient and more convenient for thetester. Newer spirometers are now availablethat use the two parameters: FEV1 andFEV6. Predicted values for FEV6 have beenvalidated and published (see Hankinson andSwanney).
These new office spirometers are small and thus portable. They are inexpensive,easy to use, and accurate. Such aspirometer is illustrated in Figure 2.
3
Airflow Limitationis Determined by:

Of course, all smokers should stop smoking,but patients who are developing airflowobstruction have an absolutely critical need to really stop smoking. Methods ofsmoking cessation and other therapies usefulin early stages of COPD can change thecourse of the disease.
In the Lung Health Study, for example,patients with airflow obstruction who stoppedsmoking actually had an improvement inFEV1 followed by only a slight decline over afive-year follow-up period. By contrast, thosepatients who continued to smoke had a muchmore rapid deterioration (see Figure 3).However, in the Lung Health Study, nopatient died of COPD within the first five yearsof follow-up. The most common cause of deathwas lung cancer, followed by heart attack,and stroke (see Table 2). Thus, findingspirometric abnormalities in heavy smokers isa strong signal to look for other diseases, suchas lung cancer and to institute therapies, suchas the control of blood pressure and abnormallipid,s to reduce the risk of heart attack andstroke.
4
Who Should be Treated?
Effect of smoking cessation on FEV1 overtime, as seen in the Lung Health Study.Mean postbronchodilator forced expirato-ry volume at 1 second (FEV1) for partici-pants in the smoking intervention andplacebo group who are sustained quitters(o), and those who continued to smoke(•). The two curves diverge sharply afterbaseline.
Figure 3
Follow-up, year
Screen 2 2 3 4 512.4
2.5
2.6
2.7
2.8
2.9
Post
bron
chod
ilato
r FE
V
L1
Table 2
Causes of Death Within Five Years in the Lung Health Study.Smoking SmokingIntervention Intervention Usual
Cause of Death & Ipratropium & Placebo Care Total
Lung cancer 18 20 19 57Cardiovascular disease 18 7 12 37Other 18 17 20 55Total 54 44 51 149
Adapted from: Anthonisen NR, Connett JE, Kiley JP, Altose MD, Bailey WC, Buist AS, et al: Effects of smoking intervention and the use of an inhaled anti-cholinergic bronchodilator on the rate of decline of FEV1. The Lung Health Study. JAMA 1994;272:1501. Total enrolled: 5,887 persons.

Smoking cessation has been proven toimprove lung function and to increase lifespan. It has also been shown to lessen therisk of heart attack and stroke, and, afteryears of no smoking, the risk of lung cancerdeclines. A practical method in smokingcessation is briefly presented below (Table3) and discussed further on the next page.
5
The most important stop-smokingintervention is serious counseling about theimportance of stopping smoking and thedevelopment of a cessation plan. Picking aquit date is key. Nicotine replacement shouldbe started on the quit date. Nicotinereplacement products available over-the-counter or by prescription are listed in Table 3.
Suggested Treatment
Table 3
Drugs Used for Smoking Cessation. (Food and Drug Administration [FDA], Approved):
Drug and Method of Administration Unit Dose Dose IntervalNicotine polacrilex (oral) 2 - 4 mg Every 1 - 2 hours** Fifteen to 30 pieces may be chewed over 24 hours.
Transdermal nicotine patch 21, 14, and 7 mg Over 24 hours15, 10, and 5 mg Over 16 hours22 and 11 mg Over 24 hours
Nasal nicotine spray 0.5 mg/inhalation/nostril 8 - 40 mg/day in hourly or p.r.n. dosing
Nicotine inhaler 10 mg/inhaler Inhale for 20 minutes6 - 16 times/day
Nicotine lozenge 2 mg Every 1-2 hours
Bupropion sustained-release 150 mg 150 mg for 3 days, tablets (Zyban®) then 300 mg/day
(Start 2 wks before quit date)
Also Useful:
Clonidine transdermal patch 0.2 mgOne patch changed
weekly for 3 to 10 weeks
Nortriptyline tablets 25, 50, and 75 mg Maximum dose of 75 to 100 mg per day, treated for 8 to 12 weeks

The non-nicotine product, bupropion, is atleast as effective as nicotine replacement insmoking cessation. When nicotinereplacement and bupropion are usedtogether, up to a 35.5% biologically provenquit rate can be achieved at one year,compared to a 15.6% success rate with nopharmacologic interventions. Whenmedication is successful, cessation usuallyoccurs within two weeks. Re-treatment isappropriate up to seven or eight times for
those who fail. Start bupropion two weeksbefore quit date to help insure success inquitting.
The retardation of decline in FEV1 over 30years has been demonstrated (see Figure 4).Even patients who stopped smoking at age65 had a survival benefit. Thus, it is nevertoo Iate to stop smoking, but it is far betterto stop at a young age and beforeadvanced emphysema develops.
6
Never smoked or notsusceptible to smoke
Stopped atage 45 y
Smokedregularly andsusceptible to its effects
100
75
50
25
025 50 75Age
Disability
FEV
1, % o
f va
lue
at a
ge 2
5
Death
Stopped atage 65 y
Figure 4
1
Suggested Treatment (cont.)
The effect of smoking cessation on decrement in FEV1 (dotted oblique lines), compared withpatients who have never smoked or who are not susceptible to cigarette smoke (upper solidlines), and also compared with patients who stopped smoking late and are deteriorating fromthe harmful effects of cigarette smoke. The percent FEV1 when the disability most commonlyoccurs (approximately 30%), and where death occurs (approximately 10%), are indicated onthe dotted horizontal lines. The percent of predicted FEV1 at age 25 is on the vertical axis andage on the horizontal axis.
From: Peto R, Speizer FE, Cochrane AL, Moore F, Fletcher CM, Tinker CM, et al: The relevance in adults of air-flow obstruc-tion, but not of mucus hypersecretion, to mortality from chronic lung disease. Results from 20 years of prospective observa-tion. Am Rev Respir Dis 1983;128:492.

Influenza virus vaccine should be given everyFall to anyone with airflow obstruction. Thisis particularly important for people over theage of 50. Pneumococcal vaccine should begiven at least once in a lifetime and probablyrepeated every six years. Today, two newproducts, oseltamivir (Tamiflu™), andzanamivir (Relenza®), can modify the clinicalcourse of both influenza A and B.Amantadine and Ranitidine are effective onlyin A strains of influenza.
Inhaled bronchodilators reduce symptomsand improve lung function in the majority ofpatients with early-stage disease. Ipratropiumis the first step in therapy. Beta agonists suchas albuterol are also of significant value.Ipratropium and albuterol are available in thesame metered-dose inhaler (Combivent®).Salmeterol (Serevent) and formoterol(Foradil) are long-acting bronchodilators and,when used twice daily, are useful alternatives.Other novel bronchodilators are soon to bereleased; including tiotropium (Spivera®) a24-hour anti-cholinergic to be released in theU.S.A. in the near future. Salmeterol(Serevent®) and formoterol (Foradil) are bothcompatible with the use of ipratropium.Together, both medications may improvelung function and mitigate symptoms. Allpatients must learn the proper technique forusing metered-dose inhalers and newerinhalation devices coming to the market, foruse in the delivery of anticholinergics, betaagonists, combinations, and corticosteriods.
Inhaled corticosteriods have not beenshown to alter the rate of decline in FEV1 inat least five randomized, controlled, clinicaltrials. However, inhaled budesonide,fluticasone, and triamcinolone have all beenshown to improve symptoms and to reducethe consumption of healthcare resources inpatients with severe COPD. A reduction ofbone density was found during the conductof one of these trials. Thus, anysymptomatic benefits should be weightedagainst potential systemic side effects in thelong-term.
The empiric use of antibiotics is wellestablished in the management of acuteexacerbations of chronic bronchitis. Bacterialinvasion is often present following a cold,when there is increased cough, increasedsputum volume, and the appearance ofsputum purulence (i.e., yellow or green).These common invaders, the aerobes, areH. influenzae, S. pneumonia, C.pneumoniae, and M. pneumoniae. Theseagents are effectively treated withmacrolides, fluoroquinolones, secondgeneration cephalosporins, trimethoprimsulfa, or doxycycline when given empiricallyfor five to seven days. A sputum culture isnot necessary.
Oral corticosteriods, (i.e., 40 mg prednisoneper day, or equivalent) given for a shortperiod of time, (i.e., approximately 7-14days), can attenuate the degree of acuteairflow obstruction during exacerbationsand can often abort the progression to asevere exacerbation of COPD, thus
7
Other Therapy

diminishing the need for hospitalization (seeTable 4 above).
Future Directions
It is now known that the inflammatorymediators involved in the pathogenesis ofCOPD, which lead to airway inflammationand destruction of alveolar walls, aredifferent from those involved in asthma. Anumber of new pharmacologic entities arebeing produced to deal with early-stage
disease. Longer-acting anticholinergic drugs,mucoregulators, and immunomodulators areon the horizon and are soon to be released.But, even today, great progress is beingmade in slowing the course of disease inpatients with early stages of COPD andrelated disorders through early identificationand intervention. This is why the earlyidentification of airflow obstruction by theroutine use of simple office spirometry is ofparamount importance. lt is in this arenathat the primary healthcare practitioner willplay a leading role.
8
Other Therapy (cont.)
Table 4Therapy for COPD
Maintenace Management
• Stop Smoking Quit date, nicotine replacement, bupropion
• Inhaled Bronchodilators AnticholinergicsBeta AgonistsCombinations
• Inhaled Corticosteroids(in advanced COPD)
Exacerbations
• Antibiotics Broad spectrum• Corticosteroids Systemic prednisone• Inhaled Bronchodilators (See list above)

Lung Health Study Research Group: Effect ofinhaled triamcinolone on the decline in pulmonary function in chronic obstructive pulmonary disease. New Engl J Med2000;343:1902-1909.
Mannino DM, Gagnon RC, Petty TL, Lydick E:Obstructive lung disease and low lung function inadults in the United States. Arch Intern Med2000;160:1683-1689.
Niewoehner DE, Erbland ML, Deupree RH,Collins D, Gross NJ, Light RW, et al: Effect of sys-temic glucocorticoids on exacerbations of chronicobstructive pulmonary disease. Department ofVeterans Affairs Cooperative Study Group. N EnglJ Med 1999;340:1941-1947.
Peto R, Speizer FE, Cochrane AL, Moore F,Fletcher CM, Tinker CM, et al: The relevance inadults of air-flow obstruction, but not of mucushypersecretion, to mortality from chronic lungdisease. Results from 20 years of prospectiveobservation. Am Rev Respir Dis 1983;128:491-500.
Soriano JB, Vestbo J, Pride NB, et al: Sirvival inCOPD patients after regular use of fluticasonepropionate and salmuterol in general practice.Evidence of improved survival in COPD patientswith the regular use of both agents. Eur Respir J2002; 20:819-825.
Swanney MP, Jensen RL, Crichton DA, BeckertLE, Cardno LA, Crapo RO: FEV6 is an acceptablesurrogate for FVC in the spirometric diagnosis of airway obstruction and restriction. Am J RespirCrit Care Med 2000;162:917-919.
Vinken W, et al: Improved health outcomes inpatients with COPD during one year’s treatmentwith tiotropium. Eur Respir J 2002;19:209-216.
Anthonisen NR, Connett JE, Kiley JP, AltoseMD, Bailey WC, Buist AS, et al: Effects ofsmoking intervention and the use of an inhaledanticholinergic bronchodilator on the rate ofdecline of FEV1. The Lung Health Study. JAMA1994;272:1497-1505.
Burge PS, Calverley PM, Jones PW, Spencer S,Anderson JA, Maslen TK: Randomised, doubleblind, placebo controlled study of fluticasonepropionate in patients with moderate to severechronic obstructive pulmonary disease: TheISOLDE Trial. BMJ 2000;320:1297-1303.
Dale LC, Ebbert JO, Hays JT, Hurt RD:Treatment of nicotine dependence. Mayo ClinicProc 2000;75:1311-1316.
Ferguson GT, Enright PL, Buist AS, HigginsMW: Office spirometry for lung health assess-ment in adults. A consensus statement from theNational Lung Health Education Program. Chest2000;117:1146-1161.
Guyatt GH, Townsend M, Nogradi S, et al:Acute response to bronchodilator — an imper-fect guide for bronchodilator therapy. ArchIntern Med 1988;148:1949-1952.
Hankinson JL, Odencrantz JR, Fedan KB:Spirometric reference values from a sample ofthe general U.S. population. Am J Respir CritCare Med 1999;159:179-187.
Hurt RD, Sachs DP, Glover ED, Offord KP,Johnston JA, Dale LC, et al: A comparison ofsustained-released bupropion and placebo forsmoking cessation. N Engl J Med1997;337:1195-1202.
Jorenby DE, Lieschow SJ, Nides MA, RennardSI, Johnston JA, Hughes AR, et al: A controlledtrial of sustained-release bupropion, a nicotinepatch, or both for smoking cessation. N Engl J Med 1999;340:685-691.
9
References

WEBSITES
American Association for Respiratory Care (AARC)www.aarc.org
National Emphysema Prevention Program (NEPP)www.nepp.org
National Lung Health Education Program (NLHEP)www.nlhep.org
US COPD Coalition www.uscopd.com
MEDICAL ARTICLES
• Petty TL, Weinmann GG: Building a nationalstrategy for the prevention and managmentof and research in chronic obstructivepulmonary disease. JAMA 1997;277:246-253.
• Petty TL (ed): Strategies in preserving lunghealth and preventing COPD and associateddiseases. The National Lung Health EducationProgram (NLHEP). Chest 1998;113:123S-163S.
• Petty TL (ed): Strategies in preserving lunghealth and preventing COPD and associateddiseases. The National Lung Health EducationProgram (NLHEP). Respir Care 1998;43:183-216.
• Ferguson GT, Enright PL, Buist AS, HigginsMW: Office spirometry for lung healthassessment in adults. A consensus statementfrom the National Lung Health EducationProgram. Chest 2000;117:1146-1161.
• Mannino DM, Gagnon RC, Petty TL, Lydick E:Obstructive lung disease and low lungfunction in adults in the United States. ArchIntern Med 2000;160:1683-1689.
10
Selected Resources
MEDICAL BOOKS
Simple Spirometry for Frontline Practitioners SnowdriftPulmonaryConference.orgSnowdrift Pulmonary Conference, Inc.899 Logan Street, Suite 203Denver, CO 80203(303) 996-0868
Frontline Treatment of COPD, 2nd ed.Book, CD, or audioSnowdrift Pulmonary Conference, Inc.or free from Boehringer Ingelheim Pharmaceuticals, lnc.900 Ridgebury RoadP.O. Box 368Ridgefield, CT 06877-0368(203) 798-5264
Frontline Advice for COPD PatientsSnowdrift Pulmonary Conference, Inc. or free from Boehringer Ingelheim Pharmaceuticals, Inc. 900 Ridgebury RoadP.O.Box 368Ridgefield, CT 06877-0368(203) 798-5264
Frontline Update on COPD(in press - 2003)Snowdrift Pulmonary Conference, Inc. or free from Boehringer Ingelheim Pharmaceuticals, Inc. 900 Ridgebury RoadP.O.Box 368Ridgefield, CT 06877-0368(203) 798-5264

Appendix A
Pulmonary Function Reimbursement (as of 6/03)
Indication ICD 9 CM Code
Shortness of Breath 786.09
Cough 786.2
Chronic Bronchitis 491.
Emphysema 492.
Asthma 493.
COPD 496.
Pre-operative Respiratory Exam V72.82
History of Tobacco Use V15.82
Description CPT Code Average Reimbursement
Spirometry 94010 $30
Bronchospasm Evaluations 94060 $57
Maximum Voluntary Ventilation 94200 $18
Respiratory Flow Volume Loop 94375 $37
11

NOTES

National Lung Health Education Program (NLHEP)899 Logan St, Suite 203
Denver, CO 80203Fax: 303-996-0870
E-mail: [email protected] Site: nlhep.org
Printing and distribution have been made possible by educational grants from:
Medical Technologies, Inc.
Revised 6/03















![Acute or chronic pulmonary emphysema? Or both?—A ......emphysema or acute alveolar dilation, respectively [3 , 5]. In some cases, an interstitial emphysema is described [, 636].](https://static.fdocuments.net/doc/165x107/6138f505a4cdb41a985b64ce/acute-or-chronic-pulmonary-emphysema-or-bothaa-emphysema-or-acute-alveolar.jpg)