Liver, Biliary Tree, and Gallbladder
52
Chapter 27 Liver, Biliary Tree, and Gallbladder William E. Brant LIVER Imaging Methods CT, MR, and US all produce high-quality images of the liver parenchyma. Dynamic bolus contrast–enhanced multidetector CT (MDCT) is the current method of choice for most hepatic imaging. Fast imaging techniques that control motion have increased the role of MR as a problem solver and often as the primary hepatic imaging modality. MR is preferred whenever iodinated contrast cannot be used. US is used as a screening method for patients with abdominal symptoms and suspected diffuse or focal liver disease. Color flow and spectral Doppler are used to assess hepatic vessels and tumor vascularity. Radionuclide imaging is used in the characterization of cavernous hemangiomas and focal nodular hyperplasia. MDCT of the liver is performed using a three- or four-phase protocol of multiple scans of the entire liver. Initial noncontrast images are followed by rapid bolus IV contrast injection by a mechanical injector. Immediate images are optimally obtained during the peak arterial enhancement phase to detect hypervascular tumors and other lesions supplied primarily by the hepatic artery. Arterial-phase-enhancing lesions, like hepatocellular carcinoma (HCC), are high attenuation on a background of lower-attenuation, minimally enhanced parenchyma. Maximum enhancement of the liver is attained during the portal venous phase to demonstrate hypovascular lesions as low-attenuating masses on a background of brightly enhanced parenchyma. Delayed images are obtained several minutes after contrast injection to document late contrast fill-in of hemangioma and delayed enhancement of cholangiocarcinoma. Hepatic MR is performed with a broad array of fast spin-echo, breath-hold gradient recall, short-time inversion-recovery, fat-suppressed, or in-phase/out-of-phase pulse sequences. The goal is to maximize lesion detection by the striking contrast resolution of MR while minimizing motion artifact by rapid-scan breath-hold sequences. Dynamic contrast enhancement is achieved with MR by repeating full liver scans multiple times in the first minutes following gadolinium injection. US is used as a rapid screening modality to detect diseases of the gallbladder, biliary tree, and liver. Hepatic US imaging is reviewed in Chapter 36. Radionuclide imaging of the liver is inferior to CT and MR for lesion detection but offers functional information in characterizing lesions, such as focal nodular hyperplasia. Radionuclide blood pool imaging is very useful for definitive diagnosis of cavernous hemangioma. Hepatic radionuclide imaging is reviewed in Section XII. Fine-needle aspiration for cytology and core needle biopsy for histology, guided by US or CT, are popular and safe methods to obtain tissue diagnoses. Anatomy Couinaud Segments The vascular anatomy that defines the surgical approach to lesion resection is the anatomy most relevant to
-
Upload
sergiu-busuioc -
Category
Documents
-
view
993 -
download
3
Transcript of Liver, Biliary Tree, and Gallbladder

Chapter 27Liver, Biliary Tree, and Gallbladder
William E. Brant
LIVER
Imaging MethodsCT, MR, and US all produce high-quality images of the liver parenchyma. Dynamic bolus contrast–enhancedmultidetector CT (MDCT) is the current method of choice for most hepatic imaging. Fast imaging techniquesthat control motion have increased the role of MR as a problem solver and often as the primary hepaticimaging modality. MR is preferred whenever iodinated contrast cannot be used. US is used as a screeningmethod for patients with abdominal symptoms and suspected diffuse or focal liver disease. Color flow andspectral Doppler are used to assess hepatic vessels and tumor vascularity. Radionuclide imaging is used inthe characterization of cavernous hemangiomas and focal nodular hyperplasia.
MDCT of the liver is performed using a three- or four-phase protocol of multiple scans of the entire liver.Initial noncontrast images are followed by rapid bolus IV contrast injection by a mechanical injector.Immediate images are optimally obtained during the peak arterial enhancement phase to detecthypervascular tumors and other lesions supplied primarily by the hepatic artery. Arterial-phase-enhancinglesions, like hepatocellular carcinoma (HCC), are high attenuation on a background of lower-attenuation,minimally enhanced parenchyma. Maximum enhancement of the liver is attained during the portal venousphase to demonstrate hypovascular lesions as low-attenuating masses on a background of brightly enhancedparenchyma. Delayed images are obtained several minutes after contrast injection to document late contrastfill-in of hemangioma and delayed enhancement of cholangiocarcinoma.
Hepatic MR is performed with a broad array of fast spin-echo, breath-hold gradient recall, short-timeinversion-recovery, fat-suppressed, or in-phase/out-of-phase pulse sequences. The goal is to maximizelesion detection by the striking contrast resolution of MR while minimizing motion artifact by rapid-scanbreath-hold sequences. Dynamic contrast enhancement is achieved with MR by repeating full liver scansmultiple times in the first minutes following gadolinium injection.
US is used as a rapid screening modality to detect diseases of the gallbladder, biliary tree, and liver. HepaticUS imaging is reviewed in Chapter 36.
Radionuclide imaging of the liver is inferior to CT and MR for lesion detection but offers functional informationin characterizing lesions, such as focal nodular hyperplasia. Radionuclide blood pool imaging is very usefulfor definitive diagnosis of cavernous hemangioma. Hepatic radionuclide imaging is reviewed in Section XII.
Fine-needle aspiration for cytology and core needle biopsy for histology, guided by US or CT, are popularand safe methods to obtain tissue diagnoses.
Anatomy
Couinaud SegmentsThe vascular anatomy that defines the surgical approach to lesion resection is the anatomy most relevant to

P.757liver imaging. A numbering system
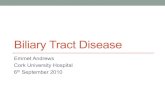
developed by Couinaud (pronounced “kwee-NO”) is commonly used internationally and providesstandardized identification of hepatic segments (Fig. 27.1) (Table 27.1). The eight Couinaud segments haveseparate vascular inflow, outflow, and biliary drainage and can each be resected without damaging theremaining segments. Division of the liver into eight segments is based on a concept of three longitudinalplanes and two transverse planes. A longitudinal plane through the middle hepatic vein, inferior vena cava(IVC), and gallbladder fossa divides the liver into right and left lobes. A longitudinal plane through the righthepatic vein divides the right lobe into anterior (VIII and V) and posterior (VII and VI) segments. Alongitudinal plane through the left hepatic vein divides the left lobe into medial (IVa and IVb) and lateral (IIand III) segments. A transverse plane through the left portal vein divides the left lobe into superior (IVa andII) and inferior (IVb and III) segments. An oblique transverse plane through the right portal vein divides theright lobe into superior (VIII and VII) and inferior (V and VI) segments. Segment I is the caudate lobe, whichextends between the fissure of the ligamentum venosum and the IVC. Hepatic venous drainage from thecaudate lobe is directly into the IVC via small veins.
FIGURE 27.1. Couinaud Liver Segments. A. Superior portion of the liver. B.Inferior portion of the liver. CT scans illustrate the Couinaud classification ofnumbering of liver segments. The longitudinal plane of the right hepatic vein dividesVIII from VII in the superior portion of the liver and V from VI in the inferior portion ofthe liver. The longitudinal plane of the middle hepatic vein through the gallbladderfossa separates IVa from VIII in the superior liver and IVb from V in the inferior liver.The longitudinal plane of the left hepatic vein and fissure of the ligamentum teresseparates IVa from II in the superior liver and IVb from III in the inferior liver. Theaxial plane of the left portal vein separates IVa superiorly from IVb inferiorly and IIsuperiorly from III inferiorly in the left lobe. The axial plane of the right portal veinseparates VIII and VII superiorly from V and VI inferiorly in the right lobe. Thecaudate lobe (segment I) extends between the fissure of the ligamentum venosumanteriorly and the inferior vena cava posteriorly.

P.758
Blood supply to the liver is approximately two thirds via the portal vein and one third via the hepatic artery.
When IV contrast is administered as a bolus during rapid CT scanning, the maximum liver parenchymalenhancement will be delayed 1 to 2 minutes following initiation of injection. This delay reflects the transit timeof contrast agent through the GI tract and spleen before accessing the liver through the portal vein. Tumors,which are supplied primarily by the hepatic artery, will enhance maximally during the early hepatic arterialphase, while the liver parenchyma enhances maximally during the portal venous phase.
TABLE 27.1 American and International Nomenclature for AnatomicSegments of the Liver
American International Number
Caudate lobe Caudate lobe I
Left lobe
Lateral segment Left lateral superior subsegment II
Medial segment Left lateral inferior subsegment III
Left medial subsegment IVa
IVb
Right lobe
Anterior segment Right anterior inferior subsegment V
Posterior segment Right anterior superior subsegment VIII
Right posterior inferior subsegment VI
Right posterior superior subsegment VII
Adapted from Dodd GD. An American's guide to Couinaud's numberingsystem. AJR Am J Roentgenol 1993;161:574-575.

Perfusion abnormalities are seen on post–IV contrast CT and MR because of variations in hepatic arterialand portal venous blood supply to various areas of the liver (1,2). This dual blood supply has acompensatory relationship: arterial flow increases when portal venous flow decreases. Transientenhancement differences are seen during either arterial phase imaging or portal venous phase imaging onMDCT and dynamic MR. Portal venous flow may be altered by: (1) portal blockade by tumor or thrombus; (2)extrinsic compression caused by ribs or diaphragmatic slips, or by tumors on the liver capsule; or (3) “thirdinflow” from systemic veins in the pericholecystic, parabiliary, and epigastric-paraumbilical venous systems(Fig. 27.2). Hepatic arterial flow may be increased by: (1) focal hypervascular lesions; (2) inflammation ofadjacent organs (cholecystitis, pancreatitis); or (3) aberrant hepatic arterial supply. Regional differences inblood supply related to these factors explain patterns of enhancement abnormalities as well as alteredpatterns of diffuse liver disease, such as focal fatty deposition and focal fatty sparing in diffuse fattyinfiltration.
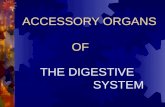
FIGURE 27.2. Perfusion Defect. A common perfusion defect (white arrow)is seen in segment IVb adjacent to the fissure of the ligamentum teres (blackarrowhead). This perfusion defect is related to “third inflow” fromparaumbilical systemic veins. Focal fatty infiltration is commonly seen in thislocation. Importantly, this normal variant must not be mistaken for aneoplasm.
On CT, the density of normal liver parenchyma is equal to or greater than the density of normal spleenparenchyma on unenhanced images. Following bolus IV contrast administration, the normal parenchymalenhancement is less than that of the spleen during the arterial phase and equal to or greater than that of the

P.759
spleen during the portal venous phase.
On T1WI MR, the normal liver is of slightly higher signal intensity than the spleen, and most focal lesionsappear as lower-intensity defects. On T2WIs, the normal liver is less than or equal to the spleen in signalstrength, and most lesions appear as high-intensity foci.
Diffuse Liver Disease
HepatomegalyEnlargement of the liver is usually judged subjectively, based on imaging studies. Rounding of the inferiorborder of the liver and extension of the right lobe of the liver inferior to the lower pole of the right kidney areevidence of hepatomegaly. A liver length of greater than 15.5 cm, measured in the midclavicular line, isconsidered enlarged. A Reidel lobe is a normal variant of hepatic shape found most often in women. It refersto an elongated inferior tip of the right lobe of the liver. When a Reidel lobe is present, the left lobe of the liveris correspondingly smaller in size. The left lobe of the liver may, as a normal variant, be elongated andsurround a portion of the spleen. Causes of hepatomegaly are listed in Table 27.2.
Fatty infiltration is a common and nonspecific response of hepatocytes to injury and toxins. Hepatocytesbecome filled with cholesterol and triglycerides. Causes include alcoholism, obesity, malnutrition,hyperalimentation, steroid therapy, diabetes mellitus, pancreatitis, glycogen storage disease, andchemotherapy. Imaging is the best diagnostic method to document the condition, since laboratory evaluationmay be normal.
On CT, fat infiltration lowers the attenuation of the hepatic parenchyma and makes the liver appear lessdense than the spleen (Fig. 27.3). Differences in density between liver and spleen are most reliably judgedon noncontrast images. On postcontrast images, the spleen enhances maximally 1 to 2 minutes beforemaximal liver enhancement and is thus transiently brighter than the normal liver. Fatty-infiltrated liversenhance less than normal livers. On US, the liver parenchyma is increased in echogenicity in areas of fatinfiltration. The echogenicity of the fatty liver is significantly greater than the echogenicity of the normal kidneyparenchyma. This density difference (fat is bright on US and dark on CT) has been called the “flip-flop sign.”Conventional spin-echo MR images show no significant abnormalities with fat infiltration. Gradient-echoimaging with fat and water molecules in-phase and out-of-phase
is the MR method most sensitive to fatty infiltration. On in-phase images, the signal from water and fatmolecules are additive. On out-of-phase images, the signals from water and fat cancel out each other. A lossof signal intensity between in-phase and out-of-phase images is indicative of fatty infiltration (Fig. 27.4). Thisis the same technique used to characterize benign adrenal adenomas (see Chapter 33).
TABLE 27.2 Causes of Hepatomegaly
Vascular Congestion Congestive heart failure Hepatic vein thrombosisMetabolic/diffuse infiltration Fatty infiltration Alcohol Drugs/chemotherapy Hepatic toxins

Gaucher disease and lipidoses Carbohydrate Glycogen storage diseases Diabetes mellitus Iron Hemochromatosis Amyloid AmyloidosisTumor/cellular infiltrate Diffuse metastases Diffuse hepatocellular carcinoma Lymphoma Extramedullary hematopoiesis Systemic mastocytosisCysts Polycystic diseaseInflammation/infection Hepatitis Sarcoidosis Tuberculosis Malaria
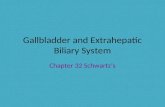
FIGURE 27.3. Diffuse Fatty Infiltration Seen on CT. CT reveals the densityof the enhanced liver parenchyma (L) to be significantly less than the densityof the enhanced splenic parenchyma (S). Portal (p) and hepatic (h) veins runtheir normal courses without displacement or distortion. V, inferior vena cava;Ao, aorta.

P.760
Characteristic features of fatty infiltration include lack of mass effect (no bulging of the liver contour ordisplacement of intrahepatic blood vessels) and angulated geometric boundaries between involved anduninvolved parenchyma. Areas of fat infiltration may be multifocal, with interdigitating fingers of normal andabnormal parenchyma. Fatty changes can develop within 3 weeks of hepatocyte insult and may resolvewithin 6 days of
removing the insult. Patterns of fatty infiltration are strongly related to hepatic blood flow.
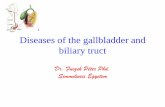
FIGURE 27.4. Diffuse Fatty Infiltration Seen on MR. A. In-phase gradient-recallMR. B. Out-of-phase gradient recall MR. The out-of-phase image shows distinctloss of signal (darkening) of the entire liver parenchyma compared to the in-phaseimage. The out-of-phase MR image is easily recognized by the black linesurrounding soft tissue structures at the interface with abdominal fat.
Diffuse fatty infiltration involving the entire liver is the most common pattern. However, the degree of fatinfiltration is commonly not uniform throughout the liver.
Focal fatty infiltration involves a geographic or fan-shaped portion of the liver with the same imaging featuresas diffuse infiltration. Vessels run their normal course through the area of involvement. Focal fatty infiltrationmay simulate a liver tumor; however, the area of involvement has a density characteristic of fat. Focal fattyinfiltration is most common adjacent to the falciform ligament, gallbladder, and porta hepatis.
Focal sparing in a diffusely fatty-infiltrated liver may be the most confusing pattern, because spared areas ofnormal parenchyma may simulate a liver tumor (Fig. 27.5). The fat-spared area is most commonly located insegment IV. The fat-spared area is hypoechoic relative to the rest of the liver on US and is of higher densitythan the rest of the liver on CT. The remainder of the liver demonstrates features characteristic of diffusefatty infiltration.
Nonalcoholic steatohepatitis (NASH) describes fatty liver caused by an inflammatory response that is notcaused by excessive alcohol intake. NASH is related to obesity, type 2 diabetes, hyperlipidemia, andanorexia nervosa. It is a rare cause of acute fulminant hepatic failure and may progress to cirrhosis.Histology shows steatosis with parenchymal inflammation and fibrosis. Imaging features are those of diffuse

P.761
fatty liver.
FIGURE 27.5. Fatty Infiltration With Focal Sparing. A. US image demonstrates afocal hypoechoic area of normal liver (NL) near the portal vein (p) in a liver (FL) thatis diffusely increased in echogenicity because of fatty infiltration. B. CT imageobtained without contrast enhancement demonstrates the spared area of normalliver (arrow) to be high density compared to the lower density of the fatty replacedliver (FL). Note the characteristic “flip-flop” appearance of fat density between CTand US. S, spleen.
Acute hepatitis most commonly causes no abnormalities on hepatic imaging. In some patients, diffuseedema lowers the parenchyma echogenicity and causes the portal venules to appear unusually bright on US(3). In acute fulminant hepatitis, areas of necrosis show as ill-defined areas of low density on CT.
Chronic hepatitis is characterized pathologically by portal and perilobular inflammation and fibrosis. Imagingstudies are insensitive to early pathologic changes. Fatty changes are minimal and the liver is usually notenlarged. Perihepatic lymph nodes are commonly visualized. US may show a subtle coarse increase inhepatic echogenicity. The primary role of imaging patients with chronic hepatitis is to detect hepatocellularcarcinoma.
Cirrhosis is characterized pathologically by diffuse parenchymal destruction, fibrosis with alteration ofhepatic architecture, and innumerable regenerative nodules that replace normal liver parenchyma. Causes ofcirrhosis include hepatic toxins (alcohol, drugs); infection (viral hepatitis, especially types B and C); biliaryobstruction; and heredity (Wilson disease). In the United States, 75% of patients with cirrhosis are chronicalcoholics. In Asia
and Africa, most cases of cirrhosis are caused by chronic active hepatitis. A variety of morphologicalterations are seen on imaging studies (Fig. 27.6) (4,5). These include: (1) hepatomegaly (early), (2) hepaticatrophy (late), (3) coarsening of hepatic parenchymal texture, (4) irregularity (nodularity) of the liver surface,

(5) hypertrophy of the caudate lobe with shrinkage of the right lobe, and (6) regenerating nodules.Extrahepatic signs of cirrhosis include evidence of portal hypertension, splenomegaly, and ascites. Thepathologic changes of cirrhosis are irreversible, but disease progression can be limited or stopped byeliminating the causative agent (stop drinking alcohol). Transjugular intrahepatic portosystemic shunts (TIPS)are effective treatment for portal hypertension and long-term control of esophageal variceal bleeding. Livertransplantation is now established as effective treatment for end-stage liver disease.
FIGURE 27.6. Cirrhosis and Portal Hypertension. A CT scan revealsatrophy of the liver (L) with diffuse nodularity of its surface (open arrows) andsplenomegaly (S). Numerous enhancing portosystemic collateral vessels areevident, including perihepatic (long black arrows), gastrohepatic(arrowheads), and gastric varices (short arrow). A dilated periumbilical vein(white arrow) is seen coursing out of the fissure of the ligamentum teres intothe falciform ligament. Ascites (a) is also evident. St, stomach; V, inferiorvena cava; A, aorta.
US demonstrates heterogeneous parenchyma with coarsening of the echotexture and decreasedvisualization of small portal triad structures. High-frequency detailed scanning of the liver surface reveals finenodules. CT may be normal in the early stages, or it may reveal parenchymal inhomogeneity with patchyareas of increased and decreased attenuation (6). Fine or coarse nodularity of the liver surface ischaracteristic. Areas of fatty replacement may be evident. MR shows heterogeneous parenchymal signal onT1WIs and T2WIs. High-signal fibrosis on T2WIs is the predominant cause of the heterogeneousappearance.
TABLE 27.3 Causes of Nodules in a Cirrhotic Liver

P.762
Regenerative nodules (nodules <10 mm)Adenomatous hyperplastic nodules (nodules >10 mm)Hepatocellular carcinomaConfluent fibrosisFocal fat infiltrationFocal fat sparingMetastases
Nodules in CirrhosisNodules are a constant feature of cirrhosis (Table 27.3), and the challenge is to differentiate the ubiquitousbenign nodule from HCC (7). The most common nodules are regenerative nodules (Fig. 27.7), which are aroutine pathologic feature of cirrhosis caused by the body's attempted repair of hepatocyte injury.Regenerative nodules are composed primarily of hepatocytes that are surrounded by coarse fibrousseptations. They have the same imaging characteristics as hepatic parenchyma but stand out as nodulesbecause of their surrounding fibrous bands. Regenerative nodules are 3 to 10 mm in size. Smallregenerative nodules cause the micronodular pattern of alcoholic cirrhosis. On CT, most regenerativenodules are isointense with parenchyma and are not detected. Iron deposits in regenerating nodules(siderotic nodules) will cause a slight increase in CT attenuation, causing them to appear slightlyhyperintense. Regenerative nodules may be hypointense, isointense, or hyperintense on T1WIs, but they donot show the early arterial enhancement post–gadolinium administration that is typical of HCC. On T2WIs,regenerative nodules are hypointense (siderotic nodules) or isointense but are not
hyperintense, providing differentiation from most liver metastases and from dysplastic nodules. Dysplasticnodules (adenomatous hyperplastic nodules) are proliferative precancerous lesions found in 15% to 25% ofcirrhotic livers. On CT and US, adenomatous hyperplastic nodules resemble regenerative nodules but arelarger than 10 mm in diameter. On MR, non–iron-containing adenomatous hyperplastic nodules arehyperintense on T1WIs and hypointense to isointense on T2WIs. High signal on a T2WI is indicative of foci ofcellular atypia or malignancy. Small HCCs are variable in signal on both T1WIs and T2WIs. The mostcharacteristic MR appearance of small HCCs is hyperintense on T1WIs and moderately hypointense onT2WIs, with homogeneous early arterial phase enhancement with rapid washout postcontrast (see Fig.27.17). Rapid growth is characteristic. Lesions >3 cm usually have a distinct capsule. On CT, small HCCsappear as low-density, encapsulated masses that enhance rapidly and quickly become hypodense with boluscontrast dynamic scanning. Ringlike enhancement of the tumor capsule is characteristic.

FIGURE 27.7. Regenerative Nodules in Cirrhosis. CT image filmed at anarrow window shows innumerable low-density small nodules evidentthroughout the liver in this patient with cirrhosis. Needle biopsy confirmedbenign regenerative nodules.
Confluent fibrosis describes the masslike areas of fibrosis found in livers with advanced cirrhosis. Extensivefibrosis produces wedge-shaped or radiating bandlike masses that are hypodense on noncontrast CT andmay become hyperdense post–contrast administration. Volume loss of the affected portion of the liver is akey feature. A whole hepatic segment or lobe may be replaced by fibrosis. The areas of fibrosis arehypointense to liver parenchyma on T1WIs and hyperintense on T2WIs. As mentioned previously, focal fatinfiltration or focal fat sparing may also produce nodules in the cirrhotic liver. Metastases, especially thosefrom breast carcinoma, may mimic the appearance of cirrhosis, with regenerative nodules. Followingchemotherapy, tissue retraction of necrosing metastases with surrounding scarring may produce a conditiontermed pseudocirrhosis (6).
Portal hypertension is a pathologic increase in portal venous pressure that results in the formation ofportosystemic collateral vessels that divert blood flow away from the liver and into the systemic circulation.Causes of portal hypertension include progressive vascular fibrosis associated with chronic liver disease,portal vein thrombosis or compression, and parasitic infections (schistosomiasis). Portal hypertension carriesthe risk of hemorrhage from varices and hepatic encephalopathy. The signs of portal hypertension include:(1) visualization of portosystemic collaterals (coronary, gastroesophageal, splenorenal, paraumbilical,hemorrhoidal, and retroperitoneal) (Fig. 27.6); (2) increased portal vein diameter (>13 mm); (3) increasedsuperior mesenteric and splenic vein diameters (>10 mm); (4) portal vein thrombosis; (5) calcifications in theportal and mesenteric veins; (6) edema in the mesentery, omentum, and retroperitoneum; (7) splenomegalyowing to vascular congestion; and (8) ascites (8).

FIGURE 27.8. Portal Vein Thrombosis: Multinodular HepatocellularCarcinoma. Contrast-enhanced CT demonstrates multiple hypodensenodules representing hepatocellular carcinoma that is replacing the righthepatic lobe. The portal vein (pv) is invaded by tumor (arrow), seen as afilling defect with the vein. The hepatic artery (arrowhead) is enlargedbecause of cirrhosis and portal hypertension.
Portal vein thrombosis may occur as a complication of cirrhosis, or it may be caused by portal veininvasion or compression by tumor (Fig. 27.8), hypercoagulable states, or inflammation (pancreatitis). Thecause is unknown in 8% to 15% of patients. On CT and US, the thrombus is seen as a hypodense plugwithin the portal vein. On MR, the thrombus is hyperintense on T1WIs when acute and isointense whenchronic. Signal in the thrombus is increased on T2WIs. Portal hypertension is exacerbated, or may becaused, by portal vein thrombosis. Cavernous transformation of the portal vein develops when smallcollateral veins adjacent to the portal vein expand and replace the obliterated portal vein. These collateralveins appear as a tangle of small vessels surrounding the thrombosed portal vein (8).
Budd-Chiari syndrome is caused by obstruction to hepatic venous outflow that may be a result ofobstruction of the suprahepatic IVC by a congenital membranous web (primary type) or by thrombosis of thehepatic veins caused by tumor, hypercoagulable states, or trauma (secondary type). Blood flow to the rightand left hepatic lobes is severely impaired, resulting in a characteristic “flip-flop” pattern on contrast-enhanced CT. On early images, the central liver enhances prominently, whereas the peripheral liverenhances weakly (Fig. 27.9). On delayed images, the periphery of the liver is enhanced, whereas contrasthas

P.763washed out of the central liver. The caudate lobe is spared because of its separate venous drainage to theIVC. The caudate lobe is characteristically enlarged and enhances normally. Thrombi may be seen in thehepatic veins, or they may be reduced in caliber and difficult to visualize. Comma-shaped intrahepaticcollateral vessels may be seen on CT or MR (the “comma sign”). Multiple benign hepatic nodules up to 3 cmcommonly develop. Most are detected by prominent contrast enhancement during the arterial phase or mildcontrast enhancement during the portal venous phase (9).
FIGURE 27.9. Budd-Chiari Syndrome. Early phase CT images show themarkedly heterogeneous liver with prominent central and weak peripheralenhancement that is characteristic of Budd-Chiari syndrome. Tumor invasionfrom a right adrenal carcinoma is seen as a filling defect (arrow) within theinferior vena cava.
Passive hepatic congestion is a common complication of congestive heart failure and constrictivepericarditis. Hepatic venous drainage is impaired, and the liver becomes engorged and swollen. Findingsinclude distension of the hepatic veins and IVC, reflux of IV contrast into the hepatic veins and IVC,increased pulsatility of the portal vein, and inhomogeneous contrast enhancement of the liver. Secondaryfindings commonly present include hepatomegaly, cardiomegaly, pleural effusions, and ascites.
Hemochromatosis may be primary (hereditary) or secondary owing to excessive iron intake from eitherparenteral or dietary sources. In severe cases, CT demonstrates a diffuse increase in liver density, to 75 to130 H. MR is more sensitive to hepatic iron overload because of the superparamagnetic effect of iron. MRdemonstrates marked diffuse low signal intensity on T2WIs (Fig. 27.10) and moderate loss of signal intensityon T1WIs (10). Long-standing hemochromatosis places the patient at risk for cirrhosis and hepatocellularcarcinoma.
Gas in the portal venous system is often an ominous sign associated with bowel ischemia in adults (Fig.27.11) and necrotizing enterocolitis in infants. Additional causes include recent colonoscopy, enemaadministration, gastrostomy tube placement, abdominal trauma, inflammatory bowel disease, perforated

P.764
gastric ulcer, necrotizing pancreatitis, diverticulitis, and abdominal abscess (8). CT reveals air in branchingtubular structures that extends to the liver capsule. Air is commonly evident within
the mesenteric and portal veins. Plain radiographs show streaks of low density in the periphery of the liver.In distinction, air in the biliary tree is more central, not extending to within 2 cm of the liver capsule.
FIGURE 27.10. Hemochromatosis. T2W MR image demonstrates markedlow signal intensity in both liver and spleen. The low signal is caused by irondeposition in the reticuloendothelial system—in this case of secondaryhemochromatosis caused by multiple blood transfusions.

FIGURE 27.11. Portal Venous Gas. Noncontrast CT image reveals gas inthe portal vein, seen as air-density tubular structures extending to theperiphery of the liver. Gas in the biliary tree is central and does not extendinto the peripheral 2 cm of the liver. In this case, portal venous gas wasassociated with infarction of the small bowel.
Liver MassesA major challenge of liver imaging is to differentiate common and benign liver masses, such as cavernoushemangioma and simple hepatic cysts, from malignant masses such as metastases and hepatoma. US candefinitively characterize hepatic cysts; however, benign and malignant solid masses overlap in sonographicappearance. CT can characterize most cysts and cavernous hemangiomas, but only with optimal techniqueand contrast administration. On MR, simple cysts and hemangiomas are hypointense on T1WIs andextremely hyperintense on T2WIs. These benign masses are typically homogeneous and have sharp outermargins. Malignant lesions on MR tend to be inhomogeneous with unsharp outer margins, peritumoraledema, and central necrosis. Most focal lesions are hypointense on T1WIs and hyperintense on T2WIs.Hyperintensity of focal lesions on T1WIs may be a result of the presence of fat, blood, proteinaceousmaterial, or melanin in melanoma metastases (Table 27.4). Diffuse hypointensity of liver, caused by diffuse

edema or iron overload, may make any lesion appear relatively hyperintense. Hypointensity on T2WIs iscommonly a result of fibrosis (Table 27.5).
TABLE 27.4 Causes of Hyperintensity in Focal Liver Lesions on MR T1WIs
Fat deposits Focal fat infiltration Fat deposition in tumor Hepatoma Lipoma Angiomyolipoma Hepatic adenomaBlood Hematoma Hemorrhage into tumorProteinaceous material Proteinaceous fluid in cysts Necrosis/hemorrhage in tumor Abscess HematomaCopper Intratumoral copper in hepatomaMelanin Melanoma metastasisContrast enhancement Gadolinium administration Lipiodol administrationGhosting artifact Result of blood flow in adjacent vesselsHypointensity of liver parenchyma Edema caused by passive hepatic congestion Iron deposition in hepatocytes
TABLE 27.5 Causes of Hypointensity in Focal Liver Lesions on MR T2WIs
Fibrous capsule Hepatoma (24% to 42% of HCC) Hepatic adenoma Focal nodular hyperplasia (rare)Fibrous central scar Fibrolamellar HCC Focal nodular hyperplasia
HCC, hepatocellular carcinoma.

P.765
Metastases are the most common malignant masses in the liver. Metastases are 20 times more commonthan primary liver malignancies. Of all patients who die of malignancy, 24% to 36% have liver involvement.Hepatic metastases most commonly originate from the GI tract, breast, and lung. A wide spectrum ofappearance of metastatic disease is seen on all imaging studies (Fig. 27.12) (11). Metastases may beuniformly solid, necrotic, cystic, or calcified; they may be avascular, hypovascular, or hypervascular; they arecommonly irregular and poorly marginated but may be sharp and well defined. Most characteristic is bandlikeperipheral enhancement on arterial phase images, with rapid washout on delayed CT and MR images.Metastatic disease must be considered in the differential
of virtually all hepatic masses (Table 27.6). Multiplicity of lesions favors metastatic disease.
FIGURE 27.12. Metastases. Metastases from adenocarcinoma of the colonappear as numerous low-attenuation nodules of varying size on this portalvenous phase, postcontrast CT. Note how the metastatic disease causesnodularity of the liver contour and the resemblance to regenerative nodulesin cirrhosis (see Fig. 27.7).
TABLE 27.6 Causes of Multiple Small (10-mm) Lesions in the Liver
Regenerative nodules in cirrhosisMicroabscesses (immunocompromised patient)Multiple bacterial abscesses

HistoplasmosisLymphomaKaposi sarcoma (AIDS patient)Hepatocellular carcinoma (multinodular form)SarcoidosisGamna-Gandy bodies (portal hypertension)Metastases Breast carcinoma Lung carcinoma Ovarian carcinoma Gastric carcinoma Malignant melanoma Prostate carcinoma
Cavernous hemangioma is second only to metastases as the most common cause of a liver mass (12). Itis the most common benign liver neoplasm, found in 7% to 20% of the population and more commonly inwomen. Up to 10% of patients have multiple lesions, which are easily mistaken for metastases. Manyhemangiomas are discovered incidentally on hepatic imaging performed for other reasons. The tumorconsists of large, thin-walled, blood-filled vascular spaces separated by fibrous septa. Blood flow through themaze of vascular spaces is extremely slow, resulting in characteristic imaging findings. Thrombosis within thevascular channels may result in central fibrosis and calcification. Most lesions are smaller than 5 cm, causeno symptoms, and are considered benign incidental findings. Larger lesions (>6 cm) occasionally causesymptoms by mass effect, hemorrhage, or arteriovenous shunting. The size of most cavernous hemangiomasis stable over time. Enlargement of a lesion is cause for reassessment.
US demonstrates a well-defined, uniformly hyperechoic mass in 80% of patients. In a patient with no historyof malignant disease and normal liver chemistries, follow-up only is generally recommended. No Dopplersignal is obtained from most cavernous hemangiomas because the flow is too slow.
CT generally shows a well-defined, hypodense mass on unenhanced scans. Because the lesion consistsmostly of blood, attenuation of the hemangioma is similar to that of blood vessels within the liver. Thecharacteristic pattern of enhancement with bolus IV contrast is nodular enhancement from the periphery ofthe lesion (Fig. 27.13) that gradually becomes isodense or hyperdense compared to the liver parenchyma.The degree of contrast enhancement parallels that of hepatic blood vessels during all postcontrast phases.The contrast enhancement persists for 20 to 30 minutes following injection because of slow flow within thelesion.

P.766
FIGURE 27.13. Cavernous Hemangioma. Images from a contrast-enhanced helical CT demonstrate the characteristic nodular pattern ofenhancement from the periphery of the lesion.
Radionuclide scanning using technetium-labeled red blood cells as a blood pool agent is extremely accuratein the diagnosis of cavernous hemangioma. Hemangiomas are characterized by prolonged, intense activitywithin the lesion on delayed images.
MR demonstrates a well-defined homogeneous mass that is hypointense or isointense on T1WIs andbrightens markedly with increasing amounts of T2 weighting. Areas of fibrosis remain dark on all imagesequences. However, the MR appearance of cavernous hemangiomas overlaps that of cysts, abscesses,and hypervascular metastases. A specific diagnosis can be made by IV administration of gadolinium andobserving early puddling peripheral enhancement in a pattern similar to that seen in contrast-enhanced CT.
Biopsy may be required in atypical cases. Percutaneous biopsy can be safely performed using small needles(20-gauge and smaller). The characteristic finding is blood with normal epithelial cells and no malignant cells.Biopsy with large-bore needles has been associated with hemorrhage and death.
Hepatocellular carcinoma is the most common primary malignancy of the liver. Risk factors includecirrhosis, chronic hepatitis, and a variety of carcinogens (sex hormones, aflatoxin, Thorotrast). In the UnitedStates, most HCCs are found in patients with cirrhosis (usually because of alcohol abuse). In Asia, mostHCCs are found in patients with chronic active hepatitis. Hepatomas demonstrate three major growthpatterns that affect their imaging appearance: diffuse infiltrative, solitary massive (Figs. 27.14, 27.15), andmultinodular (Fig. 27.8). Detection of the diffuse pattern of tumor is particularly difficult,
especially when the liver parenchyma is already altered by diffuse hepatic disease. Approximately 24% oftumors are surrounded by a fibrous capsule. The encapsulated HCC, a variant of the solitary form, is foundmore frequently in Asian populations and has a better prognosis. Intratumoral hemorrhage and necrosis arecommon because of a lack of stroma within the tumor. Calcifications (punctate, stippled, or rimlike) occur inapproximately 10% of cases. Most lesions are hypervascular and demonstrate contrast enhancement onarterial phase images, with diminishing enhancement on delayed phase images (see Fig. 27.17). Detectionof hepatoma on a background of cirrhosis and regenerative nodules is a major imaging challenge. Elevation

in serum !-fetoprotein is found in 90% of patients and is strongly suggestive of hepatoma in patients withcirrhosis. The tumor metastasizes to lungs, abdominal lymph nodes, adrenal glands, and bone (13).
FIGURE 27.14. Hepatocellular Carcinoma on CT. Three-phase helical CTdemonstrates the enhancement pattern of a larger hepatocellular carcinomain the right lobe. The tumor is slightly hyperdense to parenchyma on theunenhanced scan (upper left) and shows intense enhancement on the early(arterial phase—upper right) scan and delayed (venous phase—lower) scan.The central low density is a result of necrosis. Note the satellite lesions(arrows).

FIGURE 27.15. Hepatocellular Carcinoma on MR. Postcontrast T1WIshows the typical mosaic pattern of large hepatocellular carcinomas. Notethe prominent enhancement in the periphery of the tumor.
TABLE 27.7 Fat-Containing Lesions in the Liver
Hepatic adenomaHepatocellular carcinomaFocal fatty depositionLipomaTeratomaLiposarcoma (primary or metastatic)Postoperative packing material (omentum)Focal intrahepatic extramedullary hematopoiesis
Several imaging features are highly characteristic of HCC when present. Invasion of tumor into portal andhepatic veins occurs in up to 48% of cases (Fig. 27.8). Tumor thrombus is visualized as a low-density plugwithin an expanded vein. The intraluminal tumor enhances with contrast administration on CT and MR andmay demonstrate arterial signal with Doppler US. Portal vein thrombus is more common than hepatic veinthrombus. A tumor capsule, when present, is visualized as a sharply marginated rim of tissue that enhancesin 90% of cases. The capsule has low signal intensity on both T1WIs and T2WIs and is hypoechoic on US.Satellite nodules of tumor are common (Fig. 27.14). Fatty metamorphosis is a common histologic finding inHCC. CT may demonstrate a focal area of tumor with attenuation values of fat (Table 27.7) (14). MRconfirmation of fat is performed with chemical shift imaging. A mosaic appearance of the tumor is considered

P.767
to be characteristic but is found primarily in larger lesions (Fig. 27.15). The mosaic pattern appears asmultiple nodular areas of differing CT attenuation. The pattern is more obvious with enhancement ofseptations on postcontrast scans. Arterioportal shunting is seen as early or prolonged enhancement of theportal vein or as a wedge-shaped area of parenchymal enhancement adjacent to the tumor. Abundantcopper-binding protein in cancer cells may lead to excessive copper accumulation within the tumor. Highcopper concentration causes the tumor to appear hyperdense on noncontrast CT and hyperdense (becauseof T1 shortening effect) on T1WIs on MR.
Focal nodular hyperplasia (FNH) forms a solid mass consisting of abnormally arranged hepatocytes, bileducts, and Kupffer cells. Most lesions are smaller than 5 cm in
diameter and are hypervascular, with a central fibrous scar containing thick-walled blood vessels. Lesionsare lobulated and well circumscribed but lack a capsule. These are benign lesions that do not requiretreatment but must be differentiated from hepatic adenoma and fibrolamellar carcinoma.
In contrast to hepatic adenoma, hemorrhage, necrosis, and infarction are extremely rare in FNH. Similar tohepatic adenoma, FNH is found most commonly in women, but it is twice as common as hepatic adenomaand is not related to oral contraceptive use. Most tumors (80% to 95%) are solitary. Because of the presenceof Kupffer cells, most (50% to 70%) FNH nodules will show normal or increased radionuclide activity ontechnetium sulfur colloid liver-spleen scans (15). This finding is highly indicative of FNH.
On CT, MR, and US, most tumors appear homogeneous and solid. A central core scar with radiating septais characteristic but present in only 60%. Because the cellular makeup of FNH is very similar to that ofnormal hepatic parenchyma, the lesion is usually isodense on noncontrast images (Fig. 27.16). The typicalfinding on contrast-enhanced CT and MR is intense, brief (approximately 1 minute), uniform tumorenhancement during the arterial phase. FNH is inconspicuous on US, detectable only by mass effect (bulgingcontour) or slight alterations in parenchymal echotexture. Some lesions have a hypoechoic halo. The centralscar, if present, is often poorly visualized. Color flow imaging may show the lesion's hypervascularity. MDCTshows homogeneous hyperenhancement during the arterial phase. The lesion is often isodense during theportal phase, with enhancement of the central scar on delayed images. On MR, FNH appears homogeneousand isointense to slightly hypointense to normal parenchyma on T1WIs and isointense to slightlyhyperintense on T2WIs (7). The central scar is hypointense on T1WIs and hyperintense on T2WIs. FNHshows a characteristic very intense homogeneous enhancement on arterial phase postcontrast images. Thecentral scar and radiating septa enhance on delayed postcontrast images.
Hepatic adenomas are rare benign tumors that carry a risk of life-threatening hemorrhage and potential formalignant degeneration. Surgical removal of the tumor is advocated. They are found most commonly inwomen on long-term oral contraceptives. Additional risk factors include androgen steroid intake and glycogenstorage disease. The tumor consists of sheets and cords of benign hepatocytes without a distinct acinararchitecture. The hepatocytes occasionally contain abundant fat, detectable by imaging studies. Kupffer cellsare present in some tumors but are nonfunctional; thus, hepatic adenomas appear as cold defects ontechnetium sulfur colloid radionuclide scans. Tumors have poor connective tissue support, making themsusceptible to hemorrhage. Most tumors are solitary, smooth, and encapsulated. They do not have centralscars. Tumor size is commonly 8 to 15 cm but may be up to 30 cm. Areas of necrosis, hemorrhage, andfibrosis are common (16). Liver adenomatosis is characterized by the presence of multiple adenomas in anotherwise normal liver in patients without risk factors for hepatic adenomas.
US is sensitive to high fat content or intratumoral hemorrhage, which makes the lesions appear hyperechoic.CT shows well-circumscribed tumors that are often low in attenuation because of internal fat, necrosis, or oldhemorrhage. Calcifications in areas of old hemorrhage or necrosis are present in 15% of cases. Postcontrastscans show intense homogeneous enhancement during the arterial phase that becomes isodense with liver

P.768
on portal venous and delayed phase scans. Tumors are hyperintense on T1WIs because of fat orhemorrhage. On T2WIs, most are hyperdense to liver and are commonly heterogeneous because ofhemorrhage or necrosis. Dynamic postgadolinium scans are similar to postcontrast CT, showing intensearterial phase enhancement (Fig. 27.17), with isointensity on portal phase and delayed images.
Fibrolamellar carcinoma is a hepatocellular malignancy with clinical and pathologic features that are distinctfrom HCC (17). Tumors typically present as a large liver mass in a young adult (mean age, 23 years) withnone of the risk factors for HCC and without elevation of !-fetoprotein levels. Cords of tumor are surroundedby prominent fibrous bands that emanate from a central fibrotic scar. The surrounding liver is usually normal,without features of cirrhosis or chronic liver disease. The characteristic appearance is a large, lobulatedhepatic mass with central scar and calcifications. The central scar with radiating septa mimics theappearance of FNH. Satellite tumor nodules are occasionally present (10% to 15%). Hemorrhage andnecrosis are uncommon (10%) but are occasionally massive, resulting in a multicystic appearance of thetumor. Although the tumor is less aggressive than HCC, the stage at presentation tends to be advanced, withmalignant adenopathy present. Aggressive surgical management is indicated.
US shows a large, lobulated, well-defined mass with mixed echogenicity. The central scar is echogenic, ifvisible. On precontrast CT, the tumor is low attenuation. Calcification may be evident within the fibrous scar.The tumor enhances prominently and heterogenously on both arterial and portal venous phases (Fig. 27.18).Enhancement of the scar is most evident on delayed scans. MR shows a usually homogeneous hypointensemass (86%) or an isointense mass (14%) on T1WIs. On T2WIs the mass is usually hyperintense and muchmore heterogeneous. The fibrous scar is hypointense on all image sequences. Gadolinium enhancementshows the same pattern as CT.
Lymphoma involving the liver is usually diffusely infiltrative and undetectable by imaging methods. Themultiple-nodule pattern found in 10% of cases resembles
metastatic disease. Some cases present as a large, poorly defined, hypodense mass with or without satellitenodules. On MR, lesions are hypodense on T1WIs and hyperdense on T2WIs. Lesions enhance poorly or notat all (Fig. 27.19).

FIGURE 27.16. Focal Nodular Hyperplasia. The lesion (arrows), consisting ofliver elements, is isodense with the hepatic parenchyma on a T1WI (A) and agradient-recall two-dimensional time-of-flight image (B). The lesion is clearlydepicted by intense enhancement during the arterial phase (C), post–gadoliniumadministration. This lesion lacks a central scar. Note the mottled early enhancementof the portion of the spleen (arrowhead) included on the image.
Benign hepatic cyst is the second most common benign hepatic mass, found in 5% of the population (18).Most are solitary, but they may be multiple, especially in patients with adult polycystic disease or tuberoussclerosis. Cysts range in size from microscopic to 20 cm. Hepatic cysts do not communicate with the biliarytree. Tiny cysts are responsible for many of the “hypoattenuating lesions too small to characterize” seen onMDCT. Larger cysts tend to occur in clusters with cysts of varying size, resulting in sharply defined, butlobulated, margins and septations. Hepatic polycystic disease is part of the spectrum of autosomal-dominantpolycystic disease and occasionally occurs in the absence of polycystic kidneys.

P.769
FIGURE 27.17. Hepatic Adenoma. Postgadolinium, T1W, fat-suppressedMR image shows intense homogeneous enhancement during arterial phaseof a biopsy-proven hepatic adenoma (arrow). The MR appearance isindistinguishable from that of a small hepatocellular carcinoma.
US is the best imaging modality to characterize hepatic cysts. Typical cysts are anechoic with thin walls andsepta and posterior acoustic enhancement. Occasionally, hepatic cysts have internal debris, especially if theyhave been infected. CT shows low internal attenuation near water (Fig. 27.20) (18). MR shows low internalsignal on T1WIs and high internal signal on T2WIs. Cysts do not enhance following contrast administration.
Pyogenic abscess is usually caused by Escherichia coli, Staphylococcus aureus, Streptococcus, oranaerobic bacteria (19). Patients present with fever and pain. Destruction of liver results in a solitary cavity ora tight group of individual loculated abscesses (Fig. 27.21). A peripheral rim enhances with contrast. Gas ispresent within the lesion in 20% of cases (3). Diagnosis is confirmed by percutaneous aspiration. Catheter orsurgical drainage is indicated.

FIGURE 27.18. Fibrolamellar Hepatocellular Carcinoma. CT scandemonstrates a large tumor (between white arrows) extending caudally fromthe right lobe of the liver. A characteristic stellate central scar (black arrow)is present.

P.770
FIGURE 27.19. Hepatic Lymphoma. CT shows a poorly marginated,hypodense, nonenhancing nodule (arrow) that proved on biopsy to be non-Hodgkin lymphoma.
Amebic abscess is usually solitary, with thick nodular walls (3). The lesion may be indistinguishable frompyogenic abscess (Fig. 27.22); however, the patient is often
more acutely ill and has a history of travel to endemic areas (India, Africa, East Asia, Central and SouthAmerica). Amebic abscesses commonly occur in the right lobe of the liver, often cause elevation of the righthemidiaphragm, and may rupture through the diaphragm into the pleural space. In the United States, thediagnosis is typically confirmed by serology and the patient is treated with metronidazole. In endemic areas,the diagnosis is confirmed by aspiration of “anchovy paste” material, and the patient is treated by repeatedaspiration or catheter drainage.

FIGURE 27.20. Hepatic Cysts. Multiple hepatic cysts are an incidentalfinding on this postcontrast CT in a 78-year-old patient.
FIGURE 27.21. Pyogenic Abscess. CT scan shows multiple low-density

areas separated by enhancing septa and representing abscess locules.Several air bubbles (arrowhead) are evident within the lesion.
FIGURE 27.22. Amebic Abscess. Postcontrast CT image reveals a thick-walled fluid collection in the right hepatic lobe. Differentiation of amebic frompyogenic liver abscess is made by history, serology, or image-guidedaspiration.
Echinococcus cyst is caused by infestation with Echinococcus granulosus or E multilocularis tapeworm(19). The parasite is endemic in central and northern Europe, the Mediterranean, northern Asia, China,Japan, Turkey, and parts of North America. The liver is the most common organ affected (95%). Single ormultiple cystic masses usually have well-defined walls that commonly calcify (50%). The cyst wall andseptations usually enhance. Daughter cysts may be visualized within the parent cyst (75%). Diagnosticaspiration carries a risk of anaphylactic reaction. Treatment is mebendazole or surgical excision.
Cystic/necrotic tumor must always be considered for atypical cystic masses. Metastases may be necrotic orpredominantly cystic. Biliary cystadenoma and cystadenocarcinomas are rare primary tumors that resemblemucinous cystic tumors of the pancreas. Undifferentiated embryonal sarcomas are seen in older children,adolescents, and young adults (18).

P.771
Small hypoattenuating lesions are detected with increased frequency on MDCT because of thinnercollimation, improved resolution, and rapid, multiphase, postcontrast scanning (Fig. 27.23). Lesions smallerthan 1 cm
are difficult to characterize and often too small to biopsy. Differential diagnoses include cysts, hemangiomas,and metastases. Statistically, most of these tiny lesions are benign. In a patient with known malignancy,follow-up scans are needed to exclude metastatic disease. In a series of patients with known malignancy,lesions were metastases in 12% of cases (20).
FIGURE 27.23. Too Small to Characterize. Multidetector CT showsmultiple, tiny, low-attenuation lesions (arrowhead) that are too small todefinitively characterize. Even in patients with known malignancy, theselesions are usually benign. However, on follow-up in some patients, they willprove to be early metastatic lesions. They are usually identified only on high-quality postcontrast CT. Image-guided biopsy cannot usually be performedbecause the lesions cannot be identified on US or noncontrast CT.
BILIARY TREE
Imaging MethodsImaging of the biliary tree uses assorted techniques that differ in degrees of invasiveness. US and CT are

highly sensitive in the detection of dilation of the bile ducts, though they are somewhat less effective inidentifying its cause. US is the preferred screening method for biliary obstruction because of its low cost andconvenience. Unenhanced helical CT has a reported sensitivity of 88% in detection of stones in the commonbile duct. MR can also demonstrate biliary dilation and may be more effective than CT or US indemonstrating associated tumors.
MR cholangiopancreatography (MRCP), performed using extreme T2W sequences, offers a noninvasivemethod of high-resolution imaging of the biliary tree (21). MRCP takes advantage of the long T2characteristic of bile. Extreme T2 weighting demonstrates bright bile ducts with dark surrounding soft tissues(Fig. 27.24). However, any static fluid will also be bright on MRCP images, so ascites, hepatic and renalcysts, and fluid in the bowel may obscure the biliary tree. Similar to contrast cholangiography, stones areseen as hypodense filling defects (Table 27.8).
Endoscopic retrograde cholangiography and percutaneous transhepatic cholangiography supplement cross-sectional imaging methods by providing access to the biliary tree for contrast injection and subsequentcatheter drainage or biliary stent placement. Operative cholangiography is used to visualize nonpalpable bileduct stones at surgery, and T-tube cholangiography is used to visualize common duct stones followingsurgery. Radionuclide imaging utilizing technetium-99m-iminodiacetic acid is useful for showing the patencyof biliary-enteric anastomoses and for demonstrating bile leaks and fistulae. Scintigraphy has the greatestsensitivity for early obstruction. IV cholangiography involves the use of highly toxic contrast agents and hasbeen abandoned in favor of other techniques. Functional CT and MR cholangiography using oralcholangiographic agents, iopanoic acid (Telepaque) for CT, and mangafodipir trisodium for MR are underinvestigation.
FIGURE 27.24. Normal MR Cholangiopancreatography (MRCP). Imagefrom a MRCP in a patient who has had a cholecystectomy shows the cysticduct remnant (arrowhead), normal common bile duct (straight arrow), normalpancreatic duct (curved arrow), and normal major intrahepatic bile ducts(squiggly arrow).

P.772
TABLE 27.8 Causes of Filling Defects in the Bile Ducts
Biliary stonesAir bubblesBlood clotsNeoplasms Cholangiocarcinoma Ampullary carcinoma Granular cell myoblastoma Mesenchymal tumorParasites Ascaris lumbricoides Liver fluke
Anatomy of the Biliary TractThe bile ducts arise as bile capillaries between hepatocytes and join progressively larger branches until twomain trunks are formed, draining the right and left lobes of the liver. The ducts of the left hepatic lobe aremore anterior than those of the right hepatic lobe. This relationship must be kept in mind when contrastcholangiography is performed. Contrast agents flow to the most dependent portions of the biliary tree andmay not opacify nondependent ducts. Failure to fill ducts before gravitational repositioning must not beinterpreted as evidence of obstruction.
The right and left hepatic ducts combine to form the common hepatic duct (CHD), which courses with theportal vein and hepatic artery in the porta hepatis. The cystic duct courses posteriorly and inferiorly from thegallbladder to join the CHD and form the common bile duct (CBD). The CBD runs ventral to the portal veinand to the right of the hepatic artery, descending from the porta hepatis along the free right margin of thehepatoduodenal ligament to the duodenal bulb. The distal third of the CBD turns caudally and descends inthe groove between the descending duodenum and the head of the pancreas, just anterior to the IVC. TheCBD tapers distally as it ends in the sphincter of Oddi, which protrudes into the duodenum
as the ampulla of Vater. The CBD and the pancreatic duct share a common orifice in 60% of individuals andhave separate orifices in the remainder. However, because of their close proximity, tumors of the ampullaregion generally obstruct both ducts. The CHD and CBD are considered to be extrahepatic bile ducts(EHBDs).
Normal intrahepatic bile ducts (IHBDs) are occasionally seen on US and on postcontrast helical CT with thin(5-mm) collimation. Normal IHBDs do not exceed 40% of the diameter of the adjacent portal vein, or 2 mm indiameter in the central liver or 1.8 mm in diameter in the peripheral liver. The extrahepatic CBD is routinelyvisualized and does not exceed 6 to 7 mm in internal diameter. Normal ducts appear larger on contrastcholangiography studies because of distention and magnification. Slightly larger common ducts are alsonormal in elderly patients because of elastic tissue degeneration with aging. Cholecystectomy is not provento alter normal common duct size. Care must be taken to differentiate an enlarged common duct from anenlarged hepatic artery. Color Doppler is useful to make this differentiation on US. Contrast enhancement ofblood vessels makes differentiation easy on CT.
MRCP and cholangiographic studies demonstrate IHBD branches that parallel the portal veins andcorrespond to the Couinaud segments of the liver (22). The right hepatic duct drains segments V to VIII and

is formed by the junction of the more horizontal coursing right posterior duct draining VI and VII and the morevertically coursing right anterior duct draining V and VIII. The left hepatic duct is formed by segmental ductsdraining segments II, III, and IV. The duct of the caudate lobe (I) joins either the right or left hepatic duct.Variations include drainage of the right posterior duct into the left hepatic duct (13% to 19%); tripleconfluence, with the right posterior, right anterior, and left hepatic ducts uniting at a single position (11%);and anomalies of the cystic duct, including low insertion on the CBD, long parallel course with the CHD, andinsertion on the medial rather than the lateral side of the CBD. These anomalies have significant importanceto the biliary surgeon.
Biliary DilatationCT, US, and MR are highly effective at demonstrating the anatomic finding of biliary dilatation, which isusually equated with biliary obstruction. However, biliary obstruction may be present intermittently or in theearly stage without biliary dilation being present. Alternatively, biliary dilatation may be present withoutobstruction, such as after surgical decompression or bypass. Patients with clinical evidence of biliaryobstruction (i.e., elevated alkaline phosphatase and direct hyperbilirubinemia) may not have biliary dilation.Hepatitis causes swelling of hepatocytes, which blocks biliary capillaries and causes intrahepatic cholestasiswithout surgical obstruction.
FIGURE 27.25. Biliary Dilation. A CT scan demonstrates dilatedintrahepatic ducts (black arrowheads), which are easily differentiated fromportal veins (white arrowhead) and hepatic veins by contrast enhancement ofthe blood vessels. Note that the diameter of the bile ducts clearly exceeds

P.773
40% of the diameter of the adjacent portal vein. Biliary dilatation in thispatient was caused by adenocarcinoma of the head of the pancreas.
Signs of biliary dilation include the following: (1) multiple branching tubular, round, or oval structures thatcourse toward the porta hepatis; (2) diameter of intrahepatic bile ducts larger than 40% of the diameter of theadjacent portal vein (Fig. 27.25); (3) dilation of the common duct greater than 6 mm; and (4) gallbladderdiameter greater than 5 cm, when obstruction is distal to the cystic duct. Benign disease is responsible forapproximately 75% of cases of obstructive jaundice in the adult, while malignant disease causes theremainder. Gradual tapering of a dilated common duct suggests benign stricture. Gallstones may beidentified in the bile duct surrounded by a crescent of bile. Abrupt termination of a dilated common duct ischaracteristic of a malignant process (23).
Infected bile is present in up to 10% of cases of complete biliary obstruction and 60% of cases of partial orintermittent biliary obstruction. IV antibiotic therapy is warranted prior to biliary interventional procedures inthe obstructed patient.
Causes of biliary dilation and obstruction (Table 27.9) include the following.
Choledocholithiasis is responsible for approximately 20% of cases of obstructive jaundice in the adult (Fig.27.26). Gallstones are present in the gallbladder in
10% of the population, but the presence of stones in the gallbladder does not necessarily mean that stonesare the cause of ductal obstruction. In addition, 1% to 3% of patients with choledocholithiasis will have nostones in the gallbladder.
TABLE 27.9 Causes of Biliary Tract Obstruction
BENIGN (75% of cases) Benign stricture Surgery/instrumentation Trauma Stone passage Pancreatitis Cholangitis Choledochal cyst Stone impacted in duct Parasite (Ascariasis) Liver cystMALIGNANT (25% of cases) Pancreatic carcinoma Ampullary/duodenal carcinoma Cholangiocarcinoma Metastasis
The sensitivity of US for stones in the bile ducts ranges from 20% to 80%. Stone detection by US is muchimproved when the CBD is dilated and the pancreatic head is well visualized. CT sensitivity is 70% to 80%,

with stones appearing as intraluminal masses of varying attenuation. The “target sign” or “crescent sign”describes the appearance of an intraluminal stone that is partially surrounded by a crescent of low-attenuation bile (24). Contrast studies and MRCP have the highest sensitivity for stone detection (95% to99%) and demonstrate stones as dark filling defects within bright bile (Fig. 27.27).
FIGURE 27.26. Obstructing Stone in Common Bile Duct. Serial CTimages obtained from a jaundiced patient demonstrate dilatation of thecommon bile duct (small arrows) caused by an obstructing high-densitygallstone (large arrow) impacted in the distal common bile duct. Note thecourse of the common bile duct in relationship to the head of the pancreas(p) and descending duodenum (d).

P.774
FIGURE 27.27. Choledocholithiasis. MR cholangiopancreatography imagedemonstrates two stones (arrow) seen as filling defects in the distal commonbile duct. Ascites (a) outlines the liver. A normal gallbladder (gb) is evident.
Benign stricture is the cause of 40% to 45% of obstructive jaundice in the adult. Causes of benign strictureinclude trauma, surgery, prior biliary interventional procedures, recurrent cholangitis, previous passage ofstones through the bile ducts, radiation therapy, and perforated duodenal ulcer. The wall of the involved CBDenhances minimally with benign strictures, while hyperenhancement of the CBD during the portal venousphase is evidence of malignant stricture (25).
Pancreatitis is responsible for approximately 8% of cases of biliary obstruction. Inflammation, fibrosis, andinflammatory masses narrow the bile ducts.
Primary sclerosing cholangitis (PSC) is associated with a history of ulcerative colitis in 50% to 70% ofcases (26). PSC is characterized by insidious onset of jaundice, with progressive disease affecting bothIHBDs and EHBDs. Alternating dilation and stenosis (Fig. 27.28) produces a characteristic beaded pattern ofthe IHBDs. Small saccular outpouchings (duct diverticula), demonstrated on cholangiography, are consideredto be pathognomonic. Complications include biliary cirrhosis (50%) and cholangiocarcinoma.
AIDS-associated cholangitis is characterized by thickening of the walls of the bile ducts and the gallbladder
because of inflammation and edema. Infection by opportunistic organisms, most commonly cytomegalovirusand Cryptosporidium, as well as reaction to HIV itself, are implicated as the causes of observed disease. Bileducts are commonly dilated in association with stenosis at the ampulla. Ulcers in the common duct,

inflammatory changes in the duodenum, and additional evidence of infection with opportunistic organismsare commonly associated.
FIGURE 27.28. Primary Sclerosing Cholangitis. Radiograph from anendoscopic retrograde cholangiography demonstrates the focal irregularstrictures and focal mild dilatation of intrahepatic bile ducts that are typical ofearly stage sclerosing cholangitis.
Recurrent pyogenic cholangitis has been called Oriental cholangiohepatitis because it is an endemicdisease in Southeast Asia (27). It is characterized by recurrent attacks of jaundice, abdominal pain, fever,and chills. Intrahepatic and extrahepatic bile ducts are dilated and filled with soft pigmented stones and pus.The disease is associated with parasitic infestation (clonorchiasis, ascariasis) and nutritional deficiency.Findings include intraductal stones, severe extrahepatic biliary dilation, focal strictures, and straightening andrigidity of intrahepatic ducts. Complications include liver abscess, biloma, pancreatitis, andcholangiocarcinoma.
Caroli disease is an uncommon congenital anomaly of the biliary tract characterized by saccular ectasia ofthe IHBDs without biliary obstruction (28). Only one hepatic lobe or segment may be affected. The EHBDsare spared in 50% of cases. Findings include: (1) saccular dilatation of IHBDs, giving the appearance oncross-sectional imaging of scattered intrahepatic cysts that communicate with the biliary tree; (2) enhancing

P.775
fibrovascular bundles seen centrally within many of the dilated ducts, producing the characteristic “central dotsign;” (3) segmental distribution of the bile duct abnormality, with normal appearance of unaffected liversegments; (4) cholangiography showing a characteristic pattern of focal biliary narrowing and sacculardilatation; and (5) dilatation of the CBD (10 to 30 mm) in half of cases. The disease is associated withmedullary sponge kidney and autosomal-recessive polycystic kidney disease. Complications includepyogenic cholangitis, liver abscess, and biliary stones. Cholangiocarcinoma develops in 7% of cases. Mostcases present in childhood. Autosomal-recessive inheritance is evident in many cases.
Choledochal cysts are uncommon congenital anomalies of the biliary tree characterized by cystic dilation ofthe bile ducts (29). Many (60%) present in infancy or childhood, while others present in adulthood. Some arediscovered by fetal US. The condition is much more common in females (70% to 84% of cases). Patientspresent with abdominal pain, mass, and jaundice. The Todani classification (1977) is typically used todescribe choledochal cysts (Fig. 27.29). Type 1 lesions are most common (80% to 90%) and appear asfusiform or saccular dilatations (Fig. 27.30) of the CHD, CBD, or segments of each. Type 2 lesions arediverticula of the CBD attached by a narrow
stalk. Type 3 lesions are termed choledochoceles and are focal dilatations of the intraduodenal portion of theCBD, closely resembling ureteroceles. Type IV lesions are defined as multiple focal dilatations of the IHBDsand EHBDs usually with a focal large cystic dilatation of the CBD. Type 5 lesions are referred to as Carolidisease, which is more properly classified as a disease separate from choledochal cyst.
FIGURE 27.29. Classification of Congenital Biliary Cysts. Type 1choledochal cysts (80% to 90% of cases) are focal, saccular or fusiform,dilatations of the common bile duct. Type 2 cysts (2%) are true diverticula of

the common bile duct. Type 3 cysts (1.4% to 5%) are termedcholedochoceles and are dilatations of the terminal intraduodenal portion ofthe common bile duct. A type 4 classification (19%) refers to multipleintrahepatic and extrahepatic bile duct cysts. Caroli disease is classified astype 5.
FIGURE 27.30. Type 1 Choledochal Cyst. Radiograph from endoscopicretrograde cholangiography demonstrates saccular dilation (arrow) of thecommon bile duct, which is typical of the most common form of choledochalcyst: type 1.
Pancreatic and ampullary carcinomas are the cause of 20% to 25% of cases of biliary obstruction in theadult. Metastatic disease from lung, breast, GI tumors, and lymphoma accounts for 2% of cases.
Cholangiocarcinoma is the second most common malignant primary hepatic tumor (30). Tumors arise from

P.776
Cholangiocarcinoma is the second most common malignant primary hepatic tumor (30). Tumors arise fromthe epithelium of bile ducts and are usually adenocarcinomas (90%). Growth patterns include mass forming,periductal infiltrating, and intraductal polypoid. Peripheral cholangiocarcinoma (10%) presents as anintrahepatic hypodense mass, with adjacent biliary dilatation present in only 25% of cases (Fig. 27.31).MDCT demonstrates delayed, mild, thin, incomplete, rimlike enhancement with low tumoral attenuation inmost cases. Hilar cholangiocarcinoma (Klatskin tumor) (25%) occurs near the junction of the right and leftbile ducts (Fig. 27.32). The tumor is usually small, poorly differentiated, and aggressive and causesobstruction of both ductal systems. Extrahepatic cholangiocarcinoma (65%) causes stenosis or obstruction ofthe CBD in most cases (95%) and presents as an intraductal polypoid mass in 5%. Infiltratingcholangiocarcinoma shows thickening of the wall of the involved bile duct, with
hyperenhancement during the arterial phase (25). Predisposing conditions include choledochal cyst,ulcerative colitis, Caroli disease, Clonorchis sinensis infection, and PSC. The tumor may be infiltrative,desmoplastic, and small, making imaging detection as well as needle biopsy difficult. Abrupt stricture andthickening of the duct wall may be the only findings. Cross-sectional imaging is used to detect adenopathyand hepatic metastases. Prognosis is poor, with fewer than 20% of tumors being resectable.
FIGURE 27.31. Cholangiocarcinoma: Peripheral. Postcontrast, T1W, fat-suppressed MR shows a heterogeneous mass (between arrows) within theliver. Biopsy confirmed cholangiocarcinoma. No dilated bile ducts wereevident.

FIGURE 27.32. Cholangiocarcinoma: Hilar. Percutaneous transhepaticcholangiogram (PTC) demonstrates abrupt focal narrowing (short arrows) ofthe proximal common bile duct (cd) near the bifurcation. The intrahepatic bileducts are diffusely dilated. The common bile duct shows normal narrowing atthe ampulla of Vater (open arrow). The PTC needle (long arrow) is evident.D, duodenum.
Gas in the Biliary TractGas in the biliary tract is most commonly encountered in the patient with a surgically created biliary-entericanastomosis or who has received a sphincterotomy to facilitate stone passage (Table 27.10).
Cholecystoduodenal fistula is most commonly caused by erosion of a gallstone through the gallbladderand into the duodenum. When the gallstone is large, it may cause small bowel obstruction, i.e., “gallstoneileus.” The gallstone may also erode into the colon and pass spontaneously in the feces.Cholecystoduodenal fistula is most common in women because of the higher incidence of gallstones.
Choledochoduodenal fistula is caused by a penetrating peptic ulcer eroding into the common bile duct(Fig. 27.33).

GALLBLADDER
Imaging MethodsUS is the imaging method of choice for the gallbladder. It offers high anatomic detail, convenience, and costefficiency. Gallbladder US is reviewed in detail in Chapter 36. Cholescintigraphy utilizing technetium-99m-iminodiacetic acid has sensitivity and specificity comparable to US for the diagnosis of acute cholecystitis.Oral cholecystograms have been abandoned in favor of other imaging methods. However, oral biliarycontrast agents, previously used for oral cholecystograms, are currently utilized for CT cholangiography.Plain radiographs demonstrate calcified gallstones, porcelain gallbladder, and emphysematous cholecystitis.CT, as the imaging method of choice for the acute abdomen, frequently provides imaging diagnosis ofgallbladder disease (31).
TABLE 27.10 Causes of Gas in the Biliary Tract
Postsurgical Sphincterotomy Choledochoduodenostomy CholedochojejunostomyBiliary-enteric fistula Cholecystoduodenal fistula (gallstone erodes into CBD) Choledochoduodenal fistula (ulcer penetrates CBD) Surgery/trauma Tumor erosion with fistulaInfection Emphysematous cholecystitis Pyogenic cholangitis
CBD, common bile duct.

FIGURE 27.33. Choledochoduodenal Fistula. An upper GI seriesdemonstrates filling of the bile ducts because of a penetrating duodenal ulcerthat created a fistula (large arrow) between the duodenum (d) and the bileducts (small arrow).
AnatomyThe gallbladder lies on the underside of the liver, in the fossa formed by the junction of the left and rightlobes. While the position of the fundus is inconsistent, the neck of the gallbladder is invariably positioned inthe porta hepatis and major interlobar fissure. The gallbladder fundus frequently causes a mass impressionon the top of the duodenal bulb. Kinking and folding of the gallbladder is common and generally easilyrecognized by careful image analysis. The so-called phrygian cap, which is descriptive of folding of thegallbladder fundus, is a common normal variant. Septa within the gallbladder may be partial or complete. Thespiral valves of Heister are small folds in the cystic duct.
The normal gallbladder is well distended with bile following a 4-hour fast and is easily visualized. Agallbladder larger than 5 cm in diameter is considered enlarged (hydropic), while a gallbladder smaller than 2cm in diameter is considered contracted. The normal gallbladder wall does not exceed 3 mm in thickness—measured from gallbladder lumen to liver parenchyma—when the gallbladder is distended. The normalgallbladder lumen is free of particulate debris and is fluid density on imaging studies.

P.777
FIGURE 27.34. Cholelithiasis. A. CT reveals numerous subtle low-attenuationfloating gallstones (arrow) within the gallbladder. The stones are nearly isodensewith bile. Stones may be overlooked on CT because they are isodense with bile orbecause of their small size. B. Coronal T2WI shows a large gallstone (arrow) as afilling defect within high-signal bile.
Gallstones are present in 8% of the general population and 15% of the population aged 40 to 60 years.Approximately 85% of gallstones are predominantly cholesterol, while 15% are predominantly bilirubin(pigment stones) related to hemolytic anemia. Approximately 10% of stones are sufficiently radiopaque to bedetected by conventional radiographs as laminated or faceted calcifications. Fissures within gallstones maycontain nitrogen gas that appears on plain film as branching linear lucencies resembling a “crow's foot.”Gallstones are most common in women (female:male = 4:1) and in patients with hemolytic anemia, diseasesof the ileum, cirrhosis, and diabetes mellitus (32).
US detects 95% of all gallstones, whereas CT detects only 80% to 85%. Gallstones vary in CT attenuation,from fat density to calcium density (Fig. 27.34). Up to 20% of gallstones are isodense with bile and notdetected by CT, while some gallstones are missed because of their small size. Care must be taken to avoidinterpreting contrast in adjacent bowel as cholelithiasis.
Contrast studies, MRCP, and T2WIs demonstrate gallstones as “filling defects”—rounded or faceted darkobjects within high-density bile.
Differential considerations for lesions in the gallbladder that may be mistaken for gallstones include thefollowing.
Sludge balls or tumefactive biliary sludge result from biliary stasis. The bile thickens and forms mobilemasses that move with changes in patient position.
Cholesterol polyps are common benign, polypoid masses that result from accumulation of triglycerides andcholesterol in macrophages in the gallbladder wall. They are of no clinical significance. All are 10 mm orsmaller.

Adenomyomatosis may be focal and present as a polypoid mass fixed to the gallbladder wall.
Adenomatous polyps are small, usually flat masses fixed to the gallbladder wall.
Gallbladder carcinoma may present as a polypoid mass. Most are 1 cm or larger. Gallstones are usuallypresent.
Acute CholecystitisAcute inflammation of the gallbladder is caused by gallstones obstructing the cystic duct in 90% of cases.Acalculous cholecystitis occurs nearly always in patients with predisposing conditions (listed subsequently).Cholescintigraphy and US have comparable sensitivities and specificities in the diagnosis of acutecholecystitis.
Scintigraphic diagnosis of acute cholecystitis is based on obstruction of the cystic duct with nonvisualizationof the gallbladder. The normal gallbladder demonstrates progressive accumulation of radionuclide activityover 30 minutes to 1 hour following injection of technetium-99m-iminodiacetic acid. Delayed visualization ofthe gallbladder may be seen in patients with biliary stasis caused by fasting or hyperalimentation. Delayedimages taken at 4 hours post-radionuclide injection are needed to assess for this possibility. The test isconsidered positive if there is prompt tracer accumulation in the liver with excretion of tracer into the boweland without gallbladder visualization at 4 hours. The test may be considered positive at 1 hour post-radionuclide injection if the gallbladder does not visualize within 20 minutes of IV injection of morphine.
FIGURE 27.35. Acute Cholecystitis. Postcontrast CT demonstrates fluid(black arrow) around the enhancing mucosa (white arrowhead) of thegallbladder and a small, high-attenuation gallstone (thin arrow) within thegallbladder lumen in a patient with acute, severe right upper quadrant pain.Surgery confirmed acute cholecystitis.

P.778Confident US diagnosis of acute cholecystitis requires the presence of three findings: cholelithiasis; edema ofthe gallbladder wall, seen as a band of echolucency in the wall; and a positive sonographic Murphy sign.
CT demonstrates the following (Fig. 27.35): gallstones, distended gallbladder, thickened gallbladder wall,subserosal edema, high-density bile, intraluminal sloughed membranes, inflammatory stranding inpericholecystic fat, pericholecystic fluid, blurring of the interface between gallbladder and liver, and prominentarterial phase enhancement of the liver adjacent to the gallbladder (31).
Acalculous cholecystitis causes special problems in diagnosis because the cystic duct is often not obstructed.Inflammation may be the result of gallbladder wall ischemia or direct bacterial infection. Patients at risk foracalculous cholecystitis include those with biliary stasis caused by lack of oral intake, posttrauma, postburn,postsurgery, or on total parenteral nutrition. Scintigraphy usually demonstrates lack of gallbladdervisualization. Although this finding is 90% to 95% sensitive for acalculous cholecystitis, it is only 38%specific. False-positive conditions for nonvisualization include hyperalimentation and prolonged severeillness, which are predisposing conditions for acalculous cholecystitis. US demonstrates a distended tendergallbladder with thickened wall but without stones. Many patients are too ill to elicit a reliable sonographicMurphy sign.
Sludge is a term used to describe the presence of thick particulate matter in highly concentrated bile.Calcium bilirubinate and cholesterol crystals precipitate in the bile when biliary stasis is prolonged because ofa lack of oral intake, hyperalimentation, or biliary obstruction. Sludge appears as echodense bile on US andas high-attenuation bile on CT. Because sludge may be found in a fasting but otherwise normal patient, itspresence is not definitive evidence of gallbladder disease. Pus, blood, and milk of calcium are additionalcauses of dense bile.
Complications of acute cholecystitis include the following.
Gangrenous cholecystitis indicates the presence of necrosis of the gallbladder wall. The patient is at risk forgallbladder perforation. Findings include mucosal irregularity and asymmetric thickening of the gallbladderwall with multiple lucent layers, indicating mucosal ulceration and reactive edema.
Perforation of the gallbladder is a life-threatening complication seen in 5% to 10% of cases. Perforation mayoccur adjacent to the liver, resulting in pericholecystic abscess; into the peritoneal cavity, resulting ingeneralized peritonitis; or into adjacent bowel, resulting in biliary-enteric fistula. Overall mortality is as high as24%. A focal pericholecystic fluid collection suggests pericholecystic abscess.
Emphysematous cholecystitis results from infection of the gallbladder with gas-forming organisms, usually Ecoli or Clostridium perfringens. Approximately 40% of patients are diabetic. Gallstones may or may not bepresent. Gas is demonstrated within the wall or within the lumen of the gallbladder by plain film or CT. OnUS, intramural gas has an arc-like configuration that is difficult to differentiate from calcification and porcelaingallbladder.
Mirizzi syndrome refers to the condition of biliary obstruction resulting from a gallstone in the cystic ducteroding into the adjacent common duct and causing an inflammatory mass that obstructs the common duct.Visualization of a stone at the junction of the cystic duct and the common hepatic duct in a patient with biliaryobstruction and gallbladder inflammation suggests the diagnosis.
Chronic cholecystitis includes a spectrum of pathology that shares the presence of gallstones and chronicgallbladder inflammation. Patients with chronic cholecystitis complain of recurrent attacks of right upper

P.779
quadrant pain and biliary colic. Imaging findings include gallstones, thickening of the gallbladder wall,contraction of the gallbladder lumen, delayed visualization of the gallbladder on cholescintigraphy, and poorcontractility. Variants of chronic cholecystitis include the following.
Porcelain gallbladder describes the presence of dystrophic calcification in the wall of an obstructed andchronically inflamed gallbladder (Fig. 27.36). The condition is associated with gallstones in 90% of cases.Porcelain gallbladder carries a 10% to 20% risk of gallbladder carcinoma. Cholecystectomy is usuallyindicated.
Milk of calcium bile, also called limy bile, is associated with an obstructed cystic duct, chronic cholecystitis,and gallstones. Particulate matter with a high concentration of
calcium compounds is precipitated in the bile, making the bile radiopaque on plain films or CT. Dependentlayering of bile can be demonstrated on plain film radiographs. The bile is extremely echogenic on US, andgallstones may be visualized within it.
FIGURE 27.36. Porcelain Gallbladder. Conventional radiograph of the rightupper quadrant of the abdomen shows calcification (arrows) in the wall of thegallbladder (gb). This finding is indicative of chronic obstruction of the cysticduct with chronic cholecystitis. The risk of gallbladder carcinoma isincreased.

FIGURE 27.37. Adenomyomatosis of the Gallbladder. An MRcholangiopancreatography image shows focal thickening of the wall ofgallbladder fundus with a Rokitansky-Aschoff sinus (arrow) extending intothe thickened wall.
Xanthogranulomatous cholecystitis is an uncommon variant of chronic cholecystitis characterized by nodulardeposits of lipid-laden macrophages in the gallbladder wall and proliferative fibrosis. Imaging findings includemarked wall thickening (2 cm), fat-density nodules in the wall, and narrowing of the lumen. Cholelithiasis isfrequently present. The condition is difficult to differentiate from gallbladder carcinoma.
Thickening of the gallbladder wall is present when the wall thickness at the hepatic aspect of thegallbladder exceeds 3 mm in patients who have fasted at least 8 hours. Conditions associated with wallthickening include the following.
Acute and Chronic CholecystitisWall thickening is a usual feature of acute cholecystitis and is present in 50% of cases of chroniccholecystitis.
Hepatitis causes reduction in bile flow, which results in reduced gallbladder volume and thickening of thegallbladder wall in approximately half of patients.

P.780Portal venous hypertension and congestive heart failure may cause wall thickening by passive venouscongestion.
AIDS is associated with thickening of the gallbladder wall and the walls of the bile ducts. Opportunisticorganisms are sometimes present.
Hypoalbuminemia is associated with thickened gallbladder wall in 60% of patients.
Gallbladder carcinoma usually presents as a focal mass but may cause only focal wall thickening.
Adenomyomatosis is the most frequent benign condition of the gallbladder and is characterized byhyperplasia of the mucosa and smooth muscle. It is usually focal and in the fundus, but may be diffuse,involving the entire gallbladder. Outpouchings of mucosa into or through the muscularis form characteristicRokitansky-Aschoff sinuses (Fig. 27.37). The condition has no malignant potential. Coexisting gallstones arecommonly present (33).
Gallbladder CarcinomaAdenocarcinoma of the gallbladder is commonly overlooked or misdiagnosed preoperatively. The presence ofgallstones in 70% to 80% of cases masks the findings of cancer, especially with US examination.Gallbladder carcinoma is most often a tumor of elderly women (>60 years, female:male = 4:1). Patientspresent with pain, anorexia, weight loss, and jaundice. Calcification of the gallbladder wall (porcelaingallbladder) is a risk factor. Imaging findings include the following: (1) intraluminal soft tissue mass (Fig.27.38); (2) focal or diffuse thickening of the gallbladder wall; (3) soft tissue mass replacing the gallbladder;(4) gallstones; (5) extension of tumor into the liver, bile ducts, and adjacent bowel; (6) dilated bile ducts; and(7) metastases to periportal and peripancreatic lymph nodes and liver. Most tumors are unresectable atdiscovery (34).

FIGURE 27.38. Gallbladder Carcinoma. Postcontrast CT shows anenhancing soft tissue mass (arrow) within the lumen of the gallbladder. Directinvasion of tumor into the adjacent liver parenchyma is evident (arrowhead).
REFERENCES
1. Colagrande S, Centi N, La Villa G, Villari N. Transient hepatic attenuation differences. AJR Am JRoentgenol 2004;183:459–464.
2. Yoshimitsu K, Honda H, Kuroiwa T, Irie H, et al. Unusual hemodynamics and pseudolesions of thenoncirrhotic liver at CT. Radiographics 2001;21:S81-S96.
3. Mortele KJ, Segatto E, Ros PR. The infected liver: radiologic-pathologic correlation. Radiographics2004;24:937–955.
4. Dodd GDI, Baron RL, Oliver JHI, Federle MP. Spectrum of imaging findings of the liver in end-stagecirrhosis: part II, focal abnormalities. AJR Am J Roentgenol 1999;173:1185–1192.
5. Dodd GDI, Baron RL, Oliver JHI, Federle MP. Spectrum of imaging findings of the liver in end-stagecirrhosis: part I, gross morphology and diffuse abnormalities. AJR Am J Roentgenol 1999;173:1031–1036.
6. Gupta AA, Kim DC, Krinsky GA, Lee VS. CT and MRI of cirrhosis and its mimics. AJR Am JRoentgenol 2004;183:1595–1601.
7. Hussain SM, Zondervan PE, Ijzermans JNM, Schalm SW, et al. Benign versus malignant hepaticnodules: MR imaging findings with pathologic correlation. Radiographics 2002;22:1023–1039.
8. Gallego C, Velasco M, Marcuello P, Tejedor D, De Campo L, Friera A. Congenital and acquiredanomalies of the portal venous system. Radiographics 2003;22:141–159.
9. Brancatelli G, Federle MP, Graziola L, Golfieri R, Lencioni R. Benign regenerative nodules in Budd-Chiari syndrome and other vascular disorders of the liver: radiologic-pathologic and clinical correlation.Radiographics 2002;22:847–862.
10. Tani I, Kurihara Y, Kawaguchi A, et al. MR imaging of diffuse liver disease. AJR Am J Roentgenol2000;174:965–971.
11. Sica GT, Ji H, Ros PR. CT and MR imaging of hepatic metastases. AJR Am J Roentgenol

2000;174:691–698.
12. Vilgrain M, Boulos L, Vullierme M-P, Denys A, Terris B, Menu Y. Imaging of atypical hemangiomasof the liver with pathologic correlation. Radiographics 2000;20:379–397.
13. Lee KHY, O’Malley MEO, Kachura JR, Haider M, Hanbidge A. Hepatocellular carcinoma: imagingand imaging-guided intervention. AJR Am J Roentgenol 2003;180:1015–1022.
14. Prasad SR, Wang H, Rosas H, et al. Fat-containing lesions of the liver: radiologic-pathologiccorrelation. Radiographics 2005;25:321–331.
15. Hussain SM, Terkivatan T, Zondervan PE, et al. Focal nodular hyperplasia: findings at state-of-the-art MR imaging, US, CT, and pathologic analysis. Radiographics 2004;24:3–19.
16. Graziola L, Federle MP, Brancatelli G, et al. Hepatic adenomas: imaging and pathologic findings.Radiographics 2001;21:877–894.
17. McLarney JK, Rucker PT, Bender GN, et al. Fibrolamellar carcinoma of the liver: radiologic-pathologic correlation. Radiographics 1999;19:453–471.
18. Mortele KJ, Ros PR. Cystic focal liver lesions in the adult: differential CT and MR imaging features.Radiographics 2001;21:895–910.
19. Kawamoto S, Soyer PA, Fishman EK, Bluemke DA. Nonneoplastic liver disease: evaluation with CTand MR imaging. Radiographics 1998;18:827–848.
20. Schwartz LH, Gandras EJ, Colangelo SM, Ercolani MC, Panicek DM. Prevalence and importance ofsmall hepatic lesions found at CT in patients with cancer. Radiology 1999;210:71–74.
21. Jara H, Barish MA. MR cholangiopancreatography techniques. Semin Ultrasound CT MRI1999;20:281–293.
22. Mortele KJ, Ros PR. Anatomic variants of the biliary tree: MR cholangiographic findings and clinicalapplications. AJR Am J Roentgenol 2001;177:389–394.
23. Soto JA, Alvarez O, Lopera JE, et al. Biliary obstruction: findings at MR cholangiography and cross-sectional MR imaging. Radiographics 2000;20:353–366.
24. Miller FH, Hwang CM, Gabriel H, Goodhartz LA, Omar AJ, Parsons WG III. Contrast-enhanced

P.781
helical CT of choledocholithiasis. AJR Am J Roentgenol 2003;181:125–130.
25. Choi SH, Han JK, Lee JM, et al. Differentiating malignant from benign common bile duct stricturewith multiphasic helical CT. Radiology 2005;236:178–183.
26. Vitellas KM, Keogan MT, Freed KS, et al. Radiologic manifestations of sclerosing cholangitis withemphasis on MR cholangiopancreatography. Radiographics 2000;20:959–975.
27. Lim JH. Oriental cholangiohepatitis: pathologic, clinical, and radiologic features. AJR Am JRoentgenol 1991;157:1–8.
28. Levy AD, Rohrmann CA Jr, Murakata LA, Lonergan GJ. Caroli's disease: radiologic spectrum withpathologic correlation. AJR Am J Roentgenol 2002;179:1053–1057.
29. Kim OH, Chung HJ, Choi BG. Imaging of the choledochal cyst. Radiographics 1995;15:69–88.
30. Lim JH. Cholangiocarcinoma: morphologic classification according to growth pattern and imagingfindings. AJR Am J Roentgenol 2003;181:819–827.
31. Grand D, Horton KM, Fishman EK. CT of the gallbladder: spectrum of disease. AJR Am JRoentgenol 2004;183:163–170.
32. Bortoff GA, Chen MYM, Ott DJ, Wolfman NT, Routh WD. Gallbladder stones: imaging andintervention. Radiographics 2000;20:751–766.
33. Levy AD, Murakata LA, Abbott RM, Rohrmann CA Jr. Benign tumors and tumorlike lesions of thegallbladder and extrahepatic bile ducts: radiologic-pathologic correlation. Radiographics 2002;22: 387–413.
34. Levy AD, Murkata LA, Rohrmann CA Jr. Gallbladder carcinoma: radiologic-pathologic correlation.Radiographics 2001;21:295–314.