Mucogingival surgical procedures

of 9
-
Upload
shebashebut -
Category
Documents
-
view
232 -
download
0
Transcript of Mucogingival surgical procedures
-
7/27/2019 Mucogingival surgical procedures
1/9
Periodonticscogingival su rgica l p rocedures: A review of the iiterature
Jilireza Hae r i , MS , DMD , MH SV Francis G. Ser io, DMD, M S "
This article provides an in-depth review of the iiterature on mucogingival surgical techniques. Indicationsand contraindications of various surgical procedures are discussed with reference to the literature. Sur-gical techniques and indications for increasing the zone of keratinized tissue, such as free autogenousgrafts, applications of freeze-dried skin, and dermal matrix allografts, are described. Procedures to attainroot coverage, such as various autogenous grafts and guided tissue regeneration techniques, aiong withappiication of chemicais such as citric acid to improve their success, are aiso described. (Quintessence Int1999;30:475-483)Key w or ds : al logratt, autogenou s graft, guided tissue regeneration, keratinized tissue,mucogingivai surgery, root coverage
iLjfucogingival surgery is defined, according fo tbeGlossary of Periodontal Teims,^ as "a periodontaly, position, an d/o r the amo unt of gingiva." This termas been changed since it was first in trod uce d byiedman^ in the 1950s as surgery designed to correctroblems such as pockets extending apical to theiicogingival junction, malpositioned frenum or muscleachment, and inadequate depth of the vestibule.Qoval of tbe frenum and deepening of the vestibuleto correct these problems because the primaryp, the lack of attached gingiva, was overlooked.. the 1960s, investigators sucb as Bjorn ,' Nabers,*an^ developed mucogingival surgical tech-es such as free gingival grafts to increase tbe zonebratinized tissue. Miller,^ however, introduced theperiodontal plastic surgery as "surgical proce-used to correct or eliminate anatomic, develop-nfal, or traumatic deformities of the gingiva andoiar mucosa." This further expanded the objectiveke surgery from creating an adequate zone of at-d gingiva to root coverage, along with correctionproblems such as root sensitivity, esthetic concerns.
Eld fhe prevention of root caries. His intention in per-OTming periodontal plastic surgery was to restore the3sf t issue to the cem en toe na m el junc tion andffeate a normal, healthy gingival sulcus.
'Assislant Proiessor. Department of Periodonlics, University of Missis-sippi, Sctiooi ot Dentistry, Jackso n, M ississippi
Ch airm an, Dep artme nt of Per io donl ic s, Uniuersi ty ofMississippi. School of Dentistry, Jackson, Mississippi.
int requests; Dr Aineza Hae r i , Assistant Professor, Department o tUniversity of Mississipp i, Schooi of Dentistry, 3500 N ortfi State
et, Rcom D307, Jackson, Mississippi 39216-4505 Fax:601-984-6130.
INDICATIONS FOR INCREASING THE ZONEOF KERATINIZED TISSUEHow much keratinized tissue is adequate?
As mentioned, for decades the goal of mucogingivalsurgical procedures was to gain keratinized tissue inareas with tnucogingival problems. The primary objec-tive was to widen the zone of attacbed gingiva to im-prove periodontai healtb. In tbe past, many held sucha philosophy without detemiining how much kera-tinized tissue, if any, was required to achieve health. Inthe 1970s, Lang and Loe' conducted studies to estab-lish a relationship between tbe width of keratinizedtissue and bcalth. They concluded that a rninimum of2 mm of keratinized tissue is necessary to achievehealth. Despite effective oral hygiene, areas wifh lessthan 2 mm of keratinized tissue exhibited persistent in-flamtnation. However, observations by Dorfman et al*indicated that less than 1 mm of attached gingiva isadequate when inflammation is under control. Theyemphasized that therapy should be directed at control-ling the bacterial plaque and reducing inflatnmation.An increase in the band of keratinized tissue is indi-cated in areas of persistent attachment loss. The workof oth er researchers''"'-^ confirmed this conclusion.
Importance of keratinized tissue inrestorative and orthodontic treatmentThe width of keratinized fissue for teeth involving sub-gingival restorative margins has been of concern tosotne investigators. Donaldson'^ emphasized the propercontouring of provisional crowns. Physiologic contourappears to cause less recession than poorly contouredcrowns. He also noted that such crowns must have
Jintessence International 475
-
7/27/2019 Mucogingival surgical procedures
2/9
Hae ri/Serio
proper margins to avoid exertion of pressure on the sur-rounding tissue. Maynard and Wilson'-' stated that atleast 3 mm of attached gingiva is required if restorativemargins are to he placed in the gingival crevice. Theyalso mentioned that the thicloiess of the keratinized tis-sue is adequate when a periodontal probe cannot heseen through the margin of the free gingiva. Other in-vestigators'''* have confirmed that subgingival restora-tions with a narrow zone of keratinized tissue favor gin-gival recession and inflamtnation. Stetler and Bissada'"proposed a minimum of 2 mm of attached gingiva whenmargins are to be placed subgingivally.Orthodontic movement of teeth is another concern inareas with minimal attached gingiva. Batenhorst et al"observed formation of alveolar dehiscences on the facialsurfaces of the mandibular incisors in monkeys as teethwere moved facially and occlusally. Resorption of the ce-mentum and dentin was also observed with facial ortho-dontic movement. Steiner et al,'" in another study onmonkeys, discovered significant recession of the gingivalmargin as teeth were orthodontically moved labially.Maynard and Wilson"' recommended that muco-gingival surgery be performed prior to orthodontictreatment when there is a lack of keratinized tissueand there is demonstrable stress from the frenum onthe margin. Other situations, such as eruption of themandibular incisors labial to adjacent teeth, warrantmucogingival surgery. Maynard,^" in a retrospectivestudy of patients with mucogingival probletns in needof orthodontic therapy, reemphasized the need formucogingival surgery prior to orthodontic therapy tostabilize the attachment levels.Boyd" reviewed and discussed the indications andtiming of mucogingival therapy with respect to ortho-dontic intervention. He suggested early correction ofmucogingival problems, in the absence of malocclu-sion, to prevent further breakdow n. However, if a mal-occlusion exists, consultation with the orthodontist isnecessary to discover the nature and direction ofmovement. If there is a mucogingival problem labial toa tooth to be positioned lingually, then the orthodon-tic procedure would be undertaken first. The attachedgingiva must be reevaluated after completion of theorthodontic treatment.
Coatom et aF^ had a different opinion toward theneed for mucogingival therapy on patients with ortho-dontic problems. Their results indicated that a mini-mal width of keratinized tissue (less than 2 mm) iscapable of withstanding the stresses of orthodonticmovements. Orthodontics should precede surgical in-tervention in areas with a prominent root or faciallytipped teeth with at least a minimal width of kera-tinized tissue. In their study, 47% of the teeth had anincrease in the zone of keratinized tissue following or-thodontic therapy. However, in their opinion, a free
gingival graft was necessary prior to orthodontic treat-ment in areas that eompletely lacked keratinized tis-sue. In general, it seems to be the consen sus among in-vestigators that a laci< of keratinized tissue warrantsmucogingival surgery prior to orthodontic therapy.
SURGICAL PROCEDURES TOINCREASE KERATINIZED TISSUE
Free gingival graftSince the 1960s, the free gingival grafting techniquehas been the most predictable and popular method ofincreasing the band of keratinized tissue around teethwith mucogingival defects. Nabers,'' in 1966, oudinedthis technique; he suggested removal of the sulciilarepithelium, leaving the lamina propria intact. An inci-sion at the mucogingival junction was made to exposethe underlying connective tissue. The gingival tissuewas excised from the palate and contoured and suturedin place to the periosteum. The connective tissue of thedonor tissue contacted the connective tissue of the re-cipient area to maintain the blood supply to the graft.The area was covered with rubber dam m aterial, and asurgical dressing was placed to cover the rubber dam,
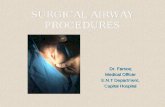
Others have contributed to advances in free gingivalgraft therapy. Pennel and coworkers" recommendedthe use of a periosteal fenestration to enhance graftstability. Dordick et aF'' evaluated placement of graftsdirectly on bone. After an initiai lag in healing whenplaced directly on bone, grafts placed on both perios-teum and bone looked similar after 3 weeks. They alsoshowed that nonpathologic dehiscences and fenestra-tions could be covered directly with donor tissue.Modern free gingival grafting tech nique has beenreviewed by Cohen.^" Advantages of this treatmentremain the high degree of predictabihty, the simplicity,and the possibilities for root coverage. Disadvantagesinclude the necessity of a second operative site, thepotentially compromised blood supply, greater dis-comfort, and possible hemostasis problems, especiallyat the don or site. Preparation is essentially the same aswas outlined by Nabers,-' It is critical that the free gin-gival margin be removed to allow creeping attachmentto occur. Figures la to lc illustrate the free gingivalgraft technique.
Freeze-dried skin andacellular dermal matrix allograftDonor materials, such as freeze-dried skin, have heenused to eliminate the second surgical site. This mater-ial has been shown to be biologically compatible withthe human oral tissue^^^^* and is nonimmunogenic.'"-"'
476 Volume 30, Num ber 7.1999
-
7/27/2019 Mucogingival surgical procedures
3/9
Haeri/Serio
Fig la The mandibular central incisor Fig 1b The autogenous graft is suturedexhibits a muc ogingival de fecl . place over the recipient bed Fig 1c The 4-weei i postope rat ivevievu reveals the keratinized tissue cre-ated as weil as partial roct coverage.
ig 2a The mandibuiar canine and premoiars exhibit mu cogin gi-ai defects. Fig 2b An Aiioderm ailcgraft is placed over the recipient bed.
Recently, an acellular dermal matrix allograft mater-n alternative to autogen ous tissue for gingival grafts.material has been utilized successfully in burn vic-tns since 1992 and for mucogingival surgeries since
34 The ailograft is a biocompatible, aceliular con-
ile leaving the basem ent me mb rane complex and
removing the immunogenic target cells while main-ining a structural framework to support fibroblast mi-tested to confirm the absence of the imm unogenic
Fig 2c The v\ew 3 months after surgery reveals an adequateband of keratin i zat ion created with tinis m aterial.
dergoing the viral inactivation step. Once this is ac-complished, the tissue is freeze dried and packaged.The use of Allodertu resuited in an increase in theband of kerat inized t issue with excellent colormatch."'** Alloderm appears to have more shrinkage,as compared with free-gingival graft. This factor is cur-rently under investigation (Figs 2a to 2c).
477
-
7/27/2019 Mucogingival surgical procedures
4/9
Haeri/Serio
INDICATIONS FOR INCREASING ROOT COVERAGEIn addition to being used to increase tbe zone ofattaebed gingiva, mucogingival surgical procedures areaiso used to gain root coverage, Probiems witb estbet-ies, root caries, and at times sensitivity of the exposedroot surface often warrant sucb procedures. In tbeirearly work, Sullivan and Atkins'' predicted possibleroot coverage using conventional free gingival grafts.They found that narrow recession defects have agreater cbance of complete repair than deep, widedefects, Avascularity of the exposed root surfaces isthe primary factor for the lower success in areas withdeep, wide defects,Miller^*^ redefined a recession and root coverage clas-sification. His classification is based on tbe depth of tberecession in relation to tbe mucogingival unction andthe amount of remaining interproximal bone. Greaterroot coverage is possible when tbe interproximal boneis in a more coronal position, Witb some minor tech-nique modifications, even deep, wide defects can bepredictably covered. Recession defects tbat extend api-cal to tbe mucogingivai junction in tbe presence of in-terproximal bone loss cannot be repaired completely.
SURGICAL PROCEDURES TOATTAIN ROOT COVERAGE
Lateral sliding flapThe lateral positioned flap was first introduced in1956 by Grupe and Warren.^^ They covered theexposed root suriace hy using a sliding flap operation.This was accomplished by removing the epithelial lin-ing around the defect and making a full-tbickness flaparound the adjacent tooth. After making a verticaiineision to free the pedicle, the flap was moved to coverthe defect. A frenectomy was often combined with such
procedure. Grupe-*" modified tbis tecbnique to retainthe marginai gingiva of the donor site. The tnajor ad-vantage of this procedure is the intact vaseularity of tbedonor tissue. One disadvantage of this procedure is thelimited supply of keratinized tissue at the donor site.Bahat et aH' introdueed the transpositional flap tech-nique to overcome the problem of lack of keratinizedtissue of the donor site. Tbey made 2 vertical releasingincisions at tbe line angles of the adjacent teeth andthen raised a fuli-thickness flap. They fheri slid the inter-dental papilla of the adjacent teetb to cover the defect.Cohen's atlas" outlines the lateral pedicie flap tech-nique quite clearly. Several caveats must be remem-bered. The procedure is contraindieated in areas withdeep interproximal poekets, severe interproximal boneloss, or excessive root prominence or where deep or
extensive root abrasion or erosion exists. Tension onthe flap after it is positioned should not be excessive.The pedicle height should not be excessive withrespect to its width. Tbc graft needs a wide base toensure proper perfusion of tbe coronal extent of theflap. Bone sbould never be left exposed over a rootsurface. Tbis will lead to bone loss and recession atthe donor site.
Coronally positioned flapAnother procedure to gain root coverage is the coro-nally repositioned flap (Figs 3a to 3c). Restrepo'''made a full-tbiekness flap to tbe vestibular fornixalong with 2 vertical releasing incisions. The flap waspositioned coronally to cover the root surface. Hefound that problems such as a reduction of thevestibular depth following surgery are of short dura-tion and that the depth will revert back to normaldepth with muscie function, Allen and Miller"^ used asplit-thickness flap instead of a full-tbiekness flap intheir technique. Approximately 84% of tbe sites hadcomplete root coverage, Tbe mean percentage in cov-ering tbe denuded roots was 98%.A 2-step procedure was introduced to increase thezone of keratinized tissue prior to coronal positioningof thefiap,"'^First, a free gingival graft was placed apicalto the denuded area to gain keratinized tissue. After 2months of healing, coronal repositioning of the flapwas performed for root coverage. Maynard-"' preferredtbe 2-step procedure over the lateral sliding flap be-cause handling areas that involved thin adjacent gin-giva during surgery made root coverage less pre-dictable. He stated several criteria for success of the2-step technique, including reduction of any rootprominence, adequate release of the flap, healing time,interproximal bone crests to be at nonnal height, pres-ence of sballow crevices interproximally, and tissueheight to be witbin 1 mm of tbe cementoenamel june-tion on adjacent tectb,MatteH^ evaluated the 2-step technique and discov-ered 65% root coverage on a predictable basis,Guinard and Caffesse'" compared the lateral slidingflap and coronally repositioned flap with a free gingi-val graft. They discovered no difference between thetwo regarding tbe gain in root coverage. A mean gainof 2.71 mm of root coverage was discovered 6 monthspos topera tively following botb procedure s, which wascomparable to results obtained by Matter.'*^A semilunar coronally positioned flap to cover thedenuded root surface was introduced by Tarnow.^' Thistechnique has an advantage over tbe other coronallypositioned flap tecbnique because it requires no su-tures. Approximately 2 to 3 mm of root coverage wasobtained with this procedure.
478 Volunie30, Number 7,1999
-
7/27/2019 Mucogingival surgical procedures
5/9
Haeri/Sero
Fig 3a The patient was conce rned a boul ine appea rance o Ihemaxillary an ten O teeth. Fig 3b A full-thickness flap is raised and piaced cotonaliy tocover the exposed rool surfaces.
Free gingival graft to cover the root surfacehe free gingival graft has been utilized to cover the
Hoibrook and Ochsenbein-*- evaluated root cover-ge with free auto gen ous grafts in 35 patients. They
and 76.6% in areas with recessions of 3 to 5m and greater than 5 mm, respectively. Total eover-
were (1) elimination of the dead space under the(2 ) harvesting of thin grafts (1.5 mm) for
Miller^* used citric acid treatment prior to placing
Vot coverage.
Creeping attachment
4d}. Creeping attachinentmore likely to occur in areas of na rrow recession.chment app roxim ately 1 year following surgery.
Fig 3c S IX months ioliowing surgery, there is more than 60% rootco^ierage on centrai and iateral inciso/s.
giva. Similar results were obtained by Bcil et al^" 1 yearpostoperatively. Harris^^ evaluated creeping attaehmentfollowing a connective tissue graft with partial-thicknessdouble pedicle graft. Creeping attachment occurred in95.5''.''ci of the subjects and was approximately 0.8 mm.Citric acid application
Application of citric acid to improve the success of rootcoverage has been evaluated by many investigators.Register and Burdick,^^ in their histoiogic study ondogs, discovered that application of citrie acid (pH 1,0),applied for 2 minutes on the root surface, induced flapreattachment and cementogenesis. Garrett and cowork-ers" discovered that citric acid treattnent in conjunc-tion with root planing exposed collagen fibrils. Thesefibrils were absent on surfaces that are not root planed.Citric acid also removes the radicular smear layer andopens the dentinal tubules to allow the formation ofnew cementum.'^ In addition, it demineralizes the rootsurface and removes residual endotoxins, thus render-ing the environment favorable for a ttachment,'*479
-
7/27/2019 Mucogingival surgical procedures
6/9
Haeri/Serio
Fig 4a Ttie mandibular ce nt o! incisors require a iree gingival Fig 4b A Iree gingivai grafl is placed to create a zone of kera-gratt. linization.
Fig 4c One month following tfie surgery, a wide zone of kera-tinized tissue has been creaied Fig 4d One year fo:iowing surgery, 3 mm ot creeping attachmerithas oocuired on the right central incisor.
According to iVIiller,^* citric acid application is oneof the factors that increases the success of the rootcoverage utilizing free autogenous grafts. Liu andSolt"" discovered significant increase in the amount ofkeratinized tissue after use of citric acid with a 2-stepfree gingival graft followed by a coronally positionedflap. Tolmie et aP' obtained an overall mean root cov-erage of S.SO/b using citric acid.Evaluations by Ibbott et al*^' indicated no differ-ence between the citric acid-treated and the un-treated group. They found no clinical justification fortbe use of citric acid prior to free gingival grafting tocover the denuded roots. Approximately 50% to 60%mean root coverage was obtained in their study. Thiswas confirmed by Bertrand and Dunlap,'^^ who statedthat the success of the root coverage is dependent onthe proper case selection rather tban citric acid ap-plication . They repo rted 70% coverage for bothgroups.In general, there seems to be controversy over tbeuse of this material. Although several investigatorshave reported improvements using citric acid, compar-ative studies refute such findings.
Double-papilla repositioned flapIn some cases if the adjacent gingiva and the interden-tal papilla of the tooth with gingival recession arehealthy, then it is possible to slide tfie papilla of iheadjacent teeth from eitber side to cover the defect.This procedure is called the double-papilla reposi-tioned flap. Cohen and Ross" stated the advantages ofdouble-papilla repositioned flap technique over thelateral sliding flap: One benefit is tbe minimal arnountof exposure of the underlying periodontium at thedonor sites. This reduces damage to the tissues, heal-ing time, and postoperative complications. There isless tension of the donor tissue, and there is a greateramount of keratinized tissue at the interdental papil-lary area. They recommended this procedure for areaswith no interproximai destruction.'"
This is a predictable method to achieve root cover-age, according to Harris.^'' However, he placed a con-nective tissue graft to cover the denuded root surfacebefore suturing the papillae over tbe graft. Completeroot coverage was attained in 80% of the cases, withoverall mean root coverage of 97.4%.
480 Volume 30, Number 7,1999
-
7/27/2019 Mucogingival surgical procedures
7/9
Haeri/Serio
The mandibular right first premoiar Fig 5b A subep ithelial conne ctive tissue Fig 5c Two months following surgery com-tiibits a muc ogingival delec t with existing gra lt is pl ac ed o n the root surfa ce a fter piete root coverage is achievedcession. making a spiit-th ickness enveiope llap
Subepithelial connective tissue graft
ess nap with v ertical inc isions w as created at thehe palate to cover the den uded roots and sutured place. A periodo ntal dressing was placed over the
n the nond cnuded portion of the root and the con-Raetzke*^ placed the connective tissue graft under
e support and nourishment. An overall mean root
illustrated in Figs 5a to 5c.Nelson^' developed a mucogingival graft procedure
e connective tissue. Ne lson''' reported lOO /o eover-
ns (7- to 10-mm recessions).
As stated previously, Harris^" reflected a partial-thickness flap, utilizing connective tissue with doublepapilla sliding to cover the graft. He achieved 100%root coverage in 80% of cases. Overall, 97.4% of theroot surface was covered in this study. In a recentstudy, H arris " obtained a mean coverage of 94.8% byutihzing this technique.
Guided tissue regenerationThe principles of guided tissue regeneration have beenapplied to treat recession as well as to promote regen-eration of periodontal osseous defects. Tinti et aF usedexpanded polyietrafluoroethylene (e-PTFE) {Gore-Tex,WL Gore) to treat facial recessions in humans. A ull-thickness flap was reflected to approximately 3 mm api-cal to the bony crest. A partial-thickness flap was madefrom the base oi' the full-thickness flap in the apical di-rection. A semilunar incision was dissected to allowcoronal movement of the flap without creating any ten-sion. The root surface was heavily scaled and flaftenedwith a diamond bur. The membrane was trimmed andplaced to cover the root surface. The flap was coronaiiydisplaced to cover the membrane. Their results indi-cated root coverage that ranged from 28.6% to 75%,One problem with this technique is the difficulty inproviding adequate space for regeneration and coverageof the membrane. In a different study, titanium-rein-forced e-PTFE was used to create space for regenera-tion between the root surface and the membrane.^^ Useof this membrane resulted in a more predictable, faster,and simpler surgical procedure. The use of a trapezoidalflap and better suturing techniques could eliminate theproblems associated with coronaiiy positioning the flapand maintaining an adequate blood supply.'"481
-
7/27/2019 Mucogingival surgical procedures
8/9
Hae ri/Serio
Bioresorbable membranes have also been utilized forroot coverage of the denuded root surface. Roccuzzo ctaF ' evaluated Guidor resorbablc tncmbrane (Guidor)and titanium-reinforced e-PTFE tnembrane for thetreatrnent of human buccal gingival recession. Their re-sults indicated no difference between the 2 rnembranesin the amount of root coverage achieved. Mean rootcoverage of 82.4o/o and 83.2% was obtained for theGuidor and c-PTFE rnembranes, respectively.Pini Prato et al'- compared a 2-stage free gingivalgraft followed by placement of a coronally positionedflap with e-PTFE. Their findings indicated no differ-ence in the amount of root coverage in both groups.Root coverage of 72.7% and 70.Wo was obtained forthe membrane and the control groups, respectively.However, the root coverage was more successful inareas of shallow recession when the coronally posi-tioned flap (SLS^/o) was used than when guided tissueregeneration (63.5''.'o) was employed. In deeper reces-sions, guided tissue regeneration provided better rootcoverage (76.6'o) than did the control (65.8%).
CONCLUSIONVarious mucogingival surgical procedures werereviewed. The objectives, indications, and factors forthe success of these procedures were described, andresults obtained from different studies were discussed.The surgeon must be knowledgeable and up to datewith the literature and reported findings so that he orshe will be able to select the best surgical approach in-dicated for the patient to improve the results andachieve a more predictable outcome.
REFERENCES1. Glossary of Periodontal Terms (ed 3). Chicago: A merica nAcademy of Periodontology 1992.2. Fr iedman N. Mucog ing iva l su rgery . Tex Den t J I957 ;75 :3 5 8 -3 6 2 .3. Bjorn H . Free t ransplantat ion of g ingival propria. Sverige
Tatid l Tidning 1963:22:684-689.4. Nabe rs ] . Free g ingival grafts. Periodo ntics 1966 ;4;243-2 45.5. Cow an A. Sulcus deep ening incor pora t ing muco sal graft .
JPer iodon to l 1965 ;36 :188-192 .6 . Mi l l e r PD. Regene ra t ive and recons t ru c t ive per i odon ta iplastic surgery. Dent Clin North Am 1988;32 287-306.7 Lang NP, Loe H. The relat ionship betw een the wid th of ker-atinized gingiva and gingivai health. J Periodontoi I972;43;623-627.8. Dorfmail HS, Ketinedy JE, Bird WC. Lotigitudinal evaiua-tion of free autog eno us gingival autografts, J Cliti Perio don-to i 1980:7:316-324.9. De Trey E, Bernimoulin J. Influence of free gingival grafts
on the heal th of the m arginal g ingiva. J Clin P eriod ontoi1980 ;7 :381-393 .
10 . Hangorsky U, Bissada N. Clinical assessment of free gingi-';'vai graft effectiveness on the ma inte na nce of period ontal-heai th . J Peridontol 1980:51:274-278.
11. Salkin LM, F reed man A L. Stein M D, Bassiou ny M . A longi- 'tud ina l s tudy of un t rea ted muc og ing iva l defec t s . J Per i - -odontol 1987 :58:164 -166. ;
12 . Freedm an AL, Salkin LM , Stein M D, Gr een K. A 10 yearlongitudinal study of untr eate d m ucoging ival defects. J Peri-odon to i 1992 ;63 :71-72 .
13 . Donaldson D. The etiologj ' of gingival recession associated 'with temporary crowns. J Periodontoi 1974;45:468-471. '-
14. Ma ynard |G , Wi i son RD . Phys io log ic d imens io ns of thepc rio don tium significant to the restora tive dentist. J Peri- 'odontol 1979:50:170-17415 . Ericsson I, Lindhe J. Recession in sites with inadequate widthof the keratinized gingiva. J Chn Periodontoi 1984:11:95-103.16 . Stetler KJ, Bissada NF. Significance of the width of kera-tinized gingiva on the pe riod onta l sta tus of teeth with sub-marginai res torat ions . J Periodontoi 1987;58.696-70t) .17 Bate nhors t KF , Bow ers G M , Wiliiam s JE. Tissue changes re-sulting from facial tipp ing an d extru sion of incisors in mon-keys. J Periodontoi 1974;45 :660-668.18. Steiner GG, Pearson JK, Ainamo J. Changes of the marginalperiodontium as a result of labial tooth movement in mon-keys. J Periodontoi 1981:52:31 4-320.19. Ma ynard JG, Wi l son R D. Diagnos i s and managemen t ofmucogingivai probiems in children. Dent Child North Am1980 :24 :683-703 .20. Maynard JG. The rationale for mucogingival therapy in the
child and adolescent. Int J Periodont Rest Dent 1987:7(1):3 7 - 5 1 .
2 1 . Boyd RL. Mueogingival considerations and their relation-ships to orthodo ntics . J Periodontoi 1978:49:67-76.
22 . Coa tom GW, B ehre nts RG, Bissada N F. Th e width of kera-tinized gingiva during orthodontic treatment: Its significanti m p a c t o n p e r i o d o n t a i s t a t u s . J P e r i o d o n t o i 19 8 1 ;5 2 ;3 0 7 - 3 1 3 .
23. Pennel BM, Tabor JC . King KO, Towner JD. F r i t z BD,Higgason JD. Free masticatory mucosa graft. J Periodontoi1969 :40 :162-166 .24. Dordick B, Coslet JG, Seibert JS. Clinical evaluation of freeaut oge nou s grafts placed on alve olar bone . Part I. Clinicaipredictabi l ity , J Periodontoi 1976;47:559-56725 . Coh en ES. Atlas of Cosm etic and R econstructive Periodontal
Surgery, ed 2. Baitimore, MD: Lea & Febiger, 1994:84-98.26. Yukna RA, Sullivan WM. Evaluation of resultant tissue typefol lowing tbe in traoral t ransplantat ion of various lyophil-ized soft tissues. J Per iodo nt Res 1978:13:177-184.
27. Carroi i PB, Tow HD. Vernino AR. The use of al logenicfreeze-dried skin grafts in the oral environment. Oral Surg1974:37:163.
2 8. Mishkin DJ. Shelley LR Jr, Neville BW. Histologie study of af reez e-d r ie d sk in a l log raf t in a hu ma n . A case repo r t .JPer iodon to l 1983 :54 :534-537 .29. Abbott WM. Sell KW. Alteration of histocompatibility andspecies antigens in skin by freeze-drying. Surg Forum 1972;
2 3 : 2 8 2 .30. Abb ott W M, H em bre e JS. Ab senc e of antigenicity in freeze-dried skin ailografts. Cryobiology 1970:6:416.3 1 . Yukna RA, Turner DW. Robinson LJ. Variable antigenicityof lyophilized allogenic an d lyop hilized xe nog enic sidn inguinea pigs. Int J Periodont Res 1977; 12 : 19 7 - 2 0 3 ,
482 Volume 3D, Num ber 7, 1999
-
7/27/2019 Mucogingival surgical procedures
9/9