Pneumonia: Community- and Hospital-acquired pneumonia · ATHENS 2019 GREECE | 27-29 JUNE Pneumonia:...
71
ATHENS 2019 GREECE | 27-29 JUNE Pneumonia: Community- and Hospital-acquired pneumonia Adamantia Liapikou, MD, PhD SOTIRIA Chest Diseases Hospital, Athens
Transcript of Pneumonia: Community- and Hospital-acquired pneumonia · ATHENS 2019 GREECE | 27-29 JUNE Pneumonia:...
ATHENS 2019GREECE | 27-29 JUNE
Pneumonia:Community-andHospital-acquired
pneumoniaAdamantiaLiapikou,MD,PhD
SOTIRIAChestDiseasesHospital,Athens
ATHENS 2019GREECE | 27-29 JUNE
Conflict of Interest Disclosure
NOTHINGTODECLARE
ATHENS 2019GREECE | 27-29 JUNE
Community-acquiredpneumonia
§ Epidemiology§ Etiology-Diagnosis§ Prognosis§ Therapy§ Prevention
Clinical Infectious Diseases 2007;44:S27–72
Clinical Microbiology and Infection,Vol17;Sup6,Nov2011
ATHENS 2019GREECE | 27-29 JUNEEPIDEMIOLOGY
ØCAPincidencerangesbetween1,7-11,6/1000cases/yearinadults
ØMorecommoninchildren<5yrsandadults>40yrsØMorecommoninpatientswithcomorbidities
ØPeakincidenceduringwintermonthsØMortalityoutsidethehospitalislow,butin-hospitalmortalityrangesbetween5–10%andreaches30–50%inICUpatients
ATHENS 2019GREECE | 27-29 JUNE
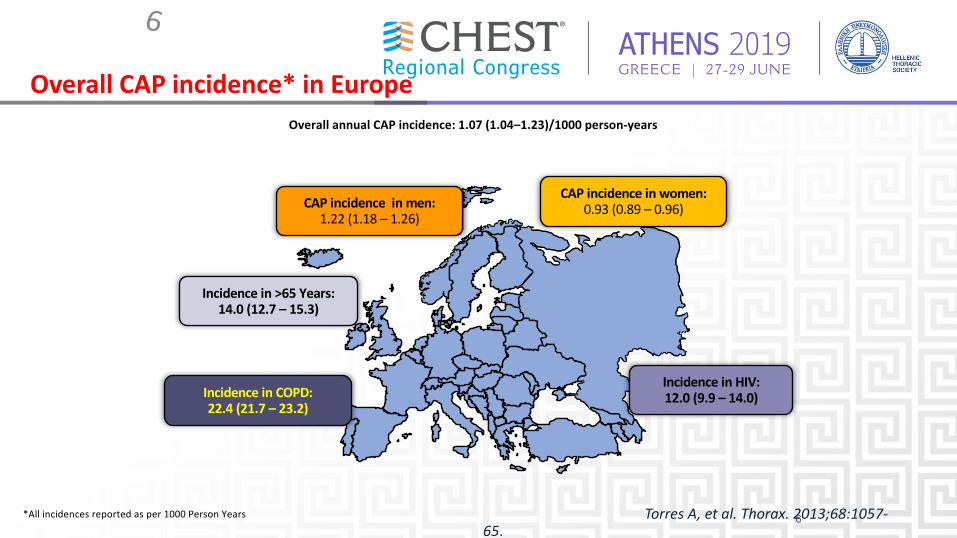
Overall CAP incidence* in Europe
6
Overall annual CAP incidence: 1.07 (1.04–1.23)/1000 person-years
CAP incidence in men: 1.22 (1.18 – 1.26)
Incidence in >65 Years:14.0 (12.7 – 15.3)
Incidence in COPD:22.4 (21.7 – 23.2)
Incidence in HIV:12.0 (9.9 – 14.0)
CAP incidence in women:0.93 (0.89 – 0.96)
6Torres A, et al. Thorax. 2013;68:1057-65.
*All incidences reported as per 1000 Person Years
ATHENS 2019GREECE | 27-29 JUNE
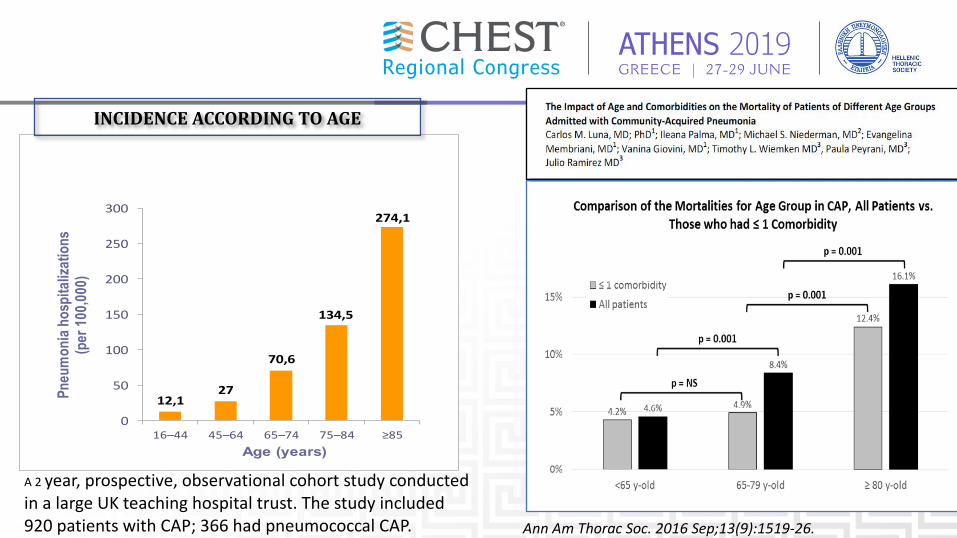
Ann Am Thorac Soc. 2016 Sep;13(9):1519-26.
12,127
70,6
134,5
274,1
0
50
100
150
200
250
300
16–44 45–64 65–74 75–84 ≥85
Pneu
mon
ia ho
spita
lizat
ions
(p
er 10
0,000
)
Age (years)
A 2 year, prospective, observational cohort study conducted in a large UK teaching hospital trust. The study included 920 patients with CAP; 366 had pneumococcal CAP.
INCIDENCEACCORDINGTOAGE
ATHENS 2019GREECE | 27-29 JUNE
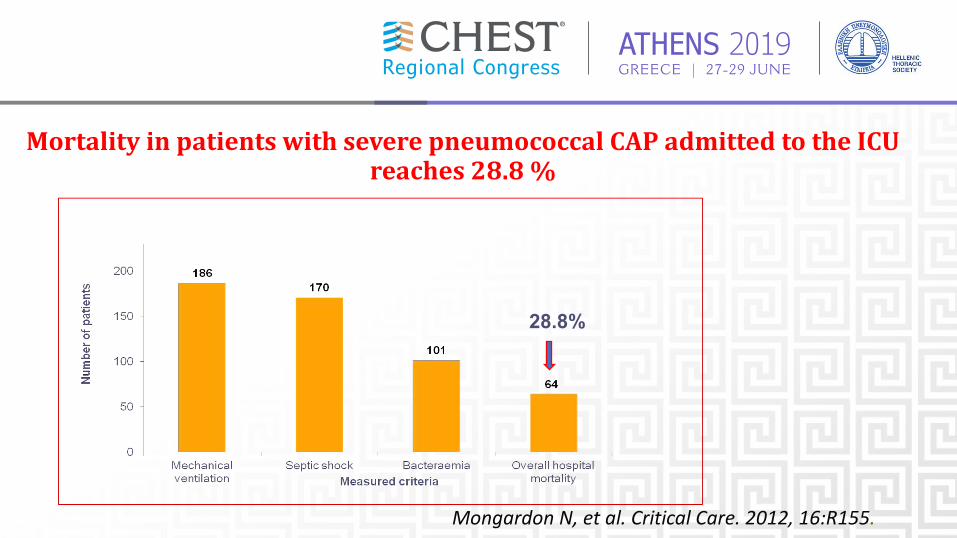
28.8%
Mongardon N, et al. Critical Care. 2012, 16:R155.
MortalityinpatientswithseverepneumococcalCAPadmittedtotheICUreaches28.8%
ATHENS 2019GREECE | 27-29 JUNE
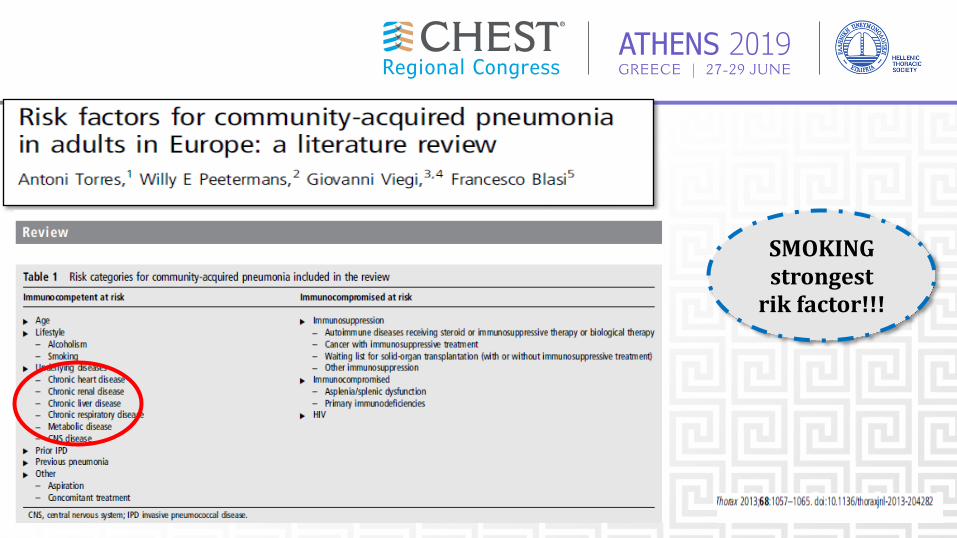
SMOKINGstrongestrik factor!!!
ATHENS 2019GREECE | 27-29 JUNE
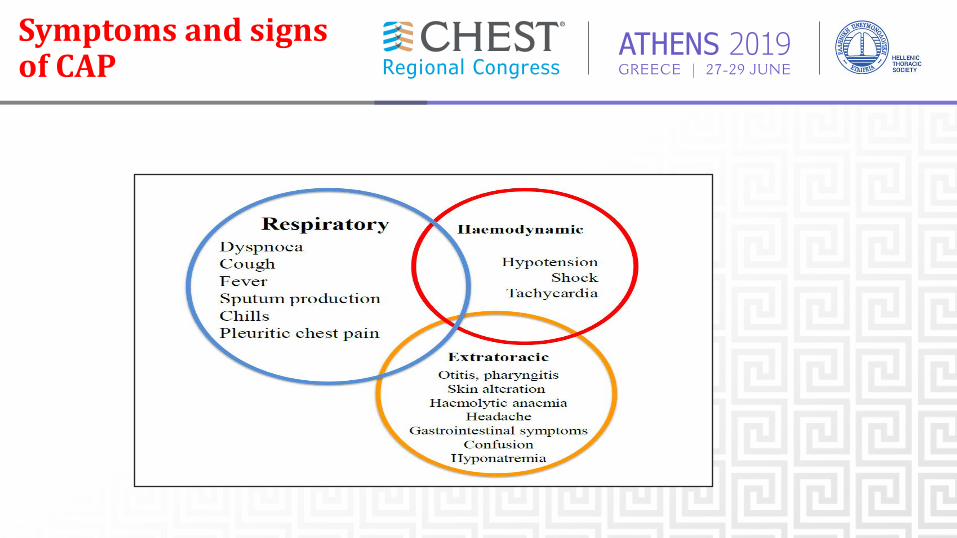
SymptomsandsignsofCAP
ATHENS 2019GREECE | 27-29 JUNE
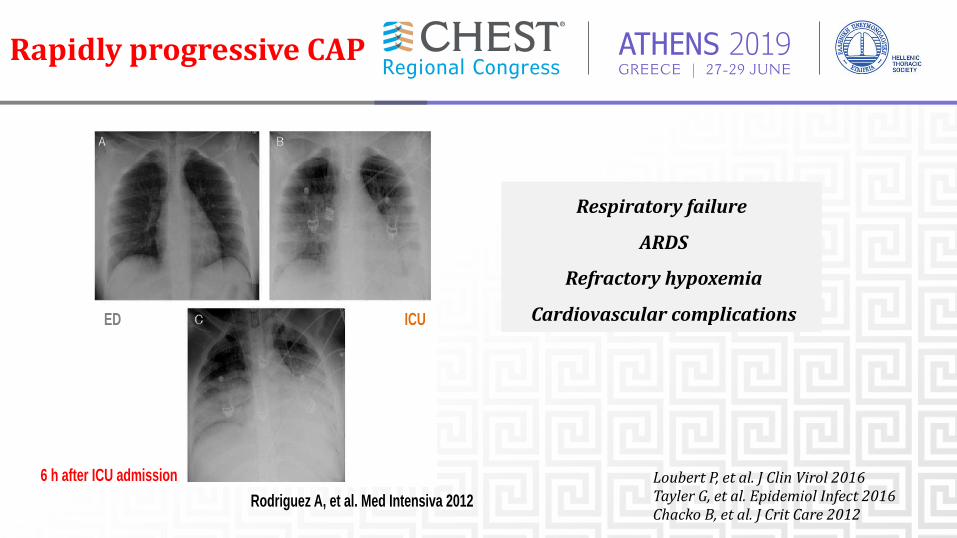
Rapidlyprogressive CAP
Rodriguez A, et al. Med Intensiva 2012
ED ICU
6 h after ICU admission
Respiratory failure
ARDS
Refractory hypoxemia
Cardiovascularcomplications
Loubert P,etal.JClin Virol 2016Tayler G,etal.Epidemiol Infect2016Chacko B,etal.JCrit Care 2012
ATHENS 2019GREECE | 27-29 JUNE
ETIOLOGY
ATHENS 2019GREECE | 27-29 JUNE
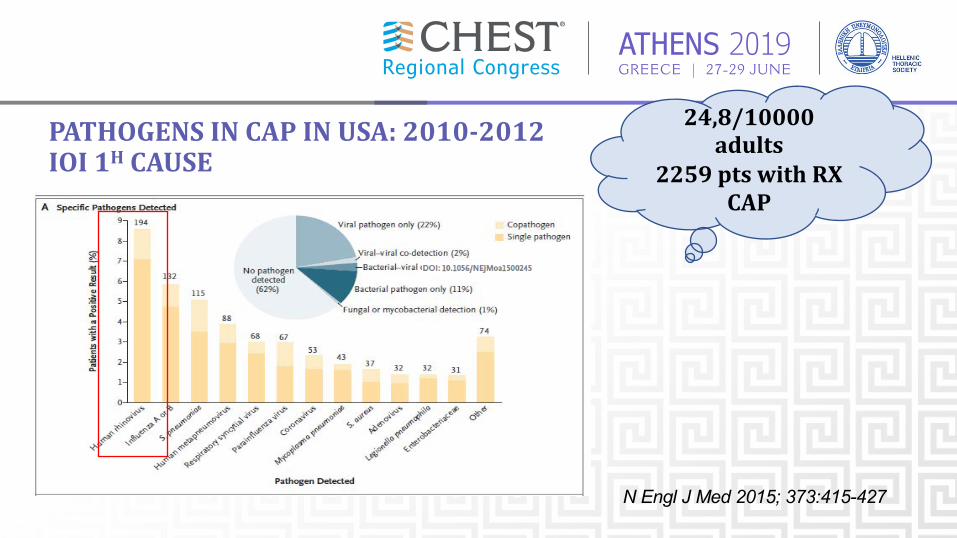
More than 100 microbes can cause CAP. A microbiologic diagnosis wasconfirmed in 38 to 87 percent of cases of CAP in studies that usedspecialized tests to detect various pathogens."Typical" organisms include S. pneumoniae, Haemophilus influenzae,Staphylococcus aureus, group A streptococci, Moraxella catarrhalis,anaerobes, and aerobic gram-negative bacteria."Atypical" pneumonia refers to pneumonia caused by Legionella spp, M.pneumoniae, C. pneumoniae, and Chlamydia psittaci; although imprecise, weuse this term because of its acceptance among clinicians.Polymicrobial aetiology -mixed infection, 2%-13%
ETIOLOGY
ATHENS 2019GREECE | 27-29 JUNE
PATHOGENSINCAP IN USA:2010-2012ΙΟΙ1Η CAUSE
N Engl J Med 2015; 373:415-427
24,8/10000adults
2259ptswithRXCAP
ATHENS 2019GREECE | 27-29 JUNE
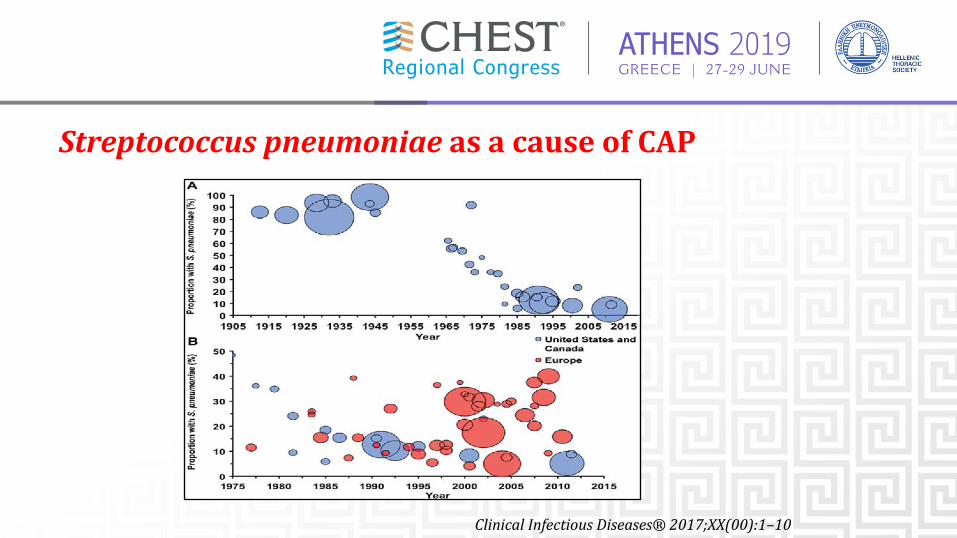
StreptococcuspneumoniaeasacauseofCAP
ClinicalInfectiousDiseases®2017;XX(00):1–10
ATHENS 2019GREECE | 27-29 JUNE
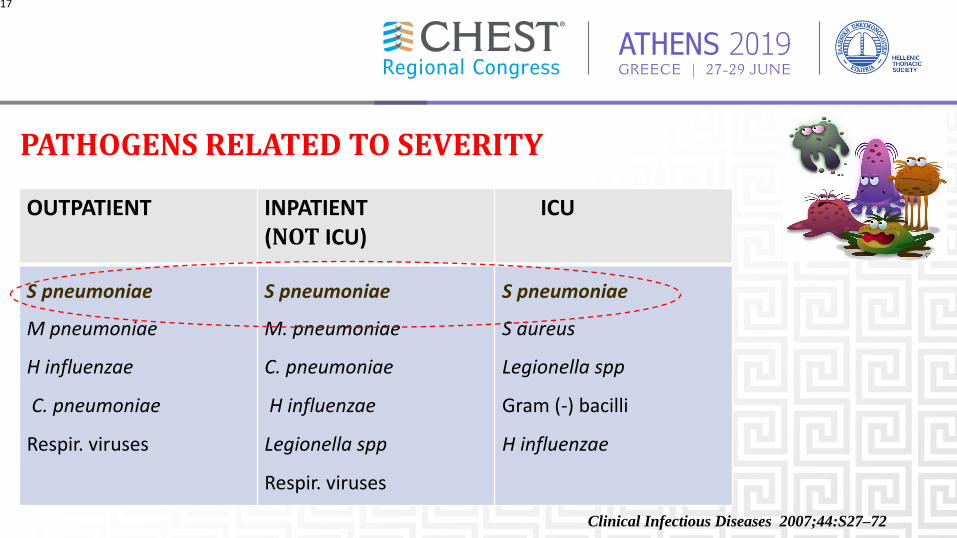
PATHOGENSRELATEDTOSEVERITY
OUTPATIENT INPATIENT(NOT ICU)
ICU
S pneumoniae
M pneumoniae
H influenzae
C. pneumoniae
Respir. viruses
S pneumoniae
M. pneumoniae
C. pneumoniae
H influenzae
Legionella spp
Respir. viruses
S pneumoniae
S aureus
Legionella spp
Gram (-) bacilli
H influenzae
17
Clinical Infectious Diseases 2007;44:S27–72
ATHENS 2019GREECE | 27-29 JUNE
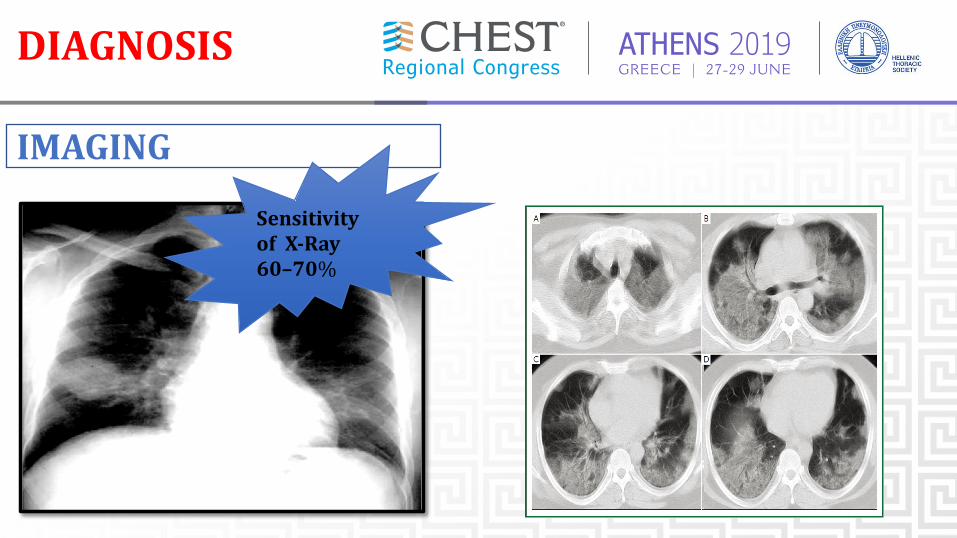
DIAGNOSIS
IMAGING
SensitivityofX-Ray60–70%
ATHENS 2019GREECE | 27-29 JUNE
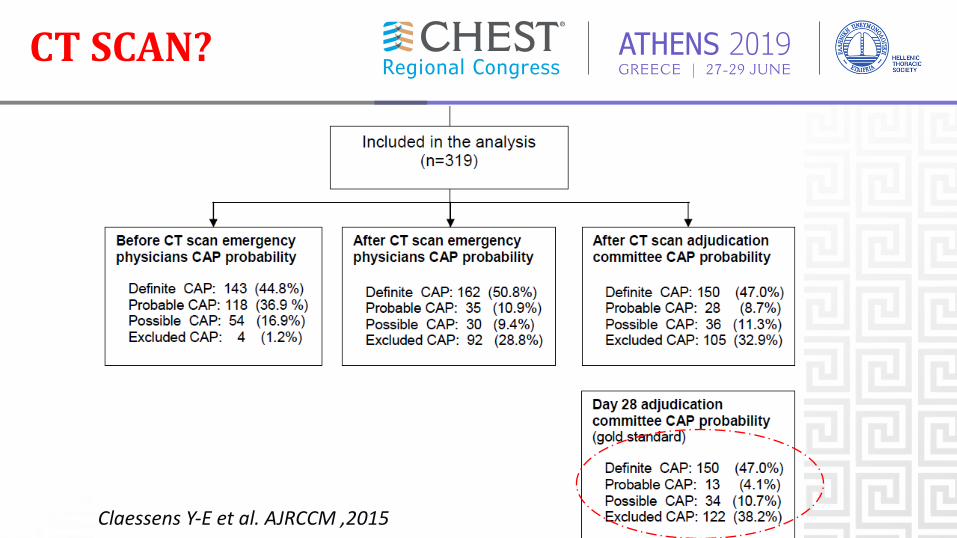
CTSCAN?
Claessens Y-E et al. AJRCCM ,2015
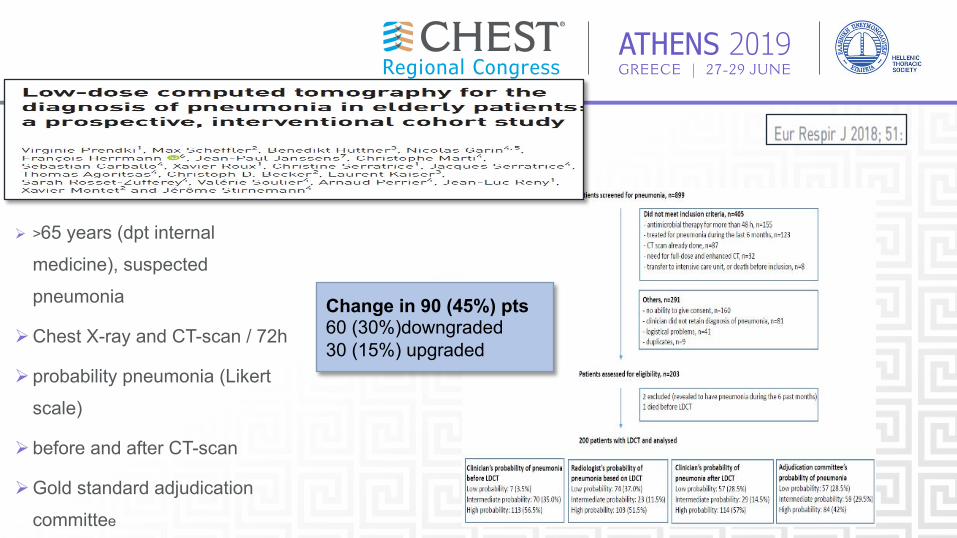
ATHENS 2019GREECE | 27-29 JUNE
Ø >65 years (dpt internal
medicine), suspected
pneumonia
ØChest X-ray and CT-scan / 72h
Ø probability pneumonia (Likert
scale)
Ø before and after CT-scan
ØGold standard adjudication
committee
Change in 90 (45%) pts60 (30%)downgraded30 (15%) upgraded
ATHENS 2019GREECE | 27-29 JUNE
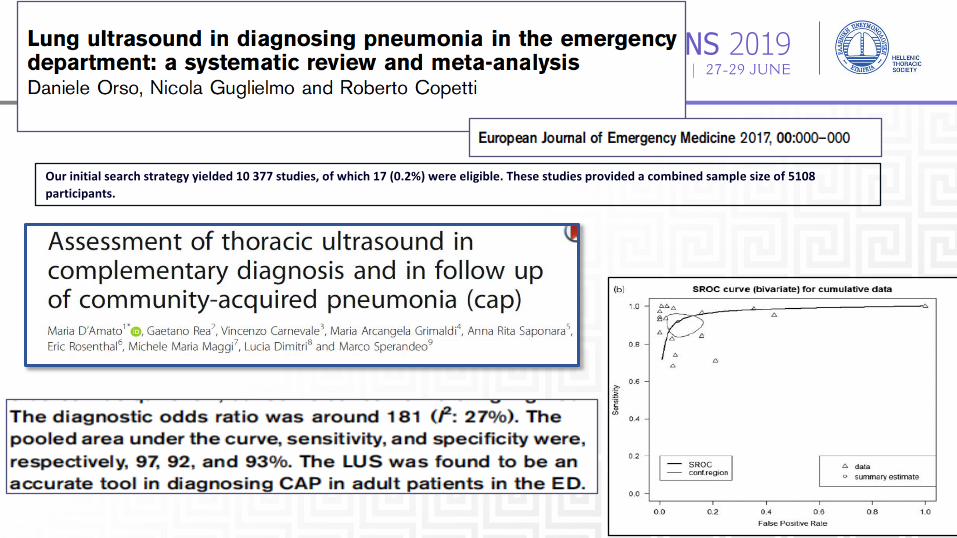
Our initial search strategy yielded 10 377 studies, of which 17 (0.2%) were eligible. These studies provided a combined sample size of 5108participants.
ATHENS 2019GREECE | 27-29 JUNE
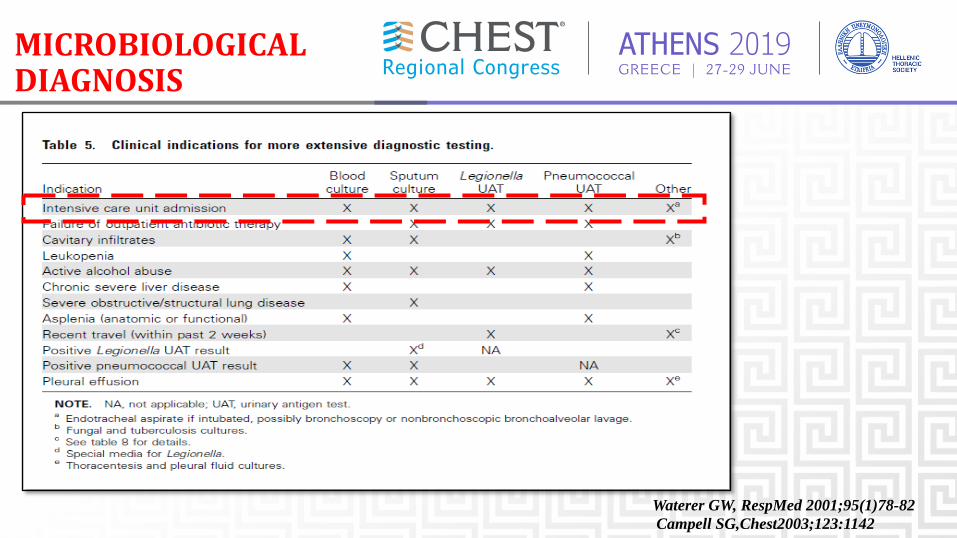
MICROBIOLOGICALDIAGNOSIS
Waterer GW, RespMed 2001;95(1)78-82Campell SG,Chest2003;123:1142
ATHENS 2019GREECE | 27-29 JUNE
Sputum: Gram staining and culture Expectorated sputum should be deep cough specimen obtained before antibiotic treatmentand it should be rapidly transported and processedwithin a few hours of collection.
Blood cultures (2 sets)2 sets of blood cultures should be drawn before initiation of antibiotic therapy during thefirst 24 hours.
Clinical Infectious Diseases 2007; 44:S27–72
ATHENS 2019GREECE | 27-29 JUNE
URINEANTIGEN
§ ΑgSpneumoniae shouldbeperformedin patientsadmittedtothehospitalforreasonsofillnessseverityand wheneverapleural fluidsampleisobtainedinthesettingofaparapneumonic effusion
§ UrineL.pneumophilaserogroup1Αgdetectionshould beperformedinpatientsadmittedtothehospitalforreasonsofseverityandinotherpatientswherethisinfectionis clinicallyorepidemiologicallysuspected
§ Thetestretainsvalidityevenaftertheinitiationofantibiotictherapy
Clin Microbiol Infect 2011; 17(Suppl. 6): E1–E59
ATHENS 2019GREECE | 27-29 JUNE
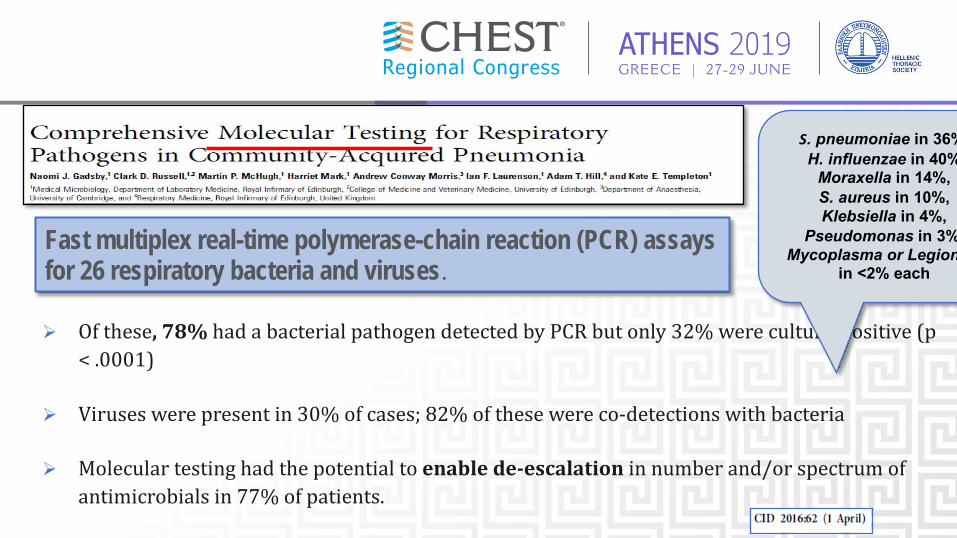
Ø Ofthese,78%hadabacterialpathogendetectedbyPCRbutonly32%wereculture-positive(p<.0001)
Ø Viruseswerepresentin30%ofcases;82%ofthesewereco-detectionswithbacteria
Ø Moleculartestinghadthepotentialtoenablede-escalationinnumberand/orspectrumofantimicrobialsin77%ofpatients.
Fast multiplex real-time polymerase-chain reaction (PCR) assays for 26 respiratory bacteria and viruses.
S. pneumoniae in 36%,H. influenzae in 40%,
Moraxella in 14%, S. aureus in 10%, Klebsiella in 4%,
Pseudomonas in 3%, Mycoplasma or Legionella
in <2% each
ATHENS 2019GREECE | 27-29 JUNE
ATHENS 2019GREECE | 27-29 JUNE
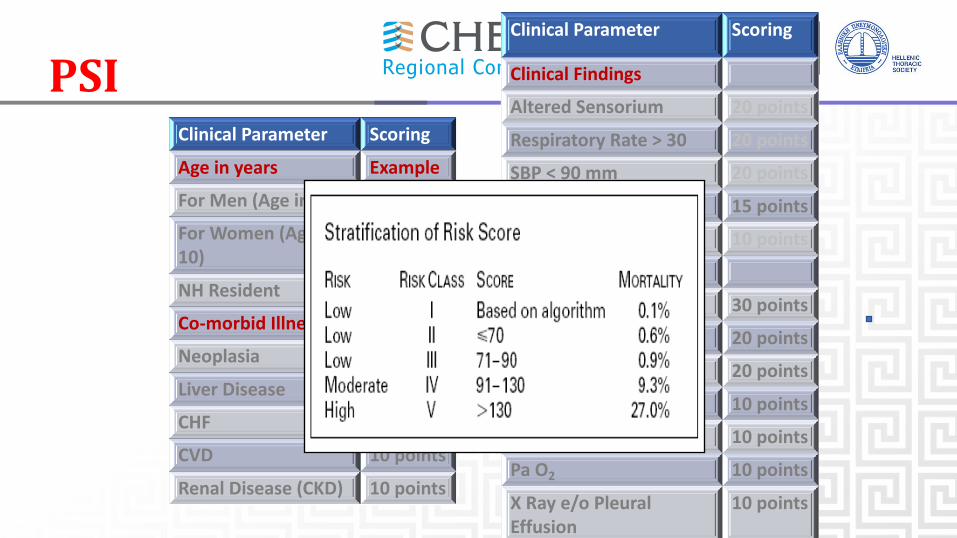
Clinical Parameter Scoring
Age in years Example
For Men (Age in yrs) 50
For Women (Age -10)
(50-10)
NH Resident 10 points
Co-morbid Illnesses
Neoplasia 30 points
Liver Disease 20 points
CHF 10 points
CVD 10 points
Renal Disease (CKD) 10 points
Clinical Parameter Scoring
Clinical Findings
Altered Sensorium 20 points
Respiratory Rate > 30 20 points
SBP < 90 mm 20 points
Temp < 350 C or > 400 C 15 points
Pulse > 125 per min 10 points
Investigation Findings
Arterial pH < 7.35 30 points
BUN > 30 20 points
Serum Na < 130 20 points
Hematocrit < 30% 10 points
Blood Glucose > 250 10 points
Pa O2 10 points
X Ray e/o Pleural Effusion
10 points
PSI
ATHENS 2019GREECE | 27-29 JUNE
ATHENS 2019GREECE | 27-29 JUNE
ATHENS 2019GREECE | 27-29 JUNE
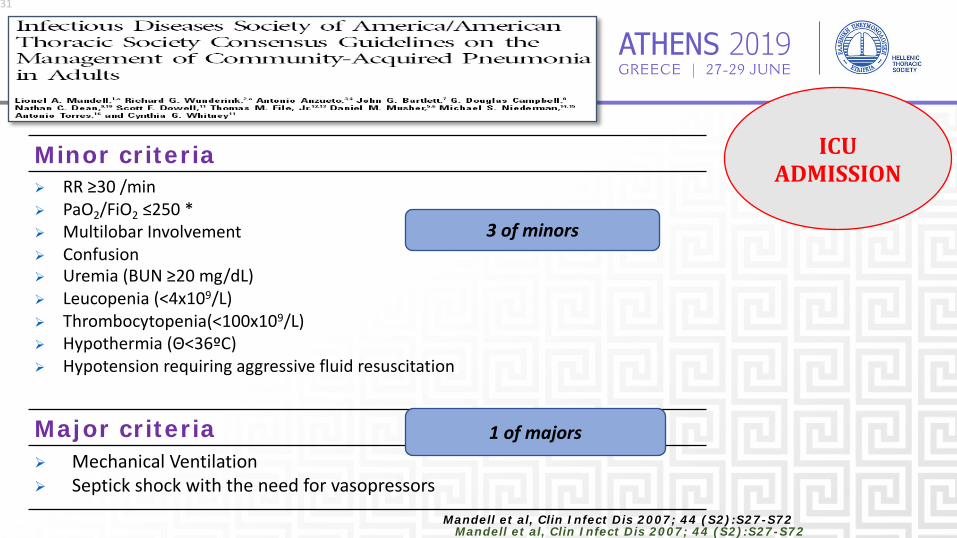
Minor criteriaØ RR ≥30 /minØ PaO2/FiO2 ≤250 *Ø Multilobar InvolvementØ ConfusionØ Uremia (BUN ≥20 mg/dL)Ø Leucopenia (<4x109/L)Ø Thrombocytopenia(<100x109/L)Ø Hypothermia (Θ<36ºC)Ø Hypotension requiring aggressive fluid resuscitation
Major criteriaØ Mechanical VentilationØ Septick shock with the need for vasopressors
31
Mandell et al, Clin Infect Dis 2007; 44 (S2):S27-S72
3 of minors
1 of majors
Mandell et al, Clin Infect Dis 2007; 44 (S2):S27-S72
ICUADMISSION

ATHENS 2019GREECE | 27-29 JUNE
THERAPY
ATHENS 2019GREECE | 27-29 JUNE
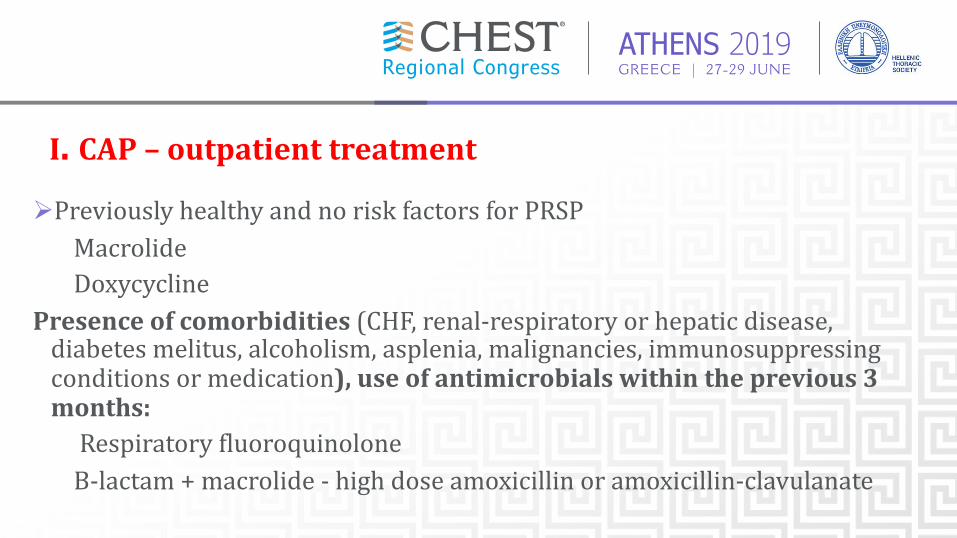
I. CAP– outpatienttreatmentØPreviouslyhealthyandnoriskfactorsforPRSP
MacrolideDoxycycline
Presenceofcomorbidities (CHF,renal-respiratoryorhepaticdisease,diabetesmelitus,alcoholism,asplenia, malignancies,immunosuppressingconditionsormedication),useofantimicrobialswithintheprevious3months:RespiratoryfluoroquinoloneΒ-lactam +macrolide- highdoseamoxicillinoramoxicillin-clavulanate
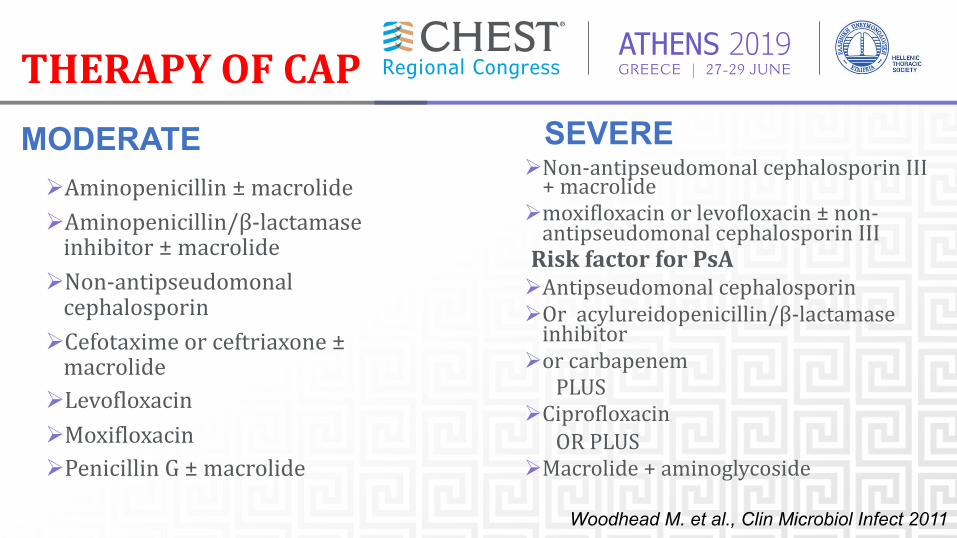
ATHENS 2019GREECE | 27-29 JUNETHERAPYOFCAP
MODERATEØAminopenicillin± macrolideØAminopenicillin/β-lactamaseinhibitor ± macrolide
ØNon-antipseudomonalcephalosporin
ØCefotaxime or ceftriaxone ±macrolide
ØLevofloxacinØMoxifloxacinØPenicillinG± macrolide
ØNon-antipseudomonal cephalosporin III+macrolideØmoxifloxacin or levofloxacin ± non-antipseudomonal cephalosporin IIIRiskfactor for PsAØAntipseudomonal cephalosporinØOr acylureidopenicillin/β-lactamaseinhibitor
Øor carbapenemPLUS
ØCiprofloxacinORPLUS
ØMacrolide +aminoglycoside
Woodhead M. et al., Clin Microbiol Infect 2011
SEVERE
ATHENS 2019GREECE | 27-29 JUNE
ATHENS 2019GREECE | 27-29 JUNE
DURATIONOFTHERAPY
- In clinical practice, a standard 10-14 days approach is still used to decide duration of antibiotic therapy in CAP patients.
- ATS/IDSA 2007 and ERS 2011 guidelines recommendations suggest to individualize duration of antibiotic therapy on patients’ characteristicsnicalpractice, a standard 10-14 days approach is still used to decide duration of
antibiotic therapy in CAP patients.
- ATS/IDSA 2007 and ERS 2011 guidelines recommendations suggest to individualize duration of antibiotic therapy on patients’ characteristics.
Woodhead M, Clin Microbiol Infect 2011Mandell LA, CID 2007
ERJ 2010; 36(1):128–34
- Patients with CAP should be treated for a minimum of 5 days (level I evidence), should be afebrile for 48–72 h, and should have no more than 1 CAP-associated sign of clinical instability before discontinuation of therapy (level
II evidence).
ATHENS 2019GREECE | 27-29 JUNE
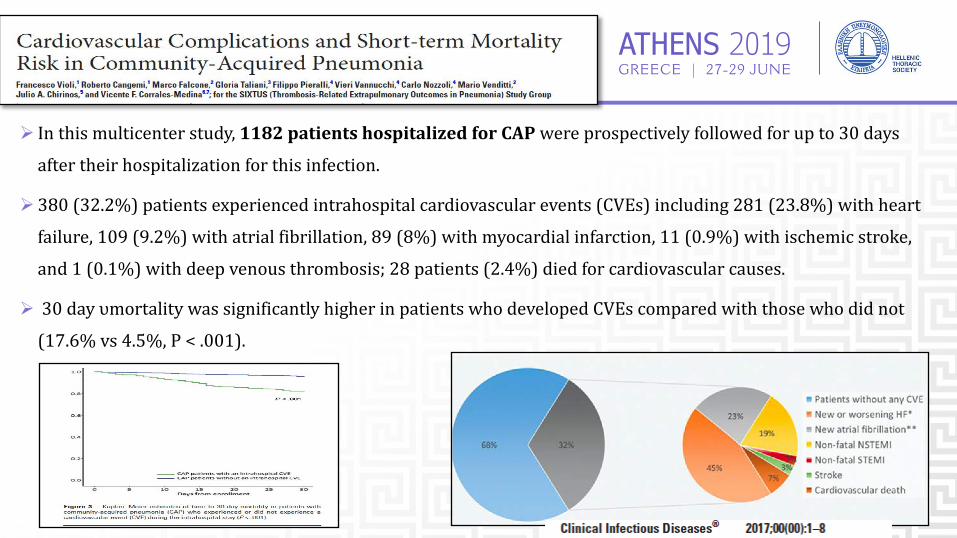
Ø Inthismulticenterstudy,1182patientshospitalizedforCAPwereprospectivelyfollowedforupto30days
aftertheirhospitalizationforthisinfection.
Ø 380(32.2%)patientsexperiencedintrahospitalcardiovascularevents(CVEs)including281(23.8%)withheart
failure,109(9.2%)withatrialfibrillation,89(8%)withmyocardialinfarction,11(0.9%)withischemicstroke,
and1(0.1%)withdeepvenousthrombosis;28patients(2.4%)diedforcardiovascularcauses.
Ø 30dayυmortalitywassignificantlyhigherinpatientswhodevelopedCVEscomparedwiththosewhodidnot
(17.6%vs4.5%,P<.001).
ATHENS 2019GREECE | 27-29 JUNE
38
PREVENTION
ØSmokingCessationØΕμβολιασμόςØ InfluenzaØ Inactivatedvaccineforpeople>50yo,thoseatriskforinfluenzacomplications,pregnancy,householdcontactsofhigh-riskpersonsandhealthcareworkers
Ø Intranasallive,attenuatedvaccine:5-49 yo withoutchronicunderlyingdz
Ø Pneumococcal(PPV23,PCV13)Immunocompetent≥65yo,chronicillnessandimmunocompromised≤64yo
ATHENS 2019GREECE | 27-29 JUNE
Hospital-acquiredpneumonia
NewGuidelines(2016fromATS,2017fromERS)• Definitions• Pathogenesis• Etiology• Diagnosis:invasiveornon-invasivetechniques• Therapy§

ATHENS 2019GREECE | 27-29 JUNEHAP
NNVAP NIV
MVHAP
ATHENS 2019GREECE | 27-29 JUNE
MAINFOCUS(2005)
Ø HCAP(HEALTHCAREASSOCIATEDPNEUMONIA)
Ø MDR(MULTIDRUGRESISTANTBACTERIA)
Pseudomonasaeruginosa,Acinetobacterspp.,Staphylococcusaureus
ATHENS 2019GREECE | 27-29 JUNEEPIDEMIOLOGY
§ HAP/VAPtogetheraccountfor22%ofallhospital-associatedinfections
▸ HAP:5- 20cases/1000admissions,higherratesamongimmunocompromised,surgery &elderly.
Ølesssevere,butseriouscomplicationsstilloccurin~50%ofpatientswith20%requireICUadmission
▸VAP ~10%incidenceofVAPinpatientsrequiringventilation
▸ All-causemortality inpatientswithVAP20-50%,attributablemortality13%
▸ prolongslengthofventilationby7.6- 11.5days
▸ prolongshospitalizationby11.5- 13.1days
▸ $40Kexcesscostperpatient(USdata)
▸ $46millionexcesscostannually(Canadiandata)
Clin Infect Dis 2016; 63: e61-e111Giuliano KK: 2018, Davies G: Pa Patient Saf Advis 2012,Baker D:2018
ATHENS 2019GREECE | 27-29 JUNE
ATHENS 2019GREECE | 27-29 JUNE
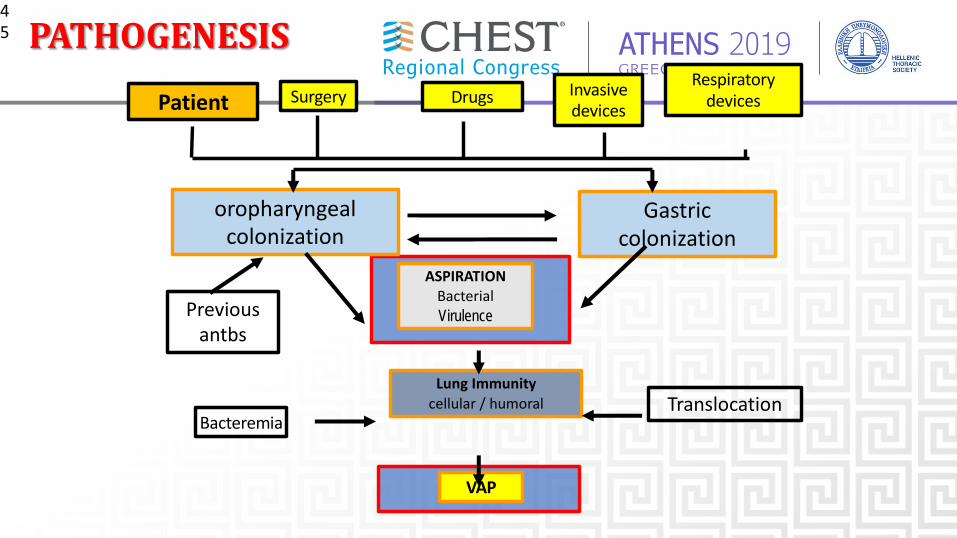
Patient Surgery Drugs Invasive devices
Respiratory devices
Gastric colonization
oropharyngeal colonization
ASPIRATIONΒacterialVirulence
Lung Immunitycellular / humoral Translocation
Bacteremia
VAP
Previous antbs
45 PATHOGENESIS
ATHENS 2019GREECE | 27-29 JUNE
MICROBIOLOGYOFHAP/VAPCorepathogensStr. pneumoniaeMethicillin-susceptibleStaphylococcusaureus(MSSA)Haemophilus influenzaeGram(-)EnterobacteriaeceaeEscherichiacoliKlebsiellapneumoniaeEnterobacterspp.Proteusspp.Serratiamarcescens
American Thoracic Society. GuidelinesAm J Respir Crit Care Med 2005
ATHENS 2019GREECE | 27-29 JUNE
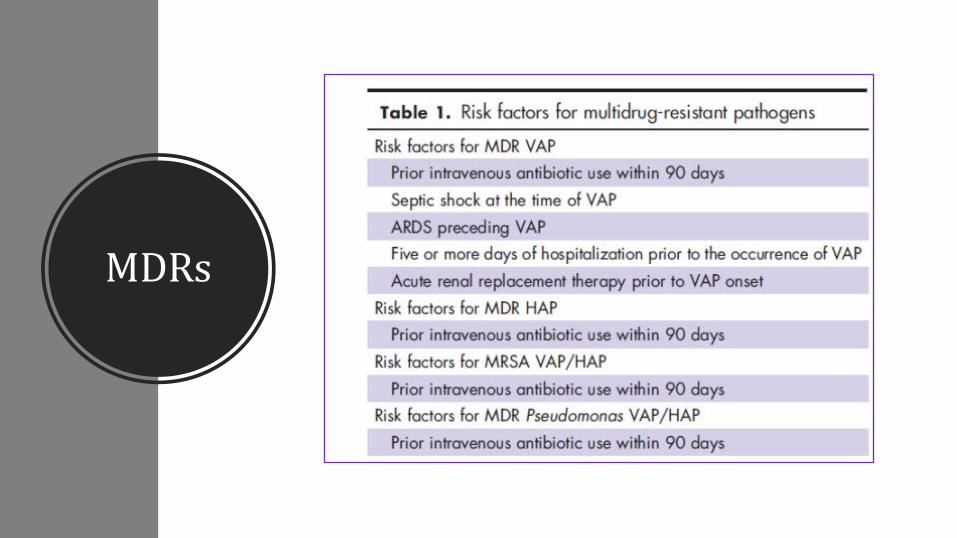
MDRs
Ø Methicillin-resistantS.aureus (MRSA)Ø Pseudomonasaeruginosa resistanttoantipseudomonalpenicillins,cephalosporins,carbapenems,andquinolones
Ø Acinetobacterbaumanii
Ø Vancomycin-resistantEnterococcusØ Enterobacteriaceaeproducingextended-spectrumB-lactamases(ESBL)
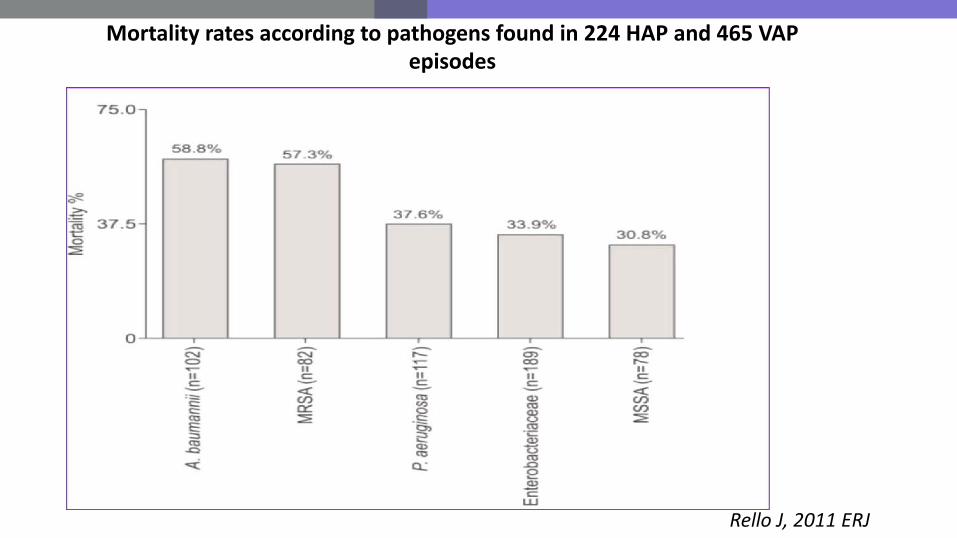
Rello J, 2011 ERJ
Mortality rates according to pathogens found in 224 HAP and 465 VAP episodes

ATHENS 2019GREECE | 27-29 JUNE
DIAGNOSTICSTRATEGY
NOGOLDSTADARD
ATHENS 2019GREECE | 27-29 JUNE
50
???

ATHENS 2019GREECE | 27-29 JUNE
ClinicalDiagnosticStrategy
ClinicalsuspicionØ PatientonMV+infiltrateCXR
Ø+2/3findingsØ Symptomsà infection:
Ø(1)Fever,(2)purulenttrachealsecretions
Ø Laboratoryà infection:
Ø(3)Leukocytosis orleukopenia
ØHypoxemia
DifferentialdiagnosisPChemicalaspirationwithoutinfection
PAtelectasis
PPulmonaryembolism
PARDS
PPulmonaryhemorrhage
PLungcontusion
PDrugreaction
POther
ATHENS 2019GREECE | 27-29 JUNE
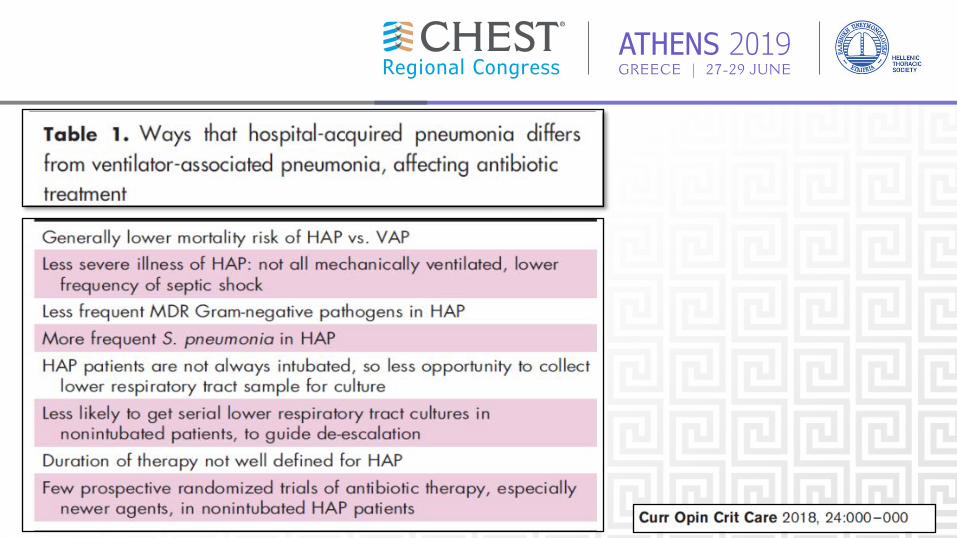
InPatientsWithSuspectedHAP(Non-VAP),ShouldTreatmentBeGuidedbytheResultsofMicrobiologicStudiesPerformedonRespiratorySamples,orShouldTreatmentBeEmpiric?
ØTreataccordingtotheresultsofmicrobiologicstudiesperformedonrespiratorysamplesobtainednoninvasively, ratherthanbeingtreatedempirically(weakrecommendation,verylow-qualityevidence).
ØRemarks:Non-invasivemethodstoobtainrespiratorysamplesincludethefollowing:
Ø spontaneousexpectoration,
Ø sputuminduction,
Ø naso-trachealsuctioninginapatientwhoisunabletocooperatetoproduceasputumsample,and
Ø endotrachealaspirationinapatientwithHAPwhosubsequentlyrequiresmechanicalventilation.
ATHENS 2019GREECE | 27-29 JUNE
Non-invasivesamplingwithsemi-quantitativeculturestodiagnose
VAP(weakrecommendation,low-qualityevidence).
Remarks:Invasiverespiratorysamplingincludesbronchoscopictechniques(ie,bronchoalveolarlavage[BAL],protectedspecimenbrush[PSB])andblindbronchialsampling(ie,mini-BAL).Noninvasiverespiratorysamplingreferstoendotrachealaspiration.

ATHENS 2019GREECE | 27-29 JUNE
ATHENS 2019GREECE | 27-29 JUNE
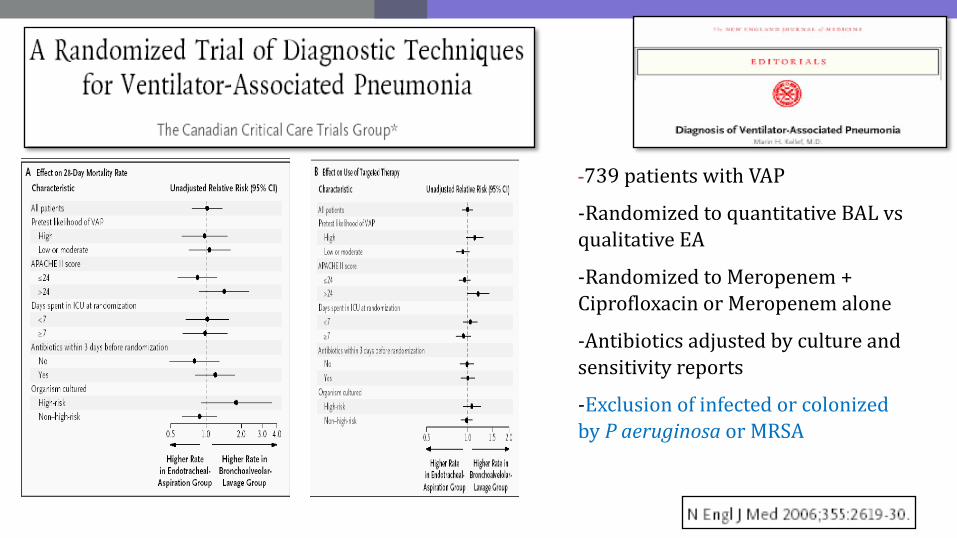
-739patients with VAP
-Randomized to quantitative BALvsqualitative EA
-Randomized to Meropenem+Ciprofloxacin or Meropenemalone
-Antibiotics adjusted by cultureandsensitivity reports
-Exclusion of infected or colonizedby Paeruginosa or MRSA
ATHENS 2019GREECE | 27-29 JUNE
Using clinicalcriteriaalone,ratherthanusingserumPCT plusclinicalcriteria,todecidewhetherornottoinitiateantibiotictherapy(strongrecommendation,moderate-qualityevidence)
Usingclinicalcriteriaalone,ratherthanusingCPIS plusclinicalcriteria,todecidewhetherornottoinitiateantibiotictherapy(weakrecommendation,low-qualityevidence).
Usingclinicalcriteriaalone,ratherthanusingbroncho-alveolarlavagefluid(BALF)sTREM-1plusclinicalcriteria,todecidewhetherornottoinitiateantibiotictherapy(strongrecommendation,moderate-qualityevidence).
Kalil 2016, Torres 2017
BIOMARKERS
ATHENS 2019GREECE | 27-29 JUNETHERAPY
Whatchanged?ØEmpirictreatmentshouldcoverMDRpathogensinanypatientwithriskfactorsregardlessofthetimeofonsetofinfection
ØEachhospitalgenerateantibiogramstoguidehealthcareprofessionalswithrespecttotheoptimalchoiceofantibiotics.
ATHENS 2019GREECE | 27-29 JUNE
INITIALEMPIRICTREATMENT
ØTakeintoconsiderationthelocalmicrobiologypatternsofICUorhospital
ØTheinitialantibiotictreatmentismostlikelytobeappropriatewhengivenbaseduponaprotocoladjustedtothelocalresistancepatterns
ØPatientsinwhomHAP/VAPissuspectedshouldbeadministeredinitialempiricaltreatmentaftersamplesformicrobiologicalculturesarecollected.
ATHENS 2019GREECE | 27-29 JUNE
MDRs
ATHENS 2019GREECE | 27-29 JUNE
THERAPYVAP
Kalil etal,CID2016
ATHENS 2019GREECE | 27-29 JUNE
62
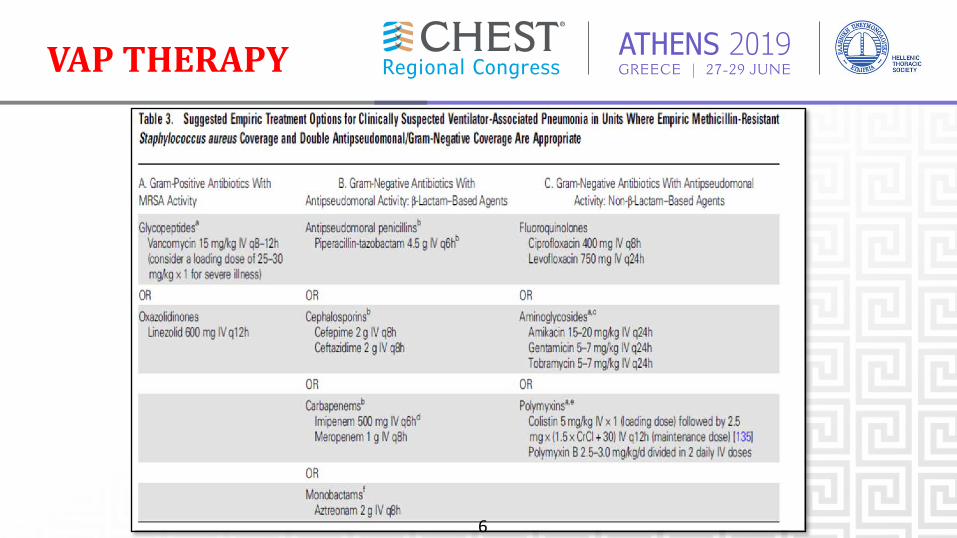
VAPTHERAPY
ATHENS 2019GREECE | 27-29 JUNE
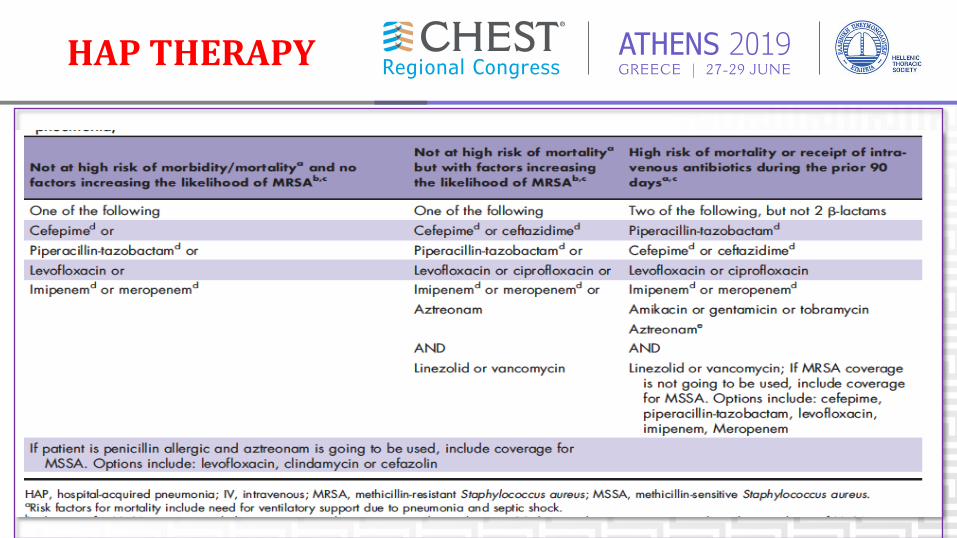
HAPTHERAPY

ATHENS 2019GREECE | 27-29 JUNE
EMPIRICALTHERAPYFORHAP
§ MRSAcoveragewhenwehaveriskfactorforresistanceorhighriskformortality(needforventilatorysupportorsepticshock) (weakrecommendation,verylow-qualityevidence)
ØPseud.aeruginosa coveragewith2antbs whenwehaveriskfactorforresistanceorhighriskformortality(strongrecommendation, verylow-qualityevidence)
ØNOTusingaminoglycoside asthesoleantb agent
ATHENS 2019GREECE | 27-29 JUNE
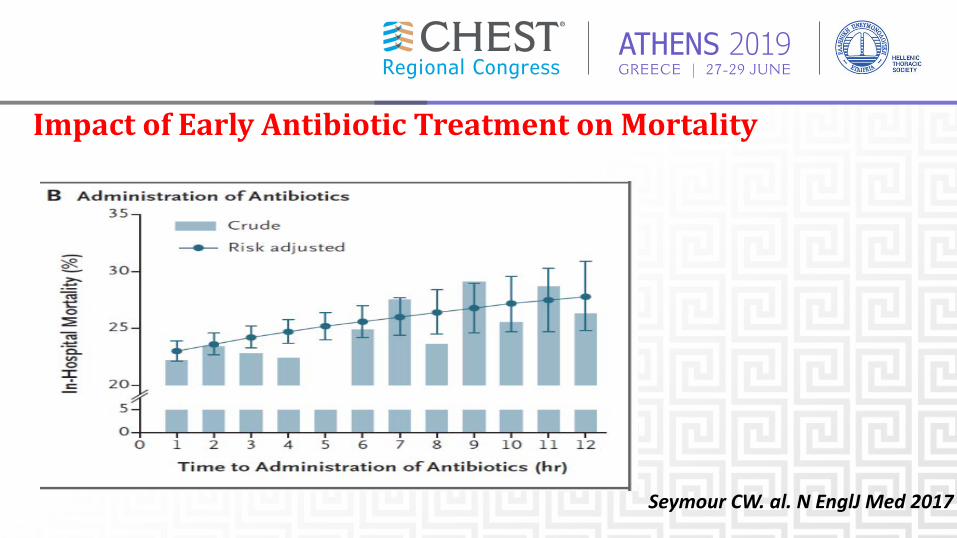
ImpactofEarlyAntibioticTreatmentonMortality
Seymour CW. al. N EnglJ Med 2017
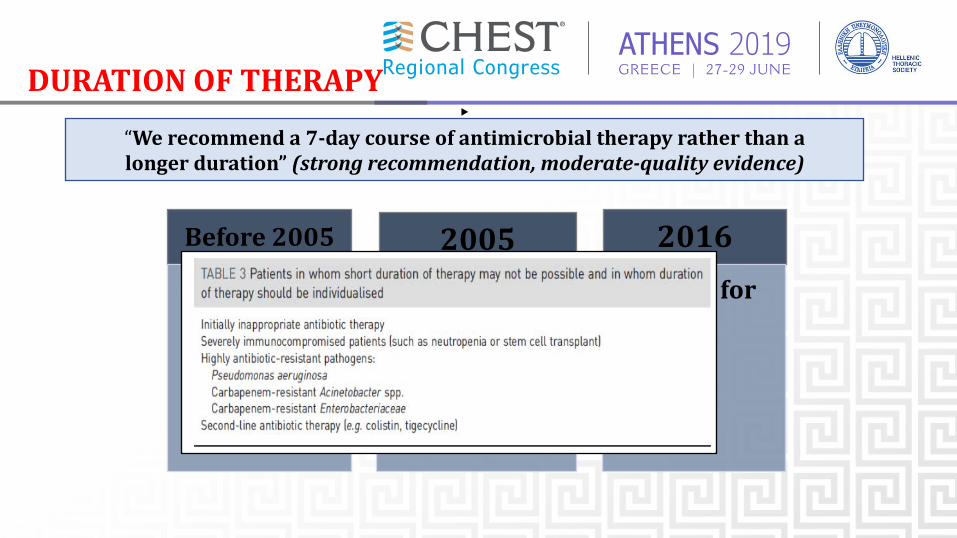
ATHENS 2019GREECE | 27-29 JUNEDURATIONOFTHERAPY
Before2005
• 14-21days2005
• 7daysforclinicalimprovement
• 14daysforPseudaerugHAP/VAP
2016• 7daysforall
▸“Werecommenda7-daycourseofantimicrobialtherapyratherthanalongerduration”(strongrecommendation,moderate-qualityevidence)
ATHENS 2019GREECE | 27-29 JUNE
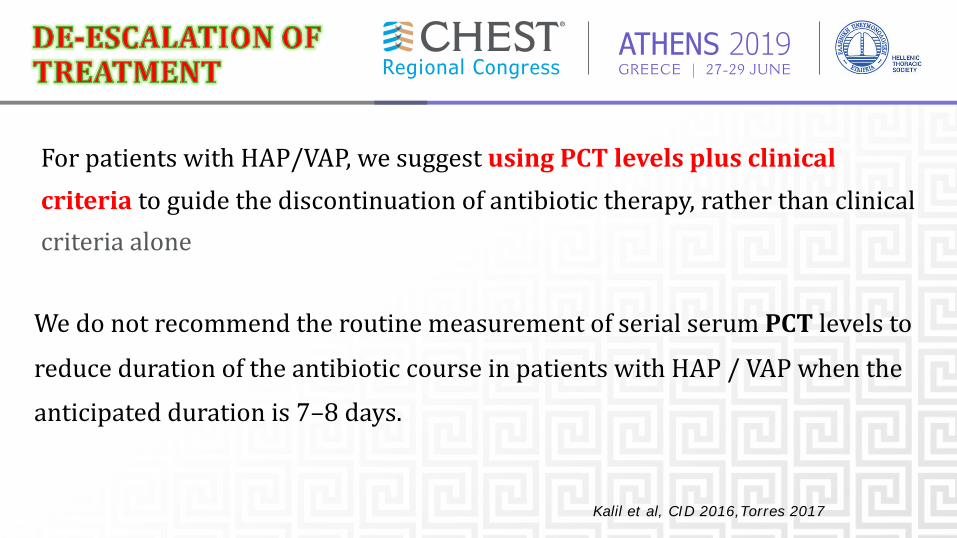
ForpatientswithHAP/VAP,wesuggestusingPCT levelsplusclinicalcriteria toguidethediscontinuationofantibiotictherapy,ratherthanclinicalcriteriaalone
Kalil et al, CID 2016,Torres 2017
WedonotrecommendtheroutinemeasurementofserialserumPCT levelstoreducedurationoftheantibioticcourseinpatientswithHAP/VAPwhentheanticipateddurationis7–8days.
ATHENS 2019GREECE | 27-29 JUNE
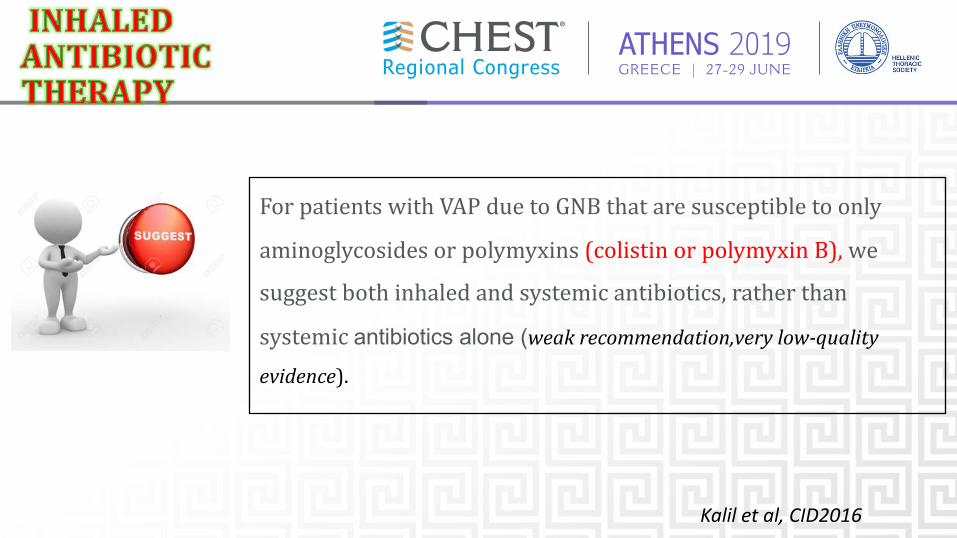
ForpatientswithVAPduetoGNBthataresusceptibletoonlyaminoglycosidesorpolymyxins(colistin orpolymyxinB),wesuggestbothinhaledandsystemicantibiotics,ratherthansystemicantibiotics alone (weakrecommendation,verylow-quality
evidence).
Kalil et al, CID2016
ATHENS 2019GREECE | 27-29 JUNE
§ 68 years old male with history of COPD (GOLD IV) is intubated due to hypercapnic coma
§ On day 4 of hospitalization, he developed fever(38° C), hypotension and a new left-sided infiltrate
§ ICU has an incidence of MRSA >20%
WHICH IS THE RECOMMENDED ANTIBIOTIC THERAPY?
QUESTION
ATHENS 2019GREECE | 27-29 JUNE
A. MeropenemB.Ciprofloxacin+linezolidC.AminoglycosideD.Vancomycinandcefepime +ciproxinE.Noneoftheabove
ATHENS 2019GREECE | 27-29 JUNE
Thankyouforyourattention!