Peri operative arrhyth
89
Perioperative Arrhythmias Dr K.K.KISHORE
-
Upload
krishna-kishore -
Category
Health & Medicine
-
view
38 -
download
1
Transcript of Peri operative arrhyth

Perioperative Arrhythmias
Dr K.K.KISHORE

Definition- “Abnormality of cardiac rate, rhythm or conduction
which can be either lethal (sudden cardiac death), or symptomatic (syncope, near syncope, dizziness, or palpitations) or asymptomatic”.
Dysrhythmias represent an important cause of perioperative complications because during this period there are several clinical situations that may trigger changes in cardiac rhythm.
Most perioperative dysrhythmias are benign, without significant hemodynamic consequences.

Incidence- Seen in 70.2% of patients subjected to general
anaesthesia for various surgical procedures. Varies from patients undergoing cardiac or non-
cardiac surgery as well as on monitoring modality.
Incidence varies from16.3 to 61.7%with intermittent ECG monitoring & 89%with continuous holter monitoring in patients undergoing non-cardiac surgery,
In patients undergoing cardiac surgery - reported incidence of > 90%.

Action Potentials Dysrhythmias are secondary to changes in cardiac ion
channels (sodium, calcium, and potassium channels) and adrenergic receptors are the targets.
Phase 0-initiates the conduction in the cardiac tissue. In atria and ventricles the impulse originates in the
sodium current. In the sinoatrial (SA) and atrioventricular (AV) nodes
phase 0 is produced by calcium current. Phases 1- represent repolarization, Phase 2- plateau (maintained by calcium current)
and Phase 3- is maintained by potassium current. During Phase 4- nodal cells undergo spontaneous
depolarization while atrial and ventricular tissues are hyperpolarized.


Pathogenesis 1. Injury or damage (pathology) to the
cardiac conduction systems. 2. Re-entry: Reentry is a mechanism that may
precipitate a wide variety of supraventricular and ventricular arrhythmias.
3. Automaticity: Abnormal depolarization of atrial or ventricular muscle cell during the periods of action potential can lead to arrhythmias.
4. Mutations in ion channels: Since these channels are mainly responsible for depolarization, mutation can lead to arrhythmias.
5. Ectopic foci/ irritable foci

Automaticity Automaticity refers to abnormal atrial or ventricular
depolarization during the repolarization (phases 2 or 3) or resting (phase 4) period of the action potential.
Some molecular substrates, such as prolongation of the QT interval and low potassium (K+) concentrations can trigger automaticity.
Mutations in ion channels responsible for repolarization, and that can prolong it, make cardiac cells more sensitive to dysrhythmias
Factors that increase automaticity include increased activity of the sympathetic nervous system, hypokalemia, hypomagnesemia, catecholamines, digoxin, hypoxemia, and atrial and ventricular dilation
Re-Entry
Three factors must be present for reentry to occur: 1) presence of two conduction pathways; 2) unidirectional blockade of one of the pathways
prevents progression of the impulse, but is allows retrograde conduction; and
3) reduced impulse velocity in one of the pathways giving time for the other pathway to depolarize.
Reentry is the mechanism of several supraventricular and ventricular dysrhythmias implying the presence of a pathologic circuit of electrical impulse around a functional or anatomic loop, which is seen in Wolff-Parkinson-White syndrome (WPW).
Ischemia also predisposes the development of reentry tachycardia.

UnidirectionalBlock
Recovery of Excitability & Reentry
BidirectionalConduction
Mechanism of Reentry

Drugs that terminate reentry do this by two mechanisms:
1.Suppression of the current responsible for phase 0 of the action potential that prolongs or blocks conduction in the reentry pathway, interrupting the dysrhythmia.
2. Drugs that prolong the action potential (with K+-channel blocking properties) prolong cellular and reentry circuit refractory period, blocking propagation of impulses through the circuit.
The main mechanism of monomorphic VT is also reentry around the infarcted myocardium.

Causes Hypovolemia Hypoxia Hypo/Hyperkalemia Hypomagnesaemia / Hypocalcaemia Hypoglycemia Hypothermia Acidosis Mechanical Irritation (e.g. central
venous lines, pulmonary art.
catheter, chest tube)
Cardiac ischaemia Light plane of
anaesthesia/pain Toxins/ Drugs Tamponade, Cardiac Tension pneumothorax Thrombosis (Coronary or
pulmonary) Trauma Surgical cause (Traction to
intestine, oculocardiac reflex, neurosurgical causes, cardiac compression on beating heart bypass surgery etc.)

These factors can grossly be divided into following categories:
1. Patient related factors 2. Anaesthesia related factors 3. Surgery related factors

1. Patient related factors- a. Preexisting cardiac disease b. Central nervous system disease - Patients
with intracranial disease especially SAH may show ECG abnormalities- changes in QT intervals, development of Q waves, ST-segment changes, and occurrences of U waves.
c. Old age - Postoperative atrial fibrillation (AF) is a frequent complication in the elderly patients undergoing thoracic surgery.Aging causes degenerative change in atrial anatomy and is also accompanied by relative changes in atrial pathology.
2.Anaesthesia related factors- a. Tracheal intubation – It is one of the most
commonest causes of arrhythmias during induction as well as during the perioperative period, most often associated with haemodynamic disturbances.
b. General anaesthetics – The drugs used for induction, maintenance as well as for reversal of general anaesthesia are not primarily arrhythmogenic, but arrhythmias can be produced in the presence of a variety of triggering agents and clinical situations generating high catecholamines such as light plane of anaesthesia with hypertension and tachycardia,hypoxaemia, hypercarbia, exogenous epinephrine and aminophylline.
Halothane or enflurane produces arrhythmias, probably by a reentrant mechanism.

c. Local anaesthesia – Parasympathetic nervous system predominance →
bradyarrhythmias. d. Electrolyte imbalance and abnormal arterial
bloodgases – hypercarbia, hypoxaemia or electrolyte imbalance produce arrhythmias either by producing reentrant mechanism or by altering phase depolarization of conducting fibers.Hypokalemia or hyperkalemia may also lead to arrhythmias.
e. Central venous cannulation – Stimulation of carotid sinus reflexes may occur due to pressure from fingers during jugular vein cannulation as excess insertion ofthe central venous catheter into the right atrium during centralvenous cannulation may also lead to arrhythmias.

3. Surgery related factors- a. Cardiac surgery – A spectrum of cardiac
arrhythmias can be observed during the immediate period following the release of aortic cross clamp when myocardium is recovering from the ischaemic insult and regaining normal sinus rhythm. Surgical manipulation such as retraction of the heart during operation on beating heart, venous cannulation or taking sutures over the atrium can also precipitate arrhythmias.
b. Non-cardiac surgery –Vagal stimulation due to traction on the peritoneum or direct pressure on the vagus nerve during carotid artery surgery may produce bradycardia or atrioventricular (AV) blocks, or even asystole.
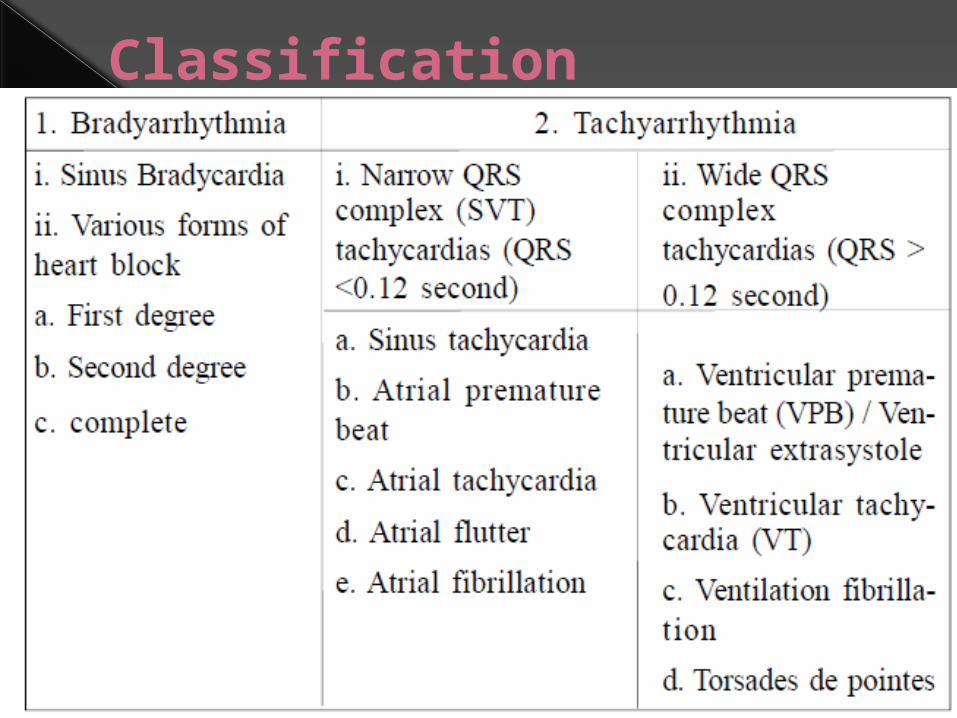
Classification

Bradyarrhythmias a.Sinus Bradycardia- HR ≤ 60 beats per minute. In patients on chronic beta-blocker therapy as in
(CAD)- heart rate ≤ 50 beats/min. Causes- 1. Drug effects: β blockers, digitalis and other
anti-arrhythmic drugs 2. Acute myocardial ischaemia 3. Hypothermia 4. Underlying hypothyroidism, cholestatic
jaundice or raised intracranial pressure. 5. Chronic degenerative change such as fibrosis
of the atrium and sinus node.

Treatment: Asymptomatic bradycardia -does not require treatment. Symptomatic bradyarrhythmias - Atropine- 0.5 to 1.0 mg (IV bolus), repeated every 3 to 5 minutes, if required (maximum dose =
0.04 mg.kg-1). Should be used cautiously in patients with CAD, since
excessive increase in heart rate may worsen ischaemia because of increased myocardial oxygen consumption or reduced diastolic filling time.
Still persists- Isoprenaline can be administered as an IV bolus of 5 to 10 μg followed by an infusion of 2 to 10μg.min-1.
Other alternative is dopamine infusion 5 to 20μg.min-1. While treating sinus bradycardia, various causes or factors
contributing should be searched and treatment started. Be ready for percutaneous and transvenous pacing.

Heart blocks- (AVHB) are broadly classified into three
categories- a) First degree heart block b) Second degree heart block c) Complete heart block May be transient or permanent. Transient AVHB can be produced by acute MI
and general anaesthetics such as enflurane or halothane in patients using calcium channel blocker drug (CCB) or amiodarone.
Permanent AVHB-usually idiopathic, other causes CAD and Lev’s or Lenegre disease, where fibrosis of the conducting system occurs.

1st Degree Heart Block- This is simple prolongation of the PR interval >
0.22 sec. Every atrial depolarization is followed by conduction
to the ventricle but with delay. The treatment is usually not necessary however,
the patients should be carefully observed for progression to a higher degree of block, that requires prompt treatment
2nd Degree Heart Block- In "classic" Type I (Wenckebach) AV block the
PR interval gets longer (by shorter increments) until a nonconducted P wave occurs.
In Type II (Mobitz)AV block the PR intervals are constant until a nonconducted P wave occurs. There must be two consecutive constant PR intervals to diagnose Type II AV block .


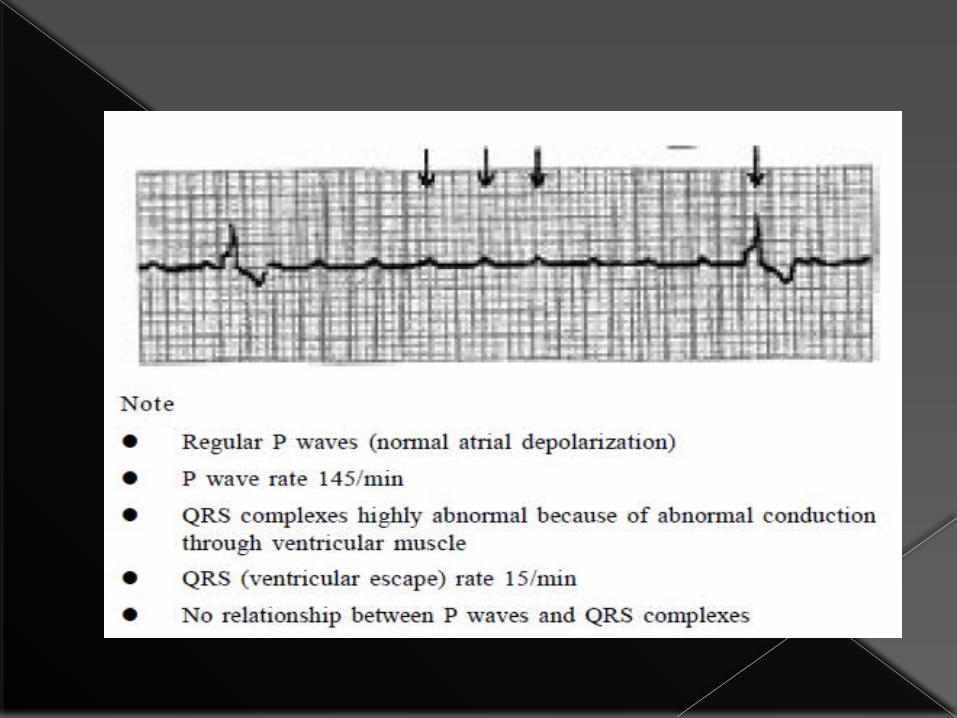
3rd Degree Heart Block- Complete AV dissociation because the atria
and ventricles are each controlled by separate pacemakers.
Based on the QRS rhythm –Narrow/Wide QRS rhythm
Narrow complex: This is due to disease in the AV node or the proximal bundle of His.
The escape rhythm occurs with an adequate rate (50-60 b.p.m.) and is relatively reliable.
It occurs because of inferior wall MI and toxic concentration of drugs such as digitalis, verapamil or βblockers in perioperative period.

Broad complex: Occurs because of disease in the Purkinje system.
The escape pacemaker arises from the distal Purkinje network or the ventricular myocardium.
Rhythm -slow (15-40 b.p.m) and relatively insignificant or unharmful.
In the elderly- usually caused by degenerative fibrosis and calcification of the distal conduction system (Lenegre’s disease) or the more proximal conduction system (Lev’s disease).
It may occur after closure of ventricular septal defect (VSD) and sometimes following aortic valve replacement (AVR).
In younger patients, broad complex AV block may be caused by perioperative myocardial ischaemia.

Management - Treatment is not required in narrow complex
3° block except for eradication of toxic causes. Occasionally, permanent pacing is advocated for
symptomatic, isolated AVblock. While in broad complex, pacing is indicated
to maintain the normal haemodynamics.


Tachyarrhythmias

Definition- Supraventricular tachycardia can be defined as
sustained, non-sinus related, acceleration of the cardiac rhythm, originating above the AV node.

Narrow QRS complex (QRS<0.12)
a. Sinus tachycardia- HR > 100 beats/minute. Prolonged tachycardia for long duration can induce
ischaemia in CAD patients. Causes- Anaemia because of blood loss Pain Inadequate anaesthesia Hypovolaemia Fever Hypercarbia Thyrotoxicosis/ thyroid crisis Cardiac failure with compensatory sinus tachycardia Catecholamines excess

Treatment: Precipitating factors must be identified and
corrected. Drug therapy -especially required in patients with
ischaemic heart disease who develop ST segment changes to prevent further myocardial ischaemia.
Beta-blockers -Esmolol is preferred drug . It has half-life of 10min with bolus dose of 500
mcg.kg-1 over 1 min, Followed by an infusion of 50-300mcg.kg-1.min-1. If continuous use is required-longer lasting cardio
selective drugs such as Metoprolol in the dose of 5 to 10mg given slowly intravenously (IV) at 5min interval to a total dose of 15 mg.
Another drug - Propranolol 0.1 mg.kg-1.

Recently, Landiolol has been introduced into clinical practice in some countries.
β-blocker whose cardioselective properties are greater than the esmolol and has a shorter half-life (2 to 4 minutes), as it is rapidly hydrolyzed by plasma esterases.
Dexmedetomidine 0.3 mg.kg-1 used to treat persistent sinus tachycardia resistant to treatment with esmolol and suggested that this drug could be useful in patients with bronchospasm and tachycardia
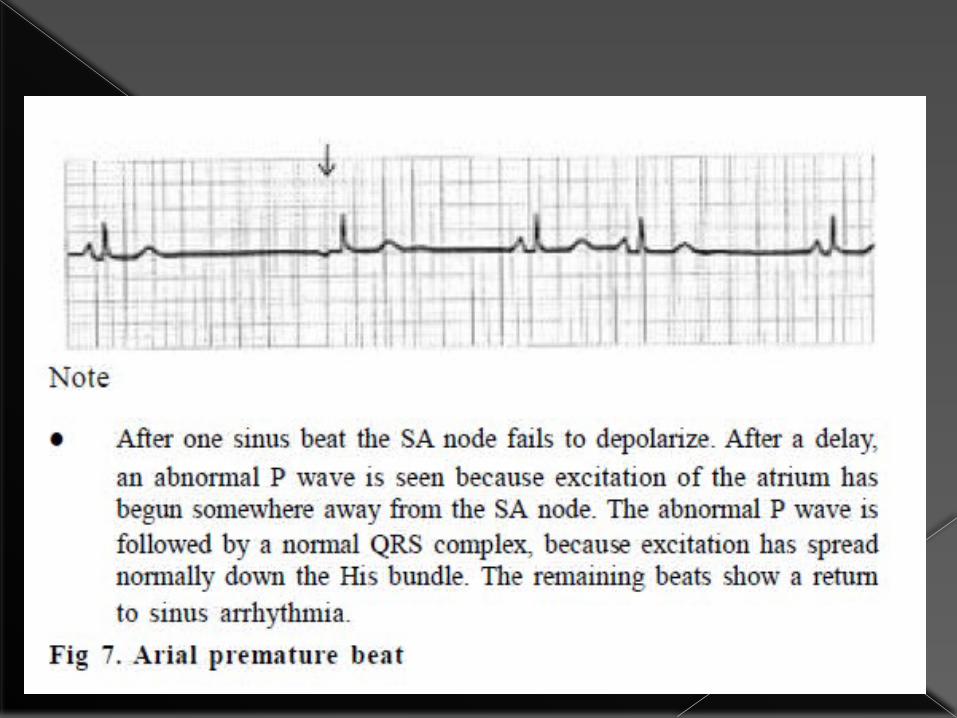
b.Atrial premature beat- Represents 10% of all intraoperative
arrhythmias. ECG -appear as early and abnormal ‘P’
waves and are usually but not always, followed by normal QRS complexes.
Duration of QRS wave- normal but wide QRS wave may be present due to aberrant ventricular conduction, which mimics premature ventricular beat.
Treatment- Not normally required unless the ectopic
beats provoke more significant arrhythmias, where βblockade may be effective.
c.Atrial tachycardia: Found in 6% of patients undergoing non cardiac
surgery. It is nonparoxysmal, narrow QRS rhythm with
retrograde or nonapparent P waves and a rate <70 beats/min
If faster usually <130 beats/min, it is termed as acceleratedAV junctional rhythm.
Those arrhythmias can lead to fall in blood pressure upto 15%in patients without cardiac disease and upto 30%in diseased heart.


Treatment- Usually no treatment is required; Carotid sinus massage and verapamil are
often helpful in symptomatic patients. IV adenosine in 6 to 12 mg doses is another
alternative. Treatment with class Ia, Ic or III drugs is
usually successful e.g.disopyramide 2mg.kg-1 over 10min.

d.Atrial flutter- Usually associated with organic ischaemic heart
disease. Atrial rate varies between 280 and 350min-1 but
is usually around 300min-1. Most often every second flutter beat conducts
giving a ventricular rate of 150 min-1. Occasionally every beat conducts, producing a
heart rate of 300min-1. ECG: The ECG shows regular saw tooth-like
atrial flutter waves between QRST complexes. If they are not clearly visible,AV conduction may be
transiently impaired by carotid sinus massage or by the administration of AV nodal blocking drugs such as verapamil.

Treatment: Treatment of an acute paroxysm is electrical
cardioversion. Prophylaxis is achieved with class Ia, Ic or III
drugs in diseased heart patients.
e.Atrial fibrillation (AF) It accounts for > 90% of supraventricular tachycardia (SVT) in
the perioperative setting. Causes- Raised atrial pressure, increased atrial muscle mass, atrial
fibrosis or inflammation and infiltration of the atrium. Rheumatic disease often associated with cardiac causes
such as mitral valve disease, myocarditis and coronary artery disease.
Systemic diseases include hyperthyroidism, pulmonary embolism and electrolyte imbalance.
Can be seen in up to 60% of adult patients undergoing myocardial revascularization, and it usually peaks on the third postoperative day when inflammatory response is greater.
When caused by rheumatic mitral stenosis, the onset of atrial fibrillation results in considerable worsening of cardiac failure.

Clinically the patient has a very irregular pulse, as opposed to a basically regular pulse with an occasional irregularity (extrasystoles) or recurring irregular pattems.
ECG -fine oscillations of the baseline (so called fibrillation) and no clear P waves.
QRS rhythm is usually 160-180min-1 but it slows with treatment.
ECG changes are more indicative in lead II . AF may be acute or recent onset (<48 hrs) and
chronic


Treatment- In the recent onset AF, initial treatment is directed
towards the control of ventricular response rate with agents that slow AV node conduction.
The precipitating or provoking agents should be removed or treated first.
Intravenous beta blockers or calcium channel blockers produce rapid control of rate, regardless of the level of sympathetic tone.
However beta-blockers are preferred over calcium channel blocker (CCB) during intraoperative period due to shorter duration of action and lesser negative inotropic effects.
Amiodarone can also be effective after cardiac surgeries
Class Ic or III antiarhythmics can be used

If haemodynamically unstable- DC cardioversion is the most effective method of converting AF to sinus rhythm.
ChronicAF is often found in patients with rheumatic heart disease undergoing cardiac surgery and may have atrial thrombi, therefore, any attempt to restore sinus rhythm by DC cardioversion may be associated with increased risk of systemic or pulmonary embolisation.
Successful cardioversion is relatively rare in chronic AF.
The control of ventricular rate is the preferred approach in these cases.

The most useful drug for chronic AF is digoxin. The patients with chronic AF undergoing
noncardiac surgery should be evaluated for the presence of atrial clot by echocardiogram prior to surgery.
In the presence of atrial clot, control of ventricular response rate with appropriate medication is instituted during perioperative period, if necessary.
Statins have been tested in the preoperative period to reduce the incidence of peri- and postoperative AF

When deciding for perioperative elective electrical cardioversion that initially an attack dose of an antiarhythmic agent should be administered to minimize the recurrence of SVT after the shock.
Adenosine is the drug of choice to treat SVTs involving the SA or AV node (6 mg IV rapid flush, which can be repeated as 12 mg bolus), important especially in cases of node reentry, which is not the main mechanisms of perioperative SVTs.

Wide QRS complex (QRS>0.12)
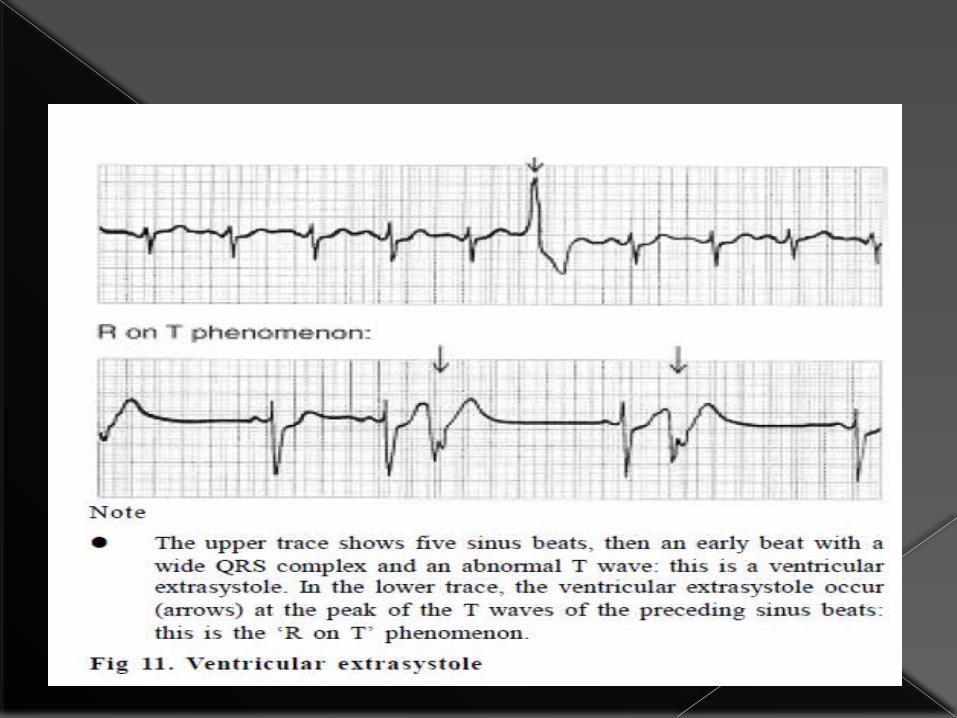
a.Ventricular premature beat (VPB)-
VPB results from ectopic foci arising from below AV node and give rise to wide (>0.12 sec) bizarre QRS complex.
More common in anaesthetized patients with pre existing cardiac disease.
New onset of VPB, may occur in the presence of coronary artery insufficiency, myocardial infarction, digitalis toxicity with hypokalemia and hypoxaemia.
ECG -broad (>0.125) and bizarre QRS complex because it arises from an abnormal (ectopic) site in the ventricular myocardium.

Treatment: Underlying abnormalities in these patients should be
corrected immediately. No treatment is generally required for isolated VPB
in asymptomatic and healthy patients. However VPB which are multiple (>5 beats/min),
multifocal, or bigemminal or occur near the vulnerable period of the preceding ventricular repolarization (the so called R on T phenomenon), associated with haemodynamic disturbance or convert to worse arrhythmias require prompt treatment.
Lidocaine- initial bolus dose of 1.5mg.kg-1 followed by infusion of 1 to 4 mg.min-1 can be given.
Other drugs from class I, II or III are used to treat these types of arrhythmias.
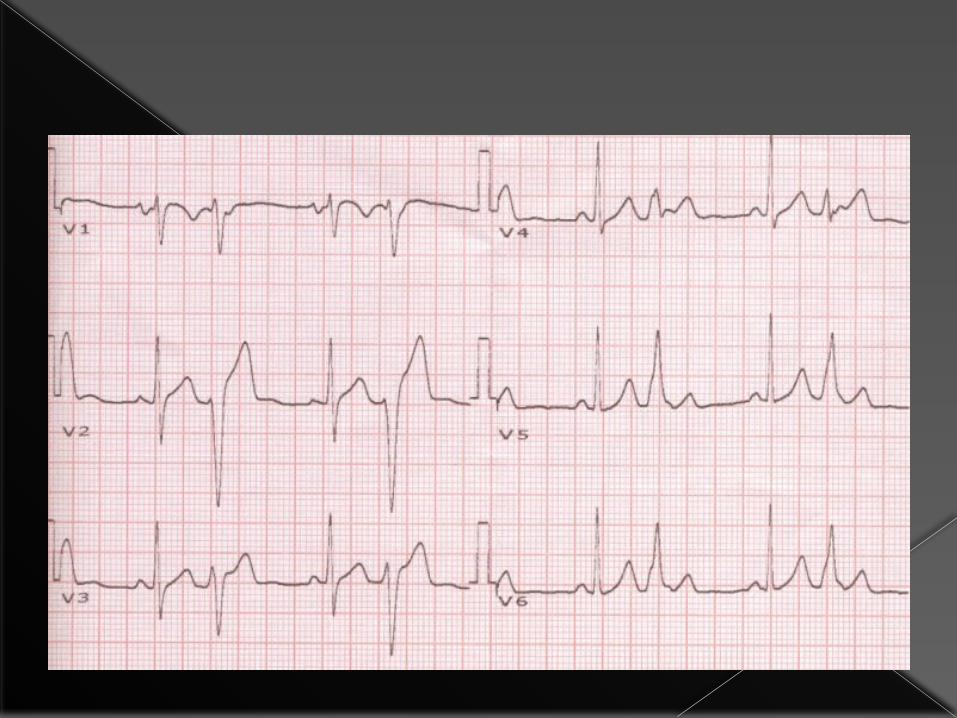
b.Ventricular tachycardia- Defined as three or more ventricular beats occurring
at a rate of 120 bpm or more lasting 30 seconds or less without hemodynamic compromise
It may be potentially and life threatening. Can be divided according to their morphology
(monomorphic or polymorphic) and duration (sustained or non-sustained).
Main mechanism of monomorphic VT -formation of a reentrant pathway around a tissue scar of a healed myocardial infarction.
In monomorphic VT the amplitude of the QRS complex is constant,
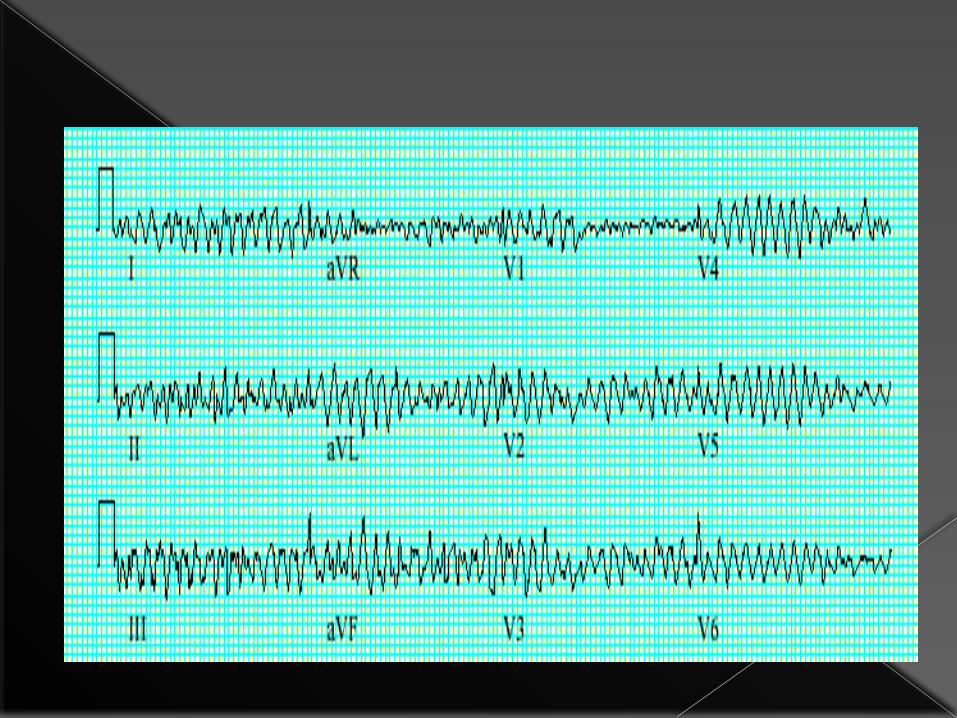
In polymorphic VT the morphology of the QRS changes continuously.

NSVT is a common perioperative occurrence and in the absence of cardiac disease it does not require treatment.
In patients with cardiopathies this non-sustained rhythm can predict malignant ventricular dysrhythmias.
The main strategy- prevention, instituting immediate treatment when possible risk factors arise.
A study of patients undergoing cardiac surgery demonstrated that correction of magnesium after ECC reduced the incidence of non-sustained VT.

Examination reveals pulse rate of 120-220bpm. The ECG shows a rapid ventricular rhythm with
broad (often 0.14s or more), abnormal QRS complexes.
Dissociated P waves activity may be seen and have no fixed relation to wide QRS complex.



Monomorphic VT

V1
Polymorphic VT

Treatment : May be urgent depending on the haemodynamic
situation. If the cardiac output and the blood pressure are very
depressed, emergency DC cardioversion must be considered.
On the other hand, if the blood pressure and cardiac output are well maintained, intravenous therapy with class I drugs is usually advised.
First-line drug treatment consists of lidocaine (50-100mg i.v. over 5 min) followed by a lidocaine infusion (2-4 mg.min-1 i.v.).
DC-cardioversion may be necessary if medical therapy is unsuccessful.
The administration of multiple antiarrhythmic drugs should be avoided.

Patients with recurrent episodes or unresponsive to lidocaine,may require therapy with
Procainamide (10-15 mg.kg-1 loading dose followed by an infusion of 2 to 6 mg.min-1) or
Bretylium (5 to 10 mg.min-1 over 2 to 5 min then infusion of 1-2 mg.min-1) or
Amiodarone in the dose of 150 mg IV over 10 minutes followed by an infusion of 1 mg.min-1 for 6 hours and 0.5 mg.min-1 thereafter.
IV amiodarone has been shown to be as effective as bretylium with added advantage of less hypotension as compared to IV bretylium.

C.Ventricular fibrillation (VF) It is very rapid and irregular ventricular
activation with no mechanical effect. It is usually intiated from an ischaemic
myocardium or an aberrant foci (especially in acute perioperative myocardial infarction), ventricular tachycardia or torsades de pointes.
On ECG, there are no defined QRS complexes, shows shapeless rapid oscillations and on pulse oximetry, there is acute fall in SpO2 because of low or no cardiac output.
Causes include myocardial ischaemia, hypoxaemia, electrolyte imbalance and drug effects.

Treatment: Cardiopulmonary resuscitationmust be
performed as rapidly as possible. Asynchronous external defibrillation should be
performed using 200-360J. A precordial thump is occasionally effective in
terminating VF, but should be attempted only if a defibrillator is not available immediately.
Intravenous bretyium5-10mg.kg-1 over 5 min can be useful on some occasion.
Supporting pharmacological therapy such as lidocaine, amiodarone and procainamide are used only to prevent recurrence of VF.

d. Torsades de pointes These arrhythmias are usually short in duration
and spontaneously revert to sinus rhythm. Occasionally it can change to VF. On ECG, it is characterized by rapid, irregular
sharp complexes that continuously change from an upright to an inverted position.
Between spells of tachycardia the ECG shows a prolonged QT interval; the corrected QT is equal to or greater than 0.44s.

Treatment: 1. Any electrolyte disturbance is corrected. 2. Causative drug and precipitating factors
should be stopped and removed. 3. Intravenous isoprenaline may be effective
when QT prolongation is acquired. 4. βBlockade is advised if the QT prologation is
congenital


PEA

ASYSTOLE


Anesthetics and Arrhythmias

Anesthetics and Arrhythmias

Anti Arrhythmic Drugs

Class Action Examples Side Effects1A Fast sodium channel blocker varies
depolarization and action potentialduration
Quinidine,procainamide,disopyramide
Class: nausea, vomitingQuinidine: hemolyticanemia, thrombocytopenia,tinnitusProcainamide: lupus
1B Lidocaine,Mexiletine
Lidocaine: dizziness,confusion, seizures, comaMexiletine: tremor, ataxia,rash
1C Flecainide,Propafenone
Flecainide: pro-arrhythmia,nausea, dizzyness
2 beta-blockers SA node & AV nodeconduction
Propranolol,metoprolol
Class: CHF, bronchospasm,bradycardia, hypotension
3 Prolong action potential by blockingK+ channels
Amiodarone,sotalol
Amiodarone: hepatitis,pulmonary fibrosis, thyroiddisorders, peripheralneuropathySotalol: bronchospasm
4 calcium channel blockers AV nodeconduction
Verapamil,dilitiazem
Class: AV block,hypotension, bradycardia,constipation

Class I drugs- These are membrane-depressant drugs that reduce
the rate of entry of sodium into the cell. They may slow conduction, delay recovery or
reduce the spontaneous discharge rate of myocardial cells.
Class Ia drugs (e.g. disopyramide) lengthen the action potential, and
Class Ic (flecainide, propafenone) do not affect the duration of the action potential.
Lidocaine- Loading dose 1mg.kg-1, repeat every 5min, continuous 30-50 μg.kg-1.min-1.
Procainamide -20mg.min-1 IVinfusion (Max total dose 17mg.kg-1; infusion 1-4mg.min-1
Class II drugs- These antisympathetic drugs prevent the effects
of catecholamines on the action potential. Most are β-adrenergic antagonists.
Cardioselective β-blockers (β1) include metoprolol,atenolol, and acebutalol.
Propranolol -0.1mg.kg-1 by slow IV over 10min

Class III drugs- These prolong the action potential and do not
affect sodium transport through the membrane. There are two major drugs in this class;
amiodarone and sotalol. Sotalol is also a β-blocker. Amiodarone -150mgIVover10min;360mg/IV
over6hr Amiodarone also has class II (blocking adrenergic
receptors) and class IV (calcium blockers) properties.
Bretylium- 5mg.kg-1 IV push, repeat in 5 min at 10mg.kg-1, upto max dose of 35 mg.kg-1
Class IV drugs The non-dihydropyridine calcium antagonists
that reduce the plateau phase of the action potential are particularly effective at slowing conduction in nodal tissue.
Verapamil and diltiazem are the most important drugs in this group
Adenosine- Adenosine is useful to classify SVTs because
tachycardia caused by atrial reentry such as AF or flutter have transient response of decreased frequency after adenosine, but it does not terminate the dysrhythmia; on the other hand,
SVTs due to reentry in the AV node ceases after adenosine.
Ventricular dysrhythmias do not respond to adenosine because these dysrhythmias originate in distal tissues of the conduction system.
This also allows the use of adenosine to distinguish between wide-complex SVT and VT, since adenosine causes rapid AV block, with a half-life of 9 seconds, and terminates most SVTs due to reentry;

According to the 2005 guidelines of the American Heart Association, it should not be used for differential diagnosis between wide-complex SVT and VT due to its vasodilator properties, bronchospasm, paradoxal increase in conduction in the accessory pathway, persistent bradycardia or asystole, and degeneration to ventricular fibrillation (VF).
Prodysrhythmia
A term used to describe antiarhythmic drug-induced dysrhythmia
Class Ia drugs can also slow down conduction and prolong repolarization, and may cause TdP.
Class Ib drugs (lidocaine and mexiletine) are more selective to abnormal or damaged myocytes and are not associated with prodysrhythmia.
Class Ic drugs should not be used in patients with structural cardiomyopathies due to the high risk of prodysrhythmia
In patients after MI slow conduction due to class Ic antiarhythmics leads to an increase in reentry allowing the development of VT and, therefore, class Ic drugs should not be used in patients with ischemia

Beta blockers (class II) may be used to treat SVTs, as well as calcium channel blockers (class IV), and they do not have a great risk of prodysrhythmic phenomena.
Class III agents (amiodarone, sotalol,and dofetilide) block potassium channels prolonging repolarization,and have the potential to induce TdP.
Some antiarhythmic drugs such as verapamil and amiodarone, Procainamide, sotalol, and bipyridyl can occasionally lead to TdP, although amiodarone prolongs the QT interval by more than 500 msecs.

Drugs causing bradydysrhythmias -βetablockers,calcium channel blockers, amiodarone, clonidine,and dexmedetomidine.
Inotropics -dobutamine and milrinone, may precipitate arrhythmias and ventricular fibrillation.
Dobutamine is directly dysrhythmogenic, causing dose-dependent tachycardia;
doses higher than 5 μg.kg-1.min-1 are prone to cause dysrhythmias and generate little benefit in oxygen transportation.
Milrinone increases the inotropism without activating adrenergic receptors, but it also has a dysrhythmic potential.

Digoxin increases intracellular calcium in cardiac myocytes, slows AV node conduction, and can increase automaticity, triggering any type of dysrhythmia, the most common being premature ventricular contraction, heart blocks of any degree (although rarely Mobitz type II), paroxysmal atrial tachycardia with heart block, accelerated junctional rhythm, and bidirectional VT.
Risk factors for digoxin intoxication include renal dysfunction and electrolyte imbalance, such as hypokalemia, hypomagnesemia, and hypercalcemia.

SUMMARY After the diagnosis of dysrhythmia the distinction
between benign dysrhythmia and those that carry the risk of sudden death is fundamental.
The choice of anesthetic agents is important to minimize episodes of tachydysrhythmias.
Prevention is as important as treating dysrhythmias. Recognition of risk factors, adequate selection of
drugs for each patient, and monitoring represent the most important steps in prevention.
Electrolytes should be monitored and corrected whenever necessary.
Supraventricular tachycardia responds to treatment with adenosine, while AF does not, although in both cases the frequency is controlled by beta-blockers or calcium channel blockers

Amiodarone and sotalol are class III drugs and they prolong the action potential and repolarization, and are currently among the most used antiarhythmics drugs.
Digoxin, magnesium,and adenosine have unique antidysrhythmic properties.
The management in perioperative dysrhythmias does not always include the use of antiarhythmics agents, although the use of antiarhythmic drugs should not be delayed when indicated.