Perinatal Jaundice · PPT file: slide ... IVIG, Metalloporphyrins, Phenobarbital . Infant GA > 35...
68
Perinatal Jaundice สมพร โชตินฤมล หน่วยทารกแรกเกิด ภาควิชากุมารเวชศาสตร์ มหาวิทยาลัยเชียงใหม่ เอกสารประกอบการสอน: 1. เอกสารประกอบการสอน: 1. PDF file: Neonatal hyperbilirubinemia 2. PPT file: slide ประกอบการสอน 2. เอกสารอ่านเพิ่มเติม: Up to Date 3 files
Transcript of Perinatal Jaundice · PPT file: slide ... IVIG, Metalloporphyrins, Phenobarbital . Infant GA > 35...
Perinatal Jaundice
สมพร โชตนฤมล หนวยทารกแรกเกด ภาควชากมารเวชศาสตร
มหาวทยาลยเชยงใหม
เอกสารประกอบการสอน:
1. เอกสารประกอบการสอน: 1. PDF file: Neonatal hyperbilirubinemia 2. PPT file: slide ประกอบการสอน
2. เอกสารอานเพมเตม: Up to Date 3 files
เกณฑมาตรฐานผประกอบวชาชพเวชกรรม 2555 หมวดท 2 การจ าแนกตามระบบอวยวะ P41

เกณฑมาตรฐานผประกอบวชาชพเวชกรรม 2555 ภาวะผดปกต ตามระบบอวยวะ P64-65

Scope: Perinatal jaundice
• Bilirubin metabolism – Fetal bilirubin metabolism – Neonatal bilirubin metabolism
• Hyperbilirubinemia ,Jaundice – Indirect or Unconjugated hyperbilirubinemia
• Physiologic jaundice • Pathologic jaundice
– (Directed or Conjugated hyperbilirubinemia)
• Common causes of neonatal jaundice
• Assessment of jaundice infant • Management (phototherapy, exchange transfusion) and Follow up

Jaundice in perinatal period
• Perinatal period: – Period immediately before and after birth – Start: 20-28 weeks of gestation – End: 4 weeks after birth (28 days)
• Jaundice: – French: jaune ; Greek: ikteros = yellow
– Yellow staining of the skin and sclerae by abnormally high blood levels of the bilirubin.
• Hyperbilirubinemia: 2 definitions
– Visible jaundice – Bilirubin level more than 95 percentile of normal (Bhutani curve)

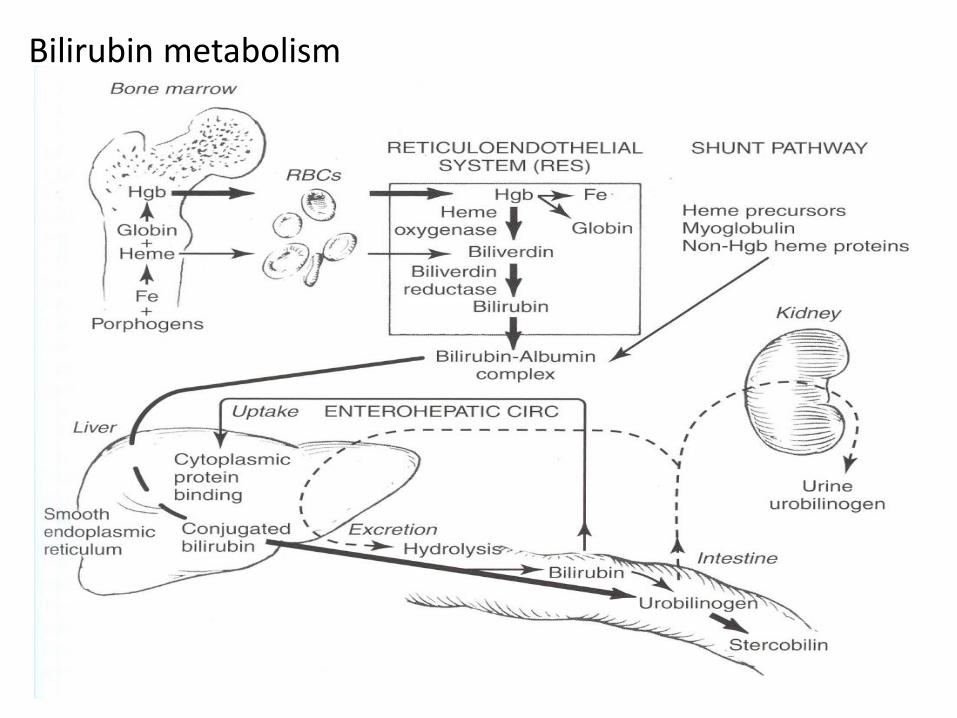
Bilirubin metabolism
Bilirubin metabolism

Bilirubin metabolism: 1:Production
• RBC 85%, Hemoprotein 15%
– Fetal and newborn Bilirubin load More than adult
– 1 g of hemoglobin form 34 mg of bilirubin
• Heme oxygenase in RE system
• End product: 86% of CO production>> Exhaled CO
• Biliver:
– can not excrete through placenta
– Water soluble
• Unconjugated bilirubin
– Fat soluble, Non polar, Water-insoluble
– Excrete through placenta
– excret through GI tract by Conjugate in liver>> Conjugated bilirubin then
• Biliverdin>>>>Unconjugated bilirubin
– Fetus excrete Unconjugated BB via placenta
– Newborn excrete Unconjugated BB via liver

Bilirubin metabolism: 2:Transport of bilirubin in plasma
• Unconjugated BB bind with albumin • Albumin 1 g bind with Unconjugated BB 7-8 mg • Free form BB: excess bilirubin binding capacity
• Low level of BB: Antioxidant , good for cell membrane • High level of BB: Toxic to brain • Only free Unconjugated BB cross blood brain barrier
• Four form of bilirubin in plasma
1. Unconjugated BB bind with albumin(not cross blood brain barrier): Major component 2. Free form unconjugated bilirubin (cross blood brain barrier, neurotoxic) 3. Conjugated bilirubin(water soluble excrete through liver and kidney) 4. Conjugated bilirubin bind with albumin = delta bilirubin
• Diazo reagent test
– Indirect diazo reagent test = 1+2 – Direct diazo reagent test = 3

Bilirubin metabolism: 2:Transport of bilirubin in plasma
• Unconjugated bilirubin is toxic to brain
1. Acute bilirubin encephalopathy (Reversible>>>Nonreversible)
2. Chronic bilirubin encephalopathy
(Kernicterus)
• Phototherapy and Exchange transfusion
– aims to reduce toxic unconjugated bilirubin

Bilirubin metabolism: 3:Hepatic uptake of bilirubin
• Bound unconjugated BB >> liver cell
– Passive process: diffusion
– Active process: in liver cytoplasm
• A-Ligandin (Glutathione-S-transferase A)
• B-ligandin (Y protein)
• Z-protein
• Not a rate limiting step in early after birth

Bilirubin metabolism: 4:Conjugation of bilirubin
• Endoplasmic reticulum of liver cell • Conjugated BB
– Mono and Diglucuronide – polar, water-soluble
• Enzyme – Enzyme UGT1A1 in endoplasmic reticulum ( Limited amount in newborn) (uridine diphosphoglucuronate glucurunosyl transferase – UDP glucuronate glucuronosyltransferase in canalicular portion of hepatocyt
membrane
• UGT activity in human term newborn is 1 % of adult and increase in exponential rate to adult level at 3 months old

Perinatal development of UDP glucuronyl transferase activity

Hepatic bilirubin UGT activity in term newborn
Bilirubin metabolism: 5: Excretion of bilirubin
• Conjugated bilirubin >> bile
• Bile concentration 100 time of hepatocyte concentration by energy dependent concentrative process
• NOT rate limiting step in newborn but in hepatic cellular injury, obstruction.
• Conjugated hyperbilirubinemia: uncommon in newborn

Bilirubin metabolism: 6: Enterohepatic absorption of bilirubin
• Conjugated BB (poorly absorbed) deconjugate to Unconjugated (absorb to circulation) – Enteric mucosa enzyme: beta-glucuronidase
• Present in newborn, not adult
• Absorption at duodenum and colon • Absorption depend on diet, caloric intake • Intestinal bacterial reduce bilirubin to urobilinogen and
stercobilinogen • Most excreted BB is in stool>urine
• Enterohepatic circulation is one of important causes of neonatal
hyperbilirubinemia

Summary
Bilirubin metabolism
1. Bilirubin production
2. Transport of bilirubin in plasma
3. Hepatic uptake of bilirubin
4. Conjugation of bilirubin
5. Excretion of Bilirubin
6. Enterohepatic circulation of bilirubin
Physiologic mechanism of neonatal jaundice
1. Increase bilirubin production
2. Decrease conjugation
3. Increase enterohepatic circulation

Neonatal jaundice
• Chemical ( indirect bilirubin > 1 mg%) almost all newborn
• Clinical (visible or > 5-7mg/dL) > 2/3 of all newborn – (adult and children visible jaundice at > 2 mg/dl)
• Cord blood ~ 1.7 mg% (almost all <2 mg%)
• Measurement
– Clinical: • Visible jaundice distribution
• Golden yellow or greenish yellow
– Laboratory measurement • Diazo reagent: Total bilirubin/ Direct bilirubin >> Indirect bilirubin= TB-DB
• Direct spectrophotometric micro technique = Microbilirubin = Total bilirubin
• Non invasive technique: Transcutaneous bilirubin = Total bilirubin


Neonatal Jaundice
Unconjugated : Indirect BB
• Golden yellow
• Direct BB< 2 mg%
• Direct BB < 20 % of Total BB
• Cause – Physiologic process
– Pathologic process
• High level: Neurologic complication
• Common in perinatal period
Conjugated : Direct bilirubin
• Greenish yellow
• Direct BB > 2 mg%
• Direct BB > 20 % of TB
• Always pathologic process
– Mostly liver and biliary system
• Long-term: Liver damage
• Uncommon in perinatal period
สาเหตของ Unconjugated hyperbilirubinemia
• สาเหตทพบบอย (ในประเทศไทย) –Physiologic –ABO incompatibility –G6PD –Breast feedings –Breast milk jaundice
• สาเหตทควรทราบ –Polycythemia –Large hematoma –Hypothyroidism –Rh / Minor bl gr incompatible –Congenital infections –Sick infants : sepsis, asphyxia

Physiologic jaundice • Physiologic natural history 1. Jaundice after 24 hours
2. Direct bilirubin less than 2 mg%
3. Maximum level
1. TB 12 mg% in term-White
2. TB 16-18 mg% in term-Thai, SEA
4. Day of Maximum bilirubin
1. Term 4-5 DOL (days of life)
2. Preterm 6-7 DOL
3. Thai newborn 6-10 DOL
5. Duration of jaundice
1. less than 14 DOL in formula feed
2. Less than 21 DOL in breast feed
-It is the most common cause of indirect hyperbilirubinemia in perinatal period
• Factors effect physiologic jaundice
1. Gestational age
2. Feeding: Type of milk Volume of milk intake
3. Race:
Higher:SEA
Lower : White, Black
4. Diabetic mother
-Most of physiologic jaundice will do no harm
-Physiologic jaundice may do harm in certain conditions: preterm, sick neonates

Hemolytic disease of the newborn Isomimmunization
• Positive antiglobulin test (DAT, Coombs test, Coombs’test) – Direct coombs’ test: antibody detect on RBC – Indirect coombs’test: antibody detect in serum
• ABO hemolytic disease of the newborn
• Rh hemolytic disease of the newborn (erythroblastosis fetalis)
• Others blood group

ABO hemolytic disease of the newborn
Blood group O Mother who has IgG subclass antibody

ABO hemolytic disease of the newborn ABO-HDN
• Most common cause of immune hemolytic disease in newborn
• Milder than Rh HDN
• Early onset, mild to moderate jaundice and anemia
• Innate antibody IgG subclass
• Can occur in first pregnancy
• Coombs’test +ve or –ve
(Indirect > Direct coombs’)
• Criteria for DX
1. Jaundice usually in first 24 hours
2. Mother: O,
Infant: A/B
3. Microspherocyte and polychromasia on blood smear
4. Increase reticulocyte count
5. Evidence of hemolysis



Rh hemolytic disease of the newborn Rh-HDN
• NOT common in Thailand
• Antigen in Rh: D,d C,c E.e
• Rh positive= D antigen, No
innate anti D antibody)
• Early onset, severe jaundice and anemia
• Severe anemia >>Hydrops fetalis, Erythroblastosis fetalis, extramedullary hematopoiesis
• Mother: Rh positive
Infant: Rh negative
• Coombs’test +ve (Direct >Indirect coombs’)
• Pregnancy after sensitized – Transfusion of Rh positive
blood
– Abortion
– Invasive prenatal diagnosis
– Delivery
• Preventable by IV Rhogam (Human anti D immunoglobulin) during pregnancy and after delivery



Extramedullary hematopoiesis (in rubella syndrome)
Hydrops fetalis
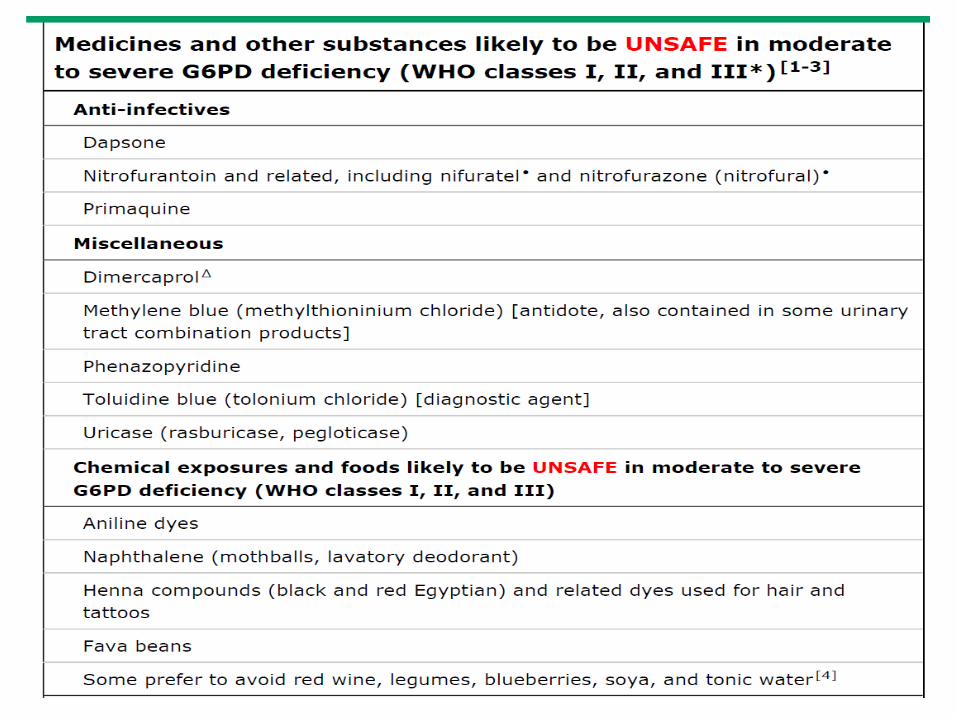
G6PD deficiency
• X linked disorder, DAT test negative, The most common enzymatic disorder of RBC
• Neonatal jaundice may be caused by – Hemolysis – Defect in conjugation
• Onset could be early or late • Causes of hemolysis may not be found • G6PD test: positive or falsely negative
• If hemolysis : Non immune hemolytic anemia
– Decrease Hct and high reticulocyte count – Fragmented RBC/ blister cell
• If no hemolysis : – normal blood smear and Hct – Normal reticulocyte count


Bite cell Eccentrocyte



unconjugated hyperbilirubinemia after the second weeks of life
• Common – Breast milk juandice
• Treatable, important – Congenital hypothyroid
• Gut obstruction: pyrolic stenosis • Trisomy 21st • Rare genetics
– Gilbert syndrome – Crigler-Nijjar syndrome type 1 – Crigler-Nijjar syndrome type 2

Breast-feeding juandice • Breast-feeding failure juandice • Onset first 2-6 days of life • Cause by in adequate intake>> increase
enterohepatic circulation • Diagnostic clues
– Breast feeding with limited milk supply – Excessive post natal weight loss – Stool and urine frequency less than normal – Delay meconium elimination
• Prevent by early and frequent effective breast feeding
Breast milk juandice
• Incidence 1:200 • Onset after the first 5-7 days of life • Healthy appearance, good weight gain, breast-feeding baby • Common cause of Indirect hyperblirubinemia during after 2
weeks to 2 -4 months • Genetics susceptibility in SEA, G6PD related to
polymorphism of UGT1A1 gene • Non esterified long chain fatty acid, progesterone
metaboite in breast milk may suppress conjugation of bilirubin
• Beta glucuronidase in breast milk may increase enterohepatic circulation

Congenital hypothyroid
• Incidence 1:5000-6000
• Prolong, exaggerated juandice
• Impair uptake , reduce hepatic ligandin
• Decrease conjugation, suboptimum UGT activity
• All infants with prolong unconjugated hyperbilirubinemia more than normal duration must have thyroid function test. (TSH,T4)

Crigler Najjar, Gilbert, Lucey Driscoll
• Crigler Najjar type 1 – Severe , rare AR hereditary – Absent hepatic UGT activity – Mutation at coding area of UGT1A1 gene: not
functioning enzyme – Severe, early onset, unremitting, TB>20 mg% – No Hemolysis, disorder of conjugation – Not rsponse to phenobarbital – Phototherapy and exchange transfusion for liver
transplantation – Poor prognosis

Crigler Najjar, Gilbert, Lucey Driscoll
• Crigler Najjar type 2 (Arias disease) – More common than type 1, AR and AD hereditary
– Life long low hepatic UGT activity
– Mutation at promotor area of UGT1A1 gene: decrease enzyme activity
– early onset, unremitting, TB <20 mg%
– No Hemolysis, disorder of conjugation
– Phototherapy and response to phenobarbital
– better prognosis

Bilirubin toxicity
• Acute bilirubin encephalopathy: Reversible – Early clinical signLethargy with high bilirubin level, Absent/diminsh
Moro reflex (usually > 20 mg%) – Early Laboratory sigh: Abnormal brain stem evolked response
• Acute Permanent bilirubin toxicity (Kernicterus) – Onset progress within 24 hours – Phase 1:Poor sucking, hypotonia,depressed sensorium – Phase 2:Fever, Retrocolis, hypertonia, Opisthotonos – Phase 3:High pitch cry, hearing impaired, athetosis
• Chronic classic sign of Kernicterus – Choreoathetoid cerebral palsy, Upward gaze palsy – Sensory neural hearing loss – Dental dysplasia in infancy – Intellectual may be spare

Bilirubin Encephalopathy / Kernicterus causes by indirect bilirubin NOT direct bilirubin
Putamens and caudate nucleus
Assessment of jaundice infant : History taking
Mother’s history Gravida , Para , Gestational age Blood group, VDRL, anti HIV Illness during pregnancy eg. DM, TORCH Medication during pregnancy eg, sulfa Type of delivery and complication Family history Neonatal jaundice in sibling Blood and liver disease in family

Assessment of jaundice infant: History taking
Infant’s history Age in hours NOT in days Apgar score Birth weight Infant well being after birth Feeding : breast or bottle , adequate amount ? Stool/ urine : frequency , amount, color
Assessment of jaundice infants: Physical exam
General appearance : signs of bilirubin encephalopathy Body weight : term newborn loss 6-8% preterm loss 10-15% Extravascular blood : cephalhematoma, ecchymosis Polycythemia / anemia Dermal icteric zone : limited value Hepatosplenomegaly Evidence of congenital infection Evidence of hypothyroidism
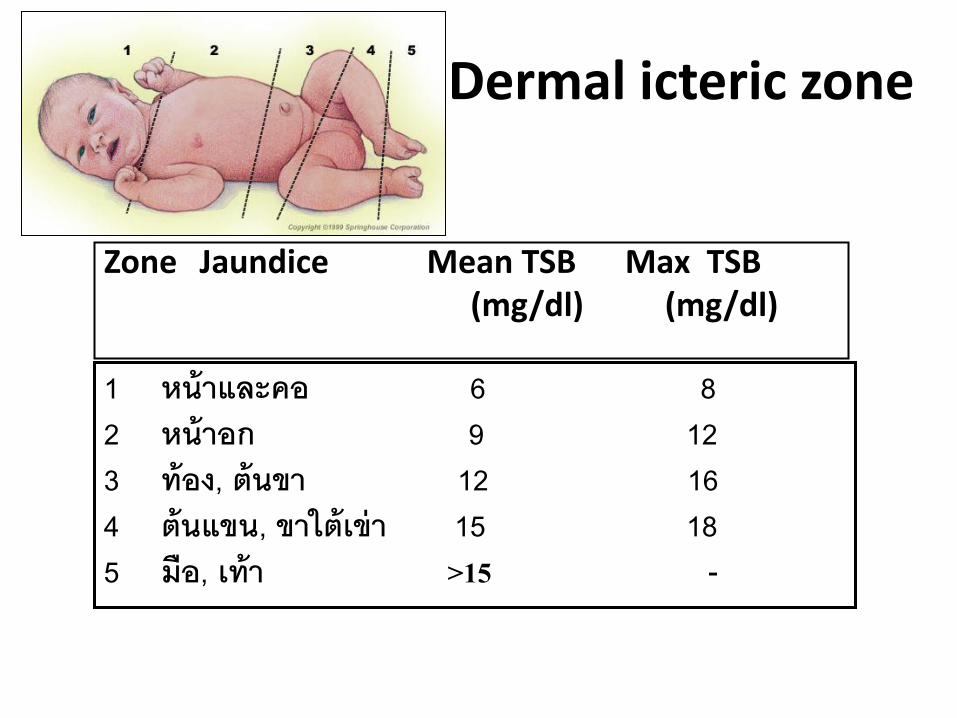
Dermal icteric zone
Zone Jaundice Mean TSB Max TSB (mg/dl) (mg/dl)
1 หนาและคอ 6 8 2 หนาอก 9 12 3 ทอง, ตนขา 12 16 4 ตนแขน, ขาใตเขา 15 18 5 มอ, เทา >15 -

Lab investigation 1. ABO and Rh blood group : Mother & Infants
2. Coombs’ test : Mother & Infants
3. G6PD
4. Evidence of hemolysis or blood loss
Hct, Blood smear, Reticulocyte count
5. Bilirubin level
Microbilirubin, Total bilirubin, Direct bilirubin

Diagnostic approach
Polycythemia: Hct>65% Anemia: Hct<45% Normal RC: see table


Management 1. Phototherapy
Change indirect bilirubin to nontoxic,water soluble form
2. Exchange transfusion
Remove indirect bilirubin from blood
3. Medication eg. IVIG, Metalloporphyrins, Phenobarbital

Infant GA > 35 weeks : guidelines for phototherapy
Risk factors : hemolysis, G6PD def, asphyxia, significant lethargy, temp instability, sepsis, acidosis, albumin < 3 g/dL

Infant GA > 35 weeks : guidelines exchange transfusion
Risk factors : hemolysis, G6PD def, asphyxia, significant lethargy, temp instability, sepsis, acidosis

Infant GA < 35 weeks : management

Phototherapy

Phototherapy
• Indications – Hyperbilirubinemia consider from TSB
• Contraindications – Congenital porphyria: Bullous eruptions, agitation – Concomitant use of photosensitive drugs: Photosensitivity – Therapy with matalloporphyrin: Transient erythrema – Cholestasis jaudice: Bronze baby syndrome

Phototherapy
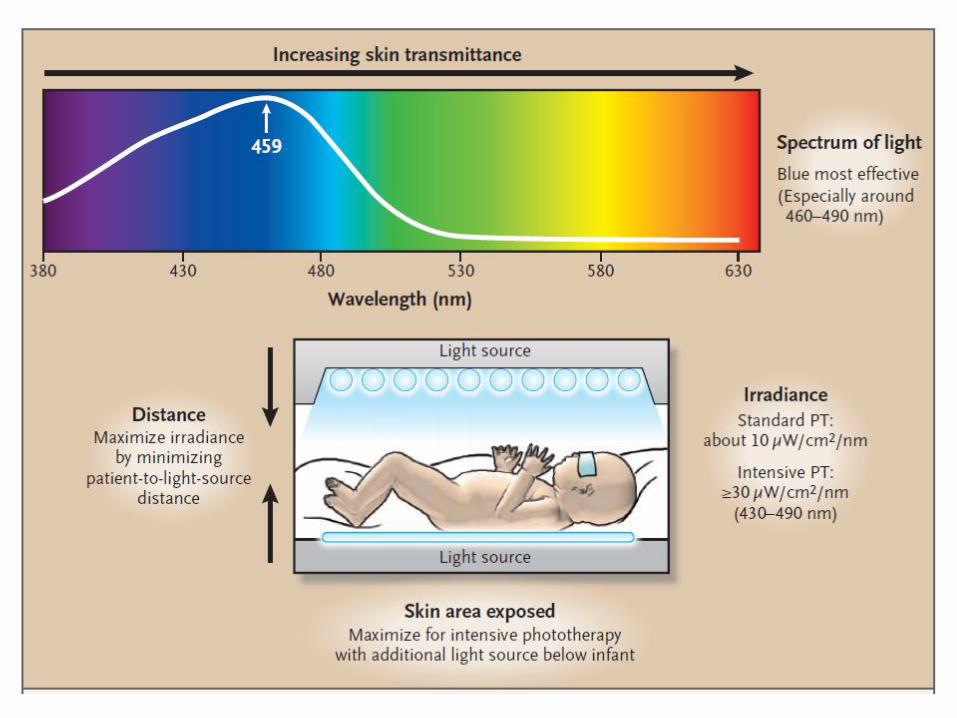
• Spectral qualities of the delivery light
– Bilirubin absorbs light: wavelength range 400-500 nm
– Peak absorption at 450-470 nm
– Best effective wavelegth 460-490 nm ( better skin prenetration)
• Irradiance (intensity of light)
– Spectral irradiance: irradiance at effective wavelength
– Micro W/cm2/nm
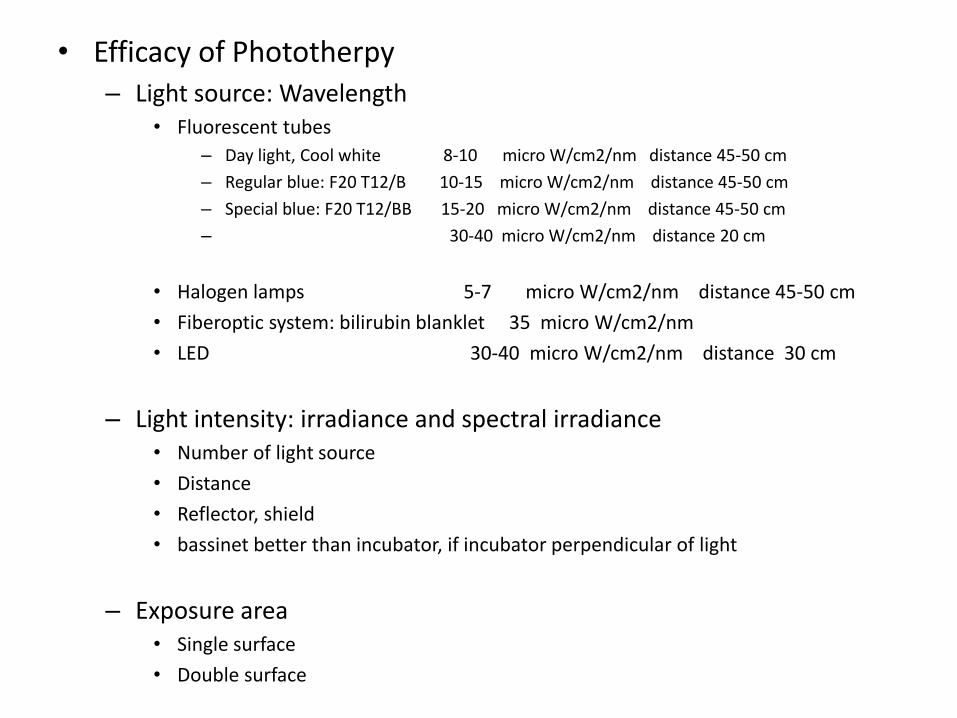
• Efficacy of Phototherpy – Light source: Wavelength
• Fluorescent tubes
– Day light, Cool white 8-10 micro W/cm2/nm distance 45-50 cm
– Regular blue: F20 T12/B 10-15 micro W/cm2/nm distance 45-50 cm
– Special blue: F20 T12/BB 15-20 micro W/cm2/nm distance 45-50 cm
– 30-40 micro W/cm2/nm distance 20 cm
• Halogen lamps 5-7 micro W/cm2/nm distance 45-50 cm
• Fiberoptic system: bilirubin blanklet 35 micro W/cm2/nm
• LED 30-40 micro W/cm2/nm distance 30 cm
– Light intensity: irradiance and spectral irradiance • Number of light source
• Distance
• Reflector, shield
• bassinet better than incubator, if incubator perpendicular of light
– Exposure area • Single surface
• Double surface

Phototherapy
• Standard phototherpy
• Intensive phototherpy – Wavelenght 430-490 nm – Spectral irradiance >30 micro W/cm2/nm – Greatest body area exposure
• Distance as close as posible to infant : light type • Surface of exposure: double surface • Reflector, clear glass shield • Ventilation and monitor phototherpay unit
• Efficacy
– Evident within 4-6 hours – Reduce more than 2 mg/dl
Phototherapy
• Complications of Phototherapy
– Bronze baby syndrome
– Diarrhea or loose stools
– Dehydration
– Skin rash: erythrema, increased pigmentation, burn, blistering
– Retinal damage
– Interfere mother and infant bonding, separation which may increase risk of breast feeding failure


Exchange Transfusion
• Total exchange transfusion:
– Blood volume
• Term newborn 80 ml per kg
• Preterm newborn 100 ml per kg
– Double volume exchange transfusion
• Weight (Kg) x 80-100 ml (per Kg) x 2

Exchange Transfusion
• ABO hemolytic disease of the newborn
• Choice of Blood for exchange Transfusion
– PRBC: O and cross match mother ’s blood
– FFP: AB or infant ‘s blood group
– Fresh whole blood group O is less prefer than PRBC+FFP
– Newly collected blood, less than 5-7 days.

Exchange transfusion
• Complications: – Death or permanent sequele risk less than 1%, sick NB
12%
– CVS: Apnea/Brady cardia/Tachycardia/acidosis/ vascular spasm
– Electrolyte, Hematologic, Metabolic complications
– Complication related to blood and catheter
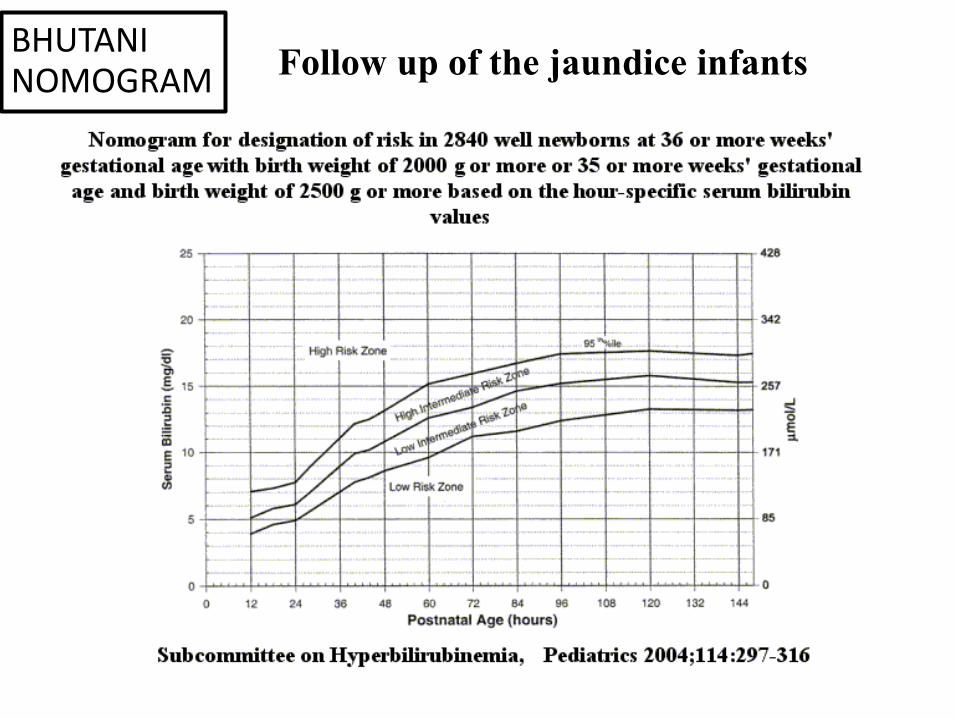
Follow up of the jaundice infants BHUTANI NOMOGRAM