M yocarditis and inflammatory cardiomyopathy: microbiological and
15
Cardiovascular Research 60 (2003) 11–25 www.elsevier.com / locate / cardiores Review Myocarditis and inflammatory cardiomyopathy: microbiological and molecular biological aspects * Fiorella Calabrese , Gaetano Thiene Department of Pathology, University of Padua Medical School, Via Gabelli, 61, 35121 Padua, Italy Received 5 February 2003; received in revised form 20 May 2003; accepted 5 June 2003 Abstract Myocarditis is an inflammatory disease of the myocardium associated with cardiac dysfunction. The natural history of myocarditis is frequently characterised by the evolution in dilated cardiomyopathy. Due to its variable clinical manifestation from latent to very severe clinical forms, such as acute congestive heart failure and sudden death, its prevalence is still unknown and probably underestimated. In spite of the development of various diagnostic modalities, early and definite diagnosis of myocarditis still depends on the detection of inflammatory infiltrates in endomyocardial biopsy specimens according to the Dallas criteria. Routine application of immuno- histochemistry, used for identification and characterisation of inflammatory cell populations, has now significantly increased the sensistivity of the diagnosis of inflammatory cardiomyopathy.Various molecular techniques, such as PCR, gene sequencing and real-time PCR, often applied on the same endomyocardial specimen, have become an essential part of the diagnostic armamentarium for rapid, specific and sensitive identification of infective agents. The correct application of molecular techniques will allow increasingly more information to be obtained: new epidemiology, new patient risk stratification and overall more appropriate medical treatment. 2003 European Society of Cardiology. Published by Elsevier B.V. All rights reserved. Keywords: Myocarditis; Cardiomyopathy; Inflammation; Inflammation / infection 1. Introduction: role of endomyocardial biopsy sis, is a frequent observation. This subtle substrate, to- gether with the possible inflammatory involvement of the According to the current WHO classification of car- conduction system, seems highly arrhythmogenic and may diomyopathies, myocarditis is an inflammatory heart mus- account for unexpected arrhythmic cardiac arrest [3]. cle disease associated with cardiac dysfunction, and dilated Heterogeneity of symptoms, including subclinical or cardiomyopathy (DC) may represent the chronic phase of asymptomatic forms, could be the reason why the preval- the disease [1]. Clinical features of the disease are variable ence of myocarditis is still unknown and probably under- including unexplained congestive heart failure, chest pain estimated. The large spectrum of clinical forms—from mimicking myocardial infarction [2], arrhythmias, syncope subclinical to severe—depends on several factors such as and sudden death. Sudden death may occur both in the genetic determinants of infective agents, the genetics, age active or healed phases as a consequence of life-threaten- and gender of the host, and host immunocompetence. ing ventricular arrhythmias that develop mostly in the In spite of the development of various diagnostic setting of an unstable vulnerable myocardial substrate, modalities, early and definite diagnosis of myocarditis still namely inflammatory infiltrates, interstitial edema, myocar- depends on the detection of inflammatory infiltrates in dial necrosis and fibrosis. Patchy inflammatory infiltrate, in endomyocardial biopsy (EMB) specimens according to the the form of a starry sky-like feature ( ,14 leucocytes / Dallas criteria [4]. The major limitation of EMB remains 2 mm ), and not necessarily associated with myocyte necro- the low sensitivity due to sampling error, particularly in the presence of focal disease. The size and number of the heart biopsy specimens as well as the processing of *Corresponding author. Tel.: 139-049-827-2268; fax: 139-049-827- 2269. E-mail address: [email protected] (F. Calabrese). Time for primary review 21 days. 0008-6363 / 03 / $ – see front matter 2003 European Society of Cardiology. Published by Elsevier B.V. All rights reserved. doi:10.1016 / S0008-6363(03)00475-9 Downloaded from https://academic.oup.com/cardiovascres/article-abstract/60/1/11/321091 by guest on 03 April 2019
Transcript of M yocarditis and inflammatory cardiomyopathy: microbiological and

Cardiovascular Research 60 (2003) 11–25www.elsevier.com/ locate/cardiores
Review
M yocarditis and inflammatory cardiomyopathy: microbiological andmolecular biological aspects
*Fiorella Calabrese , Gaetano ThieneDepartment of Pathology, University of Padua Medical School, Via Gabelli, 61, 35121Padua, Italy
Received 5 February 2003; received in revised form 20 May 2003; accepted 5 June 2003
Abstract
Myocarditis is an inflammatory disease of the myocardium associated with cardiac dysfunction. The natural history of myocarditis isfrequently characterised by the evolution in dilated cardiomyopathy. Due to its variable clinical manifestation from latent to very severeclinical forms, such as acute congestive heart failure and sudden death, its prevalence is still unknown and probably underestimated. Inspite of the development of various diagnostic modalities, early and definite diagnosis of myocarditis still depends on the detection ofinflammatory infiltrates in endomyocardial biopsy specimens according to the Dallas criteria. Routine application of immuno-histochemistry, used for identification and characterisation of inflammatory cell populations, has now significantly increased thesensistivity of the diagnosis of inflammatory cardiomyopathy. Various molecular techniques, such as PCR, gene sequencing and real-timePCR, often applied on the same endomyocardial specimen, have become an essential part of the diagnostic armamentarium for rapid,specific and sensitive identification of infective agents. The correct application of molecular techniques will allow increasingly moreinformation to be obtained: new epidemiology, new patient risk stratification and overall more appropriate medical treatment. 2003 European Society of Cardiology. Published by Elsevier B.V. All rights reserved.
Keywords: Myocarditis; Cardiomyopathy; Inflammation; Inflammation/ infection
1 . Introduction: role of endomyocardial biopsy sis, is a frequent observation. This subtle substrate, to-gether with the possible inflammatory involvement of the
According to the current WHO classification of car- conduction system, seems highly arrhythmogenic and maydiomyopathies, myocarditis is an inflammatory heart mus- account for unexpected arrhythmic cardiac arrest[3].cle disease associated with cardiac dysfunction, and dilated Heterogeneity of symptoms, including subclinical orcardiomyopathy (DC) may represent the chronic phase of asymptomatic forms, could be the reason why the preval-the disease[1]. Clinical features of the disease are variable ence of myocarditis is still unknown and probably under-including unexplained congestive heart failure, chest pain estimated. The large spectrum of clinical forms—frommimicking myocardial infarction[2], arrhythmias, syncope subclinical to severe—depends on several factors such asand sudden death. Sudden death may occur both in the genetic determinants of infective agents, the genetics, ageactive or healed phases as a consequence of life-threaten- and gender of the host, and host immunocompetence.ing ventricular arrhythmias that develop mostly in the In spite of the development of various diagnosticsetting of an unstable vulnerable myocardial substrate, modalities, early and definite diagnosis of myocarditis stillnamely inflammatory infiltrates, interstitial edema, myocar- depends on the detection of inflammatory infiltrates indial necrosis and fibrosis. Patchy inflammatory infiltrate, in endomyocardial biopsy (EMB) specimens according to thethe form of a starry sky-like feature (,14 leucocytes/ Dallas criteria[4]. The major limitation of EMB remains
2mm ), and not necessarily associated with myocyte necro- the low sensitivity due to sampling error, particularly inthe presence of focal disease. The size and number of theheart biopsy specimens as well as the processing of*Corresponding author. Tel.:139-049-827-2268; fax:139-049-827-
2269.E-mail address: [email protected](F. Calabrese). Time for primary review 21 days.
0008-6363/03/$ – see front matter 2003 European Society of Cardiology. Published by Elsevier B.V. All rights reserved.doi:10.1016/S0008-6363(03)00475-9
Dow
nloaded from https://academ
ic.oup.com/cardiovascres/article-abstract/60/1/11/321091 by guest on 03 April 2019

12 F. Calabrese, G. Thiene / Cardiovascular Research 60 (2003) 11–25
myocarditis of|50% using four to five biopsy samples.When 17 biopsy specimens per case were considered, thesensitivity reached 79%[7]. It has also been shown thatserial sectioning and multiple level examination of EMBsincrease the sensitivity of EMB in the evaluation ofmyocarditis[9,10], thus facilitating the diagnosis of focalmyocarditis with a rate of sensitivity similar to that indiffuse myocarditis[10].
Although some authors have demonstrated that biven-tricular EMB (obtaining several samples from multipleareas of the left and right ventricles) may improve thesensitivity in the detection of myocarditis[11], it should beemphasised that this aggressive approach increases the riskof complications. However most experts in the field agreethat an actual increase in the sensitivity of EMB has nowbeen reached using immunohistochemistry together withroutine histology. A large panel of monoclonal and poly-clonal antibodies is now mandatory to identify and char-acterize the inflammatory cell population as well as theactivated immunological processes[12–15].
Even though sampling and processing techniques havesignificantly increased the sensitivity of EMB in theevaluation of myocarditis, morphological analysis today isstill greatly limited in the detection of infective pathogens,particularly viral agents, the commonest cause of inflam-matory cardiomyopathy (IC). Viral myocarditides usually
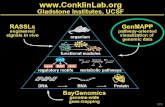
Fig. 1. Adenoviral (AV) myocarditis in a young adult man (37 years old). lack specific cytopathic effects (Fig. 1a,b), especially those(a) Histology of EMB showing lymphomonocyte inflammatory cell caused by RNA viruses. With the exception of some rareinfiltrates associated with myocyte injury. No viral inclusion bodies are
forms of cytomegaloviral myocarditis, these effects, whenevident. Hematoxylin and eosin3100. (b) PCR analysis for adenovirus:observed, neither necessarily imply the presence nor arelane 1: DNA marker; lane 2: AV positive control; lane 3: EMB AV PCR
positive; lane 4: beta-globin (house-keeping gene); lane 5: negative useful in detecting the type of virus, since they maycontrol (reagents without template). represent degenerative changes or myocyte nuclear hy-
perplasia.
specimens are known to influence the sensitivity of EMBin the detection of myocarditis. 2 . Etiology
The greater sensitivity of the Stanford-Caves and Cordisbioptomes over other small bioptomes has been proven by IC has multiple causes, both non-infectious and infecti-previous reports[5,6]. In particular, the number of biopsy ous, and viruses account for the disease in the majority ofsamples also directly increases the likelihood of detecting paediatric cases (Table 1).foci of myocarditis. Chow et al.[7] and Hauck et al.[8] Different cardiotropic viruses have been implicated inindependently reported a sensitivity for detection of more than 50% of paediatric cases with IC[16,17]. The
T able 1Myocarditis: infective agents
Viruses RNA Picornavirus (entero, rhino); orthomyxovirus (influenza A,B); paramyxovirus (rubeola, mumps);retrovirus (HIV-1); hepatitis C virus (HCV)
Viruses DNA Adenovirus, herpesvirus (cytomegalo, Epstein–Barr virus, varicella-zoster), Parvovirus BigBacteria Staphylococcus, Streptococcus, Pneumococcus, Meningococcus, Gonococcus,
Salmonella, Corynebacterium diphtheriae, Haemophilus influenzae,Mycoplasma pneumoniae, Brucella species
Mycobacteria Tuberculosis, Avium intracellulare,LepraeFungi Aspergillus, Candida, Actinomyces, Blastomyces, Cryptococcus, HistoplasmaProtozoa Toxoplasma gondii, Trypanosoma cruziRickettsiae Coxiella burnetti (Q fever),Rickettsia rickettsii, Rickettsia tsutsugamuschiChlamydiae Trachomatis, PsittaciParasitic Trichinella spiralis
Dow
nloaded from https://academ
ic.oup.com/cardiovascres/article-abstract/60/1/11/321091 by guest on 03 April 2019

F. Calabrese, G. Thiene / Cardiovascular Research 60 (2003) 11–25 13
remaining forms may be triggered by other environmental the characteristic cytomegaly, and the intranuclear inclu-factors such as toxins, alcohol, cytotoxic chemotherapy, sions may not be basophilic[34–36].metabolic abnormalities or more frequently sustained by During or following mumps, mild or subclinicalimmunologic mechanisms. These latter may characterize myocardial infection may be present with 15% of casesthe autoimmune myocarditis ab initio or more often are the showing ST-T wave changes. Mumps-induced myocarditisconsequence of viral myocarditis itself[18]. has been demonstrated to be the first step in the patho-
Among cardiotropic viral agents, coxsackie viruses are genesis of endocardial fibroelastosis[17,37]. In recentthought to be most frequently implicated[19,20]. Group B years the incidence of the disease, which was previouslycoxsackie viruses consist of six serotypes within the considered a significant cause of infant mortality, hasenterovirus genusPicornaviridae, a large family of single- dramatically declined, probably due to mumps vaccine.stranded positive-sense RNA viruses. In the WHO record Parvovirus B19, the causative agent of erythema infec-during the 10-year period from 1975 through 1985, the tiosum, also called fifth disease, has been reported to be acoxsackie B viruses represent the most frequent inflamma- rare but severe cause of myocarditis in infants and childrentory agents in cardiovascular disease (34.6 per 1000), [38–40]. The virus has also been considered as beingfollowed by influenza B virus (17.4 per 1000), influenza A responsible for hydrops fetalis and foetal death[41,42].(11.7 per 1000), coxsackie A (9.1 per 1000) and cyto- The B19 receptor (erythrocyte P antigen) has been recog-megalovirus (CMV) (8.0 per 1000)[21]. nized on foetal myocardial cells[38,42] suggesting that
The prevalence of the enteroviruses as infective agents intrauterine myocarditis contributes to the development ofassociated with myocarditis has been reported in several fetal hydrops after parvovirus B19 infection.clinical studies[19–22]. Patients with IC had significantly The importance of hepatitis C virus (HCV) in patientshigher serological titres when compared with controls with myocarditis and DC has recently been stressed[43–[23–25]. In contrast, a coxsackie virus infection could be 45]. Myocyte tropism has also been demonstrated byproven in only 2% of consecutively studied myocarditis Takeda et al. using in situ hybridisation[46] and recentlypatients in a 5-year study at a military hospital in Finland, by our group using immunohistochemistry with TORDJI-where traditional enteroviral diagnostic methods were used 22 monoclonal antibody[45].[26]. Variable aetiology was found and was mainly repre- IC caused by other non-viral infective agents is nowa-sented by vaccine inoculation, followed by other infective days rare. It usually occurs in immunosuppressed patientsagents such as adenovirus, Epstein–Barr virus,Myco- with secondary involvement of the myocardium.plasma pneumoniae and Chlamydia. Myocarditis is the most common cause of death in
Using molecular techniques, the frequency of myocar- diphtheria by the action of exotoxin produced bydial enteroviral infection is now estimated in|30–50% of Corynebacterium diphtheriae. Although still a cause ofcases with infectious etiology[16,17,27,28].Various respi- morbidity and mortality in developing countries[47],ratory tract viruses—adenoviruses, Epstein–Barr viruses diphtheria is now rare in the West, most probably because(EBV), influenza viruses, etc.—may cause myocarditis at of vaccination. It re-appeared in Scandinavia in the mid-variable frequencies[20,21,26,29]. In particular, adeno- 1980s, mostly in alcoholics[48].viruses have been shown to be an important cause of Non-rheumatic myocarditis may be a complication ofmyocarditis and dilated cardiomyopathy both in childhood beta-haemolytic streptococci (Streptococcus pyogenes),[16,17] and adulthood[30]. due to bacterial exotoxins[49]. Rheumatic carditis with
It is noteworthy that rhinovirus-associated myocarditis involvement of both the valvular apparatus andhas been rarely reported in the literature[31], although perimyocardium accounts for the majority of pediatricseveral cases have been registered with the U.S. Centers hospitalizations and cardiac deaths world-wide, particu-for Disease Control[21]. larly in developing countries. Immune responses to group
Cytomegalovirus (CMV) is a recognized cause of acute A streptococcal antigens during pharyngitis, resulting ininfectious myocarditis in the herpes group of viruses, antibodies and immunocompetent cells that cross-reactalthough CMV is considered to be uncommon in previous- with myocardial antigens, are thought to be central to thely healthy people[32]. However some authors detected a pathogenesis of rheumatic carditis. The recent finding ofCMV-specific genome in the myocytes of EMBs in up to enteroviral RNA replication and protein synthesis in15% of patients with acute myopericarditis[33]. Therefore valvular tissue from patients with chronic rheumatic heartCMV infection may be considered a more frequent cause disease may provide intriguing evidence for a viral etiolo-of myocarditis than was previously thought. CMV in- gy or cofactor, at least in some cases[50]. Bacterialfection is a peculiar viral disease in transplant recipients, endotoxin is also considered to play a role in meningococ-with multiorgan involvement[32–34], since specific cyto- cal myocarditis. Myocarditis has been found in up to 78%pathic features are only exceptionally observed. In trans- of cases of meningococcal septicaemia with marked endo-planted patients, treated with ganciclovir for a previous toxinaemia[51].CMV infection, the biopsy features of CMV myocarditis Even though rarely, myocarditis has been found inappear modified since the infected cells often do not show Salmonella septicaemia caused bySalmonella typhi or
Dow
nloaded from https://academ
ic.oup.com/cardiovascres/article-abstract/60/1/11/321091 by guest on 03 April 2019

14 F. Calabrese, G. Thiene / Cardiovascular Research 60 (2003) 11–25
paratyphi. Yersiniosis myocarditis, probably more frequent the increasing number of immunocompromised patients.than is commonly thought, is in most cases a quite mild The major risk factors for severe fungal disease includeform and considered to be immune in the pathogenesis administration of broad-spectrum antibiotics, corticoste-[52]. Myocarditis is a well documented complication (1– roids and cytotoxic agents, invasive medical procedures8% of cases) inBorrelia burgdorrferi infection. In- and HIV. In this latter condition the association of fungalvolvement of the specialized myocardium may account the and other infective agents may be quite frequent[67].onset of atrioventricular block[53]. Mycoplasma pneumo- Pre-mortem diagnosis of fungal myocarditis is difficultniae infection is commonly accompanied by mild myocar- since clinical findings of myocardial involvement are oftenditis with up to 33% of cases exhibiting ECG changes[54]. absent or ambiguous, blood cultures are often negative and
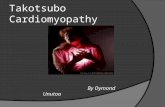
Chlamydia psittaci infection is complicated by sub- other laboratory tests are not effective.clinical or asymptomatic myocarditis in 5–15% of cases Among parasitic infections,Trichinella spiralis is most[55], but cardiac insufficiency may be marked[56]. In prone to cause myocarditis, however other elmints canChlamydia trachomatis infection myocarditis is rare. A infect the myocardium usually in the setting of multi-organfew published cases have been reported in the literature, involvement (Fig. 2a–d).even fatal, with the majority of these involving smallchildren [55]. Chlamydia pneumoniae infection combinedwith myocarditis has been also described as a mild form 3 . Pathogenesis[57], although one case of sudden death in a young athlete[58]. Acute myocarditis, more frequently viral forms, can be
Cardiac involvement is often found in the setting of resolved without sequela, however progression in therickettsial infection with vasculitis as a prominent feature, chronic form, DC, is not a rare event. Two differentbecause the rickettsiae have special tropism for endothelial theories have been recognized to explain myocyte damagecells. Even though endocarditis is considered more com- and the progression from acute myocarditis to chronicmon, myocarditis may also present in Q fever caused by forms/DC: autoimmunity and direct cytotoxicity due toCoxiella burnetii [59]. persistent viral infection.
Tripanozoma cruzi (Chagas’ disease) is a well-recog-nized cause of myocarditis and cardiomyopathy in both 3 .1. Autoimmunityurban and rural areas of South America[60]. Also theAfrican trypanosomes,Tripanozoma gambiense and Tri- In 1957 Witebsky et al., modelling on Koch’s post-panozoma rhodesiense, occasionally cause myocarditis and ulates, proposed rationales to explain the autoimmuneinflammatory cardiomyopathy[61]. basis of clinical disease: an autoimmune response, as either
Toxoplasma gondii poses significant problems among humoral or cell-mediated, is recognized when a specificrecipients of cardiac transplants. A study reported that 57% antigen is identified and when an analogous autoimmuneof transplanted patients lacking antibodies to that agent response is induced in an experimental animal[68].developed toxoplasma myocarditis[62]. However, tox- Aberrant cellular and humoral immune responses haveoplasmosis may become reactivated in antibody-positive been proposed to explain the progression of viral myocar-transplant recipients, and myocarditis has been reported in ditis.4–53% of transplant cases. This great variation rate isprobably due to differences in antibody testing methods 3 .1.1. Aberrant cellular immune response[63]. After the introduction of pyrimethamine prophylaxis, The original discovery that T-cells play a major role inthis complication has decreased substantially. the pathogenesis of coxsackie virus B infection was
Myocarditis seems to be quite frequent in AIDS pa- reported over two decades ago. Mice depleted of T-cells bytients, with a rate of 45–52% of cases[64]. Cardiac pre-treatment with antithymocyte serum and then infecteddysfunction in AIDS may, however, have various forms of with coxsackie virus B3 exhibit a marked reduction inpathogenesis. The aetiology of myocarditis in AIDS is also myocardial disease. The degree of cardiac inflammationvariable and may be difficult to establish, especially in and necrosis was much less than that found in immuno-cases with multiple opportunistic infections. Viruses are logically intact mice or in mice reconstituted with bothconsidered to be the most common cause, such as the bone marrow and thymus cells[69].human immunodeficiency virus (HIV) itself and coxsackie Inflammation of the heart muscle can be transferred intoviruses. In one autopsy study,Toxoplasma gondii infection non-immunized recipient mice by purified T-cells fromof the myocardium was found in 12% of cases[65]. mice with active myocarditis[70].
Fungal myocarditis frequently occurs in the setting ofdisseminated disease. The major fungal pathogen respon-3 .1.2. Aberrant humoral immune responsesible for myocardial infection isAspergillus fumigatus The hypothesis that humoral immunity plays a role in[66]. The incidence of invasive fungal disease has dramati- the development of post-infectious myocarditis is derivedcally increased over the past few decades corresponding to from the finding that immunization with cardiac myosin in
Dow
nloaded from https://academ
ic.oup.com/cardiovascres/article-abstract/60/1/11/321091 by guest on 03 April 2019

F. Calabrese, G. Thiene / Cardiovascular Research 60 (2003) 11–25 15
Fig. 2. EMB in multiorganToxocara canis infection. Toxocara larva in myocardium (hematoxylin and eosin3100) (a) with birefringence of the larva atpolarized light (b) and giant cell granulomatous reaction hematoxylin and eosin360 (c). Toxocara larva in liver biopsy (cross-section), hematoxylin andeosin330 (d). Courtesy of Dr F. Bomio, Lugano, Switzerland.
susceptible strains of mice induces myocarditis[71]. This deduced amino acid sequence of viral precursor polypro-result was further supported by subsequent studies: mice tein with the sequence of murine cardiac myosin showedimmunized with cardiac C protein[72] or streptococcal M however a very low degree of genetic homology[80].protein peptide[73] developed T-cell dependent myocar- It is very likely that the development of autoimmuneditis, or adoptive transfer of myosin-reactive cells or myocarditis following viral myocarditis is sustained by asplenocytes after myocardial infarction[74] or transplanta- complex interaction between cellular and humoral immunetion of a normal heart into a virus-treated host after response as proposed by Rose and Hill[80].documentation of viral clearance[75] led to the develop- Abnormal human leucocyte antigen (HLA) expressionment of T-cell dependent myocarditis. Even though cel- on endomyocardial biopsy[12,13,81] increased levels oflular necrosis may explain the presentation of cardiac circulating cytokines and cardiac autoantibodies[82,83]released myosin to the immune system thus triggering the are similarly also found in human myocarditis /DC, highlyautoimmune disease, recent studies suggest that molecular suggestive of an immune pathogenetic mechanisms of viralmimicry may also be involved in the pathogenesis of myocarditis in the clinical setting.autoimmune myocarditis.
The finding of cross-reactive epitopes between cardiac 3 .2. Persistent viral infectionmyosin and infectious agents confirms this concept[76–78]. Molecular mimicry has been proposed as an explana- Continuous virus replication or persistent viral infectiontion for coxsackie virus B3-induced autoimmune myocar- in the heart could play a role in the maintenance and/orditis. The hypothesis is supported by data from studies of progression of disease.monoclonal antibodies directed against coxsackie virus Molecular investigations have shown coxsackie virus B3group B that recognizes epitopes on murine cardiac myosin to persist in mouse myocardium in different models for up[79]. Comparison of the nucleotide sequence and the to 56 days[84,85] and in hamsters for up to 180 days[85].
Dow
nloaded from https://academ
ic.oup.com/cardiovascres/article-abstract/60/1/11/321091 by guest on 03 April 2019

16 F. Calabrese, G. Thiene / Cardiovascular Research 60 (2003) 11–25
Viral RNA was found to persist from 80 days to 12 months above), have various limits because of low sensitivity andin other non-productive picornavirus myocardium infec- specificity.tions in mice[86]. Molecular studies in various experimen-tal models show that enterovirus can persist in the chronic 4 .1. Culturestages of myocarditis[87]. The mechanisms of enteroviruspersistence so far is not well known. A defective virus, It is important to recognize that the traditional methodsmainly resulting from the altered function of the viral RNA of pathogen identification by culture isolation, phenotypicpolymerase[88], is now considered to be one of the expression via biochemical reactions and determination ofpossible mechanisms of persisting enteroviral infection. antibiotic sensitivity remain the gold standard for|90% ofTherefore acute myocytolytic inflammatory disease infectious disease pathogens. However many infectiveevolves to persistent infection with a defective virus, agents, particularly viruses, can not be cultivated as theyunable to induce cytolysis or elicit the host cellular are very difficult to isolate.immune response. For many viruses, such as enteroviruses, isolation
Tam and Messner recently demonstrated that viral RNA procedures are poorly standardized and virus isolation dataperseveres in a double-stranded form in a murine model of may vary considerably among laboratories. The type andcoxsackie virus B1 infection of skeletal muscle. It is quality of the specimen, the timing of specimen collection,possible that double-stranded RNA is resistant to ribonu- and storage before arrival in the laboratory can highlyclease activity and is connected to reduced viral antigen influence the sensitivity[96]. The choice of cell types usedexpression, which in turn minimizes immune-mediated for virus isolation is also important. For example no singlekilling of persistently infected cells[89]. Therefore, if cell line supports the growth of all known enteroviruscoxsackie virus B3 persists in a double-stranded form, it serotypes[97] and many serotypes of adenovirus do notmay be responsible for the long half-life of viral RNA replicate efficiently in conventional cell cultures (Hep-2during the chronic phase of infection. and A549 cells)[98].
Recently some authors have demonstrated that coxsackie Virus isolation from blood components is useful forvirus B3 protease 2A can directly cleave dystrophin in providing evidence of systemic infection but not formyocytes, these data support the idea of a mechanism of providing information on specific organ disease.direct viral destruction during the pathogenesis of chronic Detection of enterovirus in the alimentary tract (throatmyocarditis /DC[90]. swabs, rectal swabs, or stool specimens) allows only
The activation of mitogen-activated protein kinase circumstantial evidence of etiology, since viral shedding at(MAPK) as a consequence of the P21 guanosine tri- these sites may occur in asymptomatic subjects, especiallyphosphatase-activating protein (RasGAP) cleavage, has in infants and during epidemic seasons[99].been more recently suggested to also play a role in the Isolation of a virus, particularly of enterovirus fromdevelopment of chronic myocarditis. The MAPK pathway affected tissues of patients with severe inflammatoryis a mechanism employed by different viruses for control myocardial diseases, has seldom been successful[100–of cell proliferation and survival[91]. During enteroviral 103].replication, activation of MAPKs may participate in themobilization of intracellular calcium and may thereby 4 .2. Serologycontribute to morphological and physiological destructionof infected myocytes[92]. Following the isolation of a virus, the identification and
Several studies have also documented viral persistence overall serotypic characterization can be determined byin the myocardium of patients with DC until end-stage neutralization of infectivity with serotype-specific antisera.disease requiring cardiac transplantation[28,93–95]. Serologic diagnosis requires demonstration of IgM
antibody or a fourfold increase in IgG antibody titre whenpaired serologies are obtained and is therefore retrospec-
4 . Diagnostic tools for infective myocarditis tive.Every viral family includes, however, a large number of
Different diagnostic tools are known to detect infective serotypes (among the family Picornaviridae, 66 serotypesagents responsible for IC. Non-viral infective agents are have been identified for the genus enterovirus) and typingoften morphologically distinctive and identifiable by direct by neutralization, with reference antisera for all serotypesmicroscopic examination with routine and special stains individually, is surely not practical. In order to overcome(Gram’s, Gomori’s, periodic acid-Schiff, Ziehl-Neelsen, this problem for the enterovirus family, equine type-spe-etc.). For these forms microbiologic culture and other cific hyperimmune sera have been mixed to providelaboratory tests are considered important for definitive intersecting pools containing different combinations ofidentification of causative infective agents. individual antisera[96].
For viruses, the main pathogens of IC, traditional Serotypic identification of an enterovirus isolate general-diagnostic tools, including morphological analysis (see ly takes 1–2 weeks and usually has little impact on patient
Dow
nloaded from https://academ
ic.oup.com/cardiovascres/article-abstract/60/1/11/321091 by guest on 03 April 2019

F. Calabrese, G. Thiene / Cardiovascular Research 60 (2003) 11–25 17
care. Consequently, in the clinical setting a generic diag- target sequence (i.e. the pathogen in question) from verynosis of ‘enterovirus infection’ it is often put forward low numbers, as RNA viral genomes usually are, towithout further specifying the serotype[97]. literally millions of copies without cloning technology.
Another important limit of serological analysis is in the The decision to develop and apply PCR for routinehigh background prevalence of these responses. This likely diagnosis of infective myocarditis must be considered inreflects the ubiquity of many viruses (enterovirus, adeno- relation to the speed, sensitivity and specificity of morevirus, etc.), which circulate seasonally among the general conventional culture and/or serological methods[16,17].population. Moreover immunoglobulin M responses may However it should be stressed that the presence offrequently be detectable for 6 months or longer after acute bacterial or viral nucleotide sequences does not auto-infection (such as for enterovirus)[104], may decline very matically imply a direct role in the pathogenesis ofrapidly resulting in negative values after only a few weeks myocarditis. Indeed an infective agent detected by molecu-(such as parvovirus B19)[105] or can result as a false lar techniques, especially with PCR/nested-PCR, may notnegative in immunodeficient persons or children younger be a cofactor but just an innocent bystander. Therefore it isthan 4 years (such as for EBV)[106]. extremely important to use a molecular technique as a
Direct detection of different antigens in peripheral blood diagnostic tool ancillary to other mandatory investiga-leukocytes by immunocytochemical staining (antigenemia) tions—clinical and morphological—and apply it withis now used efficiently for the diagnosis of different skilled expertise.infective agents, particularly for viruses. Direct detection Enterovirus, particularly coxsackie virus B, was the firstof the lower matrix phosphoprotein (pp65) in peripheral virus investigated in myocarditis / IC based on coxsackieblood leukocytes has now been demonstrated to be a very virus B3 experimental studies that provided inferential datasensitive tool for the diagnosis and monitoring of CMV to implicate enteroviruses as etiologic agents in humaninfection. However the tool is almost laborious and shows myocarditis[20,108,109]. Several reports have investi-quite low sensitivity for detecting the very early or chronic gated the presence of enteroviral genome using PCR,phase of the disease[107]. overcoming the limits of the non-specificity of slot-blot
and the low sensitivity of in situ hybridization and4 .3. Molecular biology technical problems particularly when RNA probes are used
[110,111].4 .3.1. Etiological diagnosis of inflammatory cardio- However enteroviral RNA amplification studies, per-myopathy formed either on EMB specimens or on fragments from
The development of molecular biological techniques, whole heart, have produced controversial data[94,112–particularly amplification methods such as polymerase 125].chain reaction (PCR) or nested-PCR, allows the detection InTable 2the principal studies that investigated only theof low copy of viral genomes even from an extremely presence of enterovirus are reported: the rate of viralsmall amount of tissue such as endomyocardial samples. amplification ranged from 0 to 80% for myocarditis andPCR is an enzymatic amplification technique whereby very from 0 to 57.9% for DC. The wide discrepancy in resultsfew copies of RNA or DNA sequences can be amplified could have different explanations. It may be due to themore than a million-fold. This allows transformation of a different detection procedures adopted by the investigators
T able 2Enteroviral PCR proven myocarditis /dilated cardiomyopathy
Authors, year Material Myocarditis DC
Weiss et al.[112], 1992 EMB – 5/11 (45%)Grasso et al.[113], 1992 NH – 0/21(0%)Katsuragi et al.[114], 1993 NH 0/1 (0%) 3/11 (27%)Schwaiger et al.[115], 1993 EMB – 6/19 (31.6%)Giacca et al.[116], 1994 EMB 1/3 (33%) 4/53 (7%)Khan et al.[117], 1994 EMB – 16/8 (50%)Nicholson et al.[118], 1995 NH 5/6 (83%) –Ueno et al.[119], 1995 EMB 4/5 (80%) 7/42 (17%)Andreoletti et al.[120], 1996 EMB – 11/19 (57.9%)Muir et al. [121], 1996 NH 5/75 (6.6%)Fujioka et al.[122], 1996 EMB 6/31 (19%) 5/28(18%)Archard et al.[123], 1998 EMB – 9/21 (42.9%)Pauschinger et al.[30], 1999 EMB 18/45 (40%) –Calabrese et al.[94], 1999 NH 1/2 (50%) 1/27 (3%)Li et al. [124], 2000 EMB 6/11 (54.5%) 3/8 (37.5%)Crespo-Leiro et al.[125], 2000 NH – 0/68 (0%)
DC, dilated cardiomyopathy; EMB, endomyocardial biopsy; F, female; M, male; NH, native heart.
Dow
nloaded from https://academ
ic.oup.com/cardiovascres/article-abstract/60/1/11/321091 by guest on 03 April 2019

18 F. Calabrese, G. Thiene / Cardiovascular Research 60 (2003) 11–25
as well as to the prevalence of enteroviruses in local Patients were not, however, evaluated for the presence ofpopulations and the stage of the disease. This discrepancy microorganisms, and thus many of the patients treated withemphasizes the need for a standardization of protocols immunosuppressive therapy may have harboured viral(RNA extraction, reverse transcriptase and PCR reaction) material, not detected by routine morphology. It is wellto achieve the same level of sensitivity as the PCR known that, when there is active viral replication, immuno-technique used in different molecular laboratories. More suppression may be harmful. Our retrospective studyrecently other cardiotropic viruses have been investigated confirms the inefficacy of immunosuppressive therapy inusing molecular techniques and it has been shown that patients with per proven viral myocarditis[83]. Immuno-enterovirus is not the sole viral cause of IC. Adenovirus, suppressive therapy has been demonstrated to have benefi-especially in pediatric myocarditis, is another key etiologi- cial effects only when the autoimmune reaction is associ-cal agent that should be investigated when the etiology is ated with IC[85,132].sought: adenovirus were found to be more prevalent than Different molecular strategies have now been developedenterovirus in the case series of Martin et al.[16] and as and applied to improve identification of an infective agentcommon as enterovirus in our recent study[17] performed thus achieving a more complete etiological diagnosis.on children where myocarditis was the most frequent cause Positive PCR results obtained on EMB should be alwaysof heart failure. investigated on a blood sample collected at the time of
EMB may be technically difficult to carry out in biopsy. A type of algorithm might be developed forchildren for a diagnosis of myocarditis, which frequently conclusive molecular diagnosis of myocarditis. The ab-complicates infectious respiratory disorders. sence of a viral genome in the blood sample rules out the
Recently Towbin’s group have demonstrated that trache- possibility of passive blood contamination while viralal aspirates may be a useful substrate for identification of blood positivity requires additional investigation usingcausative agents by PCR analysis in young patients with quantitative PCR analysis. The presence of viral genomicmyocarditis and presumed pneumonitis. In this study all copies, significantly less in the EMB than in blood, doesPCR performed on EMB specimens demonstrated results not necessarily mean that the heart is infected due toidentical to those obtained by tracheal aspirate PCR[126]. viremia, a situation that has recently been reported in a
Even though enterovirus and adenovirus are the princi- case of fatal parvovirus myocarditis[40].pal infective agents detected in myocardial specimens from On more than 600 EMBs (from 1992 to 2001) frompatients with IC, other cardiotropic viruses are now seen as patients with IC investigated by PCR in our molecularimportant pathogens[43,127,128].Thus a specimen from laboratory, concomitant viral detection, both in blood andpatients with clinical suspicion of IC should always be EMB, was observed in only one EBV positive case. Theinvestigated for at least for eight cardiotropic viruses: frequent occurrence of negative PCR blood finding hasenterovirus, adenovirus, CMV, EBV, parvovirus b19, HCV been reported by other authors[16,17]. This is in keepingand influenza virus A and B. An exact etiological diag- with the hypothesis that the viruses are in the blood onlynosis, providing new prognostic information as well as for a brief period followed by rapid clearance from thespecific therapeutic indications, is now extremely impor- bloodstream, whereas false negatives may be due to poortant for appropriate management of patients. handling of blood samples.
Viral infection represents an independent unfavourable Among molecular biological techniques used to dif-prognostic factor in patients[27], particularly in the ferentiate viral genomes[24,116,133,134],gene sequenc-paediatric population, affected by IC either as acute ing is the most informative allowing not only exactmyocarditis or DC[16,17]. In our experience all patients characterization of the infective agent but also elucidationwith viral PCR proven DC underwent heart transplantation of the molecular basis of cardiotropism as well as car-or died within 1 year of diagnosis[17]. diovirulence.
The importance of specific viral treatment in cases with Genomic sites determining the virulence phenotypes areproven molecular diagnosis has been recently stressed by now considered the principal factors responsible for theseveral authors[17,28,82,129]. severity of the disease. Different reports have documented
Apart from the ongoing European Study of Epidemiolo- that the quantity of virus recovered from the myocardiumgy and Treatment of Cardiac Inflammatory Disease did not correlate with the extent of myocardial lesions.(ESETCID) trial [130], the Myocarditis Treatment Trial is This is particularly true for RNA viruses, such as en-the only large multicenter randomized study to have ever teroviruses. Most of the efforts of the experts in the field,been accomplished[131]. Patients in this trial, classified using strains engineered in the laboratory, have beenwith active myocarditis based on the Dallas criteria, principally addressed to the study of the coxsackie virus Breceived immunosuppressive therapy (either azathioprine genome[135,136].A recent work, which used two pheno-and prednisone or cyclosporine and prednisone vs. typically and genotypically distinct clinical CVB3 strainsplacebo) in addition to conventional therapy. The results for constructing six intratypic chimeric viruses, has iden-were inconclusive without any hemodynamic or prognostic tified cardiovirulence determinants in the coxsackie virusbenefit after 6 months of immunosuppressive treatment. B3 59 non-translated region (59NTR) [137].
Dow
nloaded from https://academ
ic.oup.com/cardiovascres/article-abstract/60/1/11/321091 by guest on 03 April 2019

F. Calabrese, G. Thiene / Cardiovascular Research 60 (2003) 11–25 19
Identification of cardiovirulent strains could provide notonly important prognostic indications on the clinicalprogression of the disease but also useful therapeuticsuggestions on responsiveness to specific medical treat-ment. Moreover, in the future the knowledge of genomicsites which determine the cardiovirulence could lead to thedevelopment of vaccines for patients with a major risk oflethal complications[138].
It is now equally important to have more preciseetiological characterization in order to exactly define theinfective status of viruses. The detection of viral replica-tion has been demonstrated to be quite useful not only forthose DNA viruses known to be in the latent form, but alsofor RNA viruses. Different authors have shown that thedetection of CMV mRNA transcripts (early and late gene)may be considered diagnostic markers of the disease withexpression of early gene preceding the antigenemia de-tection in most cases[139]. Both qualitative and quantita-tive determination of human CMV immediate-early andlate (pp67) transcripts are now used for monitoring ofCMV infections in the post transplantation period[140].
During viral replication of the enterovirus genome, asingle-strand monocistronic RNA of positive polarity(plus-strand) acts as a template for the transcription of areplicate minus-strand RNA intermediate through the
polRNA-dependent RNA polymerase (3D ). This minus-polstrand RNA is then used as a template again for the 3D
to generate multiple copies of viral plus-strand genomesthat are translated into enteroviral structural proteins andultimately packaged into new virions. The identification ofminus-strand enteroviral RNA is an indicator of activeviral replication in enteroviral positive cases (positivestrands). Some authors have emphasised the importance ofdistinguishing between active viral replication and thelatent persistence of enteroviral genomes not only forprognosis with different clinical course but also for a more
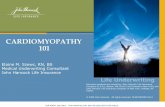
Fig. 3. AV myocarditis in a female child (2 years old). (a) Histology ofappropriate treatment regime[17,28,141]. A high fre-EMB showing focus of lymphocytes associated with myocyte necrosis,
quency of active enteroviral RNA replication was detected hematoxylin and eosin3100; (b) PCR analysis for AV: lane 1: DNAnot only in patients with myocarditis or clinically sus- marker; lane 2: beta-globin (house-keeping gene); lane 3: AV positivepected myocarditis but also in patients with end stage control; lane 4: EMB AV PCR positive; lane 5: negative control (reagents
without template); (c) histology of EMB, 6 months after therapy withDCM [17,28], where the active viral replication wasspecific immunoglobulin; note the complete absence of inflammatory cellassociated with a poor prognosis.infiltration, hematoxylin and eosin360; (d) PCR analysis for adenovirus:
Similar data are reported in HCV myocarditis where lane 1: DNA marker; lane 2: beta-globin (house-keeping gene); lane 3:both positive and negative strands of HCV RNA were AV positive control; lane 4 EMB (after therapy) AV PCR negative; lane 4:detected in cardiac tissue from patients with acute and uninfected cell line; lane 5: negative control (reagents without template).
chronic forms[43,44].
4 .3.2. Monitoring of inflammatory cardiomyopathy three out of eight viral myocarditis cases followed by EMBPCR analysis (including detection of viral replicative merged into DC with PCR evidence of persistent viral
status and viral load) should be applied on follow-up genome and two of them died[17]. In these cases thebiopsies of patients with viral myocarditis and may progression into DC provides further evidence of the linkrepresent the best way to verify the efficacy of specific between viral myocarditis and DC.antiviral therapy (Fig. 3a–d) [142]. The diagnosis of viral myocarditis, which ‘per se’ is
Furthermore viral persistence has been also detected by difficult particularly when based only on morphologicalseveral studies that investigated the viral genome on features, becomes quite challenging in the monitoring ofsubsequent biopsies[17,112,143]. In our recent study, post-transplant endomyocardial biopsies where inflamma-
Dow
nloaded from https://academ
ic.oup.com/cardiovascres/article-abstract/60/1/11/321091 by guest on 03 April 2019

20 F. Calabrese, G. Thiene / Cardiovascular Research 60 (2003) 11–25
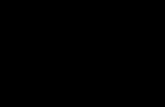
tory infiltrates within the myocardium, as a result of viralinfection, are difficult to differentiate histologically fromthose of acute cellular rejection (Fig. 4a–c).
CMV is generally regarded as the most importantinfectious agent affecting organ transplant recipients, andlatently infected allografts constitute a major source of thevirus. The disease may result from either primary infectionor reactivation of the virus in the immunosuppressedpatient. More recently Towbin’s group in a large series ofcases (553 consecutive biopsy samples from 149 transplantrecipients) has demonstrated that different types of cardiot-ropic viruses are frequently implicated[144]. In thisinvestigation the authors stressed the crucial role of theviruses to adversely influence graft survival especiallyfavouring chronic vascular rejection. Previous studies haveshown an association between CMV infection and vascularrejection and coronary artery disease[145,146].Differenthypotheses have been postulated for the pathogenesis ofallograft substrates of vasculopathy. It has been speculatedFig. 3. (continued)that viruses may transform infected cells and thereby alter
Fig. 4. Post-transplant cytomegaloviral (CMV) myocarditis: (a) histology of EMB showing interstitial edema and polymorphous inflammatory cellinfiltration. No cytomegaly and/or viral inclusion bodies are seen; hematoxylin and eosin350; (b) histology of EMB (3 months after therapy withganciclovir; note the absence of inflammatory cell infiltration), hematoxylin and eosin350; (c) RT-PCR analysis for CMV: lane 1: DNA marker; lane 2:CMV positive control; lane 3: EMB (a: before treatment): CMV positive; lane 4: negative control (reagents without template); lane 5: skipped slot; lane 6:DNA marker; lane 7: CMV positive control; lane 8: EMB (b: after ganciclovir therapy): CMV PCR negative; lane 9: negative control (reagents withouttemplate).
Dow
nloaded from https://academ
ic.oup.com/cardiovascres/article-abstract/60/1/11/321091 by guest on 03 April 2019

F. Calabrese, G. Thiene / Cardiovascular Research 60 (2003) 11–25 21
T able 3aViral PCR1 myocarditis /dilated cardiomyopathy: recurrence of viral infection
Sex/age Clinical presentation Histology Viral PCR Viral recurrence
M/15 CHF AM EV 1
M/17 Dyspnea DC EV –M/16 Dyspnea DC EV –F/13 Fatigue DC AV/EV –F/1 CHF DC EV –M/6 Acute CHF AM HSV 1
M/1.5 Fatigue DC EV –F/18 CHF DC EV
AM, active myocarditis; AV, adenovirus; CHF, congestive heart failure; DC, dilated cardiomyopathy; EBV, Epstein–Barr virus; EV, enterovirus; HSV,herpes simplex virus.
a From Calabrese et al.[17].
release of growth factors leading to cellular proliferation in minute quantities; (ii) detection of agents that are[147]. In addition, viruses may act directly to cause difficult to cultivate or which cannot be cultivated; (iii)vascular endothelial damage within the heart, leading to detection of latent and active infections; (iv) strain typing;increased expression of cell adhesion molecules and other and (v) detection of virulence and antimicrobial resistanceinflammatory mediators that then promote leukocyte re- determinants.cruitment to the site. Viral particles, attached to the blood Correct application of molecular techniques will allowvessel wall, may also serve to activate the immune system, increasingly more information to be obtained: new epi-with resultant damage to the vascular endothelial surface, demiology, current patient risk stratification and overalland viral particles may serve to alter alloantigenicity more appropriate medical treatment.resulting in rejection[148]. The high cost of biopsy processing including molecular
De novo viral infection is not surprising in heart investigation with an apparently unfavourable cost:benefittransplant recipients, given the immunocompromised ratio, is counterbalanced by the current high morbidity andstatus, however the possibility of recurrence of viral mortality (56% of patients die within 4.3 years of diag-myocarditis, favoured also by the immunosuppression nosis) calling for precise etiological diagnosis with inher-regimen, should be considered as well (Table 3) [17]. ent therapeutic implications.
The demonstration of viral disease recurrence in all William Osler, acutely ahead of his time, stated: ‘‘Therecardiac grafts after cardiac transplantation stresses the are three phases to treatment: diagnosis, diagnosis andimportance of etiologic characterization of myocarditis at diagnosis’’, stressing that the best patient managementthe time of transplantation. Strict surveillance of these resides fundamentally in the most accurate diagnosispatients using molecular techniques after transplantation is provided by expertise and experience[149].mandatory for early detection of the recurrent myocarditisand consequently administration of more specific treat-ment, including antiviral therapy. R eferences
[1] R ichardson P, McKenna WJ, Bristow M et al. Report of the 19955 . Conclusion WHO/ISFC task force on the definition of cardiomyopathies.
Circulation 1996;93:841–842.[2] A ngelini A, Calzolari V, Calabrese F et al. Myocarditis mimickingIC, either as acute myocarditis or chronic myocarditis /
acute myocardial infarction: role of endomyocardial biopsy in theDC, is frequently triggered and often maintained by viraldifferential diagnosis. Heart 2000;84:245–250.
infection. To date morphological studies, including im- [3] B asso C, Calabrese F, Corrado D, Thiene G. Postmortem diagnosismunohistochemistry for inflammatory cell characterization, in sudden cardiac victims: macroscopic, microscopic and molecular
findings. Cardiovasc Res 2001;50:290–300.associated with molecular analysis for viral detection,[4] A retz HT. Myocarditis: the Dallas criteria. Hum Patholmake EMB the gold standard for final diagnosis of the
1987;18:619–624.disease.[5] E dwards WD. Myocarditis and endomyocardial biopsy. Cardiol Clin
Various molecular techniques such as PCR, gene se- 1984;2:647–656.quencing and real time PCR, often applied on the same [6] E dwards WD, Holmes DR, Reeders GS. Diagnosis of activeendomyocardial specimen, have become an essential part lymphocytic myocarditis by endomyocardial biopsy: quantitative
criteria for light microscopy. Mayo Clin Proc 1982;57:419–425.of the diagnostic armamentarium for rapid, specific and[7] C how LH, Radio SJ, Sears TD, McManus BM. Insensitivity of rightsensitive identification of infective agents. The advantages
ventricular endomyocardial biopsy in the diagnosis of myocarditis. Jof PCR analysis for definitive diagnosis of viral inflamma- Am Coll Cardiol 1989;14:915–920.tory cardiomyopathy can be summarized as follows: (i) [8] H auck AJ, Kearney DL, Edwards WD. Evaluation of postmortemrapid detection of specific microbial nucleic acid sequences endomyocardial biopsy specimens from 38 patients with
Dow
nloaded from https://academ
ic.oup.com/cardiovascres/article-abstract/60/1/11/321091 by guest on 03 April 2019

22 F. Calabrese, G. Thiene / Cardiovascular Research 60 (2003) 11–25
lymphocytic myocarditis: implications for role of sampling error. adenoviral genome in the myocardium of adult patients withMayo Clin Proc 1989;64:1235–1245. idiopathic left ventricular dysfunction. Circulation 1999;99:1348–
1354.[9] T hiene G, Bartoloni G, Poletti A, Boffa GM. Tecniche, indicazioni`ed utilita della biopsia endomiocardica. In: Baroldi G, Thiene G, [31] S pencer MJ, Cherry JD, Adams FH, Byatt PH. Supraventricular
editors, Biopsia endomiocardica. Testo atlante, Padova: Piccin; tachycardia in an infant associated with a rhinoviral infection1996, pp. 5–45. (letter). J Pediatr 1975;86:811–812.
[10] B urke AP, Farb A, Robinowitz M, Virmani R. Serial sectioning and [32] W reghitt T, Cary N. Virus infections in heart transplant recipientsmultiple level examination of endomyocardial biopsies for the and evidence for involvement of the heart. In: Banatvala JE, editor,diagnosis of myocarditis. Mod Pathol 1991;4:690–693. Viral infections of the heart, London: Hodder and Stoughton; 1993,
pp. 240–250.[11] F rustaci A, Bellocci F, Osen EG. Results of biventricular endo-myocardial biopsy in survivors of cardiac arrest with apparently [33] M aisch B, Schonian U, Crombach M et al. Cytomegalovirusnormal hearts. Am J Cardiol 1994;74:890–895. associated inflammatory heart muscle disease. Scand J Infect Dis
1993;88(Suppl.):135–148.[12] H erskowitz A, Ahmed-Ansari A, Neumann DA et al. Induction ofmajor histocompatibility complex antigens within the myocardium [34] B andrup U, Morlensen SA. Histopathological aspects of myocarditisof patients with active myocarditis: a non-histologic marker of with special reference to mumps, cytomegalovirus infection and themyocarditis. J Am Coll Cardiol 1990;15:624–632. role of endomyocardial biopsy. In: Bolte HD, editor, Viral heart
disease, Berlin: Springer; 1984, pp. 13–25.[13] K uhl U, Seeberg B, Schultheiss HP, Strauer BE. Immunohistologicalcharacterization of infiltrating lymphocytes in biopsies of patients [35] P artanen J, Nieminen MS, Krogerus L et al. Cytomegaloviruswith clinically suspected dilated cardiomyopathy. Eur Heart J myocarditis in transplanted heart verified by endomyocardial biopsy.1994;15(Suppl. C):62–67. Clin Cardiol 1991;14:847–849.
[14] K uhl U, Noutsias M, Schultheiss HP. Immunohistochemistry in [36] S tewart S, Cary NRB, Goddard MJ, Billingham M. Infection. In:dilated cardiomyopathy. Eur Heart J 1995;16(Suppl. O):100–106. Stewart S, Cary NRB, Goddard MJ, Billingham M, editors, Atlas of
biopsy pathology for heart and lung transplantation, Arnold; 2000,[15] A ngelini A, Crosato M, Boffa GM et al. Active versus borderlinepp. 37–41.myocarditis: clinicopathological correlates and prognostic implica-
tions. Heart 2002;87:210–215. [37] N i J, Bowles NE, Kim YH et al. Viral infection of the myocardiumin endocardial fibroelastosis. Molecular evidence for the role of[16] M artin AB, Webber S, Fricker FJ et al. Acute myocarditis. Rapidmumps virus as an etiologic agent. Circulation 1997;95:133–139.diagnosis by PCR in children. Circulation 1994;90:330–339.
[38] P orter HJ, Quantrill AM, Fleming KA. B19 parvovirus infection of[17] C alabrese F, Rigo E, Milanesi O et al. Molecular diagnosis ofmyocardial cells. Lancet 1988;1:535–536.myocarditis and dilated cardiomyopathy in children:
clinicopathologic features and prognostic implications. Diagn Mol [39] S chowengerdt KO, Ni J, Denfield SW et al. Association of par-Pathol 2002;11:212–221. vovirus B19 genome in children with myocarditis and cardiac
allograft rejection: diagnosis using the polymerase chain reaction.[18] L iu PP, Mason JW. Advances in the understanding of myocarditis.Circulation 1997;96:3549–3554.Circulation 2001;104:1076–1082.
[40] M urry CE, Jerome KR, Reichenbach DD. Fatal parvovirus myocar-[19] G erzen P, Granath A, Holmgren B, Zetterquist S. Acute myocarditis.ditis in a 5-year-old girl. Hum Pathol 2001;32:342–345.A follow-up study. Br Heart J 1972;34:575–583.
[41] H all CJ. Parvovirus B19 infection in pregnancy. Arch Dis Child[20] W oodruff JF. Viral myocarditis: a review. Am J PatholFetal Neonatal Ed 1994;71:F4–5.1980;101:425–484.
[42] Y oung NS. Parvovirus. In: Fields BN, Knipe DM, Howley PM,[21] G rist NR, Reid D. Epidemiology of viral infections of the heart. In:editors, Virology, Philadelphia: Lippincot-Raven; 1996, pp. 2199–Banatvala JE, editor, Viral infections of the heart, London: Hodder2220.and Stoughton; 1993, pp. 23–31.
[43] M atsumori A, Matoba Y, Sasayama S. Dilated cardiomyopathy[22] K asper EK, Agema WR, Hutchins GM, Deckers JW, Hare JM,associated with hepatitis C virus infection. CirculationBaughman KL. The causes of dilated cardiomyopathy: a1995;92:2519–2525.clinicopathologic review of 673 consecutive patients. J Am Coll
Cardiol 1994;23:586–590. [44] O kabe M, Fukuda K, Arakawa K, Kikuchi M. Chronic variant ofmyocarditis associated with hepatitis C virus infection. Circulation[23] C ambridge G, MacArthur CG, Waterson AP, Goodwin JF, Oakley1997;96:22–24.CM. Antibodies to Coxsackie B viruses in congestive car-
diomyopathy. Br Heart J 1979;41:692–696. [45] F rustaci A, Calabrese F, Chimenti C, Pieroni M, Thiene G, MaseriA. Lone hepatitis C virus myocarditis responsive to immunosuppres-[24] M uir P, Nicholson F, Tilzey AJ, Signy M, English TA, Banatvalasive therapy. Chest 2002;122:1348–1356.JE. Chronic relapsing pericarditis and dilated cardiomyopathy:
serological evidence of persistent enterovirus infection. Lancet [46] T akeda A, Sakata A, Takeda N. Detection of hepatitis C virus RNA1989;1:804–807. in the hearts of patients with hepatogenic cardiomyopathy. Mol Cell
Biochem 1999;195:257–261.[25] K eeling PJ, Lukaszyk A, Poloniecki J et al. A prospective case-control study of antibodies to coxsackie B virus in idiopathic dilated [47] H avaldar PV. Diphtheria in the eighties: experience in a south Indiancardiomyopathy. J Am Coll Cardiol 1994;23:593–598. district hospital. J Indian Med Assoc 1992;90:155–156.
[26] K arjalainen J, Nieminen MS, Heikkila J. Influenza A1 myocarditis [48] B jorkholm B, Olling S, Larsson P, Hagberg L. An outbreak ofin conscripts. Acta Med Scand 1980;207:27–30. diphtheria among Swedish alcoholics. Infection 1987;15:354–358.
[27] W hy HJ, Meany BT, Richardson PJ et al. Clinical and prognostic [49] P utterman C, Caraco Y, Shalit M. Acute non-rheumatic perimyocar-significance of detection of enteroviral RNA in the myocardium of ditis complicating streptococcal tonsillitis. Cardiology 1991;78:156–patients with myocarditis or dilated cardiomyopathy. Circulation 160.1994;89:2582–2589. [50] L i Y, Pan Z, Ji Y, Peng T, Archard LC, Zhang H. Enterovirus
[28] F ujioka S, Kitaura Y, Ukimura A et al. Evaluation of viral infection replication in valvular tissue from patients with chronic rheumaticin the myocardium of patients with idiopathic dilated car- heart disease. Eur Heart J 2002;23:567–573.diomyopathy. J Am Coll Cardiol 2000;36:1920–1926. [51] H ardman JM, Earle KM. Myocarditis in 200 fatal meningococcal
[29] H eber MM, Yu C, Towbin JA, Rogers BB. Fatal Epstein–Barr virus infections. Arch Pathol 1969;87:318–325.myocarditis in a child with repetitive myocarditis. Pediatr Pathol [52] Z ollner B, Sobottka I, von der Lippe G et al. Perimyocarditis causedLab Med 1995;15:805–812. by Yersinia enterocolitica serotype 0:3. Dtsch Med Wochenschr
[30] P auschinger M, Bowles NE, Fuentes-Garcia FJ et al. Detection of 1992;117:1794–1797.
Dow
nloaded from https://academ
ic.oup.com/cardiovascres/article-abstract/60/1/11/321091 by guest on 03 April 2019

F. Calabrese, G. Thiene / Cardiovascular Research 60 (2003) 11–25 23
[53] v an der Linde MR, Crijns HJ, de Koning J et al. Range of [74] M aisel A, Cesario D, Baird S, Rehman J, Haghighi P, Carter S.atrioventricular conduction disturbances in Lyme borreliosis: a Experimental autoimmune myocarditis produced by adoptive trans-report of four cases and review of other published reports. Br Heart fer of splenocytes after myocardial infarction. Circ ResJ 1990;63:162–168. 1998;82:458–463.
[54] K arjalainen J. A loud third heart sound and asymptomatic myocar- [75] N akamura H, Yamamura T, Umemoto S et al. Autoimmune responseditis during Mycoplasma pneumoniae infection. Eur Heart J in chronic ongoing myocarditis demonstrated by heterotopic cardiac1990;11:960–963. transplantation in mice. Circulation 1996;94:3348–5334.
[55] O deh M, Oliven A. Chlamydial infections of the heart. Eur J Clin [76] P rabhakar BS, Srinivasappa J, Beisel KW, Notkins AL. Virus-Microbiol Infect Dis 1992;11:885–893. induced autoimmunity: cross-reactivity of antiviral antibodies with
[56] P age SR, Stewart JT, Bernstein JJ. A progressive pericardial self-components. In: Schultheiss H-P, editor, New concepts in viraleffusion caused by psittacosis. Br Heart J 1988;60:87–89. heart disease, Berlin: Springer; 1988, pp. 168–178.
[57] F ryden A, Kihlstrom E, Maller R, Persson K, Romanus V, Ansehn S. [77] D avies JM. Molecular mimicry: can epitope mimicry induce au-A clinical and epidemiological study of ‘ornithosis’ caused by toimmune disease? Immunol Cell Biol 1997;75:113–126.Chlamydia psittaci and Chlamydia pneumoniae (strain TWAR). [78] F airweather D, Lawson CM, Chapman AJ et al. Wild isolates ofScand J Infect Dis 1989;21:681–691. murine cytomegalovirus induce myocarditis and antibodies that
[58] W esslen L, Pahlson C, Friman G, Fohlman J, Lindquist O, Johan- cross-react with virus and cardiac myosin. Immunologysson C. Myocarditis caused byChlamydia pneumoniae (TWAR) and
1998;94:263–270.sudden unexpected death in a Swedish elite orienteer. Lancet
[79] W eller AH, Simpson K, Herzum M, Van Houten N, Huber SA.1992;340:427–428.
Coxsackievirus-B3-induced myocarditis: virus receptor antibodies[59] F ournier PE, Etienne J, Harle JR, Habib G, Raoult D. Myocarditis, a
modulate myocarditis. J Immunol 1989;143:1843–1850.rare but severe manifestation of Q fever: report of eight cases and[80] R ose NR, Hill SL. The pathogenesis of postinfectious myocarditis.review of the literature. Clin Infect Dis 2001;32:1440–1447.
Clin Immunol Immunopathol 1996;80:S92–99.[60] P arada H, Carrasco HA, Anez N, Fuenmayor C, Inglessis I. Cardiac[81] C aforio AL. Role of autoimmunity in dilated cardiomyopathy. Brinvolvement is a constant finding in acute Chagas’ disease: a
Heart J 1994;72:S30–34.clinical, parasitological and histopathological study. Int J Cardiol[82] C aforio AL, Mahon NJ, Tona F, McKenna WJ. Circulating cardiac1997;60:49–54.
autoantibodies in dilated cardiomyopathy and myocarditis: patho-[61] T sala Mbala P, Blackett K, Mbonifor CL, Leke R, Etoundi J.genetic and clinical significance. Eur J Heart Fail 2002;4:411–417.Functional and immunologic involvement in human African
[83] F rustaci A, Chimenti C, Calabrese F et al. A. Immunosuppressivetrypanosomiasis caused byTrypanosoma gambiense. Bull Soctherapy for active lymphocytic myocarditis: virologic and immuno-Pathol Exot Filiales 1988;81:490–501.logic profile of responders versus non-responders. Circulation[62] W reghitt TG, Hakim M, Gray JJ et al. Toxoplasmosis in heart and2003;107:857–863.heart and lung transplant recipients. J Clin Pathol 1989;42:194–199.
[84] K lingel K, Hohenadl C, Canu A et al. Ongoing enterovirus-induced[63] W reghitt T, Cary N. Virus infections in heart transplant recipientsmyocarditis is associated with persistent heart muscle infection:and evidence for involvement of the heart. In: Banatvala JE, editor,quantitative analysis of virus replication, tissue damage, and inflam-Viral infections of the heart, London: Hodder and Stoughton; 1993,mation. Proc Natl Acad Sci USA 1992;89:314–318.pp. 240–250.
[85] K oide H, Kitaura Y, Deguchi H, Ukimura A, Kawamura K, Hirai K.[64] A nderson DW, Virmani R, Reilly JM et al. Prevalent myocarditis atViral genomic detection in the hearts of C3H/He mice withnecropsy in the acquired immunodeficiency syndrome. J Am Collexperimental Coxsackievirus B3 myocarditis by gene amplificationCardiol 1988;11:792–799.using the polymerase chain reaction. Jpn Circ J 1992;56:148–156.[65] H ofman P, Drici MD, Gibelin P, Michiels JF, Thyss A. Prevalence
[86] K yu B, Matsumori A, Sato Y, Okada I, Chapman NM, Tracy S.of toxoplasma myocarditis in patients with the acquired immuno-Cardiac persistence of cardioviral RNA detected by polymerasedeficiency syndrome. Br Heart J 1993;70:376–381.chain reaction in a murine model of dilated cardiomyopathy.[66] N osanchuk JD. Fungal myocarditis. Front Biosci 2002;7:1423–Circulation 1992;86:522–530.1438.
[87] G luck B, Schmidtke M, Merkle I, Stelzner A, Gemsa D. Persistent[67] C alabrese F, Angelini A, Cecchetto A,Valente M, Livi U, Thiene G.expression of cytokines in the chronic stage of CVB3-inducedHIV infection in the first heart transplantation in Italy: fatalmyocarditis in NMRI mice. J Mol Cell Cardiol 2001;33:1615–1626.outcome. Case report. APMIS 1998;106:470–474.
[88] M uir P, Archard LC. There is evidence for persistent enterovirus[68] W itebsky E, Rose NR, Terplan K, Paine JR, Egan RW. Chronicinfection in chronic medical conditions in human. Med Virolthyroiditis and autoimmunization. J Am Med Assoc 1957;164:1439–1994;4:245–250.1447.
[89] T am PE, Messner RP. Molecular mechanisms of coxsackievirus[69] W oodruff JF, Woodroff JJ. Involvement of T lymphocytes in thepersistence in chronic inflammatory myopathy: viral RNA persistspathogenesis of coxsackie virus B3 heart disease. J Immunolthrough formation of a double-stranded complex without associated1974;113:1723–1726.genomic mutations or evolution. J Virol 1999;73:10113–10121.[70] P ummerer CL, Grassl G, Sailer M, Bachmaier KV, Penninger JM,
[90] B adorff C, Lee GH, Lamphear BJ et al. Enteroviral protease 2ANeu N. Cardiac myosin-induced myocarditis: target recognition bycleaves dystrophin: evidence of cytoskeletal disruption in an ac-autoreactive T cells requires prior activation of cardiac interstitialquired cardiomyopathy. Nat Med 1999;5:320–326.cells. Lab Invest 1996;74:845852.
[91] F enton M, Sinclair AJ. Divergent requirements for the MAPK/ERK[71] N eu N, Rose NR, Beisel KW, Herskowitz A, Gurri-Glass G, Craigsignal transduction pathway during initial virus infection of quies-SW. Cardiac myosin induces myocarditis in genetically predisposedcent primary B cell and disruption of Epstein–Barr virus latency bymice. J Immunol 1987;139:3630–3636.phorbol esters. J Virol 1999;73:8913–8916.[72] K asahara H, Itoh M, Sugiyama T et al. Autoimmune myocarditis
induced in mice by cardiac C-protein. Cloning of complementary [92] O pavsky M, Martino T, Rabinovitch M et al. Enhanced ERK1/2DNA encoding murine cardiac C-protein and partial characterization activation in mice susceptible to coxsackievirus-induced myocar-of the antigenic peptides. J Clin Invest 1994;94:1026–1036. ditis. J Clin Invest 2002;109:1561–1569.
[73] H uber SA, Cunningham MW. Streptococcal M protein peptide with [93] B owles NE, Rose ML, Taylor P et al. End-stage dilated car-similarity to myosin induces CD41 T cell-dependent myocarditis in diomyopathy. Persistence of enterovirus RNA in myocardium atMRL/11 mice and induces partial tolerance against coxsakieviral cardiac transplantation and lack of immune response. Circulationmyocarditis. J Immunol 1996;156:3528–3534. 1989;80:1128–1136.
Dow
nloaded from https://academ
ic.oup.com/cardiovascres/article-abstract/60/1/11/321091 by guest on 03 April 2019

24 F. Calabrese, G. Thiene / Cardiovascular Research 60 (2003) 11–25
[94] C alabrese F,Valente M, Thiene G et al. Enteroviral genome in native genome and its significance in cardiomyopathy. Cardiology1993;83:4–13.hearts may influence outcome of patients who undergo cardiac
[115] S chwaiger A, Umlauft F, Weyrer K et al. Detection of enteroviraltransplantation. Diagn Mol Pathol 1999;8:39–46.ribonucleic acid in myocardial biopsies from patients with[95] K andolf R, Klingel K, Zell R et al. Molecular mechanisms in theidiopathic dilated cardiomyopathy by polymerase chain reaction.pathogenesis of enteroviral heart disease: acute and persistentAm Heart J 1993;126:406–410.infections. Clin Immunol Immunopathol 1993;68:153–158.
[116] G iacca M, Severini GM, Mestroni L et al. Low frequency of[96] G randien M, Forsgren M, Ehrnst A. Enteroviruses. In: Lennette EH,detection by nested polymerase chain reaction of enterovirusLennette A, Lennette ET, editors, Diagnostic procedures for viral,ribonucleic acid in endomyocardial tissue of patients withrickettsial, and chlamydial infections, 7th ed, Washington, DC:idiopathic dilated cardiomyopathy. J Am Coll CardiolAmerican Public Health Association; 1995, pp. 279–297.1994;24:1033–1040.[97] R otbart HA, Romero JR. Laboratory diagnosis of enteroviral
[117] K han M, Why H, Richardson P, Archard L. Nucleotide sequencinginfections. In: Rotbart HA, editor, Human enterovirus infections,of PCR products shows the presence of Coxsackie-B3 virus inWashington, DC: American Society for Microbiology; 1995, pp.endomyocardial biopsies from patients with myocarditis or dilated401–418.cardiomyopathy. Biochem Soc Trans 1994;22:176S.[98] B rown M, Petric M. Evaluation of cell line 293 for virus isolation in
[118] N icholson F, Ajetunmobi JF, Li M et al. Molecular detection androutine viral diagnosis. J Clin Microbiol 1986;23:704–708.serotypic analysis of enterovirus RNA in archival specimens from
[99] K ogon A, Spigland I, Frothingham TE et al. The virus watchpatients with acute myocarditis. Br Heart J 1995;74:522–527.
program: a continuing surveillance of viral infections in met-[119] U eno H, Yokota Y, Shiotani H et al. Significance of detection of
ropolitan New York families. VII. Observations on viral excretion,enterovirus RNA in myocardial tissue by reverse transcription-
seroimmunity, intrafamilial spread and illness association in coxsac-polymerase chain reaction. Int J Cardiol 1995;51:157–164.
kie and echovirus infections. Am J Epidemiol 1969;89:51–61. [120] A ndreoletti L, Hober D, Decoene C et al. Detection of enteroviral[100] S utton GC, Harding H, Trueheart RRRP, Clark HP. Coxsackie B4 RNA by polymerase chain reaction in endomyocardial tissue of
myocarditis in an adult: successful isolation of virus from ventricu- patients with chronic disease. J Med Virol 1996;48:53–59.lar myocardium. Clin Aviation Aerospace Med 1967;38:66–69. [121] M uir P, Nicholson F, Illavia SJ et al. Serological and molecular
[101] M aller HM, Powars DF, Horowitz RE, Portnoy B. Fatal myocar- evidence of enterovirus infection in patients with end-stage dilatedditis associated with ECHO virus, type 22, infection in a child with cardiomyopathy. Heart 1996;76:243–249.apparent immunological deficiency. J Pediatr 1967;71:204–210. [122] F ujioka S, Koide H, Kitaura Y, Deguchi H, Kawamura K, Hirai K.
[102] L ongson M, Cole FM, Davies D. Isolation of a Coxsackie virus Molecular detection and differentiation of enteroviruses in endo-group B, type 5, from the heart of a fatal case of myocarditis in an myocardial biopsies and pericardial effusions from dilated car-adult. J Clin Pathol 1969;22:654–658. diomyopathy and myocarditis. Am Heart J 1996;131:760–765.
[103] L erner A, Wilson FM, Reyes MP. Enteroviruses and the heart (with [123] A rchard LC, Khan MA, Soteriou BA et al. Characterization ofspecial emphasis on the probable role of coxsackieviruses, group Coxsackie B virus RNA in myocardium from patients with dilatedB, types 1–5). II. Observations in humans. Mod Concepts Cardiov- cardiomyopathy by nucleotide sequencing of reverse transcription-asc Dis 1975;44:11–15. nested polymerase chain reaction products. Human Pathol
[104] M uir P, Nicholson F, Banatvala JE, Bingley PJ. Coxsackie B virus 1998;29:578–584.and postviral fatigue syndrome. Br Med J 1991;302:658–659. [124] L i Y, Bourlet T, Andreoletti L et al. Enteroviral capsid protein VP1
[105] M odrow S, Dorsh S. Antibody responses in parvovirus B19 is present in myocardial tissue from some patients with myocarditisinfected patients. Pathol Biol 2002;50:326–331. or dilated cardiomyopathy. Circulation 2000;101:231–234.
[106] H enle W, Henle G, Andersson J et al. Antibody responses to [125] C respo-Leiro MG, Hermida-Prieto M, Pena F et al. Absence ofEpstein–Barr virus-determined nuclear antigen (EBNA)-1 and enteroviral RNA in hearts explanted from patients with dilatedEBNA-2 in acute and chronic Epstein–Barr virus infection. Proc cardiomyopathy. J Heart Lung Transplant 2000;19:134–138.Natl Acad Sci USA 1987;84:570–574. [126] A khtar N, Ni J, Stromberg D, Rosenthal GL, Bowles NE, Towbin
[107] G rangeot-Keros L, Cointe D. Diagnosis and prognosis marker of JA. Tracheal aspirate as a substrate for polymerase chain reactionHCMV infection. J Clin Virol 2001;21:213–221. detection of viral genome in childhood pneumonia and myocar-
[108] G auntt C, Godeney E, Lutton CW et al. Mechanism(s) of coxsac- ditis. Circulation 1999;99:2011–2018.kievirus-induced myocarditis in the mouse. In: de la Maza L, [127] S chonian U, Crombach M, Maser S, Maisch B. Cytomegalovirus-Pterson E, editors, Medical virology, 8th ed, Hillsdale, NJ: associated heart muscle disease. Eur Heart J 1995;S16:46–49.Lawrence Erlbaum; 1988, pp. 161–182. [128] K lingel K, Selinka HC, Sauter M, Bock CT, Szalay G, Kandorlf R.
[109] R otbart H. Human enterovirus infections: molecular approaches to Molecular mechanisms in enterovirus and parvovirus B19 associ-diagnosis and pathogenesis. In: Semler B, Ehrenfeld E, editors, ated myocarditis and inflammatory cardiomyopathy. Eur Heart JMolecular aspects of picornavirus infection and detection, Suppl I 2002;4:8–12.Washington, DC: American Society for Microbiology; 1989, pp. [129] F eldman AM, McNamara D. Myocarditis. N Engl J Med243–264. 2000;343:1388–1398.
[110] C ronin ME, Love LA, Miller FW, McClintock PR, Plotz PH. The [130] M aish B, Hufnagel G, Schonian U, Hengstenberg C for thenatural history of encephalomyocarditis virus-induced myositis and ESETCID investigators. The European Study of Epidemiology andmyocarditis in mice. Viral persistence demonstrated by in situ Treatment of Cardiac Inflammatory Disease (ESETCID). Eur Hearthybridization. J Exp Med 1988;168:1639–1648. J 1995;S16:172–175.
[111] E aston AJ, Eglin RP. The detection of coxsackievirus RNA in [131] M ason JW, O’Connell JB, Herskowitz A. A clinical trial ofcardiac tissue by in situ hybridization. J Gen Virol 1988;69:285– immunosuppressive and immunomodulatory treatment for myocar-291. ditis. N Engl J Med 1995;333:269–275.
[112] W eiss L, Liu XF, Hang KL, Billingham ME. Detection of [132] W ojnicz R, Nowalany-Kozielska E, Wojciechowska C et al.enteroviral RNA in idiopathic dilated cardiomyopathy and other Randomized, placebo-controlled study for immunosuppressivehuman cardiac tissues. J Clin Invest 1992;90:156–159. treatment of inflammatory dilated cardiomyopathy: 2-year follow-
[113] G rasso M, Arbustini E, Silini E et al. Search for Coxsackievirus B3 up results. Circulation 2001;104:39–45.RNA in idiopathic dilated cardiomyopathy using gene amplifica- [133] K ammerer U, Kunkel B, Korn K. Nested PCR for specifiction by polymerase chain reaction. Am J Cardiol 1992;69:658–664. detection and rapid identification of human picornaviruses. J Clin
[114] K atsuragi M, Yutani C, Mukai T et al. Detection of enteroviral Microbiol 1994;32:285–291.
Dow
nloaded from https://academ
ic.oup.com/cardiovascres/article-abstract/60/1/11/321091 by guest on 03 April 2019

F. Calabrese, G. Thiene / Cardiovascular Research 60 (2003) 11–25 25
[134] C hapman NM, Tracy S, Gauntt CJ, Fortmueller U. Molecular replication in the myocardium of patients with left ventriculardetection and identification of enteroviruses using enzymatic dysfunction and clinically suspected myocarditis. Circulationamplification and nucleic acid hybridization. J Clin Microbiol 1999;99:889–895.1990;28:843–850. [142] W alls T, Shankar AG, Shingadia D. Adenovirus: an increasingly
[135] C hapman NM, Tu Z, Tracy S, Gauntt CJ. An infectious cDNA important pathogen in paediatric bone marrow transplant patients.copy of the genome of a non-cardiovirulent coxsackievirus B3 Lancet Infect Dis 2003;3:79–86.strain: its complete sequence analysis and comparison to the [143] J in O, Sole M, Butany J. Detection of enterovirus RNA ingenomes of cardiovirulent coxsackieviruses. Arch Virol myocardial biopsies from patients with myocarditis and car-1994;135:115–130. diomyopathy using gene amplification by polymerase chain re-
[136] C ameron-Wilson CL, Pandolfino YA, Zhang HY, Pozzeto B, action. Circulation 1990;82:8–16.Archard LC. Nucleotide sequence of an attenuated mutant of [144] S hirali GS, Ni J, Chinnock RF et al. Association of viral genomecoxsackievirus B3 compared with the cardiovirulent wildtype: with graft loss in children after cardiac transplantation. N Engl Jassessment of candidate mutations by analysis of a revertant to Med 2000;344:1498–1503.cardiovirulence. Clin Diagn Virol 1998;9:99–105. [145] L oebe M, Schuler S, Zais O, Warnecke H, Fleck E, Hetzer R. Role
[137] D unn JJ, Chapman NM, Tracy S, Romero JR. Genomic deter- of cytomegalovirus infection in the development of coronary arteryminants of cardiovirulence in coxsackievirus B3 clinical isolates: disease in the transplanted heart. J Heart Transplant 1990;9:707–localization to the 59 non-translated region. J Virol 2000;74:4787– 711.4794. [146] K oskinen PK, Nieminen MS, Krogerus LA et al. Cytomegalovirus
[138] H ofling K, Kim KS, Leser JS et al. Progress toward vaccines infection and accelerated cardiac allograft vasculopathy in humanagainst virus that cause heart disease. Herz 2000;25:286–290. cardiac allografts. J Heart Lung Transplant 1993;12:724–729.
[139] L am KM, Oldenburg N, Khan MA et al. Significance of reverse [147] B enditt EP, Barrett T, McDougall JK. Viruses in the etiology oftranscription polymerase chain reaction in the detection of human atherosclerosis. Proc Natl Acad Sci USA 1983;80:6386–6389.cytomegalovirus gene transcripts in thoracic organ transplant [148] v an Dorp WT, Jones E, Bruggeman CA, Daha MR, van Es LA, vanrecipients. J Heart Lung Transplant 1998;17:555–565. der Wouder FJ. Direct induction of MHC class I, but not class II
[140] G erna G, Baldanti F, Middeldorp J, Lilleri D. Use of CMV expression on endothelial cells by cytomegalovirus. Transplanta-transcripts for monitoring of CMV infections in transplant recipi- tion 1989;48:469–472.ents. Int J Antimicrob Agents 2000;16:455–460. [149] O sler W. Principles and practice of medicine. New York: D.
[141] P auschinger M, Doerner A, Kuehl U et al. Enteroviral RNA Appleton; 1892.
Dow
nloaded from https://academ
ic.oup.com/cardiovascres/article-abstract/60/1/11/321091 by guest on 03 April 2019