Cardiomyopathy (Mary)

of 47
-
Upload
patricia-marie-buenafe -
Category
Documents
-
view
231 -
download
0
Transcript of Cardiomyopathy (Mary)
-
7/27/2019 Cardiomyopathy (Mary)
1/47
1
INTRODUCTION
Myocardial (heart muscle) dysfunction occurs very commonly, usually due to other
diseases such as coronary artery disease, high blood pressure, and diseases of the heart valves.
Disease originating in the heart muscle itself (cardiomyopathy) is much rarer.
Unfortunately, by the time it is diagnosed, the disease often has reached an advanced
stage and heart failure has occurred. Consequently, about 50 percent of patients with dilated
cardiomyopathy live 5 years once heart failure is diagnosed; about 25 percent live 10 years after
such a diagnosis. Typically, patients die from a continued decline in heart muscle strength, but
some die suddenly of irregular heartbeats.
For patients with advanced disease, heart transplantation greatly improves survival: 75
percent of patients live 5 years after a transplantation. However, the disease also may remain
fairly stable for years, especially with treatment and regular evaluation by a physician.
Cardiomyopathy is a result of pre-existing medical condition and can lead to a more
serious heart disease. There are 79, 320 cases of death cause cardiomyopathy in the whole
world. The following Table1.1 is showing the mortality rate based from (WHO) World Health
Organization Statistics Information Systems compiled January, 2004 .
Table 1.1 Mortality Statistics
http://www.rightdiagnosis.com/artic/nhlbi_cardiomyopathy_nhlbi.htm#Hearthttp://www.rightdiagnosis.com/artic/nhlbi_cardiomyopathy_nhlbi.htm#Heart -
7/27/2019 Cardiomyopathy (Mary)
2/47
2
WORLDWIDE MORBILITY CASES OF DILATED CARDIOMYOPATHY
The following Table 1.2 attempts to show morbidity extrapolate prevalence rate for
Dilated cardiomyopathy to the populations of various countries and regions. These prevalence
extrapolations for Dilated cardiomyopathy are only estimates, based on applying the prevalence
rates from the US (or a similar country) to the population of other countries, and therefore may
have very limited relevance to the actual prevalence of Dilated cardiomyopathy in any region:
Country/Region Extrapolated Prevalence Population Estimated Used
Dilated cardiomyopathy inNorth America(Extrapolated Statistics)
USA 587,310 293,655,4051
Canada 65,015 32,507,8742
Mexico 209,919 104,959,5942
Dilated cardiomyopathy in Central America (Extrapolated Statistics)
Belize 545 272,9452
Guatemala 28,561 14,280,5962
Nicaragua 10,719 5,359,7592
Dilated cardiomyopathy in Caribbean (Extrapolated Statistics)
Puerto Rico 7,795 3,897,9602
Dilated cardiomyopathy inSouth America(Extrapolated Statistics)
Brazil 368,202 184,101,1092
Chile 31,647 15,823,9572
Colombia 84,621 2,310,7752
Paraguay 12,382 6,191,3682
Peru 55,088 27,544,3052
Venezuela 50,034 25,017,3872
Dilated cardiomyopathy in Northern Europe (Extrapolated Statistics)
Denmark 10,826 5,413,3922
Finland 10,429 5,214,5122
Iceland 587 293,9662
Sweden 17,972 8,986,4002
Dilated cardiomyopathy in Western Europe (Extrapolated Statistics)
Britain (United Kingdom)120,541 60,270,708 for UK2
Belgium 20,696 10,348,2762
France 120,848 60,424,2132
Ireland 7,939 3,969,5582
Luxembourg 925 62,6902
Monaco 64 32,2702
Netherlands(Holland) 32,636 16,318,1992
http://www.rightdiagnosis.com/medical/north_america.htmhttp://www.rightdiagnosis.com/medical/north_america.htmhttp://www.rightdiagnosis.com/medical/north_america.htmhttp://www.rightdiagnosis.com/travel-health/canada.htmhttp://www.rightdiagnosis.com/travel-health/canada.htmhttp://www.rightdiagnosis.com/travel-health/mexico.htmhttp://www.rightdiagnosis.com/travel-health/mexico.htmhttp://www.rightdiagnosis.com/travel-health/belize.htmhttp://www.rightdiagnosis.com/travel-health/belize.htmhttp://www.rightdiagnosis.com/travel-health/guatemala.htmhttp://www.rightdiagnosis.com/travel-health/guatemala.htmhttp://www.rightdiagnosis.com/travel-health/nicaragua.htmhttp://www.rightdiagnosis.com/travel-health/nicaragua.htmhttp://www.rightdiagnosis.com/nursing-homes/puerto-rico.htmhttp://www.rightdiagnosis.com/nursing-homes/puerto-rico.htmhttp://www.rightdiagnosis.com/risk/south_america.htmhttp://www.rightdiagnosis.com/risk/south_america.htmhttp://www.rightdiagnosis.com/risk/south_america.htmhttp://www.rightdiagnosis.com/travel-health/brazil.htmhttp://www.rightdiagnosis.com/travel-health/brazil.htmhttp://www.rightdiagnosis.com/travel-health/chile.htmhttp://www.rightdiagnosis.com/travel-health/chile.htmhttp://www.rightdiagnosis.com/travel-health/colombia.htmhttp://www.rightdiagnosis.com/travel-health/colombia.htmhttp://www.rightdiagnosis.com/travel-health/paraguay.htmhttp://www.rightdiagnosis.com/travel-health/peru.htmhttp://www.rightdiagnosis.com/travel-health/peru.htmhttp://www.rightdiagnosis.com/travel-health/venezuela.htmhttp://www.rightdiagnosis.com/travel-health/venezuela.htmhttp://www.rightdiagnosis.com/travel-health/denmark.htmhttp://www.rightdiagnosis.com/travel-health/denmark.htmhttp://www.rightdiagnosis.com/travel-health/finland.htmhttp://www.rightdiagnosis.com/travel-health/finland.htmhttp://www.rightdiagnosis.com/travel-health/iceland.htmhttp://www.rightdiagnosis.com/travel-health/iceland.htmhttp://www.rightdiagnosis.com/travel-health/sweden.htmhttp://www.rightdiagnosis.com/travel-health/sweden.htmhttp://www.rightdiagnosis.com/travel-health/united-kingdom.htmhttp://www.rightdiagnosis.com/travel-health/united-kingdom.htmhttp://www.rightdiagnosis.com/travel-health/united-kingdom.htmhttp://www.rightdiagnosis.com/travel-health/belgium.htmhttp://www.rightdiagnosis.com/travel-health/belgium.htmhttp://www.rightdiagnosis.com/travel-health/france.htmhttp://www.rightdiagnosis.com/travel-health/france.htmhttp://www.rightdiagnosis.com/travel-health/ireland.htmhttp://www.rightdiagnosis.com/travel-health/ireland.htmhttp://www.rightdiagnosis.com/travel-health/luxembourg.htmhttp://www.rightdiagnosis.com/travel-health/luxembourg.htmhttp://www.rightdiagnosis.com/travel-health/monaco.htmhttp://www.rightdiagnosis.com/travel-health/monaco.htmhttp://www.rightdiagnosis.com/travel-health/netherlands.htmhttp://www.rightdiagnosis.com/travel-health/netherlands.htmhttp://www.rightdiagnosis.com/medical/holland.htmhttp://www.rightdiagnosis.com/medical/holland.htmhttp://www.rightdiagnosis.com/medical/holland.htmhttp://www.rightdiagnosis.com/medical/holland.htmhttp://www.rightdiagnosis.com/travel-health/netherlands.htmhttp://www.rightdiagnosis.com/travel-health/monaco.htmhttp://www.rightdiagnosis.com/travel-health/luxembourg.htmhttp://www.rightdiagnosis.com/travel-health/ireland.htmhttp://www.rightdiagnosis.com/travel-health/france.htmhttp://www.rightdiagnosis.com/travel-health/belgium.htmhttp://www.rightdiagnosis.com/travel-health/united-kingdom.htmhttp://www.rightdiagnosis.com/travel-health/sweden.htmhttp://www.rightdiagnosis.com/travel-health/iceland.htmhttp://www.rightdiagnosis.com/travel-health/finland.htmhttp://www.rightdiagnosis.com/travel-health/denmark.htmhttp://www.rightdiagnosis.com/travel-health/venezuela.htmhttp://www.rightdiagnosis.com/travel-health/peru.htmhttp://www.rightdiagnosis.com/travel-health/paraguay.htmhttp://www.rightdiagnosis.com/travel-health/colombia.htmhttp://www.rightdiagnosis.com/travel-health/chile.htmhttp://www.rightdiagnosis.com/travel-health/brazil.htmhttp://www.rightdiagnosis.com/risk/south_america.htmhttp://www.rightdiagnosis.com/nursing-homes/puerto-rico.htmhttp://www.rightdiagnosis.com/travel-health/nicaragua.htmhttp://www.rightdiagnosis.com/travel-health/guatemala.htmhttp://www.rightdiagnosis.com/travel-health/belize.htmhttp://www.rightdiagnosis.com/travel-health/mexico.htmhttp://www.rightdiagnosis.com/travel-health/canada.htmhttp://www.rightdiagnosis.com/medical/north_america.htm -
7/27/2019 Cardiomyopathy (Mary)
3/47
3
United Kingdom 120,541 60,270,7082
Wales 5,836 2,918,0002
Dilated cardiomyopathy in Central Europe (Extrapolated Statistics)
Austria 16,349 8,174,7622
Czech Republic
2,492 1,0246,178
2
Germany 164,849 82,424,609
2
Hungary 20,064 10,032,3752
Liechtenstein 66 33,4362
Poland 77,252 38,626,3492
Slovakia 10,847 5,423,5672
Slovenia 4,022 2,011,4732
Switzerland 14,901 7,450,8672
Dilated cardiomyopathy in Eastern Europe (Extrapolated Statistics)
Belarus 20,621 10,310,5202
Estonia 2,683 1,341,6642
Latvia 4,612 2,306,3062
Lithuania 7,215 3,607,8992
Russia 287,948 143,974,0592
Ukraine 95,464 7,732,0792
Dilated cardiomyopathy in the Southwestern Europe (Extrapolated Statistics)
Azerbaijan 15,736 7,868,3852
Georgia 9,387 ,693,8922
Portugal 21,048 10,524,1452
Spain 80,561 0,280,7802
Dilated cardiomyopathy in Southern Europe (Extrapolated Statistics)
Greece 21,295 10,647,5292
Italy 116,114 58,057,4772
Dilated cardiomyopathy in the Southeastern Europe (Extrapolated Statistics)
Albania 7,089 3,544,8082
Bosnia and Herzegovina 815 07,6082
Bulgaria 15,035 7,517,9732
Croatia 8,993 ,496,8692
Macedonia
4,080 2,040,085
2
Romania 44,711 22,355,551
2
Serbia and Montenegro 21,651 10,825,9002
Dilated cardiomyopathy in Northern Asia (Extrapolated Statistics)
Mongolia 5,502 2,751,3142
Dilated cardiomyopathy in Central Asia (Extrapolated Statistics)
Kazakhstan 30,287 15,143,7042
http://www.rightdiagnosis.com/travel-health/united-kingdom.htmhttp://www.rightdiagnosis.com/travel-health/united-kingdom.htmhttp://www.rightdiagnosis.com/medical/wales.htmhttp://www.rightdiagnosis.com/travel-health/austria.htmhttp://www.rightdiagnosis.com/travel-health/austria.htmhttp://www.rightdiagnosis.com/travel-health/czech-republic.htmhttp://www.rightdiagnosis.com/travel-health/czech-republic.htmhttp://www.rightdiagnosis.com/travel-health/germany.htmhttp://www.rightdiagnosis.com/travel-health/hungary.htmhttp://www.rightdiagnosis.com/travel-health/liechtenstein.htmhttp://www.rightdiagnosis.com/travel-health/liechtenstein.htmhttp://www.rightdiagnosis.com/travel-health/poland.htmhttp://www.rightdiagnosis.com/travel-health/poland.htmhttp://www.rightdiagnosis.com/travel-health/slovakia.htmhttp://www.rightdiagnosis.com/travel-health/slovakia.htmhttp://www.rightdiagnosis.com/travel-health/slovenia.htmhttp://www.rightdiagnosis.com/travel-health/slovenia.htmhttp://www.rightdiagnosis.com/travel-health/switzerland.htmhttp://www.rightdiagnosis.com/travel-health/switzerland.htmhttp://www.rightdiagnosis.com/travel-health/belarus.htmhttp://www.rightdiagnosis.com/travel-health/belarus.htmhttp://www.rightdiagnosis.com/travel-health/estonia.htmhttp://www.rightdiagnosis.com/travel-health/estonia.htmhttp://www.rightdiagnosis.com/travel-health/latvia.htmhttp://www.rightdiagnosis.com/travel-health/latvia.htmhttp://www.rightdiagnosis.com/travel-health/lithuania.htmhttp://www.rightdiagnosis.com/travel-health/lithuania.htmhttp://www.rightdiagnosis.com/travel-health/russia.htmhttp://www.rightdiagnosis.com/travel-health/russia.htmhttp://www.rightdiagnosis.com/travel-health/ukraine.htmhttp://www.rightdiagnosis.com/travel-health/azerbaijan.htmhttp://www.rightdiagnosis.com/travel-health/azerbaijan.htmhttp://www.rightdiagnosis.com/travel-health/georgia.htmhttp://www.rightdiagnosis.com/travel-health/georgia.htmhttp://www.rightdiagnosis.com/travel-health/portugal.htmhttp://www.rightdiagnosis.com/travel-health/portugal.htmhttp://www.rightdiagnosis.com/travel-health/spain.htmhttp://www.rightdiagnosis.com/travel-health/spain.htmhttp://www.rightdiagnosis.com/travel-health/greece.htmhttp://www.rightdiagnosis.com/travel-health/greece.htmhttp://www.rightdiagnosis.com/travel-health/italy.htmhttp://www.rightdiagnosis.com/travel-health/albania.htmhttp://www.rightdiagnosis.com/travel-health/albania.htmhttp://www.rightdiagnosis.com/travel-health/bulgaria.htmhttp://www.rightdiagnosis.com/travel-health/bulgaria.htmhttp://www.rightdiagnosis.com/travel-health/croatia.htmhttp://www.rightdiagnosis.com/travel-health/croatia.htmhttp://www.rightdiagnosis.com/medical/macedonia.htmhttp://www.rightdiagnosis.com/medical/macedonia.htmhttp://www.rightdiagnosis.com/travel-health/romania.htmhttp://www.rightdiagnosis.com/travel-health/romania.htmhttp://www.rightdiagnosis.com/travel-health/mongolia.htmhttp://www.rightdiagnosis.com/travel-health/mongolia.htmhttp://www.rightdiagnosis.com/travel-health/kazakhstan.htmhttp://www.rightdiagnosis.com/travel-health/kazakhstan.htmhttp://www.rightdiagnosis.com/travel-health/mongolia.htmhttp://www.rightdiagnosis.com/travel-health/romania.htmhttp://www.rightdiagnosis.com/medical/macedonia.htmhttp://www.rightdiagnosis.com/travel-health/croatia.htmhttp://www.rightdiagnosis.com/travel-health/bulgaria.htmhttp://www.rightdiagnosis.com/travel-health/albania.htmhttp://www.rightdiagnosis.com/travel-health/italy.htmhttp://www.rightdiagnosis.com/travel-health/greece.htmhttp://www.rightdiagnosis.com/travel-health/spain.htmhttp://www.rightdiagnosis.com/travel-health/portugal.htmhttp://www.rightdiagnosis.com/travel-health/georgia.htmhttp://www.rightdiagnosis.com/travel-health/azerbaijan.htmhttp://www.rightdiagnosis.com/travel-health/ukraine.htmhttp://www.rightdiagnosis.com/travel-health/russia.htmhttp://www.rightdiagnosis.com/travel-health/lithuania.htmhttp://www.rightdiagnosis.com/travel-health/latvia.htmhttp://www.rightdiagnosis.com/travel-health/estonia.htmhttp://www.rightdiagnosis.com/travel-health/belarus.htmhttp://www.rightdiagnosis.com/travel-health/switzerland.htmhttp://www.rightdiagnosis.com/travel-health/slovenia.htmhttp://www.rightdiagnosis.com/travel-health/slovakia.htmhttp://www.rightdiagnosis.com/travel-health/poland.htmhttp://www.rightdiagnosis.com/travel-health/liechtenstein.htmhttp://www.rightdiagnosis.com/travel-health/hungary.htmhttp://www.rightdiagnosis.com/travel-health/germany.htmhttp://www.rightdiagnosis.com/travel-health/czech-republic.htmhttp://www.rightdiagnosis.com/travel-health/austria.htmhttp://www.rightdiagnosis.com/medical/wales.htmhttp://www.rightdiagnosis.com/travel-health/united-kingdom.htm -
7/27/2019 Cardiomyopathy (Mary)
4/47
4
Tajikistan 14,023 7,011,5562
Uzbekistan 52,820 26,410,4162
Dilated cardiomyopathy in Eastern Asia (Extrapolated Statistics)
China 2,597,695 1,298,847,6242
Hong Kong s.a.r. 13,710 6,855,125
2
Japan 254,666 127,333,002
2
Macau s.a.r. 890 45,2862
North Korea 45,395 22,697,5532
South Korea 96,467 8,233,7602
Taiwan 45,499 22,749,8382
Dilated cardiomyopathy in Southwestern Asia (Extrapolated Statistics)
Turkey 137,787 68,893,9182
Dilated cardiomyopathy in Southern Asia (Extrapolated Statistics)
Afghanistan 57,027 28,513,6772
Bangladesh 282,680 141,340,4762
Bhutan 4,371 2,185,5692
India 2,130,141 1,065,070,6072
Pakistan 318,392 159,196,3362
Sri Lanka 39,810 19,905,1652
Dilated cardiomyopathy in Southeastern Asia (Extrapolated Statistics)
East Timor 2,038 1,019,2522
Indonesia 476,905 238,452,9522
Laos 12,136 6,068,1172
Malaysia 47,044 23,522,4822
Philippines 172,483 86,241,6972
Singapore 8,707 ,353,8932
Thailand 129,731 64,865,5232
Vietnam 165,325 82,662,8002
Dilated cardiomyopathy in the Middle East (Extrapolated Statistics)
Gaza strip 2,649 1,324,9912
Iran 135,006 67,503,2052
Iraq 50,749 25,374,6912
Israel
12,398 6,199,008
2
Jordan 11,222 5,611,202
2
Kuwait 4,515 2,257,5492
Lebanon 7,554 3,777,2182
Saudi Arabia 51,591 25,795,9382
Syria 36,033 18,016,8742
United Arab Emirates 5,047 2,523,9152
http://www.rightdiagnosis.com/travel-health/tajikistan.htmhttp://www.rightdiagnosis.com/travel-health/uzbekistan.htmhttp://www.rightdiagnosis.com/travel-health/china.htmhttp://www.rightdiagnosis.com/travel-health/china.htmhttp://www.rightdiagnosis.com/travel-health/japan.htmhttp://www.rightdiagnosis.com/travel-health/japan.htmhttp://www.rightdiagnosis.com/travel-health/north-korea.htmhttp://www.rightdiagnosis.com/travel-health/north-korea.htmhttp://www.rightdiagnosis.com/travel-health/south-korea.htmhttp://www.rightdiagnosis.com/travel-health/south-korea.htmhttp://www.rightdiagnosis.com/travel-health/taiwan.htmhttp://www.rightdiagnosis.com/travel-health/taiwan.htmhttp://www.rightdiagnosis.com/travel-health/turkey.htmhttp://www.rightdiagnosis.com/travel-health/afghanistan.htmhttp://www.rightdiagnosis.com/travel-health/afghanistan.htmhttp://www.rightdiagnosis.com/travel-health/bangladesh.htmhttp://www.rightdiagnosis.com/travel-health/bangladesh.htmhttp://www.rightdiagnosis.com/travel-health/bhutan.htmhttp://www.rightdiagnosis.com/travel-health/bhutan.htmhttp://www.rightdiagnosis.com/travel-health/india.htmhttp://www.rightdiagnosis.com/travel-health/india.htmhttp://www.rightdiagnosis.com/travel-health/pakistan.htmhttp://www.rightdiagnosis.com/travel-health/pakistan.htmhttp://www.rightdiagnosis.com/travel-health/sri-lanka.htmhttp://www.rightdiagnosis.com/travel-health/sri-lanka.htmhttp://www.rightdiagnosis.com/travel-health/east-timor.htmhttp://www.rightdiagnosis.com/travel-health/indonesia.htmhttp://www.rightdiagnosis.com/travel-health/indonesia.htmhttp://www.rightdiagnosis.com/travel-health/laos.htmhttp://www.rightdiagnosis.com/travel-health/laos.htmhttp://www.rightdiagnosis.com/travel-health/malaysia.htmhttp://www.rightdiagnosis.com/travel-health/malaysia.htmhttp://www.rightdiagnosis.com/travel-health/philippines.htmhttp://www.rightdiagnosis.com/travel-health/philippines.htmhttp://www.rightdiagnosis.com/travel-health/singapore.htmhttp://www.rightdiagnosis.com/travel-health/singapore.htmhttp://www.rightdiagnosis.com/travel-health/thailand.htmhttp://www.rightdiagnosis.com/travel-health/thailand.htmhttp://www.rightdiagnosis.com/travel-health/vietnam.htmhttp://www.rightdiagnosis.com/travel-health/vietnam.htmhttp://www.rightdiagnosis.com/travel-health/iran.htmhttp://www.rightdiagnosis.com/travel-health/iran.htmhttp://www.rightdiagnosis.com/travel-health/iraq.htmhttp://www.rightdiagnosis.com/travel-health/iraq.htmhttp://www.rightdiagnosis.com/travel-health/israel.htmhttp://www.rightdiagnosis.com/travel-health/israel.htmhttp://www.rightdiagnosis.com/travel-health/jordan.htmhttp://www.rightdiagnosis.com/travel-health/jordan.htmhttp://www.rightdiagnosis.com/travel-health/kuwait.htmhttp://www.rightdiagnosis.com/travel-health/kuwait.htmhttp://www.rightdiagnosis.com/travel-health/lebanon.htmhttp://www.rightdiagnosis.com/travel-health/lebanon.htmhttp://www.rightdiagnosis.com/travel-health/saudi-arabia.htmhttp://www.rightdiagnosis.com/travel-health/saudi-arabia.htmhttp://www.rightdiagnosis.com/travel-health/syria.htmhttp://www.rightdiagnosis.com/travel-health/syria.htmhttp://www.rightdiagnosis.com/travel-health/united-arab-emirates.htmhttp://www.rightdiagnosis.com/travel-health/united-arab-emirates.htmhttp://www.rightdiagnosis.com/travel-health/united-arab-emirates.htmhttp://www.rightdiagnosis.com/travel-health/syria.htmhttp://www.rightdiagnosis.com/travel-health/saudi-arabia.htmhttp://www.rightdiagnosis.com/travel-health/lebanon.htmhttp://www.rightdiagnosis.com/travel-health/kuwait.htmhttp://www.rightdiagnosis.com/travel-health/jordan.htmhttp://www.rightdiagnosis.com/travel-health/israel.htmhttp://www.rightdiagnosis.com/travel-health/iraq.htmhttp://www.rightdiagnosis.com/travel-health/iran.htmhttp://www.rightdiagnosis.com/travel-health/vietnam.htmhttp://www.rightdiagnosis.com/travel-health/thailand.htmhttp://www.rightdiagnosis.com/travel-health/singapore.htmhttp://www.rightdiagnosis.com/travel-health/philippines.htmhttp://www.rightdiagnosis.com/travel-health/malaysia.htmhttp://www.rightdiagnosis.com/travel-health/laos.htmhttp://www.rightdiagnosis.com/travel-health/indonesia.htmhttp://www.rightdiagnosis.com/travel-health/east-timor.htmhttp://www.rightdiagnosis.com/travel-health/sri-lanka.htmhttp://www.rightdiagnosis.com/travel-health/pakistan.htmhttp://www.rightdiagnosis.com/travel-health/india.htmhttp://www.rightdiagnosis.com/travel-health/bhutan.htmhttp://www.rightdiagnosis.com/travel-health/bangladesh.htmhttp://www.rightdiagnosis.com/travel-health/afghanistan.htmhttp://www.rightdiagnosis.com/travel-health/turkey.htmhttp://www.rightdiagnosis.com/travel-health/taiwan.htmhttp://www.rightdiagnosis.com/travel-health/south-korea.htmhttp://www.rightdiagnosis.com/travel-health/north-korea.htmhttp://www.rightdiagnosis.com/travel-health/japan.htmhttp://www.rightdiagnosis.com/travel-health/china.htmhttp://www.rightdiagnosis.com/travel-health/uzbekistan.htmhttp://www.rightdiagnosis.com/travel-health/tajikistan.htm -
7/27/2019 Cardiomyopathy (Mary)
5/47
5
West Bank 4,622 2,311,2042
Yemen 40,049 20,024,8672
Dilated cardiomyopathy in Northern Africa (Extrapolated Statistics)
Egypt 152,234 76,117,4212
Libya
11,263 5,631,585
2
Sudan 78,296 39,148,162
2
Dilated cardiomyopathy inWestern Africa(Extrapolated Statistics)
Congo Brazzaville 5,996 2,998,0402
Ghana 41,514 20,757,0322
Liberia 6,781 3,390,6352
Niger 22,721 11,360,5382
Nigeria 35,500 12,5750,3562
Senegal 21,704 10,852,1472
Sierra leone 11,767 5,883,8892
Dilated cardiomyopathy inCentral Africa(Extrapolated Statistics)
Central African Republic 7,484 3,742,4822
Chad 19,077 9,538,5442
Congo Kinshasa 116,634 58,317,0302
Rwanda 16,477 8,238,6732
Dilated cardiomyopathy inEastern Africa(Extrapolated Statistics)
Ethiopia 142,673 71,336,5712
Kenya 65,964 32,982,1092
Somalia 16,609 8,304,6012
Tanzania 72,141 36,070,7992
Uganda 52,780 26,390,2582
Dilated cardiomyopathy in Southern Africa (Extrapolated Statistics)
Angola 21,957 10,978,5522
Botswana 3,278 1,639,2312
South Africa 88,896 4,448,4702
Swaziland 2,338 1,169,2412
Zambia 22,051 11,025,6902
Zimbabwe 7,343 1,2671,8602
Dilated cardiomyopathy inOceania(Extrapolated Statistics)Australia 39,826 19,913,144
2
New Zealand 7,987 3,993,8172
Papua New Guinea 10,840 5,420,2802
Table 1.2 Morbidity Extrapolate Prevalence rate for Dilated Cardiomyopathy
Source:US Census Bureau, Population Estimates, 2004US Census Bureau, International Data Base, 2004
http://www.rightdiagnosis.com/travel-health/yemen.htmhttp://www.rightdiagnosis.com/travel-health/egypt.htmhttp://www.rightdiagnosis.com/travel-health/egypt.htmhttp://www.rightdiagnosis.com/travel-health/libya.htmhttp://www.rightdiagnosis.com/travel-health/libya.htmhttp://www.rightdiagnosis.com/travel-health/sudan.htmhttp://www.rightdiagnosis.com/travel-health/sudan.htmhttp://www.rightdiagnosis.com/risk/africa.htmhttp://www.rightdiagnosis.com/risk/africa.htmhttp://www.rightdiagnosis.com/risk/africa.htmhttp://www.rightdiagnosis.com/travel-health/ghana.htmhttp://www.rightdiagnosis.com/travel-health/ghana.htmhttp://www.rightdiagnosis.com/travel-health/liberia.htmhttp://www.rightdiagnosis.com/travel-health/liberia.htmhttp://www.rightdiagnosis.com/travel-health/niger.htmhttp://www.rightdiagnosis.com/travel-health/niger.htmhttp://www.rightdiagnosis.com/travel-health/nigeria.htmhttp://www.rightdiagnosis.com/travel-health/nigeria.htmhttp://www.rightdiagnosis.com/travel-health/senegal.htmhttp://www.rightdiagnosis.com/travel-health/senegal.htmhttp://www.rightdiagnosis.com/travel-health/sierra-leone.htmhttp://www.rightdiagnosis.com/travel-health/sierra-leone.htmhttp://www.rightdiagnosis.com/risk/africa.htmhttp://www.rightdiagnosis.com/risk/africa.htmhttp://www.rightdiagnosis.com/risk/africa.htmhttp://www.rightdiagnosis.com/travel-health/central-african-republic.htmhttp://www.rightdiagnosis.com/travel-health/central-african-republic.htmhttp://www.rightdiagnosis.com/travel-health/chad.htmhttp://www.rightdiagnosis.com/travel-health/chad.htmhttp://www.rightdiagnosis.com/travel-health/rwanda.htmhttp://www.rightdiagnosis.com/travel-health/rwanda.htmhttp://www.rightdiagnosis.com/risk/africa.htmhttp://www.rightdiagnosis.com/risk/africa.htmhttp://www.rightdiagnosis.com/risk/africa.htmhttp://www.rightdiagnosis.com/travel-health/ethiopia.htmhttp://www.rightdiagnosis.com/travel-health/ethiopia.htmhttp://www.rightdiagnosis.com/travel-health/kenya.htmhttp://www.rightdiagnosis.com/travel-health/kenya.htmhttp://www.rightdiagnosis.com/travel-health/somalia.htmhttp://www.rightdiagnosis.com/travel-health/somalia.htmhttp://www.rightdiagnosis.com/travel-health/tanzania.htmhttp://www.rightdiagnosis.com/travel-health/tanzania.htmhttp://www.rightdiagnosis.com/travel-health/uganda.htmhttp://www.rightdiagnosis.com/travel-health/uganda.htmhttp://www.rightdiagnosis.com/travel-health/angola.htmhttp://www.rightdiagnosis.com/travel-health/angola.htmhttp://www.rightdiagnosis.com/travel-health/botswana.htmhttp://www.rightdiagnosis.com/travel-health/botswana.htmhttp://www.rightdiagnosis.com/travel-health/south-africa.htmhttp://www.rightdiagnosis.com/travel-health/south-africa.htmhttp://www.rightdiagnosis.com/travel-health/swaziland.htmhttp://www.rightdiagnosis.com/travel-health/swaziland.htmhttp://www.rightdiagnosis.com/travel-health/zambia.htmhttp://www.rightdiagnosis.com/travel-health/zambia.htmhttp://www.rightdiagnosis.com/travel-health/zimbabwe.htmhttp://www.rightdiagnosis.com/travel-health/zimbabwe.htmhttp://www.rightdiagnosis.com/medical/oceania.htmhttp://www.rightdiagnosis.com/medical/oceania.htmhttp://www.rightdiagnosis.com/medical/oceania.htmhttp://www.rightdiagnosis.com/travel-health/australia.htmhttp://www.rightdiagnosis.com/travel-health/australia.htmhttp://www.rightdiagnosis.com/travel-health/new-zealand.htmhttp://www.rightdiagnosis.com/travel-health/new-zealand.htmhttp://www.rightdiagnosis.com/travel-health/papua-new-guinea.htmhttp://www.rightdiagnosis.com/travel-health/papua-new-guinea.htmhttp://www.rightdiagnosis.com/travel-health/papua-new-guinea.htmhttp://www.rightdiagnosis.com/travel-health/new-zealand.htmhttp://www.rightdiagnosis.com/travel-health/australia.htmhttp://www.rightdiagnosis.com/medical/oceania.htmhttp://www.rightdiagnosis.com/travel-health/zimbabwe.htmhttp://www.rightdiagnosis.com/travel-health/zambia.htmhttp://www.rightdiagnosis.com/travel-health/swaziland.htmhttp://www.rightdiagnosis.com/travel-health/south-africa.htmhttp://www.rightdiagnosis.com/travel-health/botswana.htmhttp://www.rightdiagnosis.com/travel-health/angola.htmhttp://www.rightdiagnosis.com/travel-health/uganda.htmhttp://www.rightdiagnosis.com/travel-health/tanzania.htmhttp://www.rightdiagnosis.com/travel-health/somalia.htmhttp://www.rightdiagnosis.com/travel-health/kenya.htmhttp://www.rightdiagnosis.com/travel-health/ethiopia.htmhttp://www.rightdiagnosis.com/risk/africa.htmhttp://www.rightdiagnosis.com/travel-health/rwanda.htmhttp://www.rightdiagnosis.com/travel-health/chad.htmhttp://www.rightdiagnosis.com/travel-health/central-african-republic.htmhttp://www.rightdiagnosis.com/risk/africa.htmhttp://www.rightdiagnosis.com/travel-health/sierra-leone.htmhttp://www.rightdiagnosis.com/travel-health/senegal.htmhttp://www.rightdiagnosis.com/travel-health/nigeria.htmhttp://www.rightdiagnosis.com/travel-health/niger.htmhttp://www.rightdiagnosis.com/travel-health/liberia.htmhttp://www.rightdiagnosis.com/travel-health/ghana.htmhttp://www.rightdiagnosis.com/risk/africa.htmhttp://www.rightdiagnosis.com/travel-health/sudan.htmhttp://www.rightdiagnosis.com/travel-health/libya.htmhttp://www.rightdiagnosis.com/travel-health/egypt.htmhttp://www.rightdiagnosis.com/travel-health/yemen.htm -
7/27/2019 Cardiomyopathy (Mary)
6/47
6
LOCAL MORBIDITY STATISTICS
In this Table 1.3 shows the morbidity rate in the Philippines on 2000- 2004 & 2005. The
disease of the heart was 7th
most leading cause of morbidity cases ranges 43, 898. And highest
most leading cause is Acute Lower Respiratory Infection ranging 690,566.
Table 1.3 Morbidit:10 Leading Causes, Number and Rate.
OBJECTIVES OF THE STUDY
General Objectives
Readers will be able to gain more knowledge and information about cardiomyopathy. As
third year students, we learned patient based heart complication. In this matter, what we learned
inside the room will be able to apply to an actual patient depending on the condition his needs.
Patient centered
- Gather all necessary data of the patient that are related to heart disease that are available
as is may be helpful to case study.
- Present the definition of the complete diagnosis that will explain the illness or
complication.
-
7/27/2019 Cardiomyopathy (Mary)
7/47
7
- Study the anatomy and physiology of that certain body part that is affected by the
complication.
- Trace the pathophysiology of cardiac disease (cardiomyopathy).
- Determined the possible diagnostic test needed for the case including implication and
nursing responsibility for the needs of the patient.
- Formulate a nursing care base plan on the possible secondary complication.
- Evaluate complications to nursing practice, education and research.
- To render health teachings and guidelines to those patients in the future for them to
prevent the risk of heart failure.
- The student nurse wants to learn actual complication that may occur on the future.
Nurse centered
After the completion of the case study the student nurse should be able to:
- Present comprehensive and detailed report regarding the complication.
- Have a well-structured nursing diagnosis of the complication based on patient integration
data.
- Understand the factors that might have been contributed to the development of the
complication.
- To provide an organized and structured nursing interventions as a response to the patient
anticipated needs.- Provide relevant information on available alternative therapies and management.
NURSING ASSESSMENT
FAMILY GENOGRAM
Mr. Ferding (code name) not his real name is the youngest siblings from Mr.
Swirding(father of client, 65, deceased ) and Mrs. Sorayna(mother of client, 72, deceased). Five
of the family members are alive and well. Three of his brother and two sisters died with a history
of cardiac arrest and 2 died in spontaneous abortion.
His grandparents on mother side and father side, most of them died in cardiac arrest as he
stated when we did an interview with him. SeeFigure 1.1 to elaborate more on his family tree.
-
7/27/2019 Cardiomyopathy (Mary)
8/47
8
Figure 1.1FAMILY TREE
(FAMILY HEALTH/ ILLNESS HISTORY)
PERSONAL HISTORYMr. Ferding (code name) not his real name is a 53 yrs. old male born on April 30 1959.
His parents are both gone, he has siblings 7 of them are already gone while 6 are still alive. He
married his wife (Esme) at the age of 25 yrs. old. Now he is a father of 6 children.
Mr. Ferding and his family are protestant. He is a carpenter and is earning enough to
support his family including their education.
Lifestyle and Activities of Daily Living
Family Lifestyle
Mr. Ferding works 6 days a week fixing and repairing houses while his wife takes care of
their children at home. Their children are quite good and they are cooperative when they are told
to do so.
-
7/27/2019 Cardiomyopathy (Mary)
9/47
9
Activities of Daily Living
Mr. Ferding usually gets up at 5 am to prepare himself to go for work. He will just eat at
6 AM, at 7 AM he will now go to his work. During morning until 12 at noon then have his lunch
for 1 hr. After 1 hr. he will now start working again for another 5 hrs. When he comes home at 5
pm he will just take a short break. He will then make sure that all his children is home at 7-8
before they eat their dinner. At 9 pm Mr. Ferding usually on bed ready to sleep and prepare for
the next day routine.
Eating Pattern
Mr. Ferding stated that he likes to eat heavy meals because of the kind of his work. He
eats fried rice in the morning to sustain his activities. He also eats rice and partner usually with
meat or fish and vegetables at noon and dinner. His wife is the one who prepares his food for
work.
Bowel and Bladder Elimination
Mr. Ferding stated that he is usually defecates once a day. Sometimes he exerts effort just
to expel it. But when he feels like he is constipated, he drinks warm liquid after a while he will
then go to the toilet. He also stated that he have no hard time urinating, there is no pain or any
burning sensation.
Family Relationship
Mr. Ferding stated that he is a family man. He always makes sure that all his children is
equally given attention to. He also added that his children are open to share their problems. And
as a father he always gives advice with an open minded.
Home and Neighborhood Condition
Ms. Ferdings house is consisting of 3 bedrooms, 1 for him and his wife, 1 for his girls
and the other is for his boys. The bedroom of his children is consisting of bunk beds. They have
living room and kitchen. They have friendly neighbors and never had been in the fight before.
HISTORY OF PAST AND PRESENT ILLNESS
Past Illness
According to Mr. Ferding 20 years ago he was a smoker then , and was diagnosed with
hypertension. He did not comply with maintenance medication because he cannot afford it
-
7/27/2019 Cardiomyopathy (Mary)
10/47
10
and he feel like he still have hypertension after a while so he thought he was ok and no need to
take it.
Present Illness
Mr. Ferding decided to go to the hospital because of excessive coughing and feeling of
easy fatigability.
June 22- 2 weeks prior to admission Mr. Ferding experiences slight chills and fever but he still
went to work. When he came home he took Biogesic for his fever and since his daughter is a
nurse he just ask her to take his vital signs. Everything was normal but a slightly elevated
temperature. The next morning he felt ok. Then decided to go back to work
July 6 -1 day prior to admission experienced coughing and feeling of easy fatigability. He did
not got to work and he took a rest hoping that it will go away.
July 7 - 1 hour prior to admission Mr. Ferding experiencedexcessive coughing and DOB.
ACTUAL PHYSICAL ASSESSMENT
Nutrition assessmentThe muscle tone of the patient was firm and developed with unequal strength on the
upper peripheral extremities. Body fat was equally distributed in the waist thighs and triceps.
Posture was erect but difficulty walking. The patient experienced easy fatigability. Skin is
rough, dry and decrease skin turgor. Nail was firm and pale nail beds. Hair was brittle and
dry. Lips are puffy with visible fissures on the corner of the mouth. Eyes are clear and pale.
There was normal reflex. Apical rate of 73 bpm and a blood pressure of 110/70.
Skin and nail assessment
Brown color skin, there was a thick but smooth texture with a clammy temperature.
Skin turgor of 5 seconds. There was a presence ofgrade 2 edema in the lower extremities.
Patient had a black dry hair. Scalp was symmetrical smooth and there was no presence of lesion
and no parasites. There was a round nail with 180O
nail base, thick in texture and immobile.
-
7/27/2019 Cardiomyopathy (Mary)
11/47
11
Head and Neck
Head was symmetrical round hard and smooth. Face was symmetrical centered head
position. Neck had a smooth and control movement and ROM of (flexion-45O
, extension-55O
,
lateral abduction-40O
, and rotation-70O
.) trachea and thyroid are in the midline position and
non-tender.
Eyes and Ears
Blinking was symmetrical and involuntary. Cornea was transparent, iris and pupils are
round and equal. Iris was clear and uniform in color. There was no discharge and tenderness on
the lacrimal apparatus upon palpation. Pinna of the ear was aligned with corner of the eye. Skin
smooth without nodule and color was the same with the face. Auricle tragus was non-tender
upon palpation. Mastoid process was not-tender when palpated, warm in temperature and easily
palpated without edema.
Mouth throat and nose
Lips and surrounding tissues are relatively symmetrical in position. There was fissure
and puffiness on the side of the mouth when smiling. Tongue was fissure and moves smoothly
and slightly pale in color. Color of the nose was the same as the face, smooth and symmetrical
in appearance. There was visible nasal flaring during inspiration. There are no nodules, masses
or pain reported during palpation. Sinuses are non-tender during palpation.
Chest and Lungs
Color in the chest was slightly pallor, intercostals space is retracting during with RR of
24 bpm. Chest symmetrical was equal. There was no pain upon palpation but there was a
presence of wheezing sound on both lung fields.
Heart
Apical pulse was 73 bpm upon auscultation with 53 PR upon palpation.
Peripheral vascular
-
7/27/2019 Cardiomyopathy (Mary)
12/47
12
Brachial artery blood pressure of 110/70 mmhg, 53 bpm PR. Extremities are slightly
pallor. Temperature of 34.2O
can identify pain. Radial pulse was weak and slow. Lower
extremities are slightly pallor with grade 2 bipedal edema. Verbalized no calf pain.
ANATOMY AND PHYSIOLOGY
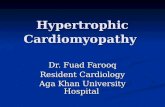
Figure 1.2 Layers of the heart
Pericardial cavitythe space between the layers of the pericardium contains
approximately 1030 ml of fluid. Parietal pericardium-surround almost the entire ascending
aorta and main pulmonary artery as well as portion of the inferior and superior vena cava and
the pulmonary vein. Fibrous pericardium ( Parietal Layer) surrounds the heart and attaches to the
great vessels which are several large blood vessels that return blood to the heart. Coronary blood
vessel the blood vessels that supplies oxygen and nutrient to the heart itself. Endocardium is the
inner layer of the heart where the blood is filled during cardiac relaxation. Myocardium is
responsible for contraction and expelling blood during cardiac contraction. Epicardium( Visceral
Pericardium ) contains the epicardial coronary arteries and veins. This is the inner lining of the
pericardium; it is delicate inner lining of the parietal pericardium and is the outer lining the great
vessel. (See figure 1.2)
-
7/27/2019 Cardiomyopathy (Mary)
13/47
13
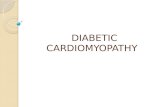
Figure 1.3 Blood flow illustration
Blood Flow
First, superior vena cava carries deoxygenated blood from the upper extremities whileinferior vena cava carries .deoxygenated blood from lower extremities. From the vena cavas
blood will drain in the right atrium. From the right atrium blood will now go to the right ventricle
through the tricuspid valve. From right ventricle deoxygenated blood will pass through the
pulmonary valve and pulmonary artery going to the pulmonary trunk and lungs for the process of
oxygenation. In the lungs blood will release carbon dioxide and will be oxygenized. Blood will
pass through the pulmonary vein down to the left atria. From left atria the mitral valve will open
and will be drain down to the left ventricle. The left ventricle now will pump the oxygenated
blood towards the aortic valve ascending and descending aorta. The oxygenated blood is now
going to for the systemic circulation.
The movement of the blood through the heart is controlled by the opening and closing of
the valves and the contraction and relaxation of the myocardium. Coronary circulation delivers
oxygenated blood to myocardium and removes carbon dioxide from it. Deoxygenated blood
-
7/27/2019 Cardiomyopathy (Mary)
14/47
14
from the heat returns to the atria via coronary sinus. (See Figure 1.3)Malfunction of this system can
result to angina pectoris or myocardial infarction.
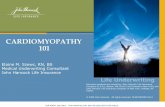
Figure 1.4 SA node and AV node
Conduction system of the heart
The conduction system of the heart consists of specialized cardiac muscle tissue that
generates and distributes action potential. Components of this system are the sinoatrial (SA) node
this is the peacemaker, and initiate the cardiac contraction by passing electric impulse to
atrioventricular (AV) node(See Figure 1.4),in which this node passes the electric impulse going to
the bundle of his. From the bundle of His electric impulse will pass through the purkenji fibers.
Thus, cardiac contraction happens.
-
7/27/2019 Cardiomyopathy (Mary)
15/47
15
PATHOPHYSIOLOGY(Patient based)
Figure 1.5 Pathophysiology (Patient-Based)
-
7/27/2019 Cardiomyopathy (Mary)
16/47
16
Figure 1.6 Pathophysiology(book based)
-
7/27/2019 Cardiomyopathy (Mary)
17/47
17
DEFINITION OF THE DISEASE
Heart muscle disease is called cardiomyopathy and is a problem with the physical shape
of the muscle. Often its origin is unknown. Cardiomyopathy is a serious condition that can lead
to heart failure, dysrhythmias and death.
SYNTHESIS OF THE DISEASE
RISK FACTORS (patient based)
Genetic factor-if the person has a family history of heart diseases 20-30%
possibility that he/she will acquire that disease from them as it already runs on the genes.
(Daniels 2010). From the start a person with family history of cardiomyopathy has
already a cardiac abnormalities and its unknown if this will progress to full
cardiomyopathy to later life. There is a presence of disease genes (dystrophin, tatazzin,
cardiac actin, desmin, Lamin A/C, delta-sarcoglycan, cardiac beta myocin heavy chain,
and cardiac troponin T-gene).
The mutation in Lamin A/C is the one that causes cardiomyopathy. Other
mutations are the cause in addition skeletal muscle myopathy. Dystrophin mutation are
the cause of the rare X-linked dilated cardiomyopathy without skeletal muscle
involvement and a progressive course in young men. Other mutation in dystrophin gene,
mainly deletion , are the cause of muscular dystrophy Becker and Duchenne which arealso present in dilated cardiomyopathy.
Age-the higher the age of a person the higher the risk for heart diseases because of the
degeneration of the tissues. And the presence of atherosclerotic disease that usually
occurs in the late stage of life. This atherosclerosis causes a strain in the heart muscle
because of compensatory mechanism of the body usually being a tachycardic.
Gender- male is more prone to having cardiac related diseases than the female because of
the vices (smoking, drinking). This activity causes the destruction and toxicity of cells in
the heart.
PRECIPITATING FACTOR
Smoking- cigarrete contain a chemical nicotine that is responsible in the hardening of the
arteries that causes increase workload in the heart that may lead to myocardial disease or
heart failure. While the carbon monoxide toxicity causes the heart to weakens.
-
7/27/2019 Cardiomyopathy (Mary)
18/47
18
Respiratory infection- bacterial infection causes increase in secretion causing coughing
and increase in oxygen demand leading to a compensatory mechanism of the body such
as increase in heart rate and respiratory rate.
easy fatigability s being experienced because of the increase in oxygen demand
cough because of the reaction of bacterial infection in the RR system
Pulse deficit most possible is because of the medication specifically the Digoxin.
SIGNS AND SYMPTOMS (patient based)
Signs and symptoms Rationale
Fever
The high temperature of the patient is caused
by respiratory infection by the inflammation of
the tracheal and bronchial area, due to
pathogenic invasion. The inflammation willcause releasing of pyrogens from cells. These
endogenous pyrogens will stimulate the release
of prostaglandin that will trigger thehypothalamic thermostat to higher temperature.
Hypertension
Or high blood pressure. It is because ofdecrease vascular regulation(atherosclerosis)
resulting from malfunction of arterial blood
flow due to formation of clots. And then therewould be elevated blood pressure that will lead
to increased heart rate.
Easy fatigability
Due to continuous exertion of heart andincrease in oxygen demand. It will cause an
overuse stage and eventually the body willexperience of feeling weakness, tiredness and
listlessness.
Impaired gas exchange
Due to myocardial dysfunction secondary to
decrease mayocardial contraction there would
be an abnormal perfusion. That explains theamount of blood ejected from left ventricle
diminished and the heart cannot pump enough
blood to meet body needs. It will cause limited
airflow which leads to decreased cardiacoutput.
Activity intolerance
Due to long term HPN and irregular cardiacpattern there is an impaired heart muscle
resulting to decrease its capacity to function
normally also resulting to decrease bloodvolume and oxygen in the systemic circulation
causing easy fatigability
-
7/27/2019 Cardiomyopathy (Mary)
19/47
19
Nail and skin color changes
Decrease cardiac output and decrease arterial
perfusion will cause abnormal process ofcirculation to a capillary bed in blood tissue
that affects the skin color changes and the
extremities.
Abnormal urine output
-Decrease cardiac output and decrease RBCwill cause R-A-A stimulation. It means thatthere is re-absorption of sodium and water in
the blood. It will bring about by fluids and
electrolytes imbalances.-Due to decrease kidney function there is an
improper absorption of water and wastes from
the blood stream.
Edema
Due to decrease kidney function and R-A-A
stimulation the retention of too much salt
causes the body to retain water. This water
then leaks into the interstitial tissue space. Thisis what we call edema.
TREATMENT
DIAGNOSTICS AND LABORATORY PROCEDURES
General nursing responsibilities
Check doctors order
Explain to the client the importance of the test and what it is for
ECG
Before
Remove all metals attached to the body
Make sure your health care provider knows about all the medications you are taking, as
some can interfere with test results.
Exercising or drinking cold water immediately before an ECG may cause false results.
An ECG is painless. No electricity is sent through the body. The electrodes may feel cold
when first applied. In rare cases, some people may develop a rash or irritation where the
patches were placed.
-
7/27/2019 Cardiomyopathy (Mary)
20/47
20
During
You will be asked to lie down. The health care provider will clean several areas on your
arms, legs, and chest, and then attach small patches called electrodes to the areas. It may
be necessary to shave or clip some hair so the patches stick to the skin. The number of
patches used may vary.
The patches are connected by wires to a machine that turns the heart's electrical signals
into wavy lines, which are often printed on paper. The test results are reviewed by the
doctor.
You usually need to remain still during the procedure. The health care provider may also
ask you to hold your breath for a few seconds as the test is being done. Any movement,
including muscle tremors such as shivering, can alter the results. So it is important to be
relaxed and relatively warm during an ECG recording.
Sometimes this test is done while you are exercising or under minimal stress to monitor
changes in the heart. This type of ECG is often called a stress test.
After
Remove the patches slowly
Diagnostic/laboratory
procedure
Date
ordered:
July 7,2012
General
description
Indication
or
purpose
Result Normal
values
Analysis and
interpretation
ECG Dateresult in:July 7,
2012
Standardized
recording of
electrical activity
of the heart
To detect
cardiac
ischemia
and
abnormal
rhythms.
PR-0.30
secondsQRS-0.06
seconds
QT-0.26
seconds
PR-0.12-
0.20 sec
QRS-0.06-0.12 sec
QT-0.32-
0.44 sec
The PR wave
was prolong.
The QRS is
normal.
The QT is
shorter than
normal.
URINE TEST
Before
Instruct the patient to void directly into a clean, dry container. Sterile, disposable
containers are recommended.
-
7/27/2019 Cardiomyopathy (Mary)
21/47
21
During
Cover all specimens tightly, label properly and send immediately to the laboratory.
If a urine sample is obtained from an indwelling catheter, it may be necessary to clamp
the catheter for about 15-30 minutes before obtaining the sample. Clean the specimen
port with antiseptic before aspirating the urine sample with a needle and a syringe.
After
Observe standard precautions when handling urine specimens.
If the specimen cannot be delivered to the laboratory or tested within an hour, it should
be refrigerated or have an appropriate preservative added
Diagnostic/labo
ratory
procedure
Date ordered:July 7 2012
General
description
Indicatio
n or
purpose
Result Normalvalues
Analysis and
interpretatio
n
URINE TEST Date resultin:July 7 2012
Urine test is atest where in
urine is being
collected to
examine in a
microscope
Todetermine
the proper
function
of the
kidney
Color-yellow
Transparency-
clear
PH-4.0
Specific
gravity-1.020
Albumin-trace
Sugar-negative
Pus cels-HPF-
2.4
RBC/HPF-2.4
Epithelial
cells-few
A.urates- few
Color-yellow
Transparency
- clear
PH-4.6-8
Specific
gravity-1.003-1.025
Albumin-Sugar-Nil
Pus cells-
RBC-1-
02/lowpower field
1/ highpower field
Epithelialcells, and Aurates can
be found in
the urates ina fewnumber
Color is normal
Transparency
normal
PH- is innormal range
Specificgravity-is innormal range
No sugar foundindicating itsnormal
RBC is slightly
above the
normal range
And it isnormal for theepithelial and A
urates to befound in theurine providingin a fewnumber.
BLOOD TEST
Before
Nurses must help position patients properly, like rolling the patient over, in order to
complete the necessary diagnostic testing.
-
7/27/2019 Cardiomyopathy (Mary)
22/47
22
Check a patient's vital signs (blood pressure, pulse, breathing rate), assess physical
condition and keep an eye on any monitors that the patient needs to remain hooked
up to during the tests, such as a heart monitor or ventilator. Nurses may also be
required to connect or disconnect any monitors or devices that can interfere with the
testing.
During
Draw the sample before giving or one hour after giving I.M. injections. I.M. injections
will increase the total CK level.
Be sure to obtain the blood samples on schedule. Always note on the laboratory slip, the
time the sample was drawn and the hours elapsed since onset of chest pain. Be sure to
draw blood samples in a 7-ml red top tube.
Be sure to handle the sample gently to prevent hemolysis. Always have the sample
transported to the lab promptly because CK activity diminishes significantly after 2 hours
at room temperature.
After the procedure
Apply cotton ball with slight pressure to the site to bleeding.
Test results are reported to the patient's doctor, specialists and others in need of the
information by nurses. Results may be phoned in, faxed or sent electronically via a
computer. It may be the nurse's responsibility to check for the results of the tests as well.
They may be in charge of entering the results into the patient's medical record. Nurses
must also notify the patient's physician when abnormal or critical results that require an
immediate response, such as abnormal blood work with critical potassium levels, are
found.
Diagnostic/labo
ratory
procedure
Date ordered:July 7 ,2012
General
descriptio
n
Indicatio
n or
purpose
Result Normalvalues
Analysis and
interpretatio
n
Blood test Date resultin:July 7, 2012
Blood
chemistryGive
specific
information about
the
condition
of your
organs.
RBS-6.88
BUN-4.0
Createnine-
98.3
CK-MB-8.18
Troponin I-Nil
RBS-3.85-
9.0mmol/l
BUN-1.7-
8.3mmol/l
Createnine-
60-
120mmol/l
CK-MB-0-
RBS is in
normal range
BUN is in
normal range
CREATENIN
E is in normal
range
CK-MB is is
-
7/27/2019 Cardiomyopathy (Mary)
23/47
23
Sodium-141.9
Potassium-
3.45
Hemoglobin-
144
Hematocrit-43
WBC-11.4
Neutrophils-.7
Platelet count-
248
25IV/l
Troponin-
Nil
Sodium-
135-
145mmol/l
Potassium-
3.5-
5.5mmol/l
Hemoglobi
n-125-
175mmol/l
Hematocrit-
0.40-0.52
WBC-5-10x10/l
Neutrophils
-0.45-0.65
Platelet
count-150-
400x10?l
normal range
There is no
troponin I
found
SODIUM is
in normal
range
POTASSIU
M is slightly
low
HEMOGLOB
IN is in
normal range
HEMATOCR
IT is in
normal range
WBC is
slightly
elevated
NEUTROPHI
LS is in
normal range
PLATELET
COUNT is in
normal range
Diagnostic/labo
ratory
procedure
Date ordered:July 7, 2012
General
descriptio
n
Indicatio
n or
purpose
Result Normalvalues
Analysis and
interpretatio
n
Blood test Date resultin:July 7 2012
HEMATOLOGY
To
determine
the total
volume of
blood
HGB-143
WBC-8.8
RBC-5.0
HCT-0.43
HGB-140-
180gm/l
WBC-5-
10x10mo/l
RBC-4.5-
6.3x10/l
HCT-0.40-
0.54L/L
HGB is in
normal range
WBC is in
normal range
RBC is in nor
mal range
HCT is in
normal range
-
7/27/2019 Cardiomyopathy (Mary)
24/47
24
Diagnostic/labo
ratory
procedure
Date ordered:
Date result
in:
General
descriptio
n
Indicatio
n or
purpose
Result Normalvalues
Analysis and
interpretatio
n
Blood test July 7 2012 Chemicalchemistry
To
determine
the proper
functionof the
heart
BUN-2.8
CREATENIN
E-70.8
SODIUM-
143.8
POTASSIUM-
3.55
BUN-2.1-
7.1mmo1/l
CREATENINE-62-106mmol/l
SODIUM-135-148mmol/l
POTASSIUM-3.5-5.3mmol/l
BUN,
CREATENIN
E, SODIUM,
POTASSIUM
are all in
normal
range
IVF
Before
Lean the site with cotton balls with alcohol
During
Make sure to maintain bed rest
Continues cardiac monitoring
Report any abnormal findings to the physicians
Increase the rate of infusion as prescribe, but monitor for fluid overload
No evidence of dehydration should be noticed
Check the IV site for redness, swelling and infiltration
After
Apply cotton balls to the site to prevent bleeding
MEDICAL
MANAGEMENT
Date ordered:
July 7
Date started:July 7
Date
Changed:July 8
GENERAL
DISCRIPTION
INDICATION
PORPOSE
CLIENTS
RESPONSE
1
D5LRS 1LxKVO
D5LRS are fluids
which are intended to
be administeredbecause hypertonic
solution are those thathave an effectiveosmolarity greater thanthe body fluids.
This pulls the fluids
into the vascular by
osmosis resulting in anincrease vascular
volume .It raisesintravascular osmotic
pressure and providesfluid, electrolyte andcalories for energy.
Client maintain fluid
balance despite of
strict monitoring ofI&O
-
7/27/2019 Cardiomyopathy (Mary)
25/47
25
O2 THERAPHY
Before
Instruct the client and visitors about the hazard of smoking with oxygen use.
Make sure that electric devices (such as razors, hearing aids, radios, televisions, and
hearing pads) are in good working order to prevent the occurrence of short-circuit sparks.
Ensure proper delivery method (cannula, face mask, face tent)
Teach client proper use of oxygen
During
Avoids materials that generate static electricity, such as woolen blankets and synthetic
fabrics. Cotton blankets should be used, and client and caregivers should be advised to
wear cotton fabrics.
Regulate flow if necessary
After
Always make sure that the oxygen tank is properly closed
MEDICAL
MANAGEMENT
Date ordered
July 7, 2012
Date started
July 7, 2012
GENERAL
DESCRIPTION
INDICATION
PORPOSE
CLIENTS
RESPONSE
OXYGEN 1-2
liter/min
Oxygen is a
colorless gas that
exists in the air that
all living things
needed in order to
live.
To provide enough
oxygen despite of
difficulty of
breathing
Patient was relieved
experiencing DOB
DRUGS
General nursing responsibilities
Before
Check doctors order
Explain to the patient what the medication is for. During:During
Give the medication on time.
After:
Document the medication done.
-
7/27/2019 Cardiomyopathy (Mary)
26/47
26
CEFTRIAXONE
Before
Read carefully the name cephalosporins have similar sounding and similar spelled
names.
Reconstitute 1 mL of cephalosporin to 5 mL of sterile water.
Determine allergy to the cephalosporin through skin testing.
During
Do no infuse rapidly, it causes pain and irritation
Name of the
drug:
Date ordered:July 7, 2012
Route:
IV infusion
General
action
Indication Clients response to the actual
adverse reactionDate started:July 7, 2012
3rd generation
cephalosporin
antibiotic
Lower
respiratory
infection due
to pneumonia
The client did not manifest any
S&S of infection
Generic
name:Ceftriaxone
sodium
Dosage and
frequency:
1 gm Q12Brand name:Rocephin
Datediscontinued:
July 9, 2012
FUROSEMIDE
Before
Do not confuse Lasix with Lanoxin (a cardiac glycoside)
Asses closely for a sign of vascular thrombosis and embolism.
Take Blood Pressure before administering the medication give IV injection slowly, may
cause pain and irritation.
During
Do not infuse rapidly
After
For rapid diuresis observe for dehydration.
Assess for S and Sx for hyperkalemia.
Let the client change the position from lying to sitting the stand slowly.
Supplement diet with vegetable and fruits that are high in potassium. (ex. Bananas,
peaches and oranges.)
-
7/27/2019 Cardiomyopathy (Mary)
27/47
27
Name of the
drug:
Date ordered:
July 7, 2012Route:
IV bolus
General
action
Indication Clients response to the actual
adverse reaction
Date started:
July 7, 2012
Loop Diuretic Edema There was in increase in urine
output from 45cc in 2 hrs. to
300cc in 5 hrs.Generic
Name:
Furosemide
Dosage and
frequency:
40 mg
Q 6
(12 , 6)Brand
Name:
Lasix
Date
discontinued:
July 8 2012
AMIODARONE HYDROCHLORIDE
Before
Correct potassium and Magnesium
During
Follow recommended dietary guidelines. Avoid or limit salt and fluid as directed. Avoid
grape fruit.
After
Record BP and pulse for providers review. Identify specific levels to hold drugs. HR
-
7/27/2019 Cardiomyopathy (Mary)
28/47
28
LOSARTAN POTASSIUM
Before
Do not confuse Lozaar with Zocor (Antihyperlipidimic) .
Take pulse rate and BP before administering medication.
After
Low fat, low sodium diet and avoid grape fruit.
Do not change position suddenly.
Name of the
drug:
Date
ordered:
July 7, 2012
Route:
Oral
General action Indication Clients response to the
actual adverse reaction
Date started:
July 7, 2012
Date
discontinued:
July 9, 2012
Antihypertensive,
Angiotensin II
receptor blocker
Antihypertensive,
alone or with
combination with
other
antihypertensive
drugs(including
diuretics).
Reduces risk of
stroke in clients
with
hypertension and
left ventricular
hypertrophy.
The patient maintains a
normal blood pressure of
110/70 mmhgGeneric
Name:
Losartan
Potassium
Dosage and
frequency:
50 mg
(8 )Brand
Name:
Lozaar
LEVOFLOXACIN
Before:
Check if patient is able to swallow or in need of NGT.
Prepare the medication and other materials to be used.
Name of the
drug:
Date
ordered:
July 7, 2012
Route:
Oral
General action Indication Clients response to the
actual adverse reaction
Date started:
July 7, 2012
Date
discontinued:
July 9, 2012
Flouroquinolone
Antibiotic
5 day
treatment
regimen for
community
acquired
pneumonia
due to
Streptococcus
Pneumoniae.
The patient prevent further
infectionGeneric
Name:
Levofloxacin
Dosage and
frequency:
Oral
(8 )Brand
Name:
Levaguin,
Quixin
-
7/27/2019 Cardiomyopathy (Mary)
29/47
29
DIGOXIN
Before
Monitor bradycardia/ arrhythmias, count apical rate for atleast one minute. Before
administering.
Have digoxin immune FAB available
After
Monitor for pulse deficit. (It indicates adverse drug reaction.)
For severe toxicity.
Use caution: Digoxin withdrawal may worsen heart failure.
Take at the same time each day.
Do not change brands.
Name of thedrug:
Dateordered:
July 7, 2012
Route:
Oral
Generalaction
Indication Clients response to the actualadverse reaction
Date started:
July 7, 2012
Date
discontinued:
July 9, 2012
Cardiac
Glycoside
Propylaxis
and treatment
of recurrent
paroxysmal
AV junction
rhythm.
The patient maintains a normal
heart rate of 73 bpm
Generic
Name:
Digoxin
Dosage and
frequency:
25 mg
( 8 )
Brand
Name:
Lanoxin
POTASSIUM CHLORIDE
Before
Obtain renal function test, dysfunction leads to hyperkalemia.
Prepare the medication.
During Do not draw or dissolve in the mouth.
Monitor I/O.
After
Report any sign of weakness, fatigue or cardiac arrhythmias, it is a sign of hypokalemia.
Record the medication done.
-
7/27/2019 Cardiomyopathy (Mary)
30/47
30
Monitor input/output
Name of the
drug:
Date
ordered:
July 7. 2012
Route:
Oral
General
action
Indication Clients response to the actual
adverse reaction
Date started:
July 7, 2012
Date
discontinued:
July 9, 2012
Electrolytes
Hypokalemia
with or
without
metabolic
acidosis
following in
increase
urinary
excretion.
The client maintains a normal
level of K of 3.55Generic
Name:
Potassium
Chloride
Dosage and
frequency:
O.D.
(8 )Brand
Name:
Kalium
Durule
CALCIUM GLUCONATEBefore
Do not administer together with other medication
Make sure provider is aware of all the medication prescribed.
Name of the
drug:
Date
ordered:
July 7,2012
Route:
IV
General
action
Indication Clients response to the actual
adverse reaction
Date started:
July7, 2012
Date
discontinued:
July 8, 2012
Calcium salt
Prophylaxis
of
hypocalcemia
during
exchange
transfusion
The client maintains a normal
level calcium in the bloodGeneric
Name:
Ca gluconate
Dosage and
frequency:
1 ampule
STATBrand
Name:
Cal-G
MAGNESIUM SULFATE
Before
Asses for absent patellar reflex,
-
7/27/2019 Cardiomyopathy (Mary)
31/47
31
Date started:
July 7, 2012
Date
discontinue:
July 7, 2012
Miscellaneous,
essential
element for
muscle
contraction,
certain
enzyme, and
nerve
transmission
Replacement
therapy in Mg
deficiency
especially in acute
hypomagnesaemia
accompanied by
signs of tetany
similar to those
seen in
hypocalcemia
The client maintains
normal HRGeneric
Name:
Magnesium
sulfate
Dosage and
frequency:
2 gram
STAT
BrandName:
Epsom salt
ASPIRIN
Before
Have epinephrine available to counter act hypersensitivity occurs
Note history of peptic ulcer or bleeding tendencies
During
Take with full glass of water to prevent lodging in esophagus
After
Inform the patient to report ringing in the ear, difficulty hearing, dizziness or fainting
spells, unusual increase in sweating, severe abdominal pain or mental confusion (this is a
sign of a toxic effect)
Name of the
drug:
Date
ordered:
July 7,2012
Route:
Oral
General
action
Indication Clients response to the
actual adverse reaction
Date started:
July 7, 2012
Date
discontinued:
July 7, 2012
Inhibit
platelet
aggregation
Use for
cardiovascular
disease
Patient prevents platelet
aggregationGeneric
Name:
Acetylsalicylic
Acid
Dosage and
frequency:
80 mg
OD
Brand Name:
Aspirin
DIET
Before
-
7/27/2019 Cardiomyopathy (Mary)
32/47
32
Check the doctors order. Question for any inconsistencies regardingpatients diet and
condition
Explain the importance of diet prescribed
After
Document intake as to amount and provide a separate sheet for fluid and output
Take note of patients response to the diet
ACTIVITY
BED REST
Before
Explain to the patient why it is necessary Inform the patient to wear pressure stocking and explain why it is necessary
During
Always make sure that there is somebody with him to assist his needs
Make sure your patient is changing position at least every two hours as permitted by her
doctor to avoid bed sores that will put her into risk of impaired skin integrity related to
immobility.
Always elevate the bedrails
After
Let the client stand or move in a gradual motion
MEDICAL
MANAGEMENT
Date ordered:
July 7, 2012
GENERAL
DISCRIPTION
INDICATION
PURPOSE
CLIENTS
RESPONSE
TYPE OF DIET GENERAL
DESCRIPTION
INDICATION/PURPOSE SPECIFIC FOOD
TAKEN
LFLS Low fat and low sodium
diet
To prevent the further
accumulation of
atherosclerotic plaque that
will contribute to increase
workload of the heart.
pineapple
Soft diet Fluid or soft food To prevent constipation
that may stimulate the
vagus nerve and lead to
heart failure.
Water, arozcaldo
-
7/27/2019 Cardiomyopathy (Mary)
33/47
33
Bed Rest
Date started:
STAT
A medical treatment
involving a period of
consistent (day and
night) recumbence in
bed and
Reducing activities.
Prevent any
restraints that can
cause easy
fatigability and
further problem to
the heart
The patient was
cooperative and
reduces the feeling
of easy
fatigability.
DAILY PATIENTS RECORD/EVALUATION
Days Admission-Day 1(July 7,
2012)
Day 2(July 8, 2012)
Nursing problems Cough, easy fatigability Easy fatigability
Vital signs BP-110/70, RR-17, PR-78,
Temp-36
BP-110/70, RR-24, PR-53,
Apical-78, Temp-36.2
laboratory Hematology, chemical
chemistry, urinalysis, blood
chemistry, electrolytes
None
IVF, O2 D5LRS 10 gtts (KVO) O2-2
LPM
#2 D5LRS D5LRS 10 gtts
(KVO) O2-2 LPM
Drugs Ceftriaxone 1 gm q12,furosemide 40 mg IV q6,
MgSO4 2 gm IV STAT, Ca
gluconate 1 amp IV STAT,amiodarone 200 mg OD,
Losartan 50 mg 1 tab OD,
Lanoxin 25 mg 1/2 tab OD,
levofloxacin 500 mg 1 tabOD, kalium durule 1 tab BID,
aspirin 80 mg 1 tab OD
Levofloxacin500 mg 1 tabOD, , lanoxin25 mg 1/2 tab
OD, kalium durule,
furosemide 40 mg IV q6,ceftriaxone1 gm q12,,
losartan50 mg 1 tab OD,
Kalium durule1 tab BID ,
amniodarone 200 mg OD
Diet NPO LFLS
Activity Bed rest Bed rest
http://en.wikipedia.org/wiki/Medicinehttp://en.wikipedia.org/wiki/Medicine -
7/27/2019 Cardiomyopathy (Mary)
34/47
34
DISCHARGE PLANNING
Strategy Objective Content Time frame Resources
Deep
breathing
exercises
To improve
the lung
capacity thusdecreases the
workload of
the heart
Deep Breathing Exercises
Deep breathing is a
relaxation technique that can
be self-taught. Deepbreathing releases tension
from the body and clear the
mind, improving bothphysical and mentalwellness.
We tend to breathe
shallowly or even hold ourhold our breath when we are
feeling anxious. Sometimeswe are not even aware of it.
Shallow breathing limits
your oxygen intake and addsfurther stress to your body,
creating a vicious cycle.
Breathing exercises can
break this cycle
How to do Deep BreathingExercises:
1.Sit up straight. (Do notarch your back) First exhale
completely through your
mouth.
2.Place your hands on your
stomach, just above your
waist.
2.Breathe in slowly through
your nose, pushing yourhands out with your
stomach. This ensures that
you are breathing deeply.
3.Imagine that you are
Every time
necessary
Teaching and
demonstration
-
7/27/2019 Cardiomyopathy (Mary)
35/47
35
filling your body with air
from the bottom up.
4.Hold your breath to acount of two to five, or
whatever you can handle. Itis easier to hold your breath
if you continue to hold outyour stomach.
5.Slowly and steadilybreathe out through your
mouth, feeling your hands
move back in as you slowly
contract your stomach, untilmost of the air is out.
Exhalation is a little longerthan inhalation.
6.After you get someexperience you dont need to
use your hands to check
your breathing.
You can also do the above
breathing exercise lying on
your back. Deep breathing
exercises can help you torelax before you go to sleep
for the night, or fall backasleep if you awaken in the
middle of the night.
You can also practice deep
breathing exercises standing
e.g. while sitting in traffic,
or standing in a lineup at thegrocery store. If you are
really tense and feel as if
you are holding your breath,
simply concentrate onslowly breathing in and out.
-
7/27/2019 Cardiomyopathy (Mary)
36/47
36
Strategy Objective Content Time
frame
Resources
Early
Ambulation
To improve
cardiacmuscles and
improve its
function
Safety tips for Stair Climbing
Safety and effective climbingshould be your goal for stair
climbing. The following safety
tips can help you start an
effective stair climbing regime:
Keep people informedabout stair climbing
whether at office orhome.
Always carry water orfluids with you.
Be aware of your knee
alignment as it can causea knee or ankle sprain.
Inspect the stairs before
climbing them as an
exercise.
Watch out for opening
doors at the end of thestairway.
What is the Ideal Way to
Start Stair Climbing?
Any aerobic exercise should be
started very slowly and
gradually. The ideal form of
any exercise or stair climbing
should take care of the
following:
1. 5-15 minutes of warm up
exercises are absolutely
Once a day Health teaching
http://en.wikipedia.org/wiki/Theory_of_Formshttp://en.wikipedia.org/wiki/Theory_of_Forms -
7/27/2019 Cardiomyopathy (Mary)
37/47
37
essential for starting
anyworkout session
2. Start climbing with gradual
slow steps.
3. You can alternate
between quicker and low step
routines andslower and deep
step routines.
4. Finally, relax and
cool yourself down.
Control the intensity of your
exercise and do not over-exert
yourself in your first and initial
attempt. Set a goal for yourself
like increasing the pace by
one flight of stair per week
Strategy Objective Content Time frame Resources
Low fat
Lowsodium Diet
To avoid the
formation ofatherosclerotic
plaque
By following such diet, the
risk of heart disease,
gallbladder disease,
diabetes, and even some
forms of cancer is greatly
reduced. It is also a great
way to lose weight.
Throughout
the day
Health
teachings
http://www.everydayhealth.com/fitness/basics/difference-between-exercise-and-physical-activity.aspxhttp://www.everydayhealth.com/fitness/basics/difference-between-exercise-and-physical-activity.aspx -
7/27/2019 Cardiomyopathy (Mary)
38/47
38
Example of a low fat low
sodium diet
Breakfast-scramble egg,
diced mushroom and red
and green peppers, oatmeal
with a sliced banana
Lunch- fresh fruits and
vegetables salad with baked
fish or chicken on top
Dinner- boiled fresh
vegetables
All you need is 30 minutes of
moderate-level physical
activity on most days of the
week. Examples of such
activities are brisk walking,
bicycling, raking leaves, and
gardening.
Strategy Objective Content Time frame Resources
Moderate
active ROMexercise
To prevent
sudden onsetof rapid
heartbeat
.Range-of-
motionexercise
enhance
muscleflexibility.
All you need is 20-30 minutes
of moderate-level physical
activity on most days of the
week.
Examples of such activities are
1.Chin to chest
2. Head turns
3. Head tilts
4. Shoulder movement, up and
30 minutes
everyday
Health
teachings
-
7/27/2019 Cardiomyopathy (Mary)
39/47
39
down
5. Shoulder rotation
6. Elbow bends up and down
7. Elbow bends side to side
8. Wrist rotation
9. Palm up, palm down
10. Finger bends
11. Finger spread
12. Hip and knee bend
13. Leg movement side to side
14. Leg rotation
15. Knee rotation
16. Ankle and toe bends
17. Ankle and toe rotation
-
7/27/2019 Cardiomyopathy (Mary)
40/47
40
NURSING CARE PLAN
EXCESS FLUID VOLUME
-
7/27/2019 Cardiomyopathy (Mary)
41/47
41
INEFFECTIVE BREATHING PATTERN
-
7/27/2019 Cardiomyopathy (Mary)
42/47
42
ACTIVITY INTOLERANCE
-
7/27/2019 Cardiomyopathy (Mary)
43/47
43
ACTIVITY INTOLERANCE
SUMMARY
Some people who have cardiomyopathy have no signs or symptoms and need notreatment. For other people, the disease develops quickly, symptoms are severe, and serious
complications occur.
Treatments for cardiomyopathy include lifestyle changes, medicines, surgery, implanted
devices to correct arrhythmias, and a nonsurgical procedure. These treatments can controlsymptoms, reduce complications, and stop the disease from getting worse
Cardiomyopathy is a common disease affecting more than 1 million people around theworld. There are so many contributing factors that trigger the onset of this cardiac disease. Based
on our patient some of these factors are (age, family history, gender, and history of smoking). It
is hard to predict if the person is when he/she is going to acquire the disease. Easy fatigability
-
7/27/2019 Cardiomyopathy (Mary)
44/47
44
and cough was the symptom why the patient admits himself in the hospital for he perceives that
it was a life threatening situation for her. Diagnostics was required to determine the exact
problem and the treatment is consists of combination of medication in order for his heart tofunction on is normal. But this is not enough there should be a strict and continuous monitoring
of the patient status in order for the patient to recover faster.
RECOMMENDATION
Patient with or without a family history of cardiac disease (cardiomyopathy) should be
very cautious in terms of life style and should avoid the triggering factors that will cause thisdisease to emerge. All people is risk to having different kind of diseases how much more of those
who have a history. Therefore we recommend that everyone should be concern and be
knowledgeable about things that are needed to do. As a student nurses it is our responsibility to
enforce teachings that will maintain or at least prevent the occurrence of problem and thus it willhelp create a healthy community.
LEARNING DERIVED
Policarpio, Jeffrey S.ICU is the second rotation I had since starting my clinical duty. Compared to delivery
room, ICU is more in depth when it comes to giving patient care. Due to the time spent withpatient, I was able to develop other nursing care skills. I was able to practice my skills with
compassion due to prolonged time spent with patient.
Nursing is not just giving treatment; it is how you give care. As early as now, I am
learning to incorporate compassion with my chosen profession.
Familiarizing myself with patients chart, drug administration and utilizing differenthospital machines such as mechanical ventilator, ECG and atrial defibrillator, provided me with
understanding of nursing practice in a whole new level. With this rotation, I had gained more
awareness with the practice of infection control not just for me but especially for the patient.Patients in ICU had to deal not just with their major diagnosis but also complications. In line
with this, practicing good handwashing, masking and maintaining cleanliness, is my way of
showing I care. In my mind, if I dont practice infection control, this will expose my patients tomore medical problems mainly that their immune system is already compromised.
Delivery room is a fast paced environment. In ICU, it gives me more time to know not
just my patients medical problems but my patient as a person as well. My patients need me anddepend on me with their needs, thus, I need to show that they can count on me just to relieve
them a little bit of what they are going through. Moreover, in ICU, I need to give individualized
care which gave me the opportunity to learn more about different nursing interventions.
Critical thinking is always a part of nursing practice. My ICU experience gave me the
opportunity to practice this skill, taking into consideration the welfare of my patient, thus
showing that nurses are not just mechanical workers that move in a routine manner.Nevertheless, nurses move with precise interventions and with compassion.
-
7/27/2019 Cardiomyopathy (Mary)
45/47
45
It will always be in my mind that in my chosen career, I deal with human beings. These
human beings, sometimes needs machines to survive in ICU, but it will make a big difference ifa nurse incorporates love when using those machines with them. And for sure, the patient will
know the difference of a nurse who provides interventions just for the heck of it and a nurse who
moves with passion and care.
ROWENA P. LIGON
Being in the ICU is a challenging experience a student nurse will acquire. Having an
actual patient is very crucial part in the studies of a student nurse. This is the time of realization
that life of a person is at risk if the person that will handle that patient is not equipped with
knowledge on how to handle a patient.
Knowing the Patient that as a student nurse will provide an assessment in the ICU is a
very important step. The student nurse should know to protect the privacy and the integrity of
the patient assigned to him/her. The student nurse will not only base his/her analysis from the
questions and assessment being conduct to his assigned patient, but rather to gather all the
necessary data from other sources like the laboratory results, genogram that will support to have
accurate case study.
IRISH SANTOS
Data collection, assessment taken, is where everything must start, because if a student
nurse fail to determine the needs of the patient, there will be a failure to the speedy recovery of
his Patient. Communicating skills is also a very crucial stage of assessment for a student nurse to
be able to gain their trust you must establish rapport.
Health teaching is very necessary due to lack of knowledge to some patient. Teaching them
the importance of seeking immediate help when they feel that something is wrong to them, in
order to treat the problem immediately. We have to be cautious enough about our health to livelonger and be with our love ones.
Like the famous saying: Health is wealth. Being free from disease is to live a healthy
lifestyle. It is up to the person how they will utilize the resources around them.
-
7/27/2019 Cardiomyopathy (Mary)
46/47
46
MARY LEZ D. PERRY
Though it was my first time to be assign in the ICU I learned so many things that a
student nurse should know. Some of it was very unfamiliar to me, like the negatoscope, the
solucet, and it was my first time to observed somebody doing a sunctioning. I was able to
understand how ECG is being apply to the chest. I was I able to understand what the lines meanin the ECG result. It was my first time to administer lantus to a patient. It was a very nice
experience taking care of the patient. I was able to observe what could be a patient would ned in
the situation where in nobody want to be.
MARK OLIE B. LAYAG
Being in ICU, the first thing that comes in my mind are those patients who are in critical
condition. Having an actual patient is very crucial part in the studies of a student nurse. . I felt
very nervous because I dont know what I will expect in ICU and what are the things should be
done.
You are going to analyze an ethical conflict and come up with a course of action that is
morally defensible and medically reasonable. And assist patients and their families at time of
critical illness with respect, concern for their dignity, and careful attention to pain control and
suffering.
The most I learned is to how to prioritize the needs of the patients. On how to be attentiveon monitoring because we know that these patients need to be closely monitored because of their
situation.
-
7/27/2019 Cardiomyopathy (Mary)
47/47
47
REFERENCES
MEDICAL SURGICAL (CONCEPTS AND CLINICAL APPLICATION) 2ND
EDITION
2009JOSIE QUIAMBAO UDAN
NURSES POCKET GUIDE (DIAGNOSES INTERVENTIONS AND RATIONALES
MARILYN E. DOENGES, MARY FRANCES MOORHOUSE, ALICE C. MURR
POCKET NURSES DICTIONARYBY GUPTA
CONTEMPORARY MEDICAL-SURGICAL NURSING VOLUME 1
RICK DANIELS, LAURA NOSEK, LESLIE NICOLL
DELMARS NURSES DRUG HANDBOOK 2010 EDITION
GEORGE r. SPRATTO, ADRIANNE l. WOODS
NURSES HANDBOOK OF HEALTH ASSESSMENT SIXTH EDITION
WILLIAM &LIPPINCOT
INTRODUCTION TO THE HUMAN ANATOMY 7TH
EDITION
TORTORA & DERRICKSON