OLD AGE AND WELLBEING IDA ANTWI FALLS CO-ORDINATOR/CLINICAL SPECIALIST LEAD NHS HERTFORDSHIRE JUNE...
14
OLD AGE AND WELLBEING IDA ANTWI FALLS CO-ORDINATOR/CLINICAL SPECIALIST LEAD NHS HERTFORDSHIRE JUNE 18 th 2012
-
Upload
randall-allen -
Category
Documents
-
view
221 -
download
0
Transcript of OLD AGE AND WELLBEING IDA ANTWI FALLS CO-ORDINATOR/CLINICAL SPECIALIST LEAD NHS HERTFORDSHIRE JUNE...
OLD AGE AND WELLBEING
IDA ANTWIFALLS CO-ORDINATOR/CLINICAL SPECIALIST LEADNHS HERTFORDSHIREJUNE 18th 2012
Definition of Health • “ a state of complete physical, mental and social
well-being and not merely the absence of disease or infirmity”.
• This has been seen as an unrealistic goal as few people reach this ideal state of health at any point during a lifetime.
• Definition redefined by WHO as functional health, which is where all people should be able to enjoy a health status that allows them to participate in normal, socially and economically productive and satisfying life.
What is ill-health?
• Conditions of the body or mind that cause pain, dysfunction, or distress to the person afflicted or those in contact with the person can be deemed an illness.
• Ill health means different things to different people. How people view ill health depends on a variety of factors; if they've been seriously ill before, how knowledgeable they are about illness and also what they would class as a "severe" or "mild" illness.
Concepts of ill health• Three main concepts
– ill health as disease symptoms– focuses on concepts associated with ill health e.g. vomiting, diarrhoea, pain, visible symptoms such as rashes, lumps on skin
– ill health as a subjective sensation of illness - a general feeling of being ill or unwell, also known as "Malaise". Malaise is a general feeling of uneasiness or discomfort, and is often an initial stage of an illness or disease. It is a general term for all sorts of non-visual symptoms (symptoms that are not physically apparent), such as fatigue, depression, and the general feeling of being run-down and exhausted
– ill health as a disorder or malfunction within the body. This usually relates to more serious and life threatening diseases illnesses, such as heart disease, intestinal blockage or a brain tumour.
General disease conditions of the elderly
• Heart conditions (hypertension, vascular disease, congestive heart failure, high blood pressure and coronary artery disease)
• Dementia, including Alzheimer's disease
• Depression • Incontinence (urine and
stool)
• Arthritis• Osteoporosis • Diabetes • Breathing problems,
respiratory disease • Frequent falls, which can
lead to fractures and trauma
• Parkinson's disease • Cancer
• Visual impairment, Eye problems (cataracts, glaucoma, Macular Degeneration)
• Gastrointestinal disorders
• Hearing impairment
• Memory loss• Nutrition deficit• Osteoporosis• Pressure ulcers• Sleep problems• Thyroid disease• Visual impairment
Most common elderly disease conditions
• Coronary heart disease
• Stroke
• Cancer
• Pneumonia
• Flu
• Falls (some resulting in head injury, fragility fractures, trauma)
Changes that the carer must be aware of in the care and management of the
elderly
• Slowed reaction time • Thinner skin, which can lead to breakdowns and
wounds that don't heal quickly • A weakened immune system, which can make
fighting off viruses, bacteria and diseases difficult
• Diminished sense of taste or smell, especially for smokers, which can lead to diminished appetite and dehydration

Aims of care for residents in Care Organisations
• Main objectives– to maintain the highest degree of quality of life and wellbeing
without subjecting residents to unnecessary and inappropriate medical and therapeutic interventions
– to provide sufficient support and opportunity to enable residents to manage their own disease condition (e.g. diabetes) where this a feasible and worthwhile option
Barriers to effective health management care
• Lack of sufficient training to acquire simple competencies
• Lack of structured provision of educational opportunities for nursing staff combined with lack of continuing professional education. A part consequence is a high turnover of the workforce
• High ratios of unqualified staff who may have little experience of elderly care and who may have negative attitudes to care of older people who are institutionalised
• Lack of available resources in terms of staff time, catering services, and equipment
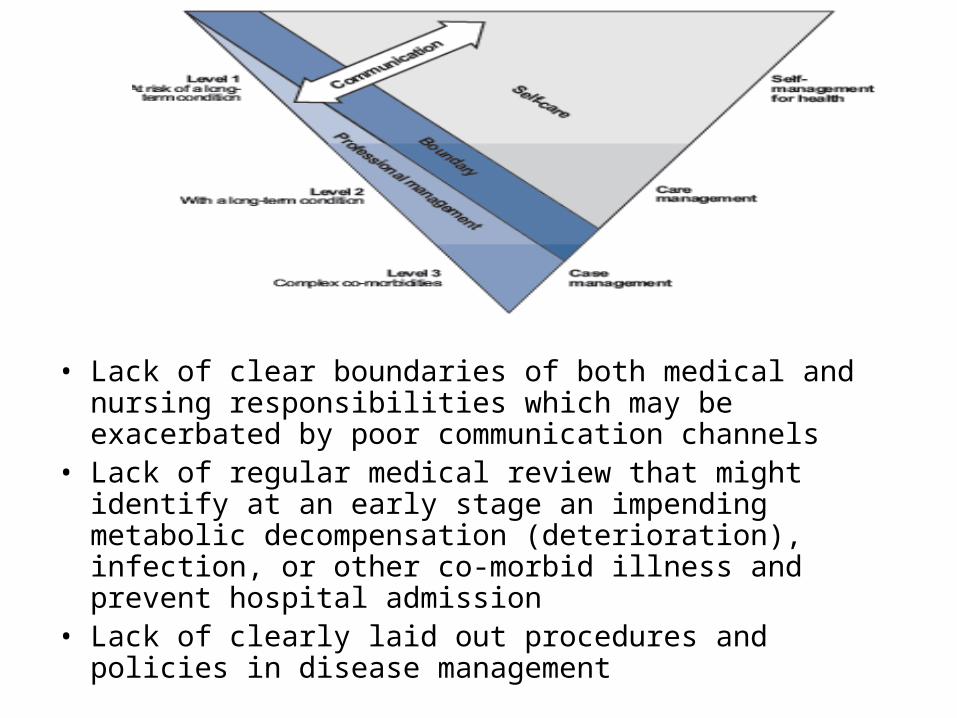
• Lack of clear boundaries of both medical and nursing responsibilities which may be exacerbated by poor communication channels
• Lack of regular medical review that might identify at an early stage an impending metabolic decompensation (deterioration), infection, or other co-morbid illness and prevent hospital admission
• Lack of clearly laid out procedures and policies in disease management
Key messages
• Lack of clarity within care settings in defining appropriate competencies in health management for different health and social care professionals.
• High level of co-morbidities and communication difficulties in service users
• Underestimation of the effect of existing co-morbidities in worsening clinical outcomes for service users; this could be exacerbated by lack of appropriate training for care staff.
• Lack of understanding and recognition of frailty among elderly service users
• Restrictive professional boundaries which prevent secondary healthcare professionals from having specific input into PVI care organisations
• Lack of national standards of diabetes care within Social Care Organisations.
• As a result of many of these barriers to care, common management difficulties arise.
Key interventions
• Training
• Clearly laid out policies
• Regular monitoring
• Regular review
• Daily team meetings
• Informed handovers