Pneumothorax
6
Pneumothorax Definition A lung can collapse for many reasons: a growing tumor blocking a major airway, an infection, even an inhaled foreign object. One type of lung collapse, known medically as a pneumothorax, occurs when air leaks into the area between your lungs and chest wall (pleural space). The pressure of the air against the lung causes it to give way, often leading to mild to severe chest pain and shortness of breath. A pneumothorax can be caused by a chest injury, certain medical treatments, lung disease or a break in an air blister on the lung's surface. A lung collapses in proportion to the amount of air that leaks into your chest cavity. Although the entire lung can collapse, a partial collapse is much more common. A small, uncomplicated pneumothorax may heal on its own in a week or two, but when the pneumothorax is more severe, the excess air is usually removed by inserting a tube or needle between your ribs into the pleural space. If air continues to build up, the increasing pressure can push your heart and blood vessels toward the uncollapsed lung, compressing both your lung and heart. Called a tension pneumothorax, this condition is life-threatening and requires immediate medical care. Symptoms If only a small amount of air enters the pleural space, you may have few signs or symptoms, though even a minimally collapsed lung is likely to cause some chest pain. When your lung has collapsed 25 percent or more, you're likely to experience: Sudden, sharp chest pain on the same side as the affected lung Shortness of breath, which may be more or less severe, depending on how much of the lung is collapsed A feeling of tightness in your chest A rapid heart rate Because a tension pneumothorax can compress the walls of your heart as well as the unaffected lung, heart function may be impaired, leading to a potentially fatal drop in blood pressure.
-
Upload
nader-smadi -
Category
Documents
-
view
9 -
download
4
Transcript of Pneumothorax

Pneumothorax
Definition A lung can collapse for many reasons: a growing tumor blocking a major airway, an infection, even an inhaled foreign object. One type of lung collapse, known medically as a pneumothorax, occurs when air leaks into the area between your lungs and chest wall (pleural space). The pressure of the air against the lung causes it to give way, often leading to mild to severe chest pain and shortness of breath. A pneumothorax can be caused by a chest injury, certain medical treatments, lung disease or a break in an air blister on the lung's surface.
A lung collapses in proportion to the amount of air that leaks into your chest cavity. Although the entire lung can collapse, a partial collapse is much more common. A small, uncomplicated pneumothorax may heal on its own in a week or two, but when the pneumothorax is more severe, the excess air is usually removed by inserting a tube or needle between your ribs into the pleural space.
If air continues to build up, the increasing pressure can push your heart and blood vessels toward the uncollapsed lung, compressing both your lung and heart. Called a tension pneumothorax, this condition is life-threatening and requires immediate medical care.
Symptoms If only a small amount of air enters the pleural space, you may have few signs or symptoms, though even a minimally collapsed lung is likely to cause some chest pain. When your lung has collapsed 25 percent or more, you're likely to experience:
Sudden, sharp chest pain on the same side as the affected lung Shortness of breath, which may be more or less severe, depending on how
much of the lung is collapsed A feeling of tightness in your chest A rapid heart rate
Because a tension pneumothorax can compress the walls of your heart as well as the unaffected lung, heart function may be impaired, leading to a potentially fatal drop in blood pressure.

Causes
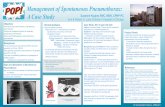
Collapsed and normal lung
Your two lungs are separated by your heart, airways and the major blood vessels in the center of your chest (mediastinum). All these structures are enclosed by your chest wall, a combination of ribs, cartilage and muscle.
Each lung is covered by a thin, moist tissue called the pleura, which also lines the chest wall. The two layers of pleura are like pieces of smooth satin that allow your lungs to expand and contract easily.
Your lungs and chest wall are both elastic, but as you inhale and exhale, your lungs recoil inward while your chest wall expands outward. The two opposing forces create a negative pressure in the pleural space between your rib cage and lung. When air enters that space, either from inside or outside your lungs, the pressure it exerts can cause all or part of the affected lung to collapse.
There are several types of pneumothorax, which are defined according to what causes them:
Primary spontaneous pneumothorax. This usually occurs in otherwise healthy people with no history of chest trauma. It's most common in tall, thin men — many of them smokers — between 20 and 40 years of age. Primary spontaneous pneumothorax is thought to develop when a small air blister (bleb) on the lung ruptures. Blebs are caused by a weakness in the lung tissue and can rupture from changes in air pressure when you're scuba diving, flying, mountain climbing or, according to some reports, listening to extremely loud music.
Primary spontaneous pneumothorax can run in families, and researchers think that genetic factors also may play a role. A primary spontaneous

pneumothorax is usually mild because pressure from the collapsed portion of the lung in turn collapses the bleb.
Secondary spontaneous pneumothorax. This develops in people who already have a lung disorder, especially emphysema, which progressively damages your lungs. Other conditions that can lead to secondary pneumothorax include tuberculosis, pneumonia, cystic fibrosis and lung cancer. In these cases, the pneumothorax occurs because the diseased lung tissue is next to the pleura.
Although the signs and symptoms of primary and secondary spontaneous pneumothorax are identical, secondary pneumothorax can be more severe and even life-threatening because diseased tissue opens a wider hole and therefore lets more air into the pleural space than does a small, ruptured bleb.
Traumatic pneumothorax. Any blunt or penetrating injury to your chest can cause lung collapse. Knife and gunshot wounds, a blow to the chest, even a deployed air bag can cause a pneumothorax. So can injuries that inadvertently occur during certain medical procedures such as the insertion of chest tubes, cardiopulmonary resuscitation (CPR) and lung or liver biopsies. Pneumothorax is especially common in people whose breathing is aided by a mechanical ventilator.
Tension pneumothorax. The most serious type of pneumothorax, this occurs when the pressure in the pleural space is greater than the atmospheric pressure, either because air becomes trapped in the pleural space or because the entering air is from a positive-pressure mechanical ventilator. The force of the air can cause the affected lung to collapse completely. It can also push the heart toward the uncollapsed lung, compressing both it and the heart. Tension pneumothorax comes on suddenly, progresses rapidly and is fatal if not treated quickly.
Risk factors Your sex. In general, men are far more likely to have a pneumothorax than
women are, though women can develop a rare form of pneumothorax (catamenial pneumothorax) related to the menstrual cycle. Catamenial pneumothorax, which mainly affects women in their 20s and 30s, seems to occur when endometrial tissue — the tissue that normally lines the uterus — spreads to the lungs, pleura or diaphragm.
Smoking. This is the leading risk factor for primary spontaneous pneumothorax; more than 90 percent of people with a primary pneumothorax are smokers or former smokers. The risk increases with the length of time and the number of cigarettes smoked.
Lung disease. Having another lung disease, especially emphysema, makes a collapsed lung more likely.
A history of pneumothorax. If you've had one pneumothorax, you're at increased risk of another, usually within one to two years of the first episode. This is especially true if the first pneumothorax was small and healed on its own.

When to seek medical advice See your doctor right away if you have chest pain and trouble breathing. Many conditions other than pneumothorax can cause these symptoms, but most require an accurate diagnosis and prompt treatment. If your chest pain is severe or breathing becomes increasingly difficult, get immediate emergency care.
Tests and diagnosis Most often, your doctor will diagnose a pneumothorax using a chest X-ray. Other tests are sometimes performed, including:
Computerized tomography (CT) scan. In certain cases, you may have a computerized tomography (CT) scan, an X-ray technique that produces more detailed images than conventional X-rays do. This is most often done if your doctor suspects a pneumothorax after an abdominal or chest procedure. A CT scan can help determine whether an underlying disease may have caused your lung to collapse — something that may not show up on a regular X-ray.
Blood tests. These may be used to measure the level of oxygen in your arterial blood.
Complications The most common complication of a spontaneous or traumatic pneumothorax is a recurrence — close to half the people who have had one pneumothorax have another, usually within a year or two of the first. You're more likely to have more than one pneumothorax if you smoke, have an existing lung disease or HIV/AIDS, or are tall and thin. And if you've had a primary spontaneous penumothorax from a ruptured bleb, it's highly possible that you have or will develop a similar bleb in the opposite lung.
Complications of a tension pneumothorax are more serious and include:
Low blood oxygen levels (hypoxemia). Because a tension pneumothorax causes near or total collapse of one lung and can compress the other, you take in less air and less oxygen enters your bloodstream. As a result, you develop lower than normal blood oxygen levels. Lack of oxygen can disrupt your body's basic functioning, and severely low levels can be life-threatening.
Respiratory failure. This occurs when blood levels of oxygen fall too low, and the level of carbon dioxide becomes too high. Severely low blood oxygen can lead to heart arrhythmias and unconsciousness, and high carbon dioxide levels to sleepiness and confusion. Eventually, respiratory failure may prove fatal.
Cardiac arrest. In a tension pneumothorax, the heart is pushed toward the unaffected lung. This can interfere with the return of blood to the heart and lead to a sudden loss of heart function. Cardiac arrest is fatal if not treated immediately.

Shock. This critical condition occurs when blood pressure drops so low that the body's vital organs are deprived of oxygen and nutrients. Shock is a major medical emergency and requires immediate care.
Treatments and drugs The goal in treating a pneumothorax is to relieve the pressure on the lung, allowing it to re-expand, and to prevent recurrences. The best method for achieving this depends on the severity of the lung collapse and sometimes on your overall health:
Observation. If your lung is less than 20 percent to 25 percent collapsed, your doctor may simply monitor your condition with a series of chest X-rays until the air is completely absorbed and your lung has re-expanded. Because it may take weeks for a pneumothorax to heal on its own, however, a needle or chest tube may be used to remove the air, even when the pneumothorax is small and nonthreatening.
Needle or chest tube insertion. When your lung has collapsed more than 25 percent, your doctor is likely to remove the air by inserting a needle or hollow tube (chest tube) into the pleural space. Chest tubes often are attached to a suction device that continuously removes air from the chest cavity and may be left in place for several hours to several days.
Other pneumothorax treatments. If you have had more than one pneumothorax, you may have treatments to prevent further recurrences. The most common is a surgical procedure called video-assisted thoracoscopy, which uses small incisions and a tiny video camera to guide the surgery. This technique leads to less pain and a shorter recovery time than other types of surgery do because the chest cavity can be accessed without breaking any ribs.
Nursing care• Open the airway by suctioning and
endotracheal intubation• Control hemorrhage• Provide care of chest tube• Do ECG daily• Check vital signs frequently

Prevention Although it's often not possible to prevent a pneumothorax, stopping smoking is the best way to reduce your risk of a first pneumothorax and avoid a recurrence.