Mo1696 Impact of Ulcerative Colitis on Patients With Primary Sclerosing Cholangitis With or Without...
1
AGA Abstracts between ileitis at the time of TPC with IPAA and pouchitis. We did find a marked difference in ileitis and pouchitis between UC and FAP groups. For this reason, and in an effort to reduce pouch complications following surgery, further studies should be designed to mechanistically investigate the ileitis in UC patients as well as to prospectively examine the ileitis-pouchitis relationship. Mo1695 Clinical, Serologic, and Genetic Associations Among Patients With Both Inflammatory Bowel Disease and Ankylosing Spondylitis Chadwick I. Williams, Dmitry Karayev, Thomas Learch, Stephan R. Targan, Carol J. Landers, Jerome I. Rotter, Eric A. Vasiliauskas, Andrew Ippoliti, Manreet Kaur, Gil Y. Melmed, David Q. Shih, Marla Dubinsky, Kent D. Taylor, Dalin Li, Michael H. Weisman, Dermot P. McGovern Background:Up to 20% of IBD patients have clinical manifestations consistent with ankylosing spondylitis (AS). Recent studies have suggested that IBD and AS ‘share' some susceptibility loci. IBD related serologies are associated with IBD disease location and severity but have not been extensively studied in AS-IBD. The aim of this study was to examine associations among clinical characteristics, genetic variation (GWAS) and IBD related serologies and AS- IBD. Methods: We retrospectively identified 811 IBD subjects with abdominal/pelvis CT scans performed at our institution that previously had genome wide association studies and IBD related serologies performed. All CT scans were reviewed by a musculoskeletal radiologist for evidence of sacroiliac joint involvement and categorized as definite AS, suspected AS or normal according to ARS guidelines. Data on age, gender, ethnicity, disease distribution, surgeries, and smoking history were obtained from chart reviews. Standard tests for associ- ation between clinical characteristics, genetic markers and serologies were used after cor- recting for ethnicity and gender. IBD related serology (ASCA, OmpC, I2, CBir-1, and ANCA) were obtained by ELISA. Genetic data were generated using Illumina technology and we were able to look at 24 and 5 of the known IBD and AS loci respectively in this dataset. Results: Of the 811 IBD patients with imaging studies, we identified 169 (20.1%) AS-IBD cases. These included both definite and suspected AS cases as designated by ASR criteria. In CD, small bowel location was protective against developing AS (p=0.02), and an inverse relationship was observed between the need for surgery and the development of AS-IBD (p= 0.04). CBir ‘positivity' in CD was associated with AS IBD (p= 0.02). UC patients who continued to smoke were at increased risk of AS-IBD (p=0.06) - a trend seen in all IBD cases (p = 0.06). NOD2 was not associated with AS-IBD (p=0.63). Significant associations were seen with the known IBD loci 8q24 (p = 0.03) and JAK2 (p = 0.05). At the JAK2 locus a linear association was seen with mean allele frequencies of 35.9%, 37.3% and 43.2% in controls, no AS-IBD and AS-IBD respectively (p = 0.002). No association was seen with the known AS loci. Utilizing a GWA approach a number of loci achieved a nominal level of significance (p < 10-4) (see table) including genes involved in NFkB activation (BTRC), cell adhesion (DSCAML1), ubiquination (USP22), oxidative stress in response to environmental factors (OSR1) and anti-proliferative processes (BTG3). Discussion: We identified clinical, smoking history and serological associations with a cohort of robustly phenotyped AS-IBD as well as some putative genetic loci that achieve a nominal level of significance and contain genes of potential functional relevance. Additional cohorts will be required to validate these findings. Mo1696 Impact of Ulcerative Colitis on Patients With Primary Sclerosing Cholangitis With or Without Dominant Stricture Udayakumar Navaneethan, Preethi GK Venkatesh, Gursimran S. Kochhar, Bret Lashner, Madhusudhan R. Sanaka, Pokala R. Kiran, Bo Shen Background and Aim: Dominant strictures in patients with primary sclerosing cholangitis (PSC) are associated with reduced liver transplantation (OLT)-free survival. The impact of ulcerative colitis (UC) in such patients is unclear. The aim of the study was to investigate the influence of UC on the outcome of PSC in patients with and without dominant strictures. Methods: A total of 222 patients with PSC (167 with UC and 55 without UC) seen and followed at our institution between 1985 and 2011 were included. Clinical and demographic variables were obtained and patients were followed-up until OLT or the date of their last clinical visit. The impact of UC in PSC patients with and without dominant strictures was analyzed. Results: A total of 68 out of 222 patients had or developed dominant bile duct stricture(s). Dominant strictures were less common in patients with PSC-UC compared to PSC alone (25.1% vs. 47.3%, p=0.002). In patients with dominant stricture without UC, S-662 AGA Abstracts one cholangiocarcinoma was found, whereas four cholangiocarcinoma and 11 colon neo- plasms (colon cancer and/or dysplasia) were found in patients with dominant stricture with UC (p = 0.005). In patients without dominant stricture but with UC, 44 had colon neoplasia and 3 had cholangiocarcinoma. In patients without dominant stricture and without UC, only one colon neoplasia was found (p = 0.009). (Table 1) In patients with dominant stricture without UC (n = 26), actuarial OLT -free survival was 0% and in those with dominant stricture and UC (n = 42) was 11.9% (p = 0.006). In PSC patients without dominant stricture and without UC (n = 29), actuarial OLT-free survival was 6.9% and in those with UC (n = 125) was 34.4% (p=0.001). (Figure 1) Conclusions: In patients with and without dominant stricture with PSC, UC patients had a higher incidence of carcinomas (both colon and cholangiocarcinoma). The presence of dominant stricture did not impact the effect of UC. However patients with isolated PSC with or without dominant stricture have reduced OLT-free survival when compared to patients with PSC and UC. Table 1 Influence of UC on frequency of colo-rectal and cholangiocarcinoma in patients with and without dominant stricture Impact of UC on the Kaplan-Meier survival curve for liver transplant free survival for PSC patients with and without dominant stricture (Log rank test) Also 0-no UC 1-UC Mo1697 Risk of Pneumocystis Jiroveci Pneumonia Among Patients With Inflammatory Bowel Disease Millie D. Long, Francis A. Farraye, Philip N. Okafor, Christopher F. Martin, Robert S. Sandler, Michael Kappelman Background & Aims: Patients with inflammatory bowel disease (IBD) may be at increased risk for infectious complications. Pneumocystis jiroveci (formerly known as pneumocystis carinii) pneumonia (PCP) is a fungal infection most often related to advanced human immunodeficiency virus (HIV) infection or use of immunosuppressive medications. Our aims were 1) to determine the incidence and relative risk of PCP in IBD patients and 2) to describe medication exposures in IBD patients with PCP. Methods: We performed a retro- spective cohort study and a descriptive case series using administrative data from IMS Health Inc, LifeLink Health Plan Claims Database, from 1997 to 2009. Patients with Crohn's disease (CD) and ulcerative colitis (UC) were identified using diagnosis (ICD9) codes and medication dispensing (NDC) codes. PCP was measured via ICD-9 code 136.3 (pneumocystis) and NDC codes for PCP-specific antibiotics. In the cohort, IBD patients were randomly matched to 4 individuals with no IBD-related claims and no HIV diagnosis. Data were extracted on comorbidities and health care utilization. PCP risk was evaluated by incidence rate ratio (IRR) and by adjusted Cox proportional hazards model for IBD overall, and stratified by CD and UC. The demographics and medication histories of the 38 cases of PCP in IBD patients were extracted in the 60 days prior to PCP. Results: A total of 50,932 patients with CD, 56,403 patients with UC, and 1269 with unspecified IBD were included in the cohort. They were matched to 434,416 individuals without IBD. The crude incidence of PCP was higher in the IBD cohort as compared to non-IBD (IRR 3.48, 95% CI 2.10-5.81, incidence rate of 10.6/100,000 in IBD and 3.0/100,000 in non-IBD cohort). When stratified by IBD subtype, risk was increased for CD (IRR 4.49, 95% CI 2.14-9.75) and for UC (IRR 2.40, 95% CI 1.11-5.10) as compared to non-IBD. On adjusted Cox analysis, controlling for utilization and comorbidities, the risk of PCP was higher in the IBD vs. non-IBD cohort (HR 2.96, 95% CI 1.75-4.99), with greater risk in CD (HR 4.01, 95% CI 1.88-8.56) than UC (HR 1.97, 95% CI 0.92 -4.20). In the IBD case series of PCP cases (n=38), the median age was 49 (IQR 43-57), 21(55.3%) were female and 21 (55.3%) were on immunosuppression, 11 (28.9%) were on corticosteroids alone, 5 (13.2%) on combination thiopurine and corticos- teroid, 1 (2.6%) on thiopurine alone and 4 (10.5%) on corticosteroids and 2 other immunos- uppressive medications. Conclusions: Although the overall incidence is quite rare, patients with IBD are at increased risk for PCP. IBD patients with PCP are predominantly on corticosteroids or combinations of immunosuppressive agents including corticosteroids prior to PCP diagnosis. Further studies should target these potentially higher risk individuals in order to determine the risk-benefit ratio of PCP prophylaxis.
Transcript of Mo1696 Impact of Ulcerative Colitis on Patients With Primary Sclerosing Cholangitis With or Without...

AG
AA
bst
ract
sbetween ileitis at the time of TPC with IPAA and pouchitis. We did find a marked differencein ileitis and pouchitis between UC and FAP groups. For this reason, and in an effortto reduce pouch complications following surgery, further studies should be designed tomechanistically investigate the ileitis in UC patients as well as to prospectively examine theileitis-pouchitis relationship.
Mo1695
Clinical, Serologic, and Genetic Associations Among Patients With BothInflammatory Bowel Disease and Ankylosing SpondylitisChadwick I. Williams, Dmitry Karayev, Thomas Learch, Stephan R. Targan, Carol J.Landers, Jerome I. Rotter, Eric A. Vasiliauskas, Andrew Ippoliti, Manreet Kaur, Gil Y.Melmed, David Q. Shih, Marla Dubinsky, Kent D. Taylor, Dalin Li, Michael H. Weisman,Dermot P. McGovern
Background:Up to 20% of IBD patients have clinicalmanifestations consistent with ankylosingspondylitis (AS). Recent studies have suggested that IBD and AS ‘share' some susceptibilityloci. IBD related serologies are associated with IBD disease location and severity but havenot been extensively studied in AS-IBD. The aim of this study was to examine associationsamong clinical characteristics, genetic variation (GWAS) and IBD related serologies and AS-IBD. Methods: We retrospectively identified 811 IBD subjects with abdominal/pelvis CTscans performed at our institution that previously had genome wide association studies andIBD related serologies performed. All CT scans were reviewed by a musculoskeletal radiologistfor evidence of sacroiliac joint involvement and categorized as definite AS, suspected AS ornormal according to ARS guidelines. Data on age, gender, ethnicity, disease distribution,surgeries, and smoking history were obtained from chart reviews. Standard tests for associ-ation between clinical characteristics, genetic markers and serologies were used after cor-recting for ethnicity and gender. IBD related serology (ASCA, OmpC, I2, CBir-1, and ANCA)were obtained by ELISA. Genetic data were generated using Illumina technology and wewere able to look at 24 and 5 of the known IBD and AS loci respectively in this dataset.Results: Of the 811 IBD patients with imaging studies, we identified 169 (20.1%) AS-IBDcases. These included both definite and suspected AS cases as designated by ASR criteria.In CD, small bowel location was protective against developing AS (p=0.02), and an inverserelationship was observed between the need for surgery and the development of AS-IBD(p= 0.04). CBir ‘positivity' in CD was associated with AS IBD (p= 0.02). UC patients whocontinued to smoke were at increased risk of AS-IBD (p=0.06) - a trend seen in all IBDcases (p = 0.06). NOD2 was not associated with AS-IBD (p=0.63). Significant associationswere seen with the known IBD loci 8q24 (p = 0.03) and JAK2 (p = 0.05). At the JAK2locus a linear association was seen with mean allele frequencies of 35.9%, 37.3% and 43.2%in controls, no AS-IBD and AS-IBD respectively (p = 0.002). No association was seen withthe known AS loci. Utilizing a GWA approach a number of loci achieved a nominal levelof significance (p < 10-4) (see table) including genes involved in NFkB activation (BTRC), celladhesion (DSCAML1), ubiquination (USP22), oxidative stress in response to environmentalfactors (OSR1) and anti-proliferative processes (BTG3). Discussion: We identified clinical,smoking history and serological associations with a cohort of robustly phenotyped AS-IBDas well as some putative genetic loci that achieve a nominal level of significance and containgenes of potential functional relevance. Additional cohorts will be required to validatethese findings.
Mo1696
Impact of Ulcerative Colitis on Patients With Primary Sclerosing CholangitisWith or Without Dominant StrictureUdayakumar Navaneethan, Preethi GK Venkatesh, Gursimran S. Kochhar, Bret Lashner,Madhusudhan R. Sanaka, Pokala R. Kiran, Bo Shen
Background and Aim: Dominant strictures in patients with primary sclerosing cholangitis(PSC) are associated with reduced liver transplantation (OLT)-free survival. The impact ofulcerative colitis (UC) in such patients is unclear. The aim of the study was to investigatethe influence of UC on the outcome of PSC in patients with and without dominant strictures.Methods: A total of 222 patients with PSC (167 with UC and 55 without UC) seen andfollowed at our institution between 1985 and 2011 were included. Clinical and demographicvariables were obtained and patients were followed-up until OLT or the date of their lastclinical visit. The impact of UC in PSC patients with and without dominant strictures wasanalyzed. Results: A total of 68 out of 222 patients had or developed dominant bile ductstricture(s). Dominant strictures were less common in patients with PSC-UC compared toPSC alone (25.1% vs. 47.3%, p=0.002). In patients with dominant stricture without UC,
S-662AGA Abstracts
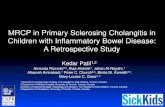
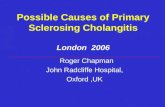
one cholangiocarcinoma was found, whereas four cholangiocarcinoma and 11 colon neo-plasms (colon cancer and/or dysplasia) were found in patients with dominant stricture withUC (p = 0.005). In patients without dominant stricture but with UC, 44 had colon neoplasiaand 3 had cholangiocarcinoma. In patients without dominant stricture and without UC,only one colon neoplasia was found (p = 0.009). (Table 1) In patients with dominantstricture without UC (n = 26), actuarial OLT -free survival was 0% and in those withdominant stricture and UC (n = 42) was 11.9% (p = 0.006). In PSC patients withoutdominant stricture and without UC (n = 29), actuarial OLT-free survival was 6.9% and inthose with UC (n = 125) was 34.4% (p=0.001). (Figure 1) Conclusions: In patients withand without dominant stricture with PSC, UC patients had a higher incidence of carcinomas(both colon and cholangiocarcinoma). The presence of dominant stricture did not impactthe effect of UC. However patients with isolated PSC with or without dominant stricturehave reduced OLT-free survival when compared to patients with PSC and UC.Table 1 Influence of UC on frequency of colo-rectal and cholangiocarcinoma in patientswith and without dominant stricture
Impact of UC on the Kaplan-Meier survival curve for liver transplant free survival for PSCpatients with and without dominant stricture (Log rank test) Also 0-no UC 1-UC
Mo1697
Risk of Pneumocystis Jiroveci Pneumonia Among Patients With InflammatoryBowel DiseaseMillie D. Long, Francis A. Farraye, Philip N. Okafor, Christopher F. Martin, Robert S.Sandler, Michael Kappelman
Background & Aims: Patients with inflammatory bowel disease (IBD) may be at increasedrisk for infectious complications. Pneumocystis jiroveci (formerly known as pneumocystiscarinii) pneumonia (PCP) is a fungal infection most often related to advanced humanimmunodeficiency virus (HIV) infection or use of immunosuppressive medications. Ouraims were 1) to determine the incidence and relative risk of PCP in IBD patients and 2) todescribe medication exposures in IBD patients with PCP. Methods: We performed a retro-spective cohort study and a descriptive case series using administrative data from IMS HealthInc, LifeLink Health Plan Claims Database, from 1997 to 2009. Patients with Crohn's disease(CD) and ulcerative colitis (UC) were identified using diagnosis (ICD9) codes and medicationdispensing (NDC) codes. PCP was measured via ICD-9 code 136.3 (pneumocystis) andNDC codes for PCP-specific antibiotics. In the cohort, IBD patients were randomly matchedto 4 individuals with no IBD-related claims and no HIV diagnosis. Data were extracted oncomorbidities and health care utilization. PCP risk was evaluated by incidence rate ratio(IRR) and by adjusted Cox proportional hazards model for IBD overall, and stratified byCD and UC. The demographics and medication histories of the 38 cases of PCP in IBDpatients were extracted in the 60 days prior to PCP. Results: A total of 50,932 patients withCD, 56,403 patients with UC, and 1269 with unspecified IBD were included in the cohort.They were matched to 434,416 individuals without IBD. The crude incidence of PCP washigher in the IBD cohort as compared to non-IBD (IRR 3.48, 95% CI 2.10-5.81, incidencerate of 10.6/100,000 in IBD and 3.0/100,000 in non-IBD cohort). When stratified by IBDsubtype, risk was increased for CD (IRR 4.49, 95% CI 2.14-9.75) and for UC (IRR 2.40,95% CI 1.11-5.10) as compared to non-IBD. On adjusted Cox analysis, controlling forutilization and comorbidities, the risk of PCP was higher in the IBD vs. non-IBD cohort(HR 2.96, 95% CI 1.75-4.99), with greater risk in CD (HR 4.01, 95% CI 1.88-8.56) thanUC (HR 1.97, 95% CI 0.92 -4.20). In the IBD case series of PCP cases (n=38), the median agewas 49 (IQR 43-57), 21(55.3%) were female and 21 (55.3%)were on immunosuppression, 11(28.9%) were on corticosteroids alone, 5 (13.2%) on combination thiopurine and corticos-teroid, 1 (2.6%) on thiopurine alone and 4 (10.5%) on corticosteroids and 2 other immunos-uppressive medications. Conclusions: Although the overall incidence is quite rare, patientswith IBD are at increased risk for PCP. IBD patients with PCP are predominantly oncorticosteroids or combinations of immunosuppressive agents including corticosteroids priorto PCP diagnosis. Further studies should target these potentially higher risk individuals inorder to determine the risk-benefit ratio of PCP prophylaxis.