Meckel’s Diverticulum Preoperatively Diagnosed by Double ...

1General Pediatric Surgery | www.smgebooks.comCopyright Ghritlaharey RK.This book chapter is open access distributed under the Creative Commons Attribu-tion 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
Meckel’s Diverticulum and Patent Vitelline Duct in Children
ABSTRACT
Meckel’s diverticulum is one of the most common congenital anomaly of the gastrointestinal tract. Although, it is considered as a disease of children but also present in the adults. Omphalomesenteric duct (vitelline duct) is an embryonic structure that connects the midgut to yolk sac. A wide variety of the anomalies may occur due to the partial or complete absence of this involution of the vitelline duct, and Meckel’s diverticulum being the most common amongst the all. Meckel’s diverticulum occurs in 1.2 - 3% of general population, and symptomatic cases are more in males. A person with Meckel’s diverticulum has a 4 to 6% lifetime risk of developing a complication of Meckel’s diverticulum. Meckel’s diverticulum is mostly asymptomatic, but may present as lower gastrointestinal bleeding, intestinal obstruction, diverticulitis, perforation peritonitis, and also observed as an incidental finding during abdominal surgery for other abdominal pathology. Meckel’s diverticulum is most commonly remembered by classic rule of 2s, although this is not the rule. Patent vitelline duct is also frequently observed in clinical practice during infancy and childhood. The clinical diagnosis of patent vitelline duct is obvious and clinically may present as flatus and fecal discharges through umbilicus. Few of the cases with patent vitelline duct may present as an acute intestinal obstruction. The diagnostic modalities used for the evaluation and diagnosis of Meckel’s diverticulum are; ultrasonography of abdomen, CT scan of the abdomen, Scintigraphy, diagnostic laparoscopy, etc and the choice of the diagnostic tools depends upon the clinical presentation. Patent vitelline duct is clinically obvious and easily detectable, and further
Rajendra K Ghritlaharey*Department of Pediatric Surgery, Gandhi Medical College and Associated, Kamla Nehru and Hamidia Hospitals, India
*Corresponding author: Rajendra K Ghritlaharey, Department of Pediatric Surgery, Gan-dhi Medical College and Associated, Kamla Nehru and Hamidia Hospitals, Bhopal, Madhya Pradesh 462001, India, Email: [email protected]
Published Date: December 04, 2014
Gr upSM

2General Pediatric Surgery | www.smgebooks.comCopyright Ghritlaharey RK.This book chapter is open access distributed under the Creative Commons Attribu-tion 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
investigations are seldom required. The treatment of a symptomatic Meckel’s diverticulum is resection. Surgical resection of Meckel’s diverticulum as diverticulectomy (wedge resection) or segmental resection of ileum containing Meckel’s diverticulum and ileoileal anastomosis, and can be accomplished either by open surgery or by laparoscopically. Patent vitelline duct is best treated by sub-umbilical incision and also require diverticulectomy or segmental resection of ileum containing Meckel’s diverticulum and ileoileal anastomosis.
Keywords: Diverticulectomy; Intestinal obstruction; Meckel’s diverticulum; Meckel’s scan; Omphalomesenteric duct; Patent vitelline duct; Pediatric surgery; Wedge resection; Segmental resection
BRIEF HISTORYA diverticulum of the ileum was first described by Fabricius Hildanus in 1598 [1,2]. Alexis de
Littre (1654-1726) in 1700, a French surgeon, who was the first to report three cases of incarcerated femoral hernia containing a small bowel diverticulum. Since then hernia sacs containing only Meckel’s diverticulum have been called as Littre’s hernia [3]. Although Littre’s original report related to the femoral hernias; 50% of the Meckel’s diverticula are in the inguinal hernias, 20% in femoral hernias, 20% in umbilical hernia and, remaining 10% in other miscellaneous hernias. In children the Meckel’s diverticula are commonly present in umbilical hernia [1,3,4]. Johann Friedrich Meckel, the Younger (1781-1833), a German anatomist studied abnormal animal and human anatomy in an attempt to explain embryological development. In the year 1809 Meckel published about a birth defect where the connection between the fetus’s intestine and the mother’s yolk sac does not close. He described diverticula of the distal ileum and linked it to a problem that occurred during embryonic development. The name Meckel’s diverticulum was derived from his name to represent the ileal diverticulum [1,3,5,6]. The presence of heterotopic pancreatic and gastric mucosa in the Meckel’s diverticulum was reported by Zenker and Salzer in 1861 and 1904, respectively [1].
EMBRYOLOGY AND ANATOMYVitellointestinal duct (omphalomesenteric duct) or vitelline duct is an embryonic structure
which communicates the apex of the midgut to the yolk sac. During fifth and seventh weeks of intrauterine life, the vitelline duct normally disappears completely. This vitelline duct for unknown reason may fails to disappear completely or partially and responsible for a wide variety of anomalies [1,3,4,6,7-10].
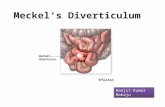
MECKEL’S DIVERTICULUMA portion of the vitellointestinal duct close to the ileum / midgut persists and thereby forming
an out pouching located on the antimesenteric border of the ileum. Meckel’s diverticulum is the most common congenital abnormality of the small intestine and it is also being the most common amongst the all anomalies related to vitelline duct abnormalities, related to its failure to disappear

3General Pediatric Surgery | www.smgebooks.comCopyright Ghritlaharey RK.This book chapter is open access distributed under the Creative Commons Attribu-tion 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
completely or partially. Meckel’s diverticulum may or may not be connected to the umbilicus by a fibrous cord; an obliterated remaining portion of the vitellointestinal duct. In about three fourth of the cases there is no fibrous connection of Meckel’ diverticulum to the umbilicus. This ileal diverticulum is a true intestinal diverticulum and contains all the layers of the ileum. It is located at antimesenteric border of the ileum and having its blood supply from primitive omphalomesenteric or vitelline veseles. Meckel’s diverticulum is most commonly remembered by rule of 2s, means it occur in 2% of general population, more than 50-60% may develop symptoms within 2 years of life, twice more common in males, located two feet proximal to the ileo cecal valve, two inches long, and mostly contains two types of heterotopic mucosa, but this is not a rule and it may vary. Meckel’s diverticulum varies in size from 1–10 cm long, 1- 4 cm in diameter, located about 25-100 cm from the ileo caecal valve. In symptomatic Meckel’s diverticula the chances of ectopic heterotopic tissues are reported to occur in 40 – 50% cases and the incidence of heterotopic mucosa in surgically resected Meckel’s diverticula were 15-50%. Meckel’s diverticulum mostly contains gastric (25-85%) and pancreatic (2- 6% %) tissues, but less commonly may also contain colonic, endometrial, duodenal and biliary tissues [1,2,6,7,9-13].
PATENT VITELLINE DUCT Patent vitelline duct is also called as Patent Vitellointestinal Duct (PVID), vitelline or umbilical
fistula, umbilical fecal fistula, or omphaloileal fistula, and it occur due to the complete failure of obliteration of the vitellointestinal / vitelline duct. The patent vitelline fistula communicates with the ileum at one end and opens at the umbilicus at other end. The patent vitelline duct is lined by mucus secreting intestinal mucosa [1,6-9,11].
VITELLINE CYSTSometimes a small middle portion of the vitellointestinal duct fails to obliterate and it persists,
result in cyst formation [7,8].
UMBILICAL SINUSA part of the vitelline duct close to the umbilicus alone fails to obliterates, and it may result in
formation of umbilical sinus. This umbilical sinus communicates with the umbilicus [7,8].
UMBILICAL POLYPThis condition is due to the persistence of the small portion of the vitellointestinal duct tissue
at umbilicus [7-9].
FIBROUS CORDWhole of the vitellointestinal duct may persist as a fibrous cord and remain connect the
intestine to the umbilicus and may be a factor for causing intestinal obstruction [1,9].

4General Pediatric Surgery | www.smgebooks.comCopyright Ghritlaharey RK.This book chapter is open access distributed under the Creative Commons Attribu-tion 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
ASSOCIATED ANOMALIESAssociate congenital anomalies are very rare and presence of Meckel’s diverticulum does not
warrant for the search for the other associated anomalies. Associate anomalies may be there and are; cardiac defects, congenital diaphragmatic hernia, duodenal atresia, esophageal atresia, imperforate anus, etc [1,9].
INCIDENCEMeckel’s diverticulum occurs in 1.2 - 3% of general population and may present at any age.
A person with Meckel’s diverticulum has a 4 to 6% lifetime risk of developing a complication of Meckel’s diverticulum. The incidence of Meckel’s diverticulum is equal in males and females, but complications are more common in males. Overall the complications of the Meckel’s diverticulum have been found more in males than females with a male to female ratio of 1.5 – 2.72:1. In symptomatic Meckel’s diverticulum, more than 50-60% of the children are less than two years of the age. Factors associate with a higher risk of complications of Meckel’s diverticulum are; age younger than 40 year, male sex, presence of heterotopic mucosa, lager length of diverticula, and narrow base / neck of diverticula, and presence of diverticular fibrous band [1-3,9-16].
CLINICAL PRESENTATIONMeckel’s diverticulum is most common congenital anomaly of the gastrointestinal tract.
Although, Meckel’s diverticulum generally remains silent and asymptomatic but life threatening complications may arise, making it an important structure for having a detailed knowledge of its anatomical and pathophysiological properties to deal with such complications. Symptomatic Meckel’s diverticulum may present as lower gastrointestinal bleeding, intestinal obstruction, diverticulitis, and perforation peritonitis. Meckel’s diverticulum may be detected incidentally during abdominal surgery for other pathology. Lower gastrointestinal bleeding and intestinal obstruction predominates in the younger patients [1,9-13,15,17,18].
Lower Gastrointestinal Bleeding
Lower gastrointestinal bleeding is the most common presentation in children. Meckel’s diverticulum accounts for about 50% of the case of lower gastrointestinal bleeding in children, more in infants and younger children. The bleeding mostly painless, frequent and sometimes massive bleeding may be there, and the stool may be as brick colored or currant jelly colored. The cause of the bleeding is the peptic ulcerations of heterotopic acid secreting gastric mucosa in the Meckel’s diverticula. In children, if there is no obvious cause (rectal polyp, fissure) for the bleeding than there is need to investigate for the Meckel’s diverticulum [1,9-13,17].
Intestinal Obstruction
Meckel’s diverticulum may present as an intestinal obstruction. In some series intestinal obstruction was observed as major presentation while in others lower gastrointestinal bleeding

5General Pediatric Surgery | www.smgebooks.comCopyright Ghritlaharey RK.This book chapter is open access distributed under the Creative Commons Attribu-tion 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
was the major presenting features. The causes / mechanism of the intestinal obstruction in Meckel’s diverticulum are; intussusception (Figure 1a), volvulus, vitelline fibrous band, internal herniation, obstruction due to fibrous band (Figure 1b,1c), incarcerated Littre’s hernia. Meckel’s diverticulum forms a pathological lead point (Figure 1d) for the occurrence of intussusceptions [1,2,9-11,13,17-20].
Figure 1a: Intussusception with bowel gangrene caused by Meckel’s diverticulum (Meckel’s not seen).
Figure 1b: Meckel’s diverticulum with fibrous cord, causing intestinal obstruction.
Figure 1c: Meckel’s diverticulum with fibrous cord, causing intestinal obstruction.

6General Pediatric Surgery | www.smgebooks.comCopyright Ghritlaharey RK.This book chapter is open access distributed under the Creative Commons Attribu-tion 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
Figure 1d: Meckel’s diverticulum as pathological lead point for intussusception (reduced).
Inflammation / Diverticulitis
Inflammation (Figure -1e) or diverticulitis of Meckel’s diverticula is mostly due to the presence of heterotopic gastric tissues and peptic ulceration. Diverticulitis may also be secondarily to infections, obstruction of the lumen of the diverticulum by enterolith, foreign bodies, parasites, etc. The clinical presentation mimic to an acute appendicitis. If the condition left untreated it may lead to perforation of Meckel’s diverticulum followed by peritonitis [1,9,10,16].
Figure 1e: Meckel’s diverticulitis, inflammation causing intestinal obstruction.
Perforation Peritonitis
In cases of Meckel’s diverticula containing heterotopic gastric mucosa, it may get ulcerated and if not treated it may progress to perforation of the Meckel’s diverticulum, and may present as perforation peritonitis. The factors responsible for perforation of the Meckel’s diverticulum are; progression of the diverticulitis, ulceration of the diverticulum and adjacent ileum due to acid producing gastric mucosa, perforation may be due to presence of foreign bodies. Clinically perforated Meckel’s diverticulum present as perforation peritonitis, but the cause of the perforation peritonitis as perforated Meckel’s diverticulitis is seldom possible pre-operatively [1,9-13,17].

7General Pediatric Surgery | www.smgebooks.comCopyright Ghritlaharey RK.This book chapter is open access distributed under the Creative Commons Attribu-tion 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
Umbilical Sinus and Umbilical Polyp
About 5% of the anomalies relating to vitelline duct may present as umbilical polyps, and umbilical sinuses. The umbilical sinus clinically may present as serous umbilical discharges, as it contains the intestinal mucosal lining. An umbilical polyp or granulation tissues in newborns are frequently observed, but majority are not actual polyps. Mostly the umbilical polyps are an isolated anomaly and not connected or associated with any intra peritoneal abnormalities. An umbilical granuloma not responding to the local treatment by chemical cauterization, one may think of that it is a true umbilical polyp containing intestinal mucosal lining. Umbilical polyp may present as serous discharge or may cause minor bleeding [1,9].
Tumors
Meckel’s diverticulum may be the site for benign and malignant tumors with a reported incidence of 0.5 to 4%. The most common neoplasm occurring at Meckel’s diverticula are; carcinoid, carcinoma, leimomas, sarcoma, lipoma, angiomas [1].
Incidental Findings
Meckel’s diverticulum may be detected while doing abdominal surgery for some other abdominal pathology [11,12,15,17].
DIAGNOSTIC WORKMeckel’s diverticula are mostly asymptomatic. In symptomatic cases various diagnostic
modalities used depends upon the clinical presentation. In cases of Meckel’s diverticula presenting as lower gastrointestinal bleeding, Meckel’s scan is a gold standard. In cases of Meckel’s diverticula presenting as intestinal obstruction and perforation peritonitis, it’s very unlikely to diagnose that Meckel’s diverticulum as a cause of it.
Roentgenograph of Abdomen
Plain x-ray of the abdomen in erect position is most useful when intestinal obstruction or perforation of viscus is the cause of concern. Plain x-ray abdomen may reveal dilated bowel loops with multiple air fluid levels in case of intestinal obstruction and may have free gas under diaphragm / in the peritoneal cavity in perforation peritonitis. Plain x-ray of the abdomen does not provide the reason of obstruction or perforation [9-11,20].
Ultrasonography (USG) of Abdomen
In majority of the cases of acute abdomen in children USG of the abdomen and pelvis can provide sufficient information. Ultrasound scans of abdomen can reveal intussusceptions, intestinal obstructions, dilated bowel loops, peritoneal collections, etc but rarely Meckel’s diverticulum as the cause of it. As Meckel’s diverticulum is a true intestinal diverticulum and it also contains all the layers of the intestine similar to that of the ileum and therefore its USG

8General Pediatric Surgery | www.smgebooks.comCopyright Ghritlaharey RK.This book chapter is open access distributed under the Creative Commons Attribu-tion 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
differentiation from rest of the bowel may be difficult. An inflamed Meckel’s diverticulum may be detected on USG abdomen as a cyst like structure or blind ending tubular structure with wall similar to bowel [9,12,17,20-22].
Color Doppler Sonography
The color Doppler sonography finding in cases of Meckel’s diverticulum are; cyst-like structure, blind ending tubular structure with wall similar to that of the bowel. Hyperaemia of the cyst-like structure may be detected, if diverticulum is inflamed. It may also reveal localized or free fluid collection in cases of inflammation or perforation. Fluid collection surrounding the cyst-like structure may be a suggestive of diverticular inflammation or perforation. In a review of 10 cases of inflamed Meckel’s diverticulum and those cases were evaluated by color Doppler sonography, and found that in 9 cases the diverticula were identified [21,23].
Barium Studies
Although conventional barium studies (small bowel follow through studies, enteroclysis, barium enema) have all been replaced by other imaging techniques for evaluation of patients with symptomatic Meckel’s diverticulum. The radiological signs on barium studies for Meckel’s diverticulum are; barium filled blind ending diverticulum, gas filled diverticulum arising from antimesenteric border of the distal ileum [20,22].
Computed Tomography (CT) Scan of Abdomen
CT scan of the can demonstrate; features of small-bowel obstruction, intussusception, free fluid in peritoneal cavity and, free air within the peritoneal cavity. Meckel’s diverticulum as the cause of the intestinal obstruction or peritonitis is difficult to diagnose on CT scan of the abdomen. A Meckel’s diverticulum may be seen on CT abdomen as tubular or rounded, blind ending fluid or gas filled structure in continuity with the adjacent small bowel. Administration of both oral and intra venous contrast material during CT scanning may help to establish the diagnosis of Meckel’s diverticulum [20, 22,24,25].
CT Enterography
Recently (2014) three cases of Meckel’s diverticulum with bleeding in adults were diagnosed on CT enterography. In all these three cases the source of bleeding were not detected on total colonoscopy, and Meckel’s scan was also negative. Resected specimens confirmed Meckel’s diverticulum in all and all three had gastric mucosa. In future, CT enterography may be used in children to investigate for symptomatic Meckel’s diverticulum [26].
Magnetic Resonance (MR) Enterography
Recently (2013) MR enterography was used to diagnose a case of Meckel’s diverticulum in a 25 year-old male and authors concluded that this MR enterography is a novel technique that combines the advantages of both the conventional enterography and the morphological imaging

9General Pediatric Surgery | www.smgebooks.comCopyright Ghritlaharey RK.This book chapter is open access distributed under the Creative Commons Attribu-tion 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
of magnetic resonance imaging. In future, magnetic resonance enterography may be used in children to investigate for symptomatic Meckel’s diverticulum [27].
Technetium 99m Scan (Meckel’s Scan)
Nuclear imaging / Scintigraphy using technetium 99m pertechnetate is considered as an investigation of choice for the diagnosis of bleeding Meckel’s diverticulum and seems to serve as a simple, safe and non -invasive tool in the diagnosis of the bleeding Meckel’s diverticulum in children. Pertechnetate ions carrying the technetium 99m isotopes are taken up and stored by the mucin secreting cells of gastric mucosa and ectopic gastric tissues, and secretes it into the lumen of the bowel. Technetium scan has been universally used for the investigation of bleeding diverticulum with a reported sensitivity of 85% -95% and specificity of 90 - 95% in pediatric age group. In a 10 year review of 954 scintiscans / technetium scans (in mixed population) for the diagnosis of Meckel’s diverticula that only 1.7% were false negative, and 0.05% had false positive results, giving a sensitivity of 85% and a specificity of 95% with an accuracy of 90%. Meckel’s scan yield positive results only when gastric mucosa is present within the Meckel’s diverticula (Figure 2). Negative Meckel’s scan doses not rule out the presence of Meckel’s diverticulum, it may suggest only that there may not be an ectopic gastric cells. False negative scan may be due to rapid dilution of the tracer, poor blood supply to the Meckel’s diverticulum, and inadequate gastric mucosa in Meckel’s diverticulum. Meckel’s scan yields higher positive results in children presenting with significant lower gastrointestinal bleeding. The use of pentagastrin, histamine and glucagon may enhance the accuracy of the Meckel’s scan. Technetium 99m - labeled RBCs scan can also be used for detection of bleeding Meckel’s diverticulum, as it persists longer in the intravascular compartment and also has improved bleeding site localization [1,9-13,17,20,22,28-32].

10General Pediatric Surgery | www.smgebooks.comCopyright Ghritlaharey RK.This book chapter is open access distributed under the Creative Commons Attribu-tion 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
Figure 2: Positive Meckel’s scan of a child presented with lower gastrointestinal bleeding.
Capsule Endoscopy
In recent years the wireless capsule endoscopy has also been used for the evaluation of the gastrointestinal bleeding not only in adults but also in children and this tool may be of some help to diagnose the cause of bleeding as Meckel’s diverticulum [9,10,33,34].
Double Balloon Enteroscopy
Double balloon enteroscopy is already an established modality for investigation in adults for lower gastrointestinal bleeding, chronic abdominal pain, Crohn’s disease, but its use in children is not being widely practiced. Meckel’s diverticulum can also be diagnosed using double balloon enteroscopy in children, but this procedure require anesthesia [35].
Colonoscopy
Colonoscopy is one of the frequently used tools for the evaluation of child with history of lower gastrointestinal bleeding. Colonoscopy is much helpful for the evaluation of the colonic pathology. This tool has its own limitations, and it usually fail to detect the cause of bleeding as Meckel’s diverticulum as it is located in the terminal ileum [10,15,34].

11General Pediatric Surgery | www.smgebooks.comCopyright Ghritlaharey RK.This book chapter is open access distributed under the Creative Commons Attribu-tion 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
Angiography / Arteriography
The role of arteriography is limited and reserved for the cases of acute hemorrhage or unexplained gastrointestinal bleeding. This may help in the localization of the site of bleeding and therapeutic embolizartion as well. Angiography would be positive only when the rate of active bleeding is more than 0.5ml / min. This tool is rarely recommended for the evaluation of a child with a history of lower gastrointestinal bleeding [1,10,22].
Fistulogram / Sonogram
The diagnosis of patent vitelline duct and umbilical sinuses are clinically obvious in majority of children. Fistulogram / sinogram may be advised in some selected cases to detect the patent vitelline duct or exclude the intestinal communication in cases of umbilical sinuses [9,11,16].
Diagnostic Laparoscopy
Laparoscopy is a useful tool for the evaluation and diagnosis of the lower gastrointestinal bleeding, recurrent abdominal pain, etc and this may reveal Meckel’s diverticulum as a cause for above in children. This laparoscopy is safe, cost effective and an effective tool not only for diagnosis but also for resection of a Meckel’s diverticulum [1,10,13,19,20,32,36-38].
MANAGEMENT OF MECKEL’S DIVERTICULUMThe treatment of a symptomatic Meckel’s diverticulum is resection. Surgical resection of
Meckel’s diverticula is diverticulectomy (wedge resection) or segmental resection of ileum containing Meckel’s and ileoileal anastomosis and still hold the best, and can be achieved by open surgery or laparoscopically. The choice of either opting for diverticulectomy or segmental resection mostly depends on the condition of the diverticula and mode of clinical presentation [1,9-13,16-20].
Diverticulectomy (Wedge Resection) of Meckel’s Diverticulum
When a Meckel’s diverticulum has narrow base, simplest is to perform diverticulectomy or wedge resection. Diverticulectomy is a simplest procedure performed for resection of a Meckel’ diverticulum. Meckel’s diverticulum can be simply removed and ileum repaired by sutures. The suturing of ileum can be achieved by; single layer, double layer, interrupted or continuous and all depends upon the choice of operating surgeons. This diverticulectomy can also be done by using staplers.
Segmental Resection of Ileum Containing Meckel’s Diverticulum and Ileoileal Anastomosis
Segmental resection of ileum with Meckel’s diverticulum and ileoileal anastomosis is required in cases of; history of bleeding, intussusceptions (caused by Meckel’s diverticula) with bowel gangrene, perforation at the base of Meckel’s diverticulum, suspicion of a presence of heterotopic

12General Pediatric Surgery | www.smgebooks.comCopyright Ghritlaharey RK.This book chapter is open access distributed under the Creative Commons Attribu-tion 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
mucosa, thickened and inflamed base, ulceration of Meckel’s diverticulum, tumors of Meckel’s diverticula. Sometimes the ulceration may not be on the Meckel’s diverticula, but it’s on the adjacent ileal mucosa and in such cases segmental ileal resection including Meckel’s diverticulum and ileoileal anastomosis is needed. In such cases, if simple diverticulectomy is performed, the ulcer may remain in the ileum and may present again with recurrent lower gastrointestinal bleeding. Gangrenous bowel is more frequently observed in developing countries due to delayed presentation and delay in seeking surgical treatment in the cases of intussusceptions caused by Meckel’s diverticula as pathological lead point, and need more bowel resections.
Segmental Resection with an Ileostomy
In a rare occasion, there is a need for exteriorization of the bowel as a temporary ileostomy. This may be needed in cases of either a general condition of a child not permitting major surgical intervention or condition of bowel is not healthy to achieve intestinal anastomosis.
MANAGEMENT OF INCIDENTALLY DETECTED MECKEL’S DIVERTICULUM
During laparotomy or laparoscopy for other abdominal procedures, Meckel’s diverticulum may be detected (Figure 2a and Figure 2b). This is a controversial matter; whether to remove or not to remove an incidentally detected Meckel’s diverticulum. In the past, if a Meckel’s diverticulum was encountered in a patient undergoing abdominal surgery for some other intra-abdominal pathology, many surgeons recommended its removal. This practice was questioned when a large series described a person with Meckel’s diverticulum has only 4.2% likelihood of complications of it and also decreasing risk with increasing age. Soltero and Bill calculated using the figure of 2% incidence of Meckel’s diverticulum; they calculated that a Meckel’s diverticulum has 4.2% likelihood of causing disease during lifetime and decreasing with old age. They further calculated that to save one patient’s life from the complications of Meckel’s diverticulum, it would be necessary to remove approximately 800 asymptomatic Meckel’s diverticula. While doing so, it would be associated with considerable, post-operative morbidity and mortality as well and therefore prophylactic removal of Meckel’s diverticulum is not justified. In a review of 1476 patients with resection of asymptomatic Meckel’s diverticula, reported 20% morbidity and 3% mortality. Justification for doing diverticulectomy or segmental resection for incidentally detected Meckel’s diverticula are; history of unexplained recurrent abdominal pain, history of lower gastrointestinal bleeding, palpable thickening of the base of the diverticula suggestive of presence of heterotopic mucosa, presence of fibrous band, inflammations, adhesion, narrow base diverticula having chances of obstruction [1,9,11,12,14,15,17,20,36].

13General Pediatric Surgery | www.smgebooks.comCopyright Ghritlaharey RK.This book chapter is open access distributed under the Creative Commons Attribu-tion 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
Figure 2a: Meckel’s diverticulum, incidentally finding during inguinal exploration in an infant (Ileal perforation detected few cm from Meckel’s diverticulum, segmental ileal resection
was done).
Figure 2b: Meckel’s diverticulum, incidentally finding during laparotomy for ileal perforation (5 year-old girl) (Two ileal perforation and perforation at base of Meckel’s
diverticulum (not seen here) also detected).
Laparoscopic Procedures for Meckel’s Diverticulum
The treatment of Meckel’s diverticulum is resection (wedge resection or segmental resection of ileum with Meckel’s diverticulum), and this can also be done safely, using laparoscopic techniques. Meckel’s diverticulectomy or segmental resection of the ileum with Meckel’s diverticulum and an ileoileal anastomosis can either be done laparoscopically or by laparoscopic assisted techniques. In recent decade, laparoscopy is being used more frequently for the management of Meckel’s diverticulum, not only for the diagnosis, but also for the definitive treatment of Meckel’s diverticulum as well. Several studies advocated use of laparoscopic procedures for removal of Meckel’s diverticulum with added advantages of minimal access surgery in children. Many authors have claimed that, laparoscopic procedures for removal of Meckel’s diverticula are safe, cost effective, fewer complications and shorter length of hospital stay with an excellent cosmetic results [1,9,10,13,19,32,36-42].

14General Pediatric Surgery | www.smgebooks.comCopyright Ghritlaharey RK.This book chapter is open access distributed under the Creative Commons Attribu-tion 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
PATENT VITELLINE DUCTPatent vitelline duct is also known as vitelline or umbilical fistula, umbilical fecal fistula, or
omphaloileal fistula and it occur due to the complete failure of obliteration of the vitellointestinal / vitelline duct. Patent vitelline fistula communicates with the ileum at one end and opens at the umbilicus at the other end and it is lined by mucus secreting intestinal mucosa. A child with patient vitelline duct (Figure 3a) may present with fecal and flatus discharges through the umbilicus. Herniation or prolapse of the bowel (Figure 3b, Figure 3c) through the patent vitelline duct (ram’s horn appearance) may be the there and may present as an acute intestinal obstruction (Figure 3d). Pre-operative diagnosis of a case of patent vitelline duct is clinically obvious in most of the cases, and diagnostic investigations are rarely needed. Very rarely dye study (fistulogram) may be required to confirm the patent vitelline duct (Figure 3e) [1,7-9,11,16,17,43,44].
Figure 3a: Patent vitelline duct.
Figure 3b: Patent vitelline duct with prolapsed ileum
Figure 3c: Patent vitelline duct with prolapsed ileum

15General Pediatric Surgery | www.smgebooks.comCopyright Ghritlaharey RK.This book chapter is open access distributed under the Creative Commons Attribu-tion 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
Figure 3d: Patent vitelline duct with prolapsed ileum with gangrene
Figure 3e: Fistulogram through patent vitelline duct, showing dye in ileum and colon
Treatment of Patent Vitelline Duct
The treatment of patent vitelline duct is also a diverticulectomy or segmental resection of ileum containing Meckel’s diverticulum and ileoileal anastomosis. During surgery an infant feeding tube or a catheter placed within the patent vitelline duct help in easy identification of the duct. It is best possible to deal a patent vitelline duct through infra or trans-umbilical incision. Operative steps for resection of patent vitelline duct through sub-umbilical incision detailed in Figure 4 (Figure 4a- Figure 4g). The connection of the patent vitelline duct at ileum may be treated either by diverticulectomy or by segmental ileal resection and anastomosis. Infra-umbilical or trans-umbilical incision provides excellent cosmetic results (Figure 4h) [9,11,16,17,43,44].

16General Pediatric Surgery | www.smgebooks.comCopyright Ghritlaharey RK.This book chapter is open access distributed under the Creative Commons Attribu-tion 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
Figure 4(4a-4g): Operative steps (sub-umbilical procedure) for patent vitelline duct.
Figure 4h: Post-operative (10th post-op day) scar following sub-umbilical procedure for patent vitelline duct.
UMBILICAL SINUS AND UMBILICAL POLYPUmbilical sinus may present with serous discharges and may need sinogram for confirmation.

17General Pediatric Surgery | www.smgebooks.comCopyright Ghritlaharey RK.This book chapter is open access distributed under the Creative Commons Attribu-tion 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
It is best treated by infra-umbilical or trans-umbilical procedure. An umbilical polyp is also frequently seen in clinical practice and may present with serous secretion or with a history of bleeding. An umbilical granuloma not responding to chemical cauterization, it may be a case of epithelial lined true umbilical polyp. Umbilical polyp may be treated with suture ligation of a polyp at its base, electric cauterization, or surgical excision [45].
POST-OPERATIVE COMPLICATIONSPost-operative complications may occur during the management of symptomatic Meckel’s
diverticula and patent vitelline ducts and are generally the same as that occurs during other abdominal surgical procedures in children, and are bleeding, wound infection, wound dehiscence, intra-peritoneal abscess formation, anastomotic leak, incisional hernia, and post-operative adhesion and intestinal obstruction. The incidence of the post-operative complications following resection of Meckel’s diverticula varies depending upon series from 0 to 13%. The nature of complications depends upon many factors and are; resection of symptomatic or asymptomatic Meckel’s diverticula, simple or complicated Meckel’s diverticula, perforated Meckel’s diverticula with peritonitis, diverticulectomy or segmental ileal resections, laparotomies or laparoscopic surgical procedures [1,9-12,15,16,37,41].
MORTALITYIn a meta-analysis done by Snyder, he analyzed 244 articles since 1950 till 2012, and concluded
that the mortality was 0.01% for the resection of Meckel’s diverticula. Mortality is reported to occur more in cases undergone resections for patent vitelline ducts and who presented with prolapsed ileum [1,11,16].
CONCLUSIONMeckel’s diverticulum is most common benign, congenital anomaly of the gastrointestinal
tract. Although, it is mostly asymptomatic but may present as lower gastrointestinal bleeding, intestinal obstruction, diverticulitis, and perforation peritonitis. Meckel’s scan is an investigation of choice for the evaluation of bleeding Meckel’s diverticula, while in other cases the diagnosis of Meckel’s diverticulum is possible only during exploratory laparotomy or laparoscopy. The surgical treatment of the diverticulum is diverticulectomy or resection of a segment of ileum containing Meckel’s diverticulum and ileoileal anastomosis, and this can be achieved by open surgery or by laparoscopically. Patent vitelline duct is not rare and few of them may present with prolapsed ileum and associated with higher morbidity and mortality, therefore a patent vitelline duct should be excised.
References1. Snyder CL. Meckel diverticulum. Pediatric Surgery. 7th edn. Coran AG, Adzick NS, Krummel TM, Laberge JM, Shamberger RC,
editors. Elsevier. 2012; 2: 1085-1092.
2. Osborne MP, Hamilton G, Shalley M. Axial volvulus of Meckel’s diverticulum. Postgrad Med J. 1978; 54: 692-693.

18General Pediatric Surgery | www.smgebooks.comCopyright Ghritlaharey RK.This book chapter is open access distributed under the Creative Commons Attribu-tion 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
3. Mirza MS. Incarcerated Littre’s femoral hernia: case report and review of the literature. J Ayub Med Coll Abbottabad. 2007; 19: 60-62.
4. Skandalakis PN, Zoras O, Skandalakis JE, Mirilas P. Littre hernia: surgical anatomy, embryology, and technique of repair. 2006; 72: 238-243.
5. O’Connell L. Johann Friedrich Meckel, the Younger (1781-1833). The Embryo project encyclopaedia. 2013.
6. Rojhan MS, Hejazi R. Incidence of Meckel’s diverticulum in 100 cadavers. Postgrad Med J. 1974; 50: 697-701.
7. Singh V. Development of midgut derivatives. Textbook of clinical embryology. 2012; 12-47.
8. Bhatnagar SM, Kothari ML, Mehta LA, Natarajan M. The alimentary system: Meckel’s diverticulum. 3rd edn. Essentials of Human Embryology. 2000; 134-135.
9. Rouma BS, Lakhoo K. Vitelline duct anomalies. Pediatric Surgery: A comprehensive text for Africa. Ameh EA, Bickler SW, Lakhoo K, Poenaru D, editors. Global HELP organization. 2011; 389-392.
10. Sharma RK, Jain VK. Emergency surgery for Meckel’s diverticulum. World J Emergency Surg. 2008; 3: 27.
11. Ghritlaharey RK, Budhwani KS, Shrivastava DK, Srivastava J. Meckel’s diverticulum and patent vitello-intestinal duct in children: A review of 11 years of experience with 46 children. J Clin Diagn Res. 2011; 5: 689-693.
12. Blevrakis E, Partalis N, Seremeti C, Sakellaris G. Meckel’s diverticulum in paediatric practice on Crete (Greece): a 10-year review. Afr J Paediatr Surg. 2011; 8: 279-282.
13. Huang CC, Lai MW, Hwang FM, Yeh YC, Chen SY, Kong MS, et al. Diverse Presentations in pediatric Meckel’s diverticulum: A review of 100 Cases. Pediatr Neonatol. 2014; 55: 369-375.
14. Soltero MJ, Bill AH. The natural history of Meckel’s diverticulum and its relation to incidental removal. A study of 202 cases of diseased Meckel’s diverticulum found in King County, Washington, over a fifteen year period. Am J Surg. 1976; 132: 168-173.
15. St-Vil D, Brandt ML, Panic S, Bensoussan AL, Blanchard H. Meckel’s diverticulum in children: a 20-year review. J Pediatr Surg. 1991; 26: 1289-1292.
16. Ameh EA, Mshelbwala PM, Dauda MM, Sabiu L, Nmadu PT. Symptomatic vitelline duct anomalies in children. S Afr J Surg. 2005; 43: 84-85.
17. Menezes M, Tareen F, Saeed A, Khan N, Puri P. Symptomatic Meckel’s diverticulum in children: a 16-year review. Pediatr Surg Int. 2008; 24: 575-577.
18. Durakbasa CU, Okur H, Mutus HM, Bas A, Ozen MA, Sehiralti V, et al. Symptomatic omphalomesenteric duct remnants in children. Pediatr Int. 2010; 52: 480-484.
19. Ruscher KA, Fisher JN, Hughes CD, Neff S, Lerer TJ, Hight DW, Bourque MD. National trends in the surgical management of Meckel’s diverticulum. J Pediatr Surg. 2011; 46: 893-896.
20. Quarrie R, Lindsey D, Bahner DP. Review of the incidence and management of Meckel’s diverticulum. Austin J Surg. 2014; 1:3.
21. Baldisserotto M. Color Doppler sonographic findings of inflamed and perforated Meckel diverticulum. J Ultrasound Med. 2004; 23: 843-848.
22. Elsayes KM, Menias CO, Harvin HJ, Francis IR. Imaging manifestations of Meckel’s diverticulum. AJR Am J Roentgenol. 2007; 189: 81-88.
23. Mizerkowski MD, Spolidoro José V N, Epifanio M, Bastos JC, Baldisserotto M. Color Doppler of Meckel’s diverticulum: report of two cases. Radiol Bras. 2011; 44: 268-270.
24. Olson DE, Kim YW, Donnelly LF. CT findings in children with Meckel diverticulum. Pediatr Radiol. 2009; 39: 659-663.
25. Bennett GL, Birnbaum BA, Balthazar EJ. CT of Meckel’s diverticulitis in 11 patients. AJR Am J Roentgenol. 2004; 182: 625-629.
26. Lee JM, Jeen CD, Kim SH, Lee JS, Nam SJ, Choi HS, et al. Meckel’s diverticulum detected by computed tomographic enterography: report of 3 cases and review of the literature. Turk J Gastroenterol. 2014; 25: 212-215.
27. Zhou FR, Huang LY, Xie HZ. Meckel’s diverticulum bleeding diagnosed with magnetic resonance enterography: a case report. World J Gastroenterol. 2013; 19: 2727-2730.
28. Anand SS, Handa R, Chauhan MS. Nuclear imaging in Meckel’s diverticulum. 2004; MJAFI 60:198-199.
29. Stathaki MI, Karkavitsas NS. [Nuclear Medicine in the diagnosis of lower gastrointestinal bleeding]. Hell J Nucl Med. 2007; 10: 197-204.
30. Karavida N, Tsikopoulos G. [Nuclear medicine applications of the gastrointestinal tract in pediatric surgery]. Hell J Nucl Med. 2010; 13: 308-313.

19General Pediatric Surgery | www.smgebooks.comCopyright Ghritlaharey RK.This book chapter is open access distributed under the Creative Commons Attribu-tion 4.0 International License, which allows users to download, copy and build upon published articles even for commercial purposes, as long as the author and publisher are properly credited.
31. Sinha CK, Pallewatte A, Easty M, De Coppi P, Pierro A, Misra D, et al. Meckel’s scan in children: a review of 183 cases referred to two paediatric surgery specialist centres over 18 years. Pediatr Surg Int. 2013; 29: 511-517.
32. Poley JR, Thielen TE, Pence JC. Bleeding Meckel’s diverticulum in a 4-month-old infant: Treatment with laparoscopic diverticulectomy. A case report and review of the literature. Clin Exp Gastroenterol. 2009; 2: 37-40.
33. Fritscher-Ravens A, Scherbakov P, Bufler P, Torroni F, Ruuska T, Nuutinen H, et al. The feasibility of wireless capsule endoscopy in detecting small intestinal pathology in children under the age of 8 years: a multicentre European study. Gut. 2009; 58: 1467-1472.
34. Xinias I, Mavroudi A, Fotoulaki M, Tsikopoulos G, Kalampakas A, Imvrios G. Wireless Capsule Endoscopy Detects Meckel’s Diverticulum in a Child with Unexplained Intestinal Blood Loss. Case Rep Gastroenterol. 2012; 6: 650-659.
35. Huang Y, Shao CH, Leung YK. Application of double balloon enteroscopy in pediatric patients. Zhonghua Er Ke Za Zhi. 2010; 48: 599-602.
36. Shalaby RY, Soliman SM, Fawy M, Samaha A. Laparoscopic management of Meckel’s diverticulum in children. J Pediatr Surg. 2005; 40: 562-567.
37. Chan KW, Lee KH, Mou JW, Cheung ST, Tam YH. Laparoscopic management of complicated Meckel’s diverticulum in children: a 10-year review. Surg Endosc. 2008; 22: 1509-1512.
38. Prasad TR, Chui CH, Jacobsen AS. Laparoscopic-assisted resection of Meckel’s diverticulum in children. JSLS. 2006; 10: 310-316.
39. Cobellis G, Cruccetti A, Mastroianni L, Amici G, Martino A. One-trocar transumbilical laparoscopic-assisted management of Meckel’s diverticulum in children. J Laparoendosc Adv Surg Tech A. 2007; 17: 238-241.
40. Sai Prasad TR, Chui CH, Singaporewalla FR, Ong CP, Low Y, Yap TL, et al. Meckel’s diverticular complications in children: is laparoscopy the order of the day? Pediatr Surg Int. 2007; 23: 141-147.
41. Chan KW, Lee KH, Mou JW, Cheung ST, Tam YH. Laparoscopic management of complicated Meckel’s diverticulum in children: a 10-year review. Surg Endosc. 2008; 22: 1509-1512.
42. Papparella A, Nino F, Noviello C, Marte A, Parmeggiani P, Martino A, et al. Laparoscopic approach to Meckel’s diverticulum. World J Gastroenterol. 2014; 20: 8173-8178.
43. Singh S, Pandey A, Ahmed I, Rawat JD, Sharma A, Srivastava NK. Prolapse of bowel via patent vitello intestinal duct-a rare occurrence. Hernia. 2011; 15: 567-569.
44. Patel RV, Kumar H, Sinha CK, Patricolo M. Neonatal prolapsed patent vitellointestinal duct. BMJ Case Rep. 2013; 2013.
45. Hsu JW, Tom WL. Omphalomesenteric duct remnants: umbilical versus umbilical cord lesions. Pediatr Dermatol. 2011; 28: 404-407.

![Diagnosis of Bleeding Meckel's Diverticulum in Adults · 2020. 7. 27. · [1, 2]. Technetium-99m pertechnetate scintigraphy, commonly known as Meckel’s scan, is considered as the](https://static.fdocuments.net/doc/165x107/61279e6912637b477c1e638d/diagnosis-of-bleeding-meckels-diverticulum-in-adults-2020-7-27-1-2-technetium-99m.jpg)