Managing Hepatitis C and CKD - The National Kidney … Clin Bulletin.pdf · >Introduction >...
6
> Introduction > Associations Between HCV and CKD > Overview of HCV Evaluation > New Options in HCV Management > Summary Managing Hepatitis C and CKD: A Clinical Update
Transcript of Managing Hepatitis C and CKD - The National Kidney … Clin Bulletin.pdf · >Introduction >...

> Introduction> Associations Between HCV and CKD> Overview of HCV Evaluation> New Options in HCV Management> Summary
Managing Hepatitis C and CKD: A Clinical Update

IntroductionHepatitis C virus (HCV) is the most common chronic blood-borne infection in the United States (U.S.) and is more prevalent among patients with chronic kidney disease (CKD) than in the general population.1,2,3 HCV is usually asymptomatic, and detection requires screening patients with risk factors and testing for serum HCV antibodies or HCV RNA (viral load). The field of HCV has dramatically changed in recent years with the advent of direct-acting antivirals (DAAs) and multi-class drug combinations. These newer therapies have been the focus of clinical research in recent years for their improved efficacy (90-100% sustained viral response (SVR) in most cases), with improved side effect profiles and better tolerability. Recently approved DAA regimens can safely and effectively treat patients with CKD and patients on dialysis.
Associations Between HCV and CKDAn estimated 2.7-3.9 million people in the U.S. have chronic HCV infection, which is associated with increased risk of liver fibrosis or cirrhosis, development of hepatocellular carcinoma, and is the leading indication for liver transplants in the U.S.4 HCV infection is prevalent in patients with kidney disease; it is associated with progression to kidney failure, and with reduced survival in the CKD population.4,5,6,7 A study by Molnar et al. found that HCV infection is associated with higher mortality risk, incidence of decreased kidney function, and progressive loss of kidney function.8 Multivariate adjusted models showed HCV infection was associated with a 2.2-fold higher mortality (fully adjusted hazard ratio (aHR), 95%CI: 2.17(2.13-2.21)), and a 15% higher incidence of decreased kidney function (aHR, 95%CI: 1.15(1.12-1.17)).
Patients with CKD often have compromised immune systems and can be at increased risk for acquiring HCV infection. For example, patients receiving dialysis potentially have percutaneous HCV exposure from intravenous administration of treatments and potential for needle stick injury. Transplant recipients are at higher risk of infection from immunosuppression regimens used to prevent allograft rejection. Risk is also influenced by other factors that are not directly related to CKD, but individual characteristics (Table 1).
There has been a strong and likely causal association between chronic HCV infection and glomerular diseases, including mixed cryoglobulinemia, membranoproliferative glomerulonephritis (MPGN), membranous nephropathy, and polyarteritis nodosa (PAN).9,10,11
Overview of HCV EvaluationDiagnostic tests consist of two broad categories: (1) serologic assays that detect antibodies to HCV, and (2) molecular assays that detect or quantify HCV RNA.12 The Centers for Disease Control and Prevention (CDC) recommends a testing sequence for identifying current HCV infection, consisting of initial HCV antibody testing (either rapid or laboratory-conducted assay) followed by an HCV RNA assay for all positive antibody tests.4,13
Several organizations have provided guidelines for which individuals should be tested. All guidelines generally recommend screening patients at increased risk for HCV (Table 1).4,13,14 Testing of patients with CKD should be considered in all patients on dialysis and in CKD patients with unexplained proteinuria, microscopic hematuria, increased aminotransferase levels, or other known risk factors for HCV acquisition.6,15
Table 1: Risk Factors for HCV Testing4,14
• Born from 1945 through 1965
• Injected illicit drugs
• Clotting factor concentrates made prior to 1987
• Blood transfusions or solid organ transplants prior to July 1992
• Long-term hemodialysis treatment
• Healthcare-related exposure to HCV-infected blood
• Recipients of blood or organs from a donor later testing HCV positive
• HIV infection
• Signs or symptoms of liver disease (e.g., abnormal liver enzyme tests)
• Children born to HCV-positive mothers (test after age 18 months of birth)
• Receiving a tattoo in an unregulated setting
• Incarceration
2

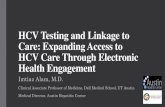
New Options in HCV ManagementResearch has led to a greater understanding of the HCV structure and life cycle. The HCV genome is a single-stranded, positive sense RNA strand with a nucleotide length of 9.6 kb, and encodes for a single polypeptide. (Figure 1).16 The virus is transmitted through blood and infects hepatocytes by interacting with co-receptors that results in its endocytosis, followed by fusion of the viral genome with the endosome and uncoating of its RNA, which is then cleaved into 10 viral proteins (3 structural and 7 nonstructural). There are at least six HCV genotypes (GT 1 - 6). Of the six genotypes, HCV GT 1-4 are the most commonly encountered clinically and HCV GT 1 is the most prevalent. Assessment of viral load and genotyping have been important determinants of successful therapeutic response to therapy.
Historically, therapy was based on interferon (IFN), pegylated interferon (pegIFN), and/or ribavirin (RBV). These therapies can be effective, but have been associated with lower SVR rates (compared to newer therapies), multiple side effects, and poor tolerability. IFN causes flu-like symptoms, autoimmune phenomenon, and psychiatric side effects. RBV causes hemolytic anemia, nausea, and fatigue. A meta-analysis by Fabrizi et al studying IFN/RBV in HCV-infected patients receiving hemodialysis showed a summary SVR rate of 56% and
discontinuation rate of 25%.17 Issues of suboptimal efficacy and tolerability have also been reported in non-dialysis CKD patients.18,19
A greater understanding of the of the HCV genome and proteins, coupled with ongoing unmet needs, has led to the discovery of multiple therapeutic targets. This, in turn has led to the development of a host of newer therapies known as direct-acting antivirals (DAAs), which are medications targeted at specific steps within the HCV life cycle. Typically, multiple classes are used in combination.
Single-class DAAs include simeprevir, sofosbuvir, and daclatasvir. Simeprevir is a macrocyclic noncovalent NS3/NS4A protease inhibitor for use in combination with IFN/RBV in HCV GT 1 infection. Sofosbuvir is a nucleotide analog NS5B polymerase inhibitor, for the treatment of HCV infection subtypes GT 1-4 as part of a regimen with RBV or IFN/RBV. Daclatasvir is a NS5A inhibitor, for use with sofosbuvir (with or without RBV) for the treatment of patients with chronic HCV GT 1 or 3 infection.
Multi-class combination antiviral medications for HCV infection include elbasvir-grazoprevir, glecaprevir-pibrentasvir, ledipasvir-sofosbuvir, ombitasvir-paritaprevir-ritonavir and dasabuvir, ombitasvir-paritaprevir-ritonavir, sofosbuvir-velpatasvir, and sofosbuvir-velpatasvir-voxilaprevir (Table 2).
Structure of HCV. HCV RNA encodes a polyprotein composed of about 3,000 amino acids. The core protein, and two envelope proteins are classified as structural proteins, while NS2, NS3, NS4A, NS4B, NS5A, and NS5B are non-structural proteins.
E1E2
IRES
Core E1 E2 NS2 NS3
Cleaved by host or virus proteases
Nucleocapsid
HCV viral particle
Lipidbilayer
Spike proteins
Structural proteins Non-structural proteins
Virus replication complexCore protein
HCV RNA
Viral (+) RNA
Viral (+) RNA
Viral (-) RNA
NS5ANS4 NS5Bp7
30001
A B
Figure 1: HCV Genomic RNA16
3

Elbasvir-grazoprevir is a once-daily tablet, which consists of a NS3/4A protease inhibitor (grazoprevir) and a NS5A replication complex inhibitor (elbasvir), approved for the treatment of chronic HCV GT 1 or 4 infections with or without RBV in adult patients. The Phase II/III C-SURFER trial evaluated elbasvir-grazoprevir in patients with HCV GT 1 infection and advanced CKD (stages 4 and 5, including patients on hemodialysis) with or without liver cirrhosis. The study showed that elbasvir-grazoprevir achieved an SVR12 in 94% of patients in the primary intent-to-treat (ITT) analysis, supporting the use of elbasvir-grazoprevir in patients with severely compromised kidney function.14,20,21
Ledipasvir-sofosbuvir is a multi-class DAA for the treatment of HCV GT 1, 4, 5, or 6, without cirrhosis or with compensated cirrhosis, or in combination with RBV in patients with decompensated cirrhosis. Ledipasvir is a NS5A inhibitor. Sofosbuvir-velpatasvir is another DAA combination for the treatment of adult patients with chronic HCV GT 1-6 infection, without cirrhosis or with compensated cirrhosis, or in combination with RBV in patients with decompensated cirrhosis. Velpatasvir is a NS5A inhibitor. No dosage recommendation can be given for patients with severe renal impairment (eGFR <30 mL/min/1.73m2) or with ESRD due to higher exposures (up to 20-fold) of the predominant sofosbuvir metabolite.22 Published reports have examined the use of sofosbuvir-based regimens in hemodialysis.23,24,25, Data from HCV-TARGET, a multicenter, longitudinal treatment cohort, showed that SVR12 rates of 82% - 83% were similar across eGFR groups (<30 mL/min; 31-45 mL/min; 46-60 mL/min; and >60 mL/min).26 Patients with eGFR ≤45 mL/min more frequently experienced anemia, worsening renal function and serious adverse events, suggesting the need for close monitoring of these patients.14,26 Studies have indicated successful use of sofosbuvir-containing regimens in kidney transplant recipients, with dose reductions in some cases.27,28
Paritaprevir-ritonavir-dasabuvir-ombitasvir is a multi-class DAA for the treatment of HCV GT1. Ombitasvir is a NS5A inhibitor, paritaprevir is a NS3/4A protease inhibitor, and ritonavir is a CYP3A inhibitor. These three therapies are combined as a fixed-dose tablet and dasabuvir (NS5B inhibitor) is a separate tablet. A single-arm, multicenter study showed an SVR12 of 90% in HCV GT1-infected patients with CKD stage 4/5 (including hemodialysis) treated with paritaprevir-ritonavir-dasabuvir-ombitasvir.29
Ombitasvir-paritaprevir-ritonavir is indicated in combination with RBV for the treatment of patients with HCV GT 4 infection without cirrhosis or with compensated cirrhosis.
Glecaprevir-pibrentasvir is a multi-class DAA for the treatment of HCV GT 1-6 without cirrhosis or with compensated cirrhosis. Glecaprevir is an NS3/4A protease inhibitor and pibrentasvir is an NS5A inhibitor. Data from the EXPEDITION-4 study showed that glecaprevir-pibrentasvir achieved an SVR12 of 98% (primary ITT) in HCV-infected patients with advanced CKD and on dialysis.30 The study included treatment-naive and -experienced patients (previous IFN or pegIFN ± RBV, or sofosbuvir and ribavirin ± pegIFN) with CKD stage 4 or 5 (including hemodialysis). The study supports the efficacy and safety of glecaprevir-pibrentasvir in patients with CKD and ESRD.14,30 The recommended duration of therapy is similar for patients without CKD. The MAGELLAN-2 study, which included liver (n=80) and kidney (n=20) transplant recipients, showed an SVR12 achieved in 99% of patients receiving glecaprevir-pibrentasvir.31
SummaryHCV infection has been associated with multiple adverse outcomes and increased risk in CKD and HCV progression. Newer treatment options are closing unmet medical needs, including pan-genotypic, multi-class combination DAAs, and offer the opportunity to manage HCV infection more effectively.
However, ongoing issues remain. For example, testing for HBV prior to starting therapy is generally recommended for DAAs, and protease inhibitors generally should be avoided in patients with decompensated cirrhosis.14,32,33,34 The U.S. Food and Drug Administration (FDA) required a Boxed Warning about the risk of HBV reactivation to be added to the drug labels of DAAs directing health care professionals to screen and monitor for HBV in all patients receiving DAA treatment.33 The presence of resistance-associated variants of HCV can attenuate the efficacy of DAAs.35 NS5A resistance variants can alter the length of therapy and necessitate the addition of RBV.
Other areas that require further study include the optimal timing of DAA therapy and impact on long-term outcomes (e.g., morbidity, mortality, quality-of-life) within the CKD population. However, overall recent data suggests that HCV-infected CKD patients can be effectively treated.
4

Table 2: Multi-Class Combination Direct Acting Antivirals36
Name Class/Description Genotype* Primary Metabolic Pathway
Recommendations for CKD (per Package Insert)
Elbasvir-Grazoprevir
- Elbasvir: NS5A inhibitor
- Grazoprevir: NS3/4A protease inhibitor
HCV GT 1 or 4
- Elbasvir: Hepatic- Grazoprevir: Hepatic
No restrictions/dose adjustments
Glecaprevir-Pibrentasvir
- Glecaprevir: NS3/4A protease inhibitor
- Pibrentasvir: NS5A inhibitor
HCV GT 1-6 - Glecaprevir: Hepatic- Pibrentasvir: Hepatic
No restrictions/dose adjustments
Ledipasvir-Sofosbuvir
- Ledipasvir: NS5A inhibitor
- Sofosbuvir: NS5B polymerase inhibitor
HCV GT 1,4,5, or 6
- Ledipasvir: Hepatic- Sofosbuvir: Renal
No dosage recommendation for patients with severe renal impairment (eGFR <30 mL/min) or with ESRD
Ombitasvir-Paritaprevir-Ritonavir and Dasabuvir
- Ombitasvir: NS5A inhibitor
- Paritaprevir: NS3/4A protease inhibitor
- Ritonavir: CYP3A inhibitor
- Dasabuvir: NS5B polymerase inhibitor
Chronic HCV GT 1
- Ombitasvir: Hepatic- Paritaprevir: Hepatic- Ritonavir: Hepatic- Dasabuvir: Hepatic
No restrictions/dose adjustments
Ombitasvir-Paritaprevir-Ritonavir
- Ombitasvir: NS5A inhibitor
- Paritaprevir: NS3/4A protease inhibitor
- Ritonavir: CYP3A inhibitor
HCV GT 4 - Ombitasvir: Hepatic- Paritaprevir: Hepatic- Ritonavir: Hepatic
No restrictions/dose adjustments
Sofosbuvir-Velpatasvir
- Sofosbuvir: NS5B polymerase inhibitor
- Velpatasvir: NS5A inhibitor
HCV GT 1-6 - Sofosbuvir: Renal- Velpatasvir: Hepatic
No dosage recommendation for patients with severe renal impairment (eGFR <30 mL/min) or with ESRD
Sofosbuvir-Velpatasvir-Voxilaprevir
- Sofosbuvir: NS5B polymerase inhibitor
- Velpatasvir: NS5A inhibitor
- Voxilaprevir: NS3/4A protease inhibitor
HCV GT 1-6 - Sofosbuvir: Renal- Velpatasvir: Hepatic- Voxilaprevir: Hepatic
No dosage recommendation for patients with severe renal impairment (eGFR <30 mL/min) or with ESRD
* Consult Package Insert for specific indications. CKD, chronic kidney disease; ESRD, end-stage renal disease; GFR, glomerular filtration rate;
HCV, Hepatitis C virus
Disclaimer: Information contained in this National Kidney Foundation educational resource is based upon current data available at the time of publication. Information is intended to help clinicians become aware of new scientific findings and developments. This educational resource is not intended to set out a preferred standard of care and should not be construed as one. Neither should the information be interpreted as prescribing an exclusive course of management.
5

1 Centers for Disease Control and Prevention (CDC). Blood safety: diseases and organisms. Available at: https://www.cdc.gov/bloodsafety/bbp/diseases-organisms.html. Accessed September 29, 2017.
2 Ladino M, Pedraza F, Roth D. Hepatitis C virus infection in chronic kidney disease. J Am Soc Nephrol. 2016;27:2238-2246.
3 Jadoul M, Martin P. Hepatitis C treatment in chronic kidney disease patients: the Kidney Disease Improving Global Outcomes (KDIGO) perspective. Blood Purif. 2017;43:206-209.
4 Centers for Disease Control and Prevention. Hepatitis C information. Available at: https://www.cdc.gov/hepatitis/hcv/index.htm. Accessed September 29, 2017.
5 Perico N, Cattaneo D, Bikbov B, Remuzzi G. Hepatitis C infection and chronic renal diseases. Clin J Am Soc Nepthol. 2009;4:207-220.
6 Kidney Disease: Improving Global Outcomes (KDIGO). KDIGO Clinical Practice Guidelines for the prevention, diagnosis, evaluation, and treatment of Hepatitis C in chronic kidney disease. Kidney Int. 2008;73(suppl 109):S1-S99.
7 Fabrizi F, Dixit V, Messa P. Impact of Hepatitis C on survival in dialysis patients: a link with cardiovascular mortality? J Viral Hepat. 2012;19:601-607.
8 Molnar M, Alhourani H, Wall B, et al. Association of Hepatitis C viral infection with incidence and progression of chronic kidney disease in a large cohort of U.S. veterans. Hepatology. 2015;61:1495-1502.
9 Kamar N, Rostaing L. Glassock R, Hirsch M, Lam A (Eds). Overview of renal disease associated with Hepatitis C virus infection. UptoDate, Waltham MA. Accessed September 29, 2017.
10 McGuire B, Julian B, Bynon J, et al. Glomerulonephritis in patients with Hepatitis C virus cirrhosis undergoing liver transplantation. Ann Intern Med. 2006;144:735.
11 Tarantino A, Campise M, Banfi G, et al. Long-term predictors of survival in essential mixed cryoglobulinemic glomerulonephritis. Kidney Int.1995;47:618.
12 Terrault N, Chopra S. Di Bisceglie A, Bloom A (eds.). Diagnosis and evaluation of chronic Hepatitis C virus infection. UptoDate, Waltham MA. Accessed September 29, 2017.
13 Centers for Disease Control and Prevention (CDC). Testing for HCV infection: an update of guidance for clinicians and laboratorians. MMWR Morb Mortal Wkly Rep. 2013;62:362-365.
14 American Association for the Study of Liver Diseases, and the Infectious Diseases Society of America (AASLD-IDSA). Recommendations for testing, managing, and treating Hepatitis C. Available at: http://www.hcvguidelines.org. Accessed September 29, 2017.
15 Gordon C, Balk E, Becker B, et al. KDOQI US commentary on the KDIGO Clinical Practice Guideline for the prevention, diagnosis, evaluation, and treatment of Hepatitis C in CKD. Am J Kidney Dis. 2008;52:811-825.
16 Moriishi K, Matsuura Y. Exploitation of lipid components by viral and host proteins for Hepatitis C virus infection. Front Microbiol. 2012;3:54.
17 Fabrizi F, Dixit V, Martin P, et al. Combined antiviral therapy of Hepatitis C virus in dialysis patients: meta-analysis of clinical trials. J Viral Hepat. 2011;18:e263-e269.
18 Fried M, Shiffman M, Reddy K, et al. Peginterferon alfa-2a plus ribavirin for chronic Hepatitis C virus infection. N Engl J Med. 2002;347:975-982.
19 McHutchinson J, Lawitz E, Shiffman M, et al. Peginterferon alfa-2b or alfa-2a with ribavirin for treatment of Hepatitis C infection. N Engl J Med. 2009;361:580-593.
20 Roth D, Nelson D, Bruchfeld A, et al. Grazoprevir plus elbasvir in treatment-naive and treatment-experienced patients with Hepatitis C virus genotype 1 infection and stage 4-5 chronic kidney disease (The C-SURFER Study): a combination phase 3 study. Lancet. 2015;386:1537-1545.
21 Bhamidimarri K. Grazoprevir plus elbasvir and other treatment options in Hepatitis C infected patients with stage 4–5 chronic kidney disease. Ann Transl Med. 2016;4(suppl 1):S13.
22 Sofosbuvir (Solvadi) Package Insert. Accessed September 29, 2017.23 Hundemer G, Sise M, Wisocky J, et al. Use of sofosbuvir-based
direct-acting antiviral therapy for Hepatitis C viral infection in patients with severe renal insufficiency. Infect Dis (Lond). 2015;47:924-929.
24 Nazario H, Ndungu M, Modi A. Sofosbuvir and simeprevir in Hepatitis C genotype 1- patients with end-stage renal disease on hemodialysis or GFR <30mL/min. Liver Int. 2016;36:798-801.
25 Kalyan Ram B, Frank C, Adam P, et al. Safety, efficacy and tolerability of half-dose sofosbuvir plus simeprevir in treatment of Hepatitis C in patients with end-stage renal disease. J Hepatol. 2015;63:763-765.
26 Saxena V, Koraishy F, Sise M, et al; HCV-TARGET. Safety and efficacy of sofosbuvir-containing regimens in Hepatitis C-infected patients with impaired renal function. Liver Int. 2016;36:807-816.
27 Sawinski D, Kaur N, Ajeti A, et al. Successful treatment of Hepatitis C in renal transplant recipients with direct-acting antiviral agents. Am J Transplant. 2016;16:1588-1595.
28 Kamar N, Marion O, Rostaing L, et al. Efficacy and safety of sofosbuvir-based antiviral therapy to treat Hepatitis C virus infection after kidney transplantation. Am J Transplant. 2016;16:1474-1479.
29 Pockros P, Reddy K, Mantry P, et al. Efficacy of direct-acting antiviral combination for patients with Hepatitis C virus genotype 1 infection and severe renal impairment or end-stage renal disease. Gastroenterology. 2016;150:1590-1598.
30 Gane E, Lawitz E, Pugatch D, et al. EXPEDITION-4: Efficacy and safety of glecaprevir/pibrentasvir (ABT-493/ABT-530) in patients with renal impairment and chronic Hepatitis C virus genotype 1-6 infection. American Association for the Study of Liver Diseases (AASLD). The Liver Meeting. Boston, MA. November 2016.
31 Reau N, Kwo P, Rhee S, et al. MAGELLAN-2: safety and efficacy of glecaprevir/pibrentasvir in liver or renal transplant adults with chronic Hepatitis C genotype 1-6 infection. J Hepatol. 2017;66:S90-S91.
32 Bersoff-Matcha S, Cao K, Jason M, et al. Hepatitis B virus reactivation associated with direct-acting antiviral therapy for chronic Hepatitis C virus: a review of cases reported to the U.S. Food and Drug Administration Adverse Event Reporting System. Ann Intern Med. 2017;166:792-798.
33 FDA Drug Safety Communication: FDA warns about the risk of Hepatitis B reactivating in some patients treated with direct-acting antivirals for Hepatitis C. Available at: https://www.fda.gov/Drugs/DrugSafety/ucm522932.htm. Accessed October 10, 2017.
34 Ferenci P, Kozbial K, Mandorfer M, Hofer H. HCV targeting of patients with cirrhosis. J Hepatol. 2015;63:1015-1022.
35 Nitta S, Asahina Y, Matsuda M. Effects of resistance-associated NS5A mutations in Hepatitis C virus on viral production and susceptibility to antiviral reagents. Sci Rep. 2016;6:34652.
36 Package Inserts: Elbasvir-Grazoprevir (Zepatier), Glecaprevir-Pibrentasvir (Mavyret), Ledipasvir-Sofosbuvir (Harvoni), Ombitasvir-Paritaprevir-Ritonavir and Dasabuvir (Viekira Pak), Ombitasvir-Paritaprevir-Ritonavir (Technivie), Sofosbuvir-Velpatasvir (Epclusa), Sofosbuvir-Velpatasvir-Voxilaprevir (Vosevi). Accessed September 29, 2017.
References
30 East 33rd Street, New York, NY 10016 800.622.9010 | kidney.org
© 2018 National Kidney Foundation, Inc. All rights reserved. 02-10-7769_KBH
Supported by


















