Managing Community-acquired Pneumonia and Hospital-acquired Pneumonia - Professor Francesco Blasi
102
Francesco Blasi Department of Physiopathology and Transplantation University of Milan Managing CAP and HAP
-
Upload
waidid -
Category
Health & Medicine
-
view
137 -
download
1
Transcript of Managing Community-acquired Pneumonia and Hospital-acquired Pneumonia - Professor Francesco Blasi

Francesco BlasiDepartment of Physiopathology and Transplantation
University of Milan
Managing CAP and HAP

GLOSSARY
CAP- is defined as a pulmonary infection developing in the community or <48 hours of hospital admission.These patients may be managed in ER, the general ward or admitted directly to the ICU.
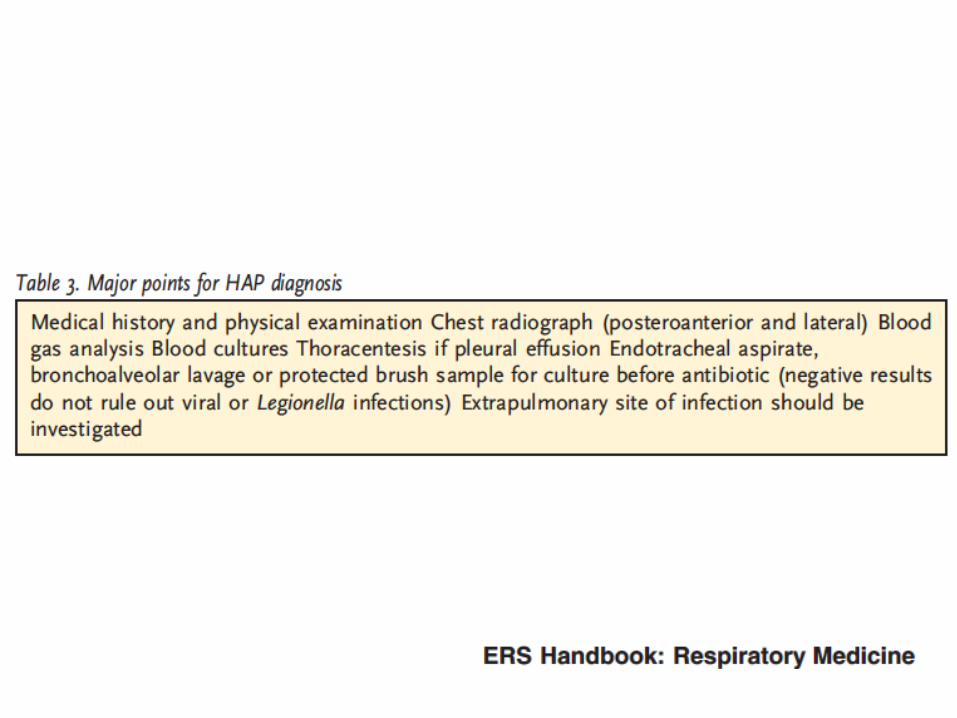
HAP is defined as a pulmonary infection developing during hospitalisation, 48 hours or more after admission, and not present or incubating at the time of admission.
VAP is defined as a pneumonia that arises more than 48–72 hours after endotracheal intubation.


Torres A, et al. Thorax 2013;68:1057–65.
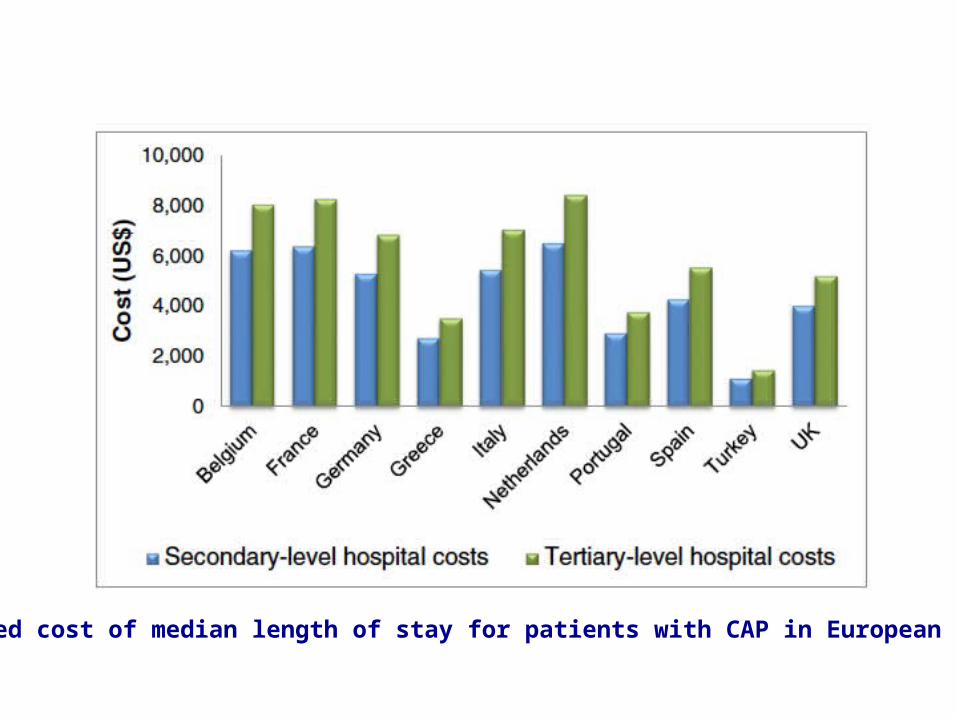
Estimated cost of median length of stay for patients with CAP in European hospitals

This was an observational, prospective study of consecutive patients coming from the community who were admitted to the Policlinico Hospital, Milan, Italy, with a diagnosis of pneumonia between April 2008 and April 2010. A total of 935 consecutive patients with pneumonia were enrolled during the study period
Aliberti A, et al CID 2012;54(4):470-8.

Risk Factors Analysis: MDR pathogens
Aliberti A, et al CID 2012;54(4):470-8.MDR multi drug resustantHCAP health care associated pneumonia

Aliberti A, et al CID 2012;54(4):470-8.MDR multi drug resistantCOPD chronic obstructive pulmonary disease

Aliberti S et al. Thorax 2013;68:997-9

New approach: Stratify risk factors
New findings: • Different risk factors have different importance for MDR prediction
•Chronic renal failure is an independent risk factor for MDR (A window of patient’s functional status)
•Patient’s targeted approach for empiric antibiotic therapy is possible
Aliberti A, et al CID 2012;54(4):470-8MDR multi drug resistant


CASE REPORT n. 1

Male, 74 y/o
Active smoker. Former parachutist.
Past medical history:
10-year history of COPD (dystrophic bullae) in LTOT since 1 year (2 L/m- 1.5 L/m). Chronic heart failure, pleural effusions since 4 years. Benign prostatic hyperplasia, depression, peptic ulcer.
Discharged 2 months before from the Internal Medicine Dpt with a diagnosis of UTI treated with ciprofloxacin.
FEV1: 64%
DLCO 47%
BGA (O2:1 L/m): pH: 7.49 PaCO2: 36 PaO2:64 HCO3: 22
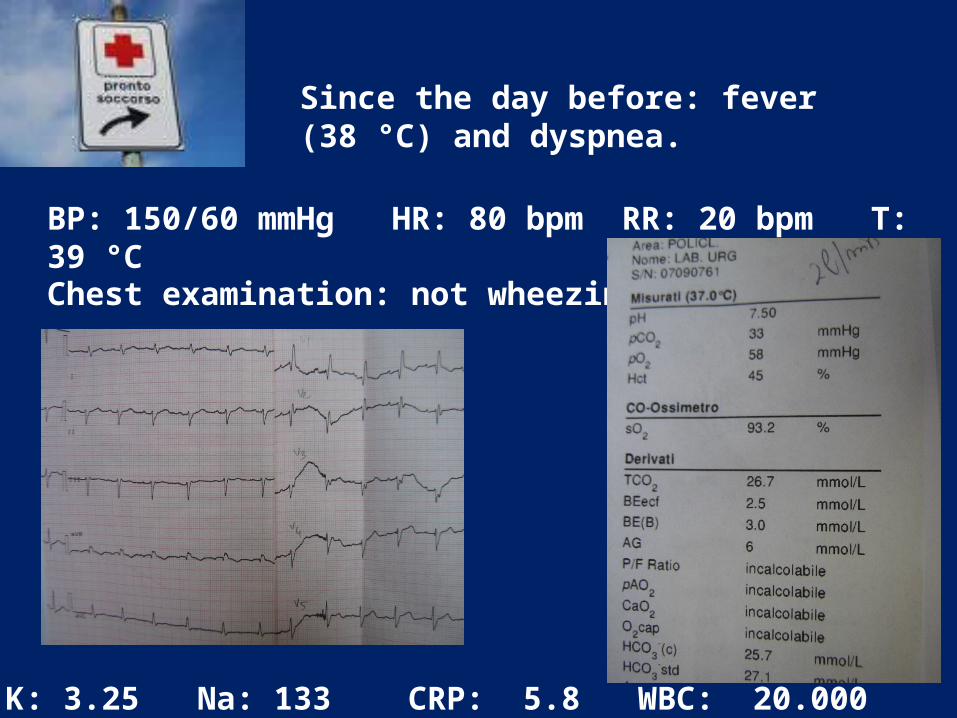
Since the day before: fever (38 °C) and dyspnea.
BP: 150/60 mmHg HR: 80 bpm RR: 20 bpm T: 39 °C
Chest examination: not wheezing
K: 3.25 Na: 133 CRP: 5.8 WBC: 20.000

PNEUMONIA
LIVER
Diaphragm

PNEUMONIA
B LINES


TREATMENT?

• Ceftriaxone 2gr ev
• Azithromycin 500 mg ev
Since the day before: fever (38 °C) and SOB.
BP: 150/ 60 mmHg HR: 80 bpm RR: 20 bpm T: 39 °C
Chest examination: non wheezing
K: 3.25 Na: 133 CRP: 5.8 WBC: 20.000

?

STRATIFYING RISK FACTORS

Aliberti A, et al CID 2012;54(4):470-8.MDR multi drug resistantCOPD chronic obstructive pulmonary disease

D1
Ceftriaxone 2gr
20.000
5.8 ---
18.000
14.6
WBC
CRP
T
Azithromycina 500
D2 D3
Ab anti-Legionella pneumophila: negative
Swab: bacteria and fungi: neg
Urinary antigens LP and SP: negative
Blood culture: negative
Ab anti-Mycoplasma: IgG negative and IgM negative
Naso-pharyngeal swab DNA CP, MP, LP: negative
Tracheal aspirate : Gram negative +++

In VII giornata
On day 3
Pleural effusion

Tracheal aspirate

WOULD YOU CHANGE?

Ceftriaxone 2gr
20.000
5.8 ---
18.000
14.6
15.000
---
14.200
5.6
WBC
CRP
T
Azithromycina 500 stopstop
Imipenem 1g q8 EVTracheal aspirate
D1 D2 D3 D4 D5
Ab anti-Legionella pneumophila: negative
Swab: bacteria and fungi: neg
Urinary antigens LP and SP: negative
Blood culture: negative
Ab anti-Mycoplasma: IgG negative and IgM negative
Naso-pharyngeal swab DNA CP, MP, LP: negative

Ceftriaxone 2gr
20.000
5.8 ---
18.000
14.6
15.000
---
14.200
5.6
12.400
---
WBC
CRP
T
Azithromycina 500 stopstop
Imipenem 1g q8 EV
D1 D2 D3 D4 D5 D6
Ab anti-Legionella pneumophila: negative
Swab: bacteria and fungi: neg
Urinary antigens LP and SP: negative
Blood culture: negative
Ab anti-Mycoplasma: IgG negative and IgM negative
Naso-pharyngeal swab DNA CP, MP, LP: negative
Tracheal aspirate

Discharged on Day 20…

TREATMENT OPTIONS FOR HOSPITALIZED PATIENTS WITH COMMUNITY-ACQUIRED PNEUMONIA (no need for intensive care treatment) (in alphabetical order) [C4]
INSIDE HOSPITAL: CAP
Aminopenicillin macrolide *#
Aminopenicillin / ß-lactamaseinhibitor # macrolide *
Non-antipseudomonal cephalosporin cefotaxime or ceftriaxone ±macrolide *
Levofloxacin #
Moxifloxacin #§
Penicillin G macrolide

TREATMENT OPTIONS FOR PATIENTS WITH SEVERE COMMUNITY-ACQUIRED PNEUMONIA [C4] (ICU OR INTERMEDIATE CARE)
INSIDE HOSPITAL: CAP
NO RISK FACTORS FOR P. aeruginosa Non-antipseudomonal cephalosporin III + macrolide *ormoxifloxacin or levofloxacin ± non-antipseudomonal cephalosporin III
RISK FACTORS FOR P. aeruginosa Antipseudomonal cephalosporin ** or acylureidopenicillin / ß-lactamaseinhibitor or carbapenem (meropenem preferred, up to 6 g possible, 3x2 in 3hours infusion)PLUSCiprofloxacin^ OR PLUSMacrolide* + aminoglycoside (gentamicin, tobramycin or amikacin)

WHAT EMPIRICAL ANTIBIOTIC TREATMENT IS RECOMMENDED FOR ASPIRATION PNEUMONIA?
INSIDE HOSPITAL: CAP
Hospital ward admitted from homeOral or iv-lactam/-lactamase inhibitoror Clindamycinor iv cephalosporin + oral metronidazoleor moxifloxacin
ICU or admitted from Nursing HomeClindamycin + cephalosporinorCephalosporin + metronidazole












CASE REPORT n. 2

Male, 56 y/o
He was referred to our ER because of new cough with sputum production, fever off and on (Tmax: 38°C) and mild dyspnea since 72 hours.
He also reported a 6-day history of malaise, sore throat and chills during the previous 15 days. Symptoms persisted in spite of NSAID
Past medical history:
-COPD (GOLD III)
- Hepatitis C, not on treatment
Allergy Hx: denied; Food exposure: denied; recent travel: denied; Family Hx: non-contributory
He was on aspirin
Tobacco 1-2 packs per day x 25 years, but no cigarettes in the prior 8 days due to feeling poorly. Trader.
He was hospitalized for 16 days during the past 2 months for surgery (bowel obstruction) and treated with different antibiotics.

VentiMask (FiO2: 31%)Vital sign
BP: 120/70 mmHg
HR: 125 r
RR: 28 bpm
T: 38 °C
SpO2: 83% on RA
PSI RC: IV
Physical examination revealed decreased breathing sound on right
chest with fine moist rales on the lower lobe
In the ER:

What kind of treatment?

In the ward:
- Ceftriaxone 2 g iv + azithromycin 500 mg iv
Pneumonia screening: sputum/BAL; blood culture, urinary antigens, serology for atypical pathogens
D1 D2 D3
- Ceftriaxone 2 g iv + azithromycin 500 mg iv
18.600
7
12.500
12
10.420
6
WBC
CRP
T
Ab anti-Legionella pneumophila: negative
Swab: bacteria and fungi: neg
Urinary antigens LP and SP: negative
Blood culture: negative
Ab anti-Mycoplasma: IgG negative and IgM negative
Naso-pharyngeal swab DNA CP, MP, LP: negative
0.30 0.25 0.10PCT

D1 D2 D3
- Ceftriaxone 2 g iv + azithromycin 500 mg iv
18.600
7
12.500
12
10.420
6
WBC
CRP
T
0.30 0.25 0.10PCT
9.000
3
0.08
D4

….AND NOW?

DISCHARGED ON DAY 6












Pneumonia and Cardiovascular events PATHOPHYSIOLOGICAL MECHANISMS
Corrales-Medina. Lancet 2012


Which patients in hospital are at risk?
Lines andMedical devices
Burns
Renal dialysis
Transplantrecipients
Cancer
Post-surgery
High dependency
Elderly
Neonates
Hospital

HAP(SENTRY surveillance system - n=31,436)
Jones et al – CID 2010
Incidence, %
Pathogen All regions United States Europe Latin
America
Staphylococcus aureus 28.0 36.3 23.0 20.1Pseudomonas aeruginosa 21.8 19.7 20.8 28.2Klebsiella spp. 9.8 8.5 10.1 12.1Escherichia coli 6.9 4.6 10.1 5.5Acinetobacter spp. 6.8 4.8 5.6 13.3Enterobacter spp. 6.3 6.5 6.2 6.2Serratia spp. 3.5 4.1 3.2 2.4Stenotroph. maltophilia 3.1 3.3 3.2 2.3
Streptococcus pneumoniae 2.9 2.5 3.6 2.4
Haemophilus influenzae 2.7 2.5 3.7 1.3

MRSA trends, Europe
EARS-NET

MDR Gram-negatives causing pneumonia
Pseudomonas aeruginosa
Acinetobacter
Enterobacteriaceae
Stenotrophomonas maltophilia

2006 2007 2008 2009 2010 20110
5
10
15
20
25
30
35
40
EARS-NET
Pro
port
ion
%
Year
AMG
FQ
NEM
PIP
CAZ
Pseudomonas aeruginosa resistance trends, Italy
2005 2006 2007 2008 2009 2010 201105
101520253035404550
Pro
port
ion
%
Year
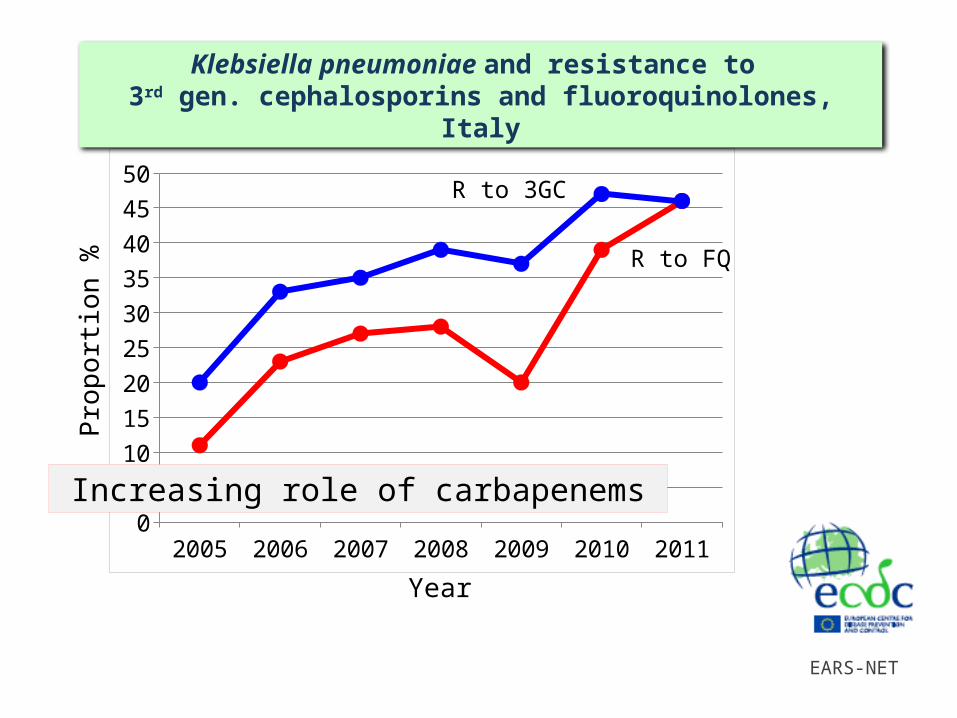
Klebsiella pneumoniae and resistance to 3rd gen. cephalosporins and fluoroquinolones, Italy
EARS-NET
R to 3GC
R to FQ
Increasing role of carbapenems

Giani et al – JCM 2009Santoriello et al – unpublished
Fontana et al – BMC Res Notes 2010Marchese et al – J Chemother 2010Ambretti et al – New Microb 2010Gaibani et al – Eurosurv 2011Mezzatesta et al – CMI 2011Agodi et al – JCM 2011Richter et al – JCM 2011Di Carlo et al – BMC Gastroenterol 2011Rossolini GM – unpublished
late 2008
The first reported cases of KPC-Kp
KPC-producing K. pneumoniae – the Italian epidemic
early 2011
AMCLI – CoSA CRE networkFrasson et al – JCM 2012ARISS – CoSA survey 2012
late 2012

AMCLI-CoSA – Italian national surveillance 2011
CRAB detected in ALL CENTERS
Nationwide cross-sectional survey, 2011(6 weeks / 25 centers / N=585 isolates)
Carbapenem-R Acinetobacter, Italy

C-02
C-19
C-01
C-25
C-09
C-13
C-16
C-23
C-21
C-08
C-20
C-17
C-11
C-14
C-12
C-05
C-03
C-15
C-07
C-06
C-04
C-24
C-18
C-22
C-10
0
10
20
30
40
50
60
70
80
90
100
CRAB proportion by center – Italian surveillance
Centers
CR
AB
pro
port
ion
(%
)
AMCLI-CoSA – Italian national surveillance 2011
Mean, 43%

CASE 3

Female, 86 y/o
She was referred to our ER because of a 7-day history of dyspnea. She also reported a history of recurrent urinary infections
Her past history was remarkable for:
- NIDDM associated with retinopathy
- Chronic vascular encephalopathy
- Essential hypertension
- Left knee joint prosthesis (25 years back)
She was on: aspirin, ibesartan, nifedipine, metformin, furosemide
She was a former worker. Non-smoker. Non-allergic.
She was admitted to the internal medicine department with a diagnosis of decompensated chronic heart failure.

AFTER 4 DAYSBP: 190/90 mmHg
HR: 115 bpm
RR: 26 bpm
T: 39 °C
SpO2: 88% in RA
Glucose: 369
Abnormal chest sounds (rales and rhonchi) were detected bilaterally in the lower lobes
EKG: sinusal rhythm; HR 115, PQ: 0.20, no modifications of ventricular reporalization


Your Diagnosis?

VentiMask (FiO2: 50%)
BP: 190/90 mmHg
HR: 115 bpm
RR: 26 bpm
T: 39 °C
SpO2: 88% in RA
Glucose: 369
Abnormal chest sounds (rales and rhonchi) were detected bilaterally in the lower lobes
EKG: sinusal rhythm; HR 115, PQ: 0.20, no modifications of ventricular reporalization

WHICH TREATMENT?

In the ward (Internal Medicine):
- Ceftriaxone 2 gr
- Levofloxacin 500 mg x 2 EV
Pneumonia screening: sputum/BAL; blood culture, urinary antigens, serology for atypical pathogens
D1 D2 D3
Ceftriaxone 2gr
22.220
19
18.700
18
17.400
18
WBC
CRP
T
Levofloxacin 500 q12
Ab anti-Legionella pneumophila: negative
Swab: bacteria and fungi: neg
Urinary antigens LP and SP: negative
Tracheal aspirate: GRAM POSITIVE
Blood culture: pending
Ab anti-Mycoplasma: IgG negative and IgM negative
Naso-pharyngeal swab DNA CP, MP, LP: negative
0.44 0.42 0.49PCT

WOULD YOU CHANGE?


Ceftriaxone 2gr
22.220
19
18.700
18
17.400
18
WBC
CRP
T
Levofloxacin 500 q12
0.44 0.42 0.49
Vancomycin 500 mg in 50 cc F at 5 ml/h
Stop
D1 D2 D3
PCT

Ceftriaxone 2gr
22.220
19
18.700
18
17.400
20
WBC
CRP
T
Levofloxacin 500 q12
0.44 0.42 ---
Vancomycin 500 mg in 50 cc F at 5 ml/h
12.800
14
0.28
11.000
11
0.21
11.550
12
0.20
11.400
13
0.20
D1 D2 D3 D4 D5 D6 D7
PCT

DAY 8:
Episode of ACPE with sudden dyspnea and hypoxemia. Good response with furosemide, nitroderivates and helmet CPAP.
On Day 8, once the episode of ACPE was treated, patient was on CPAP…
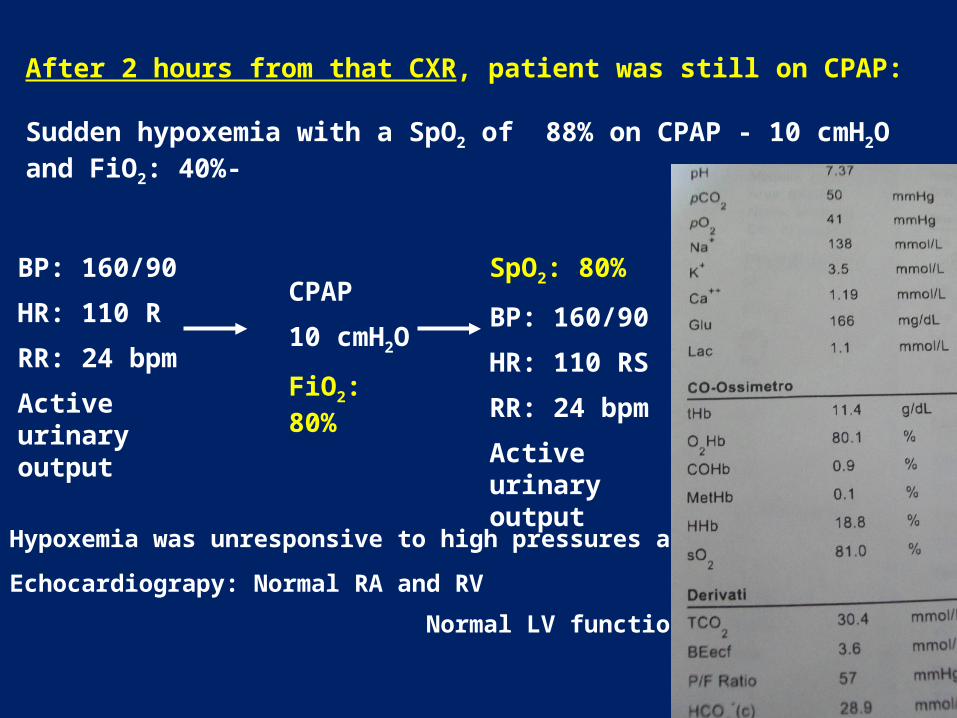
After 2 hours from that CXR, patient was still on CPAP:
Sudden hypoxemia with a SpO2 of 88% on CPAP - 10 cmH2O and FiO2: 40%-
BP: 160/90
HR: 110 R
RR: 24 bpm
Active urinary output
CPAP
10 cmH2O
FiO2: 80%
SpO2: 80%
BP: 160/90
HR: 110 RS
RR: 24 bpm
Active urinary output
Hypoxemia was unresponsive to high pressures and FiO2
Echocardiograpy: Normal RA and RV
Normal LV function


Because of the CXR findings, patient underwent Thorax CT scan:

Because of the CXR findings, patient underwent Thorax CT scan:

Levofloxacin 500 q12
Vancomycin 500 mg in 50 cc F at 5 ml/h
12.800
14
0.28
11.000
11
0.21
11.550
12
0.20
11.400
13
0.20
Blood was found during a bronchoscopy with a SpO2 75% 98%.
Patient was put on Ventimask 35%
Stop
Stop
Linezolid 600 mg q12 EV
Tobramycin EV
Imipenem 1 g q8 EV
D5 D6 D7 D8
WBC
CRP
T
PCT

EXITUS on DAY 10


HAP or VAP
Obtain lower respiratory tract sample for culture(quantitative or semiquantitative) & microscopy
Begin empiric antimicrobial therapy using algorithm and local microbiologic data (unless low clinical suspicion and
Negative microscopy of LRT sample)
Days 2 & 3: Check cultures & assess clinical response:(Temperature, WBC, CXR, Oxygenation, sputum purulence,
Haemodynamic changes and organ function)
Clinical Improvement at 48-72 hours?
Am J Respir Crit Care Med 2005;171:388-416

HAP, VAP
Clinical Improvement at 48-72 hours?
NO YES
Cultures - Cultures + Cultures - Cultures +
Search for otherPathogens,
Complications, Other Diagnosesor Other Sites of
infection
Adjust antibioticTherapy, search
For otherPathogens,
Complications Or other siesOf infection
ConsiderStoppingantibiotics
De-escalateAntibiotics, if
Possible.Treat selected
Patients for7-8 days and
reassess
Am J Respir Crit Care Med 2005;171:388-416

HAP, VAP
Late onset (5days) or risk factors for multidrug resistant pathogens
NO YES
Limited Spectrum
Ceftriaxone (1 x 2g) or Fluoroquinolone (Levofloxacin 1x750mg or Moxifloxacin 1x400mg) or
Ampicillin / sulbactam (3x3g) or
Ertapenem (1x1g)
Broad SpectrumAntipseudomonal cephalosporin (Ceftazidime 3x2g)orAntipseudomonal carbapenem (Imipenem/Cilastin 3x1g, Meropenem 3x1g)or-lactam/-lactamase inhibitor (Piperacillin/tazobactam 3x4.5g)
Plus
Antipseud fluoroquinolone (Ciprofloxacin 3x400mg, Levofloxacin 1x750mg) orAminoglycoside (Amikacin 15mg/kg/d divided bid, max 1.5g/d) (MRSA – linezolid (2x600mg) or vancomycin (2x1g initial, control blood levels))
Am J Respir Crit Care Med 2005;171:388-416


• The lack of initial improvement in PaO2/FiO2, along with an increase in the SOFA score, was the two clinical evolutionary findings that predicted mortality in a multivariate model.
• These feasible and low-cost variables should be evaluated in future trials to test interventions in patients with ICUAP.

Four Major Principles
1. Avoid inadequate treatment
2. Variable bacteriology between hospital sites
and over time
3. Avoid antibiotic overuse – accurate diagnosis and
pathogen directed therapy
4. Prevention strategies for modifiable risk factors
Am J Respir Crit Care Med 2005;171:388-416