Optimizing arousal to manage aggression: A pilot study of …€¦ · · 2014-05-14Feature...
12
Feature Article Optimizing arousal to manage aggression: A pilot study of sensory modulation Daniel Sutton, 1 Michael Wilson, 4 Kirsten Van Kessel 2 and Jane Vanderpyl 3 1 Occupational Science and Therapy, 2 Psychology, Auckland University of Technology, 3 Research, Te Pou, Auckland, New Zealand; and 4 Programs, Queensland Alliance for Mental Health, Brisbane, Queensland, Australia ABSTRACT: The dominant model that informs clinical training for preventing violence and managing aggression posits arousal as mediated downwards from higher cortical structures. This view results in an often-misplaced reliance on verbal and cognitive techniques for de-escalation. The emergence of sensory modulation, via the Six Core Strategies, is an alternative or complementary approach that is associated with reduced rates of seclusion and restraint. Sensory-based interventions are thought to promote adaptive regulation of arousal and emotion, but this connection has had limited theoretical and empirical development. This paper presents results of a pilot trial of sensory-based interventions in four inpatient mental health units in New Zealand. Narrative analysis of interview and focus group data suggest that modifications to the environment and the use of soothing stimuli moderate or optimize arousal and promote an ability to adaptively regulate emotion. Findings are discussed in light of recent advances in the neurophysiology of emotional regulation and the General Aggression Model that posits arousal and maladaptive emotional regulation as precursors to aggression. KEY WORDS: aggression, arousal, behaviour mechanism, coercion, inpatients. INTRODUCTION The training for nurses in managing violent situations has progressed significantly over the past 20 years. Practice is now guided by theory, and discrete skill modules such as de-escalation have replaced intuitive judgement about handling volatile situations (Paterson et al. 1997). The language of ‘control and restraint’ has been explicitly rejected in favour of ‘calming and restraint’ or other for- mulations that do not evoke the language of correctional services (Paterson 2009). Despite these improvements, clinicians still ‘believe in’ seclusion as a useful tool (van Doesselaar et al. 2008; p. 97), and manual restraint of inpatients is increasing (Bowers et al. 2012). These features indicate that nursing practice remains at odds with both nursing values and the evidence base for clinical practice (Sailas & Fenton 2000). This dilemma arises, in part, from limitations in our understanding of arousal and consequential gaps in our management of mediators and precursors of aggression. Chief among these precursors is autonomic arou- sal, which is known to influence affect and emotion (Schachter & Singer 1962), and can lead to aggressive behaviour (Berkowitz 2001). While arousal is mediated along afferent and efferent neurological pathways, clinical training for de-escalating aroused states has a distinct bias toward a ‘top-down’ efferent model. This ‘top-down’ model describes the modulation of emotional response from cortical brain structures that elaborate the emotions and regulate affective behaviour (Beauchaine 2001; Pank- sepp 1982). The dominance of this model is manifested in Selye’s (1936) general adaptation syndrome where the fight/flight response flows along the hypothalamus– pituitary–adrenal axis. This approach is also typified in clinical training to manage aggression through a process Correspondence: Michael Wilson, Programs, Queensland Alliance for Mental Health, 266 Brunswick Street, Fortitude Valley, Brisbane, QLD 4006, Australia. Email: [email protected] Daniel Sutton, PhD, OT/r. Michael Wilson, MA, RN. Kirsten Van Kessel, PhD. Jane Vanderpyl, PhD. Accepted November 2012. International Journal of Mental Health Nursing (2013) 22, 500–511 doi: 10.1111/inm.12010 © 2013 The Authors International Journal of Mental Health Nursing © 2013 Australian College of Mental Health Nurses Inc.
Transcript of Optimizing arousal to manage aggression: A pilot study of …€¦ · · 2014-05-14Feature...

Feature Article
Optimizing arousal to manage aggression:A pilot study of sensory modulation
Daniel Sutton,1 Michael Wilson,4 Kirsten Van Kessel2 and Jane Vanderpyl3
1Occupational Science and Therapy, 2Psychology, Auckland University of Technology, 3Research, Te Pou, Auckland,New Zealand; and 4Programs, Queensland Alliance for Mental Health, Brisbane, Queensland, Australia
ABSTRACT: The dominant model that informs clinical training for preventing violence and managingaggression posits arousal as mediated downwards from higher cortical structures. This view results inan often-misplaced reliance on verbal and cognitive techniques for de-escalation. The emergence ofsensory modulation, via the Six Core Strategies, is an alternative or complementary approach that isassociated with reduced rates of seclusion and restraint. Sensory-based interventions are thought topromote adaptive regulation of arousal and emotion, but this connection has had limited theoretical andempirical development. This paper presents results of a pilot trial of sensory-based interventions in fourinpatient mental health units in New Zealand. Narrative analysis of interview and focus group datasuggest that modifications to the environment and the use of soothing stimuli moderate or optimizearousal and promote an ability to adaptively regulate emotion. Findings are discussed in light of recentadvances in the neurophysiology of emotional regulation and the General Aggression Model that positsarousal and maladaptive emotional regulation as precursors to aggression.
KEY WORDS: aggression, arousal, behaviour mechanism, coercion, inpatients.
INTRODUCTION
The training for nurses in managing violent situations hasprogressed significantly over the past 20 years. Practice isnow guided by theory, and discrete skill modules such asde-escalation have replaced intuitive judgement abouthandling volatile situations (Paterson et al. 1997). Thelanguage of ‘control and restraint’ has been explicitlyrejected in favour of ‘calming and restraint’ or other for-mulations that do not evoke the language of correctionalservices (Paterson 2009). Despite these improvements,clinicians still ‘believe in’ seclusion as a useful tool(van Doesselaar et al. 2008; p. 97), and manual restraintof inpatients is increasing (Bowers et al. 2012). These
features indicate that nursing practice remains at oddswith both nursing values and the evidence base for clinicalpractice (Sailas & Fenton 2000). This dilemma arises, inpart, from limitations in our understanding of arousal andconsequential gaps in our management of mediators andprecursors of aggression.
Chief among these precursors is autonomic arou-sal, which is known to influence affect and emotion(Schachter & Singer 1962), and can lead to aggressivebehaviour (Berkowitz 2001). While arousal is mediatedalong afferent and efferent neurological pathways, clinicaltraining for de-escalating aroused states has a distinctbias toward a ‘top-down’ efferent model. This ‘top-down’model describes the modulation of emotional responsefrom cortical brain structures that elaborate the emotionsand regulate affective behaviour (Beauchaine 2001; Pank-sepp 1982). The dominance of this model is manifestedin Selye’s (1936) general adaptation syndrome wherethe fight/flight response flows along the hypothalamus–pituitary–adrenal axis. This approach is also typified inclinical training to manage aggression through a process
Correspondence: Michael Wilson, Programs, Queensland Alliancefor Mental Health, 266 Brunswick Street, Fortitude Valley, Brisbane,QLD 4006, Australia. Email: [email protected]
Daniel Sutton, PhD, OT/r.Michael Wilson, MA, RN.Kirsten Van Kessel, PhD.Jane Vanderpyl, PhD.Accepted November 2012.
bs_bs_banner
International Journal of Mental Health Nursing (2013) 22, 500–511 doi: 10.1111/inm.12010
© 2013 The AuthorsInternational Journal of Mental Health Nursing © 2013 Australian College of Mental Health Nurses Inc.

that employs social learning theory of aggression thatposits aggression as a cognitive process, enacted throughschema that have been learned across the lifespan. Thisview is reflected in clinical training which describes anescalation axis from anxious, to agitated, to verbally orposturally threatening, to potentially lethal behaviours,followed by stages of crisis resolution. This pathway pref-erence does not allow for an arousal process that could berecursive, and capable of self-regulation (Richter 2006).Thus, when the clinical responses of validation, negotia-tion, and warning fail, as they sometimes do, practicessuch as restraint or seclusion are often the only optionsremaining (Perkins et al. 2012).
With the launch of the Six Core Strategies to reduceseclusion and restraint (Huckshorn 2006), sensory modu-lation (Champagne 2011) emerged as a suite of sensory-based interventions that provide an alternative, afferentor ‘bottom-up’, response to arousal or aggression. As atool for reducing coercive events, sensory interventionsseem to de-escalate aroused states and eliminate the riskof restrictive responses by clinical staff (Champagne &Stromberg 2004; Cummings et al. 2010; Lee et al. 2010).Deliberate use of selected sensory inputs have beenshown to moderate arousal (Miller et al. 2007), thusallowing individuals to become aware of emotions aswell as equipping the person with a strategy and toolsfor adaptive emotional regulation (Ogden et al. 2006). Arecent review of contemporary research into the role ofemotional regulation in aggression found clear evidencethat maladaptive emotional regulation can cause aggres-sive behaviour (Roberton et al. 2012).
Under-regulation of emotions, particularly anger,usually becomes aggression as a way to terminate difficultemotional situations, while over-regulation contributes toaggression by increasing physiological arousal and raisingthe likelihood of activating suppressed emotional triggers.In the face of a difficult situation, the deliberate use ofemotion regulation strategies could enable individuals to‘contain the emotion experience sufficiently to engagein goal directed behaviours while allowing the emotionexperience to run its course’ (Roberton et al. 2012; p. 74).The problem seems to be that alternatives that promotethis outcome remain virtually unknown. A recent reviewof practice found that nurses engage in restraint, in part,because they are not aware of alternatives to taking anaggressive person to a horizontal position (Perkins et al.2012). There is a need to develop a suite of strategies tohelp nurses and other clinicians promote optimal arousalto assist the person to self-regulate emotion.
It is likely that sensory interventions perform the func-tion of allowing emotional experiences to be contained so
that adaptive behaviours can be engaged. Such ade-escalation pathway could provide a set of practicaltools for preventing distress moving to aggression.However, the relationship between sensory input andemotional regulation has not been fully established inmental health-care practice. Therefore, this paper willevaluate this connection through the lens of the arousaland regulatory experience of people who engaged in thisintervention. The qualitative findings of a trial of sensorymodulation in four inpatient mental health units in NewZealand will be presented. These findings will be dis-cussed in light of recent advances in the neurophysiologyof emotional regulation (Porges 2001) and the GeneralAggression Model (GAM) (Anderson & Bushman 2002).The purpose of this paper is to examine the potential ofusing sensory-based approaches to develop the theoryand practice of preventing, minimizing, and managingaggression in mental health settings.
The General Aggression ModelThe GAM is a framework through which the study find-ings and the application of sensory modulation practicescan be conceptualized. Aggression has been seen tradi-tionally as either an impulsive and hostile act usuallydriven by anger, or a premeditated goal-oriented behav-iour. This dichotomy limits clinical responses to inpatientaggression by locating the source of aggression in theindividual (Duxbury 2002). However, this view has beenexplicitly rejected in recent research and guidance onmanaging clinical aggression (Oud 2006; Paterson et al.2010; Richter 2006). The GAM integrates multiple theo-ries to present a framework for understanding aggression.This framework is specific to aggression that has an imme-diate intent to cause harm (i.e. not accidental) and thatincludes both non-violent and violent behaviour.
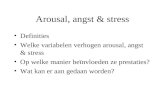
According to the model, aggression arises out of acomplex interaction of inputs (personal attributes andsituation), mediating pathways (learned cognitive scripts,affective repertoire, autonomic arousal), and outcomes(decisions and actions). Emotional regulation can beinfluenced by the ongoing interaction between a personand their environment. To illustrate this dynamic,Figure 1, adapted and modified from Anderson andBushman (2002) and Roberton et al. (2012), depicts asequence in a hypothetical emerging behavioural crisiswhen a request to lower the room temperature is denied.An individual with a dominant or hostile interpersonalstyle may become aggressive (Cookson et al. 2012) anddepending on the strength of existing scripts (e.g. retali-atory or hostile), the affective route may activate rapidly,spurred by a heightened state of autonomic arousal that
SENSORY MODULATION OF AROUSAL 501
© 2013 The AuthorsInternational Journal of Mental Health Nursing © 2013 Australian College of Mental Health Nurses Inc.

could be expected from someone with a sensory aversionto hot temperatures (Anderson et al. 2000; Berkowitz1993). The interaction of both individual and environ-mental variables can generate a process that supportsimpulsive, aggressive behaviour, triggered by cognitivescripts in memory.
The GAM asserts the primacy of cognitive triggersfor aggression, to the neglect of neurological and otherbiological factors as well as environmental stresses thatcould cause distress and lead to aggression. A recent cri-tique of the model cites the ‘squishiness’ of data thatsupport the assumptions that aggression is either learnedor cognitive, and also the inadequacy of the linearity andmechanistic properties of the model (Ferguson & Dyck2012). For our purposes, however, the GAM remains auseful schema for conceptualizing how a ‘bottom-up’sensory approach may work with cognitive approaches toprevent aggressive behaviour in mental health settings.While learned scripts in memory may play a larger roleat the outcomes stage of the process where decisionsare made, the model highlights the problem of usinga purely cognitive or verbal approach to de-escalatingaroused, agitated, or aggressive situations where person-ality and situation combine with cognitive scripts inmemory. Without an intervention that optimizes arousalor moderates affect, cognitive scripts may not even beaccessible to negotiation or change. This feature of themodel will be discussed along with recent advances inthe neurophysiology of emotional regulation as a way tounderstand the findings of the pilot study using sensoryinterventions to minimize the risk of aggression.
PILOT STUDY
In 2009, a pilot sensory modulation intervention wasintroduced into four mental health inpatient units inNew Zealand (three adult units, one youth unit), in theform of a designated space (a ‘sensory room’) equippedwith a range of items for various sensory inputs. Stafffrom multiple disciplines had initial training in thetheory and principles of sensory modulation and anintroduction to the sensory tools, as well as scheduledbrief ‘refreshers’ to discuss issues that arose in usingthe approach. Service users were oriented to the roomas part of the admission process where the purposeof the room was explained. Subsequently, when expe-riencing an increase in levels of distress, a serviceuser could access the sensory room accompanied by amember of clinical staff. Apart from responding to anoccasional request by a service user to use the sensoryroom, staff would offer the intervention as early inan escalation process as possible. When prompted byearly signs of agitation, staff would reflect the beha-viour back to the person and invite them to use theresource. Once in the sensory room, staff helped theperson select from a range of equipment to facilitatebeing comfortable in that environment. This rangeof objects included a massage chair, rocking chair,beanbag, faux-fur blankets, weighted blankets, weightedsoft toys, ‘stress’ balls, portable audio and DVD playerswith relaxing sounds and visual scenes, aromatic oils anddiffusers, scented hand creams, and adjustable colouredambient lighting.
FIG. 1: General Aggression Model with behavioural example.
D. SUTTON ET AL.502
© 2013 The AuthorsInternational Journal of Mental Health Nursing © 2013 Australian College of Mental Health Nurses Inc.

Method and sampleAn inductive, qualitative study using focus groups andinterviews was conducted in two phases to evaluate theacceptability, implementation, and impact of the inter-vention. Clinical staff and discharged service users whohad used the sensory room were invited to participate ininterviews and focus groups to discuss their experienceof the intervention. Unit managers and senior staff onthe units acted as intermediaries to recruit staff fromthe units. Community key workers or consumer advisorsapproached former service users to participate in thestudy. A semistructured interview schedule was devel-oped for the staff and service user interviews. Serviceusers were interviewed either in their home or in a privateroom in a clinical agency according to their preference.Informed consent was obtained from all participants. Theresearch was approved by the New Zealand Multi-regionEthics Committee, New Zealand Ministry of Health.
The first phase of the research occurred in late 2009and focused on initial experiences of the implementationof the sensory modulation rooms. The second phaseoccurred in 2011 and focused on how the interventionhad evolved in the four units. In both phases, participantsdescribed their experiences using the intervention. Allinterviews and focus groups were conducted by a memberof the research team who was not employed by themental health service. All interviews and focus groupswere audio-recorded and transcribed. A description ofthe sample is shown in Table 1.
AnalysisAn inductive approach was used to generate themesfrom the transcribed focus group and interview data(Graneheim & Lundman 2003; Thomas 2006). Analysiswas guided by the study objectives and involved detailed,repeated readings of the raw data in order to developkey themes from manifest content and underlying mean-ings (Graneheim & Lundman 2003). The organiza-tion, coding, and analysis of data was conducted usingnVIVO software (QSR International, Melbourne, Victo-ria, Australia). The first round of raw data was categorizedaccording to broad themes which emerged from parti-cipant responses. Further thematic analysis took place to
develop subthemes within each of the above categories. Acoding structure was developed and applied to the secondround of interviews and further themes were identified.Three members of the research team cross-checked thethemes and data to ensure consistency of the final themesand subthemes. These themes capture the perceptionsof service users and staff in relation to their experienceof using the sensory modulation rooms, and in particularthe impact of the intervention on managing distress andagitation.
FINDINGS
Three main themes emerged from the analysis: (i) facili-tating a calm state; (ii) enhancing interpersonal connec-tion; and (iii) supporting self-management. Each aspectwas an important element of sensory modulation whichcontributed to the management of distress and agitation.
(i) Facilitating a calm stateThere was agreement amongst the participants that thesensory intervention reduced arousal and induced a calmstate in the majority of the people who used it. Withinthis broad theme, several subthemes highlighted themechanisms which enabled the de-escalation of distressor agitation. The first of these relates to the ‘soothingand grounding effect’ that the sensory intervention had.For many participants, the sensory room provided aspace to withdraw to, where the room and sensory equip-ment were experienced as relaxing. As one staff memberreported, ‘I think the environment just allows peopleto soothe . . .’ (staff member (SM)9, site 4). The soothingeffect appeared to relate to the easing and comforting ofboth mind and body as reflected in service user reports:
It’s positive, calming, soothing, slowing down of racingthoughts . . . (service user (SU)12, site 4)
I remember being really, really emotional and going inthere and sort of calming down. Just looking at the col-ourful walls in there with the lights off and that, it madeyour mind feel at ease. (SU5, site 4)
The accounts indicated that soothing involves a move-ment from mental and physical harshness and speed, toa softness and slower, rhythmic pace, characteristic of thebody’s physiological state when relaxed. This alignment ofexternal input with internal processes such as brain waves,heart rate, and breathing is known as entrainment (Rider,1985), and appeared to be a key mechanism in the sensoryintervention.
In addition to aligning internal processes with exter-nal stimuli, some modalities had a stabilizing effect by
TABLE 1: Number and characteristics of interviewed sample
Interviewsample Total
Female(%)
Male(%)
Nursing(%)
Allied healthor other (%)
Clinical staff 40 90 10 72.5 27.5Service users 20 90 10
SENSORY MODULATION OF AROUSAL 503
© 2013 The AuthorsInternational Journal of Mental Health Nursing © 2013 Australian College of Mental Health Nurses Inc.

drawing attention to the service users’ somatic or bodilysenses. Many participants used terms such as ‘grounded’,‘anchored’, ‘centred’, and ‘collected’ when describingthis type of experience. The grounding effect of somaticsensation was one of the strongest subthemes in theparticipant accounts.
I really liked that feeling of being in the [massage] chair,so I got into there and it had that focus of actually centringme . . . I actually found, that sort of made me feel a lotcalmer, but . . . you know, alive and not unconnected . . .shutting off senses that were too activated and nothelpful. (SU11, site 4)
I stopped being racy for even just five minutes. I wasactually still, you know, and centred and focused.Whereas usually, I’m not like that at all, and when I getunwell, it just magnifies twenty million times, so I’mnever resting, you know, and I don’t sleep. So, to even becentred for five minutes is a really big deal. (SU14, site 4)
Sustained feedback through internal and muscu-loskeletal sensation helped service users to groundthemselves in their body and to be attuned to thepresent. Participants who had experienced psychosis,elevated mood, dissociation, and overwhelming anxietyall reported that this aspect of the intervention was asignificant factor in assisting their de-escalation, help-ing them to feel secure and oriented in space andtime:
It was good for dealing with situations where I was start-ing to feel somewhat distant . . . it was really good athelping ground me. It would get me back to the present. . . (SU2, site 4)
Being brought back to the present supported partici-pants to engage with the immediate context more con-structively ‘. . . it’s sort of like focusing on the here andnow, and what’s most helpful’ (SU14, site 4).
The ‘shifting of attention and affect’ was anotherkey subtheme in the findings. By drawing attention tothe bodily sensation or the immediate environment, thesensory intervention provided distraction from anxiousthoughts, urges to self-harm, delusional ideas, and over-whelming auditory hallucinations. For example, partici-pants stated:
I get voices in my head, so when I was in the room I couldkind of, not switch them off, but concentrate on some-thing else, and [it] kind of relieves the tension. (SU1,site 3)
. . . then you were in a room and you’ve got things dis-tracting you . . . usually for me, eventually [the agitation]passes, it can just take time . . . (SU3, site 4)
You know, with paranoia with the music that’s really quitegood, as it takes them right away. (SM2, site 2)
Distraction through strong sensory input was a signifi-cant factor in reducing agitation, if it allowed enough timefor individuals’ physiological and emotional arousal tosubside. A further aspect of shifting attention and affectwas the experience of being transported away from thepresent to another time or place:
I wanted the sound of the beach, of the waves, so I hadthat. And the smell of the hand cream reminded me ofsort of sun block . . . and so I was taken back in time togood childhood memories, felt like I was at the beach,tension was relieved and [I was] at peace. (SU11, site 4)
This positive association involved a direct emotionalresponse to specific sensory input; shifting focus away fromstressful situations or thoughts towards affective statesconnected with memories of other times and places.
Participants also commented on the importance ofexperiencing a ‘sense of safety and control’ for inducing acalm state. Having a dedicated safe space was identified asan important aspect of the intervention and the sensoryroom was perceived as being less clinical and not soprone to interruption as other spaces on the ward, includ-ing individuals’ bedrooms. For many participants, using aweighted blanket, or sitting in a beanbag, added to thesense of safe containment:
For me, the most helpful was that opportunity the sensoryroom gave me to have a quiet, relaxing space on the ward. . . it’s a safe space . . . The weighted blanket just gave mea sense of protection and safety. (SU13, site 4)
The service user accounts suggested that having theopportunity to remove oneself from potential threats andintrusions and to provide one’s body with a strong indica-tion that it is secure was important for inducing calm.Staff also saw the development of a safe space as key tothe implementation of the sensory intervention. One staffmember emphasized the importance of preserving bothtime and the space for the sensory experience:
Well I just think having that time . . . and having that sortof space really respected and recognized as a space thatyou don’t invade . . . (SM5, site 1)
Another significant subtheme was the increased senseof control created through the use of the sensory tools.Service users found that through the soothing and stabi-lizing effect of the sensory intervention they were able tothink more clearly, regulate their emotions, influencetheir immediate environment, as well as control destruc-tive behaviours:
D. SUTTON ET AL.504
© 2013 The AuthorsInternational Journal of Mental Health Nursing © 2013 Australian College of Mental Health Nurses Inc.

. . . to be mentally in a better space, you know? And thecontrol that comes with that . . . I had control over what Iwanted to feel. I knew that was going to make me feelgood and relaxed. (SU14, site 4)
I found it really good sort of to be in control of theenvironment. Like, the sound . . . the lighting, it was justbeing in control of things around you, kind of helps tocalm you down. (SU11, site 4)
It should absolutely be something that’s available,because I think that it helped me get the behavioursunder control as much as anything and had I not . . . itcould have been a lot worse. (SU2, site 4)
The participants’ accounts suggested that institutionalrestrictions and distressing symptoms resulted in a loss ofcontrol over their bodies, minds, and environment, andthe sensory intervention supported service users to regainagency over these factors.
The last subtheme related to the facilitation of acalm state was the experience of ‘expression and release’through the sensory interventions. The opportunity torelease tension and express emotion within the safe con-fines of the room was cathartic for some participants:
It kind of calms you down enough to allow your feelings tocome out instead of holding them all in . . . (SU6, site 4)
It was just somewhere where you could go and exertenergy and not be judged for it . . . to go and sit in a roomand jiggle and squeeze a ball and throw a ball in the air islike, that was okay, but pacing the corridors at 4 amwasn’t. (SU1, site 4)
Staff found that the relaxed and safe space led toservice users ‘opening up’ and expressing issues or releas-ing pent up energy. The grounding effect of being ina rocking or massage chair, or squeezing a stress ball,appeared to allow the safe discharge of energy which wasnot always possible in other parts of the ward due toperceived lack of privacy and safety.
Participants suggested that the impact was not longterm, but long enough to enable engagement in some-thing more restful, constructive, or therapeutic. Serviceusers reported being able to get some sleep or engage inmeaningful activity after using the sensory room, whilestaff found that following the use of sensory tools theycould facilitate the use of other verbal and cognitivelybased strategies:
[It] calmed her down so that she could focus; you know: wecould talk about what happened logically. (SM1, site 3)
This finding was particularly significant as it suggestedthat the intervention acted as a precursor to subsequent
cognitive and interpersonal engagement. This effectis reflected in the second major theme related tothe enhancement of relationship through the sensoryinterventions.
(ii) Enhancing interpersonal engagementAs well as having a calming effect, sensory modulation wasperceived as a tool for developing meaningful connectionbetween staff and service users. Social relationships area significant factor in managing aggression and the find-ings suggested that the sensory room and equipmentenhanced interpersonal interaction by facilitating therapid building of rapport and trust. Having someonepresent in a soothing or stabilizing manner was often asimportant to service users as the room and equipment.Service users valued the uninterrupted one to one timeand appreciated the sense of interpersonal engagementthat resulted from time in the sensory room.
I found it good for a connection with staff, ‘cause whenthey’re busy on the wards, they don’t have time to talk toyou, and at least in the sensory room . . . you actually gotthat one-on-one time for 15 minutes or so with that nurse.(SU13, site 4)
In addition to having a staff member present andattuned to their experience, service users also suggestedthat having someone to talk to was important in creatingconnection:
For me, it’s been a place, at times, where I’ve been able totalk openly and freely to nurses about what’s going on inmy head. (SU1, site 4)
A number of staff participants also described how theapplication of sensory modulation created an opportunityfor developing trust and relationship. Trialling and access-ing the sensory approach and tools with service users wasperceived as a means to rapidly build rapport and sharemeaningful experiences, even in the absence of verbalcommunication:
That rapport building as well . . . you’re not communicat-ing verbally with them, but you’ve still built up a rapport. . . they trust you . . . . talking and building up communi-cation and building up that rapport, it’s kind of just comeinstantly with that person. (SM10, site 4)
Comments such as this indicated that sensory modu-lation not only induced a relaxed atmosphere, but alsoallowed staff members to get alongside to work in closeproximity with service users. The approach encouragedstaff to ‘tune into’ and talk with service users about theirsensory and emotional experiences, while engaging insimple and practical strategies for managing their own
SENSORY MODULATION OF AROUSAL 505
© 2013 The AuthorsInternational Journal of Mental Health Nursing © 2013 Australian College of Mental Health Nurses Inc.

arousal. This aspect of self-management was the finalmajor theme in the participant accounts.
(iii) Supporting self-managementWhile the initial focus of the study was on implementingsensory modulation as an inpatient de-escalation tool,both staff and service users recognized the potential forusing the approach to increase self-awareness and self-management. By supporting service users to recognizetheir own sensory sensitivities and triggers and to developtheir own strategies, sensory modulation broadened thefocus of de-escalation practices and encouraged sharedresponsibility.
Staff members suggested that the practical nature ofthe approach enabled service users to be proactive incalming themselves:
It did take longer than giving people medication but itgave people a real strategy of how to help themselves nexttime. So instead of just sticking a plaster on it, on theproblem, which is kind of what PRN does . . . you’reactually giving somebody a really concrete way of dealingwith their problems. (SM6, site 3)
Staff participants also commented on the need to takesensory modulation beyond the sensory room and into thewider service and home environment. One commented:‘. . . there’s the tools in that room that they can figure outwhat helps, and then hopefully, they can think about howto take that home in some form’ (SM9, site 4). Serviceusers were able to describe how they integrated sensorymodulation strategies into their everyday lives: ‘I utilizethe stress ball I’ve got at home and the deep breathing allthe time which I have learnt from there, so yeah, find thatreally helpful to get through tough situations I’m facedwith’ (SU16, site 4). Accounts such as these suggested thatin addition to being an effective approach for calmingand increasing interpersonal connection, the sensorymodulation approach also enhanced service user self-awareness and capacity for self-management. By support-ing individuals to develop their own practical sensorystrategies, sensory modulation had the potential tobroaden the focus of de-escalation practices and bettersupport recovery.
DISCUSSION
This paper maps the subjective responses to deliberatesensory inputs against a cognitive model of aggression(GAM), and examines this with recent theoreticaladvances in the neurophysiology of emotional regulation(polyvagal theory). The study findings align with other
recent research which found that sensory interventionshad a calming effect in people experiencing acute distress(Chalmers et al. 2012; Novak et al. 2012). The partici-pants’ accounts provide important insights into how asensory approach can promote the reduction of agitatedstates of arousal. It is important to note here that theintervention focussed on factors known to promoteaggression, and that the behaviours that warranted theintervention were not necessarily aggressive. Throughreducing aversive stimuli and shifting the affective stateof an agitated person the intervention sought to direct acognitive script that led to a thoughtful outcome ratherthan an impulsive one. The study findings will be dis-cussed with a focus on the mechanism and utility ofreducing aversive stimuli, communicating safety, andshifting the affective state of a distressed person.
Reducing aversive stimuli andcommunicating safetyGeneral discomfort and aversive conditions, such as hottemperatures, loud noise, or unpleasant odours, increasesthe risk of aggressive behaviour by escalating negativeaffect and physiological arousal (Anderson et al. 2000;Berkowitz 1993). In the mental health inpatient unitsstudied by Johnson and Delaney (2007), a post hoc reviewof violent events that happened suddenly without appar-ent warning discovered that the signals were indeed therebut were lost in the background ‘noise’ of the environ-ment. Within the GAM framework, situational factors,including sensory aspects of the social and physical envi-ronment, may be targeted to prevent the development ofagitation and distress. People with psychiatric illnesseshave been found to be hyper- or hyposensitive to sensoryinput (Abernethy 2010; Brown et al. 2002) and mayhave associated problems moderating autonomic arousal(Porges 2004). Sensory aversion is relevant to aggressivebehaviour as ‘unusually high and low levels of arousal maybe aversive states and may therefore stimulate aggressionin the same way as other aversive or painful stimuli’(Anderson & Bushman 2002; p. 39). However, experi-mental evidence suggests that even in the presence ofsustained physiological arousal, a salient cue of safety ‘canbe associated with a relatively unusual or novel response,namely enhanced inhibition of aggression in the face ofa provocateur’ (Ward et al. 2008; p. 590). Thus, the crea-tion of physical and social environments that not onlyreduce aversive stimuli, but also communicate safety andcomfort, may aid in the prevention of aggression.
Communicating a safe environment requires an under-standing of the distinction between two types of sensoryinput. External sensory input comes from the organs that
D. SUTTON ET AL.506
© 2013 The AuthorsInternational Journal of Mental Health Nursing © 2013 Australian College of Mental Health Nurses Inc.

communicate with the external world (visual, gustatory,olfactory, auditory, and tactile), and provide informationabout the safety of our environment. Somatic senses com-municate a sense of internal safety, including awarenessof firm pressure on the skin (deep touch) and the sense ofwhere one’s limbs are in space (proprioception), and ofbalance and awareness of spatial orientation (vestibular).These somatic senses are referred to as the ‘powerhousesof calming’, as they provide a grounding orientation to theperson (Moore & Henry 2002). Together, these internaland external environmental cues signal safety throughactivating a specialized aspect of parasympathetic neuralcircuitry, promoting a ‘bottom-up’ pathway toward opti-mized arousal.
In the polyvagal theory of emotional regulation, Porges(2001) describes a specialized branch of the vagal nerve,unique to mammals, that works in a hierarchical relation-ship with sympathetic fibres and the dorsal vagus. Thisspecialized branch, the ‘ventral’ vagus – so-called becauseit controls muscles of face, head, neck, and heart – medi-ates parasympathetic influence to support adaptive socialresponses. The phylogenetic creation of this complex alsodeveloped the opposing mechanisms of excitation andinhibition to allow for rapid, but graded, shifts in meta-bolic output in response to sensory and motor stimulation(Porges 1995a; 1995b). This means that arousal is neitheran on/off node, nor does it activate along a linear trajec-tory, because not every threat stimulates arousal (Wardet al. 2008). Deliberate use of sensory inputs can promotea recursive regulation of arousal by accessing evolution-arily advanced neural pathways that promote adaptive,social behaviours.
Shifting attention and affective stateSensory input can help minimize risk of aroused behav-iour, but can also moderate arousal and affective pathwayswhere a person is already feeling unsafe, stressed, andagitated. In these situations utilizing ‘top-down’ regula-tion through higher cortical functions such as problemsolving, validation, or verbal negotiation can be limited asa de-escalation tool. The allostatic load created by pro-longed stress, along with the acute perceptual and cogni-tive changes associated with psychiatric symptoms, maycompromise a person’s ability to think and process verbalinformation clearly (McEwen 2007). A further contri-butor to this limitation is the physiological impact ofthe arousal itself. In states of stress, alarm, or rage, themuscles in the middle ear constrict, decreasing the flex-ibility of the ossicles, with the result that the human voiceis not discriminated from background sounds (Koike &Wada 2005). The mammalian reflex that makes humans
scan the environment for threats when feeling unsafe,rather than listen to each other, may contribute to theunreliability of verbal de-escalation techniques (Donovanet al. 2003; Johnson & Delaney 2007; Perkins et al. 2012).In the acuity of a moment, an appeal to the cognitivescript or the decisional process alone may go unheard orbe misconstrued. Thus, sensory calming may be an impor-tant precursor to other therapeutic approaches. Figure 2revisits the GAM to display the impact of expanding themodel to include sensory-based inputs and their neuro-logical or biological impacts on arousal and affect.
The accounts in the present pilot study indicatethat deliberate sensory inputs can shift attention awayfrom negative cognitive scripts or distressing symptomstowards the participants’ bodies or immediate environ-ment. Distraction or re-focussing of attention reducesarousal more effectively than venting of pent-up feelings(Bushman 2001), possibly through dampening the activityof the amygdala (de Gelder et al. 2012). The most helpfulforms of distraction reported by participants were activi-ties that induced a calm physical state. Examples includ-ing listening to soothing music, watching coloured lights,blowing bubbles, and doing plastic maze puzzles werefound to be soothing and useful in reducing agitation.Staff also provided significant sensory input, with thepotential to support the shifting of attention and affectivestate through their tone of voice, movements, and bodylanguage.
Stabilizing was a key mechanism for many service userparticipants. The massage chair and weighted modalities(e.g. heavy blanket) were frequently reported as beinguseful, supporting the notion that sustained stimulationof deep pressure receptors appears to be one of the mosteffective ways of inducing calm, through ‘grounding’the person in their body (Novak et al. 2012). Staff canenhance the grounding features of the weighted blankets,massage chair, and other items by encouraging serviceusers to shift their attention to the here and now and tofocus on the physical sensation.
Inducing positive experiences and the associated shiftin affective state can open up thinking and behaviouralrepertoires, which over time builds sustainable resourcesfor coping with difficult situations (Garland et al. 2010).Positive association was less frequently mentioned as acalming mechanism, but for some participants it provideda welcome escape from the present. Natural or home-likesettings were mentioned as having calming associationsin participants’ accounts. Using and finding appropriatemusic, sounds, images, smells, and tactile objects in con-junction with guided imagery can all facilitate calmingthrough positive association. It is also possible that new
SENSORY MODULATION OF AROUSAL 507
© 2013 The AuthorsInternational Journal of Mental Health Nursing © 2013 Australian College of Mental Health Nurses Inc.

associations were created during positive experiences inthe sensory room. Green and Ben-Sasson (2010) suggestthat responses to particular sensory input may be condi-tioned through repeated exposure, leading to the expec-tation of being calmed and a shift in affective state. Overtime, this may lead to the alteration an individual’s cog-nitive script from being unable to control their arousal, tobeing able to take some responsibility in managing theirdistress. The use of sensory strategies to create positiveaffect may ‘exert a countervailing force on the dysphoric,fearful, or anhedonic states characteristic of psycho-pathologies typified by emotional dysfunctions’ (Garlandet al. 2010; p. 849).
Overall, there were enough general reports of successand specific exemplars in the qualitative findings to indi-cate that sensory modulation intervention supportedde-escalation of arousal or regulation of emotion in themajority of people who used it. Staff recounted situationswhere they would have needed to use some form ofmedical or coercive practice if the sensory interventionhad not facilitated de-escalation. However, the partici-pant accounts also suggested that the effectiveness ofsensory modulation is influenced by many variables,including staff engagement with service users, earlyrecognition of agitation or disengagement by staff andservice users, an understanding of service user sensorypreferences, and the service users’ experience with
self-regulation in extreme states. Applying the GAMframework within acute mental health services wouldinvolve tailoring interventions to fit the individual constel-lation of contributing factors. ‘Any intervention that hasthe potential for increasing an organism’s experience ofsafety has the potential of recruiting the evolutionarilymore advanced neural circuits that support pro-socialbehaviours’ (Porges 2008; p. 13). A broadened viewof the factors involved in arousal opens the door tore-conceptualizing clinical training that promotes optimalarousal and a sense of safety through sensory experienceas the frontline in aggression management.
LIMITATIONS AND FUTURE RESEARCH
The data presented are from a pilot study of an interven-tion in inpatient mental health settings. The units self-selected for participation in the trial of the new practice,and participants in the interviews were volunteers whohad engaged with the sensory intervention and self-selected to discuss it. No young people participatedin focus groups or interviews after discharge, so theseresponses are from adults only. While the data are sug-gestive of useful additions to clinical training and even tothe planning of ward environments, more research isneeded to validate and understand the impact of sensorymodulation on arousal and emotion in persons with a
FIG. 2: Model of sensory-based aggression prevention pathways.
D. SUTTON ET AL.508
© 2013 The AuthorsInternational Journal of Mental Health Nursing © 2013 Australian College of Mental Health Nurses Inc.

psychiatric illness. Findings from observational studieshave provided association of sensory interventions withreduced instances of seclusion or restraint (Barton et al.2009) and the management of psychiatric symptoms(Knight et al. 2010), but controlled trials are required toestablish the empirical link between the intervention andphysiological or psychological arousal. Inpatient mentalhealth settings, with distressed clients, present uniquechallenges to research design, particularly given the inter-action of person, situation, and modifiable internal media-tors in managing clinical aggression. Further researchwould benefit from coupling the intervention with theroutine application of a validated tool for identifying thelikelihood of potential aggression, such as the DynamicAppraisal of Situational Aggression (Ogloff & Daffern2006). This could provide a better gauge for estimatingepisodes of prevented aggression rather than the usualintuitive use of a continuum of behaviours as a basis forassessing for intervention.
Assessing the impact of sensory interventions onarousal and aggression is problematic. Even though themost common measures of autonomic arousal – heartrate variability (Thayer & Brosschot 2005) and respiratorysinus arrhythmia (Porges 2008) – are non-invasive, thepractical and ethical challenges to conducting this inves-tigation in an inpatient mental health setting are daunting.The challenge remains for direct assessment in real-lifesituations of how sensory interventions recruit the ventralvagus to optimize arousal to support adaptive emotionalregulation to enable the more effective management ofaggression.
CONCLUSION
Sensory modulation (Champagne 2011) has emergedas a suite of sensory-based interventions that provide analternative, afferent, or ‘bottom-up’ response to arousalor aggression. These complementary interventions havebeen largely ignored in theoretical summaries of aggres-sion management, although they have been highlighted inrecent policy initiatives to reduce seclusion and restraint(Huckshorn 2006). Research on these practices in mentalhealth settings, though growing, is only emerging and thetheoretical basis remains underdeveloped.
The analysis of narrative data from pilot sensory inter-ventions presented here suggests that sensory tools have arole in optimizing arousal and regulating emotion. From atheoretical perspective, polyvagal theory provides a reli-able framework to integrate sensory modulation interven-tions with aggression management models. Importantly,both polyvagal theory, extant research, and the pilot study
results support a staged approach to sensory and cognitiveinterventions, as these can be mapped against the GAM.These theoretical extensions underpin contributions topractice. The use of sensory tools, originally developedwithin occupational therapy, into a mental health nursingstrategy, improves the range of effective options withinaggression management practices.
Currently, to determine the acceptability and impactof sensory-based intervention within inpatient mentalhealth services, we must rely on feedback from serviceusers and staff who have experienced it. Continued devel-opment and evaluation of this approach is needed, as itappears to be a promising component in the evolution ofmore effective and humane responses to aggression.
REFERENCESAbernethy, H. (2010). The assessment and treatment of sensory
defensiveness in adult mental health: A literature review.British Journal of Occupational Therapy, 73 (5), 210–218.
Anderson, C. A. & Bushman, B. J. (2002). Human Aggression.Annual Review of Psychology, 53, 27–51.
Anderson, C. A., Anderson, K. B., Dorr, N., DeNeve, K. M. &Flanagan, M. (2000). Temperature and aggression. In: M.Zanna (Ed.). Advances in Experimental Social Psychology,Vol. 32. (pp. 63–133). New York: Academic.
Barton, S. A., Johnson M. R. & Price, L. (2009). Achievingrestraint-free on an inpatient unit. Journal of PsychosocialNursing & Mental Health Services, 47 (1), 34–41.
Beauchaine, T. P. (2001). Vagal tone, development, and Gray’smotivational theory: Toward an integrated model of auto-nomic nervous system functioning in psychopathology.Development and Psychopathology, 13, 183–214.
Berkowitz, L. (1993). Pain and aggression – some findings andimplications. Motivation and Emotion, 17 (3), 277–293.
Berkowitz, L. (2001). Affect, aggression and antisocial behavior.In: R. J. Davidson, R. J. Scherer & H. H. Goldsmith (Eds).Handbook of Affective Sciences, (pp. 804–823). New York:Oxford University Press.
Bowers, L., Van Der Merwe, M., Paterson, B. & Stewart, D.(2012). Manual restraint and shows of force: The city 128study. International Journal of Mental Health Nursing, 21,30–40.
Brown, C., Cromwell, R. L., Filion, D., Dunn, W. & Tollefson,N. (2002). Sensory processing in schizophrenia: Missing andavoiding information. Schizophrenia Research, 55, 187–195.
Bushman, B. J., Baumeister, R. F., Phillips, C. M. (2001). Dopeople aggress to improve their mood? Catharsis beliefs,affect regulatioen opportunity, and aggressive responding.Journal of Personality and Social Psychology, 81 (1), 17–32.
Chalmers, A., Harrison, S., Mollison, K., Molloy, N. & Gray, K.(2012). Establishing sensory-based approaches in mental
SENSORY MODULATION OF AROUSAL 509
© 2013 The AuthorsInternational Journal of Mental Health Nursing © 2013 Australian College of Mental Health Nurses Inc.

health inpatient care: A multidisciplinary approach.Australasian Psychiatry, 20, 35–39.
Champagne, T. (2011). Sensory Modulation and Environment:Essential Elements of Occupation, 3rd edn revised. Sydney,NSW: Pearson Clinical and Talent Assessment.
Champagne, T. & Stromberg, N. (2004). Sensory approachesin inpatient psychiatric settings: Innovative alternatives toseclusion and restraint. Journal of Psychosocial Nursing andMental Health Services, 42 (9), 34–44.
Cookson, A., Daffern, M. & Foley, F. (2012). Relationshipbetween aggression, interpersonal style and therapeutic alli-ance during short-terms psychiatric hospitalization. Interna-tional Journal of Mental Health Nursing, 21, 20–29.
Cummings, J. S., Grandfield, S. A. & Coldwell, C. M. (2010).Caring with comfort rooms. Reducing seclusion and restraintuse in psychiatric facilities. Journal of Psychosocial Nursingand Mental Health Services, 48 (6), 26–30.
van Doeselaar, M., Sleegers, P. & Hutschemaekers, G. (2008).Professionals’ attitudes toward reducing restraint: The caseof seclusion in the Netherlands. Psychiatric Quarterly, 79(2), 97–109.
Donovan, A., Plant, R., Peller, A., Siegel, L. & Martin, A. (2003).Two-year trends in the use of seclusion and restraint amongpsychiatrically hospitalized youths. Psychiatric Services, 54,987–993.
Duxbury, J. (2002). An evaluation of staff and patient viewsof strategies employed to manage inpatient aggressionand violence on one mental health unit: A pluralistic design.Journal of Psychosocial and Mental Health Nursing, 9, 325–337.
Ferguson, C. J. & Dyck, D. (2012). Paradigm change in aggres-sion research: The time has come to retire the GeneralAggression Model. Aggression and Violent Behavior, 17 (3),220–228.
Garland, E. L., Fredrickson, B., Kring, A. M., Johnson, D. P.,Meyer, P. S. & Penn, D. L. (2010). Upward spirals of positiveemotions counter downward spirals of negativity: Insightsfrom the broaden and build theory and affective neuro-science on the treatment of emotion dysfunctions and defi-cits in psychopathology. Clinical Psychology Review, 30 (7),849–886.
de Gelder, B., Hortensius, R. & Tamietto, M. (2012). Attentionand awareness each influence amygdala activity for dynamicbodily expressions: A short review. Frontiers in IntegrativeNeuroscience, 6 (54), 1–9.
Graneheim, U. H. & Lundman, B. (2003). Qualitative contentanalysis in nursing research: Concepts, procedures andmeasures to achieve trustworthiness. Nurse EducationToday, 24 (2), 105–112.
Green, S. A. & Ben-Sasson, A. (2010). Anxiety disorders andsensory over-responsivity in children with autism spectrumdisorders: Is there a causal relationship? Journal of Autismand Developmental Disorders, 40, 1495–1504.
Huckshorn, K. A. (2006). Re-designing state mental healthpolicy to prevent the use of seclusion and restraint. Admin-
istration and Policy in Mental Health and Mental HealthServices Research, 33 (4), 482–491.
Johnson, M. E. & Delaney, K. R. (2007). Keeping the unit safe:The anatomy of escalation. Journal of the American Associa-tion of Psychiatric Nurses, 13, 43–53.
Knight, M., Adkison, L. & Kovach, J. S. (2010). A Comparisonof multisensory and traditional interventions on inpatientpsychiatry and geriatric neuropsychiatry units. Journal ofPsychosocial Nursing and Mental Health Services, 48 (1),24–31.
Koike, Y. & Wada, H. (2005). Analysis of human middle-earvibration using the finite-element method. Journal of theJapan Society for Simulation Technology, 24 (1), 3–8.
Lee, S. J., Cox, A., Whitecross, F., Williams, P. & Hollander,Y. (2010). Sensory assessment and therapy to help reduceseclusion use with service users needing psychiatric inten-sive care. Journal of Psychiatric Intensive Care, 6 (2), 83–90.
McEwen, B. S. (2007). Physiology and neurobiology of stressand adaptation: Central role of the brain. PhysiologicalReviews, 87 (3), 873–904.
Miller, L. J., Coll, J. R. & Schoen, S. A. (2007). A randomizedcontrolled pilot study of the effectiveness of occupationaltherapy for children with sensory modulation disorder.American Journal of Occupational Therapy, 61, 228–238.
Moore, K. M. & Henry, A. D. (2002). Treatment of adult psy-chiatric patients using the Wilbarger protocol. OccupationalTherapy in Mental Health, 18 (1), 43–63.
Novak, T., Scanlan, J., McCaul, D., MacDonald, N. & Clarke, T.(2012). Pilot study of a sensory room in an acute inpatientpsychiatric unit. Australasian Psychiatry, 20 (5), 401–406.
Ogden, P., Minton, K. & Pain, C. (2006). Trauma and the Body:A Sensorimotor Approach to Psychotherapy. New York:W W Norton & Co.
Ogloff, J. R. P. & Daffern, M. (2006). The dynamic appraisal ofsituational aggression: An instrument to assess risk for immi-nent aggression in psychiatric inpatients. Behavioral Sciencesand the Law, 24 (6), 799–813.
Oud, N. (2006). Aggression management training programs.In: D. Richter & R. Whittington (Eds). Violence in MentalHealth Settings: Causes, Consequences, Management, (pp.193–211). New York: Springer Science.
Panksepp, J. (1982). Toward a general psychobiological theoryof emotions. Behavioral and Brain Sciences, 5 (3), 407–467.
Paterson, B. (2009). Control and restraint: Changing thinking,practice and policy. Mental Health, 13 (2), 16–20.
Paterson, B., Leadbeater, D. & McComish, A. (1997).De-escalation in the management of aggression and violence.Nursing Times, 93 (36), 58–61.
Paterson, B., Bowie, V., Miller, G. & Leadbetter, D. (2010).Reframing the problem of violence towards mental healthnurses: A work in progress. International Journal of SocialPsychiatry, 56 (3), 310–320.
D. SUTTON ET AL.510
© 2013 The AuthorsInternational Journal of Mental Health Nursing © 2013 Australian College of Mental Health Nurses Inc.

Perkins, E., Prosser, H., Riley, D. & Whittington, R. (2012).Physical restraint in a therapeutic setting; a necessaryevil? International Journal of Law and Psychiatry, 35 (1),43–49.
Porges, S. W. (1995a). Orienting in a defensive world: Mamma-lian modifications of our evolutionary heritage – A polyvagaltheory. Psychophysiology, 32, 301–318.
Porges, S. W. (1995b). Cardiac vagal tone: A physiologicalindex of stress. Neuroscience and Behavioral Reviews, 2,225–233.
Porges, S. W. (2001). The polyvagal theory: Phylogenetic sub-strates of a social nervous system. International Journal ofPsychophysiology, 42, 123–146.
Porges, S. W. (2004). Neuroception: A subconscious systemfor detecting threats and safety. Zero to Three, May, 19–24.
Porges, S. W. (2008). The polyvagal theory: New insights intoadaptive reactions of the autonomic nervous system. Cleve-land Journal of Medicine, 75 (Suppl X), S1–S5.
Richter, D. (2006). Nonphysical conflict management and dees-calation. In: D. Richter & R. Whittington (Eds). Violencein Mental Health Settings: Causes, Consequences, Manage-ment, (pp. 125–142). New York: Springer Science.
Rider, M. S. (1985). Entrainment mechanisms are involvedin pain reduction, muscle relaxation, and music-mediatedimagery. Journal of Music Therapy, 22 (4), 183–192.
Roberton, T., Daffern, M. & Bucks, R. S. (2012). Emotionalregulation and aggression. Aggression and Violent Behavior,17, 72–82.
Sailas, E. E. S. & Fenton, M. (2000). Seclusion and restraint forpeople with serious mental illnesses. Cochrane Database ofSystematic Reviews, (2), CD001163.
Schachter, S. & Singer, J. (1962). Cognitive, social, and phy-siological determinants of emotional state. PsychologicalReview, 69, 379–399.
Selye, H. (1936). A syndrome produced by diverse nocuousagents. Nature, 138, 32.
Thayer, J. F. & Brosschot, J. F. (2005). Psychosomatics andpsychopathology: Looking up and down from the brain.Psychoneuroendocrinology, 30, 1050–1058.
Thomas, D. R. (2006). A general inductive approach foranalysing qualitative evaluation data. American Journal ofEvaluation, 27 (2), 237–246.
Ward, A., Mann, T., Westling, E. H., Creswell, J. D., Ebert, J. P.& Wallaert, M. (2008). Stepping up the pressure: Arousal canbe associated with a reduction in male aggression. AggressiveBehavior, 34, 584–592.
SENSORY MODULATION OF AROUSAL 511
© 2013 The AuthorsInternational Journal of Mental Health Nursing © 2013 Australian College of Mental Health Nurses Inc.