
notes on psyche
38
-
Upload
tabayoyong -
Category
Documents
-
view
223 -
download
0
Transcript of notes on psyche

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 1/38
8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 2/38
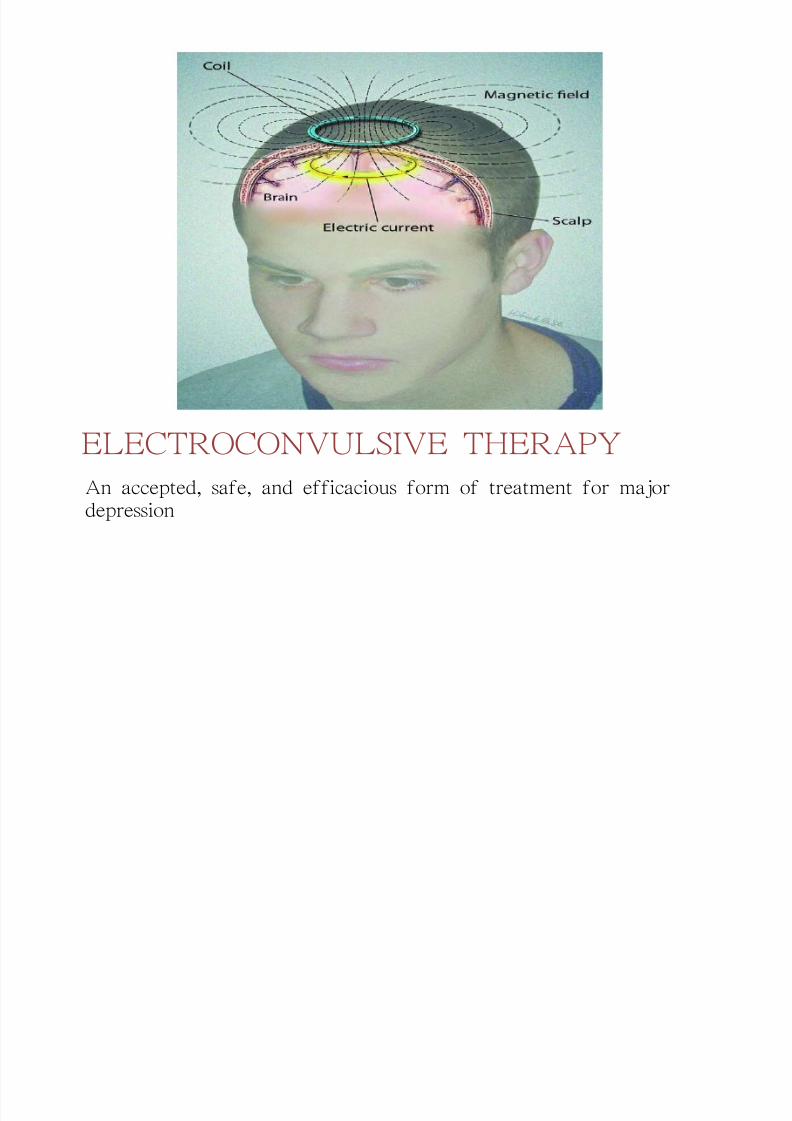
ELECTROCONVULSIVE THERAPY
An accepted, safe, and efficacious form of treatment for majordepression
8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 3/38
Indications
� Need for rapid, definitive response when a
client is suicidal or homicidal
� Extreme agitation or stupor� Risk of other treatment outweighs the risk of
ECT
�History of poor drug response , history of good ECT response
� Client prefers it.
3

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 4/38
Indications� MDD & bipolar disorder
� manic clients resistant to lithium &antipsychotic drug
� rapid cycler clients (schizophrenia,
schizoaffective syndrome� psychotic clients who are pregnant
� clients with Parkinsond s disease)

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 5/38
Contraindication
recent MI CVA
CVmalformation
intracranialmass lesion

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 6/38
Not for
DD
atypical depression and personality disorder
drug-dependent
depression secondary situational or social
Dosage
2-3x/wk, 6-12 treatment

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 7/38
Procedure

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 8/38
Preparing the client
� Pretreatment PE, labs, baseline memory abilities
� Signed informed consent
� Benzodiazepine or barbiturates should be eliminated
� Should be done by trained professional
� Nursing responsibilities
± NPO for 6-8 hours except cardiac and HPN dx
± Administer atropine one hour before tx
± Remove hairpins, contact lenses, hearing aid anddentures
± Monitor VS
8

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 9/38
During ECT
� Maintain IV line
� Place electrodes at sides of the head
� Administer Methohexital (Brevital) short-acting barbiturate
� Mechanical ventilation
� Nursing responsibilities
� Mechanically ventilate with 100% O2
� Monitor respiratory problem
� Administer benzodiazepine� Observe patient until stable
� Document and record

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 10/38
Disadvantage
T rary r li f
M ry i air nt
Cardiac ff cts HPN, arrhyth ia, alt rati n in cardiacut ut, chang s in CV dyna ics
H dyna ics incr as uscl t n , hy natr ia,
igrain
10

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 11/38
CRISISIt is an overwhelming reaction to a
threatening situation in which an individuals
usual problem-solving skills and coping
responses are inadequate for maintaining
psychological equilibrium

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 12/38
General Consideration1.Crisis occurs in all individuals at one time or
another2.Crisis is not necessarily pathological, it can
provide stimulus for growth & learning
3.Crisis is time limited and is usually resolve oneway or another in a brief period (4-6 weeks)
12
8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 13/38
Successful crisis resolution occurswhen functioning is restored orenhanced through new learning
Unsuccessful crisis resolution is whenfunctioning is not restored to pre-crisis
level, and the individual experiencesdecreased level of functioning

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 14/38

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 15/38
Type of Crisis� Developmental crisis - occurs from transition fromone stage of maturation to another in the life cycle
� Situational crisis occurs to a sudden, unexpectedevent in an individual life. These events is all aboutexperiences of loss.
� Adventitious crisis occurs in response to severe
trauma or natural disaster. These crisis can affectindividuals, communities and even nation
15

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 16/38
Sequence of Crisis Development
1. Pre-Crisis period individual has emotionalequilibrium
2. Crisis period individual has the subjective
experience of being upset, failure of usualcoping mechanism, symptoms areexperienced
3. Post-Crisis period resolution of crisis

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 17/38
Symptoms common in individual
experiencing crisis� Physical symptoms somatic complaints
� Cognitive symptoms confusion, difficultyconcentrating, racing thoughts, inability tomake decisions
� Behavioral symptoms disorganization,impulsive, angry outburst, withdrawal from
social interaction� Emotional symptoms anxiety, anger, guilt,
sadness, depression, paranoia, suspicion,helplessness, powerlessness

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 18/38
Crisis Intervention1. Assistance
± Assistance for an individual affected by a crisis± Assistance for groups or communities affected
by crisis
� Mobile crisis team
� Disaster response team
� Critical incident stress debriefing assistance
is directed at groups of professional
18
8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 19/38
Role of the Nurse
� Nurse provides direct services to people in crisis and serve as
members of crisis intervention teams
� In acute and chronic hospital setting assist individuals andfamilies responding to the crisis of serious illness,
hospitalization and death
� In community setting provide assistance to individuals and
families in developmental and situational crisis� Nurses working with a particular group of client should
anticipate situations in which crisis may occurs. They also
collaborate with other health team members to help an
individual resolve crisis

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 20/38
� the goal of crisis intervention is to return the
individual to pre-crisis level of functioning
�Emphasis is on strengthening and supportinghealthy aspects of individuals functioning

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 21/38
Principles of crisis intervention
� A problem-solving approach is use in a systematic
manner
± Assessing the individuals perception to problem
assessing strengths and weaknesses of the individual
and family support system
± Planning specific outcomes or goals based on
priorities
± Providing direct intervention
± Evaluation outcome and results of intervention
21
8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 22/38
Principles of crisis intervention
� Use the framework of Maslows hierarchy of
needs to determine the priorities forintervention
± Physical resources necessary for survival
± Social resources necessary for regaining sense
of belonging
± Psychological resources necessary for regaining
self-esteem

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 23/38
Role of crisis intervention worker
� Establishes rapport and communities
hope and optimism� Assumes an active, directive role if
necessary
� Make suggestions and offer alternatives

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 24/38
24
Terms
� Substance abuse ingestion of chemical active agent
� Addiction an illness characterized by compulsion, loss of control, & continues
patterns of abuse despite with a dysfunction habit (ANA)
� Psychological dependence continuous or intermittent craving for a substance to
avoid a dysmorphic or unpleasant mood state emotional dependence
� Tolerance ability to obtain a desired effect from a specific dose of a drug
� Physiologic dependence physical defects resulting from the multiple episodes of
a substance use - withdrawal Sx
� Behavioral dependence substance-seeking & pathological use patterns of the
person using the substance
� Codependency all the behavior patterns of family members who have been
significantly affected by another family members substance use or abuse

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 25/38
Milieu management
� For disruptive patients:
± Set limits
± Frequently observe escalating patients to intervene
± Modify the environment to minimize objects that can be used
as weapons
± Be careful in stating what the staff will do if a patient acts out
± When using restraints, provide for safety by evaluating the
patients status of hydration, nutrition, elimination, &
circulation
8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 26/38
26
Milieu management
� For withdrawn patients:
±Arrange non-threatening activities that involve
these patient in doing something
±Arrange furniture in a semicircle or around a table
±Help client to participate in decision making
±Reinforce appropriate grooming & hygiene
±Provide psychosocial rehabilitation

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 27/38

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 28/38
28
Milieu management
� For patient with hallucinations:± Attempt to provide distracting activities
± Discourage situation in which patient talk to others about
their disordered perception± Monitor television selection
± Monitor for command hallucination that might increasethe potential for patient to become dangerous
± Have staff members available in the dayroom so thatpatient can talk to real people about real people or realevents

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 29/38
Milieu management
� For disorganized patients:
±Remove disorganized patient to a lessstimulating environment
± Provide a calm environment
± Provide safe & relatively simple activitiesfor these patients

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 30/38
30
Nursing guidelines
± Build a therapeutic alliance with patient
1. Be calm
2. Accept patient
3. Keep promises
4. Be honest
5. Do not reinforce hallucinations or delusions
6. Do not touch patient without warning
7. Reinforce positive behaviors8. Avoid competitive activities
9. Do not embarrass patient
10.Allow & encourage verbalization of feelings

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 31/38
31
SCHIZOPHRENIA LIKE DISORDERS
1. Schizoaffective disorders
± Uninterruptive period of illness during which at some point the patient
experiences a MDD, manic or mixed episodes along with the negative
symptoms of schizophrenia
± In the absence of prominent mood symptoms, patient exhibits delusion or
hallucination
2. Schizophreniform disorder
± Patient exhibits features of schizopohrenia for more than 1 month butfewer that 6 months
± No impaired social or occupational function
3. Brief psychotic disorder
± Onset of at least 1 or more positive symptoms of psychosis
± Occur at least 1 day to less that an month then full recovery
4. Psychotic disorder due to a general medical condition
± Presence of prominent hallucination or delusion determined as resulting
from the direct physiologic effect of a specific medical condition

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 32/38
32
Nursing Interventions
Strengthening Differentiation Between Delusionsand Reality
� Provide patient with honest and consistent
feedback in a nonthreatening manner.� Avoid challenging the content of patient's
behaviors.
� Focus interactions on patient's behaviors.
� Administer drugs as prescribed whilemonitoring and documenting patient's responseto the drug regimen.
� Use simple and clear language when speakingwith patient.
8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 33/38

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 34/38
34
Nursing Interventions
Improving Activity Tolerance
� Assess patient's response to prescribed antipsychotic drug.
� Collaborate with patient and occupational and physical therapyspecialists to assess patient's ability to perform ADLs.
�Collaborate with patient to establish a daily, achievable routine withinphysical limitations.
� Teach strategies to manage adverse effects of antipsychotic drug thataffect patient's functional status, including:
± Change positions slowly
± Gradually increase physical activities
± Limit overdoing it in hot, sunny weather± Use sun precautions
± Use caution in activities if extrapyramidal symptoms develop.

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 35/38
Nursing Interventions
Improving Coping with Thoughts and Feelings
�Encourage patient to express feelings.
�Focus on patient's feelings and behavior.
�Provide honest perceptions of reality andfeedback about symptoms and behaviors.
�Encourage patient to explore adaptivebehaviors that increase abilities and success in
socializing and accomplishing ADLs.�Decrease environmental stimuli.

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 36/38
Nursing Interventions
Ensuring Safety
� Monitor patient for behaviors that indicateincreased anxiety and agitation.
� Collaborate with patient to identify anxiousbehaviors as well as the causes.
� Tell patient that you will help with maintainingbehavioral control.
� Establish consistent limits on patient's behaviorsand clearly communicate these limits to patient,family members, and health care providers.
�Secure all potential weapons and articles fromatient's room and the unit environment that

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 37/38
Ensuring Safety
� To prepare for possible continued escalation, form a psychiatricemergency assist team and designate a leader to facilitate aneffective and safe aggression-management process.
� Determine the need for external control, including seclusion orrestraints. Communicate the decision to patient and put plan intoaction.
� Frequently monitor patient within the guidelines of facility's policyon restrictive devices and assess the patient's level of agitation.
� When patient's level of agitation begins to decrease and self-control
is regained, establish a behavioral agreement that identifies specificbehaviors that indicate self-control against a reescalation of agitation.

8/7/2019 notes on psyche
http://slidepdf.com/reader/full/notes-on-psyche 38/38
38
Nursing Interventions
Community and Home Care Considerations
� Patients with these disorders may be insupportive housing, such as transitional living
halfway houses, foster homes, and board andcare homes. Supervision and drug managementare important areas of concern for the nurseworking in the community.
� Psychosocial rehabilitation approach may beused in the community setting, where skillsnecessary for independent living are taught. Thepatient who has been symptomatic since early
adulthood may not have learned these skills The










![NOTES ON THE CAT FELIS BOUC/-I]).downloads.hindawi.com/journals/psyche/1915/026813.pdf · 1915] Lyon--Notes on the Cat Flea lf5 Soon after the animals had been killed, their fur was](https://static.fdocuments.net/doc/165x107/5d62a13f88c99380278b9b8a/notes-on-the-cat-felis-bouc-i-1915-lyon-notes-on-the-cat-flea-lf5-soon.jpg)





