Large bowel obstruction
16
Large Bowel Obstruction
-
Upload
saravanan-sridharan -
Category
Health & Medicine
-
view
1.579 -
download
0
Transcript of Large bowel obstruction

Large Bowel Obstruction

Anatomy of Large Intestine

General
• Distal end of Ileum anus (about 1.5 m)– Smallest diameter: Sigmoid colon (where the diverticulosis
is most common to form here due to the high pressure especially during straining.)
• Primary function of the large intestine 1. Completion of absorption, esp. final absorption of water2. Normal flora manufacture certain vitamins (B complex, K)3. Formation, storage and expulsion of feces

• General characteristics – larger internal diameter– Presence of epiploic appendices– Presence of taeniae coli– Presence of the haustra
Haustra

Caecum~ A blind-ended pouch situated in the RIF~ Rest on iliacus muscle.~ 6 cm long ~ Completely covered with peritoneum. ~ No mesentery but quite mobile ~ Teniae coli converge on the base of the appendix.
Ascending colon~ 13 cm long ~ Peritoneum coverage: front & sides ~ adhered to abd wall
Right colic/ Hepatic flexure
Left colic/ Splenic flexure
~ higher than the right colic flexure ~ suspended from the diaphragm by the phrenicocolic ligament
Transverse colon~ About 38 cm long (suspended by the transverse mesocolon from the pancreas - mobile)
Descending colon~ About 25 cm long ~ Smaller diameter than asc.~ Peritoneum coverage: the front and the sides~ adhered to abd wall
Sigmoid colon~ 25 – 38 cm long ~ Continuous with the rectum in front of S3~ Extremely mobile~ Attached to the posterior pelvic wall by the fan-shaped sigmoid mesocolon.

Presentation (Cardinal Manifestation)
• Abdominal Pain– Sudden Severe Colicky Pain– Large Bowel – Lower abdominal pain
• Vomiting– The higher the obstruction the earlier it
appears and more profuse it is.– The nature of the vomitus depend on
the level of the obstruction.

• Constipation– Earlier in large Bowel Obstruction
• Abdominal Distension• Dehydration• Signs & Symptoms Of Peritonism• Low Grade Fever

On Examination
• General : – Dehydrated , In Pain , Tachycardia ,
Febrile
• P/A : Distended, Bowel Sound ↑ / ↓, Sx of peritonism

Investigations
• Abdominal X-ray – distended bowel loops– Multiple air fluid level
• CT Gastrograffin– Level of obstruction– Cause of obstruction (intraluminal,
intramural, extraluminal)
• USG Abdomen• Colonoscope


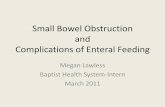
LARGE BOWEL OBSTRUCTION
The large bowel can be identified by the haustra and is distended from the ascending colon through the sigmoid. There is a definite paucity of air in the rectum caused by impacted feces leading to a buildup of fecal material and gas.


Suspected large bowel obstruction on clinical features and plain abdominal radiograph (supine)
↓INITIAL RESUSCITATION
1. Fluid resuscitation 2. Nil per oral3. Consider nasogastric decompression (RT Insertion)
especially if it is associated with small bowel dilatation and replace losses with Hartmann solution
4. Draw blood and send for FBC, BUSE, ABG, RBS and GSH5. Correction of any electrolytes imbalances6. Oxygen, Analgesic and Antibiotic therapy7. CBD and strict I/O chart8. Consider CVL insertion9. Frequent and regular monitoring of the parameters ( pulse
rate, urine output, CVP, blood pressure ) to ensure adequate resuscitation
10.Regular abdominal assessment to look for peritoneal signs indicating ischaemia , strangulation or perforation

Any peritoneal signs (tender,guarding,rebound tenderness) Yes No ↓ ↓ Surgery Gastrograffin enema study (preferred) or colonoscopy Mechanical obstruction Pseudo-obstruction ↓ Surgery Expandable metal Initial conservative management ↓ stenting for distal - treat underlying cause colorectal tumours - discontinued all anti-motility - correct electrolyte imbalances
- nasogastric decompression - Syp erythromycin 125-250mg qid - Enemas and flatus tube - Colonoscopy decompression - Consider IV neostigmine 2.5 mg slow
bolus if above fails ( should be given under cardiac monitoring due to risk of bradycardia)
Indication for surgery: - fails expectant management - grossly distended caecum (>10cm widest
diameter) with signs of impending perforation - Peritonitis
Right-sided obstruction - Right hemicolectomy with primary
anastomosis - Right hemicolectomy with exteriorization
of both ends Left –sided obstruction
- three stage procedures ; defunctioning colostomy followed later by resection of the tumour and closure of colostomy
- Two-stage or Hartmann’s procedure - One-stage procedure ; primary
resection of the tumour with anastomosis

Reference
1. J M Villar, A P Martinez. Surgical Option for Malignant Left-Sided Colonic Obstruction. Surg Today (2005) 35: 275-281
2. H Markogiannakis, A Messaris. Acute Mechanical Bowel Obstruction. World J Gastroenterol 2007 ; 13(3):432-437
3. The Management of Malignant Large Bowel Obstruction : ACPGBI Position Statement . Colorectal disease 2007; 9 (Suppl 4) 1-17

Thank You