NZ Bowel Obstruction - Massey University of Sciences/IVABS... · Donald E Thrall, DVM, PhD Ross...
43
Bowel Obstruction Donald E Thrall, DVM, PhD Ross University School of Veterinary Medicine Basseterre, St. Kitts
Transcript of NZ Bowel Obstruction - Massey University of Sciences/IVABS... · Donald E Thrall, DVM, PhD Ross...

Bowel Obstruction
Donald E Thrall, DVM, PhD
Ross University
School of Veterinary Medicine
Basseterre, St. Kitts

Bowel Obstruction
Considered commonly
Important for patient that we be
correct
Seasoned radiologists sometimes
wrong
Many times patient not
obstructed…in my practice anyway

Radiographic technique
No preparation advised
Views
LL, RL, VD
Take advantage of gas as contrast medium
Technique
Analog: Hi mAs, low kVp
• Maximizes contrast
Digital: Technique less critical
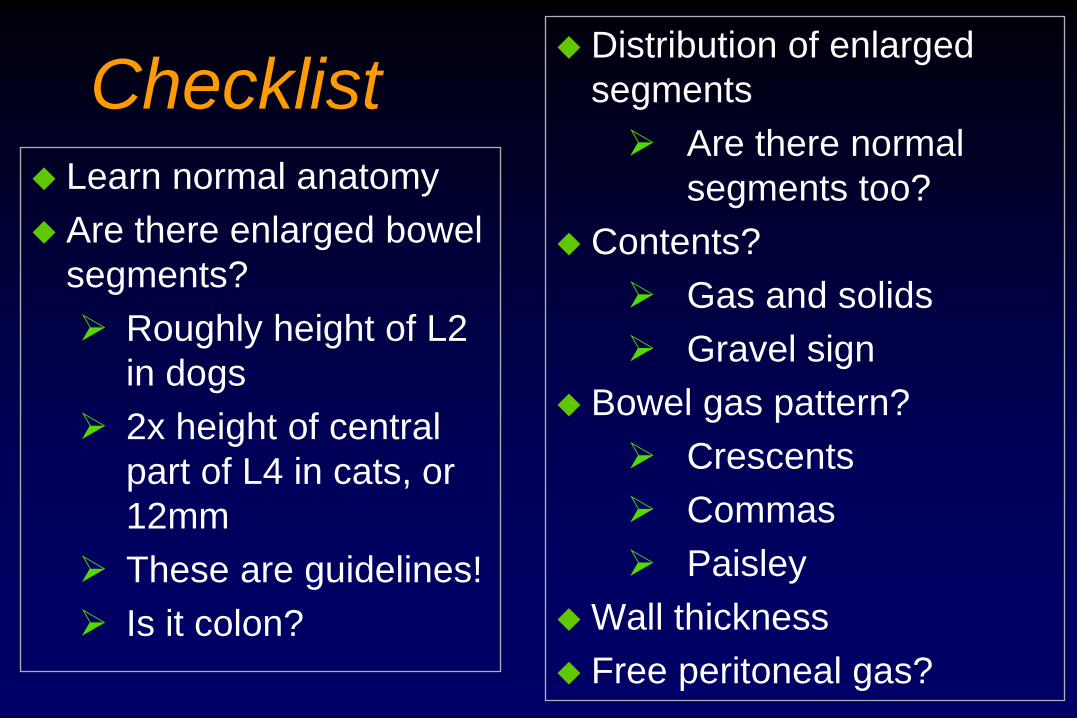
Checklist Learn normal anatomy
Are there enlarged bowel
segments?
Roughly height of L2
in dogs
2x height of central
part of L4 in cats, or
12mm
These are guidelines!
Is it colon?
Distribution of enlarged
segments
Are there normal
segments too?
Contents?
Gas and solids
Gravel sign
Bowel gas pattern?
Crescents
Commas
Paisley
Wall thickness
Free peritoneal gas?

Canine

Feline

Bowel Obstruction
Hallmark sign is enlarged bowel
Is the enlarged bowel small intestine?
Is the problem due to mechanical vs.
paralytic bowel obstruction?

Mechanical vs. Paralytic Ileus
Mechanical
Usually two populations of bowel
• Normal and Enlarged
Enlargement usually greater in mechanical
• Leads to stacking
Usually fluid and gas in lumen
• Sometimes foreign material in mechanical
– Cloth
– Gravel sign
• Often just gas in paralytic ileus
These are only guidelines and there is overlap
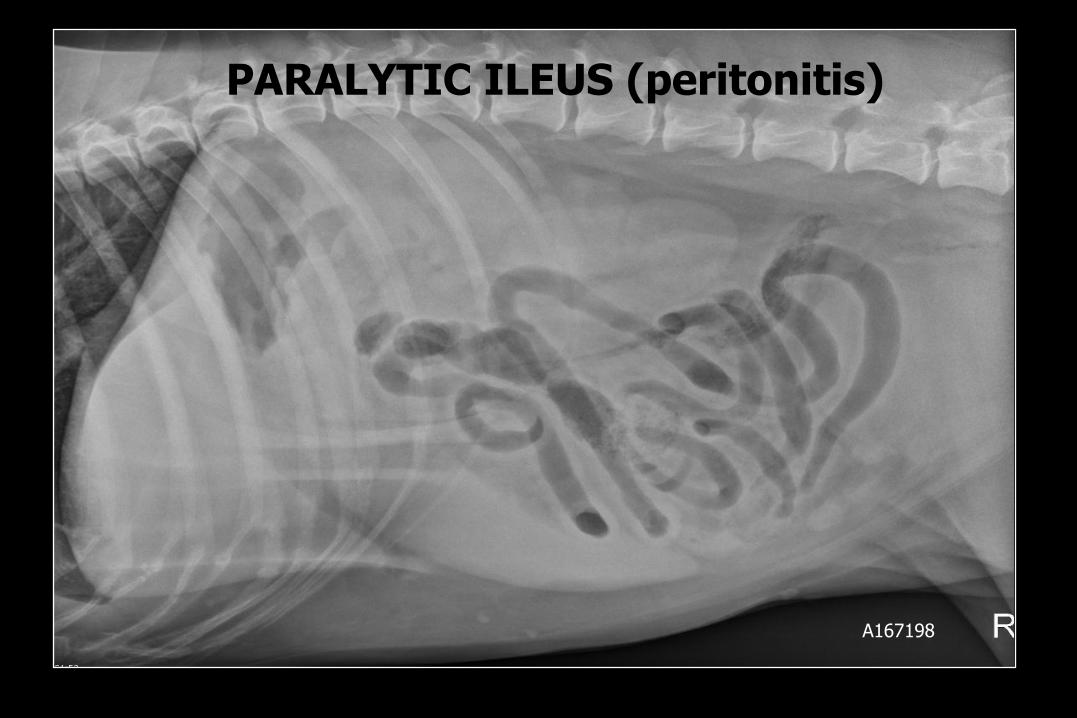
PARALYTIC ILEUS (peritonitis)
A167198
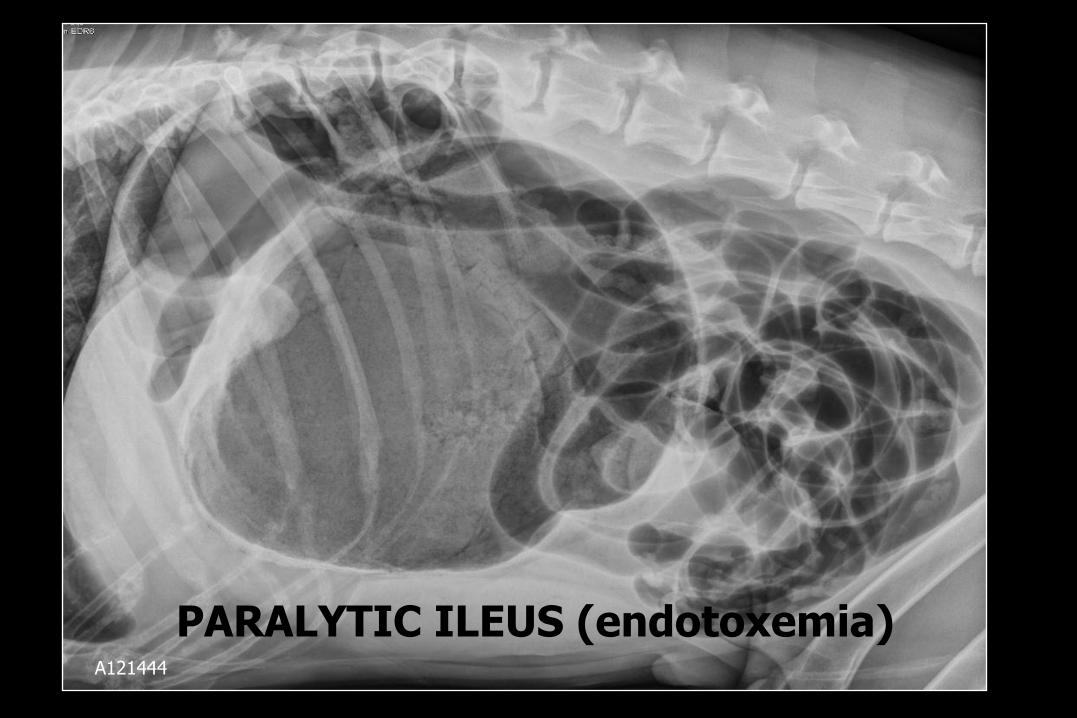
A121444
PARALYTIC ILEUS (endotoxemia)

Two Populations The presence of some small bowel segments that are normal in diameter and
others that are significantly larger…2-3X
A173605

Gravel Sign Opaque ingested
particulate matter
collecting proximal
to obstruction
More common
in chronic
partial
obstruction
Overall, not
common
Just something
to look for

I1031690
MECHANICAL: foreign material in S.I.

I1031690
MECHANICAL: foreign material

A85613
MECHANICAL: stacking Stacking

Cat, 1y
Vomiting for one week
Treated symptomatically
2 sets of radiographs declared normal
except for fecal accumulation
Emergency radiographs declared “no
evidence of obstruction”
91495
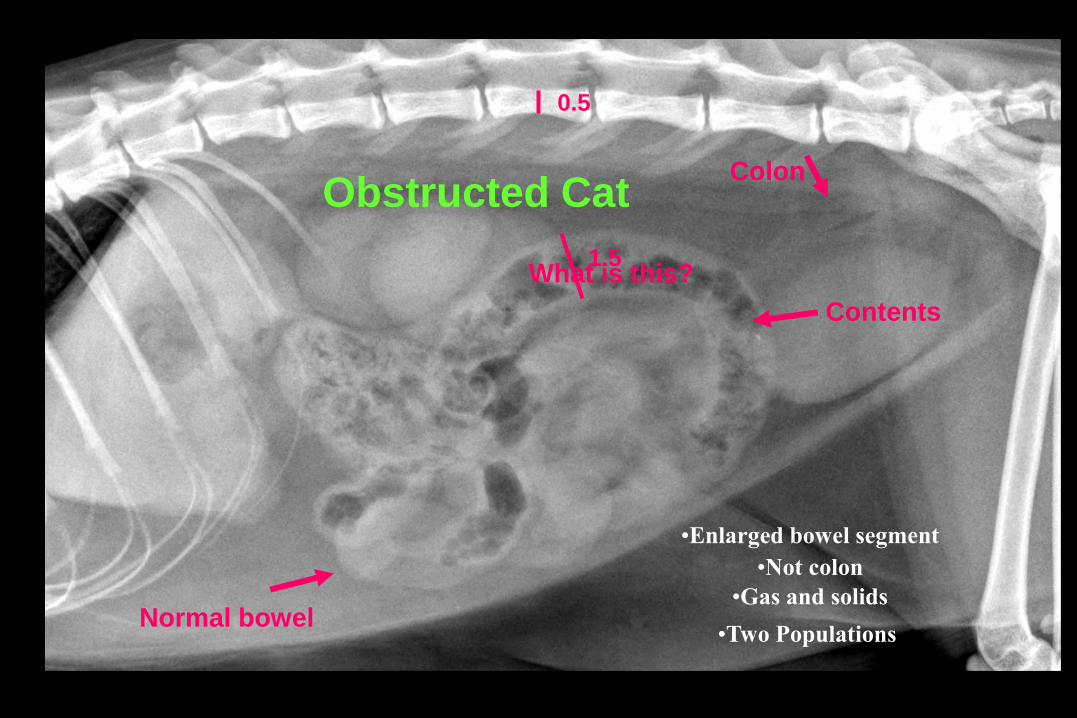
•Enlarged bowel segment
1.5
0.5
Colon
•Not colon
Contents
•Gas and solids
What is this?
Normal bowel •Two Populations
Obstructed Cat
Learning Points
Problem started when small bowel
misidentified as colon
Small bowel can have fecal-like contents
Anatomy was misinterpreted

German shepherd, 8y
3 day history of anorexia
One day history of vomiting
Taken to rDVM
Referring radiograph report: Foreign material (bone) and intestines seemed displaced
Given fluids and sent home
Vomiting continued; went back to rDVM
Referred
Dog is indiscriminant eater (paper, cans)
Mostly an indoor dog
112554

R

• Two
Populations
• Foreign
Material in
S.I.
Staffordshire, 2y Began vomiting 4d ago after shredding
and eating a sock
Became anorexic the following day
Currently vomiting approximately 4 to 5 times daily
Evaluated by local veterinarian 1d ago and no diagnostics were performed
Now has intractable vomiting
112801


• Plication
• Crescents

• Plication and crescents
Courtesy Dr. W.R.Widmer

Some patients
where obstruction
was considered

Labrador retriever, 7y
Acute anorexia and vomiting for one day
Vomited brown fluid on way to ER
Hypovolemic shock
Soft/pliable abdomen
Mildly resents palpation
No overt organomegaly or masses
113468


No obstruction seen with US WOW!!!
Septic effusion on peritoneal tap
Surgery Jejunal perforation
Foreign material but no obstruction
Died
Learning points None
Would call obstruction again

Cat, 15y
Progressive weight loss over
3 years
Seems to vomit when fed
treats
Lethargy
Abdomen not painful

113669
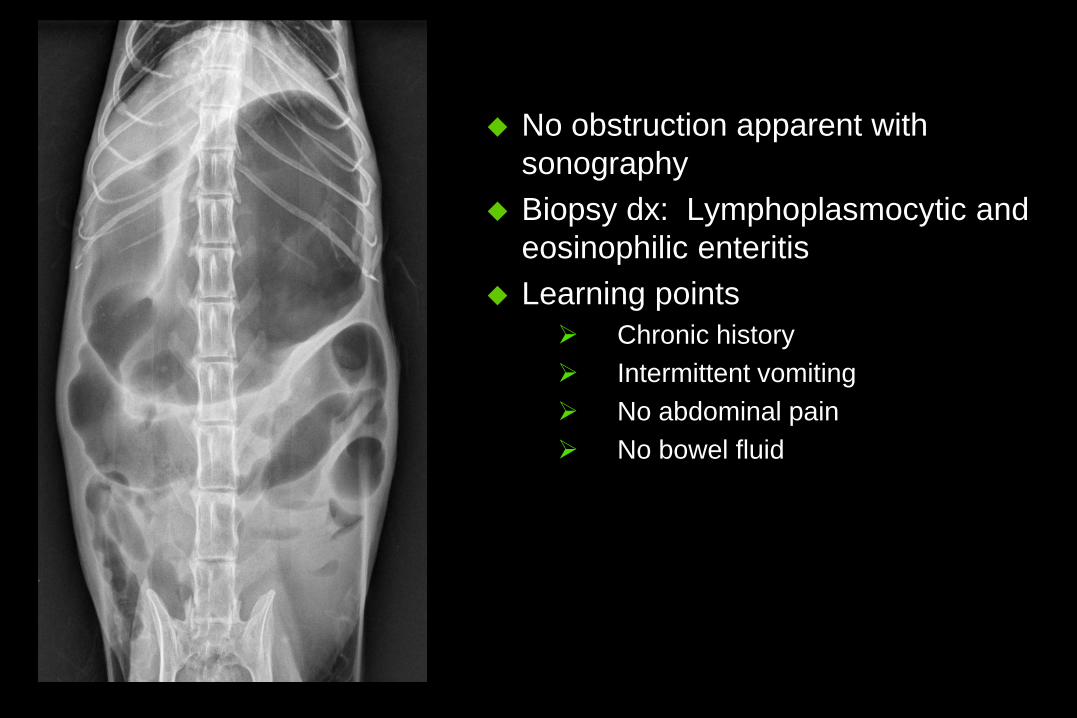
No obstruction apparent with
sonography
Biopsy dx: Lymphoplasmocytic and
eosinophilic enteritis
Learning points
Chronic history
Intermittent vomiting
No abdominal pain
No bowel fluid

What to do if
you’re confused
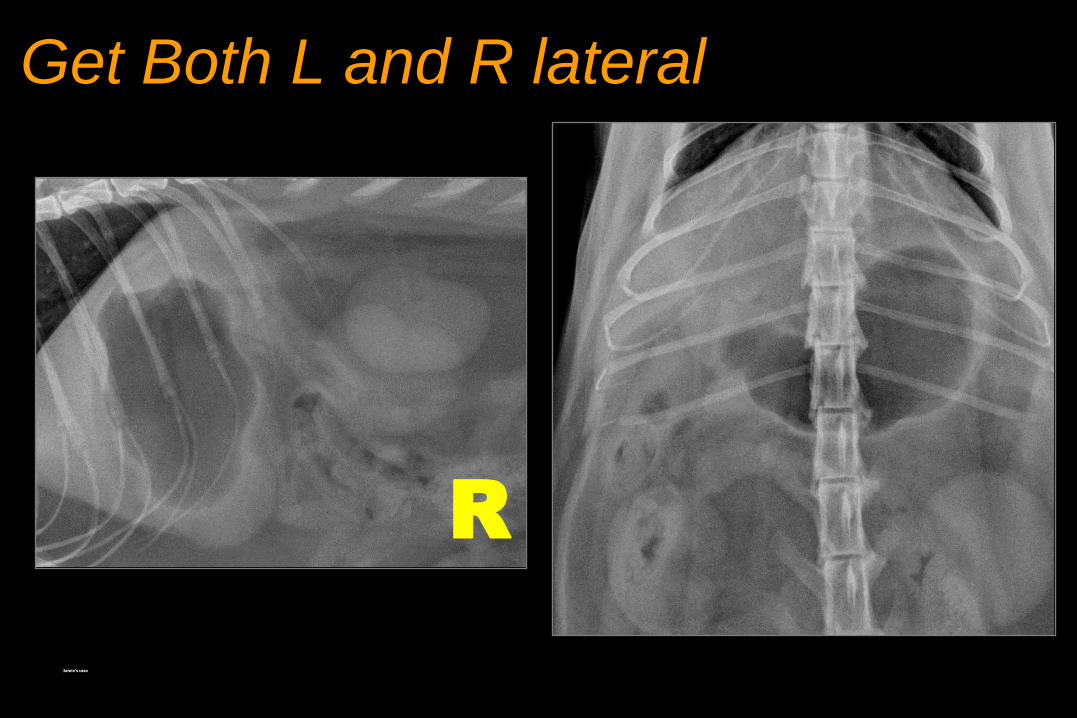
Get Both L and R lateral
Jamie’s case
R

L
L

Pneumocolon

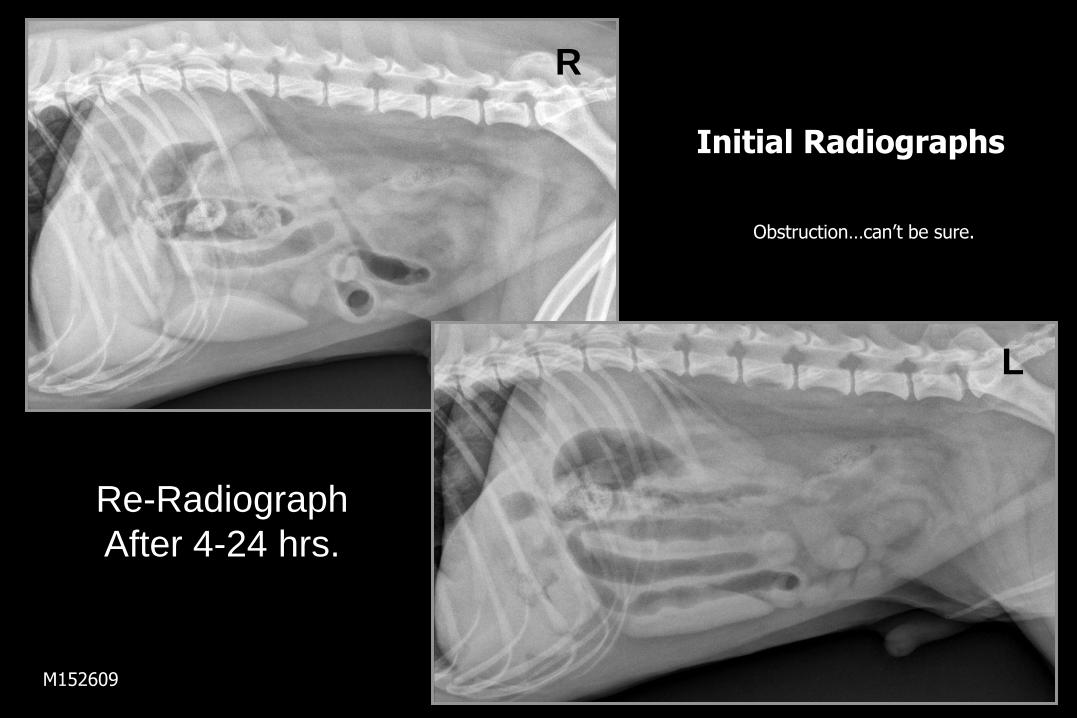
Re-Radiograph
After 4-24 hrs.
M152609
R
L
Initial Radiographs
Obstruction…can’t be sure.
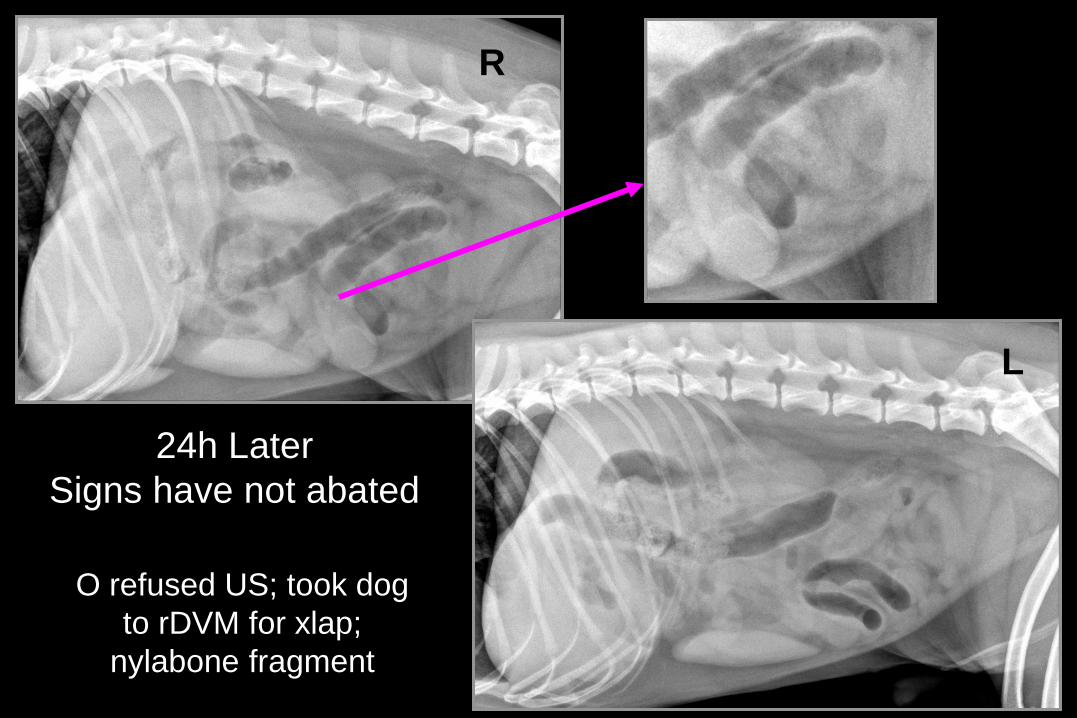
L
R
24h Later
Signs have not abated
O refused US; took dog
to rDVM for xlap;
nylabone fragment
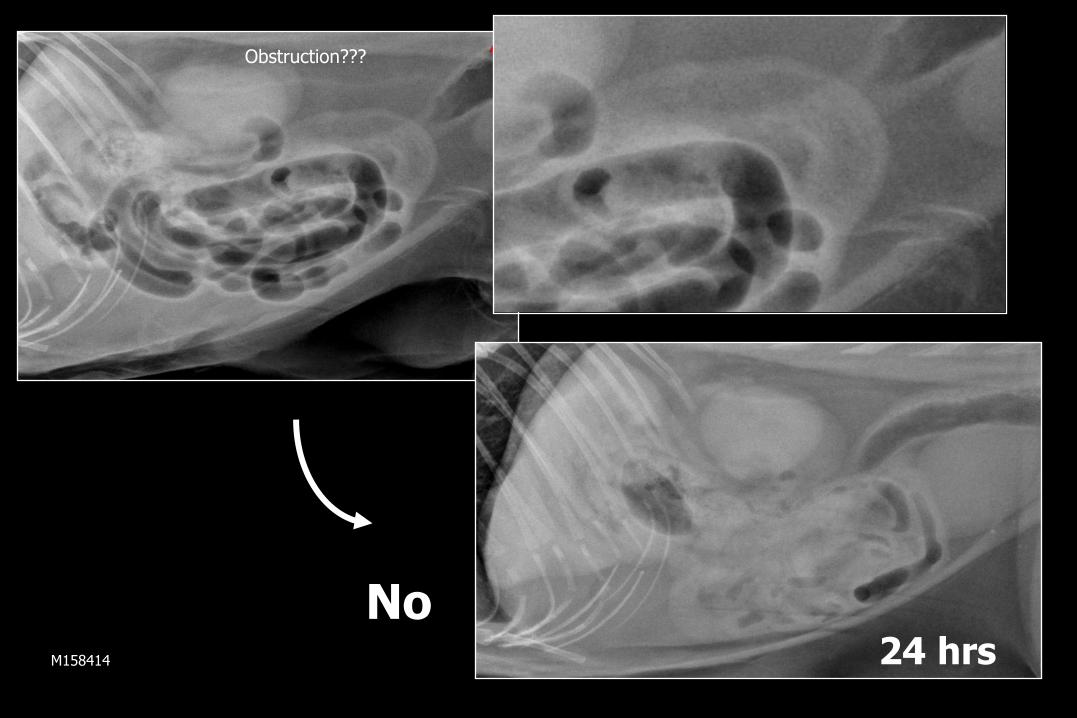
Obstruction???
24 hrs
No M158414
Upper GI Examination
Rarely done or done well in practice
Not enough barium
Wrong type of barium
Stopping too soon
Anti-motility drugs on board
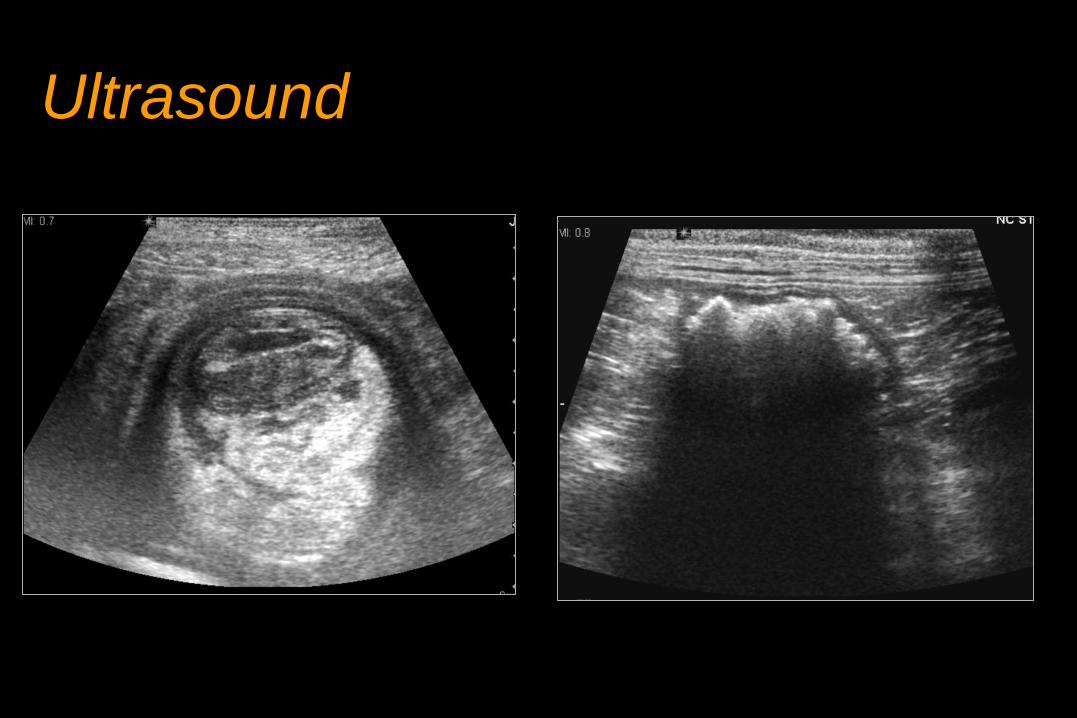
Ultrasound

Teleradiology