IBD & Pregnancy Christian Selinger Consultant Gastroenterologist.
31
IBD & Pregnancy IBD & Pregnancy Christian Selinger Christian Selinger Consultant Gastroenterologist Consultant Gastroenterologist
-
Upload
elle-winne -
Category
Documents
-
view
226 -
download
0
Transcript of IBD & Pregnancy Christian Selinger Consultant Gastroenterologist.
IBD & PregnancyIBD & Pregnancy
Christian SelingerChristian Selinger
Consultant GastroenterologistConsultant Gastroenterologist
Talk outline
Talk outline
• Can I have children?• Can I pass on IBD to my child?• Fertility issues• How to plan for pregnancy
– When to conceive– Medication before and during– Who to speak to
• Breast feeding
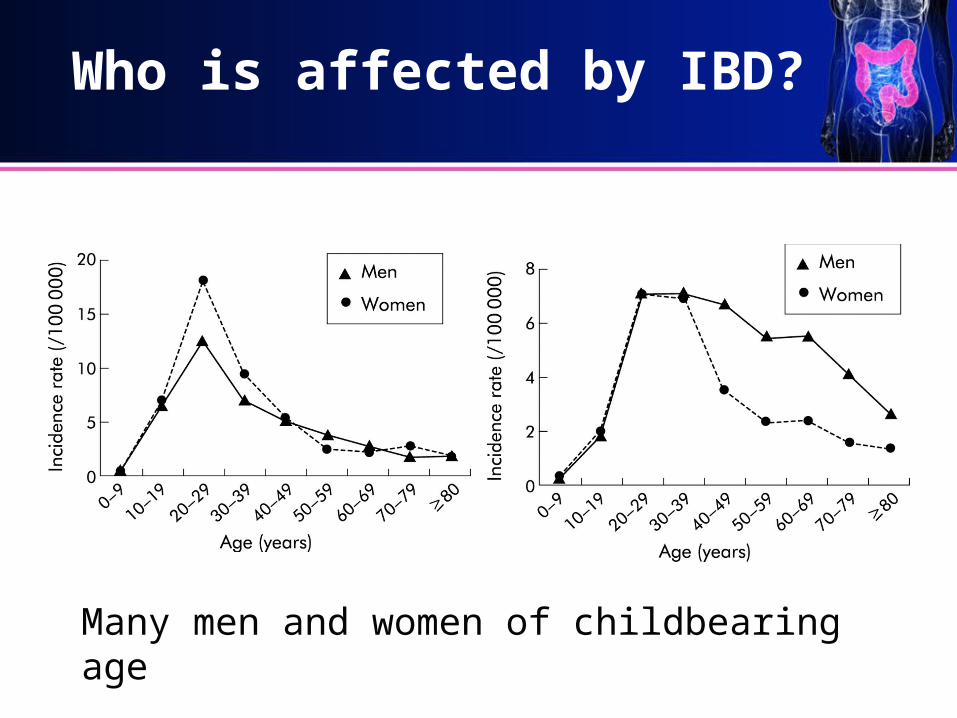
Who is affected by IBD?
Many men and women of childbearing age
Crohn’s disease Ulcerative coltis
Can I have children?
• YES
• Why talk about it then?– Not everyone knows this
• Patients• Doctors• Friends & relatives
– It should involve careful planning
Can I pass IBD on to my child?
• Developing IBD is complex– Family history / Inherited part / Genes– Environmental effects
• Smoking• “Dirt exposure”• Antibiotics in childhood• Many unknown as yet
Who gave birth after being diagnosed with IBD?
Can I pass IBD on to my child?
• Chance of passing on IBD– If one parent affected: 4-10%– If both parents affected: 30%
• Very good chance child will not get IBD
• Whether you child will get IBD depends on many other factors
Fertility
• In men– Normal– Sulphasalazine can temporarily disturb it
• In women– Generally good– Better chance of falling pregnant
• When well• Good disease control
Fertility
• Vast majority should experience little problems (other than the general public)
• Problem areas– Crohn’s disease with complex inflammation in
pelvis / “deep” pelvic surgery– Pouch surgery
• IVF works in these cases
Anyone experienced fertility problems?
Fertility
• Unable to have children – “involuntary infertility”– Overall not more common than general public
• Decided not to have children– “voluntary infertility”– Much more common in IBD – 18% versus 6% in general public
Decided not to have children
• Why?– Might not be aware that they can
• Poor knowledge• Anxiety about pregnancy, inheritance
– Bad advice• “Google”…• Friends• Some doctors not well informed
• We need to get the message out
When to have a baby?
• When well / in remission– Better chance of falling pregnant– Better chance of good course of pregnancy
• In some cases this might mean– Increased medication– Decisions around surgery
• If• What operation• when
Medication and Pregnancy
• Worth talking about
• Active disease (ongoing symptoms)– Less chance of conceiving– Worse outcomes for the baby
• Premature birth• Small baby• Loss of pregnancy
– Hence need to keep disease under control
Medication and Pregnancy
Who would you want to be?
Who stopped medication?
Who continued?
Medication and Pregnancy
• Generally benefits outweigh risks– Being well more important
• For baby and mum
– Risk to baby small
• All IBD drugs can be used– Except Methotrexate– Very poisonous (men and women)
Medication and Pregnancy
• Mesalazine– Asacol, Mesren, Mezavant, Octasa, Pentasa,
Salofalk– All extremely safe
• Thiopurines– Azathioprine, 6-Mercaptopurine– Safe in IBD– Better than steroids
Medication and Pregnancy
• Biologics– Infliximab (Remicade), Adalimumab (Humira)– Safe when needed– Generally used in severe disease
• Can I stop my medicines before falling pregnant?– For most better not– If been well a long time
• see specialist: ? well off drug
Medication and Pregnancy
• Your IBD nurse and Gastroenterologist• GP, midwife, obstetrician
– Often little knowledge of IBD drugs– Very specialist area
• BNF (drug bible), internet, pharmacist– Don’t bother– Officially all meds not licensed for pregnancy
and carry warnings
Worst case scenario
• 26 year old woman– Ulcerative colitis for 5 years– Usually on Asacol and well
• Falls pregnant unexpectedly
• Sees GP -> advised to stop meds
• Comes to clinic 10 weeks
Worst case scenario
• Symptoms– Diarrhoea 15* day, heavy bleeding– Dehydrated– Tired– Anaemia
• Problems– Needs steroids for 8 weeks and higher doses of
Asacol – Risk to pregnancy
Our advice
• Ideally plan pregnancy with us
• When questions over medications or symptoms (not only during pregnancy) contact– IBD nurse– Your specialist
• Don’t stop / change meds without speaking to us
Pregnancy course / outcomes
• Chance of flare– Same during pregnancy– Some women get much better– Very few get significantly worse
• Babies– Can be on the smaller side– Sometimes premature but few weeks only
Giving birth
• Vaginal delivery for most– Episiotomy safe unless (see below)
• Caesarean section preferred for– Woman with active peri-anal Crohn’s disease
• Fistula, seton, abscess• Well healed: can consider vaginal delivery
– Woman after pouch surgery– Too avoid tears, incontinence, worse fistulae
• Plan ahead

Breast feeding
Breast feeding
• Best possible nutrition for baby
• May protect the child from developing IBD
• All drugs (except Methotrexate) are considered safe for breast feeding
• However greater choice here– Bottle feeding and staying on drug
• Discuss with IBD nurse / specialist

Our aim
The Leeds plans
• Combined IBD clinics with obstetrician– Starts January 2014– For women during pregnancy– Also for women planning pregnancy– Aim: Joint up care throughout trying, pregnancy and
breast feeding
• Personalised information for all women (?how)– Soon after diagnosis– Well before planning pregnancy
Thank youThank you
Questions?Questions?