HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY · hypertrophic cardiomyopathy, Evaluation of obstructive...
29
1 HYPERTROPHIC HYPERTROPHIC OBSTRUCTIVE OBSTRUCTIVE CARDIOMYOPATHY CARDIOMYOPATHY Michelle Paulson Michelle Paulson Morning Report 7/21/04 Morning Report 7/21/04
Transcript of HYPERTROPHIC OBSTRUCTIVE CARDIOMYOPATHY · hypertrophic cardiomyopathy, Evaluation of obstructive...
1
HYPERTROPHIC HYPERTROPHIC OBSTRUCTIVE OBSTRUCTIVE
CARDIOMYOPATHYCARDIOMYOPATHY
Michelle PaulsonMichelle PaulsonMorning Report 7/21/04Morning Report 7/21/04

2
HOCMHOCM
!! Nondilated cardiac hypertrophy, in the Nondilated cardiac hypertrophy, in the absence of another diseaseabsence of another disease
!! Dynamic LV outflow obstruction gradient Dynamic LV outflow obstruction gradient between LV outflow tract and aorta) which between LV outflow tract and aorta) which may or may not be present at rest, but can may or may not be present at rest, but can become apparent with changes in become apparent with changes in hemodynamics hemodynamics
!! 75% of patients do NOT have a resting 75% of patients do NOT have a resting gradient and this may develop at any agegradient and this may develop at any age

3
GeneticsGenetics
!! Autosomal dominant missense mutation of gene Autosomal dominant missense mutation of gene encoding cardiac sarcomereencoding cardiac sarcomere
!! Clinically apparent in approximately 1 in 350Clinically apparent in approximately 1 in 350--625 625 peoplepeople
!! 10 genes identified thus far which contribute eg. 10 genes identified thus far which contribute eg. ßß--myosin heavy chain, cardiac troponin T and myosin heavy chain, cardiac troponin T and myosinmyosin--binding protein C (70binding protein C (70--80% of cases)80% of cases)–– Certain mutations of ßCertain mutations of ß--myosin heavy chain and myosin heavy chain and
troponin T associated with higher rates of premature troponin T associated with higher rates of premature deathdeath

4
Sarcomere. Gene with mutations associated Sarcomere. Gene with mutations associated with HCM in red.with HCM in red.Cannon Ro. NEJM 2003; 349:1016.Cannon Ro. NEJM 2003; 349:1016.

5
PathologyPathology!! Mutations lead to impaired Mutations lead to impaired
contractility which in turn contractility which in turn causes upregulation of causes upregulation of growth factors leading to growth factors leading to hypertrophy and hypertrophy and fibrosis=“sarcomere fibrosis=“sarcomere disarray”disarray”
!! Microvascular disease from Microvascular disease from abnormal coronary arteries abnormal coronary arteries with increased intimal and with increased intimal and medial collegen and medial collegen and disproportion between heart disproportion between heart muscle and vasculaturemuscle and vasculature

6
Symptoms Symptoms
*Phenotypic Diversity**Phenotypic Diversity*!! AsymptomaticAsymptomatic!! Dyspnea (most common)Dyspnea (most common)!! Chest painChest pain!! Palpitations Palpitations !! Pre / syncope (15Pre / syncope (15--25%)25%)!! Orthopnea / PNDOrthopnea / PND

7
ComplicationsComplications
!! Mitral valve diseaseMitral valve disease----mechanical dysfunction mechanical dysfunction from hypertrophy, papillary muscle insertion from hypertrophy, papillary muscle insertion abnormalityabnormality
!! Congestive heart failure (5X more likely than Congestive heart failure (5X more likely than general population)general population)
!! Atrial fibrillation (decompensation easier) and Atrial fibrillation (decompensation easier) and higher risk of thromboembolismhigher risk of thromboembolism
!! Endocarditis (esp. mitral valve)Endocarditis (esp. mitral valve)----need to give need to give antibiotics prophylaticallyantibiotics prophylatically
!! Sudden cardiac death via ventricular arrhythmiasSudden cardiac death via ventricular arrhythmias

8
Clinical Exam FindingsClinical Exam Findings
!! Harsh crescendoHarsh crescendo--decrescendo systolic decrescendo systolic ejection murmur best heard at apex and LLSBejection murmur best heard at apex and LLSB
!! Increases with changing from squatting to Increases with changing from squatting to standing position, Valsalva, NTG, standing position, Valsalva, NTG,
!! Decreases with changing from standing to Decreases with changing from standing to sitting, handgrip, leg elevation sitting, handgrip, leg elevation
!! Radiates to axilla/base (less likely to radiate Radiates to axilla/base (less likely to radiate to neck), +/to neck), +/-- S4 and LV liftS4 and LV lift
!! Carotid pulse brisk upstrokeCarotid pulse brisk upstroke

9
Diagnostic ToolsDiagnostic Tools
!! EKGEKG----LVH, inf/lat Q waves, LAD, LAE/RAELVH, inf/lat Q waves, LAD, LAE/RAE!! 2D TTE2D TTE----asymmetric hypertrophy, septum usually thicker asymmetric hypertrophy, septum usually thicker
than free wallthan free wall!! Continuous wave Doppler EchoContinuous wave Doppler Echo----resting high velocity, late resting high velocity, late
peaking jet across LV outflow tract (25% of pts)peaking jet across LV outflow tract (25% of pts)!! Exercise with EchoExercise with Echo----may identify obstruction that is not may identify obstruction that is not
apparent at restapparent at rest!! Cardiac CatheterizationCardiac Catheterization----measure gradient and provoke measure gradient and provoke
with Valsalva, amyl nitrate inhalation or infusion of with Valsalva, amyl nitrate inhalation or infusion of isoproterenolisoproterenol
!! Holter monitor/Loop monitorHolter monitor/Loop monitor----not diagnostic but can help not diagnostic but can help document ventricular tachyarrthymiasdocument ventricular tachyarrthymias

10
TTE showing LV outflow obstruction in systole.TTE showing LV outflow obstruction in systole.Nishimura and Holmes. NEJM 2004; 350: 1320.Nishimura and Holmes. NEJM 2004; 350: 1320.

11
Definitions based on TTEDefinitions based on TTE
!! OBSTRUCTIVE= 30 mmHG peak outflow gradient OBSTRUCTIVE= 30 mmHG peak outflow gradient at rest or >50 with provocationat rest or >50 with provocation
!! HYPERTROPHY=LV wall thickness > 13mm and HYPERTROPHY=LV wall thickness > 13mm and severe if >30mmsevere if >30mm
G=4vG=4v""(modified Bernoulli equation)(modified Bernoulli equation)
G=LV outflow tract gradientG=LV outflow tract gradientV=LV outflow tract velocityV=LV outflow tract velocity

12
Evaluation of RelativesEvaluation of Relatives
!! Should screen all 1st degree family Should screen all 1st degree family members with history / physical, EKG, members with history / physical, EKG, EchoEcho–– If between ages 12If between ages 12--18, needs annual 18, needs annual
assessmentassessment–– If over age 18, need reevaluation every 5 If over age 18, need reevaluation every 5
yearsyearsGenetic mutation analysis is possibleGenetic mutation analysis is possible

13Treatment AlgorithmTreatment AlgorithmMaron. JAMA 287.Maron. JAMA 287.

14
Drug TherapyDrug Therapy
!! **BEST INITIAL APPROACH TO MANAGE **BEST INITIAL APPROACH TO MANAGE SYMPTOMSSYMPTOMS****
!! GoalGoal----block catecholamines and slow heart block catecholamines and slow heart rate to increase fillingrate to increase filling
!! Beta Blocker: 60Beta Blocker: 60--80% response rate80% response rate!! Verapamil: Used if contraindication or intolerance to BB, Verapamil: Used if contraindication or intolerance to BB,
however patients with severe symptoms, pHTN, severe however patients with severe symptoms, pHTN, severe outflow obstruction, there has been an association with outflow obstruction, there has been an association with verapamil and sudden deathverapamil and sudden death
!! Disopyramide: add to BB if BB alone is not controlling Disopyramide: add to BB if BB alone is not controlling symptomssymptoms
!! Amiodarone has not been studied to see if can reduce Amiodarone has not been studied to see if can reduce SCDSCD

15
Other Things to Watch For:Other Things to Watch For:
!! Avoid dehydrationAvoid dehydration!! Correct anemiaCorrect anemia!! Avoid drugs that alter decrease preload Avoid drugs that alter decrease preload
or afterloador afterload–– eg. ACEeg. ACE--I, nitroglycerin, diuretics I, nitroglycerin, diuretics

16
What if medical management fails?What if medical management fails?
Other options:Other options:!! Surgical Septal MyectomySurgical Septal Myectomy!! Septal AblationSeptal Ablation!! Dual Chamber PacemakerDual Chamber Pacemaker
NONE HAVE SHOWN TO NONE HAVE SHOWN TO DECREASE MORTALITYDECREASE MORTALITY

17
Myectomy “Morrow procedure”Myectomy “Morrow procedure”
!! Gold standard for symptomatic HOCMGold standard for symptomatic HOCM!! Resects basal septum, can combine with mitral valve Resects basal septum, can combine with mitral valve
surgerysurgery!! 90% who undergo procedure are subsequently 90% who undergo procedure are subsequently
symptom freesymptom free----associated with increase peak oxygen associated with increase peak oxygen consumption and decrease in NYHA classification consumption and decrease in NYHA classification
!! PeriPeri--operative mortality 1operative mortality 1--2%2%!! Follow up studies 30 years out suggest patients still Follow up studies 30 years out suggest patients still
have improved symptoms and no recurrence of have improved symptoms and no recurrence of obstructionobstruction

18Myectomy ProcedureNishimura and Holmes. NEJM 2004; 350: 1320.

19
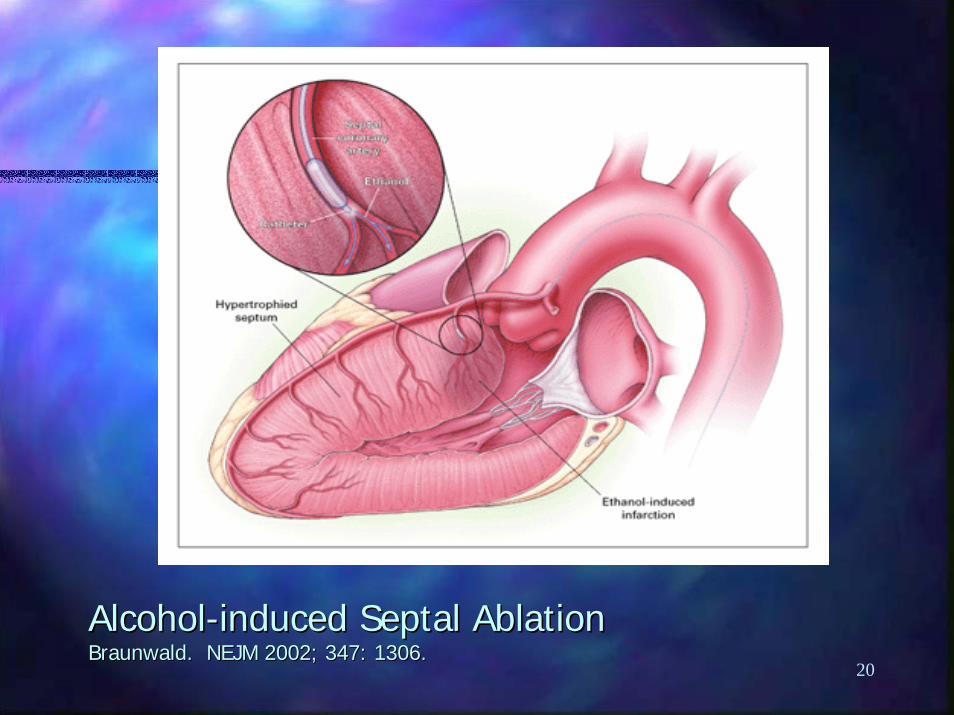
Septal AblationSeptal Ablation
!! Infusion of 100% alcohol into septal artery which Infusion of 100% alcohol into septal artery which supplies the myocardium along the outflow tract, supplies the myocardium along the outflow tract, thereby causing a myocardial infarction in this area thereby causing a myocardial infarction in this area which leads to thinning and decreasing obstructionwhich leads to thinning and decreasing obstruction
!! Complicated by complete heart block (also vfib, VSD, Complicated by complete heart block (also vfib, VSD, large MI, perforation)large MI, perforation)
!! Can be used with contrast echocardiogram to localize Can be used with contrast echocardiogram to localize area perfused by septal branch prior to alcohol area perfused by septal branch prior to alcohol administrationadministration
!! Consider if CHF NYHA IIIConsider if CHF NYHA III--IV, outflow gradient >50, IV, outflow gradient >50, septal wall >18mmseptal wall >18mm
20
AlcoholAlcohol--induced Septal Ablationinduced Septal AblationBraunwald. NEJM 2002; 347: 1306.Braunwald. NEJM 2002; 347: 1306.
21
Dual Chamber PacemakerDual Chamber Pacemaker
!! Unclear mechanism of causing symptomatic Unclear mechanism of causing symptomatic relief, may alter contraction of basal septum with relief, may alter contraction of basal septum with less outflow obstructionless outflow obstruction
!! Large placebo effectLarge placebo effect----still have large residual still have large residual gradient after pacing (30gradient after pacing (30--50mmHg)50mmHg)
!! Follow up in 5 yearsFollow up in 5 years----<40% still reported <40% still reported improvement in symptomsimprovement in symptoms
!! May be useful in pt cannot undergo surgery or May be useful in pt cannot undergo surgery or needs pacer because of bradycardia with medical needs pacer because of bradycardia with medical therapytherapy

22
Summary of nonSummary of non--pharmacological therapies.pharmacological therapies.Nishimura and Holmes. NEJM 2004; 350:1320.Nishimura and Holmes. NEJM 2004; 350:1320.

23
Sudden Death and LVHSudden Death and LVH!! 480 patients with HCM, 480 patients with HCM,
placed into categories based placed into categories based on LV wall thickness: on LV wall thickness: <15mm, 16<15mm, 16--19mm, 2019mm, 20--24mm, 2524mm, 25--29mm, 30mm+29mm, 30mm+–– Follow up of 6.5 yearsFollow up of 6.5 years–– 65/480 died=14% (23 65/480 died=14% (23
died suddenly)died suddenly)–– When LV thickness When LV thickness
accounted for, risk of SCD accounted for, risk of SCD increased with thicknessincreased with thickness
–– Spirito P Spirito P et al.et al. NEJM 2000.NEJM 2000.

24
Implanted Cardiac DefibrillatorImplanted Cardiac Defibrillator!! If there is a risk for If there is a risk for
sudden death; sudden death; unfortunately, no specific unfortunately, no specific guidelines exist for who is guidelines exist for who is a candidate a candidate
!! Currently driven by clinical Currently driven by clinical historyhistory
!! No need to do EP study No need to do EP study because inducing VT/Vfib because inducing VT/Vfib during the study does not during the study does not predict outcome of predict outcome of sudden deathsudden death
NEJM.

25
ACC/AHA GuidelinesACC/AHA Guidelines
!! CLASS IIB recommendation by CLASS IIB recommendation by ACA/AHA/NASPE 2002 guidelines ACA/AHA/NASPE 2002 guidelines regarding ICD placementregarding ICD placement
(Class IIB=Usefuless/efficacy less well established by evidence(Class IIB=Usefuless/efficacy less well established by evidence/opinion.)/opinion.)
“Familial or inherited conditions with a “Familial or inherited conditions with a high risk for life threatening ventricular high risk for life threatening ventricular tachyarrhythmias eg. long QT or tachyarrhythmias eg. long QT or hypertrophy cardiomyopathy”hypertrophy cardiomyopathy”

26
ICD / Sudden Death / HCMICD / Sudden Death / HCM!! Retrospective study of 128 patients to evaluate efficacy of Retrospective study of 128 patients to evaluate efficacy of
ICD to prevent SCD, follow up 3.1 yearsICD to prevent SCD, follow up 3.1 years!! Total of 29/128 patients had appropriate firing (23%), 21 Total of 29/128 patients had appropriate firing (23%), 21
of those stored data that showed VT/VF instigator for of those stored data that showed VT/VF instigator for dischargedischarge
!! 43 placed for secondary prophylaxis (eg. survived cardiac 43 placed for secondary prophylaxis (eg. survived cardiac arrest or had sustained VT); 19/43 had appropriate arrest or had sustained VT); 19/43 had appropriate discharge of ICD (44%)discharge of ICD (44%)
!! 85 placed for primary prophylaxis for syncope, family hx 85 placed for primary prophylaxis for syncope, family hx of SCD, NSVT, LV wall thickness > 30mm; 10/85 had of SCD, NSVT, LV wall thickness > 30mm; 10/85 had appropriate discharge of ICD (12%)appropriate discharge of ICD (12%)
!! Total of inappropriate firings 25%Total of inappropriate firings 25%!! Complications in 18/128Complications in 18/128----lead malfunction, infection, lead malfunction, infection,
hemorrhage requiring thoractomy, subclavian thrombus, hemorrhage requiring thoractomy, subclavian thrombus, hematomahematoma Maron NEJM 2000.

27
The FutureThe Future
!! Losartan decreases fibrosis and down Losartan decreases fibrosis and down regulates growth factor ß in mice trialsregulates growth factor ß in mice trials
!! Simvastatin decreases fibrosis and Simvastatin decreases fibrosis and hypertrophy in rabbits by 50%hypertrophy in rabbits by 50%
!! Routine ScreeningRoutine Screening--not feasible currentlynot feasible currently–– DNA microarrays, mass spectrometryDNA microarrays, mass spectrometry
NEED FOR HUMAN TRIALS

28
References:References:Nishimura RA and Holmes DR. Hypertrophic obstructive Nishimura RA and Holmes DR. Hypertrophic obstructive
cardiomyopathy. NEJM 2004; 350: 1320cardiomyopathy. NEJM 2004; 350: 1320--1327.1327.Up to Date. Clinical Manifestations of hypertrophic Up to Date. Clinical Manifestations of hypertrophic
cardiomyopathy, Treatment of Special Problems in obstructive cardiomyopathy, Treatment of Special Problems in obstructive hypertrophic cardiomyopathy, Evaluation of obstructive hypertrophic cardiomyopathy, Evaluation of obstructive hypertrophic cardiomyopathy, Pharmacological and hypertrophic cardiomyopathy, Pharmacological and Nonpharmacological treatment of outflow obstruction in Nonpharmacological treatment of outflow obstruction in hypertrophic cardiomyopathy. hypertrophic cardiomyopathy.
Maron BJ. Hypertrophic cardiomyopathy: a systematic review. Maron BJ. Hypertrophic cardiomyopathy: a systematic review. JAMA 2002; 287: 1308JAMA 2002; 287: 1308--1320.1320.
Marian AJ and Roberts R. To screen or not is not the questionMarian AJ and Roberts R. To screen or not is not the question--it is it is when and how to screen. Circulation 2003; 107: 2171when and how to screen. Circulation 2003; 107: 2171--2174.2174.
Roberts R and Sigwart U. New concepts in hypertrophic Roberts R and Sigwart U. New concepts in hypertrophic cardiomyopathies, part I. Circulation 2001; 104: 2113cardiomyopathies, part I. Circulation 2001; 104: 2113--2116.2116.
Roberts R and Sigwart U. New concepts in hypertrophic Roberts R and Sigwart U. New concepts in hypertrophic cardiomyopathies, part II. Circulation 2001; 104: 2249cardiomyopathies, part II. Circulation 2001; 104: 2249--2252.2252.

29
References:References:ACC/AHA/NASPE Practice Guidelines. 2002. 13ACC/AHA/NASPE Practice Guidelines. 2002. 13--15, 2515, 25--27.27.Freedman RA. Use of implantable pacemakers and implantable Freedman RA. Use of implantable pacemakers and implantable
defibrillators in hypertrophic cardiomyopathy. Current Opinion defibrillators in hypertrophic cardiomyopathy. Current Opinion in Cardiology 2001; 16: 58in Cardiology 2001; 16: 58--65.65.
Spirito Spirito et al.et al. Magnitude of left ventricular hypertrophy and risk of Magnitude of left ventricular hypertrophy and risk of sudden death in hypertrophic cardiomyopathy. NEJM 2000; sudden death in hypertrophic cardiomyopathy. NEJM 2000; 342: 1778342: 1778--85.85.
Maron BJ Maron BJ et al.et al. Efficacy of implantable cardioverterEfficacy of implantable cardioverter--defibrillators defibrillators for the prevention of sudden death in patients with hypertrophicfor the prevention of sudden death in patients with hypertrophiccardiomyopathy. NEJM 2000; 342: 365cardiomyopathy. NEJM 2000; 342: 365--73.73.