Minding the Gap: Path Innovation, Collaboration and Quality
59
Minding the Gap: Path Innovation, Collaboration and Quality Barry P. Chaiken, MD, MPH, FHIMSS CMO, DocsNetwork, Ltd. © 2009 DocsNetwork, Ltd.
-
Upload
barry-chaiken -
Category
Health & Medicine
-
view
1.042 -
download
0
Transcript of Minding the Gap: Path Innovation, Collaboration and Quality
Minding the Gap: Path Innovation, Collaboration and Quality
Barry P. Chaiken, MD, MPH, FHIMSSCMO, DocsNetwork, Ltd.
© 2009 DocsNetwork, Ltd.

Overview
Costs of Healthcare eHealth Vision Quality and Errors Clinical Information Technology Clinician Adoption Innovation and Transformation Flatteners and the Triple Convergence
© 2009 DocsNetwork, Ltd. 2
- Paul Romer, EconomistGraduate School of Business
Stanford University
© 2009 DocsNetwork, Ltd. 3
““ A crisis is a terrible thing to waste.”
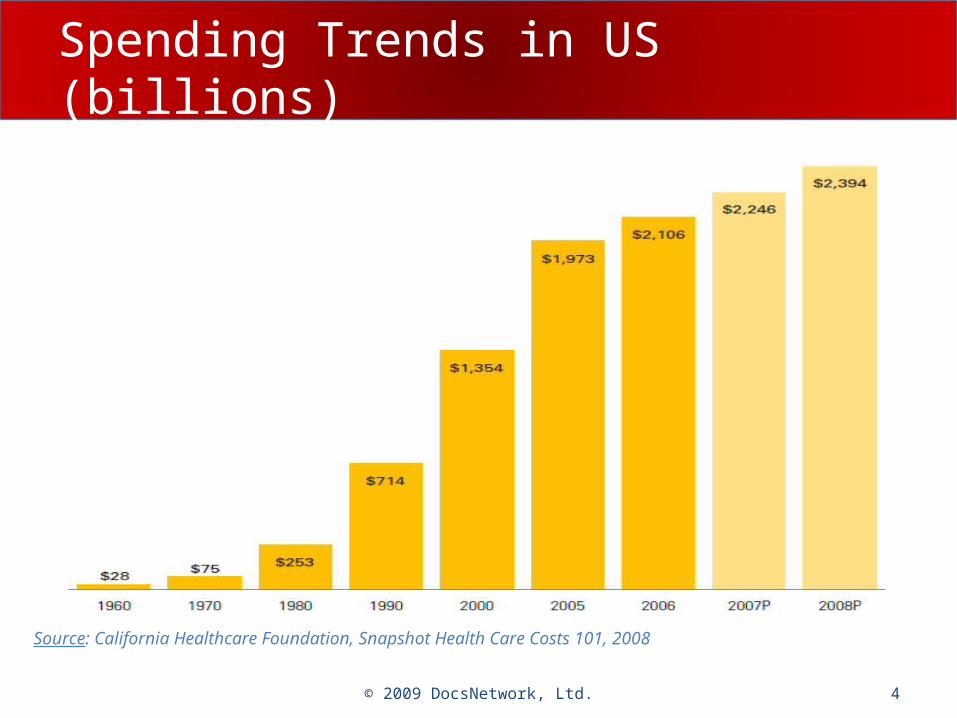
Spending Trends in US (billions)
Source: California Healthcare Foundation, Snapshot Health Care Costs 101, 2008
4© 2009 DocsNetwork, Ltd.
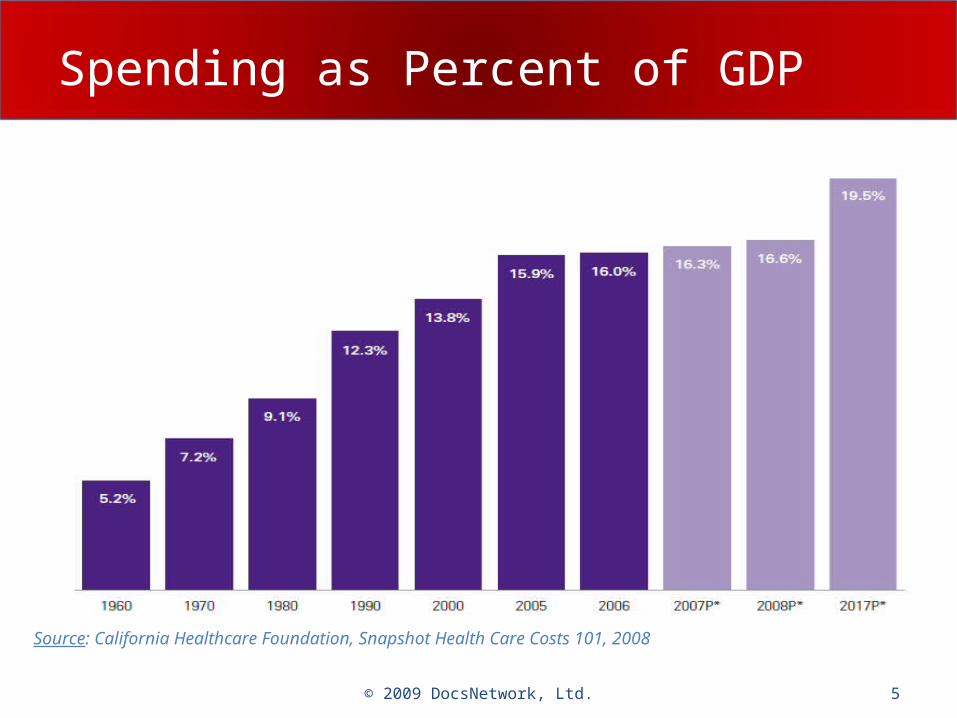
Spending as Percent of GDP
Source: California Healthcare Foundation, Snapshot Health Care Costs 101, 2008
5© 2009 DocsNetwork, Ltd.
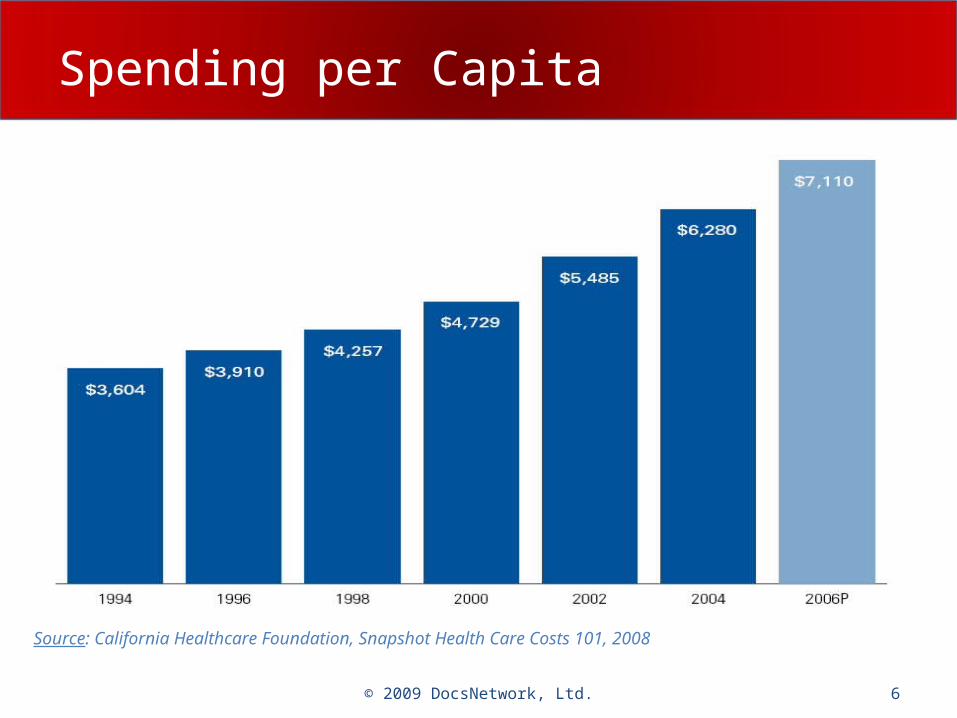
Spending per Capita
Source: California Healthcare Foundation, Snapshot Health Care Costs 101, 2008
6© 2009 DocsNetwork, Ltd.
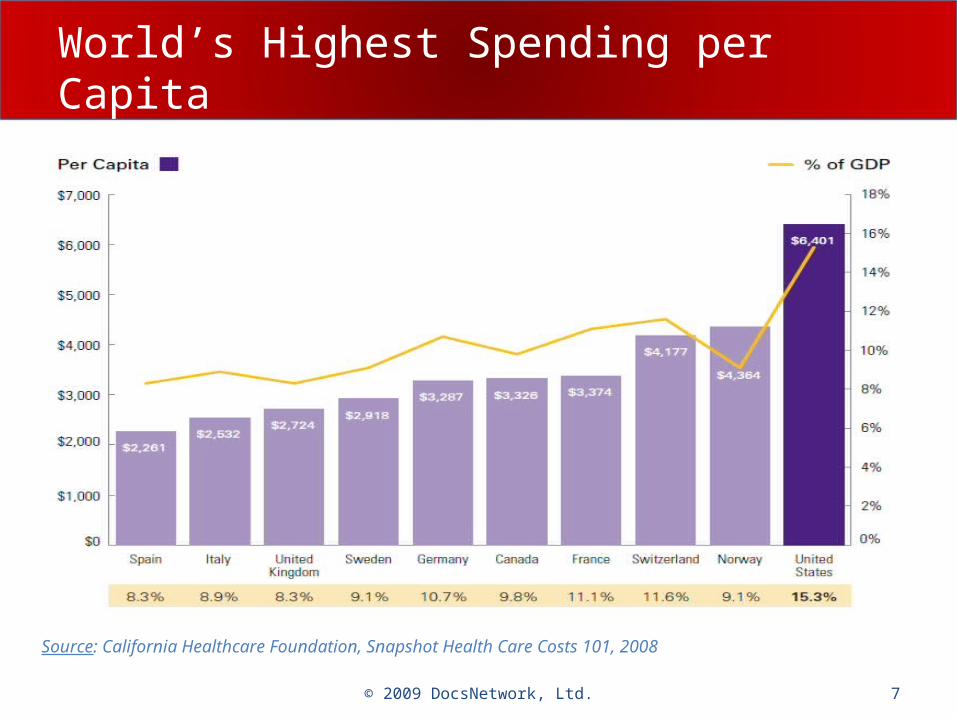
World’s Highest Spending per Capita
Source: California Healthcare Foundation, Snapshot Health Care Costs 101, 2008
7© 2009 DocsNetwork, Ltd.
Overview
Costs of Healthcare eHealth Vision Quality and Errors Clinical Information Technology Clinician Adoption Innovation and Transformation Flatteners and the Triple Convergence
© 2009 DocsNetwork, Ltd. 8
Governing for Standards, Certification
National eHealth Collaborative– Formerly American Health Information
Community (AHIC)
Healthcare Information Technology Standards Panel (HITSP)
Certification Commission for Health Information Technology (CCHIT)
National Coordinator for Health Information Technology (ONC)
© 2009 DocsNetwork, Ltd.
National eHealth Collaborative (NeHC)
Public-Private partnership– Includes all stakeholders– Successor to AHIC (2005) – gov’t. committee
Focus on health information network– Quality, safety, cost
Development aims– HIT systems– Infrastructure– Standards– Protections– Participation– Education
© 2009 DocsNetwork, Ltd.
HITSP Work Critical
Broad organization participation– Varied stakeholders
Public-private partnership Harmonize standards
– Data interchange– Vocabularies
Mobilize vendors– HIT– Medical devices
Driven by use cases
© 2009 DocsNetwork, Ltd.
CCHIT Ensures Interoperability
Mission: Accelerate adoption of HIT– Breadth of stakeholders
Certifies EHRs and their networks– Tests functionality against standards
– Ensures interoperability
– Embraces all SDOs
– Works with HITSP
Independent non-government entity
© 2009 DocsNetwork, Ltd.
HIMSS Vision for Change
Message to Pres. Obama and U.S. Congress Utilize HIT in healthcare reform
– Improve quality, reduce cost, enhance safety– EMRs, PHRs, e-prescribing– Facilitate interoperability
Immediate challenges– Leadership– Interoperability– Privacy and security– Electronic payments– Consumer empowerment– Funding
© 2009 DocsNetwork, Ltd.
Call to Action for New Administration
Invest $25 bil. on HIT (stimulus package)– Facilitate adoption of EMRs
• Hospitals and physicians• Government entities• Expand access
– Apply recognized standards• HITSP• CCHIT
– Permanently establish governing councils• Overarching coordinating entity
National eHealth Collaborative• HITSP and national standards harmonization body• Senior level HIT leader
– Expand Stark and Anti-kickback safe harbors
© 2009 DocsNetwork, Ltd.
Overview
Costs of Healthcare eHealth Vision Quality and Errors Clinical Information Technology Clinician Adoption Innovation and Transformation Healthcare’s Triple Convergence
© 2009 DocsNetwork, Ltd. 15
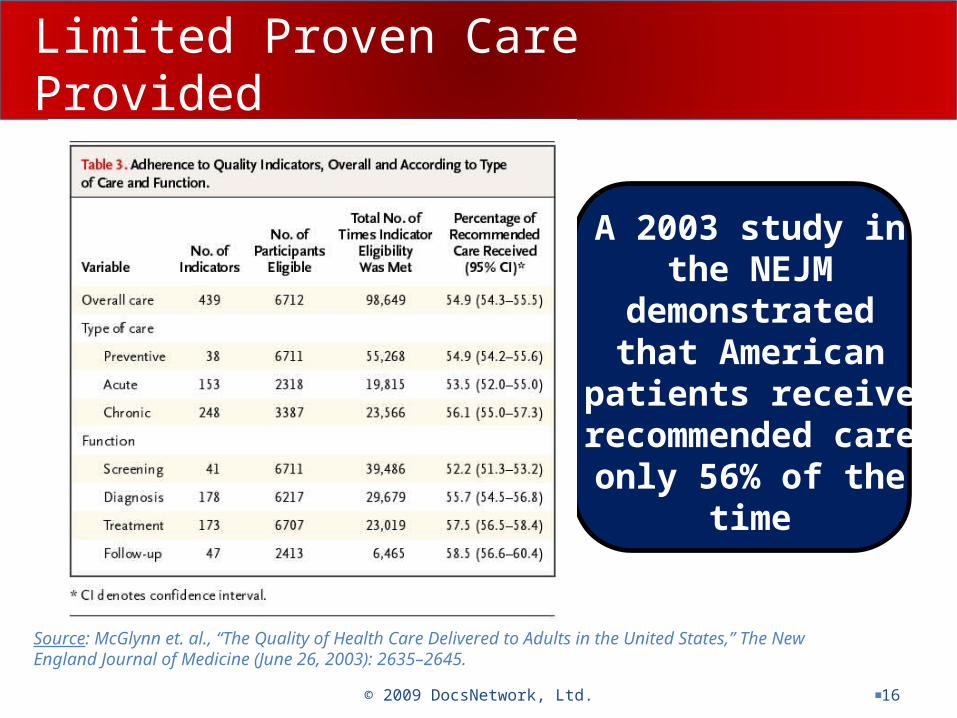
Limited Proven Care Provided
© 2009 DocsNetwork, Ltd. 16
A 2003 study in the NEJM
demonstrated that American patients
receive recommended care
only 56% of the time
Source: McGlynn et. al., “The Quality of Health Care Delivered to Adults in the United States,” The New England Journal of Medicine (June 26, 2003): 2635–2645.
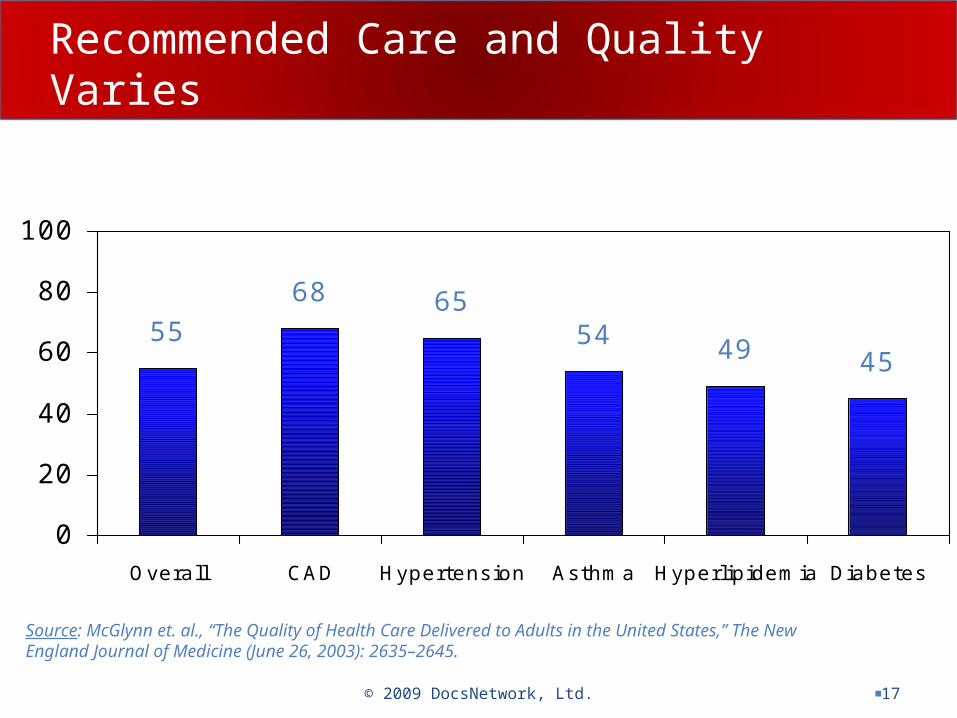
Recommended Care and Quality Varies
© 2009 DocsNetwork, Ltd. 17
Source: McGlynn et. al., “The Quality of Health Care Delivered to Adults in the United States,” The New England Journal of Medicine (June 26, 2003): 2635–2645.
55
68 6554 49 45
0
20
40
60
80
100
Overall CAD Hypertension Asthma Hyperlipidemia Diabetes
Percent Receiving Recommended Care
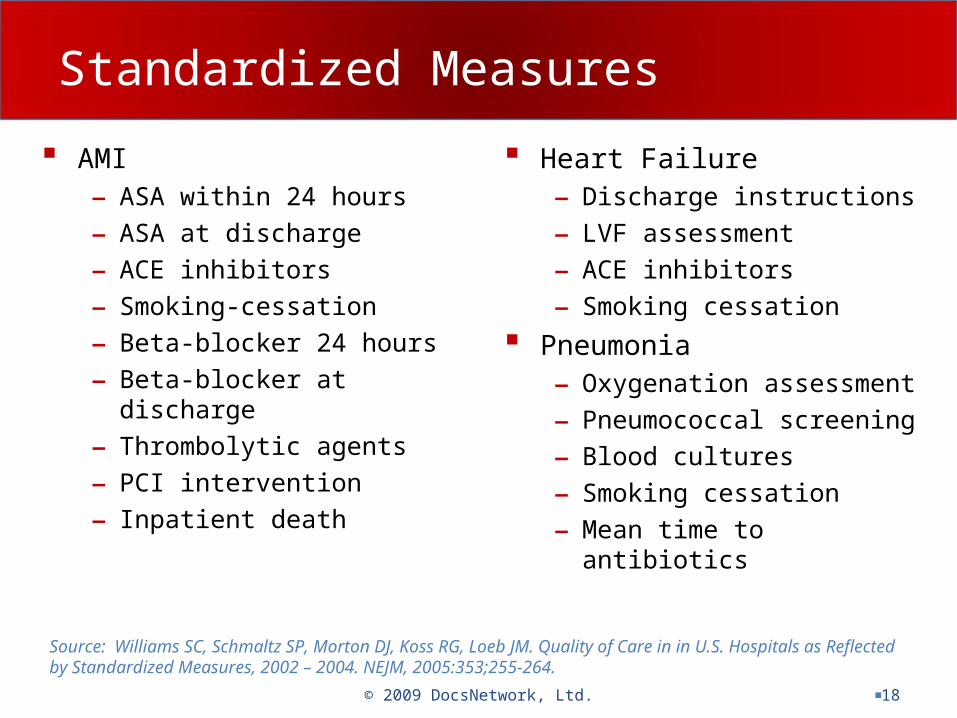
Standardized Measures
AMI– ASA within 24 hours
– ASA at discharge
– ACE inhibitors
– Smoking-cessation
– Beta-blocker 24 hours
– Beta-blocker at discharge
– Thrombolytic agents
– PCI intervention
– Inpatient death
Heart Failure– Discharge instructions
– LVF assessment
– ACE inhibitors
– Smoking cessation
Pneumonia– Oxygenation assessment
– Pneumococcal screening
– Blood cultures
– Smoking cessation
– Mean time to antibiotics
© 2009 DocsNetwork, Ltd. 18
Source: Williams SC, Schmaltz SP, Morton DJ, Koss RG, Loeb JM. Quality of Care in in U.S. Hospitals as Reflected by Standardized Measures, 2002 – 2004. NEJM, 2005:353;255-264.
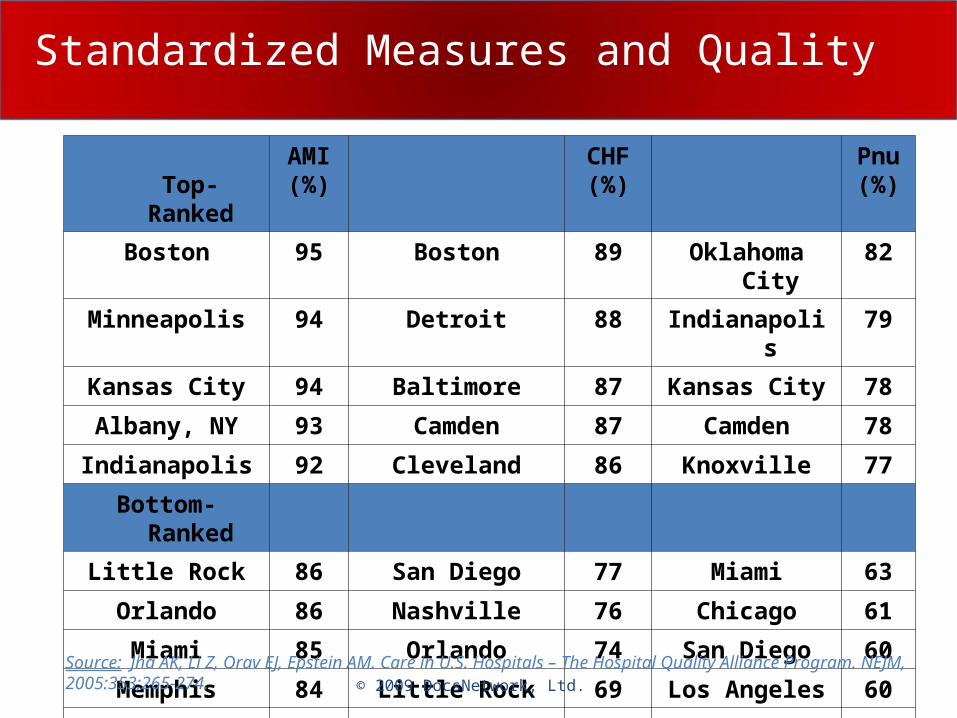
Standardized Measures and Quality
Top-RankedAMI(%)
CHF(%)
Pnu(%)
Boston 95 Boston 89 Oklahoma City 82
Minneapolis 94 Detroit 88 Indianapolis 79
Kansas City 94 Baltimore 87 Kansas City 78
Albany, NY 93 Camden 87 Camden 78
Indianapolis 92 Cleveland 86 Knoxville 77
Bottom-Ranked
Little Rock 86 San Diego 77 Miami 63
Orlando 86 Nashville 76 Chicago 61
Miami 85 Orlando 74 San Diego 60
Memphis 84 Little Rock 69 Los Angeles 60
San Bernadino 83 Lexington 68 San Bernadino 59
© 2009 DocsNetwork, Ltd.Source: Jha AK, Li Z, Orav EJ, Epstein AM. Care in U.S. Hospitals – The Hospital Quality Alliance Program. NEJM, 2005:353;265-274.
Variation in Performance
Academic institutions– AMI and CHF higher, pneumonia lower
Profit status– Not-for-profit higher for all 3 conditions
Geographic region– Midwest and Northeast outperforming the West
and South
Number of beds– Smaller hospitals do better with pneumonia
© 2009 DocsNetwork, Ltd. 20
Public Perceptions on Errors
Carelessness Incompetence Substandard providers
– Physicians
– Nurses
– Laboratory technicians
© 2009 DocsNetwork, Ltd. 21
Incompetent StarAverage Incompetent StarAverage
Fearing Clinical IT Lessons
Koppel– CPOE leads to increased errors– 22 types of errors facilitated
Garg – Unknown impact of CDS on outcomes– Performance improvement
Wears – Study results biased?– Foxes measuring the hen house
Cedars-Sinai abandons CPOE effort Failed CPOE
– 10+ years of the wrong dose?
© 2009 DocsNetwork, Ltd. 22
Perfectly Delivering Errors
Fragmented CPOE displays– Incomplete records
– Unintuitive display of data
Pharmacy inventory as CDSS– Delivering wrong doses
Concurrent digital and paper records– Lack of single patient data source
Inflexible ordering formats– Generate wrong orders
© 2009 DocsNetwork, Ltd. 23
Source: Koppel, et. al. Role of computerized physician order entry in facilitating medical errors. JAMA, 2005;293:1197-1203.
Overview
Costs of Healthcare eHealth Vision Quality and Errors Clinical Information Technology Clinician Adoption Innovation and Transformation Flatteners and the Triple Convergence
© 2009 DocsNetwork, Ltd. 24
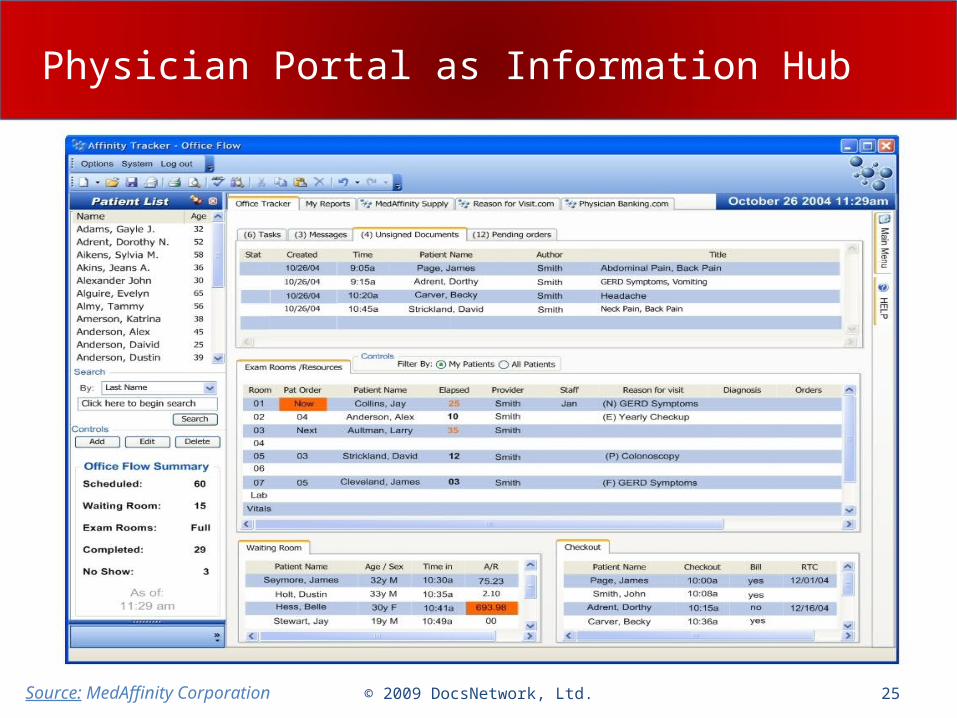
Physician Portal as Information Hub
Source: MedAffinity Corporation 25© 2009 DocsNetwork, Ltd.
Computer Physician Order Entry
Alerts to drug interaction, allergy, overdose
Accurate, up-to-date new drug information Drug-specific information
– Eliminates confusion over similar names
Improved communication– Physicians and pharmacies
© 2009 DocsNetwork, Ltd. 26
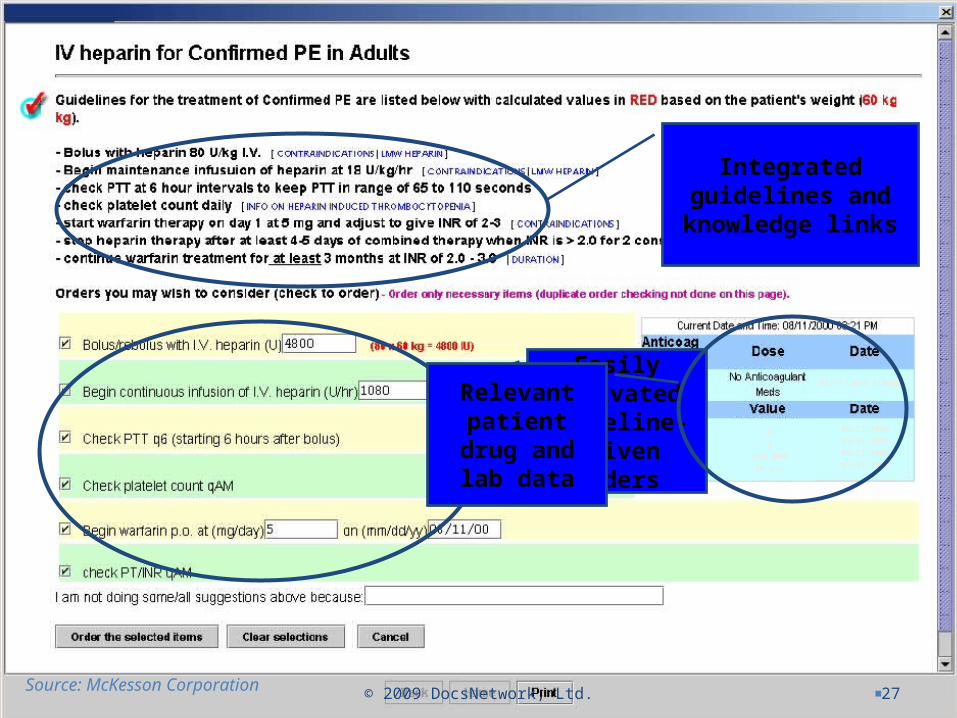
Heparin HEO Slide
© 2009 DocsNetwork, Ltd. 27
08/11/2000 8:00pm
35
1
165,000
76 mcm3
08/11/2000
08/11/2000
08/11/2000
08/11/2000
Integrated guidelines and
knowledge links
Easily activated guideline-
driven orders
Relevant patient drug and lab data
Source: McKesson Corporation
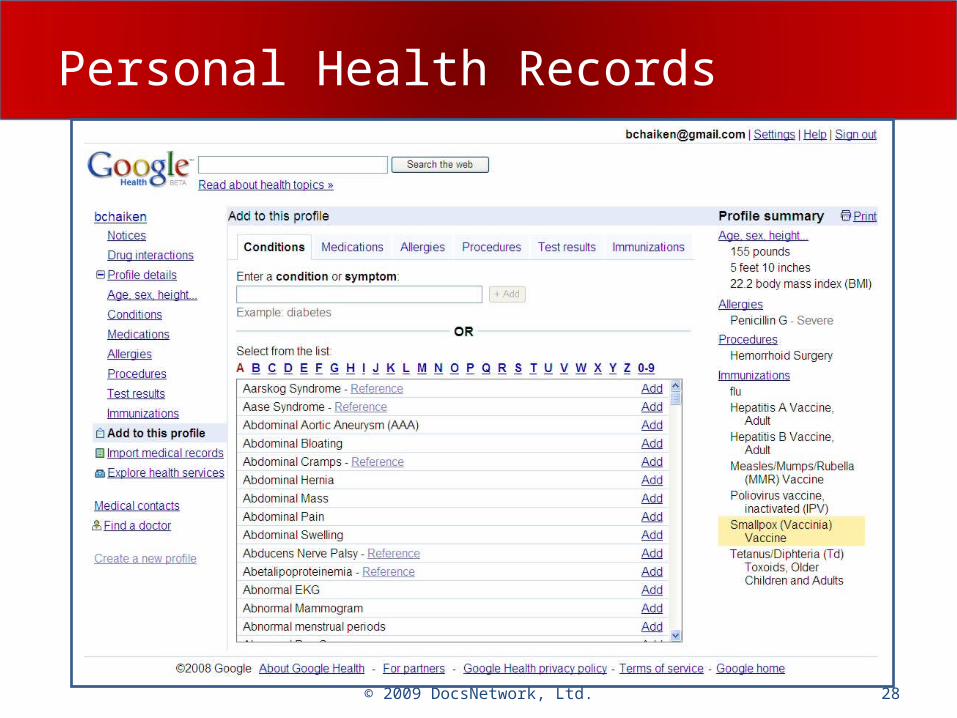
Personal Health Records
28© 2009 DocsNetwork, Ltd.
CCR Offers Key Data Points
CCR identifying information– Physicians, dates, purpose of referral
Patient identifying information– Unique patient identifiers
Patient insurance/financial information– Eligibility
Advance directives– Living wills and proxies
© 2009 DocsNetwork, Ltd. 29

CCR Comprehensive
Patient health status– Conditions, diagnosis, family history– Adverse reactions, allergies– Social history, risk factors, immunizations– Medications– Vita signs, lab results, procedures
Care documentation Care plan recommendations Practitioners
© 2009 DocsNetwork, Ltd. 30

Overview
Costs of Healthcare eHealth Vision Quality and Errors Clinical Information Technology Clinician Adoption Innovation and Transformation Flatteners and the Triple Convergence
© 2009 DocsNetwork, Ltd. 31
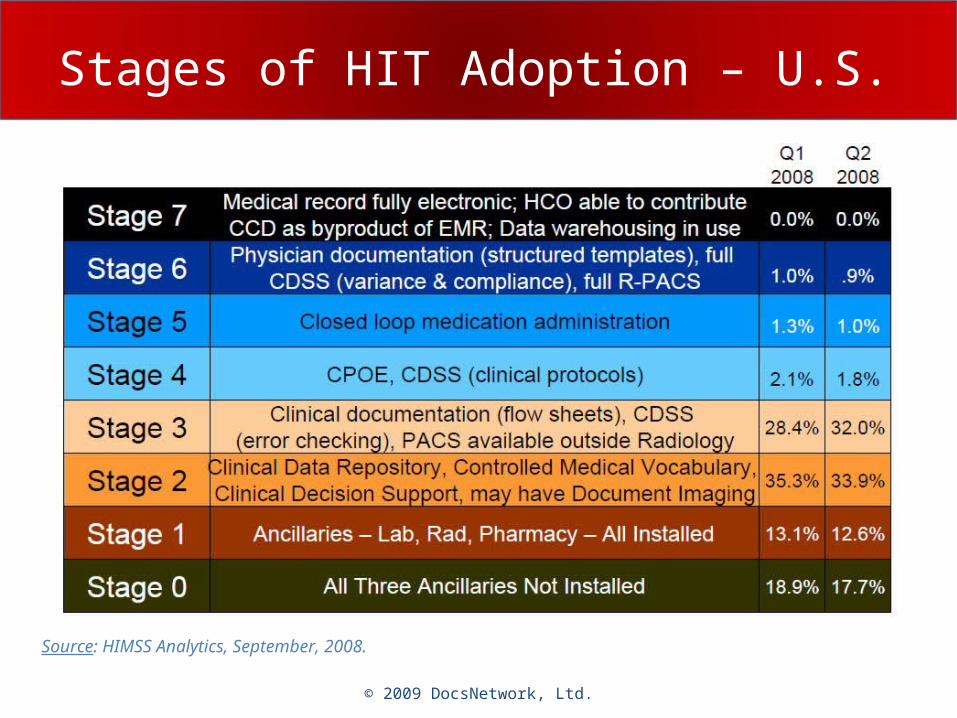
Stages of HIT Adoption – U.S.
© 2009 DocsNetwork, Ltd.
Source: HIMSS Analytics, September, 2008.
Secure Clinician Adoption
Workflow– Impact on patient care
• Quality
• Cost
– Efficiency - time• Obtain information
• Patient encounter
• Record findings
© 2009 DocsNetwork, Ltd.
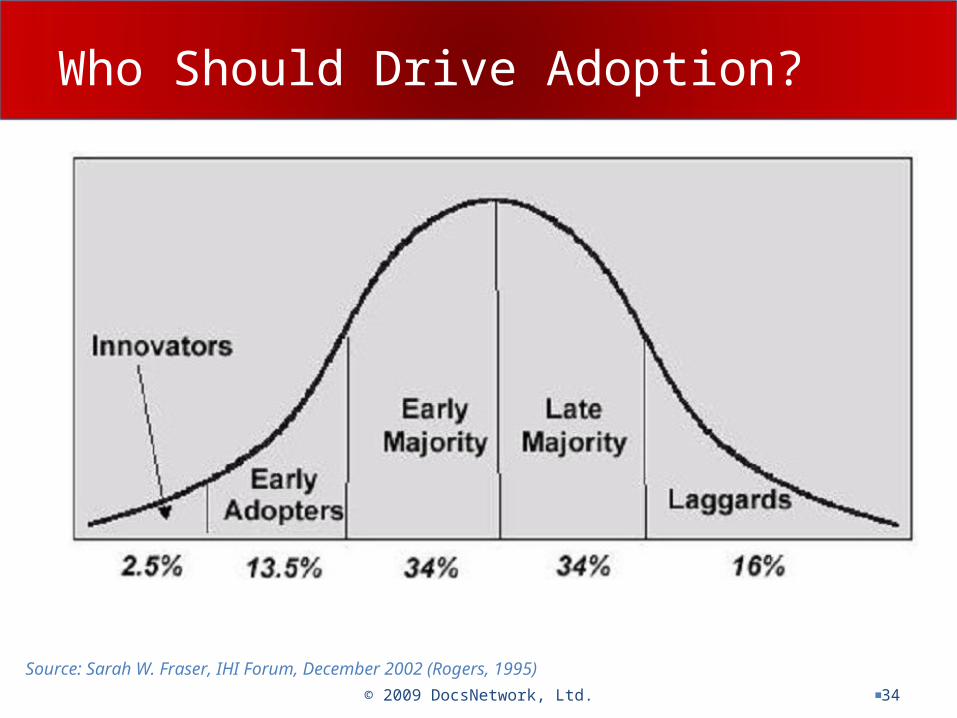
Who Should Drive Adoption?
© 2009 DocsNetwork, Ltd. 34
Source: Sarah W. Fraser, IHI Forum, December 2002 (Rogers, 1995)
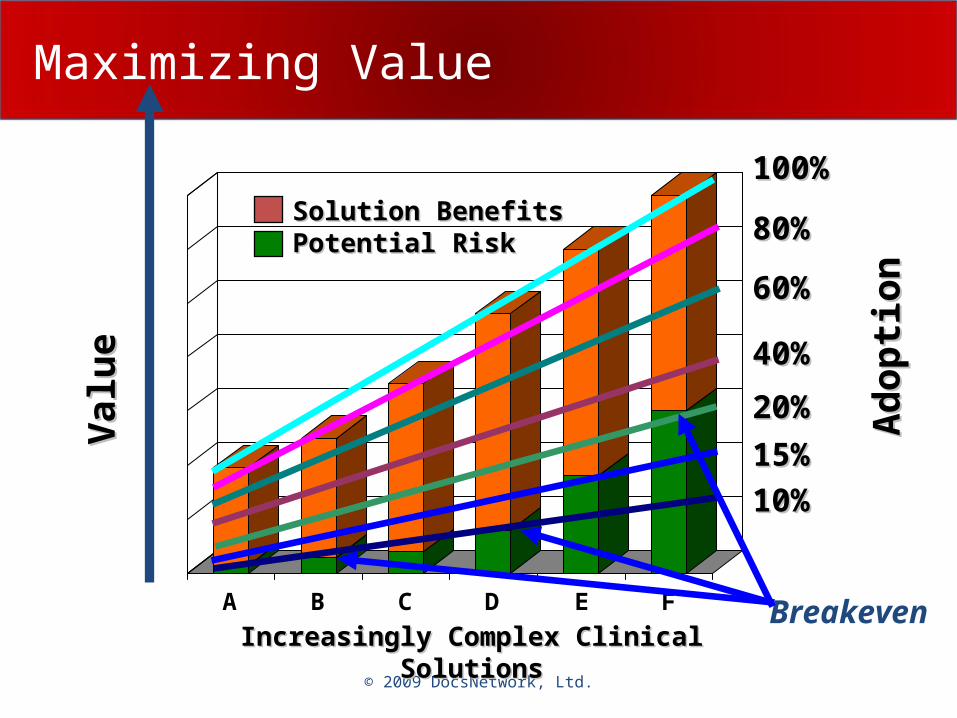
Maximizing Value
A B C D E F
© 2009 DocsNetwork, Ltd.
Val u
eV
al u
e
80%80%
60%60%
40%40%
20%20%
100%100%
15%15%
10%10%
Ad
op
tion
Ad
op
tion
Increasingly Complex Clinical Increasingly Complex Clinical SolutionsSolutions
Solution BenefitsSolution BenefitsPotential RiskPotential Risk
Breakeven
Overview
Costs of Healthcare eHealth Vision Quality and Errors Clinical Information Technology Clinician Adoption Innovation and Transformation Flatteners and the Triple Convergence
© 2009 DocsNetwork, Ltd. 36
Clinical Transformation Needed
Utilize clinical technologies Impact clinical processes Enhance quality Achieve efficiencies Necessary focus
– Clinical strategy
– Clinical business
– Process redesign
– Change management
© 2009 DocsNetwork, Ltd. 37
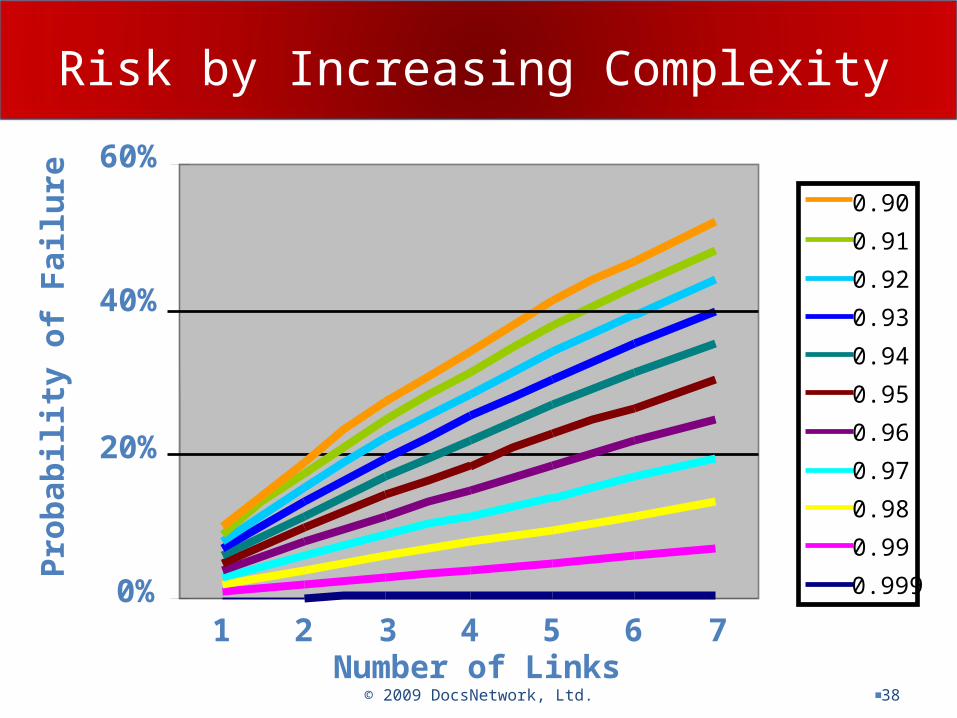
Risk by Increasing Complexity
© 2009 DocsNetwork, Ltd. 38Number of Links
Pro
bab
ilit
y o
f F
ailu
re
0.999
0.99
0.98
0.97
0.96
0.95
0.94
0.93
0.92
0.91
0.90
0%
20%
40%
60%
1 2 3 4 5 6 7
Process Redesign Tasks
Current state value stream map– Process and its sub-processes
– Collect baseline metrics
Future state value stream map– Detailed workflows
– Role definition
– Align committee structures
– Policy/procedure definition
© 2009 DocsNetwork, Ltd. 39
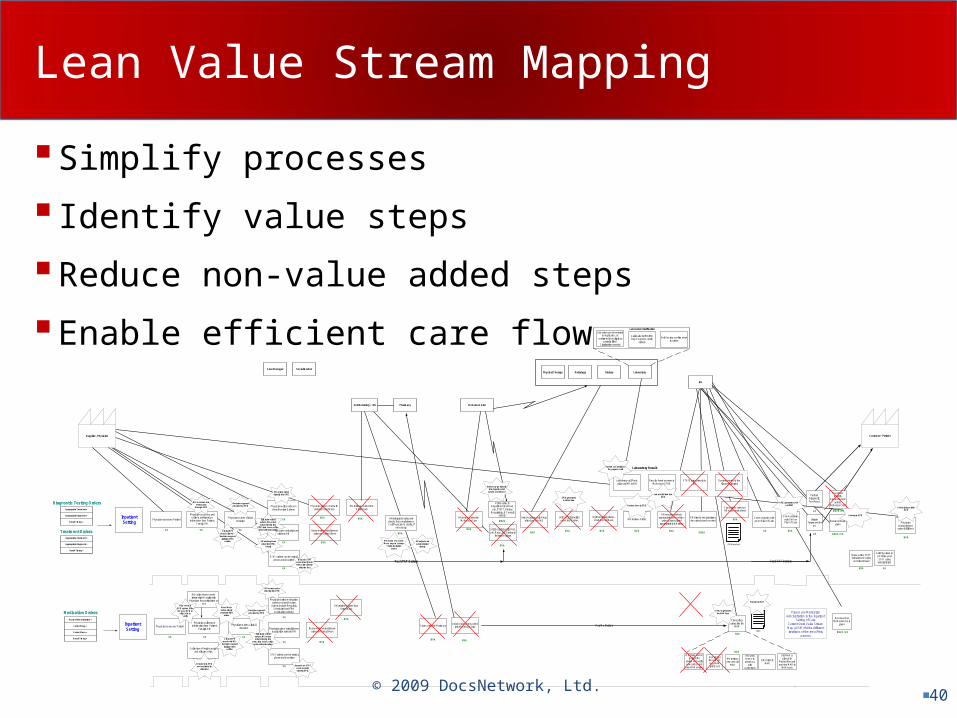
Lean Value Stream Mapping
Simplify processes
Identify value steps
Reduce non-value added steps
Enable efficient care flow
© 2009 DocsNetwork, Ltd.40
RN review new order.Move step to 1st step
of adminstrationENVA
RN enters order intoMcKesson Star
Unit Secretary / RN Pharmacy
RN
Case Manager Social Worker
Physician assesses Patient
Physician accesses andcollects additional pt.
information from Patient,Family, RN
Physician makes clinicaldecision
Physician gives verbal/phoneorder to RN
Physician places chart withorder in Order Rack
RN retrieves order fromOrder Rack
Faxes order to Pharmacy
Prints order inDepartment (For Rad,Lab, PT/OT, Dietary,
Respiratory, & Consultorders)
Unit Secretary calls Rad,Lab, Resp, SS, Dietary to
fast track orders
Unit Secretary writesorder into Kardex
Unit Secretary calls Respafter 2pm for EKG
Unit Secretary placeschart in Chart Rack RN reviews Order
RN ensures order isappropriate and confirms
order is transcribedappropriately in Kardex
Transcribesorder into the
MAR
RN directs and prioritizesthe order based on need
Transcribes order onRN's own work sheet
Administersfirst dose Rx
to pt.
Call Physician re:pt. status postSTAT orderadministered
InpatientSetting
Supplier - Physician Customer - Patient
Physician writes order onchart (Routine Orders)
McKesson Star
DietaryRadiologyPhysical Therapy Laboratory
VAVA
STAT orders can be verbal,phone and/or written
Documents inMAR when Rx is
given
VA
VA
VA
VA
Nurse writes verbal/phoneorder on Order Sheet
NVA
NVA
NVA
NVA
NVA
ENVA
NVA
For STAT Orders
NVANVA NVA NVA NVA
ENVA
Diagnostic Testing OrdersAppropriate Treatment =
Appropriate Diagnosis =
Broad Timing =
Appropriate Treatment =
Appropriate Diagnosis =
Broad Timing =
Treatment Orders
NVA
NVA
VA NVA
InitiateTreatment for
pt.
VA
VA
VA
Document caregiven
ENVA / VA
ENVA / VA
ENVA / VA
For STAT Orders
For Rx Order
RN interprets order andchecks for completeness.Call Physician to clarify, if
necessary.
Communicates withpt. on Plan of Care
PerformDiagnosticTest for pt.
Physicianacknowledgesorder fulfillment
Communicateswith CNA onPlan of Care
Off going and ongoing RNs
review and verifynew orders and
new MAR entries
At midnightthe new 24-hour MARprints out
RN reviewsnew and old
MAR
RN sendmemo topharmacy
withcorrections
RN correctsMAR
Old MAR isplaced in
Medical Recordand new MAR in
MAR book
NVA
NVA
RN Worksheet
MAR
VA
NVA
Route of administration =
Correct Drug =
Correct Dose =
Broad Timing =
Medication Orders
Nurse writes STATverbal/phone order
on Order Sheet
NVA
Physician assesses Patient
Physician collects pt.information from Patient,
Family& RN
Physician makes clinicaldecision
InpatientSetting
VAVA VA
Physician gives verbal/phonemedication order to RN
Physician writes medicationorder on chart (Routine
Orders include RegularlyScheduled and PRNmedication orders)
STAT orders can be verbal,phone and/or written
VA
VA
VA
Nurse writes verbal/phoneorder on Order Sheet
NVA
Please see MedicationAdministration in the Inpatient
Setting of CareCurrent State Value StreamMap (cVSM) for the differentiterations of the rest of this
process
Unit Sectary enters orderinto McKesson Star
NVA
RN retrieves order fromOrder Rack
NVA
Post testsresult to
medical recordand/or
McKesson Star
RN collect home medsinformation & verify with
Physician for continuation ornot
Laboratory call Panicvalues to MD or RN
Results faxed or enter inMcKesson STAR
STATS print directly toED
Routine printed to thefloor at midnight
Lab order can be enteredin duplicates, or
confirmed in multiple orpartially filled.
Clarification needed
Call made to MD/RN/Dept. Supvr to clarify
orders
Unit Sectary confirm whatto order
Lab Order Clarification
Laboratory Result
MD accesses andenters data
through EPIC
Decision supportprovided by EPIC
MD enters orderdirectly into EPIC
Eliminate verbalorders; MD entersorder directly into
EPIC from home, officeand/or other location
RN enters phoneorder into EPIC.
Rarely
Barcode STATmeds directly intoMAR with order in
after the fact
RN adjust medadminstration
timing.
Order may go directlyinto departmental
system or print out
EPIC generatesKardex view
Review done in EPIC
Lab results feed intoEPIC
System can notify byfax, pager or cell
EPIC generates CNAworklist
Enter into EPIC
Acknwledge withinEPIC
Home Med inEPIC system if theMD uses EPIC in
office -RN toverify
Home Medsautomaticalypopulate first
order
Decision supportprovided by EPIC
MD enters orderdirectly into EPIC
Eliminate verbalorders; MD entersorder directly into
EPIC from home, officeand/or other location
Barcode on STATmeds recordsorder in EPIC
EPIC to generatethe MAR View
Electronic MAR
Collection of height, weightand allegies of pt.
Entered into EPICand avaliable for
clinicians
Clinical RPhround with MD -decision support
before orderwritten
Clinical RPhround with MD -decision support
before orderwritten
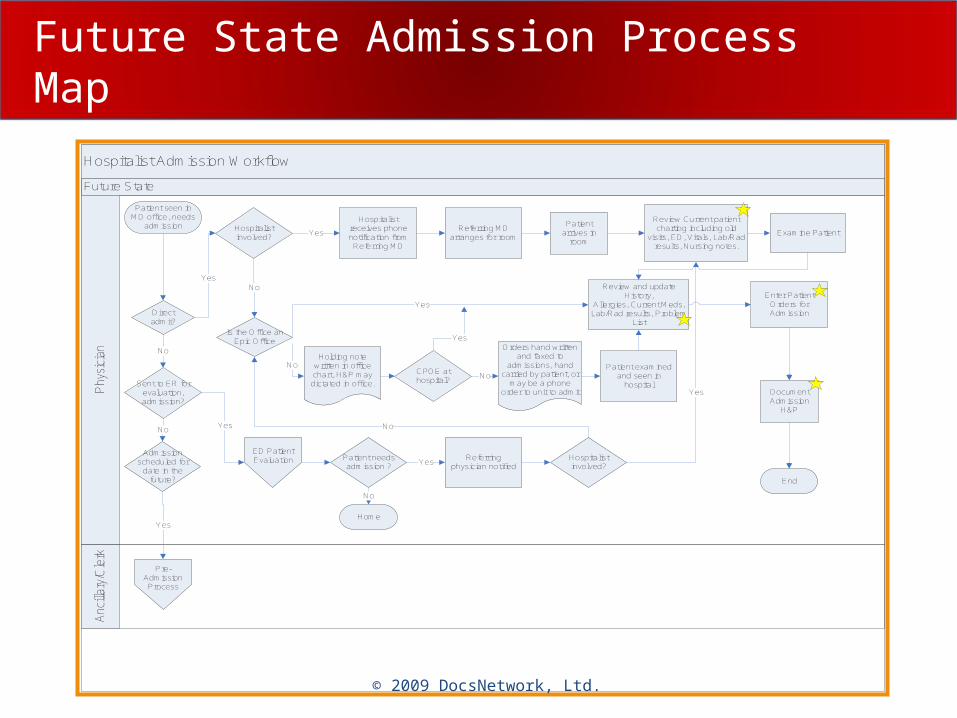
Future State Admission Process Map
© 2008 DocsNetwork, Ltd.
Future State
Hospitalist Admission Workflow
Anc
illar
y/C
lerk
Phy
sici
an
Direct admit?
No
Yes
Patient seen inMD office, needs
admission
Patient needs admission ?
Home
End
No
Holding note written in office chart, H&P may dictated in office.
Orders hand written and faxed to
admissions, hand carried by patient, or
may be a phone order to unit to admit
Hospitalist involved?
Yes
Yes
Referring physician notified
Patient examined and seen in
hospital
Hospitalist involved?
No
No
Yes
Sent to ER for evaluation, admission?
Yes
Admission scheduled for
date in the future?
No
Yes
ED Patient Evaluation
Is the Office an Epic Office
No
Enter Patient Orders for Admission
Review and update History,
Allergies, Current Meds, Lab/Rad results, Problem
List
Document Admission
H&P
Hospitalist receives phone notification from
Referring MD
Referring MD arranges for room
Patient arrives in
room
Review Current patient charting including old
visits, ED, Vitals, Lab/Rad results, Nursing notes.
Examine Patient
Pre-Admission Process
CPOE at hospital?
No
Yes
Yes
© 2009 DocsNetwork, Ltd.
Path Innovation of Clinical Processes
Required subject matter experts– Process improvement
– Clinical content and evidence-based medicine
– IT system design
Educating experts– Exchange knowledge
Cross training Teamwork
– Formation of long-standing working groups
© 2009 DocsNetwork, Ltd.
Well Designed Systems Succeed
© 2009 DocsNetwork, Ltd.
Requires Practice and Teamwork
© 2009 DocsNetwork, Ltd.
Summarizing Clinical Transformation
“every system is perfectly designed to achieve exactly the results it gets”
- Don Berwick, MDInstitute of Healthcare Improvement
© 2009 DocsNetwork, Ltd.
Overview
Costs of Healthcare eHealth Vision Quality and Errors Clinical Information Technology Clinician Adoption Innovation and Transformation Flatteners and the Triple Convergence
© 2009 DocsNetwork, Ltd. 46
Friedman’s Ten Flatteners
Fall of the Berlin Wall (Soviet Union) Internet, e-mail and browsers Workflow software
– Separating tasks
Open sourcing Out-sourcing Off-shoring Supply-chaining In-sourcing In-forming The steroids
© 2009 DocsNetwork, Ltd. 47
The Triple Convergence
Global Web-enabled playing field Combining new technologies with new processes Universal access to computers and Internet
© 2009 DocsNetwork, Ltd. 48
Triple Convergence I
Global, Web-enabled playing field Multiple forms of collaboration
– Sharing of knowledge real-time
– Irrespective of geography
– Soon, irrespective of language
© 2009 DocsNetwork, Ltd. 49
Triple Convergence II
Combining new technology with new processes– Steam engines versus electric motors
• Redesign of assembly lines
• Need for critical mass of new engineers and architects
– Snail mail versus email• PDF files, Adobe Reader
Doing things differently
© 2009 DocsNetwork, Ltd. 50
Triple Convergence III
Access by billions to computers and the Web– Knowledge easily obtained
– Collaboration no longer limited by geography
– Instantaneous sharing of discoveries
© 2009 DocsNetwork, Ltd. 51
Healthcare’s Triple Convergence
Increasing investment– Cost of doing business
Government and payor incentives Increasing use of IT
– EMR, PHR, HER, CCR
– Computerized provider order entry (CPOE)
– Clinical decision support system (CDSS)
– Physician and patient portals
© 2009 DocsNetwork, Ltd. 52
Path Innovation of Clinical Processes
Required subject matter experts– Process improvement
– Clinical content and evidence-based medicine
– IT system design
Educating experts– Exchange knowledge
Cross training Teamwork
– Formation of long-standing working groups
© 2009 DocsNetwork, Ltd. 53
Successful Use of HIT
Develop good plans– Change as needed– Include all stakeholders
Invest in governance Service the clinician
– Patient-specific data– Recognize workflows– Design easy to use reports
• Balanced scorecards Transform use of data and information
– Focus on strategic vision– Revise processes– Utilize IT to deliver to transformation
Continually monitor and improve processes Innovate
© 2009 DocsNetwork, Ltd.
African Proverb
Every morning in Africa, a gazelle wakes up.It knows it must run faster than the fastest lion or it will be killed.Every morning a lion wakes up.It knows it must outrun the slowest gazelle or it will starve to death.It doesn’t matter whether you are a lion or a gazelle.
When the sun comes up, you better start running.
© 2009 DocsNetwork, Ltd.
References Chaiken BP. Round healthcare in a flat world. Patient Safety and Quality
Healthcare. 2006;3(3):12-13. Chaiken BP. Path innovation: transcending automation. Patient Safety
and Quality Healthcare. 2005;2(3):46-47. Friedman TL. The World is Flat. 2005. New York: Farrar, Straus and
Giroux. Snapshot health care costs 101, 2008. California Healthcare Foundation.
2008. Chaiken BP. Useable clinical evidence-based guidelines…For real. Patient
Safety and Quality Healthcare. 2005;2(1):14-16. Chaiken BP. Using IT to drive teamwork and patient safety. Journal of
Quality Health Care, 2003;2(1):19-20. Chaiken BP. Revolutionary HIT: Cure for insanity. Patient Safety and
Quality Healthcare. 2007;4(6):10-11. Chaiken BP. Strategies for Success: Clinical HIT implementation. Patient
Safety and Quality Healthcare. 2008:5(4):28-31. Chaiken BP. Healthcare IT: Slogan or solution? Patient Safety and Quality
Healthcare. 2008;5(1):6. www.HIMSS.org www.CCHIT.org
© 2009 DocsNetwork, Ltd.
References
Chaiken BP, Holmquest DL. Patient safety: Modifying processes to eliminate medical errors. Journal of Quality Health Care. 2002;1(2):20-23.
Chaiken BP. Clinical decision support: Success through smart deployment. Journal of Quality Health Care, 2002:1(4):15-16.
Chaiken BP. Technology helps eliminate medical errors. Health Care Quality Means Business: Special Supplement to Managed Care. 2003;12(1):15-17.
Chaiken BP. Choosing clinical IT tools that matter to physicians. Health Management Technology. 2002;Sept.:20-22.
Chaiken BP. Physician adoption of technology linked to providing benefits. Journal of Quality Health Care, 2002;1(2):25-27.
Chaiken BP. Useable clinical evidence-based guidelines…For real. Patient Safety and Quality Healthcare. 2005;2(1):14-16.
Chaiken BP. Using IT to drive teamwork and patient safety. Journal of Quality Health Care, 2003;2(1):19-20.
Chaiken BP. Mind the Gap. Health and Hospital Networks Most Wired Online, March 9, 2005.
© 2009 DocsNetwork, Ltd.
References Williams SC, Schmaltz SP, Morton DJ, Koss RG, Loeb JM. Quality of Care in in U.S.
Hospitals as Reflected by Standardized Measures, 2002 – 2004. NEJM, 2005:353;255-264.
Health Information Technology in the United States: The Information Basis for Progress. Robert Wood Johnson Foundation, MGH Institute for Health Policy, George Washington school of Public health and Health Sciences © 2006 Robert Wood Johnson Foundation.
Koppel, et. al. Role of computerized physician order entry in facilitating medical errors. JAMA, 2005;293:1197-1203.
Garg AX, et. al. Effect of computerized clinical decision support systems on practitioner performance and patient outcomes. JAMA, 2005;293:1223-1238.
Wears RL, Berg M. Computer technology and clinical work. JAMA, 2005;293:1261-1263.
Stoll K, Jones K, Health Care: Are you better off today than you were four years ago? Families USA, September 2004.
Robinson AR, Hohmann KB, Rifkin JI, Topp D, Gilroy CM, Pickard JA, Anderson RJ. Physician and public opinions on quality of health care and the problem of medical errors. Arch Intern Med 2002;162:2186-90.
© 2008 DocsNetwork, Ltd. 58
Barry P. Chaiken, MD, MPH, FHIMSSChief Medical OfficerDocsNetwork, Ltd.
© 2009 DocsNetwork, Ltd. 59