Primary mediastinal B-cell lymphoma and mediastinal gray zone ...

of 100
Upload
ghina-ninditasariCategory
view
28download
0description
Tumor MediastinumRizki Yaruntradhani Pradwipa
Anatomy
Mediastinum is the region between the pleural sacs. Three compartments :AnteriorMiddlePosteriorHarrisons priciples of internal medicine. 17th ed
Anatomy of the MediastinumBoundariesSuperior- Thoracic inletInferior- DiaphragmAnterior- SternumPosterior- Vertebral bodiesLateral- Pleura
Mediastinum Superior (1)Batas atas: Iga 1 sampai corpus v. Th. 1 (thoracic inlet)
Batas posterior: V Th. 1-4
Batas bawah: Angulus ludovici s/d V. Th 4 (plane of sternal angle)
Mediastinum Anterior (2)Batas atas: Angulus ludovici s/d V. Th 4 (plane of sternal angle)
Batas anterior: Corpus sternalis dan Pr. Xyphoideus
Batas posterior: Pericardium
Batas bawah: Diafragma
The anterior mediastinum extends from the sternum anteriorly to the pericardium and brachiocephalic vessels posteriorly
contains the thymus gland, the anterior mediastinal lymph nodes, and the internal mammary arteries and veins. Harrisons priciples of internal medicine. 17th ed
Mediastinum Medial (3)Batas atas: Angulus ludovici s/d V. Th 4 (plane of sternal angle)
Batas anterior: Perikardium
Batas posterior: Pericardium
Batas bawah: Diafragma
AnatomyThe middle mediastinum lies between the anterior and posterior mediastina
contains the heart; the ascending and transverse arches of the aorta; the venae cavae; the brachiocephalic arteries and veins; the phrenic nerves; the trachea, main bronchi, and their contiguous lymph nodes; and the pulmonary arteries and veins. Harrisons priciples of internal medicine. 17th ed
Mediastinum Posterior (4)Batas atas: Angulus ludovici s/d V. Th 4 (plane of sternal angle)
Batas anterior: Perikardium
Batas posterior: V. Th 5-12
Batas bawah: Diafragma
AnatomyThe posterior mediastinumbounded by the pericardium and trachea anteriorly and the vertebral column posteriorly
contains the descending thoracic aorta, esophagus, thoracic duct, azygos and hemiazygos veins, and the posterior group of mediastinal lymph nodes.Harrisons priciples of internal medicine. 17th ed
Menurut KlinisiMediastinum anterior:mediastinum anterior dan medial diperluas sampai ke mediastinum superior, anterior dari bidang yg mell trakhea.
Mediastinum medial: mediastinum posterior, sebagian mediastinum superior, sebelah posterior dari bidang yang melewati anterior trakhea.
Mediastinum posterior:korpus vertebrae beserta ruang paravertebra, termasuk saraf simpatis (asal dari tumor neurogenik)
DEFINISISpecific lesions that present as a mass in the mediastinum may be discovered incidentally or identified during evaluation of thoracic or systemic symptoms
Chest 2005;128;2893-2909
ANTEROSUPERIOR MEDIASTINUM(%)
Thymic neoplasms33Lymphomas19Germ cell tumors 17Benign 9 Malignant 8Carcinoma 11Cysts 8Mesenchymal 4Endocrine 6Other 2
MIDDLE MEDIASTINUM (%)
Cysts 61Lymphomas 21Mesenchymal 8Carcinoma 6Other 4
POSTERIOR MEDIASTINUM (%)
Neurogenic 53Benign 41Malignant 12Cysts 32Mesenchymal 9Endocrine 2Other 4
The likelihood of malignancy is influenced primarily by the following three factors: mass location;patient age; the presence or absence of symptoms.Chest 2005;128;2893-2909
Mediastinal Masses
Compartment% MalignantAnterosuperior59Middle29Posterior16
Presenting Symptoms of Mediastinal MassChest pain 33Dyspnea 20Cough 18Fever, chills 19Weight loss 9Superior vena caval syndrome 8Myasthenia gravis 7Fatigue 6Dysphagia 4Night sweats 3
The most common symptoms at presentation cough (60%)chest pain (30%); fevers/ chills (20%); dyspnea (16%). Most symptoms can be categorized into the following two groups:localizing symptomssystemic symptomsChest 2005;128;2893-2909
Localizing symptomssecondary to tumor invasion. Common :respiratory compromise; dysphagia; paralysis of the limbs, diaphragm, and vocal cords; Horner syndrome; superior vena cava syndromeChest 2005;128;2893-2909
Chest 2005;128;2893-2909
Systemic symptomstypically due to the release of excess hormones, antibodies, or cytokines. A classic example is hypercalcemia, which is caused by a parathyroid adenoma.
Chest 2005;128;2893-2909
Chest 2005;128;2893-2909
Noninvasive diagnostic proceduresCT MRI Ultrasonography Radionuclide scanning Biochemical markers
CTRoutine. More detail, invasion into adjacent structure pleural or lung parenchymal metastases. Sensitive method of distinguishing between fatty, vascular, cystic, soft tissue mass. Differentiation in solid and cystic mass 100%. Solid mass-- homogeneity or inhomogeneity. Contrast enhancement of vessel.Cannot differentiate between benign and malignant tumor.
MRIAdditional useful information in separation mediastinal tumor from vessels and bronchi. Superior to CT in evaluation intraspinal extention or intrathecal spread of paravertebral mass.
Ultrasonography-- Differentiation in solid and cystic.
Radionuclide scanningThyroid I131, I123. Parathyroid Tc 99m. Octreotide Somatostatin analogue, identifiy small cell carcinoid tumors of lung. Tc-99mpertechnate scan identified gastric mucosa in suspected neuroenteric cyst in posterior portion of visceral compartment. Gallium 67 differentiate benign from malignant anterior mediastinal mass.
Biochemical markers -fetoprotein, -human chorionic gonadotropin( HCG), either one or both elevated in nonseminomatous malignant germ cell tumor. Excess than 500 ng/ml, can start chemotherapy without a tissue biopsy. 7-10% pure seminoma may elevated - HCG but nor exceed 100 ng/ml, but elevated -fetoprotein is never present.
Biochemical markersAll infant and children with paravertebral mass should evaluated for excessive norepinephrine and epinephrine production. Ferritin level for neuroblastoma.Antiacetylcholine receptor antibodies thymoma.Positron emission tomographic scanning Differentiating a noninvasive thymoma.
Invasive biopsy procedure Choice of invasive diagnostic procedures depends on:Presence or absence of local symptoms.Location and extent of lesionPresence or absence various tumor marker.
Percutaneous transthoracic fine-needle aspirationCT or sono-guide. Anterior compartment lesionpositive result nearly 100%. Complication is life-threating hemorrhage form injury internal mammary artery during parasternal needle biopsy. CT-guide is much better.
Percutaneous transthoracic fine-needle aspirationVisceral compartmenttransthoracically with passage of needle through lung. Success rate 75%. Complication pneumothorax is low. Paravertebral massCT-guide biopsy 100% success rate.
MediastinoscopyAnterior mediastinal tumor, the mediastinoscopy is NOT appropriate for biopsy May be obtain by cervical substernal extended mediastinotomy or anterior mediastinotomy. Lymph node confined to visceral compartment, biopsy via a standard cervical mediastinoscopy is used.
Thank You
ThymomasThymic carcinomaThymic CarcinoidMediastinal GCTMediastinal Teratomas (benign)Mediastinal SeminomaMediastinal Nonseminomatous GCTsMediastinal GoiterMediastinal Parathyroid AdenomaPrimary Mediastinal LymphomaHodgkin DiseaseNon Hodgkin LymphomaChest 2005;128;2893-2909Anterior Mediastinum
ThymomaPresentationMost common primary anterior mediastinal tumorM=F, most >40Most patients are asymptomaticchest pain, cough, or dyspnea related to tumor compression or invasion Half of patients suffer have associated parathymic syndromesmyasthenia gravishypogammaglobulinemiapure red cell aplasiaChest 2005;128;2893-2909
Myasthenia gravis is most frequent in women and is associated with thymomaSymptoms include diploplia, ptosis, dysphagia, weakness, and fatigue.Thirty percent to 50% of patients with thymomas have myasthenia gravis, compared to 10 to 15% of patients with myasthenia gravis who have a thymoma.
Chest 2005;128;2893-2909Tumors of the Anterior Mediastinum
Thymomas chest radiographwell-defined lobulated mass in the anterosuperior mediastinum, typically anterior to the aortic root.contrast-enhanced thoracic CT scanning encapsulated, welldefined, soft-tissue mass, often with hemorrhage, necrosis, or cyst formationcan also appear predominantly cystic with a nodular componentChest 2005;128;2893-2909Tumors of the Anterior Mediastinum
Radiographic Larger thymomas are commonly unilateral and tend to protrude into one hemithorax In rare cases, thymomas conform to the cardiac contour and may simulate cardiac enlargement on frontal radiographs Rosado-de-Christenson ML, Galobardes J, Moran C. Thymoma: radiologic-pathologic correlation. RadioGraphics 1992;12:151-168Rosado-de-Christenson ML, Galobardes J, Moran C. Thymoma: radiologic-pathologic correlation. RadioGraphics 1992;12:151-168Tumors of the Anterior Mediastinum
Computed Tomographic Computed tomography of thymomas typically reveals a homogeneous soft tissue mass located in the region of the thymus, and closely related to the root of the aorta and pulmonary arteryDo YS, JG, Lee BH, Kim KH, Oh YW, Chin SY, et al. CT findings in malignant tumors of the epithelium. J CT 1995; 19:192-197 The mass usually projects to one side of the midline, and less frequently exhibits bilateral growth Do YS, JG, Lee BH, Kim KH, Oh YW, Chin SY, et al. CT findings in malignant tumors of the epithelium. J CT 1995; 19:192-197Tumors of the Anterior Mediastinum
Magnetic Resonance Imaging MR imaging is an excellent modality for the detection and characterization of mediastinal masses and their relationship to adjacent structures The majority of thymomas are heterogeneous masses of higher signal intensity than skeletal muscleMolina P, Siegel MJ, Glazer HS. Thymic masses on MRI. AJR 1990; 155: 495-500Molina P, Siegel MJ, Glazer HS. Thymic masses on MRI. AJR 1990; 155: 495-500Tumors of the Anterior Mediastinum
ThymomaTreatmentComplete surgical excision if possibleHistologic evidence of tumor cells outside the capsule defines invasive thymomaXRT for incompletely resected or invasive tumor
Chemotherapy has been attempted for metastatic or recurrent thymoma with cisplatin, doxorubicin and cyclophosphamide. In one study of 29 patients there were 3 CR, 12 PR and a median 5 year survival of 30%
5 year survival10 year survivalEncapsulated75%63%Invasive50%30%
Surgical excision can be used for diagnosisthe sensitivity of US and CT scan guided fine-needle aspiration is increasingSurgical resection the standard of care for both noninvasive and invasive thymomasprovides the best prognosis. Adjunctive chemotherapy and radiation locally invasive or metastatic disease, or inoperable tumorsChest 2005;128;2893-2909Tumors of the Anterior Mediastinum
Chest 2005;128;2893-2909Tumors of the Anterior Mediastinum
STAGING OF THYMOMAS
StagingStage IStageIIStage IIIStage IVMacroscopically completely encapsulated, microscopically no capsular invasion Macroscopic invasion into surrounding fat or mediastinal pleura, or microscopic invasion into the capsuleMacroscopic invasion into neighboring organs, i.epericardium, great vessels, or lungA.Pleural or pericardial disseminationB. Lymphogenous or hematogenous metastasis
Masaoka staging system
Blumberg D, Port JL, Weksler B. Thymoma: a multivariate analysis of factors predicting survival. Ann Thorac Surg 2005;60:908913; discussion 914Five and 10-year survival rates
Stage5-Year Survival10-Year SurvivalI100%95%II91%81%III60%30%IVLess than 25%N/A
Thymic CarcinomaPresentationM>F, 40sIncidence rarePathologyCytologic features of malignancy: cellular necrosis, atypia, and mitosesEarly local invasion, widespread lymphatic and hematogenous metastasesRadiologyLarge, poorly defined, infiltrative, associated with pleural and pericardial effusionsPleural implants are uncommonTreatmentEtoposide/cisplatin + XRT5-year survival ranges from 15% to 90% depending on gradeComplete surgical resection is the treatment of choice and can be curativeChemotherapy and radiation therapy have roles in treating unresectable tumors
Chest 2005;128;2893-2909
Thymic CarcinoidPresentationMen, 4th/5th decadeAssociated endocrine abnormalities: Cushings syndrome due to ectopic ACTH or MENPathologyHistologically identical to carcinoid tumor at other sitesRadiologyVascular, large, lobulated, invasiveMay have areas of hemorrhage and necrosisPunctate, dystrophic calcificationTreatmentComplete surgical excisionLocal invasion, mets to regional lymph nodes and distant mets have been treated with chemotherapy and XRT, but with poor resultsChest 2005;128;2893-2909
ThymolipomaPresentationM=F, occurs over a wide age range, median age 27Most are asymptomaticPathologyMature adipose cells and thymic tissueRadiologyLarge, soft, encapsulatedMay fall into the anteroinferior mediastinum mimicking cardiomegaly or elevated hemidiaphragmCT demonstrates a combination of fat and soft tissue densities within an encapsulated massTreatmentSurgical excision curative
Mediastinal CystsGCTs young adultsrepresent 15% of anterior mediastinal masses found in adultsMalignant GCTs are more common ( 90%) in men. A mediastinal GCT should prompt a search for a primary gonadal malignancy.GCTs are classified into the following three groups based on cell type: benign teratomas; seminomas;embryonal tumors / malignant teratomas / nonseminomatousChest 2005;128;2893-2909Tumors of the Anterior Mediastinum
Mediastinal Teratomas (benign)Consisting of tissue from at least two of the three primitive germ layers, benign teratomas are the most common mediastinal GCTEctodermal tissues, which usually predominate, include skin, hair, sweat glands, and tooth-like structures. Mesodermal tissues,such as fat, cartilage, bone, and smooth muscle are less common, as are endodermal structures like respiratory and intestinal epithelium.The majority of mediastinal teratomas are mature teratomas that are histologically well-defined and benignChest 2005;128;2893-2909Tumors of the Anterior Mediastinum
Most completely asymptomaticpresenting symptomscough, dyspnea, and chest painchest radiograph well-defined, round, or lobulated massesUp to 26% are calcifiedoften have elements of bone or teethCT scanning and MRIassess resectabilityComplete surgical resection is the treatment of choice; subtotal resection can relieve symptoms.Adjunctive chemotherapy may be useful after subtotal resection
Chest 2005;128;2893-2909Tumors of the Anterior MediastinumMediastinal Teratomas (benign)
Mediastinal Seminoma25 to 50% of malignant mediastinal GCTs men ages 20 to 40 yearsdyspnea, substernal pain, weakness, cough, fever, gynecomastia, or weight loss.tumor location 10% of patients present with superior vena cava syndrome.Radiographically bulky, lobulated, homogenous masses.CT and gallium scanning is used to evaluate the extent of disease.uniquely sensitive to radiation therapylocally advanced diseaseChemotherapy followed by the surgical resection of residualChest 2005;128;2893-2909Tumors of the Anterior Mediastinum
Mediastinal Nonseminomatous GCTsembryonal cell carcinomas, endodermal thymus tumors, choriocarcinomas, yolk sac tumors, and mixed GCTs with multiple cellular componentssymptomatic and malignant85% of patients are symptomatic : chest pain, hemoptysis, cough, fever, or weight lossGynecomastia hCG secretion from certain tumor typesPredominantly affect young men. AFP and -hCG levels is important in making the diagnosisChemotherapy with bleomycin, etoposide, and cisplatin current standard of care for patients with nonseminomatous malignant GCTsPatients with residual tumor undergo surgical resectionPoorer prognosis5-year overall survival rate of 48%, compared to 86% in seminomasChest 2005;128;2893-2909Tumors of the Anterior Mediastinum
Mediastinal GoiterIn patients undergoing thyroidectomy, the incidence of mediastinal goiter is 1 to 15%Radiographicallyencapsulated, lobulated, heterogeneous tumorsclassic finding on a CT scan iscontinuity of the cervical and mediastinal components of the thyroidScintigraphySurgical resection is recommendednot usually amenable to needle biopsy,malignancy develops in a significant numberChest 2005;128;2893-2909Tumors of the Anterior Mediastinum
Mediastinal Parathyroid AdenomaThe mediastinum is the most common location at which an ectopic parathyroid tumor may develop20% of parathyroid adenomas develop in the mediastinum80% occurring in the anterior mediastinumencapsulated, round, and usually 3 cm in sizemay not be identified on a CT scanMRI or nuclear scans with 99mTc and 201Ti are more effective for the diagnosisSurgical resection is curative.
Chest 2005;128;2893-2909Tumors of the Anterior Mediastinum
Primary Mediastinal Lymphomarare entity : only 10% of lymphomas in the mediastinumLymphomausually occurs in the anterior mediastinumpart of more widespread disease.HD : 50 to 70% of mediastinal lymphomasnon-Hodgkin lymphoma :15 to 25%The three most common types of mediastinal lymphoma nodular sclerosing HDlarge B-cell lymphomaLymphoblastic lymphoma
Chest 2005;128;2893-2909Tumors of the Anterior Mediastinum
Staging
CHOP regiment in Indolent NHL Cycle 3 weeklyCyclophosphamide 500mg/m2, d1Adriamycin 25 mg/m2, d1Vincristine 1.4mg/m2 (max. 2mg), d1Prednisone 60mg/m2, d1-d5
Mediastinal cystsBronchogenic cystsEnterogenous cystsNeuroenteric cystsPericardial cystsLymphangiomasChest 2005;128;2893-2909Middle Mediastinum
Mediastinal Cysts12 to 20% of mediastinal masses and are found in the middle compartment of the mediastinumforegut cysts : embryonic abnormalityThe most common type of mediastinal cystenterogenous cysts (50 to 70%)bronchogenic cysts (7 to 15%)Tumors of the Middle MediastinumChest 2005;128;2893-2909
Bronchogenic Cystsformed during embryonic developmentanomalous budding of the laryngotracheal groove.40% symptomaticcough, dyspnea, or chest pain.well-defined round masses with a homogenous density similar to watersome bronchogenic cysts are mucoid and can give the impression of being a solid massTissue is often required : definitive diagnosisMost are removed surgically or are drained by needle aspirationTumors of the Middle MediastinumChest 2005;128;2893-2909
Enterogenous Cystsarise from the dorsal foregut lined by squamous or enteric (alimentary) epithelium may contain gastric or pancreatic tissue.Often asymptomaticif they contain gastric or pancreatic mucosa added risk of hemorrhage or rupture of the cyst from mucosal secretionsRadiographicallydifficult to distinguish these from bronchogenic cysts,More often calcifiedMost cysts should be surgically excisedVideoassisted thoracic surgery is the treatment of choice
Tumors of the Middle MediastinumChest 2005;128;2893-2909
Neuroenteric Cyststhe presence of both enteric and neural tissueComplete surgical excision is curativePericardial Cystsoccur in 1 of 100,000 peopleasymptomatic : fourth to fifth decade of lifeThe most common locationright cardiophrenic angle (70%),left cardiophrenic angle (22%).surgical removal is the treatment of choiceLymphangiomasrare congenitalLymphangiomatosis seen in young womenmore progressive form of diseasemultiple tumors are found and invade multiple organ structures, including the lung, heart, and bone.Tumors of the Middle MediastinumChest 2005;128;2893-2909
Neurogenic tumorsNerve sheath tumorsMalignant tumors of nerve sheath originAutonomic ganglionic tumorsGanglioneuromaGanglioneuroblastoma NeuroblastomaChest 2005;128;2893-2909Posterior Mediastinum
Neurogenic Tumors95% posterior mediastinal masses arise in the intercostal nerve rami or the sympathetic chain regioncomprise approximately 12 to 21% of all mediastinal masses95% occur in the posterior compartment70%-80% benign + nearly half asymptomatic;can occasionally cause compressive or neurologic symptoms.
Chest 2005;128;2893-2909Tumors of the Posterior Mediastinum
Nerve Sheath TumorsThese benign, slowly growing tumors 40 to 65% of neurogenic mediastinal massesNeurilemomas or schwannomas constitute 75% of this group of masses.often asymptomatic and are discovered incidentallyThe surgery of choice for removal of these tumors is thoroscopy, or thorocotomy when the former is not an optionrole for postoperative chemotherapy or radiation therapy when total resection not possibleChest 2005;128;2893-2909Tumors of the Posterior Mediastinum
Malignant Tumors of Nerve Sheath Originspindle cell sarcomas of the posterior mediastinummalignant neurofibromas, malignant schwannomas,and neurogenic fibrosarcomas. affect men and women equallythird to fifth decade of lifeclosely associated with neurofibromatosis5% risk of sarcomatous degeneration.Pain and nerve deficits are common. Complete surgical resection is the optimal treatmentunresectable tumorsadjuvant chemotherapy and radiation are optionsChest 2005;128;2893-2909Tumors of the Posterior Mediastinum
Autonomic Ganglionic TumorsTumors of the autonomic nervous system arise from neuronal cells rather than from the nerve sheath.50% of neuroblastomas arise in the adrenal up to 30% in the mediastinumGanglioneuroma: benign tumorsArising from the nerve ganglion cellsmost benign and differentiated of the autonomic ganglionic tumorsMost are asymptomatic and receive diagnoses in the second or third decade of lifeChest 2005;128;2893-2909Tumors of the Posterior Mediastinum
Ganglioneuroblastoma:histologic features of both ganglioneuromas and neuroblastomas. least common type of neurogenic tumor. Prognosis depends on histologic appearanceBoth sexes are equally affected in the first decade of lifeChest 2005;128;2893-2909Tumors of the Posterior Mediastinum
Neuroblastoma 95% occurring in patients 5 years of agehighly aggressive and readily metastasizing tumors80% of these tumors have calcificationTreatmentlimited-stage disease surgical resectionstage I disease, resection is usually curative.partially resectable stage II and III diseasePostoperative chemotherapy and radiationStage IV diseasecontroversy over the role of surgery;Poor prognostic factors large tumor size, poorly differentiated cell typeadvanced stage, extrathoracic originpresentation in an elderly patient
Chest 2005;128;2893-2909Tumors of the Posterior Mediastinum
KesimpulanTumors of the mediastinum wide diversity of disease states. The location and composition of a mass is critical to narrowing the differential diagnosis. Anterior mediastinal mass thymoma; teratoma; thyroid disease; and lymphoma. Middle mediastinumcongenital cysts, including foregut and pericardial cystsPosterior mediastinumNeurogenic tumors. The clinical sequelae of mediastinal massesasymptomatic symptoms of cough, chest pain, and dyspnea.Chest 2005;128;2893-2909
Thank You
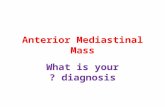
The first step in evaluating a mediastinal mass is to place it in one of the three mediastinal compartments, since each has different characteristic lesions. The most common lesions in the anterior mediastinumthymomas, lymphomas, teratomatous neoplasms, thyroid masses. Harrisons priciples of internal medicine. 17th ed
Massa mediastinal anterior8TTimomaTiroidTeratomaTesticular TumorTerrible LymphomaparaThyroid Tumor
The most common masses in the middle mediastinum are vascular masses, lymph node enlargement from metastases or granulomatous disease, pleuropericardial and bronchogenic cysts. Harrisons priciples of internal medicine. 17th ed
Massa Mediastinal MedialNOT VD90% malignantNodes: Tumor (limfoma, leukemia) Infeksi Tumor: Paru, trakhea, esofagusVaskular: Aneurisma, hematomaDuplication Cyst: Bronkogenik, enterik.
In the posterior mediastinumneurogenic tumors, meningoceles, meningomyeloceles, gastroenteric cystsesophageal diverticulaHarrisons priciples of internal medicine. 17th ed
Massa Tumor Mediastinal PosteriorHaloveenHematomaAbsesLymph NodesOsteophyteVertebral (Mets, Plasmacytoma)Extramedullary HematopoesisEsofagusNeurogenic Tumor
Horners syndrome: enophthalmos, ptosis, miosis, and ipsilateral anhidrosisPancoasts (or superior sulcus tumor) syndrome results from local extension of a tumor growing in the apex of the lung with involvement of the 8th cervical and 1st and 2nd thoracic nerves, with shoulder pain that characteristically radiates in the ulnar distribution of the arm, often with radiologic destruction of the 1st and 2nd ribs. Often Horners syndrome and Pancoasts syndrome coexist.
Type of mediastinal mass year 1970-1990 at Persahabatan Hospital32 %24%8%Jusuf A, Hudoyo A, Wibawanto A, dkk. Tumor Mediastinum (Tumor Mediastinum Nonlimfoma), Pedoman Diagnosis & Penatalaksanaan Di Indonesia. Perhimpunan Dokter Paru Indonesia, Jakarta; 2003: hal 1-2TeratomaTimomaTumor syarafLimfoma
Chart1
0.32
0.24
0.08
0.043
4,3%
Sales
Sheet1
Sales
1st Qtr32%
2nd Qtr24%
3rd Qtr8%
4th Qtr4%
To resize chart data range, drag lower right corner of range.
Differential Diagnoses
Differential diagnosis of mediastinal masses based on anatomic locationRiedel, R. F. et al. Oncologist 2006;11:887-894
Treatment strategy of Indolent NHLIndolent NHLStage I-IIAStage IIB-IV< 10 cm 10 cmRadiotherapyCRNon CRRelapse ?Lymph node biopsyTransformation ?YesNoTreatment ofAggressive NHL orRapidly progressive NHLRelapse ?YesNoTreatment ofIndolent LNHrelapse/refractoryFollow upFollow upCVPNon CR 60 yrs> 60 yrsSymptomaticAsymptomaticTolerant CTx ?YesNoCPCRFollow upNon CRStableCondition ?YesNoCVPCHOPRelapseCR
Mass Location> 2/3 of mediastinal tumors are benignanterior compartment are more likely to be malignantMalignancy59%-29%-16% : anterior-middle-posteriorAge important predictor of malignancySymptomatic patientsmore likely to have a malignancy85% vs 46%Chest 2005;128;2893-2909
**1/3 have chest pain, cough or dyspnea on presentationMyasthenia gravis occurs in 30-50% of pts with thymoma. All pts should have antiacetylcholine receptor antibodies measured prior to surgery and subsequentlyHypogammaglobulinemia occurs in 10% of pts with thymomaPure red cell aplasia occurs in 5%, but thymoma occurs in 50% of pts with red cell aplasia
****************