Splenic Lymphangioma (1)
5
Splenic Lymphangioma Ioannis Ioannidis, MD; Andrea G. Kahn, MD Splenic lymphangioma is a rare malformation of the splenic lymphatic channels, mostly seen in children. It is characterized by the presence of cysts, resulting from increases in the size and number of thin-walled lymphatic vessels that are abnormally interconnected and dilated. The condition may be restricted to the spleen, but in most cases it involves multiple organs (systemic lymphangioma- tosis). The clinical picture is variable; small lesions are often incidentally detected through imaging studies, while larger lesions can result in compression of organs, causing pain or rupture even after minor trauma. Therefore, splenic lymphangiomas should be considered in the differential diagnosis of splenomegaly or left upper quadrant pain even among adults and should be immedi- ately treated with splenectomy; delay in the therapeutic intervention can lead to life-threatening complications. (Arch Pathol Lab Med. 2015;139:278–282; doi: 10.5858/ arpa.2013-0656-RS) L ymphangiomas are benign malformations of the lym- phatic system, usually found in the neck (75%) and axilla (20%) 1 and less commonly encountered in the orbit, mediastinum, adrenal gland, kidney, bone, omentum, gastrointestinal tract, retroperitoneum, liver, and pancre- as. 2,3 They were first described by Rodender in 1828; however, the first case involving the spleen was reported in 1885 by Frink. 4,5 Between 1939 and 2010, only 189 cases of splenic lymphangiomas were reported in the literature. 6 Therefore, splenic lymphangiomas are considered uncom- mon benign tumors, occurring mainly in childhood, with only a few cases reported in adults. 7 In most patients, the lymphangiomatous process involves additional sites in a diffuse or multifocal fashion such as the liver, mediastinum, and lung, the so-called lymphangiomatosis syndrome. 7 Some cases of splenic lymphangiomas are associated with synchronous or metachronous cystic hygroma of the neck. 8 Isolated splenic lymphangiomas constitute a much rarer form; only 9 cases between 1990 and 2010 were reported. 9,10 Rarely, splenic lymphangiomas can be part of Klippel- Trenaunay syndrome (characterized by varicose veins, bony and soft tissue hypertrophy, cutaneous hemangiomas, and/ or malformations of the lymphatic system). 11 Although no consensus has yet been reached on whether splenic lymphangioma is a neoplasm or a hamartoma, most researchers support the latter opinion; its formation is proposed to be due to abnormal congenital development of lymphatic vessels. 5 It can also be attributed to bleeding or inflammation in the lymphatic system, which causes obstruction and consequent lymphangiectasia. 5,8,10 CLINICAL FEATURES The clinical manifestations of splenic lymphangiomas are usually related to the size of the spleen. 8 In most cases, isolated splenic lymphangiomas are asymptomatic and incidentally detected through abdominal ultrasonography or abdominal computed tomography. Large cystic lesions can attain sufficient size to cause significant symptoms and signs. 8,12 The symptoms may include left upper quadrant pain, loss of appetite, nausea, vomiting, and signs of abdominal distension or a palpable mass. Most are usually nonspecific and are due to compression of adjacent organs such as the stomach, diaphragm, or kidney. 8 Infection or rupture of a lymphangioma can present as an acute abdomen. 8,13 Cases have been reported of larger lymphan- giomas complicated by consumptive coagulopathy, bleed- ing, hypersplenism, and portal hypertension. 8,14 The pathophysiological consequences of a lymphangioma ex- ceeding 3 to 4 kg can be diaphragmatic immobility and lung atelectasis or pneumonia. 8,13 Rarely, hypertension due to compression of the renal artery by the splenic mass can be seen. 8,15 RADIOGRAPHIC FINDINGS In terms of imaging characteristics, the spleen may be of normal size, or splenomegaly can be present. 8 Ultrasonog- raphy typically reveals cysts of various sizes (ranging from a few millimeters to several centimeters in diameter). 8 These cystic lesions are hypoechoic or anechoic, with possible septations. 16 Minute echogenic calcifications may be iden- tified. 8 In one case report, 16 a lymphangioma presented as a mildly hyperechoic mass in the spleen. Color Doppler ultrasonography can demonstrate the vasculature of the mass (including the intrasplenic arteries and veins along the cyst walls). It may assist in determining the splenic origin by demonstrating the vessels at the splenic hilum. 8 Computed tomography usually shows low-density single or multiple thin-walled sharply marginated subcapsular cysts (Figure 1). 16 Although no significant contrast enhance- Accepted for publication December 27, 2013. From the Department of Pathology, University of South Alabama, Mobile. The authors have no relevant financial interest in the products or companies described in this article. Presented in part as a poster at the College of American Pathologists 2013 (CAP ’13) Annual Meeting; October 13, 2013; Orlando, Florida. Reprints: Ioannis Ioannidis, MD, Department of Pathology, University of South Alabama, Mobile, AL 36617 (e-mail: [email protected]). 278 Arch Pathol Lab Med—Vol 139, February 2015 Splenic Lymphangioma—Ioannidis & Kahn
-
Upload
diny-febriany-hasanah -
Category
Documents
-
view
17 -
download
4
description
n
Transcript of Splenic Lymphangioma (1)
-
Splenic LymphangiomaIoannis Ioannidis, MD; Andrea G. Kahn, MD
Splenic lymphangioma is a rare malformation of thesplenic lymphatic channels, mostly seen in children. It ischaracterized by the presence of cysts, resulting fromincreases in the size and number of thin-walled lymphaticvessels that are abnormally interconnected and dilated.The condition may be restricted to the spleen, but in mostcases it involves multiple organs (systemic lymphangioma-tosis). The clinical picture is variable; small lesions areoften incidentally detected through imaging studies, whilelarger lesions can result in compression of organs, causingpain or rupture even after minor trauma. Therefore,splenic lymphangiomas should be considered in thedifferential diagnosis of splenomegaly or left upperquadrant pain even among adults and should be immedi-ately treated with splenectomy; delay in the therapeuticintervention can lead to life-threatening complications.
(Arch Pathol Lab Med. 2015;139:278282; doi: 10.5858/arpa.2013-0656-RS)
Lymphangiomas are benign malformations of the lym-phatic system, usually found in the neck (75%) andaxilla (20%)1 and less commonly encountered in the orbit,mediastinum, adrenal gland, kidney, bone, omentum,gastrointestinal tract, retroperitoneum, liver, and pancre-as.2,3 They were first described by Rodender in 1828;however, the first case involving the spleen was reportedin 1885 by Frink.4,5 Between 1939 and 2010, only 189 casesof splenic lymphangiomas were reported in the literature.6
Therefore, splenic lymphangiomas are considered uncom-mon benign tumors, occurring mainly in childhood, withonly a few cases reported in adults.7 In most patients, thelymphangiomatous process involves additional sites in adiffuse or multifocal fashion such as the liver, mediastinum,and lung, the so-called lymphangiomatosis syndrome.7
Some cases of splenic lymphangiomas are associated withsynchronous or metachronous cystic hygroma of the neck.8
Isolated splenic lymphangiomas constitute a much rarerform; only 9 cases between 1990 and 2010 were reported.9,10
Rarely, splenic lymphangiomas can be part of Klippel-
Trenaunay syndrome (characterized by varicose veins, bonyand soft tissue hypertrophy, cutaneous hemangiomas, and/or malformations of the lymphatic system).11 Although noconsensus has yet been reached on whether spleniclymphangioma is a neoplasm or a hamartoma, mostresearchers support the latter opinion; its formation isproposed to be due to abnormal congenital development oflymphatic vessels.5 It can also be attributed to bleeding orinflammation in the lymphatic system, which causesobstruction and consequent lymphangiectasia.5,8,10
CLINICAL FEATURES
The clinical manifestations of splenic lymphangiomas areusually related to the size of the spleen.8 In most cases,isolated splenic lymphangiomas are asymptomatic andincidentally detected through abdominal ultrasonographyor abdominal computed tomography. Large cystic lesionscan attain sufficient size to cause significant symptoms andsigns.8,12 The symptoms may include left upper quadrantpain, loss of appetite, nausea, vomiting, and signs ofabdominal distension or a palpable mass. Most are usuallynonspecific and are due to compression of adjacent organssuch as the stomach, diaphragm, or kidney.8 Infection orrupture of a lymphangioma can present as an acuteabdomen.8,13 Cases have been reported of larger lymphan-giomas complicated by consumptive coagulopathy, bleed-ing, hypersplenism, and portal hypertension.8,14 Thepathophysiological consequences of a lymphangioma ex-ceeding 3 to 4 kg can be diaphragmatic immobility and lungatelectasis or pneumonia.8,13 Rarely, hypertension due tocompression of the renal artery by the splenic mass can beseen.8,15
RADIOGRAPHIC FINDINGS
In terms of imaging characteristics, the spleen may be ofnormal size, or splenomegaly can be present.8 Ultrasonog-raphy typically reveals cysts of various sizes (ranging from afew millimeters to several centimeters in diameter).8 Thesecystic lesions are hypoechoic or anechoic, with possibleseptations.16 Minute echogenic calcifications may be iden-tified.8 In one case report,16 a lymphangioma presented as amildly hyperechoic mass in the spleen.Color Doppler ultrasonography can demonstrate the
vasculature of the mass (including the intrasplenic arteriesand veins along the cyst walls). It may assist in determiningthe splenic origin by demonstrating the vessels at the splenichilum.8
Computed tomography usually shows low-density singleor multiple thin-walled sharply marginated subcapsularcysts (Figure 1).16 Although no significant contrast enhance-
Accepted for publication December 27, 2013.From the Department of Pathology, University of South Alabama,
Mobile.The authors have no relevant financial interest in the products or
companies described in this article.Presented in part as a poster at the College of American
Pathologists 2013 (CAP 13) Annual Meeting; October 13, 2013;Orlando, Florida.Reprints: Ioannis Ioannidis, MD, Department of Pathology,
University of South Alabama, Mobile, AL 36617 (e-mail:[email protected]).
278 Arch Pathol Lab MedVol 139, February 2015 Splenic LymphangiomaIoannidis & Kahn
-
ment is typically seen, rare cases are reported in theliterature in which computed tomography of solid cysticlymphangiomas showed no enhancement of the cysts butdemonstrated prominent enhancement of the solid compo-nents.16 The presence of curvilinear peripheral muralcalcifications is suggestive of cystic lymphangiomas but isnot a specific finding because it can also be seen in hydatidcysts.8,17
On T1-weighted magnetic resonance imaging, the cysticlesions can appear hypointense relative to the surroundingviscera or hyperintense when filled with hemorrhagic orproteinaceous material.7,8 On T2-weighted images, the massis characterized by multiloculated hyperintense areas thatcorrespond to the dilated lymphatic channels.7 The inter-vening septa are demonstrated as hypointense bandsbecause they bear abundant amounts of fibrous connectivetissue.8 The curvilinear peripheral mural calcifications seenon computed tomography are difficult to identify on
magnetic resonance imaging. However, the high contrastresolution of magnetic resonance imaging may help detectthe solid elements within the cystic lumen in the extremelyrare case in which malignant elements can be present.18 Inone case report,19 instead of the usual pattern of multiplewell-defined cystic lesions, there was diffuse involvementreplacing the entire spleen, with heterogeneous signalintensities on T2-weighted images and heterogeneousenhancement.Finally, positron emission tomography is not routinely
used for the diagnosis of splenic lymphangiomas. However,in a patient with 2 synchronous colon cancers that presentedwith concomitant splenic mass (initially suspected to bemetastatic), it helped confirm that the lesion was benign byrevealing no fludeoxyglucose uptake.16
GROSS FINDINGS
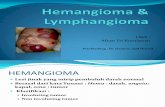
Depending on the size of the lesion, the spleen may besignificantly enlarged or within normal limits. The macro-scopic appearance of splenic lymphangioma is characterizedby a broad spectrum, including solitary nodules, multiplenodules, and diffuse lymphangiomatosis.8 Because lym-phatics are only found in the subcapsular region or in largetrabeculae, a solitary focal lymphangioma is most commonlysubcapsular and in some instances intraparenchymal. Thenodule usually consists of a single large cyst with a thickfibrous wall or multiple various-sized thin-walled cysts withhoneycombing filled with clear fluid. Solid areas may beseen, usually due to central scarring.4,20 Lymphangiomaspresenting as multiple nodules have similar-appearingsatellite lesions surrounding a larger lesion, are separatedby distinct residual splenic tissue, and can cause the spleento be nodular and enlarged.8 Cases of diffuse lymphangio-matosis can replace the spleen with expanding cysts thatresult in little remaining normal parenchyma (Figure 2).15,21
Based on the size of the dilated lymphatic channels,
Figure 1. Computed tomography showing an enlarged spleendiffusely involving multiple low-attenuation lesions.
Figure 2. A, Diffuse splenic lymphangiomatosis presenting with multiple nodules that involve the entire splenic parenchyma. B, Cross-sectionsreveal multiple cystic spaces of various diameters filled with serous fluid.
Arch Pathol Lab MedVol 139, February 2015 Splenic LymphangiomaIoannidis & Kahn 279
-
lymphangiomas can be classified as capillary (supermicro-cystic), cavernous (microcystic), or cystic (macrocystic).Therefore, if the lymphangioma consists of lymphatics thathave the size of capillaries, it is classified as capillary(microcystic), and if it consists of lymphatics that approachthe size of venules or veins, it is classified as cavernous(microcystic) or cystic (macrocystic), respectively. Thisnomenclature can be confusing as it is reminiscent of theclassification of hemangiomas, and because the distinctionis not always clear, it is not uniformly accepted amongpathologists.16,22
MICROSCOPIC FINDINGS
Histologic analysis reveals a single cyst or multiple cysticstructures (Figure 3, A) filled with eosinophilic amorphousproteinaceous material (Figure 3, B) and lined by a flat layerof attenuated endothelial cells (Figure 3, C).5,8 Rarely, thelining of the cysts may form papillary projections.23 The wallof the cysts ranges from thin and delicate to thick andobviously fibrous. A varying number of macrophages orlymphocytes can be found in the cystic spaces. Thesurrounding parenchyma may be normal or show evidenceof congestion and fibrosis. Very few cases of splenic
lymphangiomas transforming into malignant lymphangio-sarcomas have been reported.8 When atypical morphologyof the endothelium is present, careful long-term follow-upobservation of affected patients is recommended to deter-mine whether these features indicate malignancy or simplyan unusual morphologic appearance of the endothelialcells.8
Immunohistochemistry
When the histologic characteristics are not clear, theendothelial origin of the cyst may be established withimmunohistochemical techniques to demonstrate reactivityfor CD31, CD34, factor VIII, podoplanin (D2-40), or vascularendothelial growth factor receptor 3 (VEGFR-3).24 D2-40 isa monoclonal antibody against dysgerminoma, observed toselectively stain lymphatic endothelium (Figure 3, D). TheD2-40 antibody was also found to positively stain lymph-angiomas but not benign tumors of blood vessels.24 It hasbeen suggested that VEGFR-3 immunopositivity indicatespartial lymphatic endothelial differentiation or, alternatively,vascular endothelial growth factor C production by thetumor cells that stimulate proliferation of adjacent lymphat-ics.24 On the other hand, factor VIII, CD31, or CD34
Figure 3. A, Diffuse splenic lymphangiomatosis presenting with multiple cysts surrounding a central solid area with scarring (hematoxylin-eosin[H&E], original magnification34). B, The cysts are filled with amorphous proteinaceous material (H&E, original magnification310). C, The lining ofthe cysts consists of attenuated endothelial cells (H&E, original magnification 340). D, The lining of the cysts is highlighted with the lymphaticendothelial marker D2-40 (immunoperoxidase, original magnification340).
280 Arch Pathol Lab MedVol 139, February 2015 Splenic LymphangiomaIoannidis & Kahn
-
highlight endothelial cells in lymphatics and in bloodvessels.24
Electron Microscopy
Electron microscopy may assist in determining theendothelial origin of the cells lining the cyst. It can highlightthe presence of rod-shaped microtubulated bodies (Weibel-Palade bodies), which are the storage granules of endothe-lial cells.23
DIFFERENTIAL DIAGNOSIS
The differential diagnosis of splenic lymphangiomasincludes hemangiomas, true (splenic) epidermoid cysts,mesothelial cysts, and parasitic cysts (most commonly dueto Echinococcus granulosus).25 Hemangiomas are character-ized by vascular channels lined by endothelium, but they areextensively filled with red blood cells instead of theamorphous proteinaceous material of lymphangiomas. D2-40 positivity can assist in highlighting the lymphaticendothelial differentiation; however, attention should begiven to the fact that D2-40 can also stain myoepithelial cellsof blood vessels.24 True splenic cysts will have definiteepithelial lining and will be positive for cytokeratin, whilethe cells lining a mesothelial cyst will be positive formesothelial cell markers such as Wilms tumor 1 (WT-1)and calretinin.26 To exclude a hydatid cyst in a patient with acystic splenic mass, a serologic test for Echinococcus shouldbe performed. If removed, the cyst will consist of 3 layers(innermost germinal layer, intermediate laminated mem-brane, and outer fibrous layer) and contain protoscolices(attached or separated) with a double row of refractile,birefringent, acid-fast hooklets 22 to 40 lm in size and 4round suckers that comprise the hydatid sand. Finally, in ayoung patient with splenic lymphangioma, the diagnosticevaluation should be extended to include extrasplenic organsbecause it has been observed that in younger patients thelikelihood of multiorgan involvement is greater.8
TREATMENT AND PROGNOSIS
The treatment of choice for splenic lymphangiomas iscomplete surgical resection because other therapeuticmodalities (aspiration, drainage, and irradiation) haveshown unsatisfactory results.27,28 Some investigators preferconservative treatment in the case of small asymptomaticlesions detected incidentally, reserving splenectomy forlarge, multiple, or symptomatic lesions.27,29 Partial resectiontechniques have also been applied in cases of limiteddisease; however, leaving a splenic remnant in cases ofdiffuse involvement increases the risk of further growth andenlargement, sometimes requiring a second operation.Laparoscopic splenectomy is emerging as the procedure ofchoice in patients with a normal to moderately enlargedspleen but is considered a contraindication in patients withmassive splenomegaly.30 The most important aspect whenconsidering treatment options is that surgery should berecommended immediately after the diagnosis has beenestablished to avoid complications such as infection,hemorrhage, rupture, intestinal obstruction, and tumorenlargement that may eventually prevent complete remov-al.27 The prognosis of splenic lymphangioma after resectionis favorable. The main complication is recurrence, which isdemonstrated in 9.5% of patients, frequently after incom-plete resection.5
CONCLUSION
Splenic lymphangioma is a rare malformation of thesplenic lymphatic system, mostly seen in children and rarelyin adults. Although the etiology is still unclear, it isconsidered more likely a hamartomatous process ratherthan a neoplasm. Histologically, splenic lymphangioma ischaracterized by the presence of cysts lined by attenuatedendothelial cells. The condition may involve only the spleen,but in most cases it is part of a systemic malformation oflymphatic channels that affects multiple organs (systemiclymphangiomatosis). Most lesions are incidentally detectedthrough imaging studies, while larger lesions can causecompression of adjacent organs, with various symptoms.Therefore, splenic lymphangiomas should be considered inthe differential diagnosis of splenomegaly or left upperquadrant pain even among adults because they areamenable to curative treatment. Delay in their surgicalintervention may lead to severe complications such asinfection, rupture, and hemorrhage.
References
1. Kosir MA, Sonnino RE, Gauderer MW. Pediatric abdominal lymphangio-mas: a plea for early recognition. J Pediatr Surg. 1991;26(11):13091313.
2. Davidson AJ, Hartman DS. Lymphangioma of the retroperitoneum: CT andsonographic characteristic. Radiology. 1990;175(2):507510.
3. Chang WC, Liou CH, Kao HW, Hsu CC, Chen CY, Yu CY. Solitarylymphangioma of the spleen: dynamic MR findings with pathological correlation.Br J Radiol. 2007;80(949):e4e6. http://bjr.birjournals.org/content/80/949/e4.long. Accessed January 10, 2013.
4. Avigad S, Jaffe R, Frand M, Izhak Y, Rotem Y. Lymphangiomatosis withsplenic involvement. JAMA. 1976;236(20):23152317.
5. Chung SH, Park YS, Jo YJ, et al. Asymptomatic lymphangioma involving thespleen and retroperitoneum in adults. World J Gastroenterol. 2009;15(44):56205623.
6. Asch MJ, Cohen AH, Moore TC. Hepatic and splenic lymphangiomatosiswith skeletal involvement: report of a case and review of the literature. Surgery.1974;76(2):334339.
7. Solomou EG, Patriarheas GV, Mpadra FA, Karamouzis MV, Dimopoulos I.Asymptomatic adult cystic lymphangioma of the spleen: case report and reviewof the literature. Magn Reson Imaging. 2003;21(1):8184.
8. Abbott RM, Levy AD, Aguilera NS, Gorospe L, Thompson WM. From thearchives of the AFIP: primary vascular neoplasms of the spleen: radiologic-pathologic correlation. Radiographics. 2004;24(4):11371163.
9. Wadsworth DT, Newman B, Abramson SJ, Carpenter BL, Lorenzo RL.Splenic lymphangiomatosis in children. Radiology. 1997;202(1):173176.10. Patti R, Iannitto E, Di Vita G. Splenic lymphangiomatosis showing rapid
growth during lactation: a case report. World J Gastroenterol. 2010;16(9):11551157.11. Jindal R, Sullivan R, Rodda B, et al. Splenic malformation in a patient with
Klippel-Trenaunay syndrome: a case report. J Vasc Surg. 2006;43(4):848850.12. Komatsuda T, Ishida H, Konno K, et al. Splenic lymphangioma: US and CT
diagnosis and clinical manifestations. Abdom Imaging. 1999;24(4):414417.13. Moir C, Guttman F, Jequier S, Sonnino R, Youssef S. Splenic cysts:
aspiration, sclerosis, or resection. J Pediatr Surg. 1989;24(7):646648.14. Dietz WH Jr, Stuart MJ. Splenic consumptive coagulopathy in a patient
with disseminated lymphangiomatosis. J Pediatr. 1977;90(3):421423.15. Economides NG, Benton BF, Fortner TM, Miles RM. Splenic pseudocysts:
report of two cases and review of the literature. Am Surg. 1980;46(11):644648.16. Eghtedari M, Sicklick J, Kono Y, Peterson MR, Santillan CS. Unusual
imaging profile of a solitary splenic lymphangioma. Acta Radiol Short Rep. 2012;1(8). http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3738359/. Accessed January10, 2013.17. Rasheed K, Zargar SA, Telwani AA. Hydatid cyst of spleen: a diagnostic
challenge. N Am J Med Sci. 2013;5(1):1020.18. Feigenberg Z, Wysenbeek A, Avidor E, Dintsman M. Malignant lymphan-
gioma of the spleen. Isr J Med Sci. 1983;19(2):202204.19. Vanhoenacker FM, Schepper AM, Raeve H, Berneman Z. Cystic
angiomatosis with splenic involvement: unusual MRI findings. Eur Radiol.2003;13(suppl 6):L35L39.20. Chan KW, Saw D. Distinctive, multiple lymphangiomas of spleen. J Pathol.
1980;131(1):7581.21. Park JY, Song KT. Splenic cyst: a case report and review of literature. Am
Surg. 1971;37(9):544547.22. Yang F, Chen WX. Splenic lymphangioma that manifested as a solid-cystic
mass: a case report. World J Gastroenterol. 2013;19(5):781783.23. Takayama A, Nakashima O, Kobayashi K, Kojiro M. Splenic lymphangioma
with papillary endothelial proliferation: a case report and review of the literature.Pathol Int. 2003;53(7):483488.
Arch Pathol Lab MedVol 139, February 2015 Splenic LymphangiomaIoannidis & Kahn 281
-
24. Debelenko LV, Perez-Atayde AR, Mulliken JB, Liang MG, Archibald TH,Kozakewich HP. D2-40 immunohistochemical analysis of pediatric vasculartumors reveals positivity in kaposiform hemangioendothelioma. Mod Pathol.2005;18(11):14541460.25. Ferrozzi F, Bova D, Draghi F, Garlaschi G. CT findings in primary vascular
tumors of the spleen. AJR Am J Roentgenol. 1996;166(5):10971101.26. Cibas ES. Pleural, pericardial, and peritoneal fluids. In: Cibas ES,
Ducatman BS, eds. Cytology: Diagnostic Principles and Clinical Correlates. 3rded. Philadelphia, PA: Saunders; 2009:129153.
27. Yu X, Yu J, Liang P, Liu F. Real-time contrast-enhanced ultrasound indiagnosing of focal spleen lesions. Eur J Radiol. 2012;81(3):430436.28. Makrin V, Avital S, White I, Sagie B, Szold A. Laparoscopic splenectomy for
solitary splenic tumors. Surg Endosc. 2008;22(9):20092012.29. Lam KY, Tang V. Metastatic tumors to the spleen: a 25-year clinicopath-
ologic study. Arch Pathol Lab Med. 2000;124(4):526530.30. Maurus CF, Schafer M, Muller MK, Clavien PA, Weber M. Laparoscopic
versus open splenectomy for nontraumatic diseases. World J Surg. 2008;32(11):24442449.
Prepare Now for the CAP 15 Abstract Program
Dont Wait! Plan now to submit abstracts and case studies for the College of AmericanPathologists (CAP) 2015 meeting, which will be held October 4th Nashville, Tenn.Submissions for the CAP 15 Abstract Program will be accepted from:
Monday, February 9, 2015 through 6 p.m. Central timeFriday, April 10, 2015
Accepted submissions will appear online on the Archives of Pathology & LaboratoryMedicineWeb site as a supplement to the October 2015 issue. Visit the CAP 15 Web site athttp://www.cap.org/cap15 for additional abstract program information as it becomesavailable.
282 Arch Pathol Lab MedVol 139, February 2015 Splenic LymphangiomaIoannidis & Kahn