Community acquired pneumonia workshop
136
ى عل لام س ل وا لاة ص ل م وا ي ح ر ل ا ن م ح ر ل ها ل ل ما س ب م ل س هو ي ل ع ه ل ل ىا ل ص مد ح م ا* دن ي س ن ي ل س ر م ل ا* رف5 ش ا ن ي ع م ح ها ي ح ص هو ل= ىا عل و
-
Upload
hiba-ashibany -
Category
Documents
-
view
263 -
download
2
Transcript of Community acquired pneumonia workshop

والسالم والصالة الرحيم الرحمن الله بسمصلى محمد سيدنا المرسلين اشرف علىاجمعين وصحبه آله وعلى وسلم عليه الله

Community acquired pneumonia
Dr. Ali Ashur TuatiAbu Setta chest hospital

Which of the following symptoms is not bad prognostic factor for CAP?
1-fever2-Pleuretic chest pain
3-Altered mental status4-Dyspnea

Which of the following clinical findings is not poor prognostic factor in CAP?
1-low temperature < 35 C2-High temperature >40 C3-Systolic BP < 100 mmHg
3-Pulse >125 bpm5-RR > 30 bpm

Which of the following lab. Results is not risk factor for severe CAP ?
1-Na < 130 mmol/L2-Glucose =/> 250 mg%
3-PaO2 < 60 mmHg4-CRP >150 mg/L
5-Hct < 30%
When you suspect about 60-70% of patients will have complete resolving of pneumonia radiologically?
1-1 week. 2-2 weeks.4-3 weeks 4-4 weeks5-6 weeks

Which drug should not be used for treatment of sCAP due Pseudomonas aeruginosa?
1-Piperacillin-tazobactam2- Ertapenem3-Cefepime 4-Imipenem/cilastatin 5-meropenem

Community acquired pneumonia“CAP”
Dr. Ali Ashur Tuati Abu Setta Chest Hospital

Definition

Epidemiological classification of pneumonia

Health care associated pneumonia
HCAP is defined as pneumonia that occurs in non-hospitalized patient with extensive healthcare contact, as
defined by one or more of the following :●Intravenous therapy, wound care, or intravenous
chemotherapy within the prior 30 days●Residence in a nursing home or other long-term care
facility●Hospitalization in an acute care hospital for two or more
days within the prior 90 days●Attendance at hospital or hemodialysis clinic within the
prior 30 days

Incidence of CAP




(Chest X ray PA view)

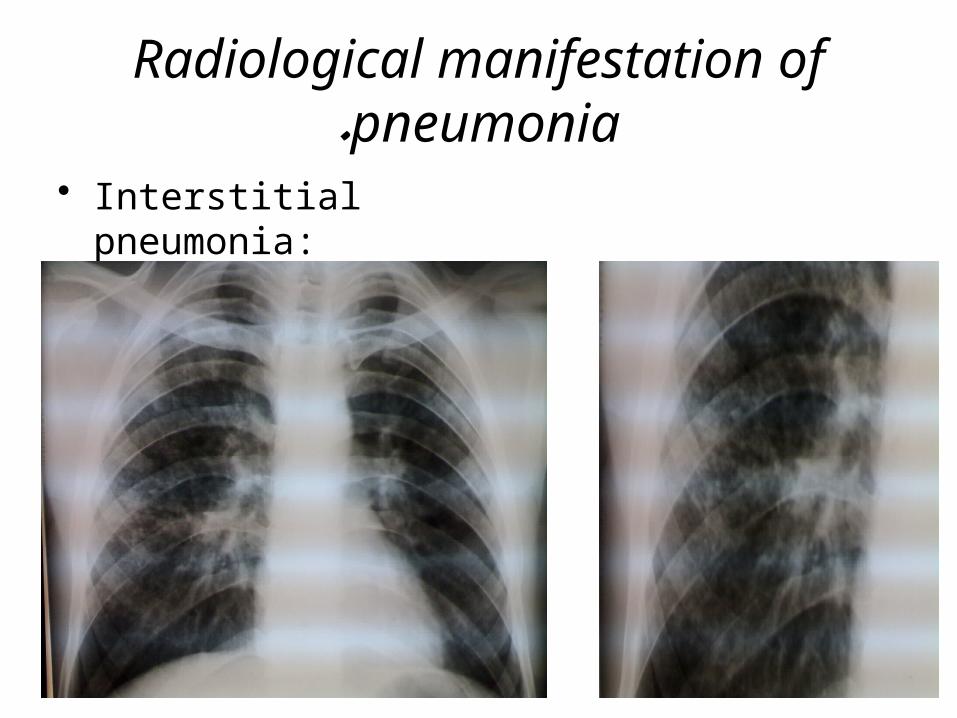
Radiological manifestation of pneumonia.
• Lobar air space pneumonia :

Radiological manifestation of pneumonia.
• Bronchopneumonia:
Radiological manifestation of pneumonia.
• Interstitial pneumonia:



Microbiological investigations in patients with CAP

Microbiological investigations in patients with CAP
All patients •Sputum: direct smear by Gram stain
and Ziehl–Neelsen stain. Culture and sensitivity testing
•Blood culture: frequently positive in pneumococc pneumonia
•Serology: acute and convalescent titers for: -Mycoplasma, -Chlamydia, -Legionella, -viral infections. -Pneumococcal Ag detection in serum or urine
•PCR: Mycoplasma can be detected from swab of oropharynx
Gram stain of sputum showing Gram-positivediplococci characteristic of Strep. pneumoniae (arrows).
Mycobacterium tuberculosis (stained red) in sputum

Severe community-acquired pneumonia “sCAP”
The previous tests plus consider: •Tracheal aspirate (TBAS), induced sputum, BAL ,
protected brush specimen (PBS) or percutaneous needle aspiration (PCNA). .Direct fluorescent antibody stain for Legionella and viruses
•Serology: .Legionella Ag in urine. .Pneumococcal Ag in sputum and blood. .Immediate IgM for Mycoplasma
•Cold agglutinins: positive in 50% of patients with Mycoplasma
Sputum direct fluorescent antibody stain showing Legionella infection.

Selected patients
•Throat/nasopharyngeal swabs: helpful in children or during influenza epidemic
•Pleural fluid: should always be sampled when present in more than trivial amounts, preferably with ultrasound (US) guidance

Identified Pathogens in CAP
Mandell LA, Bartlett JG, Dowell SF, et al: Update of practice guidelines for the management of community-acquired pneumonia in immunocompetent adults. Clin Infect Dis 2003;37:1405-1433.© 2002 The Cleveland Clinic Foundation.








Does hospital admission kills?
Multivariable analyses

Multivariable analyses
Different variables in different patients- Demographic
- Different comorbidities- Different in physical examinations
- Different in lab and radiological findings

Pneumonia severity index (PSI)



What is the limitation of PSI?

(1-)To many items in clinical practice
limitation

(2-)Young patients almost never reach high risk classes
limitation

Point totalRisk
Risk class
Recommended site of care
No predictors Low I Outpatient
≤ 70 Low II Outpatient
71 to 90 Low III
Inpatient (briefly)
91 to 130 Moderate IV
Inpatient
> 130 High V Inpatient
(3-)A prediction rule to identify low-risk patients with CPA
Pneumonia Severity Index limitation
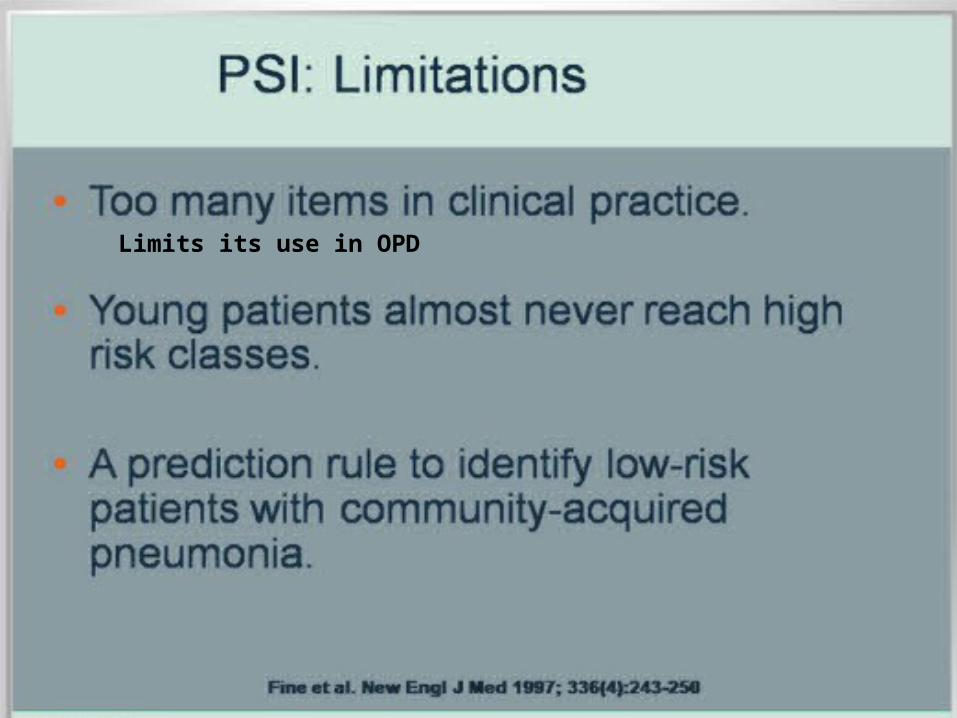
Limits its use in OPD

For all these reasons look for other practical scoring system for assessment of patient severity


Confusion Urea > 7 mmol/l Respiratory Rate: ≥ 30 /minute Blood pressure: 90/60 mmHg 65 years
IS THERE A SIMPLER WAY? CURB-65

QuestionnaireMental Test Score (10 points)
The following questions are put to the patient. Each question correctly answered scores 1 point. A score of 7-8 or less suggests cognitive impairment at the time of testing, although further and more formal tests are necessary to confirm a diagnosis of dementia, delirium or other causes of cognitive impairment.
References(1-)Hodkinson, HM (1972). "Evaluation of a mental test score for assessment of mental impairment in the elderly".
Confusion: Defined as a Mental Test Score of 8 or less, or new disorientation in person, place or time. (A urea of 7 mmol/L 20 mg/dL.)≅

Hospital CURB-65. *Defined as a Mental Test Score of 8 or less, or new disorientation in person, place or time. (A urea of 7 mmol/L 20 mg/dL.)≅
Severity scoring of CAP according to CURB-65



CRB-65

ConfusionRespiratory rate ≥ 30/min Blood pressure (SBP≤ 90 or DBP≤60)Age ≥ 65
0 1 or 2 3 or 4
Low Risk
mortality 1.2%
Intermediate Risk
mortality 8.13%
High Risk
mortality 31%
Severity scoring of CAP according to CRB-65
Likely suitable for home treatment
Consider hospital referral
Urgent hospital admission



Treatment of CAP

Shall we need to treat patient with antibiotic?




Hospital CURB-65. *Defined as a Mental Test Score of 8 or less, or new disorientation in person, place or time. (A urea of 7 mmol/L 20 mg/dL.)≅
Treatment plain according to -CURB-65

ConfusionRespiratory rate ≥ 30/min Blood pressure (SBP≤ 90 or DBP≤60)Age ≥ 65
0 1 or 2 3 or 4
Low Risk
mortality 1.2%
Intermediate Risk
mortality 8.13%
High Risk
mortality 31%
Treatment plain according to CRB-65
Likely suitable for home treatment
Consider hospital referral
Urgent hospital admission

Indications for referral to ITU
•CURB-65 score 4–5 or CRB-65 score 3-4 failing to respond rapidly to initial
management •Persisting hypoxia (PaO2 < 8 kPa (60
mmHg)) despite high concentrations of oxygen
•Progressive hypercapnia •Severe acidosis
•Circulatory shock •Reduced conscious level


Factors in empirical antibiotic choice for CAP

Empiric therapy

Risk factors for TB

Factors increasing the risk of TB
:Patient-related •Age (children > young adults < elderly)
•First-generation immigrants from high-prevalence countries
•Close contacts of patients with smear-positive pulmonary TB
•Overcrowding (prisons, collective dormitories); homelessness (doss houses and hostels)
•Chest radiographic evidence of self-healed TB •Primary infection < 1 year previously
•Smoking: cigarettes.

Factors increasing the risk of TB
Associated diseases:
•Immunosuppression: HIV, anti-TNF therapy, high-dose corticosteroids, cytotoxic agents
•Malignancy (especially lymphoma and leukaemia) •Type 1 diabetes mellitus
•Chronic renal failure •Silicosis
•Gastrointestinal disease associated with malnutrition( gastrectomy, jejuno-ileal bypass, cancer of the
pancreas, malabsorption) •Deficiency of vitamin D or A
•Recent measles: increases risk of child contracting TB

Most causative Pathogens in CAP
Mandell LA, Bartlett JG, Dowell SF, et al: Update of practice guidelines for the management of community-acquired pneumonia in immunocompetent adults. Clin Infect Dis 2003;37:1405-1433.© 2002 The Cleveland Clinic Foundation.


Mild CAP without risk factors CURB-65 = 0 or 1CRB-65 = 0



Risk factors for drug-resistant S. pneumoniae
Risk factors for drug-resistant S. pneumoniae in adults include:●Age >65 years
●Beta-lactam, macrolide, or fluoroquinolone therapy within the past 3 to 6 months
●Alcoholism●Medical comorbidities
●Immunosuppressive illness or therapy●Exposure to a child in a daycare center
Recent therapy or a repeated course of therapy with beta-lactams, macrolides, or fluoroquinolones are risk factors for pneumococcal resistance to the same class of antibiotic . Thus, an antimicrobial agent from an alternative class is preferred for a patient who has recently received one of these agents

750

Moderate CAP
CURB-65 = 2CRB-65 = 1, 2

- ertapenem
750

Severe CAPCURB-65 = 3,4,5,CRB-65 = 3,4

- ertapenem
750
severeIn patients without risk factors for or microbiologic evidence of Pseudomonas aeruginosa or MRSA
7-14
7-14
7-14
7-147-147-14
7-147-14
with

Recommendation for empiric initial antimicrobial treatment in patients with sCAP-admitted to ICU
●In patients with risk factors for or microbiologic evidence of Pseudomonas aeruginosa or MRSA
and Legionella spp.

Recommendation for empiric initial antimicrobial treatment in patients with sCAP-admitted to ICU
●In patients with risk factors for or microbiologic evidence of Pseudomonas aeruginosa

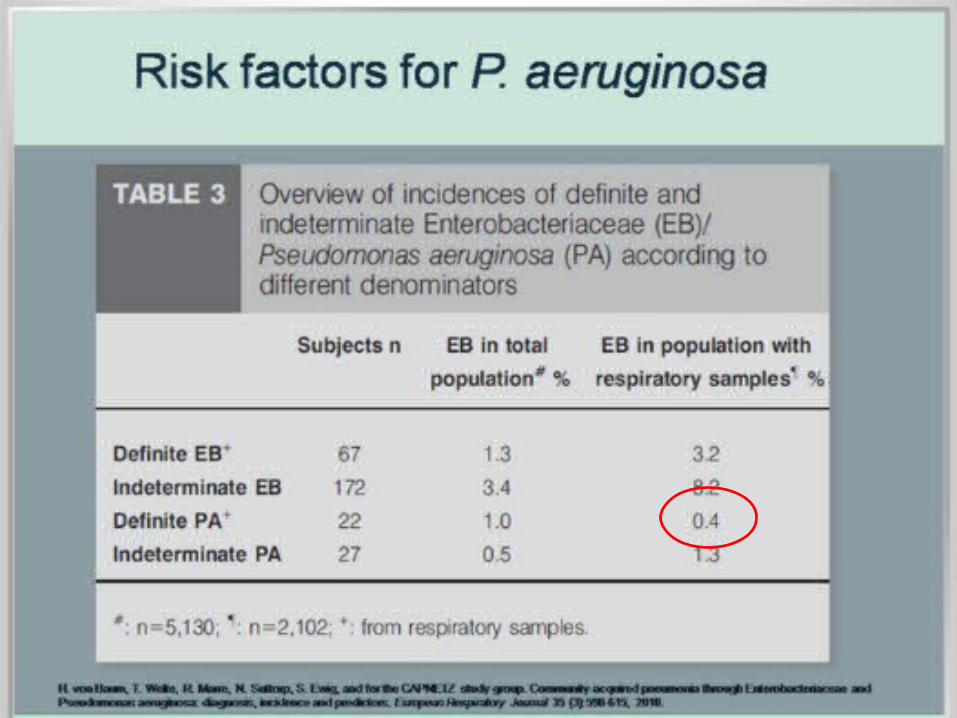


Risk factors for P. aerginosaThe ATS emphasizes certain modifying factors that increase the risk of infection with drug-resistant and unusual Risk factors for enteric gram-negative organisms are as follows: -recent antibiotic therapy, -underlying cardiopulmonary disease, -residence in a nursing home, and -multiple medical comorbidities. Risk factors for P aeruginosa are as follows: -structural lung disease such as bronchiectasis, -broad-spectrum antibiotic therapy that lasted for at least 7 days in the past month, -corticosteroid therapy with at least 10 mg of prednisone per day, and -malnutrition



8-15 days
8-15 days8-15 days

For penicillin-allergic patients
For penicillin-allergic patients, the type and severity of reaction should be assessed. The great majority of patients who are allergic to penicillin by skin testing can still receive cephalosporins (especially third-generation cephalosporins) or carbapenems. Skin testing is indicated in some situations. For penicillin-allergic patients, if skin test is positive or if there is significant concern to warrant avoidance of cephalosporin or carbapenem, options include: -aztreonam (2 g IV every six to eight hours) plus levofloxacin (750 mg daily) or -
aztreonam plus moxifloxacin plus an aminoglycoside .

-The fluoroquinolones may be administered orally when the patient is able to take oral medications. -The dose of levofloxacin is the same when given intravenously and orally, while the dose of ciprofloxacin is 750 mg orally twice daily.

Recommendation for empiric initial antimicrobial treatment in patients with sCAP-admitted to ICU
●In patients with risk factors for or microbiologic evidence of MRSA

Staphylococcus aureus
-Associated with debilitating illness and often preceded by influenza. -Radiographic features include multilobar shadowing, cavitation, pneumatocoeles and abscesses. -Dissemination to other organs may cause osteomyelitis, endocarditis or brain abscesses. -Mortality up to 30%

Cavities –Thin wall contain air only
Diagnostic criteria:- Thin wall
- Air only- Location of the lesion:
. On the surface of the lung1-Paraseptal emphysema
. In side parenchyma of the lung - Pneumatocele e.g. staph. infection
1-Paraseptal emphysema2-Pneumatocele

Pneumatocele
Pneumatocele: - Localized air collection , usually
with staph. pneumonia , but may occur with other types of pneumonias .
- Extension of inflammatory exudate into the lesion may cause formation
of air-fluid level. - More common than true lung
abscess

MRSA risk factorsCommunity associated MRSA — You can pick up MRSA outside the hospital, especially if you:
●Have skin trauma (eg, "turf burns," cuts, or sores) ●Are an athlete
●Shave or wax to remove body hair, particularly of the armpits and groin ●Have tattoos or body piercing
●Have physical contact with a person who has draining cut or sore or is carrier of MRSA
●Share personal items or equipment that is not cleaned or laundered between users (such as towels or protective sport pads)
Community-associated MRSA infections may occur more commonly in certain populations, such as daycare centers, prisons, in the military, or in athletes who play on team. Spread of MRSA within households is
common .

Methicillin-resistant Staphylococcus aureus (MRSA)
Methicillin-resistant Staphylococcus aureus (MRSA)• Vancomycin 15 mg/kg IV q12h for 7-14d
or• Linezolid 600mg IV or PO q12h for 7-14d
or• Telavancin 10mg/kg IV once daily for 7-21d
(reserved for use when alternative treatments are not suitable)

Recommendation for empiric initial antimicrobial treatment in patients with sCAP-admitted to ICU
●In patients with risk factors for or microbiologic evidence of Legionella spp.

Legionella pneumophila
-Middle to old age. -Local epidemics around contaminated source, e.g. cooling systems in hotels, hospitals.
-Person-to-person spread unusual. Some features more common, e.g. headache, confusion, malaise, myalgia, high fever and vomiting and diarrhoea. -Laboratory abnormalities include hyponatraemia, elevated liver enzymes, hypoalbuminaemia and elevated creatine kinase. -Risk factors: Smoking, corticosteroids, diabetes, chronic kidney disease increase risk

Legionella pneumophila
• Legionella pneumophila• Levofloxacin 750 mg IV q24h, then 750
mg/day PO for 7-14d or
• Moxifloxacin 400 mg IV or PO q24h for 7-14d or
• Azithromycin 500 mg IV q24h for 7-10d

New antimicrobials in CAP
• Tigecycline• Ceftaroline

New antimicrobials in CAP
• Tigecycline was approved by the FDA in 2009 for adults with CAP caused by: -S pneumoniae (penicillin-susceptible isolates),
including cases with concurrent bacteremia, -H influenza (beta-lactamase-negative isolates), -Legionella pneumophila.• In a study conducted to evaluate the efficacy of
tigecycline versus levofloxacin in hospitalized patients with CAP, tigecycline achieved cure rates similar to those of levofloxacin in hospitalized patients with CAP. For patients with risk factors, tigecycline provided generally favorable clinical outcomes.

New antimicrobials in CAP
• Although Tigecycline is indicated for CAP, data from clinical trials suggest a high incidence of adverse events, particularly gastrointestinal adverse effects >10% (nausea , vomiting , diarrhea), which may limit its use.
• Dose in CAP:• Tigecycline 100 mg IV loading dose, then 50
mg IV q12h for 7-14 d

New antimicrobials in CAP
• Ceftaroline fosamil is a parenteral cephalosporin antibacterial that was approved by the FDA in 2010 for the treatment of adults with CAP caused by: -S pneumoniae, including cases with concurrent bacteremia; -S aureus (methicillin-susceptible isolates only); -H influenza; -K pneumonia; Klebsiella oxytoca; -E coli.
• Ceftaroline, the active form of ceftaroline fosamil, has broad-spectrum in vitro activity against common causative gram-positive and gram-negative bacteria, including MRSA. However, there are no clinical data supporting the use of ceftaroline fosamil for MRSA pneumonia.
New antimicrobials in CAP• Ceftaroline fosamil is included in Joint Commission pneumonia
core measures as one of the recommended beta-lactam antibiotics for CAP in immunocompetent, non-ICU patients.
• Dose:• Ceftaroline for CAP
600 mg IV q12h; infuse over 1 h for 5-7 days • Side effects : The most common adverse reactions occurring in > 2% of patients : -Diarrhea -Nausea -Rash

Ertapenem

The β-lactam family of antibiotics
Ceftriaxone 3rdTicarcillin
Ceftazidime 3rdMezlocillin
Cefotaxime 3rdCarbenicillin
ErtapenemCefmetazoleCefuroxime 2ndAmpicillin
MeropenemCefotetanCefamandole 2ndMethicillin
AztreonamImipenemCefoxitinCephalothin 1stBenzyl-penicillin
MonobactamsCarbapenemsCephamycinsCephalosporinsPenicillins
Cefepime 4th

Ertapenem• Ertapenem is effective against Gram-negative and
Gram-positive bacteria. It is not active against MRSA, ampicillin-resistant enterococci, Pseudomonas aeruginosa, or Acinetobacter species. Ertapenem has useful activity against anaerobic bacteria.
• Note: staph. (MRSA) and Enterococcus spp. are
resistant to ertapenem.
Ertapenem • Ertapenem is marketed by Merck as a first-line treatment for
community-acquired infections.• Note: It should not be used as empirical treatment for hospital-
acquired infections (HAP) because of its lack of activity against Pseudomonas aeruginosa.
• In practice, it is reserved primarily for use against
Extended spectrum beta-lactamase (ESBL)-producing and high level AmpC-type beta lactamase producing Gram- negative bacteria (e.g. Klebsilla , and E. coli).

Ertapenem
Dosage• Ertapenem is dosed as: 1
g given by intravenous injection over 30 minutes, or 1 g diluted with 3.2 ml of 1% lidocaine given intramuscularly.
• There is no oral preparation of ertapenem available.
• Ertapenem cannot be mixed with glucose.
Ertapenem
• Side-effects• There are a few adverse effects of ertapenem like confusion
and headache, which may worsen to convulsions and seizures. The only absolute contra-indication is a previous anaphylactic reaction to ertapenem or other β-lactam antibiotic. There are no studies done in pregnant women, so the manufacturers cannot comment on its safety in pregnancy. Ertapenem is not recommended for children under 3 months of age and children with meningitis.
• Clostridium difficile colitis has been associated with its use.

Prevention• More people die from pneumococcal infections (an estimated 40,000
annually in the United States) than from any other vaccine preventable disease.
• PPV23 is recommended for: (1)- all adults ≥65 years of age, (2)-all patients with asplenia , and (3)- in younger patients <64 years of age with a number of conditions that increase the risk of invasive pneumococcal disease
-Adults who have been diagnosed with invasive pneumococcal disease should also be vaccinated because infection with one serotype does not necessarily provide protection against other serotypes. And that’s why IDSA states that patients can be given pneumococcal vaccine immediately after an episode of pneumonia. • A single revaccination is recommended in:
(1)-adults ≥65 years of age if they were vaccinated more than 5 years previously at a time when they were <65 years of age, and (2)-in immunocompromised patients five years or more after the first dose.

Evaluation of community-acquired pneumonia.
Mild Moderate Severe
Assess for risk factors

Conclusions
-CAP is a common disease in community. -Diagnosis is made by chest x ray and signs and symptoms of pulmonary infection.
-Follow up be observed best by CRP.-Severity is assessed by CRB-65 score and ATS criteria.
-Antibiotic therapy lower mortality-Antibiotic is tailored according to risk factors and
aetiologies .-Don’t use Ertapenem for treatment of pneumonia due to
MRSA, Pseudomonas aeruginosa, or Acinetobacter species.-Most risk factors for pseud. aerug. Infection are enteral
tube feeding and chronic respiratory diseases .

Conclusions-Using a guidelines, we can simplify the treatment regimens. -For
outpatients, monotherapy with either a β-lactam, a macrolide antibiotic, doxycycline, or a fluoroquinolone antibiotic should be sufficient.
-For patients requiring admission to a GMF or with the absence of risk
factors for DRSP or infection with enteric gram-negative organisms, the recommended treatment is with a combination of a β-lactam plus a macrolide or monotherapy with a fluoroquinolone antibiotic.
-For severely ill patients with CAP (eg, patients requiring admission to the
ICU or having risk factors for P aeruginosa infection), treatment should always be with a combination of at least two drugs and the drugs should be appropriately selected for the suspected organism. Examples include a β-lactam plus a macrolide antibiotic, a β-lactam plus a fluoroquinolone antibiotic, and a β-lactam plus an aminoglycoside plus a macrolide
antibiotic . GMW=general medical floor


Thank you


For penicillin-allergic patients
For penicillin-allergic patients, the type and severity of reaction should be assessed. The great majority of patients who are allergic to penicillin by skin testing can still receive cephalosporins (especially third-generation cephalosporins) or carbapenems. If there is a history of mild reaction to penicillin (not an IgE-mediated reaction, Stevens Johnson syndrome, or toxic epidermal necrolysis), it is reasonable to administer a cephalosporin or carbapenem using simple graded challenge (eg, give 1/10 of dose, observe closely for one hour, then give remaining 9/10 of dose, observe closely for one hour). Skin testing is indicated in some situations. For penicillin-allergic patients, if skin test is positive or if there is significant concern to warrant avoidance of cephalosporin or carbapenem, options include: -aztreonam (2 g IV every six to eight hours) plus levofloxacin (750 mg daily) or -aztreonam plus
moxifloxacin plus an aminoglycoside .


Empiric therapy

Factors increasing the risk of TB
:Patient-related •Age (children > young adults < elderly)
•First-generation immigrants from high-prevalence countries
•Close contacts of patients with smear-positive pulmonary TB
•Overcrowding (prisons, collective dormitories); homelessness (doss houses and hostels)
•Chest radiographic evidence of self-healed TB •Primary infection < 1 year previously
•Smoking: cigarettes and bidis (Indian cigarettes made of tobacco wrapped in temburini leaves)

MRSA diagnosis:-People with skin infections can be tested for
MRSA with a culture. Results of the test are usually available in 48 to 72 hours.
-People with infections of the lung, bone, joint, or other internal areas usually require blood tests as well as imaging studies (eg, x-ray, CT scan, echocardiogram).

New antimicrobials in CAP• Ceftaroline fosamil is included in Joint Commission pneumonia
core measures as one of the recommended beta-lactam antibiotics for CAP in immunocompetent, non-ICU patients.
• Dose:• Ceftaroline for CAP 600 mg IV q12h; infuse over 1 h for 5-7 days • Side effects The most common adverse reactions occurring in > 2% of patients receiving ceftaroline :• Diarrhea• Nausea• Rash
Dose adjustment in Renal Impairment-CrCl 31-50 mL/min: 400 mg IV q12h -CrCl 15-30 mL/min: 300 mg IV q12h
-ESRD (including hemodialysis): 200 mg IV q12h

Ertapenem• Ertapenem is effective against Gram-negative and Gram-positive
bacteria. It is not active against MRSA, ampicillin-resistant enterococci, Pseudomonas aeruginosa, or Acinetobacter species. Ertapenem has useful activity against anaerobic bacteria.
Ertapenem is active against most isolates of the following micro-organisms : -Aerobic and facultative gram-positive microorganisms: • Note: staph. (MRSA) and Enterococcus spp. are resistant to
ertapenem. -Aerobic and facultative gram-negative microorganisms: .E. coli, Haemophilus influenzae (Beta-lactamase-negative isolates only), Klebsiella pneumoniae,Moraxella catarrhalis, Proteus mirabilis,

Ertapenem -Anaerobic microorganisms: • Ertapenem is marketed by Merck as a first-line treatment for
community-acquired infections.• Note: It should not be used as empirical treatment for hospital-
acquired infections (HAP) because of its lack of activity against Pseudomonas aeruginosa. In practice, it is reserved primarily for use against Extended spectrum beta-lactamase (ESBL)-producing and high level AmpC-type beta lactamase producing Gram- negative bacteria (e.g. Klebsilla , and E. coli).

Ertapenem
• Side-effects• There are a few adverse effects of ertapenem like
confusion and headache, which may worsen to convulsions and seizures. The only absolute contra-indication is a previous anaphylactic reaction to ertapenem or other β-lactam antibiotic. There are no studies done in pregnant women, so the manufacturers cannot comment on its safety in pregnancy. In 2006, Ertapenem became approved for pediatric use in certain infections. Ertapenem is not recommended for children under 3 months of age and children with meningitis.
• Clostridium difficile colitis has been associated with its use.

Mild CAP with risk factors
•Cigarette smoking •Upper respiratory tract infections
•Alcohol •Corticosteroid therapy
•Old age •Recent influenza infection
•Pre-existing lung disease •HIV
•Indoor air pollution

MRSA symptoms:-Most people infected with community-associated
MRSA (CA-MRSA) have signs of a skin infection. The skin may have a single raised red lump that is tender, or carbuncle. The center of the raised area may ooze pus.
-It is also possible to develop an infection in areas other than the skin if the bacteria enter the bloodstream through the skin e.g. on a heart valve, in a bone, joint, or the lungs, or around devices (such as an IV line, pacemaker, or replacement joint). In these situations, symptoms may include fever and fatigue, as well as pain or swelling in the infected area.

MRSA diagnosis:-People with skin infections can be tested for
MRSA with culture.-People with infections of the lung, bone, joint,
or other internal areas usually require blood tests as well as imaging studies (eg, x-ray, CT scan, echocardiogram).

The ATS emphasizes certain modifying factors that increase the risk of infection with drug-resistant and unusual pathogens.7 Risk factors for drug-resistant Streptococcus pneumoniae (DRSP) include age greater than 65 years, β-lactam therapy within the past 3 months, immunosuppression (either as the result of an illness or induced by treatment with corticosteroids), multiple medical comorbidities, alcoholism, and exposure to a child in a day care center.7 Risk factors for enteric gram-negative organisms are as follows: recent antibiotic therapy, underlying cardiopulmonary disease, residence in a nursing home, and multiple medical comorbidities.7 Risk factors for P aeruginosa are as follows: structural lung disease such as bronchiectasis, broad-spectrum antibiotic therapy that lasted for at least 7 days in the past month, corticosteroid therapy with at least 10 mg of prednisone per day, and malnutrition

Prevention• Prevention of CAP infection is mainly with the use of a approved vaccine,
which is about 60% effective in preventing bacteremia in immunocompetent adults with pneumococcal infections.
• The vaccine PPV23 should be given routinely to: -patients older > 65 years and to
-all patients with asplenia. -The vaccine is also recommended for patients aged or < 64 years if they have certain coexisting illnesses. Revaccination is recommended for: -patients older > 65 years who initially received the vaccine more > 5 years earlier and the initial vaccine was administered at age less < 65 years.-If the initial vaccine was given at age greater > 65 years, then repeated vaccination is not indicated.
The IDSA states that patients can be given the pneumococcal vaccine immediately after an episode of pneumonia , because infection with one serotype does not necessarily provide protection against other serotypes.

Treatment of CAP

Recommendation for empiric initial antimicrobial treatment in patients with sCAP-admitted to ICU
Empiric therapy — Patients requiring admission to an ICU are more likely to have risk factors for resistant pathogens, including community-associated MRSA and
Legionella spp.
● In patients without risk factors for or microbiologic evidence of Pseudomonas aeruginosa or MRSA, use: -intravenous combination therapy with potent anti-pneumococcal beta-lactam .ceftriaxone 1 to 2 g daily, .cefotaxime 1 to 2 g every eight hours, or .ampicillin-sulbactam 1.5 to 3 g every six hours.
plus -either an advanced macrolide
(azithromycin 500 mg daily) or respiratory fluoroquinolone (levofloxacin 750 mg daily or moxifloxacin 400 mg daily) .
Although the optimal doses of the beta-lactams have not been studied adequately, use the higher doses, at least initially, until the minimum inhibitory concentrations
(MICs) against possible isolates (eg, Streptococcus pneumoniae) are known .

Confusion: Defined as a Mental Test Score of 8 or less, or new disorientation in person, place or time. (A urea of 7 mmol/L 20 mg/dL.)≅
CURB-65

QuestionnaireMental Test Score (10 points)
The following questions are put to the patient. Each question correctly answered scores 1 point. A score of 7-8 or less suggests cognitive impairment at the time of testing, although further and more formal tests are necessary to confirm a diagnosis of dementia, delirium or other causes of cognitive impairment.
References(1-)Hodkinson, HM (1972). "Evaluation of a mental test score for assessment of mental impairment in the elderly".