Obesity Primer for the Practicing Gastroenterologist ...
17
Obesity Primer for the Practicing Gastroenterologist Pichamol Jirapinyo, MD, MPH 1,2 and Christopher C. Thompson, MD, MSc 1,2 With worsening of the obesity pandemic, gastroenterologists will see more patients with this chronic disease. Given the association between obesity and several gastrointestinal conditions and the interplay between obesity pathophysiology and gut hormones, gastroenterologists can play an important role in the management of this disease. Furthermore, because more patients undergo bariatric surgery, an understanding of postsurgical anatomy and medical and endoscopic management of bariatric surgical complications is essential. This article provides clinical tools for the assessment and management of obesity for the general gastroenterologist. Tables containing high-yield practical information are also provided for quick reference. Am J Gastroenterol 2021;116:918–934. https://doi.org/10.14309/ajg.0000000000001200 INTRODUCTION Obesity has become pandemic. It is estimated that more than 650 million adults (13% worldwide) suffer from obesity (1). In the United States, the prevalence is even higher with 42.4% of adults meeting criteria for obesity (2). As of 2013, the American Medical Association officially recognized obesity as a chronic disease (3). There are several ways to define and categorize obesity. Per the Obesity Medicine Association, obesity is “a chronic, relapsing, multifactorial, and neurobehavioral disease, wherein an increase in body fat promotes adipose tissue dysfunction and abnormal fat mass physical forces, resulting in adverse metabolic, bio- mechanical, and psychosocial health consequences (4).” Tradi- tionally, obesity has also been defined as a body mass index (BMI) of at least 30 kg/m 2 . It is further categorized into class I obesity (BMI 30–34.9 kg/m 2 ), class II obesity (BMI 35–39.9 kg/m 2 ), and class III obesity (BMI $40 kg/m 2 ) (5). The use of BMI, however, is limited in certain populations, such as the elderly, muscular, and sarco- penic, because it does not distinguish between lean muscle and body fat or its location (6). Alternatively, waist circumference (WC) may be used. Specifically, for patients with a BMI of 25–34.9 kg/m 2 , WC of $40 inches (.102 cm) in men and $35 inches (.88 cm) in women suggest central obesity, which is associated with increased cardiometabolic risk (7–9). Finally, obesity may also be defined as body fat percentage of $ 25% in men and 35% in women with the healthy body fat ranging from 8% to 19% in men and 21%–35% in women (depending on age) (4,10,11). Nevertheless, accurate body composition testing can be expensive with limited availability. Furthermore, it is important to note that these cutoffs vary based on ethnicity, such as a BMI of $25 and $27 kg/m 2 being used to define obesity in Asian and Middle East populations, re- spectively, because of their higher body fat at a lower BMI and earlier appearance of comorbidities (12,13). This review is intended to serve as a clinical guide for the general gastroenterologist on the assessment and management of obesity. Tables containing high-yield information are also pro- vided for quick reference. OBESITY-RELATED GASTROINTESTINAL CONDITIONS Obesity is associated with several gastrointestinal (GI) conditions including various esophageal, gastric, small intestinal, colonic, hepatobiliary, and pancreatic diseases (14–17). Specifically, obe- sity may result in a higher incidence, earlier presentation, and more severe clinical manifestations of these diseases. For exam- ple, obesity increases the risk of gastroesophageal reflux disease, esophagitis, and esophageal adenocarcinoma by 2-, 1.8-, and 2.8- fold, respectively (18). Similarly, the incidence of nonalcoholic fatty liver disease is approximately 90% in patients with obesity, compared with 25% in the general population (19), and obesity has been shown to hasten the progression from compensated to decompensated cirrhosis (20). However, weight loss of at least 7%–10% total weight loss (TWL) has been shown to reverse histologic features of fatty liver (21). A more extensive list of obesity-related GI conditions is summarized in Table 1 and can be more deeply explored in the work of Camilleri et al. (14). Given these associations, gastroenterologists should have an increased suspicion and low threshold to look for these illnesses in this patient population. In addition, early diagnosis of obesity and timely evaluation and management may help reduce the preva- lence and severity of such disorders. OBESITY EVALUATION The obesity evaluation consists of several elements including medical, lifestyle, psychological, and endoscopic assessments. Initial evaluation During the initial encounter, physicians should assess patients’ readiness to change their health behavior using the “Stages of Change” model (22,23). Specifically, the model consists of 5 stages: (i) precontemplation: the individual is unaware of the consequences of their behavior and resistant to change, (ii) contemplation: the individual is aware of the consequences and open to change, (iii) preparation: the individual shows 1 Division of Gastroenterology, Hepatology and Endoscopy, Brigham and Women’s Hospital, Boston, Massachusetts, USA; 2 Harvard Medical School, Boston, Massachusetts, USA. Correspondence: Christopher C. Thompson, MD, MSc. E-mail: [email protected]. Received June 4, 2020; accepted December 29, 2020; published online April 6, 2021 The American Journal of GASTROENTEROLOGY VOLUME 116 | MAY 2021 www.amjgastro.com REVIEW ARTICLE 918 REVIEW ARTICLE Copyright © 2021 by The American College of Gastroenterology. Unauthorized reproduction of this article is prohibited.
Transcript of Obesity Primer for the Practicing Gastroenterologist ...

Dow
nloadedfrom
http://journals.lww.com
/ajgby
BhDMf5ePH
Kav1zEoum1tQ
fN4a+kJLhEZgbsIH
o4XMi0hC
ywCX1AW
nYQp/IlQ
rHD3i3D
0OdR
yi7TvSFl4Cf3VC
4/OAVpD
Da8K2+Ya6H
515kE=on
05/09/2021Downloadedfromhttp://journals.lww.com/ajgbyBhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD3i3D0OdRyi7TvSFl4Cf3VC4/OAVpDDa8K2+Ya6H515kE=on05/09/2021
Obesity Primer for the Practicing GastroenterologistPichamol Jirapinyo, MD, MPH1,2 and Christopher C. Thompson, MD, MSc1,2
With worsening of the obesity pandemic, gastroenterologists will see more patients with this chronic disease. Given the
association between obesity and several gastrointestinal conditions and the interplay between obesity pathophysiology and
gut hormones, gastroenterologists canplayan important role in themanagement of this disease.Furthermore, becausemore
patients undergo bariatric surgery, an understanding of postsurgical anatomy andmedical and endoscopic management of
bariatric surgical complications is essential. This article provides clinical tools for the assessment and management of
obesity for the general gastroenterologist. Tables containing high-yield practical information are also provided for quick
reference.
Am J Gastroenterol 2021;116:918–934. https://doi.org/10.14309/ajg.0000000000001200
INTRODUCTIONObesity has become pandemic. It is estimated that more than 650million adults (13% worldwide) suffer from obesity (1). In theUnited States, the prevalence is even higher with 42.4% of adultsmeeting criteria for obesity (2). As of 2013, the AmericanMedicalAssociation officially recognized obesity as a chronic disease (3).
There are several ways to define and categorize obesity. Per theObesity Medicine Association, obesity is “a chronic, relapsing,multifactorial, and neurobehavioral disease, wherein an increase inbody fat promotes adipose tissue dysfunction and abnormal fatmass physical forces, resulting in adverse metabolic, bio-mechanical, and psychosocial health consequences (4).” Tradi-tionally, obesity has also been defined as a body mass index (BMI)of at least 30kg/m2. It is further categorized into class I obesity (BMI30–34.9 kg/m2), class II obesity (BMI 35–39.9 kg/m2), and class IIIobesity (BMI$40 kg/m2) (5). The use of BMI, however, is limitedin certain populations, such as the elderly, muscular, and sarco-penic, because it does not distinguish between lean muscle andbody fat or its location (6). Alternatively, waist circumference(WC)may be used. Specifically, for patients with a BMI of 25–34.9kg/m2,WCof$40 inches (.102 cm) inmen and$35 inches (.88cm) in women suggest central obesity, which is associated withincreased cardiometabolic risk (7–9). Finally, obesity may also bedefined as body fat percentageof$ 25% inmenand 35% inwomenwith the healthy body fat ranging from 8% to 19% in men and21%–35% in women (depending on age) (4,10,11). Nevertheless,accurate body composition testing can be expensive with limitedavailability. Furthermore, it is important to note that these cutoffsvarybased on ethnicity, such as aBMIof$25and$27kg/m2 beingused to define obesity in Asian and Middle East populations, re-spectively, because of their higher body fat at a lower BMI andearlier appearance of comorbidities (12,13).
This review is intended to serve as a clinical guide for thegeneral gastroenterologist on the assessment and management ofobesity. Tables containing high-yield information are also pro-vided for quick reference.
OBESITY-RELATED GASTROINTESTINAL CONDITIONSObesity is associated with several gastrointestinal (GI) conditionsincluding various esophageal, gastric, small intestinal, colonic,hepatobiliary, and pancreatic diseases (14–17). Specifically, obe-sity may result in a higher incidence, earlier presentation, andmore severe clinical manifestations of these diseases. For exam-ple, obesity increases the risk of gastroesophageal reflux disease,esophagitis, and esophageal adenocarcinoma by 2-, 1.8-, and 2.8-fold, respectively (18). Similarly, the incidence of nonalcoholicfatty liver disease is approximately 90% in patients with obesity,compared with 25% in the general population (19), and obesityhas been shown to hasten the progression from compensated todecompensated cirrhosis (20). However, weight loss of at least7%–10% total weight loss (TWL) has been shown to reversehistologic features of fatty liver (21). A more extensive list ofobesity-relatedGI conditions is summarized inTable 1 and can bemore deeply explored in the work of Camilleri et al. (14). Giventhese associations, gastroenterologists should have an increasedsuspicion and low threshold to look for these illnesses in thispatient population. In addition, early diagnosis of obesity andtimely evaluation and management may help reduce the preva-lence and severity of such disorders.
OBESITY EVALUATIONThe obesity evaluation consists of several elements includingmedical, lifestyle, psychological, and endoscopic assessments.
Initial evaluation
During the initial encounter, physicians should assess patients’readiness to change their health behavior using the “Stages ofChange” model (22,23). Specifically, the model consists of 5stages: (i) precontemplation: the individual is unaware of theconsequences of their behavior and resistant to change, (ii)contemplation: the individual is aware of the consequences andopen to change, (iii) preparation: the individual shows
1Division of Gastroenterology, Hepatology and Endoscopy, Brigham and Women’s Hospital, Boston, Massachusetts, USA; 2Harvard Medical School, Boston,Massachusetts, USA. Correspondence: Christopher C. Thompson, MD, MSc. E-mail: [email protected] June 4, 2020; accepted December 29, 2020; published online April 6, 2021
The American Journal of GASTROENTEROLOGY VOLUME 116 | MAY 2021 www.amjgastro.com
REVIEW ARTICLE918REV
IEW
ARTICLE
Copyright © 2021 by The American College of Gastroenterology. Unauthorized reproduction of this article is prohibited.

anticipation and willingness to change within the next 6 months,(iv) action: the individual is in the process of changing their be-havior, and (v)maintenance: the individual has sustained the newbehavior for more than 6 months. For patients in the
precontemplation stage, the goal is to help move them to thecontemplation stage before referral to bariatric specialists. Mo-tivational interviewing techniques, such as the 5 A’s (Ask, Advise,Assess, Assist, and Arrange) and OARS (Open-ended questions,Affirmations, Reflections, and Summaries), can help with thisprocess to elicit and strengthen patient’s motivation along thisspectrum (24,25).
Medical evaluation
A weight-focused history, physical examination, and laboratoryevaluation should be obtained. Weights at specific time points,including around the major life events, and the effectiveness ofprevious weight loss attempts should be reviewed. Certain med-ications can cause weight gain and should be downtitrated orsubstituted with weight neutral drugs (Table 2) (26,27). Onphysical examination, BMI, WC, waist-hip ratio, and percentbody fat should be measured. Signs of obesity-associated medicalconditions including hyperpigmented skin around the neck oraxilla (acanthosis nigricans associated with insulin resistance),hirsutism (polycystic ovarian syndrome), large neck circumfer-ence (.17 inches for men or .16 inches for women suggestingincreased risk of sleep apnea), and thin, atrophic skin (Cushingdisease) should be looked for (28). Baseline laboratory shouldinclude electrolytes, renal function, fasting glucose, hemoglobinA1c (HbA1c), liver enzymes, complete blood count, lipid panel,thyroid-stimulating hormone, vitamin D, and urine albumin.
Lifestyle evaluation
Dietary and eating habits should be reviewed using a 24-hour dietrecall, food frequency questionnaire, or food log. Dietary habitsincluding eating patterns (skipping breakfast, eating one largemeal per day, emotional eating, and grazing), frequency of eatingout, and grocery shopping details should be evaluated. Further-more, onset of satiation (the point at which one becomes fullending one’s desire to eat during a single meal) and period ofsatiety (the state of being full and satisfied which regulates thetime elapsed between 2 meals) should be assessed.
Physical lifestyle should be assessed. It is important to un-derstand whether patients have an active or sedentary lifestyleand details regarding exercise (types, duration, and frequency).Total energy expenditure (TEE) is the amount of calories burnedper day. It is composed of resting energy expenditure (REE),thermic effect of meals (TEM), and energy expenditure fromphysical activity (EEPA), which is further broken down into ex-ercise and nonexercise activity thermogenesis (NEAT).
TEE ¼ REE ð60%2 75%Þ1TEM ð10%Þ1 ½exercise1NEAT� ð15%2 30%Þ
REE is the energy cost of physiological functions at rest, suchas respiration, cardiac output, and body temperature regulation.TEM is the energy required for digestion, absorption, and dis-posal of ingested nutrients. Its magnitude depends on macro-nutrient composition with proteins requiring the most energy(20%–35% of energy consumed), followed by carbohydrates(5%–15%) and fats (5%–15%) (29,30). EEPA consists of exerciseandNEAT,which is the energy expended for physical activity thatis not sleeping, eating, or exercise. As shown in the equation,changing one’s lifestyle directly affects EEPA, resulting in changesin TEE and daily net calories.
Table 1. Gastrointestinal conditions associated with obesity
Gastrointestinal
organ
Gastrointestinal conditions
associated with obesity
Esophagus •Abnormal esophageal peristalsis
•Isolated hypertensive LES pressure
•Isolated hypotensive LES pressure
•GERD•Erosive esophagitis•Barrett’s esophagus•Esophageal adenocarcinoma
Stomach •Dyspepsia•Erosive gastritis•Gastric ulcer
•Gastric cancer
•Greater fasting gastric volume
•Decreased satiation
Small intestine •Duodenal ulcer•Small intestinal bacterial overgrowth
•Diarrhea (related to changes in bile acids,
accelerated colonic transit, and increased mucosal
permeability)
•Increased absorption of glucose (related to increasedSGLT-1)
•Increased absorption of protein (specifically whey
hydrolysate)
•Increased absorption of long chain fatty acids (relatedto increased induction of lipid binding proteins)
Colon •Diverticulosis•Diverticular bleeding•Recurrent diverticulitis•Clostridium difficile infection
•Adenomatous polyps
•Sessile serrated polyps
•Colorectal cancer•Dyssynergic defecation•Incomplete rectal evacuation
•Fecal incontinence•Crohn’s disease (conflicting data)
•Earlier loss of response to biologics in IBD patients
Liver •Nonalcoholic fatty liver disease
•Nonalcoholic steatohepatitis
•Cirrhosis•Hepatocellular carcinoma
Biliary •Cholelithiasis•Cholecystitis•Cholesterolosis•Gallbladder cancer
Pancreas •Acute pancreatitis
•Pancreatic cancer
GERD, gastroesophageal reflux disease; IBD, inflammatory bowel disease; LES,lower esophageal sphincter; SGLT-1, sodium glucose linked transporter-1.
© 2021 by The American College of Gastroenterology The American Journal of GASTROENTEROLOGY
REV
IEW
ARTICLE
Obesity Primer 919
Copyright © 2021 by The American College of Gastroenterology. Unauthorized reproduction of this article is prohibited.

Psychological evaluation
Psychiatric history including anxiety, depression, and post-traumaticstress disorder shouldbe assessedbecause thismay translate into eatingdisorders. It is important to assesswhether patients suffer frombulimianervosa (recurrent episodes of binge eating 1 inappropriate com-pensatory behavior to prevent weight gain), binge eating disorder(recurrent episodes of binge eating without compensatory behavior),purging disorder (recurrent purging behavior without binge eating),andnight eating syndrome (recurrent episodesofnight eating) becausethese require referral to amental health specialist (31). Physiciansmayconsider using the Eating Disorder Examination Questionnaire forscreening purposes (Table 3) (32,33).
Endoscopic evaluation
Endoscopy may be required as part of the initial evaluation for asubgroup of patients with obesity. In addition, for those who areundergoing bariatric surgery, the International Federation for theSurgery of Obesity and Metabolic Disorders recommends that apreoperative esophagogastroduodenoscopy should be considered forall patients with and without GI symptoms (34). During this
procedure, one shouldnote thepresenceof a hiatal hernia (HillGradeI–IV), esophagitis, Barrett’s esophagus, gastric polyps, gastritis, Hel-icobacter pylori infection, and malignancy. According the systematicreview and meta-analysis conducted by the International Federationfor the Surgery of Obesity and Metabolic Disorders task force (63studies/22495 patients), abnormal esophagogastroduodenoscopyfindings are likely to be found in at least 55.5% of patients beforebariatric surgery (25.3% for a subgroup of asymptomatic patients)with 16.5% having findings that led to modification or delay of theplanned procedure and 0.2% having surgery cancelled (34).
Gastroenterologists should also be familiar with postbariatric sur-gical anatomy including normal and abnormal endoscopic findings.For Roux-en-Y gastric bypass (RYGB), the pouch and gastrojejunalanastomotic sizes shouldbeassessed.Thepresence, location, andsizeofmarginal ulceration and gastrogastric fistula should be documented.For sleeve gastrectomy (SG), the sleeve dimension/configuration andthe presence of sleeve stenosis and/or angulation should be assessed.Furthermore, given the prevalence of de novo reflux (23%) after SG,gastroenterologists should be vigilant in assessing for the presence ofesophagitis (found in up to 53%) and Barrett’s esophagus (found in
Table 2. Medications associated with weight gain, weight neutrality, and weight loss
Medication type Weight gain Weight neutral Weight loss
Antihypertensives Alpha-blockers
• Prazosin• Doxazosin• Terazosin Beta-blockers
• Atenolol• Metoprolol
• Nadolol• Propranolol
ACE inhibitors, ARBs
Beta-blockers
• Carvedilol• NebivololCalcium channel blockers
Thiazides
Antidiabetics Insulin, Meglitinides, Sulfonylureas,
Thiazolidinediones
Alpha-glucosidase inhibitors, Bromocriptine,
Colesevelam, DPP-4 inhibitors
GLP-1 agonists, Metformin,
Pramlintide, SGLT2 inhibitors
Antidepressants MAOIs, Mirtazapine SSRIs
• Citalopram• Paroxetine TCAs
SSRIs
• Fluoxetine• Sertraline
Bupropion
Antipsychotics Clozapine, Lithium Olanzapine,
Quetiapine Risperidone
Aripiprazole, Lurasidone, Ziprasidone
Anticonvulsants Carbamazepine Gabapentin,
Pregabalin, Valproic acid
Lamotrigine, Levetiracetam, Phenytoin Topiramate, Zonisamide
Contraceptives Progestin Barrier methods, Intrauterine device,
Surgical sterilization
Antihistamines First-generation antihistamines
• Diphenhydramine
• Hydroxyzine• Meclizine
Second-generation antihistamines
• Cetirizine• LoratidineThird-generation anti-histamines
• FexofenadineAlternative class of medications
• Decongestants
Steroids Glucocorticoids Inhaled steroids Topical steroids Alternative
classes of medications
• NSAIDs• DMARDs
ACE, angiotensin-converting enzyme; ARB, angiotensin II receptor blockers; DMARD, disease-modifying antirheumatic drug; DPP-4, dipeptidyl peptidase-4; GLP-1,glucagon-like peptide-1; MAOI, monoamine oxidase inhibitor; NSAID, nonsteroidal anti-inflammatory drug; SGLT2, sodium-glucose co-transporter 2; SSRI, selectiveserotonin reuptake inhibitor; TCA, tricyclic antidepressants.
The American Journal of GASTROENTEROLOGY VOLUME 116 | MAY 2021 www.amjgastro.com
REV
IEW
ARTICLE
Jirapinyo and Thompson920
Copyright © 2021 by The American College of Gastroenterology. Unauthorized reproduction of this article is prohibited.

Table 3. Eating Disorder Examination Questionnaire (EDE-Q) (32,33))
Eating Questionnaire
Instructions: The following questions are concerned with the past 4 wk (28 d) only. Please read each question carefully. Please answer all of the questions. Please only choose one answer for each question.
Thank you.
Questions 1 to 12: Please circle the appropriate number on the right. Remember that the questions only refer to the past 4 wk (28 d) only.
On how many of the past 28 d … No days 1–5 d 6–12 d 13–15 d 16–22 d 23–27 d Every day
1. Have you been deliberately trying to limit the amount of
food you eat to influence your shape or weight (whether or
not you have succeeded)?
0 1 2 3 4 5 6
2. Have you gone for long periods of time (8 waking hours or
more) without eating anything at all in order to influence your
shape or weight?
0 1 2 3 4 5 6
3. Have you tried to exclude from your diet and foods that
you like in order to influence your shape or weight (whether
or not you have succeeded)?
0 1 2 3 4 5 6
4. Have you tried to follow definite rules regarding your
eating (e.g., a calorie limit) in order to influence your shape
or weight (whether or not you have succeeded)?
0 1 2 3 4 5 6
5. Have you had a definite desire to have an empty stomach
with the aim of influencing your shape or weight?
0 1 2 3 4 5 6
6. Have you had a definite desire to have a totally flat
stomach?
0 1 2 3 4 5 6
7. Has thinking about food, eating or calories made it very
difficult to concentrate on things you are interested in (e.g.,
working, following a conversation, or reading)?
0 1 2 3 4 5 6
8. Has thinking about shape or weight made it very difficult
to concentrate on things you are interested in (e.g., working,
following a conversation, or reading)?
0 1 2 3 4 5 6
9. Have you had a definite fear of losing control over eating? 0 1 2 3 4 5 6
10. Have you had a definite fear that you might gain weight? 0 1 2 3 4 5 6
11. Have you felt fat? 0 1 2 3 4 5 6
12. Have you had a strong desire to lose weight? 0 1 2 3 4 5 6
Questions 13 to 18: Please fill in the appropriate number in the boxes on the right. Remember that the questions only refer to the past 4 wk (28 d).Over the past 4 wk (28 d)…
13. Over the past 28 d, how many times have you eaten what other people would regard as an unusually large amount of food (given the circumstances)? ………………
14. On how many of these times did you have a sense of having lost control over your eating (at the time that you were eating)? ………………
15. Over the past 28 d, on howmany DAYS have such episodes of overeating occurred (i.e., you have eaten an unusually large amount of food and have had a sense of
loss of control at the time)?
………………
16. Over the past 28 d, how many times have you made yourself sick (vomit) as a means of controlling your shape or weight? ………………
©2021by
TheAmerican
College
ofGastroenterology
TheAmerican
JournalofGASTROEN
TER
OLO
GY
REVIEW ARTICLE
Obesity
Prim
er921
Copyright
©2021
byThe
American
College
ofGastroenterology.U
nauthorizedreproduction
ofthis
articleisprohibited.

Table 3. (continued)
17. Over the past 28 d, how many times have you taken laxatives as a means of controlling your shape or weight? ………………
18. Over the past 28 d, howmany times have you exercised in a “driven” or “compulsive”way as ameans of controlling your weight, shape or amount of fat, or to burn
off calories?
………………
Questions 19 to 21: Please circle the appropriate number. Please note that for these questions the term “binge eating”means eating what others would regard as an unusually large amount of food for the
circumstances, accompanied by a sense of having lost control over eating.
19. Over the past 28 d, on how many days
have you eaten in secret (i.e. furtively)?
… Do not count episodes of binge eating
No days 1–5 d 6–12 d 13–15 d 16–22 d 23–27 d Every day0 1 2 3 4 5 6
20. On what proportion of the times that you have
eaten have you felt guilty (felt that you’ve donewrong)
because of its effect on your shape or weight?…
Do not count episodes of binge eating
None of the
times
A few of
the
times
Less than half Half of the
times
More than half Most of the time Every time
0 1 2 3 4 5 6
21. Over the past 28 d, how concerned have you
been about other people seeing you eat?…
Do not count episodes of binge eating
Not at all Slightly Moderately Markedly0 1 2 3 4 5 6
Questions 22 to 28: Please circle the appropriate number on the right. Remember that the questions only refer to the past 4 wk (28 d).
Over the past 28 d … Not at all Slightly Moderately Markedly
22. Has your weight influenced how you think about (judge)
yourself as a person?
0 1 2 3 4 5 6
23. Has your shape influenced how you think about (judge)
yourself as a person?
0 1 2 3 4 5 6
24. How much would it have upset you if you had been
asked toweigh yourself once aweek (nomore, or less, often)
for the next four weeks?
0 1 2 3 4 5 6
25. How dissatisfied have you been with your weight? 0 1 2 3 4 5 6
26. How dissatisfied have you been with your shape? 0 1 2 3 4 5 6
27. How uncomfortable have you felt seeing your body (e.g,
seeing your shape in themirror, in a shop window reflection,
while undressing or taking a bath or shower)?
0 1 2 3 4 5 6
28. How uncomfortable have you felt about others seeing
your shape or figure (e.g., in communal changing rooms,
when swimming, or wearing tight clothes)?
0 1 2 3 4 5 6
What is your weight at present? (Please give your best estimate.) …………………….
What is your height? (Please give your best estimate.) …………………….
If female: Over the past 3-to-4 mo have you missed any menstrual periods? …………………….
If so, how many? …………………….
Have you been taking the “pill”? …………………….
TheAmerican
Journal
ofGASTROEN
TER
OLO
GY
VOLU
ME116
|MAY
2021
www.am
jgastro.com
REVIEW ARTICLEJirap
inyo
andThompson
922
Copyright
©2021
byThe
American
College
ofGastroenterology.U
nauthorizedreproduction
ofthis
articleisprohibited.

Table 4. Dietary interventions for weight loss
Dietary plans Description
Energy focused
Low calorie diet • 1,200–1,600 kcal/d
Very low calorie diet •#800 kcal/d
• Prescribed for #16 wk
Protein-sparing modified fast •#800 kcal/d
• High protein (1.5 g protein/kg ideal body weight)
• Low carbohydrate (,20 g of carbohydrate per day)
• Fat restricted to the protein source
• Prescribed for #6 mo
Meal replacement • Use of liquid shakes and/or bars with a known amount of energy and
macronutrient content to replace 1–3 meals
Macronutrient focused
Low carbohydrate diet •,20% of total energy intake from carbohydrate
Low dlycemic index diet • Replace high GI diet (GI $55) with low GI diet (GI ,55)
Low fat diet •,15%–20% of total energy intake from fat
High protein •$20%–30% of total energy intake from protein
Dietary pattern focused
Atkins diet • Low carbohydrate (,20 g of carbohydrate per day; may increase to 50 g
after 2 wk)
• High protein
• High fat
Ketogenic diet • Low carbohydrate (,20 g of carbohydrate per day)
• Moderate protein (10%–20% of total energy intake from protein)
• High fat
DASH diet • Complex carbohydrate
• Lean protein (avoid red meat)
• Low-fat dairy products as the primary source of fat
• Emphasis on fruits and vegetables
Mediterranean diet • Complex carbohydrate
• Fish and poultry as the primary sources of
protein (avoid red meat)
• Olive oil as the primary source of fat
• Emphasis on plant-based food (fruits, vegetables,
grains, nuts, seeds)
Ornish diet • Vegetarian Diet
• Very low fat (,10% of total energy intake from fat)
Paleolithic diet • Emphasis on fruits, vegetables, nuts, seeds, lean meat, fish
• Avoid grains, legumes, dairy products, processed food
Zone diet • 40% of total energy intake from carbohydrate
• 30% of total energy intake from protein
• 30% of total energy intake from fat
Vegan diet • Exclusion of all animal products and byproducts
Vegetarian diet • Exclusion of all animal products
Dietary-timing focused
Intermittent fasting
Alternate-day fasting
Modified dlternate-day fasting
5:2 Intermittent fasting
Daily time-restricted feeding
• Fast every other day; no calorie restriction on non-fasting days
• 500 kcal/d on fasting days; no calorie
restriction on non-fasting days
• For 5 d/wk, eat normally without calorie restriction
• For 2 d/wk, eat 500–600 kcal/d
• 12–18 h of fasting per day; 6–12 h of feeding per day
© 2021 by The American College of Gastroenterology The American Journal of GASTROENTEROLOGY
REV
IEW
ARTICLE
Obesity Primer 923
Copyright © 2021 by The American College of Gastroenterology. Unauthorized reproduction of this article is prohibited.

11.6%) in this patient population (34,35). For laparoscopic adjustablegastric band, retroflexion to evaluate for band erosion should beperformed.
Other evaluation
After the initial evaluation, additional studies, such as direct/indirectcalorimetry, Homeostatic Model Assessment of Insulin Resistance,liver ultrasound with elastography, and magnetic resonance elas-tography, may be obtained on a case-by-case basis. Furthermore,referral to appropriate specialists for signs or symptoms of non-GIobesity-related comorbidities should be considered.
OBESITY MANAGEMENTThe spectrum of obesity treatment options includes lifestylemodification, pharmacotherapy, endoscopy, and surgery.
Lifestyle modification
Lifestyle modification (LM) is considered first-line therapy for thetreatment of obesity. It includes 3 primary components—diet, exercise,and behavioral therapy.
To achieve weight loss, an energy deficit is required. This can beaccomplishedbyrestrictingcaloric intakeor limitingcertain food types.To reduce caloric intake, women should target 1,200–1,500 kcal/d,
whereas men target 1,500–1,800 kcal/d (8). Alternatively, an indi-vidual’s energy requirement may be estimated using calorimetry oravailable equations, and an energy deficit of 500–750 kcal/d or a 30%energy deficit can be prescribed. Alternatively, instead of a formalenergy deficit target, lower calorie intake may be achieved by re-striction or elimination of particular food groups, such as carbohy-drates. According to the US Dietary Guidelines, the recommendedmacronutrient proportions consist of carbohydrate (45%–65%),protein (10%–35%), and fat (20%–35%) (36). Adjusting these pro-portions may facilitate weight loss in some individuals by simplifyingdietary goals. Although there are no universally accepted definitions,examples of macronutrient-focused diet plans include high protein($20%–30% protein), low carbohydrate (,20% carbohydrate), andlow fat (,15%–20% fat) diets (37–40). There are several randomized,controlled trials comparing diets with various macronutrient com-positions. The largest study conducted by Sacks et al. randomized 811overweight adults to 1 of 4 diets—low fat/average protein (highestcarbohydrate: 65% of calories), low fat/high protein, high fat/averageprotein, and high fat/high protein (lowest carbohydrate: 35% of cal-ories). No significant differences in weight loss were observed amongthe 4 groups at 2 years (41). Other trials also demonstrated similarresults with meta-analyses showing that adherence is the strongestpredictor for weight loss (42). Macronutrient content may affect
Table 4. (continued)
Dietary plans Description
Commercial weight loss programs
HMR
Healthy solutions plan
Decision-free plan
• Meal replacement 1 home delivered meals (low calorie diet)
• 1,200 kcal/d
• 3-2-5 daily plan (3 HMR shakes, 2 HMR entrees, 5 servings of fruits,
vegetables)
• 500–800 kcal/d
• All shakes or 3-2 daily plan (3 HMR shakes, 2 HMR entrees)
• Medically supervised
Jenny Craig • Home delivered meals (low calorie diets)
• Individual in-person or telephone-based counseling sessions
Nutrisystem • Home delivered meals (low calorie/low glycemic index diets)
• 50% of total energy intake from carbohydrate
• 25% of total energy intake from protein
• 25% of total energy intake from fat
SlimFast diet • Meal replacement 1 home delivered meals (low calorie diet)
• 2 SlimFast meal replacements (shakes, bars, cookies)
• One 500–600 kcal meal of one’s choice
• Three 100 kcal snacks
South beach diet • Home delivered meals (modified low carbohydrate diets)
• ,50 g of carbohydrate per day (weight loss phase), then 75–100g of
carbohydrate per day (maintenance phase)
• Higher protein (25%–30% of total energy intake from protein)
• Healthy fat
Weight watchers • Points-based dietary system
•Member is assigned daily andweekly points based on height, weight, age,
gender
• Food is assigned points based on calories, saturated fat, sugar (increasedpoints), and protein (decreased points)
• Zero-point foods: fruits, nonstarchy vegetables, eggs, skinless chicken,fish, beans, tofu, and plain yogurt
• In-person meetings, web-based monitoring, or personal coaching calls
The American Journal of GASTROENTEROLOGY VOLUME 116 | MAY 2021 www.amjgastro.com
REV
IEW
ARTICLE
Jirapinyo and Thompson924
Copyright © 2021 by The American College of Gastroenterology. Unauthorized reproduction of this article is prohibited.

Table 5. Commonly prescribed obesity medications
Medications Dosage/titration Mechanisms of action Efficacy Contraindications Common side effects FDA status
Phentermine (Adipex) 15 mg qd (starting dose)
37.5 mg qd
Norepinephrine-releasing
agent
6.8% TWL at 28 wk (96) Pregnancy/breastfeeding
History of CVD
MAOIs (within 14 d)
Hyperthyroidism
Glaucoma
History of drug abuse
Headache, elevated BP,
elevated HR, palpitations,
insomnia, dry mouth,
constipation, anxiety
Approved in 1960s for short-
term use (3 mo)
Orlistat (Xenical)
Alli (OTC)
120 mg tid before meals
60 mg tid before meals (for
Alli)
Pancreatic and gastric lipase
inhibitor
7.4% TWL at 1 yr (97) Pregnancy
Chronic malabsorption
syndrome
Cholestasis
Decreased absorption of fat-
soluble vitamins,
steatorrhea, oily spotting,
flatulence
Approved in 1999 for chronic
weight management
Phentermine (P)/
Topiramate ER (T) (Qsymia)
Alternative:
Phentermine (gen) 1
topiramate (gen)
P: 3.75 mg, T: 23 mg qd
(starting dose 3 14 d)
P: 7.5 mg, T: 46 mg qd
(recommended dose)
P: 15 mg, T: 92 mg qd (high
dose)
P: 15 mg qd1
T: 25 mg bid
Norepinephrine-releasing
agent (P)
1 GABA receptor
modulation (T)
7.8% TWL at 1 yr (98) Pregnancy
MAOIs (within 14 d)
Hyperthyroidism
Glaucoma
Insomnia, dry mouth,
constipation, paresthesia,
dizziness
Approved in 2012 for chronic
weight management
Naltrexone SR (N)/
Bupropion SR (B)
(Contrave)
N: 8 mg, B: 90 mg
2 tabs bid
Week 1: 1 tab qam
Week 2: 1 tab bid
Week 3: 2 tabs qam/1 tab
qpm
Week 4: 2 tabs bid
Opioid antagonist (N) 1
reuptake inhibitor of
dopamine and
norepinephrine (B)
6.1% TWL at 1 yr (99) Pregnancy
Uncontrolled HTN
Seizure disorder
Bulimia or anorexia
Chronic opioid or opioid
agonist use
Alcohol withdrawal
MAOIs (within 14 d)
Headache, nausea,
constipation, dizziness
Approved in 2014 for chronic
weight management
Liraglutide (Saxenda) 3 mg injectable qd
Week 1: 0.6 mg daily; then
increased by 0.6 mg weekly
until 3 mg daily is reached
GLP-1 agonist 8.0% TWL at 1 yr (100) Pregnancy
Personal or family history of
medullary thyroid
Carcinoma or multiple
Endocrine neoplasia
Syndrome type 2
Nausea, vomiting,
pancreatitis
Approved in 2014 for chronic
weight management
Metformin (Glucophage) 500 mg qd (starting dose)
1,000 mg bid (max dose)
Decreases hepatic glucose
production
Decreases intestinal glucose
absorption
Increases peripheral glucose
uptake
2.3 kg additional weight loss
compared to placebo (101)
Chronic heart failure
Metabolic acidosis
Diabetic ketoacidosis
Severe renal disease
Nausea, vomiting, diarrhea,
flatulence
Off-label for obesity
Approved for T2DM
©2021by
TheAmerican
College
ofGastroenterology
TheAmerican
JournalofGASTROEN
TER
OLO
GY
REVIEW ARTICLE
Obesity
Prim
er925
Copyright
©2021
byThe
American
College
ofGastroenterology.U
nauthorizedreproduction
ofthis
articleisprohibited.

patient preferences but is only one of many factors influencing ad-herence. Given the relatively equivalent efficacy of different dietaryapproaches, a diet planmay be chosen based onmetabolic risk factorsand patient preferences. Specifically, low fat diets induce greater re-duction in low-density lipoprotein,whereas lowcarbohydratediets areassociated with greater improvement in triglycerides, high-density li-poprotein, and HbA1c (41,43–46). Table 4 summarizes the morecommonly prescribed diet plans.
Physical activity is an essential component of a weight loss pro-gram. Specifically, at least 150minutes of aerobic activity per week isrecommended (at least 30 minutes per day, most days of the week)(8,47), with at least 2 resistance training days per week (minimumof1 set of 8–12 repetitions for a total of 8–10 exercises per week) (48).Resistance training is important because it helps improve musclestrength and endurance, modify coronary risk factors, and preservefat-free mass during weight loss to enhance metabolic rate (49,50).During the weight maintenance phase, higher levels of physical ac-tivity of 200–300 minutes per week are recommended (51).
Behavioral therapy targets maladaptive eating behaviors, ac-tivity, and thinking habits that contribute to obesity. It includesseveral components. Self-monitoring is perhaps the most im-portant component of behavioral therapy. Patients are advised torecord the type, amount, and total calories of their food con-sumption, and physical activity and body weight. Studies showthat individuals that routinely record their food intake lose moreweight than those who do not (52). Other components of be-havioral therapy include (i) stimulus control (such as storing foodout of sight, limiting eating places to the kitchen and dining table,and refraining from eating while engaging in other activities), (ii)problem solving (such as planning meals ahead of time whiletraveling), (iii) cognitive restructuring (such as recognizing asetback as a temporary lapse and continuing to move forwardinstead of giving up), and (iv) relapse prevention focusing onhigh-risk situations (such as vacations, illness, or periods of highstress). Traditionally, behavioral therapy is offered in group ses-sions of 10–20 individuals by registered dietitians, psychologists,exercise specialists, or other health professionals, with each ses-sion lasting 60–90 minutes. It is often held weekly during theactive weight-loss phase (6 months) and may taper to biweeklyduring the weight-maintenance phase (53).
In clinical practice, LM is usually prescribed comprehensivelyto modify both eating and activity habits. To date, there are 2landmark studies evaluating the efficacy of LM: the DiabetesPrevention Program and Look AHEAD studies (54). The Di-abetes Prevention Program study compared LM (16 sessionsduring the first 6 months, followed by monthly contacts) withmetformin with placebo at delaying or preventing developmentof type 2 diabetes (T2DM) in 3,200 patients with impaired glucosetolerance. At 1 year, LM patients lost 7 kg compared with 0.1 kgfor placebo. The risk of developing T2DMwas reduced by 58% inthe LM group compared with placebo and 31% compared withmetformin. At 10 years, participants regained almost all of theirlost weight (with no differences in weight loss among groups).Nevertheless, the incidence of T2DM remained the lowest in theLMgroup (55). In comparison, the LookAHEADstudy evaluatedthe effect of intensive lifestyle intervention (ILI) (24 sessionsduring the first 6 months, followed by 18 sessions in months7–12) vs usual care (diabetes support and education) in 5,100overweight participants with T2DM. At 1 and 4 years, patients inthe ILI and diabetes support and education experienced 8.6% vs0.7% TWL and 4.7% vs 1.1% TWL, respectively. The ILI groupT
able
5.(con
tinue
d)
Medications
Dosage/titration
Mechanismsofaction
Efficacy
Contraindications
Commonsideeffects
FDAstatus
Topiramate(Top
amax)
25mgqp
m(startingdo
se)
Increase
by25
mg/wk
200mgbid(m
axdo
se)
GABAreceptor
mod
ulation
5.3kg
additiona
lweigh
tloss
compa
redto
placeb
o(102
)
Pregn
ancy
Recen
talcoh
oluse
Metab
olicacidosis
Drowsine
ss,p
aresthesia,
dizziness
Off-labe
lfor
obesity
App
rovedform
igraine,
seizures
Bup
ropion
SR(W
ellbutrin
)30
0mgqd
400mgqd
Reu
ptakeinhibitoro
f
dopa
minean
d
norepine
phrin
e
7.5%
–8.6%
TWLat
1yr
(103
)
Pregn
ancy
Seizuredisorder
Bulim
iaor
anorexia
Alcoh
olwith
draw
al
MAOIs(with
in14
d)
Heada
che,
nausea,
constip
ation,
dizziness
Off-labe
lfor
obesity
App
rovedford
epression,
smokingce
ssation
Semaglutid
e(Ozempic)
Oral:3mgqd
for3
0d;
then
7
mgqd
for3
0d;
then
14mg
qd(if
need
ed)
SC:0
.25mgqw
for4
wee
ks;
then
0.5mgqw
for4
wk;then
1mgqw
for4
wk;then
1.7mg
qwfor4
wk;
then
2.4mgqw
GLP
-1agon
ist
6%–14
.9%
TWLat1yr(104
)Pregn
ancy
Persona
lorfam
ilyhistoryof
med
ullary
thyroid
Carcino
maor
multip
le
Endo
crinene
oplasia
Synd
rometype
2
Nau
sea,
vomiting
,
abdo
minalpa
in,inc
reased
lipasean
dam
ylase
Off-labe
lfor
obesity
App
rovedforT
2DM
CVD
,cardiovascu
lard
isease;ER,exten
dedrelease;GABA,gam
ma-am
inob
utyricacid;gen
,gen
eric;G
LP-1,glucagon-likepe
ptide-1;HTN
,hypertension;ITT,intention-to-treat;M
AOI,mon
oamineoxidaseinhibitors;O
TC,over-the-
coun
ter;SC
:sub
cutane
ous;SN
RI,serotonin-no
repine
phrin
ereup
take
inhibitor;SR
,sustained
release;
SSRI,selectiveserotoninreup
take
inhibitor;T2
DM,type2diab
etes
mellitus;T
WL,
totalw
eigh
tloss.
The American Journal of GASTROENTEROLOGY VOLUME 116 | MAY 2021 www.amjgastro.com
REV
IEW
ARTICLE
Jirapinyo and Thompson926
Copyright © 2021 by The American College of Gastroenterology. Unauthorized reproduction of this article is prohibited.

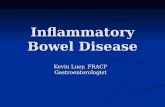
Figure 1. Primary bariatric endoscopic interventions. BMI, body mass index; GI, gastrointestinal; ITT, Intention-to-treat; TWL, total weight loss.
© 2021 by The American College of Gastroenterology The American Journal of GASTROENTEROLOGY
REV
IEW
ARTICLE
Obesity Primer 927
Copyright © 2021 by The American College of Gastroenterology. Unauthorized reproduction of this article is prohibited.

also experienced significantly greater improvement in HbA1cand several measures of cardiovascular diseases (56,57).
Overall, a comprehensive LM program should be in-corporated as part of every weight loss intervention. LM alonemay result in weight loss ranging from 1.4% to 8.6% TWLdepending on the intensity (56,58,59). Key components to successinclude a diet plan that patients can adhere to, incorporation ofphysical activity, and a behavioral treatment plan to reinforce thenecessary strategies to maintain the lost weight.
Pharmacotherapy
Weight-loss medications may be considered when patients failto respond to lifestyle modification and have a BMI of $30 or$27 kg/m2 with obesity-related comorbidities (8,60). Beforeinitiation of a weight-loss medication, current medicationsshould be reviewed to identify any that are associated withweight gain and should be substituted withmore weight-neutralmedications (Table 2). To date, there are 5 antiobesity medi-cations approved by the Food and Drug Administration
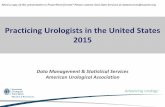
Figure 2. Bariatric surgeries. Outcome data from meta-analyses or largest available series. DI, duodeno-ileal; EWL, excess weight loss; GEJ, gastro-esophageal junction; GJA, gastrojejunal; ICV, ileocecal valve; II, ileoileal; JJA, jejunojejunal; PE, pulmonary embolism; SBO, small bowel obstruction; TWL,total weight loss.
The American Journal of GASTROENTEROLOGY VOLUME 116 | MAY 2021 www.amjgastro.com
REV
IEW
ARTICLE
Jirapinyo and Thompson928
Copyright © 2021 by The American College of Gastroenterology. Unauthorized reproduction of this article is prohibited.

Table 6. Complications of common bariatric surgeries
Complications
Time of onset since
surgery Diagnostic modalities Management strategies
Sleeve gastrectomy
Sleeve leaks Post-operative or early Cross-sectional imaging Depends on time from surgery
Esophageal stent for acute leaks
Pigtail stents for chronic leaks
Sleeve stenosis Anytime Distinguish between stenosis and twisting;
consider imaging
Hydrostatic or pneumatic balloon dilation of sleeve
depending on time from surgery and degree of stenosis
Twisted sleeve less likely to respond
Reflux and its
complications
Late Upper endoscopy High dose PPI 1/2 sucralfate for acid reflux
Cholestyramine for bile reflux
Surgical conversion to RYGB
Roux-en-Y gastric bypass
Surgical leaks Post-operative or early Cross-sectional imaging
High false negative rates for all studies
Depends on location of leak and time from surgery
Esophageal stents for acute pouch and GJ leaks
Clips for JJ leaks
Pigtail drainage for chronic walled-off leaks
GJA ulceration Early or late Do not advance endoscope deeply beyond
area of ulceration
Helicobacter pylori stool antigen or
serology
High dose PPI (soluble form) 1/2 sucralfate
Treat H. pylori if positive
Stop smoking and optimize glycemic control
Stop NSAIDs
Consider suture removal
GJA stenosis Late Upper endoscopy
Avoid UGI series given aspiration risk
Look for concomitant ulceration
Stepwise endoscopic balloon dilation
Do not overdilate (#15 mm)
Carefully direct wire into Roux limb
Foreign body removal
Consider LAMS for selected cases
Gastrogastric fistula Early or late Upper GI series sensitive
Upper endoscopy important to confirm
and rule out ulceration
If asymptomatic, PPI 1 dietary counseling
If symptomatic, closure (endoscopic [,1 cm] vs surgical)
Intestinal obstruction Early or late Cross-sectional imaging while
symptomatic to look for intussusception
and internal herniation
Surgery
Endoscopy is not indicated for extraluminal causes of
obstruction
Choledocholithiasis Late RUQ ultrasound
Cross-sectional imaging
MRCP
Device-assisted enteroscopy
Laparoscopic-assisted ERCP
EUS-directed ERCP
IR-guided percutaneous drainage
Dilated GJA Late Upper endoscopy
Dilation confirmed with GJA .15 mm
Endoscopic revision (TORe)
APC for incompetent yet not
markedly dilated GJA
Laparoscopic adjustable gastric band
Reflux esophagitis Late Upper endoscopy High dose PPI 1/2 sucralfate
Band deflation
Esophageal dilatation Late Upper endoscopy
Upper GI series
Band deflation
Surgical replacement or conversion
Band erosion Late Upper endoscopy Endoscopic removal of band if buckle is visible with
surgical removal of port
Band slippage Late Upper GI series Surgery
APC, argon plasmacoagulation; ERCP, endoscopic retrograde cholangiopancreatography; EUS, endoscopic ultrasound;GJ, gastrojejunal; GJA, gastrojejunal anastomosis;IR, interventional radiology; JJ, jejunojejunal; LAMS, lumen-apposing metal stent; MRCP, magnetic resonance cholangiopancreatography; PPI, proton pump inhibitor;RUQ, right upper quadrant; TORe, transoral outlet reduction.
© 2021 by The American College of Gastroenterology The American Journal of GASTROENTEROLOGY
REV
IEW
ARTICLE
Obesity Primer 929
Copyright © 2021 by The American College of Gastroenterology. Unauthorized reproduction of this article is prohibited.

(FDA)—phentermine, orlistat (Xenical), phentermine/topiramate (Qsymia), naltrexone/bupropion (Contrave), andliraglutide (Saxenda) (Table 5). With the exception of orlistat,which blocks absorption of 25%–30% of fat calories, thesemedications target appetite mechanisms specifically by workingin the arcuate nucleus to stimulate pro-opiomelanocortin neu-rons to promote satiety. It is important to discuss both potentialbenefits and adverse events of each medication before its initi-ation and to document the conversation, especially when themedication is used off-label. Furthermore, pregnancy is con-traindicated for all weight-lossmedications, and patients shouldbe advised to use dual contraceptive methods.
Although there is no generalizable hierarchical algorithm formedication selection, specificmedications are preferred in certainclinical settings based on efficacy, adverse events, warnings,contraindications, organ clearance, and mechanisms of action(61). For example, phentermine/topiramate should be consideredin patients with migraine, bupropion/naltrexone for those withsmoking or depression history, and liraglutide for those withdiabetes/prediabetes. In addition, certain medications should beavoided in patients with specific comorbidities. For example,patients with uncontrolled hypertension or a history of heartdisease should not be prescribed phentermine. Patients with anelevated seizure risk should avoid bupropion/naltrexone.
An effective response is defined as $5% TWL at 3 monthsafter the initiation of a weight-loss medication. If the response isdeemed ineffective (,5% TWL at 3 months) or if safety or in-tolerability issue arises, the medication should be discontinuedand switched to an alternative medication or treatment ap-proach (26).
Gelesis100 is a procedureless intervention that was FDA-approved based on pharmacotherapy thresholds and represents anew class of obesity treatments. It is a hydrogel capsule that isorally administered with water before a meal. When hydrated,Gelesis100 occupies about one-fourth of the gastric volume. Theparticles maintain their gel form while passing through the smallintestine before breaking down in the colon. A pivotal trial(GLOW trial) randomized 436 patients to Gelesis100 vs placebo.At 6 months, the Gelesis100 group experienced 6.4% TWL (vs4.4%TWL for placebo), with 59% achieving$5%TWL (62). Thistechnology is not yet commercially available.
In addition to the medications listed above, there are severalantiobesity agents under development and currently undergoingclinical trial. For a newdrug to be approved forweight loss, itmustmeet the FDA thresholds, defined as significant placebo-adjustedweight loss of$5% TWL at 1 year or$35% of patients achieving$5%TWL (whichmust be at least twice that induced by placebo).
Bariatric Endoscopy
Bariatric endoscopy may be divided into gastric and small bowelinterventions (63,64). In general, gastric interventions primarilyinduce weight loss with secondary effects on metabolic condi-tions. By contrast, small bowel interventions have direct effects onmetabolic conditions with or without weight loss. To date, thereare 3 types of bariatric endoscopic devices that are FDA-approvedand available (Figure 1).
Intragastric balloons occupy space in the stomach and seem toalter gastric motility (65). There currently are 2 IGBs available intheUnited States—Orbera (Apollo Endosurgery, Austin, TX) andObalon (Obalon Therapeutics, Carlsbad, CA). Orbera is a singlefluid-filled balloon that is placed and removed endoscopically at 6
months. Obalon is a 3-balloon system, filled with nitrogen gas,swallowed 4 weeks apart, with positioning confirmed via x-ray ormagnetic resonance. All balloons are removed endoscopically at 6months. An Orbera meta-analysis (17 studies/1,638 patients)demonstrated an 11.3% TWL at 12 months. The most commonAEs were pain and nausea (33.7%). The severe adverse event(SAE) rate was 1.6%, including migration (1.4%), perforation(0.1%), and death (0.08%) (66). For Obalon, a randomized sham-controlled trial revealed a 6.9% TWL at 12 months with an SAErate of 0.4% (67). However, the real-world experience (1,343patients) showed a 10%TWLwith an SAE rate of 0.15% includingsevere abdominal pain and gastric perforation (68).
Gastric remodeling may be performed via endoscopic sutur-ing or plication and dates back to as early as 2008 (69–71). Cur-rently, there are 2 devices that are cleared by the FDA for tissueapproximation and are used for this purpose, however, withoutspecific weight loss claims—Overstitch (Apollo Endosurgery)and Incisionless Operating Platform (USGI Medical, San Clem-ente, CA). Endoscopic sleeve gastroplasty is the most commongastric remodeling procedure that involves placing several su-tures in a running fashion along the greater curvature. A secondlayer of sutures may also be placed medially for reinforcement(72). A meta-analysis (8 studies/1772 patients) revealed its effi-cacy to be 16.5% TWL at 12 months and an SAE rate of 2.2%including pain/nausea, bleeding, perigastric leak, and fluid col-lection (73). At 5 years, a single center study (56 of 68 patientswho were eligible for the 5-year follow-up from the original co-hort of 216 patients) revealed a 15.9% TWL (compared with15.6% at 1 year) (74). In comparison, gastric plication, also knownas Primary Obesity Surgery Endoluminal (POSE), involvesplacement of tissue plications in the stomach. In contrast to en-doscopic sleeve gastroplasty which may be endoscopically re-versible, POSE focuses on serosal apposition and is not reversible.The traditional POSE procedure involves placement of plicationsprimarily in the fundus (75). A more recent pattern, also knownas distal POSE or POSE2, however, involves placement of plica-tions solely in the gastric body (76–78). A meta-analysis (5studies/586 patients) demonstrated that traditional POSE wasassociated with 12.1% and 13.2% TWL at 6 and 12–15 months,respectively, with an SAE rate of 3.2% including chest pain, low-grade fever, extragastric bleeding, and hepatic abscess (79). Withthe new plication pattern, the efficacy seemed to be higher withapproximately 15% and 17.5% TWL at 6 and 9 months, re-spectively (76–78,80). Preliminary results suggest that patientswith class III obesity may experience greater weight loss (19-20%TWL at 1 year) following ESG or distal POSE compared to thosewith class I and II (80,81).
Aspiration therapy removes a portion of food from thestomach after ingestion. The system consists of a large fenestratedgastrostomy tube (A-tube), an external port at the skin for aspi-ration, and a portable device to perform aspiration. The A-tube isplaced endoscopically via a standard pull technique, and the portis attached at 1–2 weeks. Ameta-analysis (5 studies/590 patients)demonstrated a 17.8% TWL at 1 year with an SAE rate of 4.1%including buried bumper, peritonitis, abdominal pain, andproduct malfunction (82).
In addition to weight loss efficacy, all of the approved gastricdevices and/or procedures discussed above have been shown toimprove obesity-related comorbidities, such as diabetes and fattyliver (82–86). The effect of endoscopic bariatric procedures onconception, however, remains unknown.
The American Journal of GASTROENTEROLOGY VOLUME 116 | MAY 2021 www.amjgastro.com
REV
IEW
ARTICLE
Jirapinyo and Thompson930
Copyright © 2021 by The American College of Gastroenterology. Unauthorized reproduction of this article is prohibited.

Other gastric devices including the Spatz and Elipse balloonsystems are currently undergoing FDA review, whereas somesmall bowel interventions such as duodenal-jejunal bypass linerand duodenal mucosal resurfacing are undergoing US clinicaltrials. According to the ASGE/ASMBS, a new endoscopic pro-cedure intended as a primary obesity intervention should achieve$25% excess weight loss (EWL) at 1 year with aminimumof 15%EWL over control with an SAE rate ,5% (87).
Bariatric surgery
Bariatric surgery should be considered for patients with a BMI of$40 or $35 kg/m2 with at least 1 comorbidity (88). Althoughseveral bariatric surgical procedures are available (Figure 2), SGand RYGB remain the most commonly performed.
SG involves removal of the fundus and greater curvature tocreate a tubular structure along the lesser curvature. The smallbowel remains unaltered. A meta-analysis (11 studies/over 3,000patients) revealed that patients experienced 51.5% EWL at 1 year.The pooled mortality rate was 0.6% with an AE rate of 8.9% andreoperation rate of 3% (89). In a single center study, 51 of theoriginal cohort of 165 patients experienced 60.5% EWL at 5 years(compared with 82% EWL at 1 year) (90).
RYGB is the preferred surgery for patients with obesity andconcomitant metabolic diseases or gastroesophageal reflux dis-ease.DuringRYGB, the stomach is divided into a small pouch anda larger remnant stomach. The jejunum is transected, followed byconnecting one end to the pouch at the gastrojejunal anastomosisand the other end to the proximal jejunum at the jejunojejunalanastomosis. A meta-analysis (17 studies/over 8,000 patients)revealed that patients experienced 63.3% EWL at 1 year afterRYGB.The pooledmortality ratewas 1.1%with anAE rate of 12%and reoperation rate of 5.3% (89). At 12 years, the average weightloss is 27% TWL (n5 387) (91).
In addition to SG and RYGB, other procedures that are stillbeing performed at a smaller proportion include gastric bandingand biliopancreatic diversion with duodenal switch. Further-more, there are several emerging procedures, such as minigastricbypass and single anastomosis duodenoileal bypass with sleevegastrectomy, which gastroenterologists should become familiarwith (Figure 2).
ENDOSCOPIC MANAGEMENT OF BARIATRICSURGICAL COMPLICATIONSAs the number of bariatric surgeries continues to rise, gastroen-terologists will see more patients with surgically altered anatomy.In addition to understanding normal and abnormal endoscopicfindings in this patient population (see above), gastroenterolo-gists should be familiar with potential complications and theirmanagement. Table 6 summarizes complications after each of thecommon bariatric surgeries, presenting symptoms, and man-agement strategies (92). Furthermore, nutrient deficiencies maybe seen after all bariatric surgeries, such as vitamins B1/B12, D, A,folate, iron, and calcium, with the addition of zinc and copper forbiliopancreatic diversion with duodenal switch and RYGB(93,94). Therefore, adherence to vitamin supplements should beassessed with a low threshold to check these levels, especially forthose who are not routinely followed by bariatric surgery. Inaddition, weight regain after bariatric surgery is not uncommonand is likely caused by several etiologies including medical, be-havioral, hormonal, pharmacologic, and anatomical factors.
Gastroenterologists should routinely ask for prebariatric surgical,nadir, and current weights. If weight regain is encountered, re-ferral to a multidisciplinary team, including dietitian, obesitymedicine expert, bariatric endoscopist, and bariatric surgeon, forconsideration of pharmacotherapy and/or endoscopic revision ofbariatric surgery is recommended. There are several effectiveendoscopic treatment options for weight regain; however, this isbeyond the scope of this article.
DEVELOPING EXPERTISE IN OBESITY MEDICINE ANDBARIATRIC ENDOSCOPYThere are several resources available for gastroenterologists whoplan on specializing inObesityMedicine andBariatric Endoscopy(95). These programs focus on cognitive elements, skill set de-velopment, and center requirements. American Board of ObesityMedicine credentialing is also available for board-certified gas-troenterologists without the need for additional training.
From a center standpoint, there are also several infrastructureand personnel considerations. These include having a patient-friendly waiting area (such as wide chairs and reinforced toilets)and medical equipment (such as extra-large blood pressure cuffsand bariatric scales). Staff training to reduce bias and stigma andto encourage the use of people-first language and terms such asunhealthy weight rather obese is also encouraged. Furthermore, amultidisciplinary team, which includes bariatric surgeons, bari-atric endoscopists, obesity medicine experts, dietitians, psychol-ogists, health coaches, and/or social workers, is essential and canbe assembled with the help of modern virtual platforms. In ad-dition, these platforms may be used as part of the aftercare pro-gram. Moreover, fitness applications and calorie tracking devicesmay be useful to encourage adherence to LM.
CONCLUSIONGastroenterologists will continue to see an increasing number ofpatients with obesity. These patients are at greater risk of GIcomorbidities and require special consideration. Similarly, bari-atric surgery carries various complications that necessitate uniquemanagement strategies. Finally, gastroenterologists are well po-sitioned to manage obesity medically and endoscopically andshould adopt a greater role in addressing this pandemic.
CONFLICTS OF INTEREST
Guarantor of the article: Christopher C. Thompson, MD, MSc.Specific author contributions: P.J.: wrote the manuscript. C.C.T.:critically reviewed the article for important intellectual content. Allauthors approved the final draft of the article.Financial support: NIH T32 DK007533 and P30 DK034854.Potential competing interests: P.J. has received research supportfrom Apollo Endosurgery - Research Support, Boston Scientific -Research Support, Endogastric Solutions - Consultant, Fractyl -Research Support, GI Dynamics - Consultant (Consulting fees),Research Support, Lumendi - Consultant. C.C. Thompson: ApolloEndosurgery - Consultant/Research Support (Consulting fees/Institutional Research Grants), Aspire Bariatrics - Research Support(Institutional Research Grant), BlueFlame Healthcare Venture Fund- General Partner, Boston Scientific - Consultant (Consulting fees)/Research Support (Institutional Research Grant), Covidien/Medtronic - Consultant (Consulting fees), EnVision Endoscopy -Board Member, ERBE - Institutional Research Grant, Fractyl -Consultant/Advisory Board Members (Consulting fees), FujiFilm -Institutional Research Grant, GI Dynamics - Consultant (Consulting
© 2021 by The American College of Gastroenterology The American Journal of GASTROENTEROLOGY
REV
IEW
ARTICLE
Obesity Primer 931
Copyright © 2021 by The American College of Gastroenterology. Unauthorized reproduction of this article is prohibited.

fees)/Resaerch Support (Institutional Research Grant), GI Windows- Ownership Interest, Lumendi - Consultant/Institutional ResearchGrant, Olympus/Spiration - Consultant (Consulting fees)/ResearchSupport (Equipment Loans), USGI Medical - Consultant(Consulting fees)/Advisory Board Member (Consulting fees)/Research Support (Institutional Research Grant)
REFERENCES1. Obesity and overweight. (https://www.who.int/news-room/fact-sheets/
detail/obesity-and-overweight). Accessed March 9, 2020.2. Hales CM, Carroll MD, Fryar CD, et al. Prevalence of obesity among
adults and youth: United States, 2015–2016. NCHSData Brief 2017:1–8.3. Kyle TK, Dhurandhar EJ, Allison DB. Regarding obesity as a disease:
Evolving policies and their implications. Endocrinol Metab Clin NorthAm 2016;45:511–20.
4. Definition of Obesity. Obesity Medicine Association: Centennial, CO,2017. (https://obesitymedicine.org/definition-of-obesity/). AccessedMarch 9, 2020.
5. Defining Adult Overweight and Obesity | Overweight & Obesity. CDC:Geneva, Switzerland, 2020. (https://www.cdc.gov/obesity/adult/defining.html). Accessed October 18, 2020.
6. Body Mass Index: Considerations for Practitioners. CDC: Geneva,Switzerland, 2011, pp 4.
7. Obesity Education Initiative Electronic Textbook: TreatmentGuidelines. (https://www.nhlbi.nih.gov/health-pro/guidelines/current/obesity-guidelines/e_textbook/txgd/4142.htm). Accessed March 9,2020.
8. Jensen MD, Ryan DH, Apovian CM, et al. 2013 AHA/ACC/TOSguideline for the management of overweight and obesity in adults: Areport of the American College of Cardiology/American HeartAssociation Task Force on Practice Guidelines and the Obesity Society.Circulation 2014;129:S102–38.
9. Amato MC, Guarnotta V, Giordano C. Body composition assessmentfor the definition of cardiometabolic risk. J Endocrinol Invest 2013;36:537–43.
10. Gallagher D, Heymsfield SB, Heo M, et al. Healthy percentage body fatranges: An approach for developing guidelines based on body massindex. Am J Clin Nutr 2000;72:694–701.
11. Dickey RA, Bartuska DG, Bray GW, et al. AACE/ACE PositionStatement on the Prevention, Diagnosis, and Treatment of Obesity(1998 Revision). Endocrine Practice. 1998;4(5):297–349.
12. Regional Office for the Western Pacific. The Asia-Pacific Perspective:Redefining Obesity and Its Treatment. Health CommunicationsAustralia: Sydney, Australia, 2000. (https://apps.who.int/iris/handle/10665/206936). Accessed October 19, 2020.
13. AlammarM, Alsoghayer S, El-Abd K, et al. Diagnostic accuracy of bodymass index (BMI) when diagnosing obesity in a Saudi adult populationin a primary care setting, cross sectional, retrospective study. DiabetesMetab Syndr Obes 2020;13:2515–20.
14. Camilleri M, Malhi H, Acosta A. Gastrointestinal complications ofobesity. Gastroenterology 2017;152:1656–70.
15. Delgado-Aros S, Cremonini F, Castillo JE, et al. Independent influencesof body mass and gastric volumes on satiation in humans.Gastroenterology 2004;126:432–40.
16. Wijarnpreecha K, Werlang ME, Watthanasuntorn K, et al. Obesity andrisk of small intestine bacterial overgrowth: A systematic review andmeta-analysis. Dig Dis Sci 2020;65:1414–22.
17. Eslick GD. Gastrointestinal symptoms and obesity: A meta-analysis.Obes Rev 2012;13:469–79.
18. El-Serag H. The association between obesity and GERD: A review of theepidemiological evidence. Dig Dis Sci 2008;53:2307–12.
19. Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis andmanagement of nonalcoholic fatty liver disease: Practice guidance fromthe American Association for the Study of Liver Diseases. Hepatology2018;67:328–57.
20. Berzigotti A, Albillos A, Villanueva C, et al. Effects of an intensivelifestyle intervention program on portal hypertension in patients withcirrhosis and obesity: The SportDiet study. Hepatology 2017;65:1293–305.
21. Vilar-Gomez E,Martinez-Perez Y, Calzadilla-Bertot L, et al.Weight lossthrough lifestyle modification significantly reduces features of
nonalcoholic steatohepatitis. Gastroenterology 2015;149:367–78.e5;quiz e14–5.
22. Prochaska JO, DiClemente CC, Norcross JC. In search of how peoplechange. Applications to addictive behaviors. Am Psychol 1992;47:1102–14.
23. Prochaska JO, Velicer WF. The transtheoretical model of healthbehavior change. Am J Health Promot 1997;12:38–48.
24. Alexander SC,CoxME,BolingTurerCL, et al. Do thefiveA’sworkwhenphysicians counsel about weight loss? Fam Med 2011;43:179–84.
25. Barnes RD, Ivezaj V. A systematic review of motivational interviewingfor weight loss among adults in primary care. Obes Rev 2015;16:304–18.
26. Apovian CM, Aronne LJ, Bessesen DH, et al. Pharmacologicalmanagement of obesity: An endocrine society clinical practice guideline.J Clin Endocrinol Metab 2015;100:342–62.
27. Wharton S, Raiber L, Serodio KJ, et al. Medications that cause weightgain and alternatives in Canada: A narrative review. Diabetes MetabSyndr Obes 2018;11:427–38.
28. Davies RJ, Stradling JR. The relationship between neck circumference,radiographic pharyngeal anatomy, and the obstructive sleep apnoeasyndrome. Eur Respir J 1990;3:509–14.
29. Glickman N, Mitchell HH. The total specific dynamic action of high-protein and high-carbohydrate diets on human subjects. J Nutr 1948;36:41–57.
30. Halton TL, Hu FB. The effects of high protein diets on thermogenesis,satiety andweight loss: A critical review. JAmCollNutr 2004;23:373–85.
31. Call C, Walsh BT, Attia E. From DSM-IV to DSM-5: Changes to eatingdisorder diagnoses. Curr Opin Psychiatry 2013;26:532–6.
32. Cooper Z, Fairburn C. Eating Disorder Examination. 2011. (http://doi.apa.org/getdoi.cfm?doi510.1037/t03975-000). Accessed May 24, 2020.
33. Fairburn CG, Beglin SJ. Assessment of eating disorders: Interview orself-report questionnaire? Int J Eat Disord 1994;16:363–70.
34. Brown WA, Johari Halim Shah Y, Balalis G, et al. IFSO positionstatement on the role of esophago-gastro-duodenal endoscopy prior toand after bariatric andmetabolic surgery procedures.Obes Surg 2020;30:3135–53.
35. Qumseya BJ, Qumsiyeh Y, Ponniah S, et al. Barrett’s esophagus aftersleeve gastrectomy: A systematic review andmeta-analysis. GastrointestEndosc 2020;93:343–52.e2.
36. 2015–2020 Dietary Guidelines|health.gov. (https://health.gov/our-work/food-nutrition/2015-2020-dietary-guidelines). Accessed March14, 2020.
37. Last AR, Wilson SA. Low-carbohydrate diets. Am Fam Physician 2006;73:1942–8.
38. Westerterp-Plantenga MS. How are normal, high- or low-protein dietsdefined? Br J Nutr 2007;97:217–8.
39. Longe JL (ed). The Gale Encyclopedia of Diets: A Guide to Health andNutrition. 1st edn. Gale: Detroit, the Netherlands, 2007.
40. Lichtenstein AH, Horn LV. Very Low Fat Diets. CDC: Geneva,Switzerland, 2011, pp 5.
41. Sacks FM, BrayGA,CareyVJ, et al. Comparisonofweight-loss dietswithdifferent compositions of fat, protein, and carbohydrates. N Engl J Med2009;360:859–73.
42. HuT,MillsKT, YaoL, et al. Effects of low-carbohydrate diets versus low-fat diets on metabolic risk factors: A meta-analysis of randomizedcontrolled clinical trials. Am J Epidemiol 2012;176(Suppl 7):S44–54.
43. Foster GD, Wyatt HR, Hill JO, et al. A randomized trial of a low-carbohydrate diet for obesity. N Engl J Med 2003;348:2082–90.
44. Foster GD, Wyatt HR, Hill JO, et al. Weight and metabolic outcomesafter 2 years on a low-carbohydrate versus low-fat diet: A randomizedtrial. Ann Intern Med 2010;153:147–57.
45. Stern L, Iqbal N, Seshadri P, et al. The effects of low-carbohydrate versusconventional weight loss diets in severely obese adults: One-year follow-up of a randomized trial. Ann Intern Med 2004;140:778–85.
46. Dansinger ML, Gleason JA, Griffith JL, et al. Comparison of the Atkins,Ornish, Weight Watchers, and Zone diets for weight loss and heartdisease risk reduction: A randomized trial. JAMA 2005;293:43–53.
47. Physical Activity for a HealthyWeight | HealthyWeight, Nutrition, andPhysical Activity. CDC: Geneva, Switzerland, 2019. (https://www.cdc.gov/healthyweight/physical_activity/index.html). Accessed October 19,2020.
48. American College of Sports Medicine Position Stand. Therecommended quantity and quality of exercise for developing andmaintaining cardiorespiratory and muscular fitness, and flexibility inhealthy adults. Med Sci Sports Exerc 1998;30:975–91.
The American Journal of GASTROENTEROLOGY VOLUME 116 | MAY 2021 www.amjgastro.com
REV
IEW
ARTICLE
Jirapinyo and Thompson932
Copyright © 2021 by The American College of Gastroenterology. Unauthorized reproduction of this article is prohibited.

49. Braith RW, Stewart KJ. Resistance exercise training: Its role in theprevention of cardiovascular disease. Circulation 2006;113:2642–50.
50. Williams MA, Haskell WL, Ades PA, et al. Resistance exercise inindividuals with and without cardiovascular disease: 2007 update: Ascientific statement from the American Heart Association Council onClinical Cardiology and Council on Nutrition, Physical Activity, andMetabolism. Circulation 2007;116:572–84.
51. Wadden TA, Neiberg RH,Wing RR, et al. Four-year weight losses in theLook AHEAD study: Factors associated with long-term success. Obesity(Silver Spring) 2011;19:1987–98.
52. Boutelle KN, Kirschenbaum DS. Further support for consistent self-monitoring as a vital component of successful weight control. Obes Res1998;6:219–24.
53. Wadden TA, Bray GA. Handbook of Obesity Treatment, 2nd edn.Guilford Publications: New York, 2018.
54. Apovian CM, Aronne L, Powell AG. Clinical Management of Obesity.Professional Communications: San Juan, PR, 2015.
55. Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in theincidence of type 2 diabetes with lifestyle intervention or metformin. NEngl J Med 2002;346:393–403.
56. Look AHEAD Research Group, Pi-Sunyer X, Blackburn G, et al.Reduction in weight and cardiovascular disease risk factors inindividuals with type 2 diabetes: One-year results of the look AHEADtrial. Diabetes Care 2007;30:1374–83.
57. LookAHEADResearchGroup,WingRR. Long-term effects of a lifestyleintervention on weight and cardiovascular risk factors in individualswith type 2 diabetesmellitus: Four-year results of the look AHEAD trial.Arch Intern Med 2010;170:1566–75.
58. Wadden TA, Webb VL, Moran CH, et al. Lifestyle modification forobesity: New developments in diet, physical activity, and behaviortherapy. Circulation 2012;125:1157–70.
59. Dixon JB, O’Brien PE, Playfair J, et al. Adjustable gastric banding andconventional therapy for type 2 diabetes: A randomized controlled trial.JAMA 2008;299:316–23.
60. Igel LI, Kumar RB, Saunders KH, et al. Practical use of pharmacotherapyfor obesity. Gastroenterology 2017;152:1765–79.
61. Garvey WT, Mechanick JI, Brett EM, et al. American Association ofClinical Endocrinologists and American College of Endocrinologycomprehensive clinical practice guidelines for medical care of patientswith obesity. Endocr Pract 2016;22(Suppl 3):1–203.
62. Greenway FL, Aronne LJ, Raben A, et al. A randomized, double-blind,placebo-controlled study of Gelesis100: A novel nonsystemic oralhydrogel for weight loss. Obesity (Silver Spring) 2019;27:205–16.
63. Sullivan S, Edmundowicz SA, Thompson CC. Endoscopic bariatric andmetabolic therapies: New and emerging technologies. Gastroenterology2017;152:1791–801.
64. Jirapinyo P, Thompson CC. Endoscopic bariatric and metabolictherapies: Surgical analogues and mechanisms of action. ClinGastroenterol Hepatol 2017;15:619–30.
65. Gomez V,WoodmanG, Abu Dayyeh BK. Delayed gastric emptying as aproposed mechanism of action during intragastric balloon therapy:Results of a prospective study. Obesity (Silver Spring) 2016;24:1849–53.
66. ASGE Bariatric Endoscopy Task Force and ASGE TechnologyCommittee, AbuDayyehBK, KumarN, et al. ASGEBariatric EndoscopyTask Force systematic review and meta-analysis assessing the ASGEPIVI thresholds for adopting endoscopic bariatric therapies.Gastrointest Endosc 2015;82:425–38.e5.
67. Sullivan S, Swain J, Woodman G, et al. Randomized sham-controlledtrial of the 6-month swallowable gas-filled intragastric balloon systemfor weight loss. Surg Obes Relat Dis 2018;14:1876–89.
68. Moore RL, Seger MV, Garber SM, et al. Clinical safety and effectivenessof a swallowable gas-filled intragastric balloon system for weight loss:Consecutively treated patients in the initial year of U.S.commercialization. Surg Obes Relat Dis 2019;15:417–23.
69. Brethauer SA, Chand B, Schauer P, Thompson CC. V-04: Transoralgastric volume reduction as an intervention for weight management(TRIM trial). Surg Obes Relat Dis 2009;5:S59.
70. Brethauer SA, Chand B, Schauer PR, Thompson CC. Transoral gastricvolume reduction as intervention for weight management: 12-monthfollow-up of TRIM trial. Surg Obes Relat Dis 2012;8:296–303.
71. Espinos JC, Turro R,Mata A, et al. Early experience with the IncisionlessOperating Platform (IOP) for the treatment of obesity. Obes Surg 2013;23:1375–83.
72. Kumar N, Abu Dayyeh BK, Lopez-Nava Breviere G, et al. Endoscopicsutured gastroplasty: Procedure evolution from first-in-man casesthrough current technique. Surg Endosc 2018;32:2159–64.
73. Hedjoudje A, Dayyeh BA, Cheskin LJ, et al. Efficacy and safety ofendoscopic sleeve gastroplasty: A systematic review and meta-analysis.Clin Gastroenterol Hepatol 2020;18:1043–53.e4.
74. Sharaiha RZ, Hajifathalian K, Kumar R, et al. Five-year outcomes ofendoscopic sleeve gastroplasty for the treatment of obesity. ClinGastroenterol Hepatol 2020 October 1 [Epub ahead of print.]
75. Espinos JC, Turro R, Moragas G, et al. Gastrointestinal physiologicalchanges and their relationship to weight loss following the POSEprocedure. Obes Surg 2016;26:1081–9.
76. Jirapinyo P, Thompson CC. Gastric plications for weight loss: Distalprimary obesity surgery endoluminal through a belt-and-suspendersapproach. VideoGIE 2018;3:296–300.
77. Jirapinyo P, Thompson CC. Endoscopic gastric body plication for thetreatment of obesity: Technical success and safety of a novel technique(with video). Gastrointest Endosc 2020;91:1388–94.
78. Lopez-Nava G, Asokkumar R, Turro Arau R, et al. Modified primaryobesity surgery endoluminal (POSE-2) procedure for the treatment ofobesity. VideoGIE 2020;5:91–3.
79. Jirapinyo P, Runge TM, Thompson CC. Tu1905 endoscopic gastricplication for the treatment of obesity: A systematic review and meta-analysis. Gastrointest Endosc 2018;87:AB604–5.
80. Lopez Nava G, Asokkumar R, Laster J, et al. Primary obesity surgeryendoluminal (POSE-2) procedure for treatment of obesity in clinicalpractice. Endoscopy. 2020 Nov 27 [Epub ahead of print.]
81. Barrichello S, de Moura DTH, de Moura EGH, et al. Endoscopic sleevegastroplasty in the management of overweight and obesity: Aninternational multicenter study. Gastrointest Endosc. 2019;90(5):770–80.
82. Jirapinyo P, de Moura DTH, Horton LC, et al. Effect of aspirationtherapy on obesity-related comorbidities: Systematic review and meta-analysis. Clin Endosc 2020;53:686–97.
83. PopovVB,OuA, SchulmanAR, et al. The impact of intragastric balloonson obesity-related co-morbidities: A systematic review and meta-analysis. Am J Gastroenterol 2017;112:429–39.
84. PopovVB, ThompsonCC, KumarN, et al. Effect of intragastric balloonson liver enzymes: A systematic review and meta-analysis. Dig Dis Sci2016;61:2477–87.
85. Sharaiha RZ, Kumta NA, Saumoy M, et al. Endoscopic sleevegastroplasty significantly reduces body mass index and metaboliccomplications in obese patients. Clin Gastroenterol Hepatol 2017;15:504–10.
86. Hajifathalian K, Mehta A, Ang B, et al. Improvement in insulinresistance and estimated hepatic steatosis and fibrosis after endoscopicsleeve gastroplasty. Gastrointest Endosc 2020.
87. ASGE/ASMBS Task Force on Endoscopic Bariatric Therapy, GinsbergGG, Chand B, et al. A pathway to endoscopic bariatric therapies.Gastrointest Endosc 2011;74:943–53.
88. Who Is a Candidate for Bariatric Surgery?|Patients|ASMBS. AmericanSociety for Metabolic and Bariatric Surgery: Gainesville, FL. (https://asmbs.org/patients/who-is-a-candidate-for-bariatric-surgery).Accessed March 17, 2020.
89. Chang S-H, Stoll CRT, Song J, et al. The effectiveness and risks ofbariatric surgery: An updated systematic review and meta-analysis,2003–2012. JAMA Surg 2014;149:275–87.
90. Hoyuela C. Five-year outcomes of laparoscopic sleeve gastrectomy as aprimary procedure for morbid obesity: A prospective study. World JGastrointest Surg 2017;9:109–17.
91. Adams TD, Davidson LE, Litwin SE, et al. Weight and metabolicoutcomes 12 years after gastric bypass. N Engl J Med 2017;377:1143–55.
92. SchulmanAR, ThompsonCC. Complications of bariatric surgery:Whatyou can expect to see in your GI practice. Am J Gastroenterol 2017;112:1640–55.
93. Mechanick JI, Apovian C, Brethauer S, et al. Clinical practice guidelinesfor the perioperative nutrition, metabolic, and nonsurgical support ofpatients undergoing bariatric procedures: 2019 update: Cosponsored byAmericanAssociation of Clinical Endocrinologists/AmericanCollege ofEndocrinology, The Obesity Society, American Society for Metabolicand Bariatric Surgery, Obesity Medicine Association, and AmericanSociety of Anesthesiologists. Obesity (Silver Spring) 2020;28:O1–58.
94. Parrott J, Frank L, Rabena R, et al. American Society for Metabolic andBariatric Surgery Integrated Health Nutritional guidelines for the
© 2021 by The American College of Gastroenterology The American Journal of GASTROENTEROLOGY
REV
IEW
ARTICLE
Obesity Primer 933
Copyright © 2021 by The American College of Gastroenterology. Unauthorized reproduction of this article is prohibited.

surgical weight loss patient 2016 update: Micronutrients. Surg ObesRelat Dis 2017;13:727–41.
95. Jirapinyo P, Thompson CC. How to incorporate bariatric training intoyour fellowship program. Gastroenterology 2019;157:9–13.
96. Aronne LJ, Wadden TA, Peterson C, et al. Evaluation of phentermineand topiramate versus phentermine/topiramate extended-release inobese adults. Obesity. 2013;21(11):2163–71.
97. Torgerson JS, Hauptman J, Boldrin MN, et al. Subjects (XENDOS)study: A randomized study of orlistat as an adjunct of lifestyle changesfor the prevention of type 2 diabetes in obese patients. Diabetes Care.2004;27(1):155–61.
98. Gadde KM, Allison DB, Ryan DH, et al. Effects of low-dose, controlled-release, phentermine plus topiramate combination on weight andassociated comorbidities in overweight and obese adults (CONQUER):A randomized, placebo-controlled, phase 3 trial. Lancet. 2011;1341–52.
99. Greenway FL, Fujioka K, Plodkowski RA, et al; COR-I Study Group.Effect of naltrexone plus bupropion on weight loss in overweight andobese adults (COR-I): A multicenter, randomized, double-blind,placebo-controlled, phase 3 trial. Lancet. 2010;376(9741):595–605.
100. Pi-SunyerX,AstrupA,FujiokaK, et al.A randomized, controlled trial of 3.0mg of liraglutide in weight management. N Engl J Med. 2015;373:11–22.
101. Ning H, Le J, Wang Q, et al. The effects of metformin on simple obesity:A meta-analysis. Endocrine. 2018;62:528–34.
102. Kramer CK, Leitão CB, Pinto LC, et al. Efficacy and safety of topiramateon weight loss: A meta-analysis of randomized controlled trials. ObesRev. 2011;12(5):e338-47.
103. Anderson JW, Greenway FL, Fujioka K, et al. Bupropion SR enhancesweight loss: A 48-week double-blind, placebo-controlled trial. Obesity.2002;10(7):633–41.
104. Wilding JPH, Batterham RL, Calanna S, et al. Once-weekly semaglutidein adults with overweight or obesity. N Engl J Med. 2021 [Epub ahead ofprint.]
105. Abu Dayyeh BK, Noar MD, Lavin T, et al. 176 pivotal randomized-controlled trial of the adjustable (Spatz-3) intragastric balloon system forweight loss. Gastrointest Endosc. 2019;89(6):AB58-AB59.
106. Chang SH, Stoll CR, Song J, et al. Bariatric surgery: An updatedsystematic review and meta-analysis, 2003-2012. JAMA Surg. 2014;149(3):275–87.
107. BuchwaldH, Estok R, Fahrbach K, et al.Weight and type 2 diabetes afterbariatric surgery: Systematic review andmeta-analysis. Am JMed. 2009;122(3):248–56.
108. Rothstein RI,WoodmanG, Swain J, et al. Transpyloric shuttle treatmentimproves cardiometabolic risk factors and quality of life in patients withobesity: Results from a randomized, double-blind, sham-controlled trial.Gastroenterol. 2019;156(6):S-237.
109. Hedberg J, Sunstrom J, SundbomM. Duodenal switch versus Roux-En-Y gastric bypass formorbid obesity: Systematic review andmeta-analysisof weight results, diabetes resolution and early complications in single-centre comparisons. Obes Rev. 2014;15(7):555–63.
110. Arterburn D, Johnson E, Coleman KJ, et al. Weight outcomes of sleevegastrectomy and gastric bypass compared to nonsurgical treatment. AnnSurg. 2020. Online ahead of print.
111. Sjostrom L, Narbro K, Sjostrom CD, et al. Effects of bariatric surgery onmortality in Swedish obese subjects. N Engl J Med. 2007;357(8):741–52.
112. Sovik TT, Aasheim ET, Taha O, et al. Weight loss, cardiovascular riskfactors, and quality of life after gastric bypass and duodenal switch: Arandomized trial. Ann Intern Med. 2011;155(5):281–91.
113. Khalaj A, Mousapour P, Motamedi MAK, et al. Comparing the efficacyand safety of Roux-En-Y gastric bypass with one-anastomosis gastricbypass with a biliopancreatic limb of 200 or 160 cm: 1-Year results of thetehran obesity treatment study (TOTS). Obes Surg. 2020;30(9):3528–35.
114. BrownWA, de Leon B, Guillermo P, et al. Single anastomosis duodenal-ileal bypass with sleeve gastrectomy/one anastomosis duodenal switch(SADI-S/OADS) IFSO position statement – update 2020. Obes Surg.2021;31(1):3–25.
115. Sanchez-Pernaute A, Rubio MA, Cabrerizo L, et al. Single-anastomosisduodenoileal bypasswith sleeve gastrectomy (SADI-S) for obese diabeticpatients. Surg Obes Relat Dis. 2015;11(5):1092–8.
The American Journal of GASTROENTEROLOGY VOLUME 116 | MAY 2021 www.amjgastro.com
REV
IEW
ARTICLE
Jirapinyo and Thompson934
Copyright © 2021 by The American College of Gastroenterology. Unauthorized reproduction of this article is prohibited.