
1Peri-operative smoking control French Conference of Experts Peri-operative smoking control.
35
1 Peri-operative smoking control French Conference of Experts Peri-operative smoking control
-
Upload
edgar-welch -
Category
Documents
-
view
225 -
download
1
Transcript of 1Peri-operative smoking control French Conference of Experts Peri-operative smoking control.
1Peri-operative smoking control
French Conference of Experts
Peri-operative smoking control
2Peri-operative smoking control
Background
Smoking consumption is the cause of a significant increase risk of surgical adverse events, too often neglected.
A good assumption of the responsibility of the tobacco smoke must lead to a quick benefit, reducing general and local surgical complication rate, which would constitute a significant profit in term of health and savings.

3Peri-operative smoking control
Gradation A, B, C, D or E of recommendations
Gradation des 143 recommandations
A3%
B4%
C6%
D28%E
59%
Most of the recommandations are
grade E
Recommandations level A are only 3%
4Peri-operative smoking control
6 questions
QS1: What are the tobacco related risks in surgical period?
QS2 What are the proven benefits from of quitting smoking during the surgical period?
QS3 How a smoker should be help before elective surgery?
QS4-What is the role of each health professionals in the surgical period?
Qs5- What are the specificities of an anesthesia for a smoker patient ?
QS 6: How to deal with dependent smoker hospitalized for a not anticipate surgical procedure?
5Peri-operative smoking control
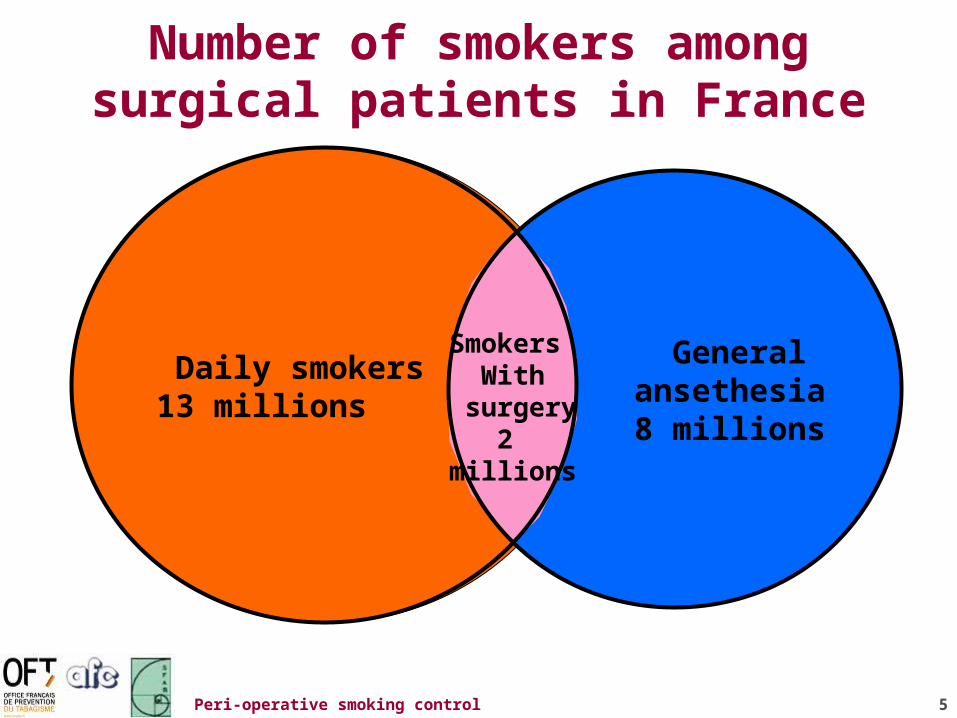
Number of smokers amongsurgical patients in France
Daily smokers 13 millions
General ansethesia8 millions
Smokers With
surgery2
millions
6Peri-operative smoking control
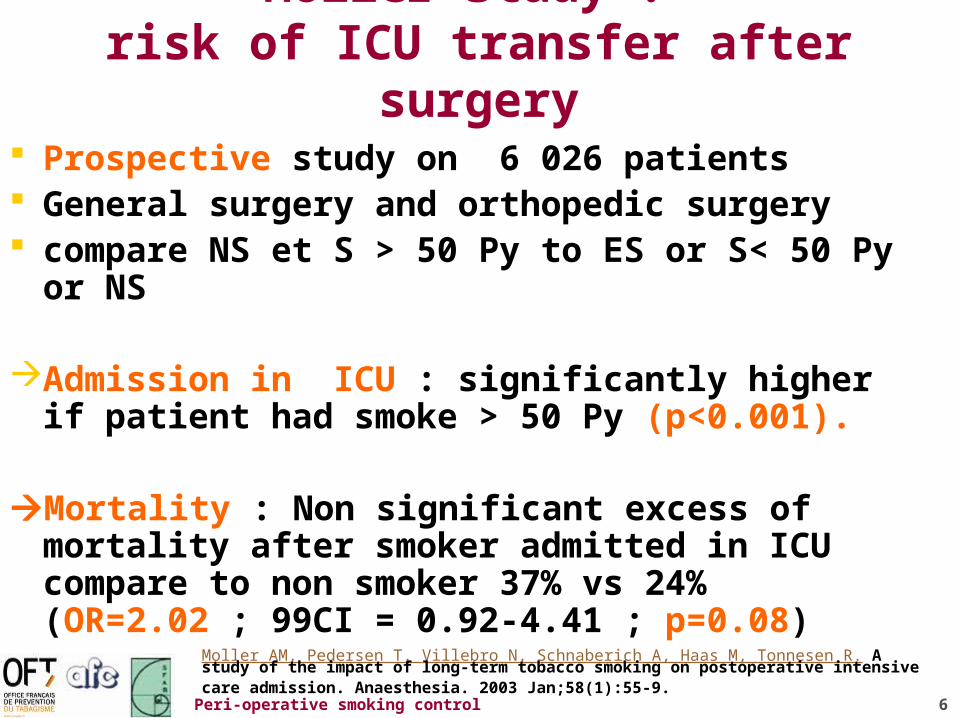
Moller study : risk of ICU transfer after surgery
Prospective study on 6 026 patients General surgery and orthopedic surgery compare NS et S > 50 Py to ES or S< 50 Py or NS
Admission in ICU : significantly higher if patient had smoke > 50 Py (p<0.001).
Mortality : Non significant excess of mortality
after smoker admitted in ICU compare to non smoker 37% vs 24% (OR=2.02 ; 99CI = 0.92-4.41 ; p=0.08)
Moller AM, Pedersen T, Villebro N, Schnaberich A, Haas M, Tonnesen R. A study of the impact of long-term tobacco smoking on postoperative intensive care admission. Anaesthesia. 2003 Jan;58(1):55-9.

7Peri-operative smoking control
General surgery mortality study Delgado-Rodriguez
Prospective study 2 989 surgical patients
Increase admission in ICU if ≥ 51 Py (OR=2.86 ; 95 CI = 1.21-6.77).
Increase death at hospital if ≥ 51 Py (OR=2.56 ; 95 CI = 1.10-5.97).
Delgado-Rodriguez M, Medina-Cuadros M, Martinez-Gallego G, Gomez-Ortega A, Mariscal-Ortiz M, Palma-Perez S, Sillero-Arenas M. A prospective study of tobacco smoking as a predictor of complications in general surgery.Infect Control Hosp Epidemiol. 2003 Jan;24(1):37-43
8Peri-operative smoking control
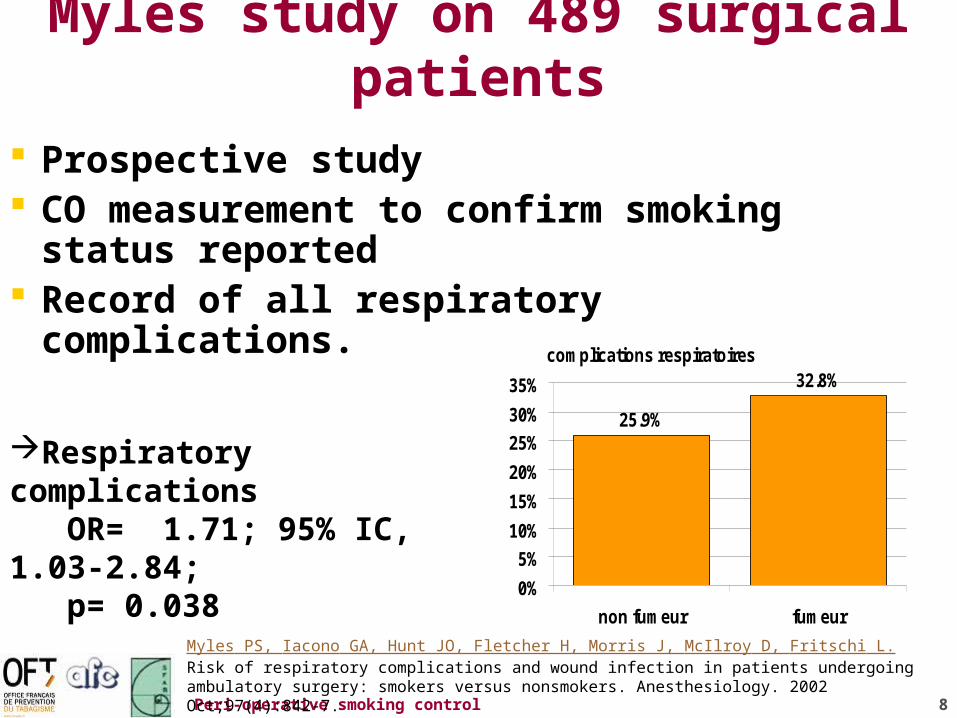
Myles study on 489 surgical patients
Prospective study CO measurement to confirm smoking
status reported Record of all respiratory complications.
Myles PS, Iacono GA, Hunt JO, Fletcher H, Morris J, McIlroy D, Fritschi L. Risk of respiratory complications and wound infection in patients undergoing ambulatory surgery: smokers versus nonsmokers. Anesthesiology. 2002 Oct;97(4):842-7.
complications respiratoires
25.9%
32.8%
0%
5%
10%
15%
20%
25%
30%
35%
non fumeur fumeur
Respiratory complications OR= 1.71; 95% IC, 1.03-2.84; p= 0.038

9Peri-operative smoking control
Schwilk study 26 961 surgical patients
Prospective study 26 961 patients (7122 =26.4% smokers)
COPD 23.3% (4.8% among smokers). 1573 complications in 1397 patients (5.2%) 1114 respiratory events
complications respiratoires
3.1%
5.5%
0%
1%
2%
3%
4%
5%
6%
non fumeur fumeur
Schwilk B, Bothner U, Schraag S, Georgieff M. Perioperative respiratory events in smokers and nonsmokers undergoing general anaesthesia. Acta Anaesthesiol Scand. 1997 Mar;41(3):348-55.
RR of respiratory events• 1.8 in smokers• 2.3 in smokers 16-39 y old)• 6.3 in overweight young smokers
RR of bronchospasm : 25.7 in young smokers with COPD

10Peri-operative smoking control
Moller randomized study cardiovascular complications
120 smokers randomized 6-8 weeks before surgery
Nurse training every week + medications as need
No specific intervention
(p=0.08) Moller AM, Villebro N, Pedersen T, Tonnesen H. Effect of preoperative smoking intervention on postoperative complications: a randomised clinical trial. Lancet. 2002 Jan 12;359(9301):114-7.
complications cardiovasculaires
0%
10%
0%
2%
4%
6%
8%
10%
12%
non fumeur fumeur
11Peri-operative smoking control
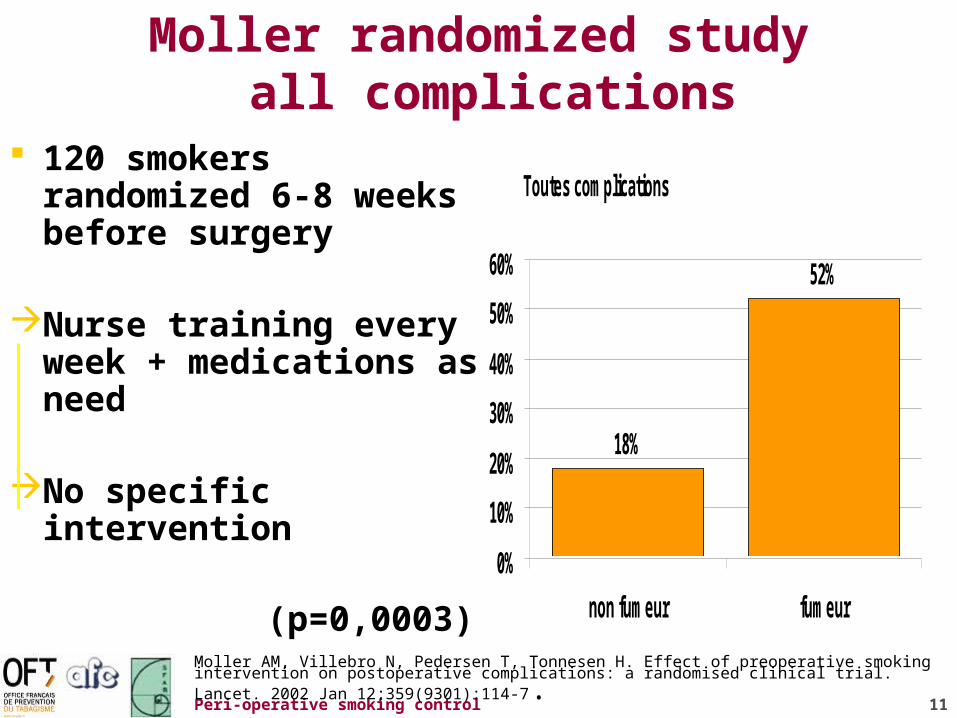
Moller randomized study all complications
120 smokers randomized 6-8 weeks before surgery
Nurse training every week + medications as need
No specific intervention
(p=0,0003) Moller AM, Villebro N, Pedersen T, Tonnesen H. Effect of preoperative smoking intervention on postoperative complications: a randomised clinical trial. Lancet. 2002 Jan 12;359(9301):114-7.
Toutes complications
18%
52%
0%
10%
20%
30%
40%
50%
60%
non fumeur fumeur
12Peri-operative smoking control
1.3 Which are the risks of general complications
(cardiovascular, respiratory, and infectious,…)?
The increase in the relative risk (RR) according to studies concerns:
The risk of being transferred to an intensive care units (RR from 2.02 to 2.86) [D],
Infectious complications (RR from 2 to 3.5) [D],
Coronary complications (RR of 3) [D], Immediate respiratory complications (RR of
1.71) [D].
13Peri-operative smoking control
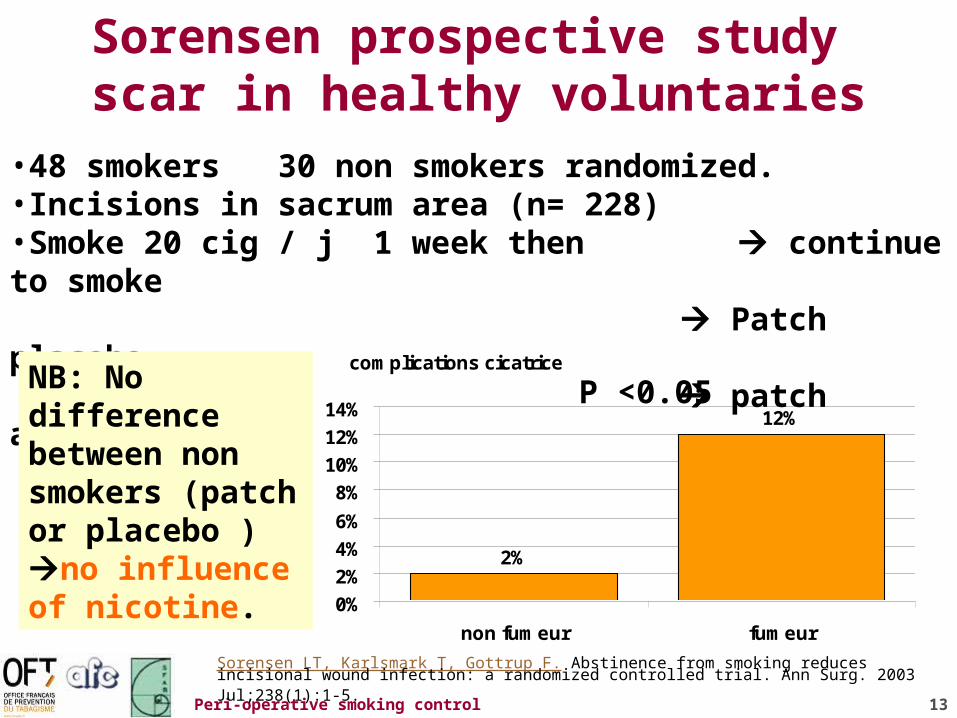
Sorensen prospective study scar in healthy voluntaries
complications cicatrice
2%
12%
0%
2%
4%
6%
8%
10%
12%
14%
non fumeur fumeur
Sorensen LT, Karlsmark T, Gottrup F. Abstinence from smoking reduces incisional wound infection: a randomized controlled trial. Ann Surg. 2003 Jul;238(1):1-5.
•48 smokers 30 non smokers randomized.•Incisions in sacrum area (n= 228)•Smoke 20 cig / j 1 week then continue to smoke
Patch placebo patch active
NB: No difference between non smokers (patch or placebo ) no influence of nicotine.
P <0.05
14Peri-operative smoking control
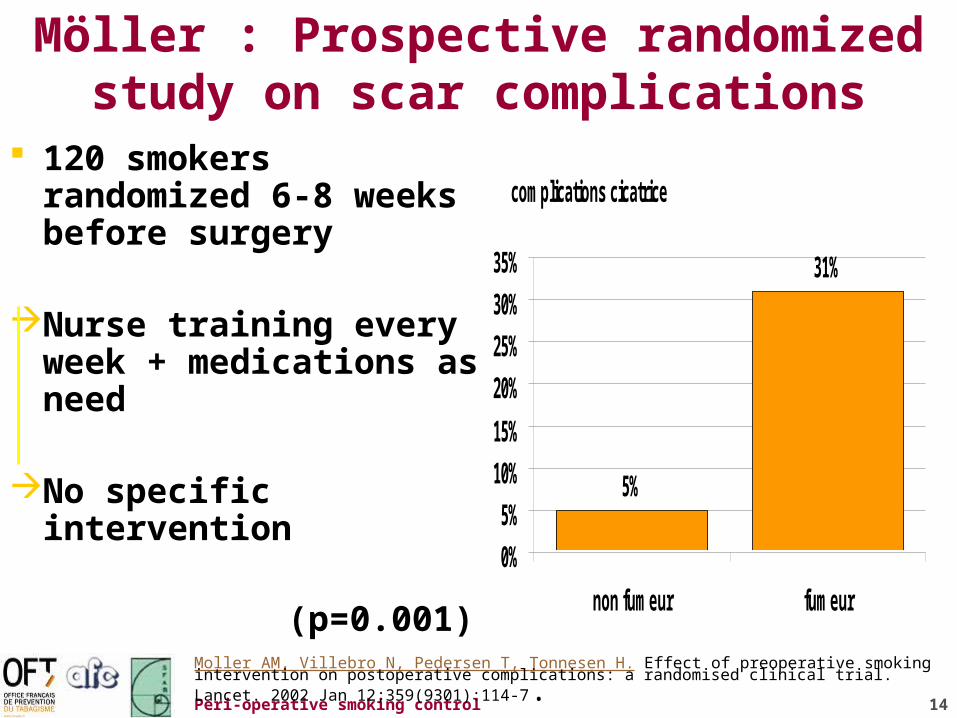
Möller : Prospective randomized study on scar complications
120 smokers randomized 6-8 weeks before surgery
Nurse training every week + medications as need
No specific intervention
(p=0.001) Moller AM, Villebro N, Pedersen T, Tonnesen H. Effect of preoperative smoking intervention on postoperative complications: a randomised clinical trial. Lancet. 2002 Jan 12;359(9301):114-7.
complications cicatrice
5%
31%
0%
5%
10%
15%
20%
25%
30%
35%
non fumeur fumeur
15Peri-operative smoking control
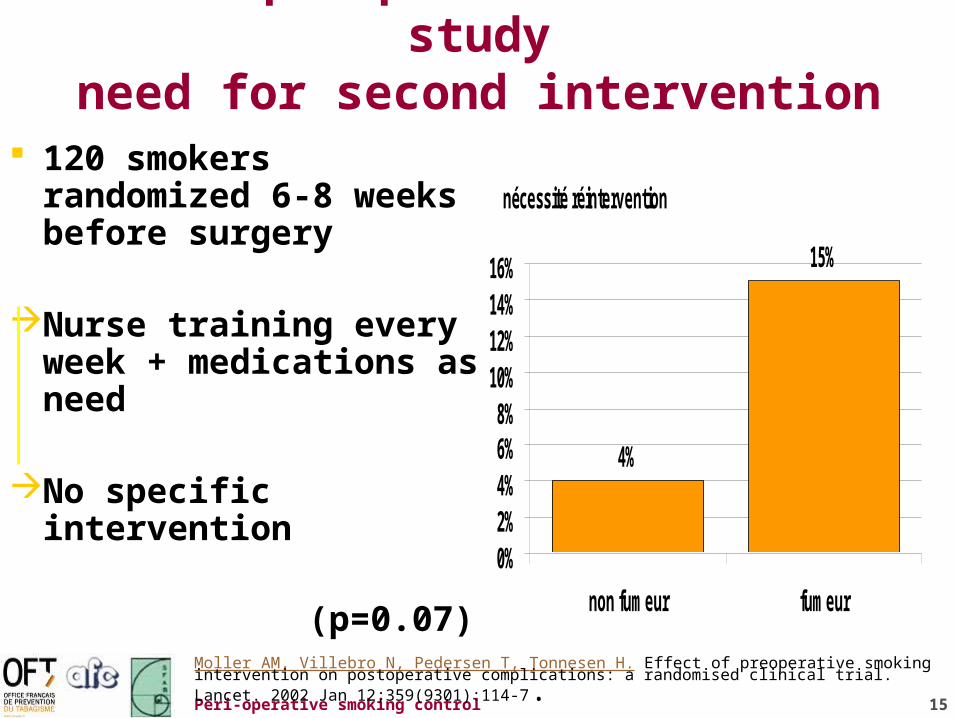
Möller prospective randomized studyneed for second intervention
120 smokers randomized 6-8 weeks before surgery
Nurse training every week + medications as need
No specific intervention
(p=0.07) Moller AM, Villebro N, Pedersen T, Tonnesen H. Effect of preoperative smoking intervention on postoperative complications: a randomised clinical trial. Lancet. 2002 Jan 12;359(9301):114-7.
nécessité réintervention
4%
15%
0%2%4%6%8%
10%12%14%16%
non fumeur fumeur
16Peri-operative smoking control
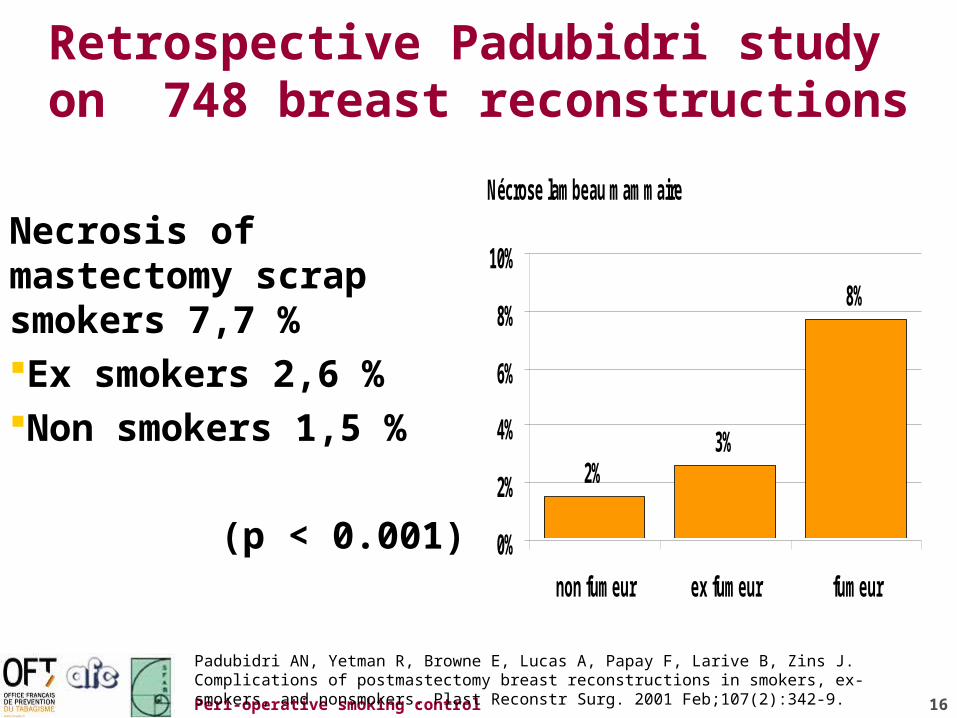
Retrospective Padubidri study on 748 breast reconstructions
Necrosis of mastectomy scrap smokers 7,7 %Ex smokers 2,6 %Non smokers 1,5 %
(p < 0.001)
Padubidri AN, Yetman R, Browne E, Lucas A, Papay F, Larive B, Zins J. Complications of postmastectomy breast reconstructions in smokers, ex-smokers, and nonsmokers. Plast Reconstr Surg. 2001 Feb;107(2):342-9.
Nécrose lambeau mammaire
2%3%
8%
0%
2%
4%
6%
8%
10%
non fumeur ex fumeur fumeur
17Peri-operative smoking control
Retrospective Möller study811 hip or knee prosthesis
232 smokers (28.6%) and 579 non-smokers
Smoking doubled the risk of prolonged hospitalization (> 15 days)
Complication of scarsmokers RR 3.2
Admission in ICUSmokers RR 8.5
Moller AM, Pedersen T, Villebro N, Munksgaard A. Effect of smoking on early complications after elective orthopaedic surgery. J Bone Joint Surg Br. 2003 Mar;85(2):178-81.
18Peri-operative smoking control
Willigendael Meta-analysis on vascular by-pass.
29 studies (4 randomized, 12 prospective and 13 retrospectives).
In randomized trial and prospective studies, the risk of by pass failure increase 3.09 (IC: 2.34-4.8 p< 0.0001) with smoking continuation.
No difference between venous and polyester by pass. Correlation between by pass permeability and intensity of
tobacco consumption.Quitting at surgery provide a permeability rate close to non
smoker rate. Continuation of smoking could be responsible of 57% of
failure (IC 95%, 50%-64%).Willigendael EM, Teijink JA, Bartelink ML, Peters RJ, Buller HR, Prins MH. Smoking and the patency of lower extremity bypass grafts: a meta-analysis. J Vasc Surg. 2005 Jul;42(1):67-74.
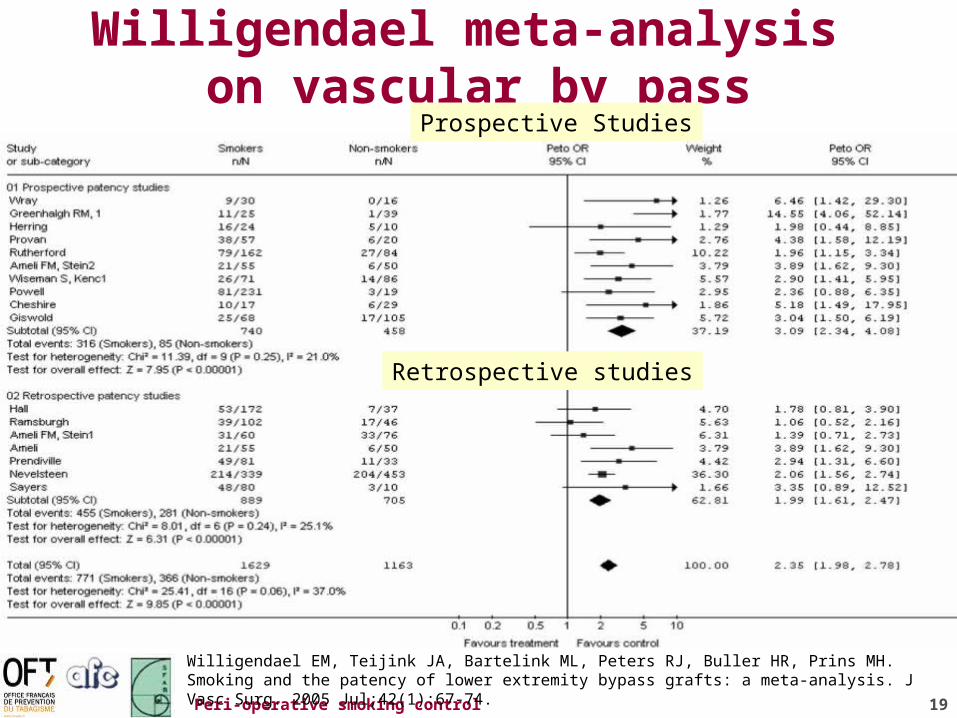
19Peri-operative smoking control
Willigendael meta-analysis on vascular by pass
Willigendael EM, Teijink JA, Bartelink ML, Peters RJ, Buller HR, Prins MH. Smoking and the patency of lower extremity bypass grafts: a meta-analysis. J Vasc Surg. 2005 Jul;42(1):67-74.
Prospective Studies
Retrospective studies
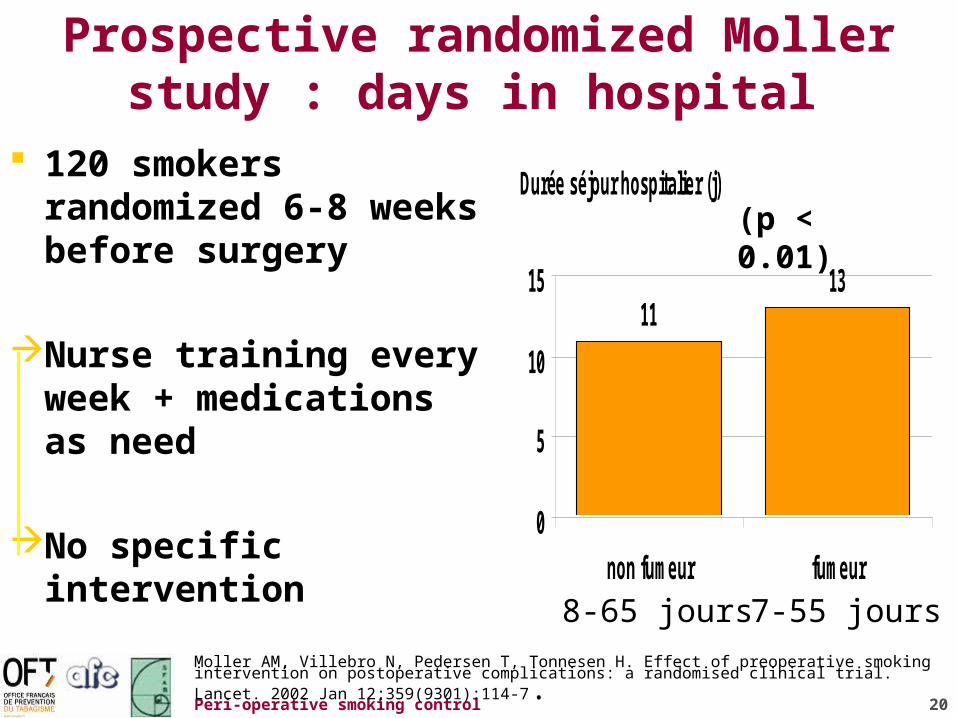
20Peri-operative smoking control
Prospective randomized Mollerstudy : days in hospital
120 smokers randomized 6-8 weeks before surgery
Nurse training every week + medications as need
No specific intervention
Moller AM, Villebro N, Pedersen T, Tonnesen H. Effect of preoperative smoking intervention on postoperative complications: a randomised clinical trial. Lancet. 2002 Jan 12;359(9301):114-7.
Durée séjour hospitalier (j)
1113
0
5
10
15
non fumeur fumeur
(p < 0.01)
8-65 jours 7-55 jours
21Peri-operative smoking control
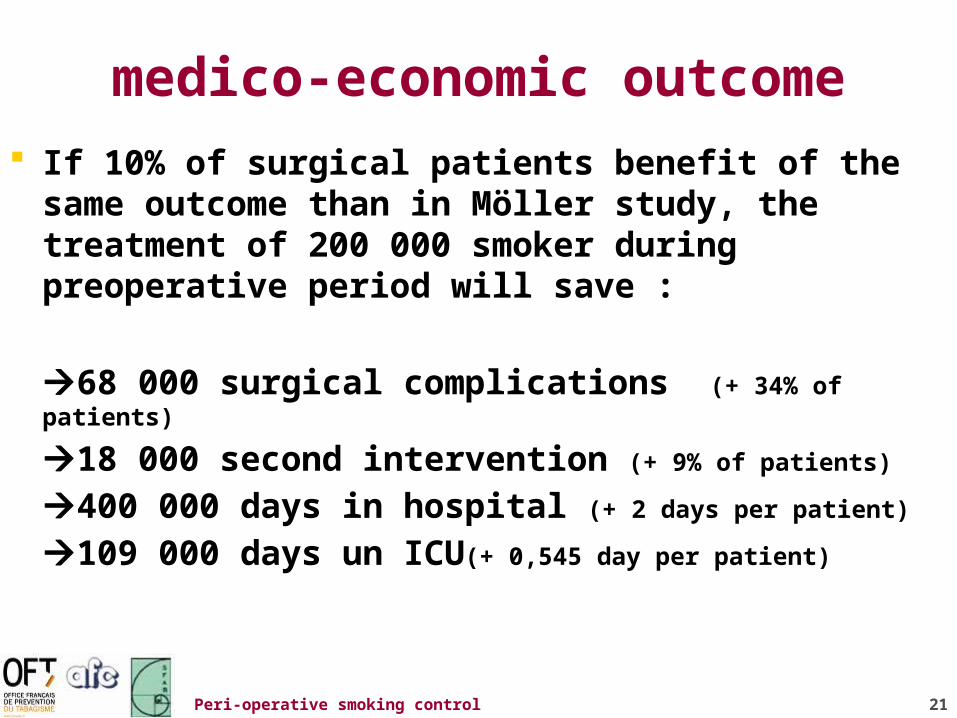
medico-economic outcome
If 10% of surgical patients benefit of the same outcome than in Möller study, the treatment of 200 000 smoker during preoperative period will save :
68 000 surgical complications (+ 34% of patients)
18 000 second intervention (+ 9% of patients)
400 000 days in hospital (+ 2 days per patient)
109 000 days un ICU(+ 0,545 day per patient)

22Peri-operative smoking control
QS 2
QS2 What are the proven benefits from of quitting
smoking during the surgical period?
23Peri-operative smoking control
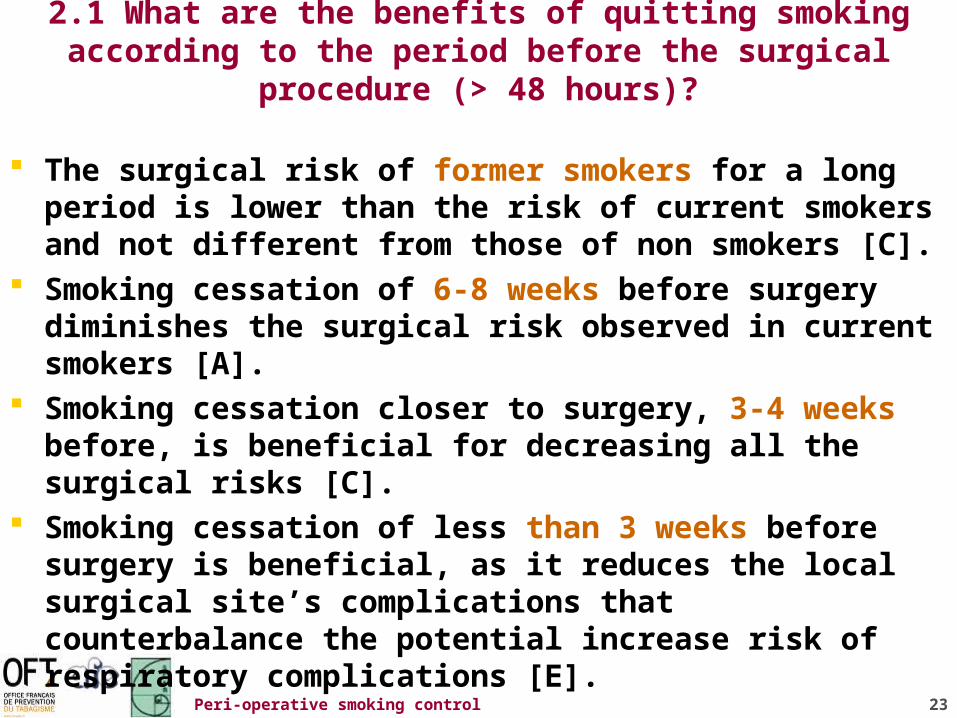
2.1 What are the benefits of quitting smoking according to the period before the surgical procedure (> 48 hours)?
The surgical risk of former smokers for a long period is lower than the risk of current smokers and not different from those of non smokers [C].
Smoking cessation of 6-8 weeks before surgery diminishes the surgical risk observed in current smokers [A].
Smoking cessation closer to surgery, 3-4 weeks before, is beneficial for decreasing all the surgical risks [C].
Smoking cessation of less than 3 weeks before surgery is beneficial, as it reduces the local surgical site’s complications that counterbalance the potential increase risk of respiratory complications [E].
24Peri-operative smoking control
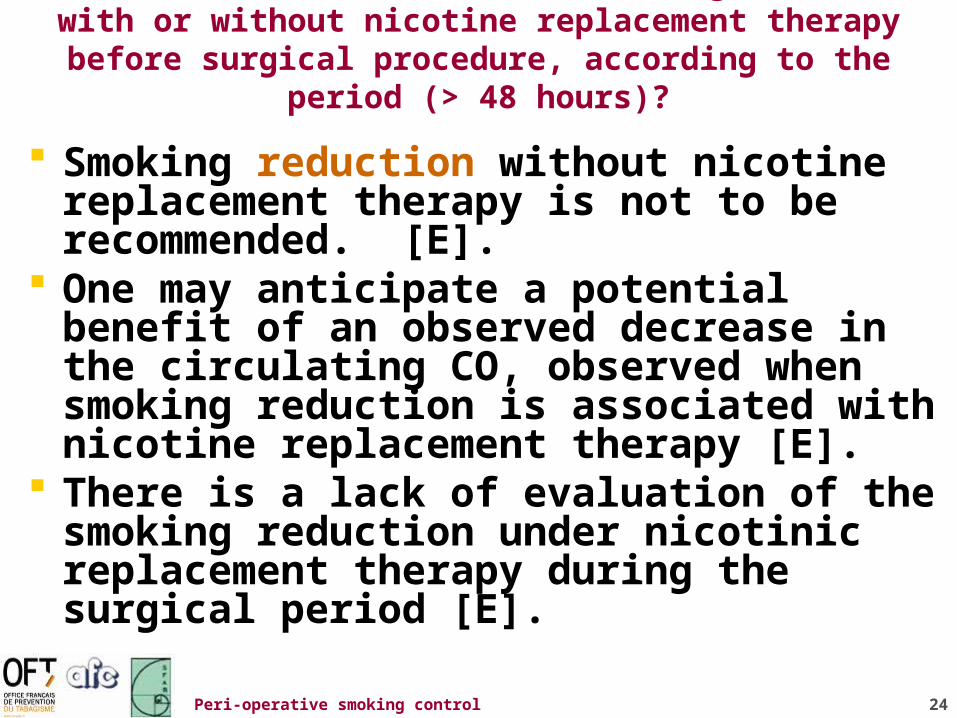
2.2 What are the benefits of smoking reduction with or without nicotine replacement therapy before surgical
procedure, according to the period (> 48 hours)?
Smoking reduction without nicotine replacement therapy is not to be recommended. [E].
One may anticipate a potential benefit of an observed decrease in the circulating CO, observed when smoking reduction is associated with nicotine replacement therapy [E].
There is a lack of evaluation of the smoking reduction under nicotinic replacement therapy during the surgical period [E].
25Peri-operative smoking control
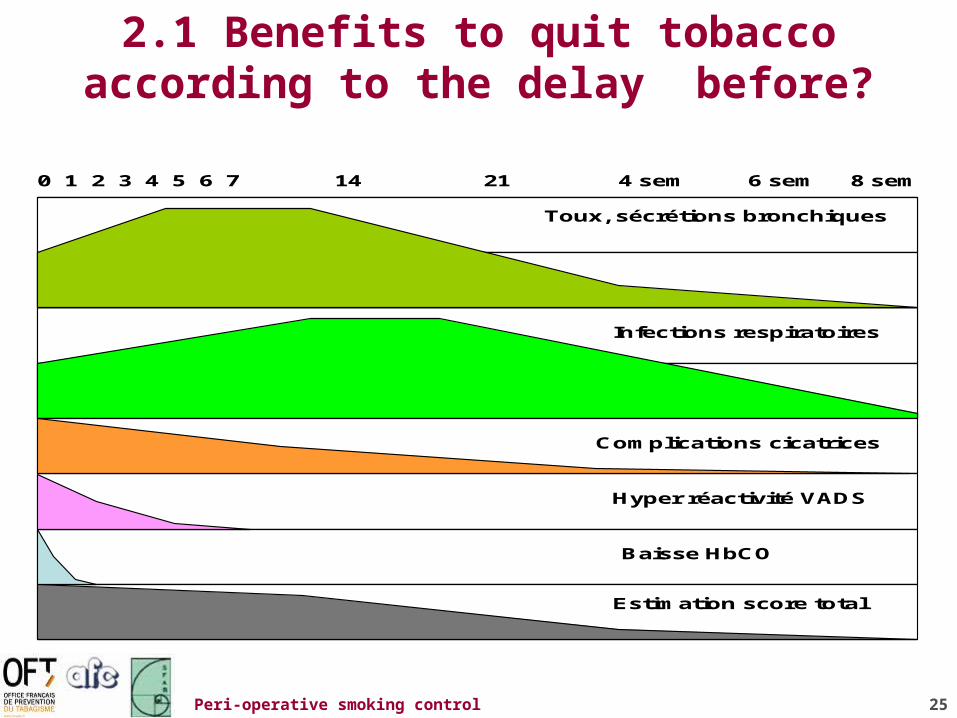
2.1 Benefits to quit tobacco according to the delay before?
0 1 2 3 4 5 6 7 14 21 4 sem 6 sem 8 sem
Toux, sécrétions bronchiques
Infections respiratoires
Complications cicatrices
Estimation score total
Baisse HbCO
Hyper réactivité VADS

26Peri-operative smoking control
2.3 What are the benefits of late smoking cessation, with or without nicotine replacement therapy, in the 48 hours
preceding a surgical procedure
From the physiological point of view, complete smoking cessation even of less than 48 hours before surgical procedure should be beneficial [E].
Temporary increase in cough and bronchial secretions are the only related adverse events that can be harmful just after smoking cessation [E].
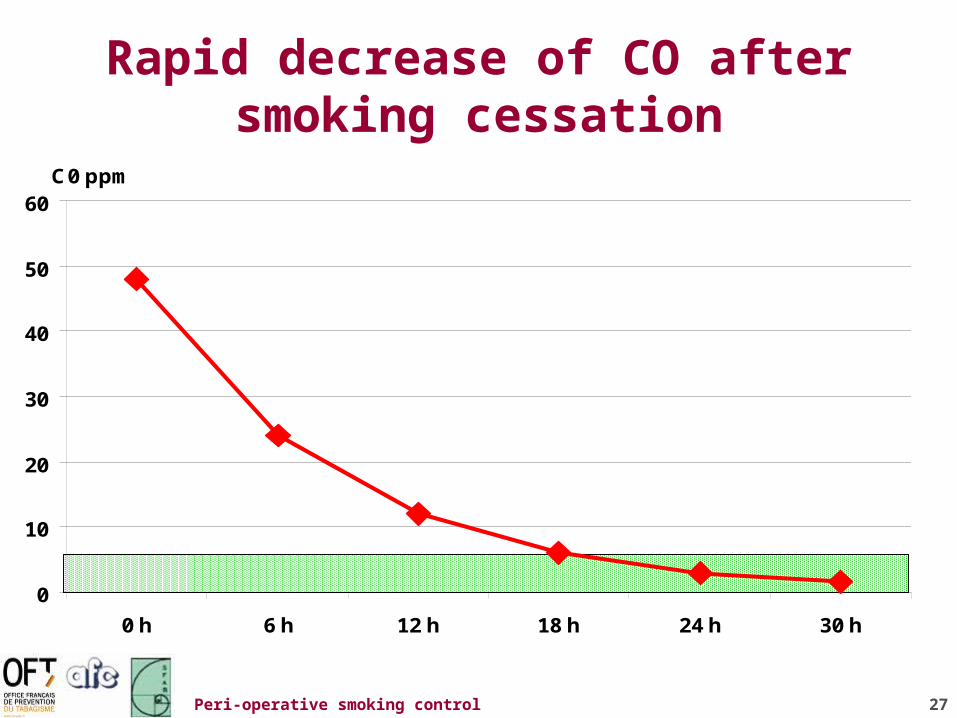
27Peri-operative smoking control
Rapid decrease of CO after smoking cessation
C0 ppm
0
10
20
30
40
50
60
0 h 6 h 12 h 18 h 24 h 30 h

28Peri-operative smoking control
Decrease of cardiac and respiratory risk in the 48 hours of quitting
score moyen de la toux lors de l'abstinence
0
0.2
0.4
0.6
0.8
1
Precessation 2 7 21
Jours d'abstinence tabagique
AbstinentsNon fumeurs
Yamashita S, Yamaguchi H, Sakaguchi M, Yamamoto S, Aoki K, Shiga Y, Hisajima Y. Effect of smoking on intraoperative sputum and postoperative pulmonary complication in minor surgical patients. Respir Med. 2004 Aug;98(8):760-6.
Cardiac risk decrease the day of quiting
Sputum production
increase initially

29Peri-operative smoking control
2.5 Does smoking cessation during the surgical period contribute to long term smoking cessation?
In the general population, the relapse rate after quitting is approximately 50% one year after cessation [A].
In the case of cardiac surgery, 50% of post coronary artery surgical patients who quit smoking had relapsed one year later [C].
Quitting smoking for a surgical procedure is a positive prognostic factor for long term smoking abstinence. However, the high relapse rate highlights the need to reinforce the prevention of relapses [E]
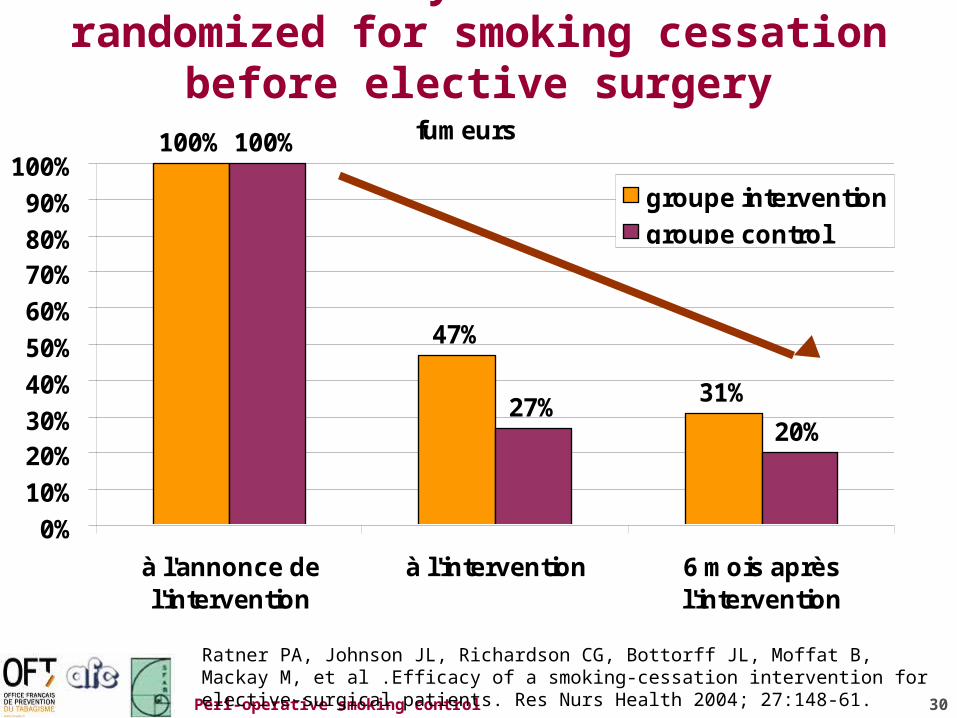
30Peri-operative smoking control
Ratner study : 237 smokers randomized for smoking cessation before elective surgery
Ratner PA, Johnson JL, Richardson CG, Bottorff JL, Moffat B, Mackay M, et al .Efficacy of a smoking-cessation intervention for elective-surgical patients. Res Nurs Health 2004; 27:148-61.
fumeurs100%
47%
31%
100%
27%20%
0%
10%
20%30%
40%
50%
60%
70%80%
90%
100%
à l'annonce del'intervention
à l'intervention 6 mois aprèsl'intervention
groupe intervention
groupe control
31Peri-operative smoking control
2.6 What are the benefits of continuous abstinence after surgery on bone consolidation and thrombosis
risk? When smoking abstinence is continued in the
postoperative period, the benefit on bone consolidation is demonstrated [D] and the benefit on skin and soft cicatrisation is probably beneficial [E].
When smoking cessation is maintained in the post operative period, benefits are seen in osseous consolidation [D], and probably in skin and soft cicatrisation [E].
The permeability of vascular bypass is improved, when smoking cessation is prolonged during the post operative period [A].
In smokers, thromboses of vascular bypass are 57% tobacco related [B].
32Peri-operative smoking control
QS 3
QS3 How a smoker should be looked after
before elective surgery?
33Peri-operative smoking control
Standard procedure for identification and treatment of smoker before surgery
Accéder à la procédure en Word ou pdf

34Peri-operative smoking control
Procedure for in patients
Accéder à la procédure en Word ou pdf
35Peri-operative smoking control
Conclusion
All surgical department has to be organized to identified smokers 6-8 weeks before surgery as soon as possible
All surgical department has to organize smoking cessation in preoperative period with adequate tools
All surgical department need to organize substitution of smoker during surgery
All surgical department had to organize follow up of formers smoker to prevent relapse


















