
Phase I study of the investigational anti-guanylyl cyclase...
39
1 156699_2_art_file_3450457_h5mfx3.docx Phase I study of the investigational anti-guanylyl cyclase antibody– drug conjugate TAK-264 (MLN0264) in adult patients with advanced gastrointestinal malignancies Authors: Khaldoun Almhanna, 1 Thea Kalebic, 2 Cristina Cruz, 3 Jason E. Faris, 4 David P. Ryan, 4 JungAh Jung, 2 Tim Wyant, 2 Adedigbo A. Fasanmade, 2 Wells Messersmith, 5 * Jordi Rodon 3 * Author affiliations: 1 Department of Gastrointestinal Oncology, Moffitt Cancer Center, Tampa, FL, USA; 2 Millennium Pharmaceuticals, Inc., a wholly owned subsidiary of Takeda Pharmaceutical Company Limited, Cambridge, MA, USA; 3 Vall d’Hebron Institute of Oncology, Vall d’Hebron University Hospital and Universitat Autònoma de Barcelona, Barcelona, Spain; 4 Hematology/Oncology, Massachusetts General Hospital Cancer Center, Boston, MA, USA; 5 Division of Medical Oncology, University of Colorado Cancer Center, Aurora, CO, USA * Co-senior authors AACR member: Jordi Rodon Ahnert #128159 Running title [60 characters max, including spaces; currently 49]: TAK-264 in advanced gastrointestinal malignancies Keywords from pull-down list of terms (2-10): Research. on July 14, 2018. © 2016 American Association for Cancer clincancerres.aacrjournals.org Downloaded from Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474
Transcript of Phase I study of the investigational anti-guanylyl cyclase...
1 156699_2_art_file_3450457_h5mfx3.docx
Phase I study of the investigational anti-guanylyl cyclase antibody–
drug conjugate TAK-264 (MLN0264) in adult patients with advanced
gastrointestinal malignancies
Authors:
Khaldoun Almhanna,1 Thea Kalebic,2 Cristina Cruz,3 Jason E. Faris,4 David P.
Ryan,4 JungAh Jung,2 Tim Wyant,2 Adedigbo A. Fasanmade,2 Wells Messersmith,5*
Jordi Rodon3*
Author affiliations:
1Department of Gastrointestinal Oncology, Moffitt Cancer Center, Tampa, FL, USA;
2Millennium Pharmaceuticals, Inc., a wholly owned subsidiary of Takeda
Pharmaceutical Company Limited, Cambridge, MA, USA; 3Vall d’Hebron Institute of
Oncology, Vall d’Hebron University Hospital and Universitat Autònoma de Barcelona,
Barcelona, Spain; 4Hematology/Oncology, Massachusetts General Hospital Cancer
Center, Boston, MA, USA; 5Division of Medical Oncology, University of Colorado
Cancer Center, Aurora, CO, USA
*Co-senior authors
AACR member: Jordi Rodon Ahnert #128159
Running title [60 characters max, including spaces; currently 49]:
TAK-264 in advanced gastrointestinal malignancies
Keywords from pull-down list of terms (2-10):
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474

2 156699_2_art_file_3450457_h5mfx3.docx
Phase I-III trials_Gastrointestinal cancers: colorectal; Phase I-III
trials_Gastrointestinal cancers: stomach; Phase I-III trials_Gastrointestinal cancers:
other; Phase I-III trials_Pancreatic cancer; Antibody immunotherapy; New targets;
Novel antitumor agents; Antibodies/immunoconjugates
User-defined key words (optional, up to 3):
Guanylyl cyclase C; antibody–drug conjugate
Financial support:
This study was funded by Millennium Pharmaceuticals Inc., a wholly owned
subsidiary of Takeda Pharmaceutical Company Limited.
Corresponding author:
Khaldoun Almhanna
Department of Gastrointestinal Oncology, Moffitt Cancer Center, 12902 Magnolia
Drive, Tampa, FL 33612, USA
E-mail: [email protected]
Tel: (813) 745-3636. Fax: (813) 745-7229
Disclosures of conflicts of interest:
KA has received honoraria from Genentech and Lilly, and served in a consulting or
advisory role for Lilly and on a speakers’ bureau for Genentech.
TK, JJ, TW, and AF are full-time employees of Millennium Pharmaceuticals, Inc., a
wholly owned subsidiary of Takeda Pharmaceutical Company Limited.
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474

3 156699_2_art_file_3450457_h5mfx3.docx
CC has received travel, accommodations, or expenses from Millennium
Pharmaceuticals, Inc.
JEF has no conflicts of interest to disclose.
DPR has no conflicts of interest to disclose.
WM has received research funding from Millennium Pharmaceuticals, Inc., a wholly
owned subsidiary of Takeda Pharmaceutical Company Limited.
JR has no conflicts of interest to disclose.
Journal: Clinical Cancer Research. Category of manuscript: Cancer Therapy:
Clinical. Abstract word count: 250 words [max 250]. Statement of translational
relevance: 150 words [Max 120-150]. Word count: 4326 [max 5000].
Tables/figures: 6 (max 6). References: 37 [Max 50].
ClinicalTrials.gov identifier: NCT01577758.
Suggested reviewers (2–5 required):
1. Steven J. Cohen, MD, Fox Chase Cancer Center, Philadelphia, PA, email:
2. Bert O'Neil, MD, Indiana Cancer Pavilion, Indiana University, Indianapolis, IN,
email: [email protected] / [email protected]
3. Tanios Bekaii-Saab, MD, The Ohio State University Comprehensive Cancer
Center, Columbus, OH, email: [email protected] / bekaii-
4. Anthony W. Tolcher, MD, FRCP(C), South Texas Accelerated Research
Therapeutics (START), San Antonio, TX, email: [email protected]
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474

4 156699_2_art_file_3450457_h5mfx3.docx
Abstract
Purpose: To assess the safety, tolerability, and preliminary antitumor activity of the
investigational anti-GCC antibody-drug conjugate TAK-264 (formerly MLN0264) in
adult patients with advanced gastrointestinal malignancies.
Experimental Design: Adult patients with GCC-expressing gastrointestinal
malignancies (H-score ≥10) were eligible for inclusion. TAK-264 was administered as
a 30-minute IV infusion once every 3 weeks for up to 17 cycles. Dose escalation
proceeded using a Bayesian continual reassessment method. At the maximum
tolerated dose (MTD), 25 patients with metastatic colorectal cancer (mCRC) were
enrolled in a prespecified dose-expansion cohort.
Results: 41 patients were enrolled, including 35 (85%) with mCRC. During dose
escalation (0.3-2.4 mg/kg), 4 of 19 patients experienced dose-limiting toxicities of
grade 4 neutropenia; the MTD was determined as 1.8 mg/kg. Patients received a
median of 2 cycles of TAK-264 (range 1-12); 9 received ≥4 cycles. Common drug-
related adverse events (AEs) included nausea and decreased appetite (each 41%),
fatigue (32%), diarrhea, anemia, alopecia, and neutropenia (each 27%); grade ≥3
AEs included neutropenia (22%), hypokalemia, and febrile neutropenia (each 7%).
Peripheral neuropathy was reported in 4 (10%) patients. Pharmacokinetic data
showed approximately dose-proportional systemic exposure and a mean plasma
half-life of around 4 days, supporting the dosing schedule. Overall, 39 patients were
response-evaluable; 3 experienced durable stable disease and 1 with gastric
adenocarcinoma had a partial response. GCC expression did not appear to correlate
with treatment duration.
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474

5 156699_2_art_file_3450457_h5mfx3.docx
Conclusions: These findings suggest that TAK-264 has a manageable safety
profile, with preliminary evidence of potential antitumor activity in specific
gastrointestinal malignancies. Further investigation is underway.
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474

6 156699_2_art_file_3450457_h5mfx3.docx
Statement of translational relevance (Max 120-150 words):
The use of antibody–drug conjugates (ADCs) to target specific antigens preferentially
expressed on cancer cells is a feasible and active treatment approach in Hodgkin
lymphoma, anaplastic large cell lymphoma, and HER2-positive breast cancer, with
multiple ADCs under investigation in other lymphomas and solid tumors. ADCs
comprise a monoclonal antibody, a linker, and a cytotoxic small-molecule drug. For
gastrointestinal cancers, the transmembrane cell surface receptor guanylyl cyclase C
(GCC) has been identified as a potential target for a monoclonal antibody, being
expressed in 60-70% of pancreatic, gastric, and esophageal cancers and 95% of
primary and metastatic colorectal cancer. This first-in-human phase 1 study
investigated TAK-264, a novel investigational ADC targeting GCC, in adult patients
with advanced, GCC-expressing gastrointestinal malignancies. Results demonstrated
a manageable safety profile at the maximum tolerated dose and preliminary evidence
of antitumor activity and early signs of clinical benefit in patients with pancreatic,
esophageal, and gastric carcinoma.
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474
7 156699_2_art_file_3450457_h5mfx3.docx
Introduction
Monoclonal antibodies are established as anticancer therapies in a number of
different malignancies. Recently, antibody-drug conjugates (ADCs) have been
approved, and several more are being investigated, for various types of cancer.
ADCs are novel targeted agents composed of a monoclonal antibody, a linker, and a
cytotoxic small-molecule drug (1, 2). The monoclonal antibody is targeted to a
specific antigen preferentially expressed on cancer cells; the cytotoxic drug is
released upon internalization (1). There are two ADCs currently approved:
brentuximab vedotin for Hodgkin lymphoma and anaplastic large cell lymphoma (3-
6) and ado-trastuzumab emtansine for HER2-positive breast cancer (7).
Brentuximab vedotin is composed of an anti-CD30 antibody, a valine-citrulline
protease-cleavable linker, and the potent microtubule-disrupting agent monomethyl
auristatin E (MMAE) (5, 6). It has demonstrated substantial efficacy in pivotal phase 2
studies, including overall response rates of 75% (34% complete remission) in
relapsed/refractory Hodgkin lymphoma and 86% (57% complete remission) in
relapsed/refractory systemic anaplastic large cell lymphoma (4, 6). Brentuximab
vedotin received accelerated approval by the FDA in 2011 and conditional approval
in Europe in 2012 for patients with relapsed or refractory Hodgkin lymphoma and
anaplastic large cell lymphoma (8, 9). Other ADCs are in development based on the
same linker/drug technology, including polatuzumab vedotin and pinatuzumab
vedotin (targeting CD79b and CD22, respectively), both of which are in phase 2
development for the treatment of diffuse large B-cell lymphoma and follicular
lymphoma (10). Ado-trastuzumab emtansine is composed of the anti-HER2 antibody
trastuzumab connected via a stable thioether linker to the potent antimicrotubule
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474

8 156699_2_art_file_3450457_h5mfx3.docx
agent derivative of maytansine 1, an inhibitor of microtubule dimerization (11, 12). It
was approved in the US and Europe in 2013 for patients with advanced or metastatic
HER2-positive breast cancer (13, 14).
Exploring the therapeutic potential of ADCs in gastrointestinal cancers is of
significant interest, as they are a leading cause of cancer-related deaths; colorectal,
pancreatic, and gastric cancer had the second-, fourth-, and fourteenth-highest
estimated rates of cancer-related deaths in the USA in 2015 (15). One potential
target is the transmembrane cell surface receptor guanylyl cyclase C (GCC), which is
normally expressed on intestinal epithelial cells but not on extragastrointestinal
tissues (16, 17). In primary and metastatic tumors derived from intestinal epithelial
cells, GCC expression is maintained during neoplastic progression (16, 18). GCC is
expressed in 60-70% of pancreatic, gastric, and esophageal cancers (19-21) and
95% of primary and metastatic colorectal cancer (mCRC) (16, 18, 22-24).
Systemically delivered GCC-targeting agents are expected to be preferentially
delivered to GCC receptors in tumor tissue, while leaving normal tissues unaffected,
as GCC is expressed on the apical side of epithelial tight junctions (10, 16, 23, 25,
26). Access to GCC receptors is enabled in tumor tissues as a result of disrupted cell
polarity, altered tight junction architecture, and disruption of its apical localization (16,
18, 22, 24). TAK-264 (formerly MLN0264) is a novel ADC consisting of a fully human
IgG1 monoclonal anti-GCC antibody conjugated via a protease-cleavable linker to
MMAE. Following binding to GCC, TAK-264 is internalized and transported to
lysosomes where MMAE is released and binds to microtubules, leading to cell cycle
arrest and apoptosis. TAK-264 has been investigated in vivo in animal models of
gastrointestinal tumors, including GCC-expressing human colorectal cancer
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474
9 156699_2_art_file_3450457_h5mfx3.docx
xenografts and pancreatic cancer xenograft models, demonstrating selective binding
and internalization into GCC-expressing tumor cells and antitumor activity (27, 28).
This phase 1, first-in-human study assessed the safety and tolerability, dose-limiting
toxicities (DLTs), maximum tolerated dose (MTD), pharmacokinetics, and preliminary
antitumor activity of TAK-264 in adult patients with advanced, GCC-expressing
gastrointestinal malignancies.
Patients and Methods
Patients
Patients aged ≥18 years diagnosed with a GCC-expressing gastrointestinal
malignancy (H-score ≥10, derivation described below), for whom standard treatment
was no longer effective or did not offer curative or life-prolonging potential, were
eligible. Eligible malignancies included, but were not limited to, mCRC, gastric
carcinoma, esophageal carcinoma, small intestine cancer, pancreatic cancer, and
unknown primary malignancies. Patients should have progressed to standard-of-care
therapies in all cases. For the prespecified expansion cohort, only patients with
mCRC were eligible. Patients required: measurable disease per Response
Evaluation Criteria in Solid Tumors (RECIST 1.1); Eastern Cooperative Oncology
Group (ECOG) performance status 0 or 1; life expectancy of ≥12 weeks; adequate
bone marrow (absolute neutrophil count [ANC] ≥1500 cells/mm3; platelet count
≥100,000/mm3), hepatic (total bilirubin ≤1.5 X upper limit of normal [ULN]; serum
alanine or aspartate aminotransferase [ALT/AST] ≤2 X ULN; serum albumin ≥3.0
g/dL), and renal (serum creatinine ≤1.5 X ULN and/or calculated creatinine clearance
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474

10 156699_2_art_file_3450457_h5mfx3.docx
≥60 mL/min) function. Patients had to have completed prior chemotherapy,
immunotherapy, or radiotherapy ≥4 weeks prior to enrollment, and to have available
archived or fresh tumor tissue. Patients were excluded if they had: any comorbidities
that in the view of the treating physician rendered the patient at high risk from
treatment complications; known infection or inflammatory bowel disease; history of
another primary malignancy not in remission for at least 3 years; New York Heart
Association class III or IV; or grade ≥2 peripheral neuropathy. All patients provided
written informed consent.
Study design
Institutional review boards/ethics committees at the participating investigational
centers approved the study, which was conducted according to the principles set out
in the Declaration of Helsinki, International Conference on Harmonisation Good
Clinical Practice guidelines, and local regulatory requirements.
In this multicenter, open-label, dose-escalation study (NCT01577758), TAK-264 was
administered once every 3 weeks as a 30-minute IV infusion (day 1 of 21-day cycles)
for up to 17 cycles or until disease progression or occurrence of unacceptable TAK-
264-related toxicity. Dose escalation was conducted using a Bayesian continual
reassessment method (CRM) based on 2-patient cohorts, according to observed
DLTs during cycle 1. DLTs were defined as: grade 4 neutropenia (ANC < 500
cells/mm3); grade ≥3 neutropenia with fever (oral temperature ≥38.5°C) and/or
infection; grade 4 thrombocytopenia (platelets <25,000/mm3); grade ≥3
thrombocytopenia with clinically meaningful bleeding at any time; grade ≥3 nausea
and/or emesis that occurred despite anti-emetic prophylaxis; grade ≥3 diarrhea that
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474
11 156699_2_art_file_3450457_h5mfx3.docx
occurred despite optimal supportive care measures; any other grade ≥3
nonhematologic toxicity with the exception of brief (<1 week) grade 3 fatigue; inability
to start the next cycle of therapy due to >2 weeks treatment delay because of a lack
of adequate recovery of TAK-264-related hematologic/nonhematologic toxicities;
other TAK-264-related grade ≥2 nonhematologic toxicities that, in the opinion of the
investigator, required a dose reduction or discontinuation of TAK-264 therapy.
The CRM algorithm is shown in Fig. 1. Dose escalation or de-escalation was based
on the observed toxicities in all DLT-evaluable patients. After the first 2 patients had
been dosed and had completed the first cycle of therapy, the CRM algorithm was
updated based on the observed DLTs, and the predicted MTD was calculated. Once
at least 6 patients had been treated at a given dose without the algorithm suggesting
escalation or de-escalation, that dose was considered the MTD. After completion of
dose escalation and MTD determination, additional patients with mCRC were
enrolled to a prespecified dose-expansion cohort to achieve up to 20 response-
evaluable patients. Among these patients, at least 6 were required to have high GCC
expression.
Objectives and Assessments
The primary objectives were to assess the safety profile of IV TAK-264 in patients
with advanced GCC-expressing gastrointestinal malignancies, determine the MTD,
and describe the pharmacokinetic profile of TAK-264, total antibody, and MMAE.
Secondary objectives were to evaluate disease response and evidence of antitumor
activity in TAK-264-treated patients and the immunogenicity of TAK-264
(antitherapeutic antibody [ATA] development).
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474

12 156699_2_art_file_3450457_h5mfx3.docx
An immunohistochemistry assay was performed to assess the expression of GCC by
utilizing a fully human antibody specific to GCC (Millennium Pharmaceuticals, Inc.).
Tissue sections 5 to 10 micron thick were dewaxed through 4, 5-minute changes of
xylene and then placed in a series of graded alcohol solutions diluted with distilled
water. Steam heat induced epitope recovery (SHIER) was conducted for 20 minutes
in the capillary gap in the upper chamber of a Black and Decker Steamer. An
automated TechMate 500 or TechMate 1000 (Roche Diagnostics) was used to
perform the staining. Following an overnight primary incubation, the visualization was
achieved using a non-biotin based peroxidase detection kit (Ultra Vision). After
completing the staining, slides were dehydrated and glass coverslips and CytoSeal
were used to permanently cover the slides. Positive staining was shown by the
presence of a brown (DAB-HRP) reaction product. Hematoxylin counter stain was
used to visualize cell and tissue morphology. All slides were stained and assessed
under microscope by two blinded pathologists at the central laboratory to assess
quality of staining and evaluate the GCC levels. Based on this semi-quantitative
method, H-score for GCC expression was calculated using the sum of the
percentage of tumor cells with GCC staining and intensity of 1+, 2+, and 3+, up to a
maximum score of 300 (100% at 3+) (29). Preclinical data suggested that both
cytoplasmic and apical GCC expression may play a role in TAK-264 efficacy (data on
file). Therefore, H-scores were determined for both cytoplasmic and apically oriented
staining and summed, giving a total maximum combined H-score of 600. The staining
was detected on tumor cells; there was no staining in the stroma or infiltrating
inflammatory cells.
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474

13 156699_2_art_file_3450457_h5mfx3.docx
Adverse events (AEs) were graded using NCI-CTCAE version 4.03. Disease
responses were assessed at the end of every second cycle by RECIST v1.1. Blood
samples were collected for pharmacokinetic analysis pre-dose and at multiple time
points post-dose. Serum levels of TAK-264 and total antibody were assayed using a
quantitative sandwich enzyme immunoassay; plasma levels of free MMAE were
determined using a liquid chromatography tandem mass spectrometry assay. Blood
samples were taken from patients before dosing and at the end of the study to
evaluate presence of antitherapeutic antibody (ATA), using validated assays to
detect TAK-264-binding antibodies and to verify whether these antibodies had
neutralizing activity.
Analysis populations and statistical analyses
The safety population included all patients who received at least 1 dose of study
drug. The DLT-evaluable population (used to determine MTD) included dose-
escalation patients who either experienced a DLT during cycle 1 or received TAK-
264 and completed all study procedures in cycle 1 without DLTs. The
pharmacokinetics-evaluable population included patients with sufficient dosing and
pharmacokinetic data to estimate pharmacokinetic parameters. The response-
evaluable population included patients with measureable disease who received TAK-
264 and had at least 1 post-baseline response assessment.
Statistical analyses were primarily descriptive and graphical in nature. Summary
tabulations were used to present the number of observations, mean, standard
deviation, median, minimum, and maximum for continuous variables, and the number
and percentage per category for categorical data. Summary statistics were calculated
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474
14 156699_2_art_file_3450457_h5mfx3.docx
for baseline characteristics, dosing, safety (including DLTs), AEs, serious AEs,
laboratory values, vital signs, efficacy (including disease response), biomarkers
(including ATA), and pharmacokinetic parameters. Progression-free survival was
estimated using the Kaplan-Meier method.
Results
Patient characteristics
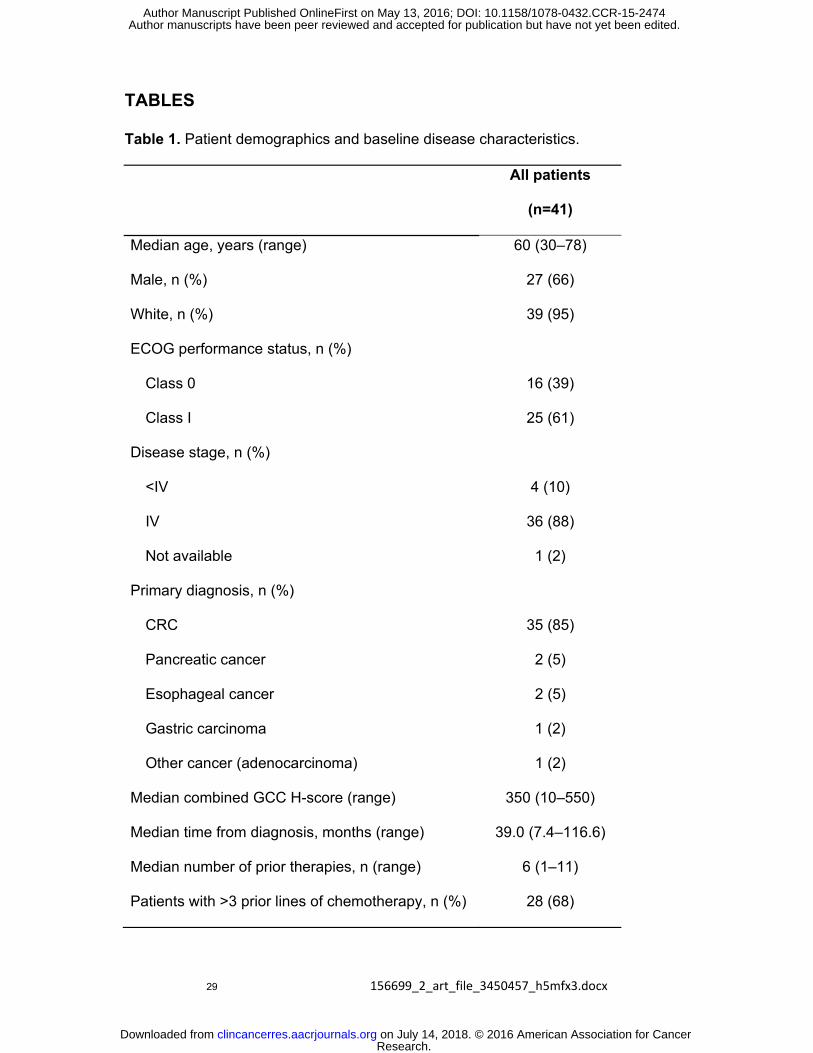
Forty one patients were enrolled at 3 sites in the US and 1 site in Spain between
June 11, 2012 and February 12, 2014 and received at least 1 dose of TAK-264
(Table 1). In 35/41 (85%) patients the primary diagnosis was mCRC, as this was the
only tumor type included in the prespecified expansion cohort. The other patients had
pancreatic, esophageal, gastric, or other type of adenocarcinoma. GCC H-score
ranged from 10 to 550; 13 patients with high GCC expression levels were enrolled in
the expansion cohort.
DLTs and MTD determination
The dose-escalation cohort included 19 patients: 2 patients each at 0.3 mg/kg, 0.6
mg/kg, 1.2 mg/kg, and 1.5 mg/kg, 6 patients at 1.8 mg/kg, 4 patients at 2.1 mg/kg,
and 1 patient at 2.4 mg/kg. There were no DLTs in the low dose groups (0.3-1.5
mg/kg). At higher doses a total of 4 patients experienced DLTs of grade 4
neutropenia. Of the 4 patients with DLTs, 3 were treated at doses above 1.8 mg/kg.
One patient in the 1.8 mg/kg dose group experienced a DLT of grade 4 febrile
neutropenia on day 12 of cycle 1. The patient discontinued the study per protocol and
the neutropenia resolved in 2 days. Two patients in the 2.1 mg/kg dose group
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474
15 156699_2_art_file_3450457_h5mfx3.docx
experienced DLTs. One patient experienced grade 4 neutropenia and grade 3 QTc
prolongation on days 10 and 14 of cycle 1, respectively. Per protocol, the patient
discontinued the study and the DLTs resolved in 4 and 7 days, respectively. The
other patient treated at 2.1 mg/kg had grade 4 neutropenia on day 15 of cycle 1,
which resolved 7 days later. At a dose of 2.4 mg/kg, one patient experienced a DLT
of grade 4 neutropenia on day 12 of cycle 1. The patient discontinued the study per
protocol and the DLT resolved in 4 days.
The MTD was determined as 1.8 mg/kg according to the Bayesian CRM method. A
total of 25 patients with mCRC were enrolled at this dose level, which included the
patients from the expansion cohort and 3 patients from the 1.8 mg/kg dose-
escalation cohort.
Treatment exposure and safety
Patients received a median of 2 cycles of TAK-264 (range 1-12). Overall, 9 (22%)
patients received ≥4 cycles and 5 (12%) patients received ≥6 cycles. Reasons for
treatment discontinuation were disease progression (n=28, 68%), symptomatic
deterioration (n=7, 17%), AEs, and subject withdrawal (each n=3, 7%).
All 41 patients reported AEs. A total of 36 patients (88%) reported at least one drug-
related AE (Table 2). The most common drug-related AEs included nausea and
decreased appetite (each n=17, 41%), fatigue (n=13, 32%), diarrhea, anemia,
alopecia, and neutropenia (each n=11, 27%). Grade ≥3 AEs were experienced by 26
patients (63%) treated at all doses (Table 2). Among these, 17 (41%) were drug-
related. The drug-related grade ≥3 AEs, across all doses, included neutropenia (n=9,
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474
16 156699_2_art_file_3450457_h5mfx3.docx
22%), hypokalemia, febrile neutropenia (each n=3, 7%), and QTc prolongation (n=2,
5%). Serious AEs were experienced by 16 patients (39%), with 9 (22%) of these
patients experiencing drug-related serious AEs including small intestinal obstruction
(3 [7%] patients), febrile neutropenia (3 [7%] patients), constipation (2 [5%] patients),
intestinal obstruction (2 [5%] patients), and pyrexia (2 [5%]) patients. Grade 1 or 2
peripheral neuropathy was reported by 4 (10%) patients over the course of the study;
3 patients without baseline peripheral neuropathy experienced grade 1 peripheral
neuropathy; two patients reported peripheral neuropathy during cycles 1 and 4,
respectively, which was reported as not resolved by the end-of-study visit
(approximately 30 days after the last dose of study drug or prior to the start of
subsequent antineoplastic therapy), and the third patient reported grade 1 peripheral
neuropathy during cycle 5, which resolved in 27 days. The fourth patient entered the
study with grade 1 peripheral neuropathy and experienced grade 2 peripheral
neuropathy events during cycles 1 and 2, which resolved in 6 and 9 days,
respectively.
A total of 3 (7%) patients had dose reductions due to AEs. There were 3 (7%)
discontinuations due to AEs, and 1 on-study death considered to be related to
disease progression. The 3 patients who discontinued due to AEs were all treated at
doses above the MTD and experienced DLTs. Therefore, per protocol, they
discontinued the study. Two of the 3 patients were treated at 2.1 mg/kg and one at
2.4 mg/kg. The patient who died of disease progression was a 51-year old male with
esophageal carcinoma who received TAK-264 at the MTD (1.8 mg/kg) and initially
discontinued due to a DLT of grade 4 neutropenia. A re-staging CT scan several
months later, without any further therapy, showed a response. The patient re-entered
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474
17 156699_2_art_file_3450457_h5mfx3.docx
the study 6 months after the initial discontinuation at a dose reduction of 1.5 mg/kg
TAK-264. Unfortunately, although the patient tolerated the infusion, his clinical status
declined and he died of disease progression 8 days after the second administration
of TAK-264. The treating physician assumed that his disease was the primary cause
of death. In this study there were no confirmed ATA-positive results detected in the
total number of samples.
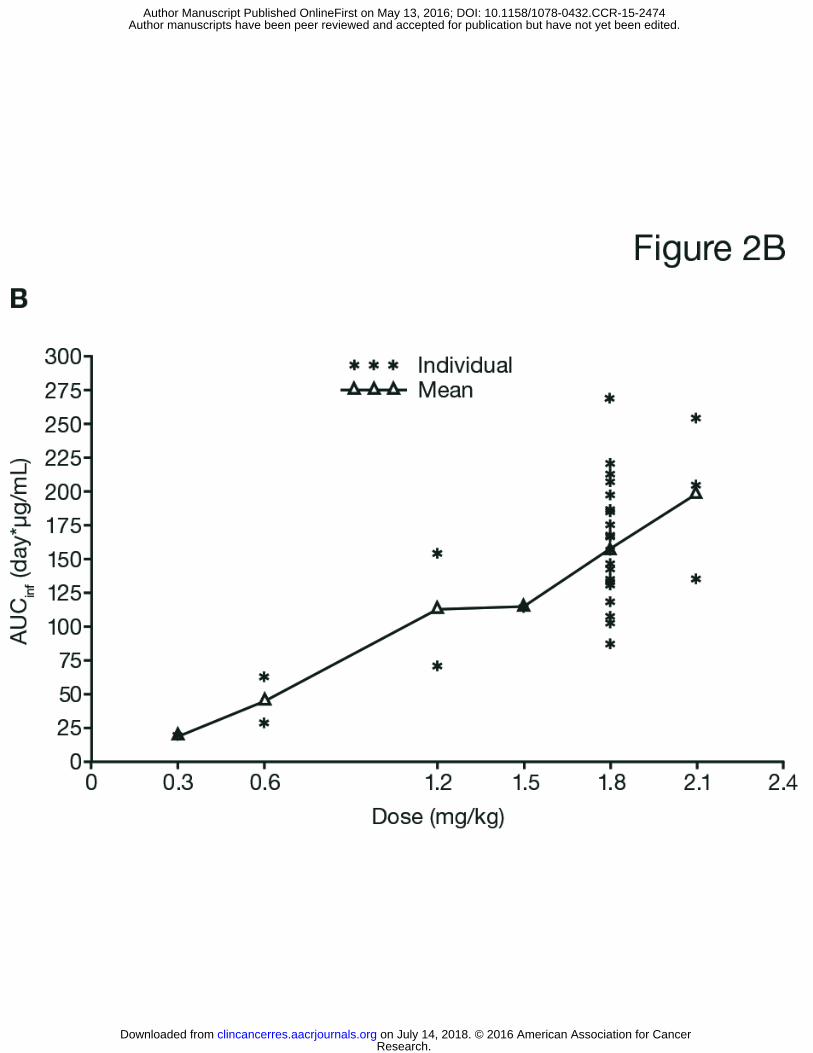
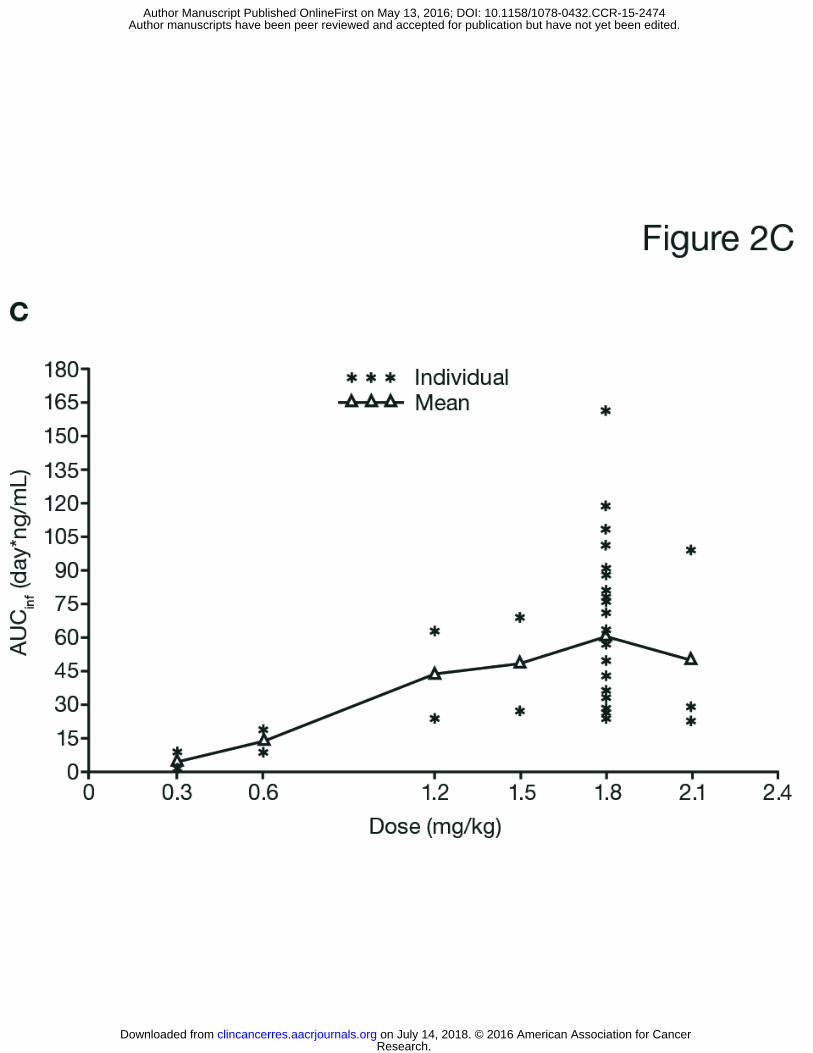
Pharmacokinetics
The pharmacokinetics-evaluable population included all 41 patients. PK samples
were collected pre-dose, post dose and on day 2, 3, 4, 8, and 15. Increases in
exposure to TAK-264 and free MMAE were approximately proportional to dose (Fig.
2). Summary statistics for TAK-264, total antibody, and MMAE pharmacokinetic
parameters during cycle 1 for patients treated at the MTD are shown in Table 3.
Median time to maximum concentration occurred immediately after infusion for TAK-
264 and total antibody, and approximately 3 days after infusion for MMAE. Median
half-life was approximately 4 days for TAK-264 and 3 days for free MMAE.
Antitumor activity
Among 39 response-evaluable patients, one partial response was observed in a 53-
year-old white male patient with gastric adenocarcinoma who had a low GCC
expression level, had received three prior therapies, and had been treated with TAK-
264 at the MTD. This response was observed after 2 treatment cycles and sustained
for 81 days. The patient was progression-free for 121 days. In addition, stable
disease was observed in 17 response-evaluable patients (44%). One 57-year-old
white female patient with pancreatic carcinoma who had a low GCC expression level
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474
18 156699_2_art_file_3450457_h5mfx3.docx
received 12 cycles of treatment. This patient was treated at 2.1 mg/kg through cycle
3 and at 1.8 mg/kg for cycles 4-12, maintaining stable disease from the first response
assessment (unscheduled) until the end of cycle 12. A 30-year-old white male patient
with pancreatic carcinoma who had a low GCC expression level received 6 cycles of
treatment at the MTD and had a best response of stable disease, which lasted for 6
cycles. Both of these patients had previously received multiple lines of treatment,
including chemotherapy, radiotherapy, and surgery. A 51-year-old white male patient
with esophageal carcinoma who had an intermediate GCC expression level was
treated at the MTD, but experienced a DLT of febrile neutropenia during cycle 1 and
discontinued, per protocol. A follow-up scan showed a decrease in the size and
number of his lung metastases, suggesting a delayed response to treatment.
Overall, progressive disease was observed as the best response in 21 response-
evaluable patients (54%). The number of treatment cycles received by each patient
according to GCC expression level is shown in Fig. 3. GCC expression, as measured
by H-score, did not appear to correlate with treatment duration.
Median PFS for the response-evaluable population was 44 days (95% CI 39-83).
Using a Cox proportional hazard model, there was no association between GCC
expression and PFS (HR 1.002, p=0.6052). There was also no difference in PFS
when dichotomized by median GCC expression (HR 0.806, p=0.6545).
Discussion
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474
19 156699_2_art_file_3450457_h5mfx3.docx
TAK-264 appeared generally well tolerated with a manageable safety profile in
patients with advanced, GCC-positive gastrointestinal malignancies. The MTD for
TAK-264, determined using a Bayesian CRM (30-32), was 1.8 mg/kg. A total of 19
patients were treated during the dose-escalation phase in order to establish the MTD,
with 8 of these patients receiving a dose below the MTD. An advantage of the CRM
algorithm used in this study was that it allowed an accurate MTD to be determined
with a minimal number of patients treated at sub-optimal levels, while utilizing
information from all treated patients to guide the dose modifications (33). It also
allowed rapid dose escalation, which was completed over approximately 12 months,
through 7 increasing doses.
DLTs were reported in 4/19 patients in the dose-escalation phase of the study. Three
of the 4 patients with DLTs of grade 4 neutropenia were treated at doses above 1.8
mg/kg (MTD), while 1 patient who experienced grade 4 febrile neutropenia was
treated at the MTD. Of the 3 patients treated at doses above the MTD, 1 patient also
experienced grade 3 QTc prolongation. The DLTs occurred during days 10-15 of
cycle 1, approximately 7-12 days after the MMAE Tmax of approximately 3 days;
MMAE has a plasma half-life of approximately 3 days, and neutrophils have a
circulation life of approximately 5 days (34). The mechanism by which TAK-264
causes neutropenia is not yet understood, but free MMAE is likely the cause as GCC
has not been found to be expressed in the bone marrow compartment; therefore a
role for this receptor in triggering neutrophil depletion seems unlikely. In other studies
using microtubule-targeting agents such as taxanes, hematologic AEs were relatively
common (35). It appears that neutrophils may be more susceptible to this toxicity
than other bone marrow-derived cells.
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474

20 156699_2_art_file_3450457_h5mfx3.docx
Other common drug-related AEs included nausea, fatigue, decreased appetite, and
diarrhea, which are often reported in patients with gastrointestinal malignancies.
Interestingly, patients receiving brentuximab vedotin, who did not suffer from
gastrointestinal malignancies, experienced a spectrum of AEs which included
nausea, fatigue, neutropenia, diarrhea, and pyrexia (3-6), which are to some extent
comparable with the AEs reported for TAK-264. The ADCs polatuzumab vedotin and
pinatuzumab vedotin were also associated with similar toxicities, including
neutropenia, peripheral neuropathy, and diarrhea (36). These ADCs incorporate the
same cytotoxic agent as TAK-264, MMAE; it is assumed that the cytotoxicity of
MMAE is related to its ability to inhibit cell division by binding tubulin, which arrests
the target cell in the G2/M stage of the cell cycle and results in apoptosis (3). In
contrast to these studies of other ADCs, peripheral neuropathy was not a commonly
reported AE with TAK-264, occurring at grade 1 or 2 in 10% of patients. It should be
noted, however, that the majority of patients participating in this study received 2
cycles of therapy. No ATA-positive samples were detected during this study and no
infusion site reactions occurred; this was consistent with expectations as TAK-264
utilizes a fully humanized antibody.
Pharmacokinetic data, including a median half-life of approximately 4 days for TAK-
264, suggest that steady-state pharmacokinetics for both the ADC and MMAE
occurred by approximately 21 days, supporting the dosing schedule employed.
Concentration-time profiles showed that TAK-264, total antibody, and MMAE
concentrations peaked following infusion then decreased to low pre-infusion
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474
21 156699_2_art_file_3450457_h5mfx3.docx
concentrations prior to the next cycle, suggesting a lack of substantial accumulation
in plasma or serum.
Preliminary response data indicated antitumor activity in this population, especially in
non-mCRC patients. The efficacy of ADCs using MMAE in gastrointestinal
malignancies is unproven, although they have been used successfully in Hodgkin
lymphoma and anaplastic large cell lymphoma (3-6). Microtubule-disrupting agents
have been shown to have varying effects in different tumor cell lines and may work
by different mechanisms depending on cell type (26, 37). In this study, duration of
disease stabilization and antitumor activity did not appear to correlate with GCC
expression level. In total, 52% of patients in the expansion cohort had high levels of
GCC expression. It is intriguing that 4 patients for whom there were early signals of
potential clinical benefit, all non-mCRC, had low levels of GCC expression relative to
the overall population. Further investigation is needed to assess the role of GCC
expression in clinical outcomes with TAK-264.
Several factors are involved in the ADC treatment response including the toxin
selection, binding affinity of the antibody, delivering the ADC and cytotoxic agent to
the tumor cells, and linker technology. While the data from this study are preliminary,
there was less than expected clinical efficacy. The selection of GCC as a target
remains experimental and more data are needed to better assess the potential of
targeting GCC in order to develop a successful treatment strategy for gastrointestinal
malignancies. Various characteristics need to be better defined (such as
heterogeneity and specificity of target expression, internalization rate, intracellular
trafficking) to interpret the limitation of clinical efficacy.
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474

22 156699_2_art_file_3450457_h5mfx3.docx
Tissues tested for GCC expression were mostly archived tissues, including some
from primary tumor during initial resection.
The relationship between primary and metastatic sites, and the effects of multiple
lines of therapy, on GCC staining characteristics is currently unknown. Further insight
into the optimal design characteristics of effective ADCs will be best gained as
additional clinical data become available. Several ADCs are currently in clinical
development, and TAK-264 is undergoing further investigation in 2 single-arm, phase
2 clinical studies in patients with gastric (NCT 02202759) and pancreatic cancer
(NCT02202785).
In conclusion, TAK-264 is a first-in-class ADC with a novel target, the GCC receptor.
The data from this first-in-human phase 1 study suggest that TAK-264 has a
manageable safety profile at the MTD of 1.8 mg/kg. Preliminary data suggest
antitumour activity and early signs of clinical benefit in patients with pancreatic,
esophageal, and gastric carcinoma. Combination strategies with active
chemotherapy agents could be considered in the future. Antitumor activity did not
appear to correlate with GCC expression levels. Evolving clinical data from the
ongoing phase 2 clinical trials of TAK-264 will provide critical insight into the design
of next generation ADCs.
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474
23 156699_2_art_file_3450457_h5mfx3.docx
Acknowledgments
The authors acknowledge Helen Johns of FireKite, an Ashfield company, part of
UDG Healthcare plc, for writing support during the development of this manuscript,
which was funded by Millennium Pharmaceuticals, Inc. ADC technology was licensed
from Seattle Genetics, Inc.
Author contribution statement:
KA, TK, CC, JEF, DPR, TW, AAF, WM, and JR designed and performed the
research. KA, CC, JEF, DPR, WM, and JR collected data. KA, TK, CC, JEF, DPR,
JJ, TW, AAF, WM, and JR analyzed and interpreted data (pharmacokinetics: AAF).
JJ performed statistical analysis. KA, TK, JJ, TW, and AAF wrote the draft
manuscript. All authors contributed to the writing and reviewing of the manuscript,
and approved the final manuscript for submission.
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474
24 156699_2_art_file_3450457_h5mfx3.docx
References
1. Leal M, Sapra P, Hurvitz SA, Senter P, Wahl A, Schutten M, et al. Antibody-drug
conjugates: an emerging modality for the treatment of cancer. Ann N Y Acad Sci
2014; 1321:41-54.
2. Teicher BA, Chari RV. Antibody conjugate therapeutics: challenges and potential.
Clin Cancer Res 2011; 17:6389-6397.
3. Fanale MA, Forero-Torres A, Rosenblatt JD, Advani RH, Franklin AR, Kennedy
DA, et al. A phase I weekly dosing study of brentuximab vedotin in patients with
relapsed/refractory CD30-positive hematologic malignancies. Clin Cancer Res
2012; 18:248-255.
4. Pro B, Advani R, Brice P, Bartlett NL, Rosenblatt JD, Illidge T, et al. Brentuximab
vedotin (SGN-35) in patients with relapsed or refractory systemic anaplastic large-
cell lymphoma: results of a phase II study. J Clin Oncol 2012; 30:2190-2196.
5. Younes A, Bartlett NL, Leonard JP, Kennedy DA, Lynch CM, Sievers EL, et al.
Brentuximab vedotin (SGN-35) for relapsed CD30-positive lymphomas. N Engl J
Med 2010; 363:1812-1821.
6. Younes A, Gopal AK, Smith SE, Ansell SM, Rosenblatt JD, Savage KJ, et al.
Results of a pivotal phase II study of brentuximab vedotin for patients with
relapsed or refractory Hodgkin's lymphoma. J Clin Oncol 2012; 30:2183-2189.
7. Lambert JM, Chari RV. Ado-trastuzumab Emtansine (T-DM1): an antibody-drug
conjugate (ADC) for HER2-positive breast cancer. J Med Chem 2014; 57:6949-
6964.
8. FDA approval: Brentuximab Vedotin.
http://www.fda.gov/AboutFDA/CentersOffices/OfficeofMedicalProductsandTobacc
o/CDER/ucm268969.htm. Accessed 11 March 2015.
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474

25 156699_2_art_file_3450457_h5mfx3.docx
9. EMA. Adcetris Summary of Product Characteristics.
http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-
_Product_Information/human/002455/WC500135055.pdf. Accessed 11 March
2015.
10. Palanca-Wessels MC, Press OW. Advances in the treatment of hematologic
malignancies using immunoconjugates. Blood 2014; 123:2293-2301.
11. Sadeghi S, Olevsky O, Hurvitz SA. Profiling and targeting HER2-positive breast
cancer using trastuzumab emtansine. Pharmgenomics Pers Med 2014; 7:329-
338.
12. LoRusso PM, Weiss D, Guardino E, Girish S, Sliwkowski MX. Trastuzumab
emtansine: a unique antibody-drug conjugate in development for human
epidermal growth factor receptor 2-positive cancer. Clin Cancer Res 2011;
17:6437-6447.
13. FDA approval: Trastuzumab Emtansine.
http://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/ucm340913.htm.
Accessed 11 March 2015.
14. EMA. Kadcyla Summary of Product Characteristics.
http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-
_Product_Information/human/002389/WC500158593.pdf. Accessed 11 March
2015.
15. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin 2015;
65:5-29.
16. Carrithers SL, Parkinson SJ, Goldstein SD, Park PK, Urbanski RW, Waldman SA.
Escherichia coli heat-stable enterotoxin receptors. A novel marker for colorectal
tumors. Dis Colon Rectum 1996; 39:171-181.
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474
26 156699_2_art_file_3450457_h5mfx3.docx
17. Hyslop T, Waldman SA. Guanylyl cyclase C as a biomarker in colorectal cancer.
Biomark Med 2013; 7:159-167.
18. Carrithers SL, Parkinson SJ, Goldstein S, Park P, Robertson DC, Waldman SA.
Escherichia coli heat-stable toxin receptors in human colonic tumors.
Gastroenterology 1994; 107:1653-1661.
19. John M, Wiedenmann B, Kruhoffer M, Adermann K, Ankorina-Stark I, Schlatter E,
et al. Guanylin stimulates regulated secretion from human neuroendocrine
pancreatic cells. Gastroenterology 1998; 114:791-797.
20. Kloeters O, Friess H, Giese N, Buechler MW, Cetin Y, Kulaksiz H. Uroguanylin
inhibits proliferation of pancreatic cancer cells. Scand J Gastroenterol 2008;
43:447-455.
21. Park J, Schulz S, Haaf J, Kairys JC, Waldman SA. Ectopic expression of guanylyl
cyclase C in adenocarcinomas of the esophagus and stomach. Cancer Epidemiol
Biomarkers Prev 2002; 11:739-744.
22. Buc E, Vartanian MD, Darcha C, Dechelotte P, Pezet D. Guanylyl cyclase C as a
reliable immunohistochemical marker and its ligand Escherichia coli heat-stable
enterotoxin as a potential protein-delivering vehicle for colorectal cancer cells. Eur
J Cancer 2005; 41:1618-1627.
23. Camci C, Sahin A, Sevinc A, Kalender ME, Oztuzcu S, Sever ON, et al.
Peripheral blood guanylyl cyclase c (GCC) expressions are associated with
prognostic parameters and response to therapy in colorectal cancer patients.
Tumour Biol 2011; 32:1265-1270.
24. Winn B, Tavares R, Matoso A, Noble L, Fanion J, Waldman SA, et al. Expression
of the intestinal biomarkers Guanylyl cyclase C and CDX2 in poorly differentiated
colorectal carcinomas. Hum Pathol 2010; 41:123-128.
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474

27 156699_2_art_file_3450457_h5mfx3.docx
25. Almenoff JS, Williams SI, Scheving LA, Judd AK, Schoolnik GK. Ligand-based
histochemical localization and capture of cells expressing heat-stable enterotoxin
receptors. Mol Microbiol 1993; 8:865-873.
26. Guarino A, Cohen MB, Overmann G, Thompson MR, Giannella RA. Binding of E.
coli heat-stable enterotoxin to rat intestinal brush borders and to basolateral
membranes. Dig Dis Sci 1987; 32:1017-1026.
27. Veiby P, Zhang J, Yang J, McDonald A, Fasanmade A, Wyant T, et al. The
Investigational Drug MLN0264 First-in-human, First in Class ADC Targeting GCC:
Phase I Dose-escalation Study and Supportive Scientific Rationale. Eur.J.Cancer
2012; 48:iv36
28. Zhang J, Gallery M, Wyant T, Stringer B, Manfredi M, Danaee H, et al. MLN0264,
an investigational, first-in-class antibody-drug conjugate (ADC) targeting guanylyl
cyclase C (GCC), demonstrates antitumor activity alone and in combination with
gemcitabine in human pancreatic cancer xenograft models expressing GCC. Mol
Cancer Ther 2013; 12(11 Suppl):PR12
29. Hirsch FR, Varella-Garcia M, Bunn PA, Jr., Di Maria MV, Veve R, Bremmes RM,
et al. Epidermal growth factor receptor in non-small-cell lung carcinomas:
correlation between gene copy number and protein expression and impact on
prognosis. J Clin Oncol 2003; 21:3798-3807.
30. Normolle D, Lawrence T. Designing dose-escalation trials with late-onset
toxicities using the time-to-event continual reassessment method. J Clin Oncol
2006; 24:4426-4433.
31. O'Quigley J, Shen LZ. Continual reassessment method: a likelihood approach.
Biometrics 1996; 52:673-684.
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474
28 156699_2_art_file_3450457_h5mfx3.docx
32. He W, Liu J, Binkowitz B, Quan H. A model-based approach in the estimation of
the maximum tolerated dose in phase I cancer clinical trials. Stat Med 2006;
25:2027-2042.
33. Le TC, Lee JJ, Siu LL. Dose escalation methods in phase I cancer clinical trials. J
Natl Cancer Inst 2009; 101:708-720.
34. Pillay J, den B, I, Vrisekoop N, Kwast LM, de Boer RJ, Borghans JA, et al. In vivo
labeling with 2H2O reveals a human neutrophil lifespan of 5.4 days. Blood 2010;
116:625-627.
35. Klute K, Nackos E, Tasaki S, Nguyen DP, Bander NH, Tagawa ST. Microtubule
inhibitor-based antibody-drug conjugates for cancer therapy. Onco Targets Ther
2014; 7:2227-2236.
36. Morschhauser F, Flinn IW, Advani R, Diefenbach CS, Kolibaba K, Press OW, et
al. Updated Results of a Phase II Randomized Study (ROMULUS) of
Polatuzumab Vedotin or Pinatuzumab Vedotin Plus Rituximab in Patients with
Relapsed/Refractory Non-Hodgkin Lymphoma. Blood (ASH abstracts) 2014; 124.
37. Gascoigne KE, Taylor SS. How do anti-mitotic drugs kill cancer cells? J Cell Sci
2009; 122:2579-2585.
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474
29 156699_2_art_file_3450457_h5mfx3.docx
TABLES
Table 1. Patient demographics and baseline disease characteristics.
All patients
(n=41)
Median age, years (range) 60 (30–78)
Male, n (%) 27 (66)
White, n (%) 39 (95)
ECOG performance status, n (%)
Class 0 16 (39)
Class I 25 (61)
Disease stage, n (%)
<IV 4 (10)
IV 36 (88)
Not available 1 (2)
Primary diagnosis, n (%)
CRC 35 (85)
Pancreatic cancer 2 (5)
Esophageal cancer 2 (5)
Gastric carcinoma 1 (2)
Other cancer (adenocarcinoma) 1 (2)
Median combined GCC H-score (range) 350 (10–550)
Median time from diagnosis, months (range) 39.0 (7.4–116.6)
Median number of prior therapies, n (range) 6 (1–11)
Patients with >3 prior lines of chemotherapy, n (%) 28 (68)
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474

30 156699_2_art_file_3450457_h5mfx3.docx
Table 2. AEs experienced by ≥10% of patients by severity
AE, n (%)
Any-grade
(N=41)
Grade 1
(N=41)
Grade 2
(N=41)
Grade 3 and 4
(N=41)
Any AE 41 (100) 3 (7) 12 (29) 26 (63)
Nausea 21 (51) 16 (39) 5 (12) 0
Decreased appetite 20 (49) 12 (29) 8 (20) 0
Fatigue 17 (41) 8 (20) 8 (20) 1 (2)
Diarrhea 16 (39) 10 (24) 3 (7) 3 (7)
Anemia 14 (34) 4 (10) 6 (15) 4 (10)
Pyrexia 13 (32) 12 (29) 1 (2) 0
Asthenia 12 (29) 5 (12) 6 (15) 1 (2)
Neutropenia 11 (27) 0 2 (5) 9 (22)*
Alopecia 11 (27) 7 (17) 4 (10) 0
Constipation 10 (24) 3 (7) 7 (17) 0
Vomiting 10 (24) 3 (7) 7 (17) 0
Aspartate aminotransferase
increased 9 (22) 9 (22) 0 0
Abdominal pain 9 (22) 5 (12) 3 (7) 1 (2)
Hypokalemia 9 (22) 5 (12) 0 4 (10)
Alanine aminotransferase
increased 7 (17) 7 (17) 0 0
Dehydration 7 (17) 3 (7) 3 (7) 1 (2)
Arthralgia 7 (17) 4 (10) 3 (7) 0
Hyponatremia 6 (15) 4 (10) 0 2 (5)
Thrombocytopenia 6 (15) 5 (12) 1 (2) 0
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474

31 156699_2_art_file_3450457_h5mfx3.docx
Musculoskeletal pain 6 (15) 3 (7) 3 (7) 0
Hyperglycemia 5 (12) 3 (7) 1 (2) 1 (2)
Gamma-glutamyltransferase
increased 5 (12) 1 (2) 2 (5) 2 (5)
Back pain 5 (12) 3 (7) 2 (5) 0
Anxiety 5 (12) 4 (10) 1 (2) 0
Insomnia 5 (12) 1 (2) 4 (10) 0
Dyspnea 5 (12) 2 (5) 3 (7) 0
Small intestinal obstruction 4 (10) 0 2 (5) 2 (5)
Hypophosphatemia 4 (10) 1 (2) 2 (5) 1 (2)
Blood alkaline phosphatase
increased 4 (10) 2 (5) 2 (5) 0
Electrocardiogram QT
prolonged 4 (10) 2 (5) 0 2 (5)
Weight decreased 4 (10) 4 (10) 0 0
Leukopenia 4 (10) 1 (2) 3 (7) 0
Headache 4 (10) 4 (10) 0 0
Cough 4 (10) 4 (10) 0 0
*5 (12%) grade 4
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474
32 156699_2_art_file_3450457_h5mfx3.docx
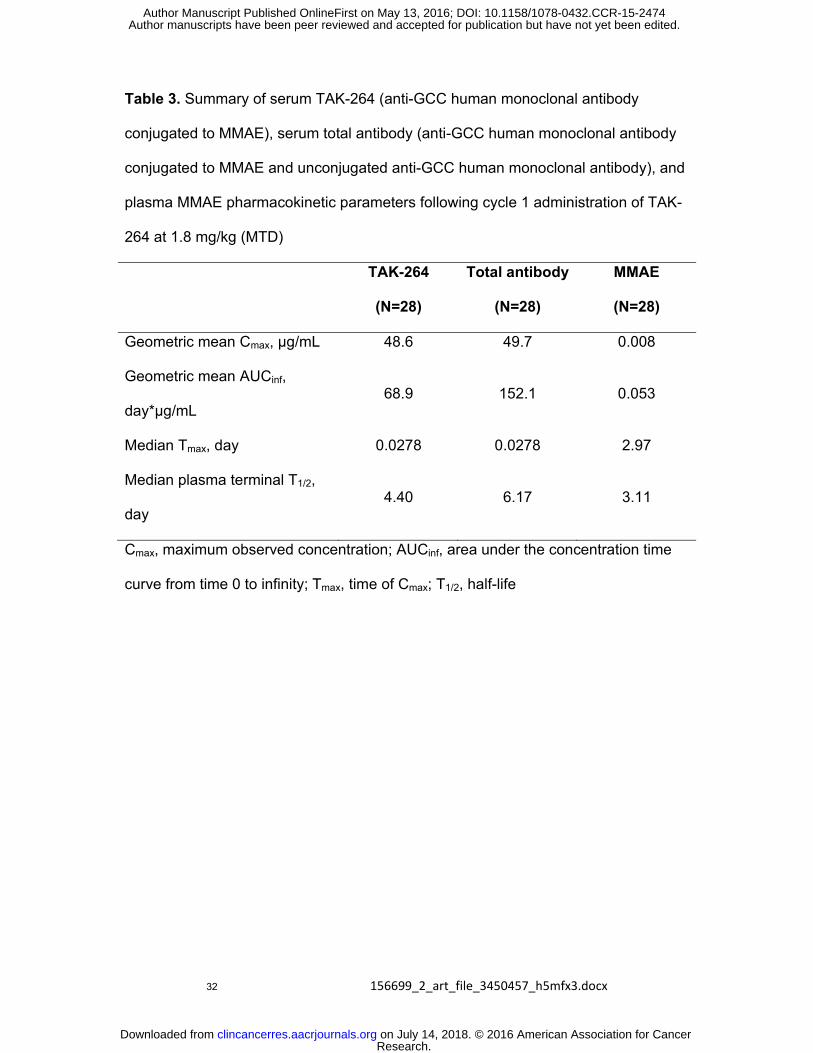
Table 3. Summary of serum TAK-264 (anti-GCC human monoclonal antibody
conjugated to MMAE), serum total antibody (anti-GCC human monoclonal antibody
conjugated to MMAE and unconjugated anti-GCC human monoclonal antibody), and
plasma MMAE pharmacokinetic parameters following cycle 1 administration of TAK-
264 at 1.8 mg/kg (MTD)
TAK-264
(N=28)
Total antibody
(N=28)
MMAE
(N=28)
Geometric mean Cmax, μg/mL 48.6 49.7 0.008
Geometric mean AUCinf,
day*μg/mL 68.9 152.1 0.053
Median Tmax, day 0.0278 0.0278 2.97
Median plasma terminal T1/2,
day 4.40 6.17 3.11
Cmax, maximum observed concentration; AUCinf, area under the concentration time
curve from time 0 to infinity; Tmax, time of Cmax; T1/2, half-life
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474
33 156699_2_art_file_3450457_h5mfx3.docx
Figure Legends
Fig 1. Schema for the CRM algorithm used for the dose-escalation portion of the
study. (CRM, continual reassessment method; DLT, dose-limiting toxicity; Mid-high,
midpoint between current dose and next dose; Mid-low, midpoint between previous dose
and current dose; MTD, maximum tolerated dose; PMTD, predicted maximum tolerated
dose. *Dosing intervals were pre-specified and not determined by the CRM algorithm.)
Fig 2. Dose-proportionality evaluation, showing cycle 1 AUCinf versus TAK-264 dose
for A) TAK-264, B) total antibody, and C) MMAE.
Fig 3. Number of TAK-264 cycles received by each patient, by GCC expression
level.
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474

Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474

Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474

Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474

Published OnlineFirst May 13, 2016.Clin Cancer Res Khaldoun Almhanna, Thea Kalebic, Cristina Cruz, et al. with advanced gastrointestinal malignanciesantibody-drug conjugate TAK-264 (MLN0264) in adult patients Phase I study of the investigational anti-guanylyl cyclase
Updated version
10.1158/1078-0432.CCR-15-2474doi:
Access the most recent version of this article at:
Manuscript
Authoredited. Author manuscripts have been peer reviewed and accepted for publication but have not yet been
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/early/2016/05/13/1078-0432.CCR-15-2474To request permission to re-use all or part of this article, use this link
Research. on July 14, 2018. © 2016 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Author Manuscript Published OnlineFirst on May 13, 2016; DOI: 10.1158/1078-0432.CCR-15-2474


















