Original Article Orbital Lymphangioma: Characteristics and ... · Lymphangioma is a benign tumor of...
8
pISSN: 1011-8942 eISSN: 2092-9382 © 2017 The Korean Ophthalmological Society This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses /by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. 194 Original Article Korean J Ophthalmol 2017;31(3):194-201 https://doi.org/10.3341/kjo.2016.0034 Orbital Lymphangioma: Characteristics and Treatment Outcomes of 12 Cases Young Jun Woo 1 , Chang Yeom Kim 1 , Bradford Sgrignoli 2 , Jin Sook Yoon 1 1 Institute of Vision Research, Department of Ophthalmology, Yonsei University College of Medicine, Seoul, Korea 2 Department of Ophthalmology, Saint John’s Episcopal Hospital, Far Rockaway, NY, USA Purpose: To report the patient characteristics and treatment outcomes in 12 cases of orbital lymphangioma. Methods: In this study, orbital lymphangioma was diagnosed based on clinical, radiologic (computed tomog- raphy, magnetic resonance imaging), and histologic findings when possible. Patients whose vision was not compromised by orbital lymphangioma, or that did not have increased intraocular pressure (IOP), received oral corticosteroids. Orbital lymphangioma that affected vision or increased IOP was treated by surgery, which included aspiration of blood or partial resection with or without injection of a sclerosant. Results: Four patients without compromised vision responded well to oral corticosteroids. Eight patients with compromised vision underwent some form of surgery. Bleeding recurred in three patients after aspiration of blood and in two after partial resection and intralesional injection of a sclerosant. Overall, five patients were treated successfully by aspiration of blood, intralesional injection of a sclerosant, and application of continuous negative pressure by appropriate drainage. Partial resection was successful in two patients with organized he- matoma. Conclusions: Orbital lymphangioma that does not compromise vision can be treated medically using oral corti- costeroids. Patients with threatened vision or elevated IOP due to acute hemorrhage should be treated by as- piration of blood, intralesional injection of a sclerosant, and application of continuous negative pressure. Partial resection may be effective only in patients with organized hematoma. Key Words: Hemorrhage, Lymphangioma, Sclerotherapy, Treatment outcome Lymphangioma is a benign tumor of the lymphatic sys- tem that is characterized by abnormal endothelial-lined channels [1]. Generally found in the head and neck region, these tumors constitute 0.3% to 4% of all orbital tumors and are not considered hamartomas because the orbit does not usually contain lymphatic vessels [2,3]. Some patients with orbital lymphangioma may develop proptosis, either slowly as the mass invades the orbit or suddenly during Received: April 11, 2016 Accepted: May 18, 2016 Corresponding Author: Jin Sook Yoon, MD, PhD. Institute of Vision Research, Department of Ophthalmology, Yonsei University College of Medicine, #50-1 Yonsei-ro, Seodaemun-gu, Seoul 03722, Korea. Tel: 82- 2-2228-3570, Fax: 82-2-312-0541, E-mail: [email protected]
Transcript of Original Article Orbital Lymphangioma: Characteristics and ... · Lymphangioma is a benign tumor of...
pISSN: 1011-8942 eISSN: 2092-9382
© 2017 The Korean Ophthalmological SocietyThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses /by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
194
Original Article
Korean J Ophthalmol 2017;31(3):194-201ht tps: / /doi.org /10.3341/k jo.2016.0034
Orbital Lymphangioma: Characteristics and Treatment Outcomes of 12 Cases
Young Jun Woo1, Chang Yeom Kim1, Bradford Sgrignoli2, Jin Sook Yoon1
1Institute of Vision Research, Department of Ophthalmology, Yonsei University College of Medicine, Seoul, Korea2Department of Ophthalmology, Saint John’s Episcopal Hospital, Far Rockaway, NY, USA
Purpose: To report the patient characteristics and treatment outcomes in 12 cases of orbital lymphangioma.
Methods: In this study, orbital lymphangioma was diagnosed based on clinical, radiologic (computed tomog-
raphy, magnetic resonance imaging), and histologic findings when possible. Patients whose vision was not
compromised by orbital lymphangioma, or that did not have increased intraocular pressure (IOP), received
oral corticosteroids. Orbital lymphangioma that affected vision or increased IOP was treated by surgery, which
included aspiration of blood or partial resection with or without injection of a sclerosant.
Results: Four patients without compromised vision responded well to oral corticosteroids. Eight patients with
compromised vision underwent some form of surgery. Bleeding recurred in three patients after aspiration of
blood and in two after partial resection and intralesional injection of a sclerosant. Overall, five patients were
treated successfully by aspiration of blood, intralesional injection of a sclerosant, and application of continuous
negative pressure by appropriate drainage. Partial resection was successful in two patients with organized he-
matoma.
Conclusions: Orbital lymphangioma that does not compromise vision can be treated medically using oral corti-
costeroids. Patients with threatened vision or elevated IOP due to acute hemorrhage should be treated by as-
piration of blood, intralesional injection of a sclerosant, and application of continuous negative pressure. Partial
resection may be effective only in patients with organized hematoma.
Key Words: Hemorrhage, Lymphangioma, Sclerotherapy, Treatment outcome
Lymphangioma is a benign tumor of the lymphatic sys- tem that is characterized by abnormal endothelial-lined channels [1]. Generally found in the head and neck region, these tumors constitute 0.3% to 4% of all orbital tumors and are not considered hamartomas because the orbit does not usually contain lymphatic vessels [2,3]. Some patients with orbital lymphangioma may develop proptosis, either slowly as the mass invades the orbit or suddenly during
Received: April 11, 2016 Accepted: May 18, 2016
Corresponding Author: Jin Sook Yoon, MD, PhD. Institute of Vision Research, Department of Ophthalmology, Yonsei University College of Medicine, #50-1 Yonsei-ro, Seodaemun-gu, Seoul 03722, Korea. Tel: 82-2-2228-3570, Fax: 82-2-312-0541, E-mail: [email protected]

195
YJ Woo, et al. Treatment of Orbital Lymphangioma
hemorrhage of a lesion [3]. In childhood, the diagnosis is often made when proptosis occurs after bleeding as a re-sult of minor trauma or upper respiratory infection, and may even occur spontaneously. The lymphangioma itself or the associated bleeding can restrict ocular motility and cause compressive optic neuropathy because of its mass [4].
Lymphangiomas can also infiltrate diffusely into sur-rounding vital structures such as the optic nerve. This char-acteristic, along with the associated hemorrhage, presents many surgical challenges and renders management of orbit-al lymphangiomas very difficult. Several methods have been used to treat orbital lymphangioma, including systemic cor-ticosteroids, injection of a sclerosant, and surgical excision, but currently, there are no definitive curative treatments [5,6]. Case reports and studies of orbital lymphangioma are rare in the Korean population. Here we describe the characteristics and treatment outcomes in 12 Korean patients with orbital lymphangioma.
Materials and Methods
We retrospectively reviewed the medical records of 12 patients that had been diagnosed with orbital lymphangio-ma between January 2005 and May 2015 at the Severance Hospital, Yonsei University College of Medicine, Seoul, Ko-rea. The diagnosis was based on clinical manifestations, imaging studies, including computed tomography and mag-netic resonance imaging (MRI), and histologic findings when possible. Ophthalmic evaluation included measure-ment of visual acuity, intraocular pressure (IOP), ocular motility, and Hertel exophthalmometry. Patients without elevated IOP and no immediate threat to vision were treat-ed with oral corticosteroids. Patients threatened with loss of vision or severe disfigurement underwent aspiration of blood or partial resection (with or without intralesional in-jection of a sclerosant and application of continuous nega-tive pressure). The study adhered to the tenets of the Dec-laration of Helsinki. Ethical approval to conduct the study was obtained from the institutional review board at the Sev-erance Hospital of Yonsei University (No. 4-2015-0342).
Results
The demographic and clinical characteristics of the pa-
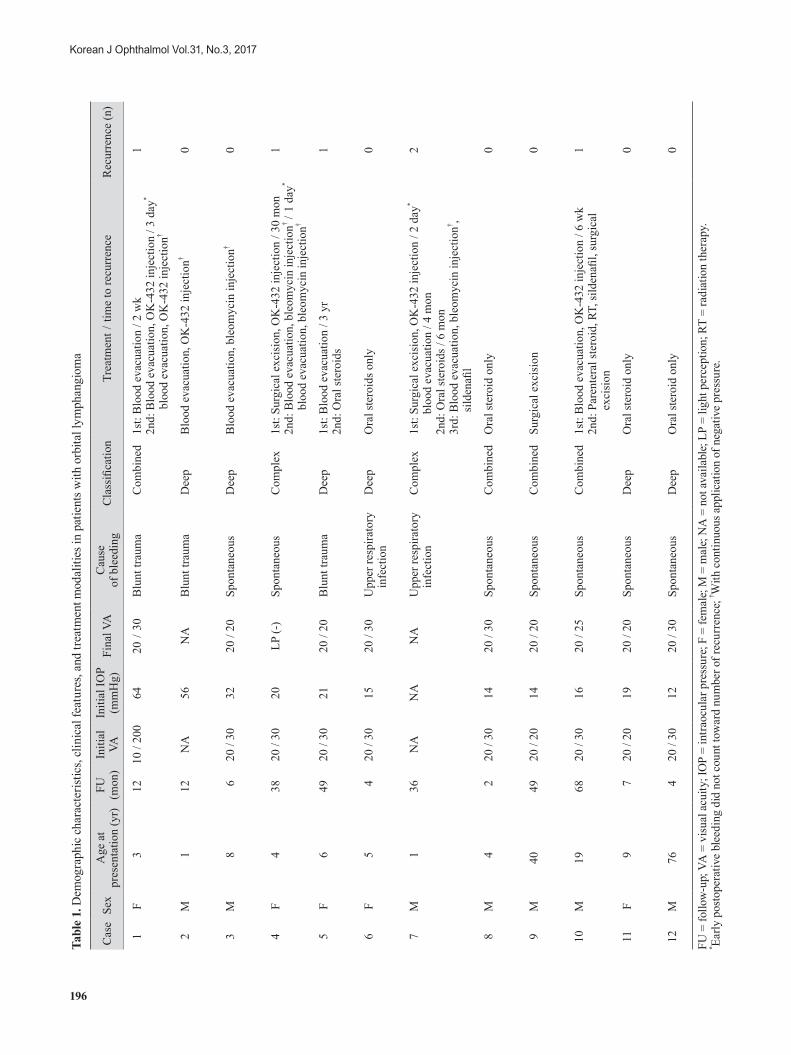
tients are detailed in Table 1. The mean patient age at pre-sentation was 14.7 years (range, 1 to 76; median, 5.5). Seven patients were male and five were female. Ten patients were diagnosed with orbital lymphangioma in childhood. The mean follow-up period was 22.8 months (range, 2 to 68). All of the patients initially presented with proptosis due to lesional hemorrhage and mass effect of the tumor. The causes of bleeding included blunt ocular trauma (n = 3), upper respiratory infection (n = 2), and a spontaneous event (n = 7). The tumors were classified as superficial (n = 0), deep (n = 6), combined (n = 4), or complex (n = 2) [5].
In patients that could be tested for visual acuity (n = 10), all but one had a visual acuity at presentation above 20 / 50. One patient had a visual acuity of 10 / 200 and two pa-tients could not be tested because of their young age. During treatment, one patient showed worsening of visual acuity to light perception negative, but the other patients did not experience any further impairment of visual acui-ty. An IOP above 21 mmHg was recorded in four patients. All patients had limited ocular motility and three had compressive optic neuropathy before or during follow-up.
Four patients (cases 6, 8, 11, and 12) were treated with oral corticosteroids only (Fig. 1A and 1B), but eight re-quired some form of surgical intervention. Five of the eight surgically treated patients experienced a recurrence of one or more hemorrhagic episodes. Among these, two patients (cases 4 and 7) underwent a partial resection and received an intralesional injection of a sclerosant, and three patients (cases 1, 5, and 10) underwent aspiration of blood (Fig. 2). In the two patients who underwent partial resection (cases 4 and 7), bleeding recurred from posterior residual lymph-angioma tissue. At reoperation, this residual tissue was difficult to approach due to its deep location. Overall, five patients (cases 1, 2, 3, 4, and 7) were treated successfully by aspiration of blood, intralesional injection of a sclero-sant (OK-432 in two cases and bleomycin in three cases), and application of continuous negative pressure by appro-priate drainage. Two patients (cases 9 and 10) experienced organized hematoma that caused proptosis for several months, but after partial resection, these patients eventual-ly had favorable outcomes (Table 1).
Case 4 description
A 4-year-old girl presented with a 1-day history of left-sided proptosis and eyelid swelling (Fig. 3A). She had
196
Korean J Ophthalmol Vol.31, No.3, 2017
Tabl
e 1.
Dem
ogra
phic
cha
ract
erist
ics,
clin
ical
feat
ures
, and
trea
tmen
t mod
aliti
es in
pat
ient
s with
orb
ital l
ymph
angi
oma
Cas
eSe
xA
ge a
t pr
esen
tatio
n (y
r)FU
(m
on)
Initi
al
VAIn
itial
IOP
(mm
Hg)
Fina
l VA
Cau
se
of b
leed
ing
Cla
ssifi
catio
nTr
eatm
ent /
tim
e to
recu
rren
ceR
ecur
renc
e (n
)
1F
312
10 /
200
6420
/ 30
Blu
nt tr
aum
aC
ombi
ned
1st:
Blo
od e
vacu
atio
n / 2
wk
2nd:
Blo
od e
vacu
atio
n, O
K-4
32 in
ject
ion
/ 3 d
ay*
b
lood
eva
cuat
ion,
OK
-432
inje
ctio
n†
1
2M
112
NA
56N
AB
lunt
trau
ma
Dee
pB
lood
eva
cuat
ion,
OK
-432
inje
ctio
n†0
3M
8 6
20 /
3032
20 /
20Sp
onta
neou
sD
eep
Blo
od e
vacu
atio
n, b
leom
ycin
inje
ctio
n† 0
4F
438
20 /
3020
LP (-
)Sp
onta
neou
sC
ompl
ex1s
t: Su
rgic
al e
xcis
ion,
OK
-432
inje
ctio
n / 3
0 m
on2n
d: B
lood
eva
cuat
ion,
ble
omyc
in in
ject
ion† /
1 da
y* b
lood
eva
cuat
ion,
ble
omyc
in in
ject
ion†
1
5F
649
20 /
3021
20 /
20B
lunt
trau
ma
Dee
p1s
t: B
lood
eva
cuat
ion
/ 3 y
r2n
d: O
ral s
tero
ids
1
6F
5 4
20 /
3015
20 /
30U
pper
resp
irato
ry
in
fect
ion
Dee
pO
ral s
tero
ids o
nly
0
7M
136
NA
NA
NA
Upp
er re
spira
tory
infe
ctio
nC
ompl
ex1s
t: Su
rgic
al e
xcis
ion,
OK
-432
inje
ctio
n / 2
day
* b
lood
eva
cuat
ion
/ 4 m
on2n
d: O
ral s
tero
ids /
6 m
on3r
d: B
lood
eva
cuat
ion,
ble
omyc
in in
ject
ion† ,
sild
enafi
l
2
8M
4 2
20 /
3014
20 /
30Sp
onta
neou
sC
ombi
ned
Ora
l ste
roid
onl
y0
9M
4049
20 /
2014
20 /
20Sp
onta
neou
sC
ombi
ned
Surg
ical
exc
isio
n0
10M
1968
20 /
3016
20 /
25Sp
onta
neou
sC
ombi
ned
1st:
Blo
od e
vacu
atio
n, O
K-4
32 in
ject
ion
/ 6 w
k2n
d: P
aren
tera
l ste
roid
, RT,
sild
enafi
l, su
rgic
al
exc
isio
n
1
11F
9 7
20 /
2019
20 /
20Sp
onta
neou
sD
eep
Ora
l ste
roid
onl
y0
12M
76 4
20 /
3012
20 /
30Sp
onta
neou
sD
eep
Ora
l ste
roid
onl
y0
FU =
follo
w-u
p; V
A =
visu
al a
cuity
; IO
P =
intra
ocul
ar p
ress
ure;
F =
fem
ale;
M =
mal
e; N
A =
not
ava
ilabl
e; L
P =
light
per
cept
ion;
RT
= ra
diat
ion
ther
apy.
* Early
pos
tope
rativ
e bl
eedi
ng d
id n
ot c
ount
tow
ard
num
ber o
f rec
urre
nce;
† With
con
tinuo
us a
pplic
atio
n of
neg
ativ
e pr
essu
re.
197
YJ Woo, et al. Treatment of Orbital Lymphangioma
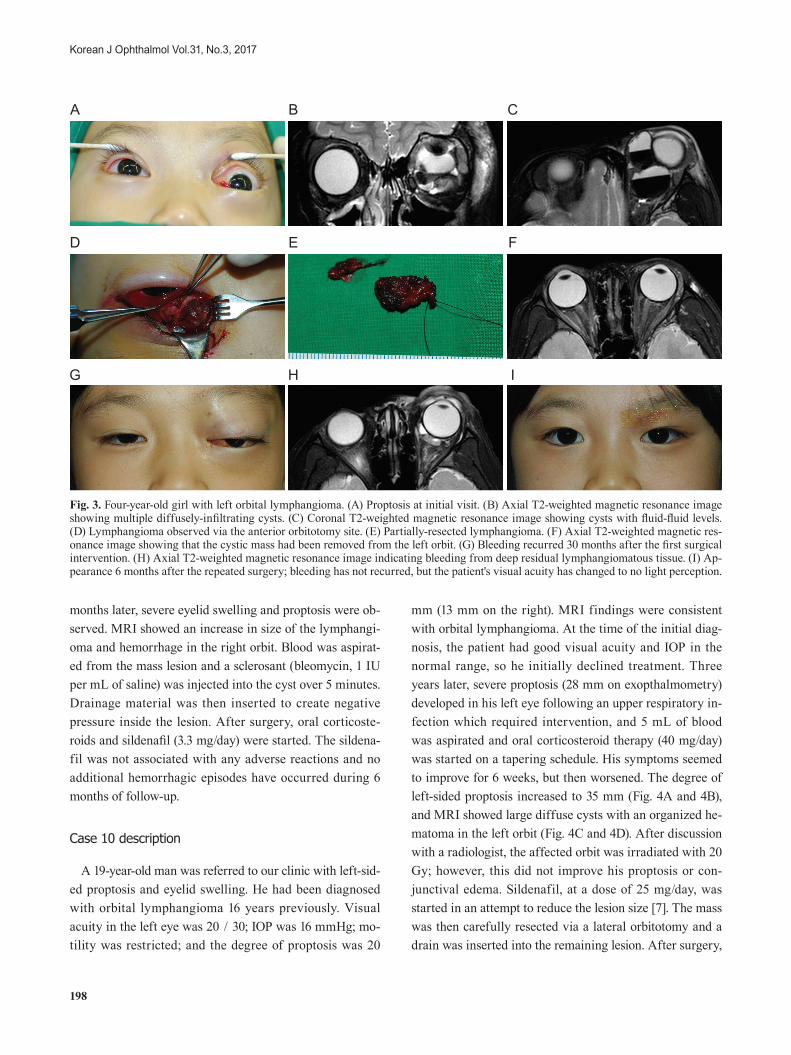
been treated with OK-432 (Picibanil; Chugai Pharmaceuti-cal, Tokyo, Japan) for a lymphatic malformation on her left forehead, frontal and temporal scalp 3 years previously, and the lesions had shrunk and little remained. Visual acu-ity in her affected eye was 20 / 30 and the IOP was 20 mmHg. Ocular motility was restricted in all directions and the degree of proptosis was 13 mm on the right and 19 mm on the left. MRI confirmed a diagnosis of lymphangioma, which consisted of multiple diffusely infiltrating cysts with fluid-fluid levels (Fig. 3B and 3C). The following day, the lesion was approached with a left upper eyelid sub-brow incision (Fig. 3D). Blood was aspirated, the lymphan-gioma was partially resected (Fig. 3E), and 0.05 mg of OK-432 diluted in 1 mL of physiologic saline was injected into the deep residual mass. The size of the mass subsequently decreased, which relieved the proptosis (Fig. 3F).
Thirty months later, the patient presented again after de-veloping severe painful proptosis and eyelid swelling, with vision that had decreased to 20 / 200 (Fig. 3G). A grade 2 relative afferent pupillary block was noted in her left eye. MRI showed recurrence of bleeding from the residual lymph-angioma tissue (Fig. 3H). Blood was aspirated via the pre-vious incision site and bleomycin (1 IU per mL of saline) was injected intralesionally over 10 minutes. A drain was inserted but did not function well. Bleeding recurred on the following day and the patient’s proptosis worsened. The previous incision site was reopened; blood was evacu-ated with a suction catheter; and the same concentration of bleomycin was injected into the residual mass over 10 min-utes. Another drain was inserted and continuous negative pressure was applied, with marked resolution of the pro-ptosis. Oral corticosteroids (10 mg/day) were given for 2 weeks and then tapered. The final visual acuity in the af-fected eye was light perception negative, most likely due to compression of the optic nerve by intraorbital hemorrhage. The hemorrhage around the optic nerve was evacuated carefully, so it is unlikely that damage to the optic nerve was caused by the surgery itself. The proptosis normalized 2 months after reoperation (Fig. 3I), and no additional hemorrhagic episodes have occurred in 12 months of fol-low-up observation.
Case 7 description
A 1-year-old boy presented with a 1-month history of right proptosis. He had previously been diagnosed with cystic lymphangioma on the right forehead. The forehead lesion had been surgically excised 7 months after birth, and remained small in size. MRI showed non-encapsulated lobulated intraconal and extraconal cystic masses in the right orbit. These were treated by aspiration of 5 mL of blood, partial resection of the mass, and an injection of OK-432 0.05 mg in 5 mL of physiologic saline into the an-terior orbitotomy site over 5 minutes. Two days later, the patient’s proptosis worsened because of hemorrhage, so 12 mL of blood was aspirated through the previous opening site and drainage material was inserted. Then, 10 mg of prednisolone was started on a tapering schedule, and the proptosis decreased. Four months after surgery, proptosis recurred in the right eye. MRI revealed a hemorrhage be-hind the previous lesion, so 12.5 mg of oral corticosteroids were administered and the proptosis slowly subsided. Six
A
B
Fig. 1. Patients with orbital lymphangioma that were successfully treated with oral corticosteroids. (A) Case 6, (B) case 8 (left col-umn, pretreatment; right column, posttreatment).
Fig. 2. Treatment modalities of patients with orbital lymphangio-ma who underwent surgical intervention and experienced recur-rent hemorrhage.
198
Korean J Ophthalmol Vol.31, No.3, 2017
months later, severe eyelid swelling and proptosis were ob-served. MRI showed an increase in size of the lymphangi-oma and hemorrhage in the right orbit. Blood was aspirat-ed from the mass lesion and a sclerosant (bleomycin, 1 IU per mL of saline) was injected into the cyst over 5 minutes. Drainage material was then inserted to create negative pressure inside the lesion. After surgery, oral corticoste-roids and sildenafil (3.3 mg/day) were started. The sildena-fil was not associated with any adverse reactions and no additional hemorrhagic episodes have occurred during 6 months of follow-up.
Case 10 description
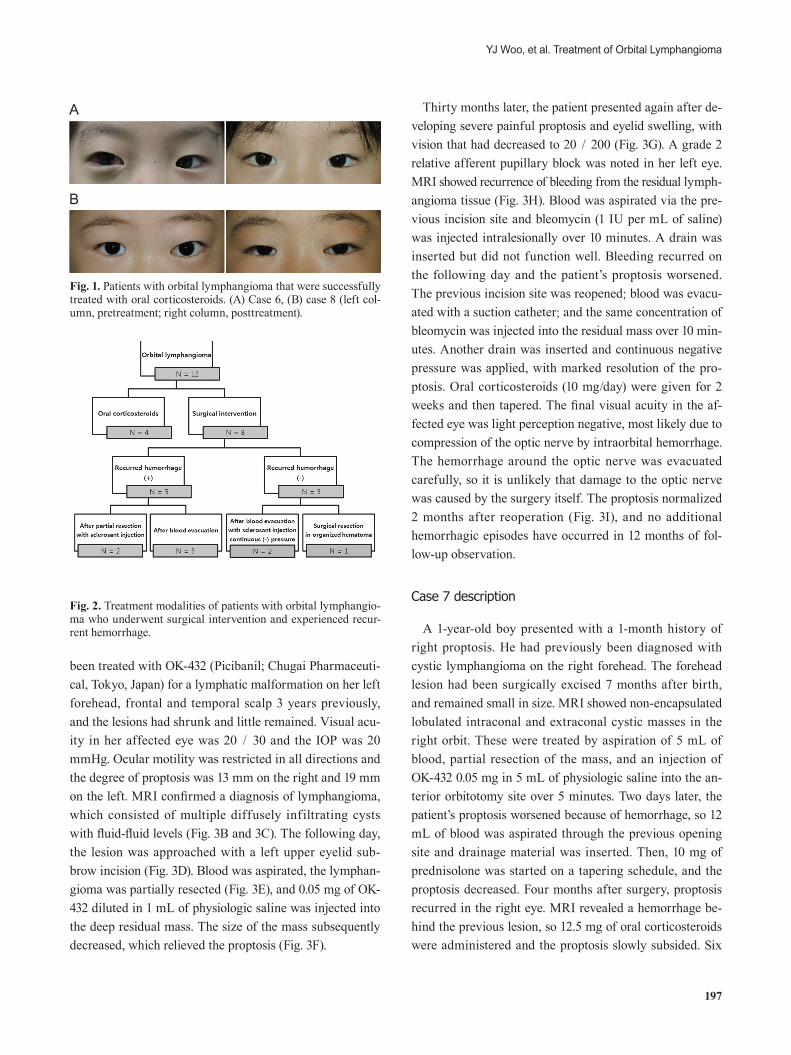
A 19-year-old man was referred to our clinic with left-sid-ed proptosis and eyelid swelling. He had been diagnosed with orbital lymphangioma 16 years previously. Visual acuity in the left eye was 20 / 30; IOP was 16 mmHg; mo-tility was restricted; and the degree of proptosis was 20
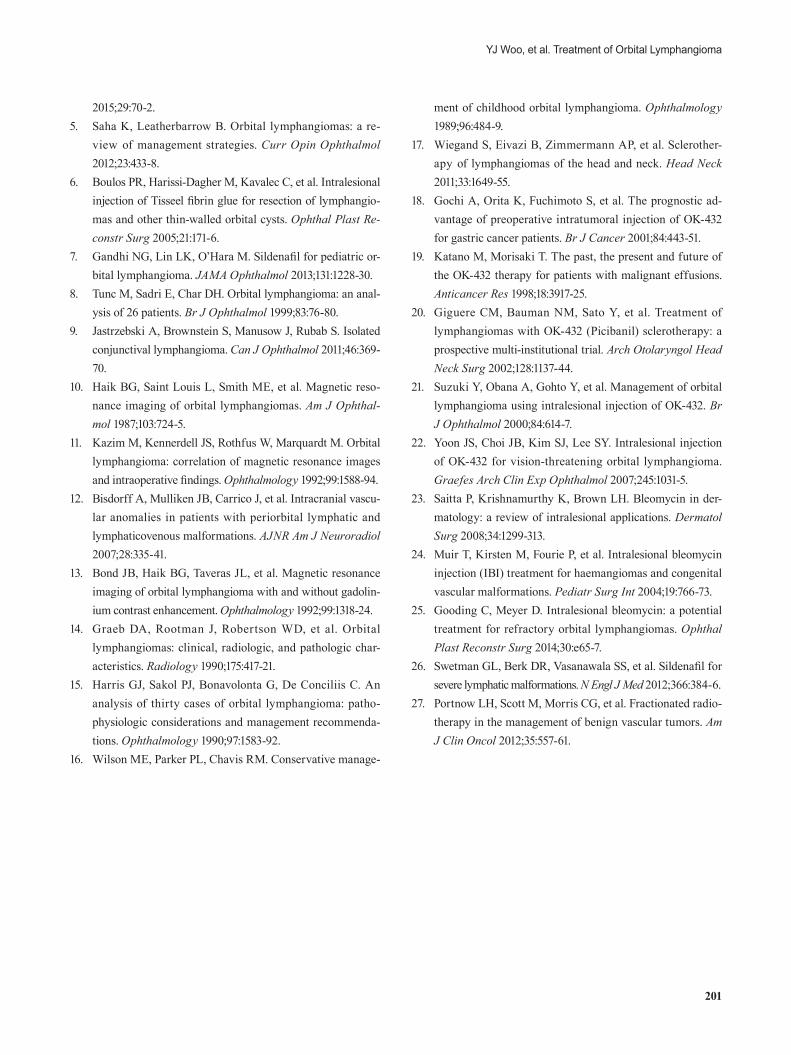
mm (13 mm on the right). MRI findings were consistent with orbital lymphangioma. At the time of the initial diag-nosis, the patient had good visual acuity and IOP in the normal range, so he initially declined treatment. Three years later, severe proptosis (28 mm on exopthalmometry) developed in his left eye following an upper respiratory in-fection which required intervention, and 5 mL of blood was aspirated and oral corticosteroid therapy (40 mg/day) was started on a tapering schedule. His symptoms seemed to improve for 6 weeks, but then worsened. The degree of left-sided proptosis increased to 35 mm (Fig. 4A and 4B), and MRI showed large diffuse cysts with an organized he-matoma in the left orbit (Fig. 4C and 4D). After discussion with a radiologist, the affected orbit was irradiated with 20 Gy; however, this did not improve his proptosis or con-junctival edema. Sildenafil, at a dose of 25 mg/day, was started in an attempt to reduce the lesion size [7]. The mass was then carefully resected via a lateral orbitotomy and a drain was inserted into the remaining lesion. After surgery,
A B C
D E F
G H I
Fig. 3. Four-year-old girl with left orbital lymphangioma. (A) Proptosis at initial visit. (B) Axial T2-weighted magnetic resonance image showing multiple diffusely-infiltrating cysts. (C) Coronal T2-weighted magnetic resonance image showing cysts with fluid-fluid levels. (D) Lymphangioma observed via the anterior orbitotomy site. (E) Partially-resected lymphangioma. (F) Axial T2-weighted magnetic res-onance image showing that the cystic mass had been removed from the left orbit. (G) Bleeding recurred 30 months after the first surgical intervention. (H) Axial T2-weighted magnetic resonance image indicating bleeding from deep residual lymphangiomatous tissue. (I) Ap-pearance 6 months after the repeated surgery; bleeding has not recurred, but the patient's visual acuity has changed to no light perception.

199
YJ Woo, et al. Treatment of Orbital Lymphangioma
the degree of proptosis was reduced to 16 mm and visual acuity was unimpaired, although hypotropia developed, along with ocular motility limitations (Fig. 4E and 4F). During 8 months of follow-up, hemorrhagic episodes have not recurred in this patient.
Discussion
Orbital lymphangioma is often detected when intrale-sional hemorrhage induces proptosis, which can occur ei-ther suddenly or gradually. Compressive optic neuropathy can develop when the hemorrhage is massive or the tumor itself compresses the optic nerve. Tunc et al. [8] reported that 85% of their patients with orbital lymphangioma had proptosis; 73% had ptosis; and 46% had reduced ocular motility. In our case series, all 12 patients had proptosis and limited ocular motility at presentation. Two patients had compressive optic neuropathy at presentation and one patient had visual acuity that deteriorated to light percep-tion negative, most likely because of prolonged compres-sion of the optic nerve by intraorbital hemorrhage.
Orbital lymphangioma can be classified into four types
based on location [5,9]. The superficial type is character-ized by subcutaneous or conjunctival lesions; the deep type shows orbital invasion; the combined type has super-ficial and deep components; and the complex type involves other head and neck structures. The tumors in our study were classified as deep, combined, and complex in six, four, and two patients, respectively. The mean age of our patients at presentation was 14.7 years, and 10 were diag-nosed with orbital lymphangioma in childhood. Because of the frequent early onset, treatment for orbital lymphangio-ma is directed at preventing amblyopia and preserving vi-sual acuity [5].
On computed tomography, orbital lymphangioma appears as a mildly enhancing cystic mass. MRI usually shows find-ings similar to those of computed tomography, but has bet-ter diagnostic accuracy because of higher resolution, and is safer because of the lack of ionizing radiation [10,11]. MRI may also indicate the presence of feeder vessels, in which case a diagnosis of orbital lymphangioma is excluded [12-14]. Overall, radiologic analysis alone has a diagnostic specificity of 77% for this type of tumor. However, orbital lymphangioma can sometimes be misdiagnosed as orbital hemangioma, rhabdomyosarcoma, or lymphoma when only imaging studies are used [7]. For this reason, in addi-tion to diagnosing the tumor based on clinical and radio-logic findings, we also confirmed the diagnosis histologi-cally when a surgical intervention was performed.
Diffuse infiltration and associated hemorrhage make this type of tumor difficult to remove surgically. Oral cortico-steroid therapy alone was effective in four of our patients, which is consistent with previous reports [14,15]. Systemic corticosteroids reduce lymphoid hypertrophy and stabilize the abnormal vasculature, leading to resolution of the lymphangioma. Therefore, orbital lymphangiomas do not necessarily require surgical intervention unless there are vision-threatening or severely disfiguring lesions [15,16].
Another useful modality for treating lymphangioma is intralesional injection of a sclerosant such as OK-432 or bleomycin [3,5,17]. OK-432 is prepared from a low-viru-lence Su strain of group A Streptococcus pyogenes of hu-man origin treated with penicillin G. It has been used to treat malignant tumors, pleural effusion, and malignant ascites [18,19]. According to Giguere et al. [20], injection of OK-432 decreases the size of head and neck lymphangio-mas. This claim is supported by case reports which demon-strated that orbital lymphangiomas are treatable with in-
A B
C D
E F
Fig. 4. Nineteen-year-old man with a 16-year history of left orbital lymphangioma. (A) Severe proptosis and conjunctival swelling before resection. (B) Exophthalmometry showing 35-mm protrusion of the left eyeball. (C) Coronal T2-weighted magnetic resonance image showing lymphangioma that occupied most of the left orbit. (D) Axial T2-weighted magnetic resonance image showing a large lymphangioma with organized hematoma an-teriorly displacing the left eyeball. (E) Reduced proptosis after partial resection. (F) Computed tomography image after partial resection.

200
Korean J Ophthalmol Vol.31, No.3, 2017
tralesional OK-432 [21,22]. Bleomycin, first isolated from Streptomyces verticillus in 1966 [23], has a sclerosing ef-fect on vascular endothelial cells and has been used to treat pleural effusion and vascular anomalies [24]. A literature search revealed that there were a few reports on the use of bleomycin injections to treat orbital lymphangioma, with no systemic or ophthalmic complications [4,25]. In our case series, five patients were successfully treated with in-tralesional injections of a sclerosant and application of continuous negative pressure. However, hemorrhage re-curred in patients who received injection of a sclerosant without application of continuous negative pressure. Thus, it is recommended that this modality be combined with as-piration of blood and application of continuous negative pressure using a correctly positioned drain.
Two patients received oral sildenafil in our study. Silde-nafil causes cystic lesions to collapse by decreasing the contractility of vascular smooth muscle [7,26]. However, we did not confirm this effect in our patients. The most com-mon adverse reactions of sildenafil are pyrexia, gastroin-testinal discomfort, cough, sleep disturbance, and migraine, but these were not observed in our cases. In one patient, orbital lymphangioma was fractionally irradiated with 20 Gy, as recommended by Portnow et al. [27], with the goal of reducing the size of the lesion. However, lymphangioma is not a rapidly proliferating lesion, so radiotherapy was ineffective for this purpose.
Five patients in our case series experienced recurrent hemorrhage. Two patients that had undergone partial re-section and intralesional injection of a sclerosant during an acute hemorrhagic episode experienced recurrence of hemorrhage from the remaining lymphangioma tissue sev-eral months after treatment. The posterior location of the residual mass made it difficult to evacuate blood and inject the sclerosant in these patients. Therefore, these findings indicate that the surgical approach becomes more difficult when bleeding occurs after partial resection. MRI showed that the mass tended to bulge toward the retrobulbar in-traconal space, because adhesions that arose after previous surgery blocked any superficial expansion. We hypothesize that a decrease in the available expansion space could in-crease the risk of compressive optic neuropathy. Three pa-tients who only underwent aspiration of blood also experi-enced recurrent hemorrhage, but blood could be easily removed through the previous incision site. In comparison, the patients in this study had favorable outcomes when
partial resection was applied, as demonstrated by the two cases of orbital lymphangioma that were associated with organized hematoma.
In summary, orbital lymphangioma that is not threaten-ing to vision can be medically treated with oral corticoste-roids. We suggest that aspiration of blood, intralesional in-jection of a sclerosant, and appropriate drainage to maintain continuous negative pressure are only necessary for pa-tients that have threatened vision, as we reported previous-ly [4]. Additionally, in cases of orbital lymphangioma that are associated with organized hematoma, partial resection can be considered to debulk the mass.
This case series describes manifestations and treatment outcomes of orbital lymphangioma in the Korean popula-tion. Our report helps to further knowledge on the clinical course, prognosis, and appropriate treatment modalities for patients with orbital lymphangioma.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This research was supported by the Bio & Medical Technology Development Program of the NRF funded by the Korean Government, Ministry of Science, ICT and Fu-ture Planning (2015M3A9E206703).
References
1. Guinto G, Guinto-Nishimura Y. Orbital lymphangiomas. World Neurosurg 2014;81:708-9.
2. Rootman J, Hay E, Graeb D, Miller R. Orbital-adnexal lymphangiomas: a spectrum of hemodynamically isolated vascular hamartomas. Ophthalmology 1986;93:1558-70.
3. Russin JJ, Rangel-Castilla L, Kalani MY, Spetzler RF. Sur-gical management, outcomes, and recurrence rate of orbital lymphangiomas. J Clin Neurosci 2015;22:877-82.
4. Lee KH, Han SH, Yoon JS. Successful treatment of orbital lymphangioma with intralesional bleomycin and applica-tion of continuous negative pressure. Korean J Ophthalmol
201
YJ Woo, et al. Treatment of Orbital Lymphangioma
2015;29:70-2.5. Saha K, Leatherbarrow B. Orbital lymphangiomas: a re-
view of management strategies. Curr Opin Ophthalmol 2012;23:433-8.
6. Boulos PR, Harissi-Dagher M, Kavalec C, et al. Intralesional injection of Tisseel fibrin glue for resection of lymphangio-mas and other thin-walled orbital cysts. Ophthal Plast Re-constr Surg 2005;21:171-6.
7. Gandhi NG, Lin LK, O’Hara M. Sildenafil for pediatric or-bital lymphangioma. JAMA Ophthalmol 2013;131:1228-30.
8. Tunc M, Sadri E, Char DH. Orbital lymphangioma: an anal-ysis of 26 patients. Br J Ophthalmol 1999;83:76-80.
9. Jastrzebski A, Brownstein S, Manusow J, Rubab S. Isolated conjunctival lymphangioma. Can J Ophthalmol 2011;46:369-70.
10. Haik BG, Saint Louis L, Smith ME, et al. Magnetic reso-nance imaging of orbital lymphangiomas. Am J Ophthal-mol 1987;103:724-5.
11. Kazim M, Kennerdell JS, Rothfus W, Marquardt M. Orbital lymphangioma: correlation of magnetic resonance images and intraoperative findings. Ophthalmology 1992;99:1588-94.
12. Bisdorff A, Mulliken JB, Carrico J, et al. Intracranial vascu-lar anomalies in patients with periorbital lymphatic and lymphaticovenous malformations. AJNR Am J Neuroradiol 2007;28:335-41.
13. Bond JB, Haik BG, Taveras JL, et al. Magnetic resonance imaging of orbital lymphangioma with and without gadolin-ium contrast enhancement. Ophthalmology 1992;99:1318-24.
14. Graeb DA, Rootman J, Robertson WD, et al. Orbital lymphangiomas: clinical, radiologic, and pathologic char-acteristics. Radiology 1990;175:417-21.
15. Harris GJ, Sakol PJ, Bonavolonta G, De Conciliis C. An analysis of thirty cases of orbital lymphangioma: patho-physiologic considerations and management recommenda-tions. Ophthalmology 1990;97:1583-92.
16. Wilson ME, Parker PL, Chavis RM. Conservative manage-
ment of childhood orbital lymphangioma. Ophthalmology 1989;96:484-9.
17. Wiegand S, Eivazi B, Zimmermann AP, et al. Sclerother-apy of lymphangiomas of the head and neck. Head Neck 2011;33:1649-55.
18. Gochi A, Orita K, Fuchimoto S, et al. The prognostic ad-vantage of preoperative intratumoral injection of OK-432 for gastric cancer patients. Br J Cancer 2001;84:443-51.
19. Katano M, Morisaki T. The past, the present and future of the OK-432 therapy for patients with malignant effusions. Anticancer Res 1998;18:3917-25.
20. Giguere CM, Bauman NM, Sato Y, et al. Treatment of lymphangiomas with OK-432 (Picibanil) sclerotherapy: a prospective multi-institutional trial. Arch Otolaryngol Head Neck Surg 2002;128:1137-44.
21. Suzuki Y, Obana A, Gohto Y, et al. Management of orbital lymphangioma using intralesional injection of OK-432. Br J Ophthalmol 2000;84:614-7.
22. Yoon JS, Choi JB, Kim SJ, Lee SY. Intralesional injection of OK-432 for vision-threatening orbital lymphangioma. Graefes Arch Clin Exp Ophthalmol 2007;245:1031-5.
23. Saitta P, Krishnamurthy K, Brown LH. Bleomycin in der-matology: a review of intralesional applications. Dermatol Surg 2008;34:1299-313.
24. Muir T, Kirsten M, Fourie P, et al. Intralesional bleomycin injection (IBI) treatment for haemangiomas and congenital vascular malformations. Pediatr Surg Int 2004;19:766-73.
25. Gooding C, Meyer D. Intralesional bleomycin: a potential treatment for refractory orbital lymphangiomas. Ophthal Plast Reconstr Surg 2014;30:e65-7.
26. Swetman GL, Berk DR, Vasanawala SS, et al. Sildenafil for severe lymphatic malformations. N Engl J Med 2012;366:384-6.
27. Portnow LH, Scott M, Morris CG, et al. Fractionated radio-therapy in the management of benign vascular tumors. Am J Clin Oncol 2012;35:557-61.