LIVER, BILIARY TRACT & PANCREAS, CPC-2 INSTRUCTOR …Robbins Pathologic Basis of Disease (9. th....
38
1 GOALS AND OBJECTIVES: GOALS 1. The primary goal of the laboratory is to illustrate and supplement the material presented in the textbook and lecture with the characteristics of the most important hepatic, biliary tract and pancreatic disorders. 2. The secondary goal of the laboratory is to develop skills needed to become a competent physician, including interpreting gross and microscopic abnormalities, analysis and interpretation of medical literature, and integration of basic scientific knowledge with clinical signs, symptoms, and disease course and test results. OBJECTIVES 1. Analyze the appearance of the gross and microscopic specimens presented and discussed in the laboratory with particular emphasis on disorders related to hepatitis, cirrhosis, cholelithiasis, pancreatitis and neoplasia. Relate the appearance to the etiology, pathogenesis, clinical presentation and course of each condition illustrated. 2. Read and discuss the paper on the pathogenesis of non-alcoholic fatty liver disease and non- alcoholic steatohepatitis with emphasis on the pathogenic mechanisms involved. 3. Review the assigned cases on Aperio. For each condition discussed, review the clinical presentation, gross and microscopic features, pathogenesis and clinical course. MANDATORY READING: 1. Robbins Pathologic Basis of Disease (9 th edition), Chapter 18 (Liver and Gallbladder) and Chapter 19 (The pancreas) a. Liver Pathology (chapter 18): • Liver Failure (acute and chronic liver failure/cirrhosis), pages 825-831 • Alcoholic liver disease, pages 842-845 • Non-Alcoholic Fatty Liver Disease (NAFLD), pages 845-847 (supplemental for paper) • Hemochromatosis, pages 847-849 • Alpha-1 antitrypsin deficiency, pages 850-852 (supplemental for paper) • Liver nodules and tumors (benign and malignant tumors), pages 867-875 a. Gallbladder (chapter 18): • Acute and chronic cholecystitis including gallstones, pages 875-879 b. Pancreas (Chapter 19): • Acute and chronic pancreatitis, pages 884-889 • Pancreatic carcinoma, pages 892-895 LIVER, BILIARY TRACT & PANCREAS, CPC-2 INSTRUCTOR HANDOUT
Transcript of LIVER, BILIARY TRACT & PANCREAS, CPC-2 INSTRUCTOR …Robbins Pathologic Basis of Disease (9. th....

1
GOALS AND OBJECTIVES:
GOALS
1. The primary goal of the laboratory is to illustrate and supplement the material presented in the textbook and lecture with the characteristics of the most important hepatic, biliary tract and pancreatic disorders.
2. The secondary goal of the laboratory is to develop skills needed to become a competent physician, including interpreting gross and microscopic abnormalities, analysis and interpretation of medical literature, and integration of basic scientific knowledge with clinical signs, symptoms, and disease course and test results.
OBJECTIVES
1. Analyze the appearance of the gross and microscopic specimens presented and discussed in the laboratory with particular emphasis on disorders related to hepatitis, cirrhosis, cholelithiasis, pancreatitis and neoplasia. Relate the appearance to the etiology, pathogenesis, clinical presentation and course of each condition illustrated.
2. Read and discuss the paper on the pathogenesis of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis with emphasis on the pathogenic mechanisms involved.
3. Review the assigned cases on Aperio. For each condition discussed, review the clinical presentation, gross and microscopic features, pathogenesis and clinical course.
MANDATORY READING:
1. Robbins Pathologic Basis of Disease (9th edition), Chapter 18 (Liver and Gallbladder) and Chapter 19 (The pancreas) a. Liver Pathology (chapter 18):
• Liver Failure (acute and chronic liver failure/cirrhosis), pages 825-831 • Alcoholic liver disease, pages 842-845 • Non-Alcoholic Fatty Liver Disease (NAFLD), pages 845-847 (supplemental for paper) • Hemochromatosis, pages 847-849 • Alpha-1 antitrypsin deficiency, pages 850-852 (supplemental for paper) • Liver nodules and tumors (benign and malignant tumors), pages 867-875
a. Gallbladder (chapter 18): • Acute and chronic cholecystitis including gallstones, pages 875-879
b. Pancreas (Chapter 19): • Acute and chronic pancreatitis, pages 884-889 • Pancreatic carcinoma, pages 892-895
LIVER, BILIARY TRACT & PANCREAS, CPC-2
INSTRUCTOR HANDOUT

2
2. Lecture notes: a. Pathology of Liver diseases I, II, III, IV. Four lectures by Dr. Leibowitz. Friday, September 27th and
Monday September 30. b. Pathology – Pancreas and Biliary tract. Dr. Stern. Monday September 30.
3. Gross guide: separate document posted on e-campus
4. Papers: posted on e-campus.
a. Human Fatty Liver Disease: Old Questions and New Insights. Science 2011; 332:1519-1523. Jonathan C. Cohen, et al.
b. Supplemental (optional): Alpha-1 antitrypsin deficiency. Respiratory Medicine 2010; 104: 763-772. Emer Kelly et al.

3
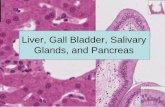
REVIEW OF NORMAL LIVER (Aperio # 605)
Use this slide as your reference to compare pathology slides with normal histology. Normal weight: 1400-1600gr. HEPATIC LOBULE: Liver is divided into hexagonal lobules oriented around the terminal hepatic veins with portal tracts at the periphery of the lobule. The hepatocytes in the vicinity of the lobule are called “centrilobular”, and those near to the portal tract are “periportal”. HEPATIC ACINI: There is a triangular zone (see diagram) divided in 3 zones. Zone 1 is the closest to the vascular supply, Zone 3 closest to hepatic venule and Zone 2 in between the previous two.
While the acinar model best describes the physiologic relationships between hepatocytes and their vascular supply, the histopathology of the liver is usually discussed on the basis of a lobular architecture.
Microscopic anatomy of the liver; the two models, hepatic lobular model and acinar model, are illustrated. In the lobular model the terminal hepatic vein (CV) is at the center of a "lobule," while the portal tracts (PV) are at the periphery. Pathologists refer to the regions of the parenchyma as "periportal and centrilobular." In the acinar model, on the basis of blood flow, three zones can be defined, zone 1 being the closest to the blood supply and zone 3 being the farthest. BD, bile duct; HA, hepatic artery.
HISTOLOGY: Hepatocytes are organized into cribriform, anastomosing sheets or “plates” extending from portal tracts to the terminal hepatic veins. Between the plates of hepatocytes are vascular sinusoids. Blood traverses the sinusoids and exits into the hepatic vein. Fenestrated and discontinuous endothelial cells line the sinusoids. Deep to the endothelial cells lays the space of Disse. Scattered Kupffer cells of the mononuclear phagocyte system are attached to the luminal face of endothelial cells, and fat-containing hepatic stellate cells (HSCs) are found in the space of Disse. Between abutting hepatocytes are bile canaliculi, which are channels 1

4
to 2um in diameter, formed by grooves in the plasma membranes of facing hepatocytes and separated from the vascular space by tight junctions.

5
1) CIRRHOSIS A 55-year-old man presents to the Emergency Department because of abdominal swelling, pain and fever.
He has a 25-year history of alcohol ingestion (approximately 1 six-pack of beer daily, more on weekends) and has noticed a yellow tinge in his eyes. His abdomen started swelling 2 months ago and it has become progressively worse. He also has had swelling of his ankles. Two days ago, he developed fever and chills. He has generalized soreness of his abdomen. His weight has increased by 20 pounds in the last two months.
Current medications include a multivitamin tablet. He has been using acetaminophen 650 mg four times a day for aches and fever.
Physical examination shows a middle-aged man who appears older than his stated age. Temperature 100.5 oF, pulse 96/min and regular, respirations 16/min, BP 105/70. Skin: mild icterus, (+) spider angiomata. HEENT: scleral icterus. Chest: clear to auscultation. Heart: regular rhythm, no murmur. Abdomen: distended, (+) fluid wave and shifting dullness, abdominal girth 120 cm (47 inches), liver edge not palpable, spleen tip is palpable 10 cm below left costal margin, diffuse tenderness, no rebound tenderness, bowel sounds active. Extremities: ++ pitting edema to knees. Neurological examination: alert, oriented, no asterixis.
Laboratory testing:
CBC: Hemoglobin 10.5 g/dL, hematocrit 31%, WBC 12,000 with 76% segmented neutrophils, 14% lymphocytes, 5% monocytes, 2% eosinophils, 3% monocytes. Platelet count 80,000.
CMP: Sodium 138 mmol/L, potassium 5 mmol/L, chloride 105 mmol/L, bicarbonate 30 mmol/L, BUN 15 mg/dL, creatinine 0.9 mg/dL, ALT 25 units/L, AST 40 units/L, alkaline phosphatase 100 units/L, bilirubin level 1.8 mg/dL.
Imaging:
Abdominal sonography: marked ascites, small liver with coarse texture, large spleen.
GROSS: Liver with nodular cirrhosis Explanations on gross guide (posted on e-campus)

6
GROSS QUESTIONS:
1. According to nodule size, how is cirrhosis classified (refer to lectures titled “Pathology of Liver Disease I-IV)?
a. Micronodular: <3mm b. Macronodular: >3mm and mixed.
2. What are the main diseases leading to cirrhosis? Alcoholic liver disease, Viral hepatitis, Extrahepatic biliary obstruction, Primary biliary cirrhosis, Hemochromatosis, Wilson’s disease, Alpha-1 antitrypsin deficiency, Cystic fibrosis, other inherited metabolic defects, Drug-induced, Non-alcoholic steatohepatitis, cryptogenic (unknown etiology).
3. How do cirrhotic patients present clinically? (Robbins) 40% of patients are asymptomatic until late in the course of disease. When symptomatic, earlier in the disease they present with non-specific clinical manifestations: anorexia, weight loss, weakness and in advanced disease they present with s/s of portal hypertension: esophageal varices and hemorrhage, hemorroidal varices, hepatic encephalopathy, splenomegaly, testicular atrophy, gynecomastia and ascites.
4. What do cirrhotic patients die of? (Robbins) • Progressive liver failure • Complications related to portal hypertension • Development of hepatocellular carcinoma

7
SLIDES TO REVIEW: Biopsy: # 755 (H&E) and #756 (trichrome)
Resection: #141 (H&E) and Aperio #140 (trichrome)
ORIENTATION TO SLIDE: Biopsy #755 shows 5 core fragments. The middle core fragment is the closest to normal liver parenchyma. Slide #141 shows central liver parenchyma, no liver capsule is present.
ABNORMAL CHANGES: At low power both liver biopsy and resection show a nodular architecture. Nests and groups of hepatocytes are surrounded by bands of collagenous connective tissue. Use special stain (trichrome) #140 and #756 for better recognition and appreciation of fibrous bands. This collagen bands contain bile ducts and blood vessels. Only sinusoids are present within cirrhotic nodules, no bile ducts or blood vessels are inside the nodules. At medium and high power observe hepatocytes, the majority contain fat, however no definitive signs of inflammation “hepatitis” including necrotic hepatocytes and neutrophils, are present within the cirrhotic nodules.
Checklist (have you seen the following structures):
__ Bridging fibrous septa
__ Parenchymal nodules containing groups of hepatocytes encircled by fibrosis, “regenerative nodules”
QUESTIONS:
5. According to Robbins, cirrhosis as the end stage of chronic liver disease, is defined by three main morphologic characteristics, name them:
• Bridging fibrous septa (fibrosis is the key feature of progressive damage of the liver) • Parenchymal nodules containing hepatocytes encircled by fibrosis. • Disruption of the architecture of the entire liver. The parenchymal injury and consequent
fibrosis are diffuse, extending throughout the liver. Focal injury DOES NOT constitute cirrhosis.
6. In normal liver, interstitial collagens (types I and III) are concentrated in portal tracts and around central veins, and thin strands of type IV collagen are present in the space of Disse. What happens in cirrhosis? (Robbins) Type I and II collagen are deposited in the space of Disse, creating fibrotic septal tracts.
7. The predominant mechanism of fibrosis is the proliferation of hepatic stellate cells and their activation into fibrogenic cells. This proliferation is initiated by: platelet-derived growth factor receptor b (PDGFR-b) from stellate cell and cytokines and chemokines by Kupffer cells and lymphocytes (Robbins).
8. Review the pathogenesis of cirrhosis, Figure 18-2 (page 837) 9. What are the three main types of portal hypertension (refer to lectures titled “Pathology of Liver
Disease I-IV)? • Pre-hepatic: thrombosis of portal vein with splenomegaly. • Post-hepatic: cardiac and hepatic vein outflow obstruction. • Hepatic: cirrhosis, schistosomiasis, granulomatous diseases (TB, sarcoid).
10. What is ascites? What percentage of ascites is caused by cirrhosis? (Robbins) Ascites is the accumulation of excess fluid in the peritoneal cavity. In 85% of cases ascites is caused by cirrhosis.
11. If numerous neutrophils are present on ascitic fluid, what is the diagnosis? Secondary peritonitis.

8
2) HEMOCHROMATOSIS A 50-year-old man presents to his internist with shortness of breath on exertion and fatigue.
He has had a hard time climbing more than one flight of stairs for the last three months and can no longer play tennis. He notes swollen ankles each evening. He gets up once or twice a night to urinate. He has no history of hypertension or heart murmur.
Physical examination shows a tanned middle-aged man who is in no distress. Temperature 98 oF, pulse 96/min and regular, respirations 18/min, BP 105/80. Skin: well-tanned, even in areas not exposed to sunlight. HEENT: not icteric, mucosa moist. Neck: supple, jugular venous distention at base of neck, no thyromegaly. Chest: soft, bibasilar rales. Heart: regular rhythm, no murmur, (+) S4, point of maximal impulse diffuse and centered at anterior axillary line. Abdomen: soft, not distended, (+) bowel sounds, liver span 12 cm in midclavicular line, spleen not palpable, no tenderness or mass. Urological examination: small testes. Extremities: (+) peripheral edema to mid-calf bilaterally. Neurological examination: non-focal.
Laboratory testing:
CBC: Hemoglobin 15.5 g/dL, hematocrit 48%, WBC 8,000 with 70% segmented neutrophils, 24% lymphocytes, 2% eosinophils, 4% monocytes. Platelet count 150,000.
CMP: Sodium 142 mmol/L, potassium 4 mmol/L, chloride 105 mmol/L, bicarbonate 26 mmol/L, BUN 10 mg/dL, creatinine 1.1 mg/dL, ALT 60 units/L, AST 70 units/L, alkaline phosphatase 110 units/L, bilirubin level 1.2 mg/dL.
Other tests: Thyroid stimulating hormone 2 mU/L, thyroxine 6 µg/dL, serum iron level 190 µg/dL, total iron binding capacity 240 µg/dL, and serum ferritin 1020 ng/mL.
Imaging:
Chest x-ray shows mild cardiomegaly and pulmonary congestion consistent with heart failure.
CT scan of the abdomen shows hyperdense liver.

9
GROSS: Explanations on gross guide (posted on e-campus)

10
GROSS QUESTIONS:
1. What are the gross characteristics of a liver with hemochromatosis (refer to lectures titled “Pathology of Liver Disease I-IV)? Enlarged liver, red-brown color, micronodular cirrhosis.
2. How do patients with hemochromatosis present? Hepatomegaly, abnormal pain, skin pigmentation, diabetes Mellitus, heart dysfunction.
3. What other organs show deposition of hemosiderin (refer to lectures titled “Pathology of Liver Disease I-IV and Robbins)?
• Pancreas: hemosiderin deposits in islet cells and acinar cells. • Heart: enlarged brown color, hemosiderin deposits in myocytes, interstitial fibrosis • Endocrine (pituitary, adrenal, thyroid and parathyroid) glands: Low gonadotropin gonadal
insufficiency (testicular atrophy). • Joints: Hemosiderin deposits in synovium, pyrophosphate deposition with damage to
articular cartilage and pseudogouty arthritis. • Skin: Increased melanin in basal melanocytes. Only about 50% of patients will have
detectable iron deposits in dermis. 4. What is the age/ sex predilection of hemochromatosis (refer to lectures titled “Pathology of Liver
Disease I-IV and Robbins)? Primarily affects males, onset after age 40. 5. According to Robbins and lectures titled “Pathology of Liver Disease I-IV”, fully developed cases of
hemochromatosis (classic triad) exhibit: • Hepatomegaly • Skin pigmentation • Diabetes
6. What percentage of patients develops hepatocellular carcinoma (refer to lectures titled “Pathology of Liver Disease I-IV)? 15%
SLIDE TO REVIEW: Aperio slide # 143
ORIENTATION TO SLIDE: This is an H&E section of liver with capsule on the right side.
ABNORMAL CHANGES: The changes are similar to slide of cirrhotic liver except that there is more fibrous tissue; many nodules are larger and contain central veins or portal zones (macronodules). At medium and high power, brown granular pigment is present throughout the parenchymal cells(hepatocytes) and occasionally also within interstitial macrophages. If a Prussian blue stain is performed (see picture below) the hepatocellular iron will be blue. There is no pigment accumulation in the bile ducts or canaliculi as would be seen in biliary stasis/cirrhosis. There is no inflammation “hepatitis” within the tissue.
Checklist (have you seen the following structures):
__ Hemosiderin granules (brown granular pigment) within cytoplasm

11
QUESTIONS:
7. What is the inheritance of primary hemochromatosis? Where is the mutation(s) located? What are the consequences of gene mutation? (refer to lectures titled “Pathology of Liver Disease I-IV and Robbins) Homozygous-recessive inherited disorder. The adult form of hemochromatosis is almost always caused by mutations of HFE, a gene located on the short arm of chromosome 6. It encodes an HLA class-I like molecule that regulates intestinal absorption of dietary iron.
8. What proteins are involved in iron metabolism? (Robbins) Hemojuvelin (from liver, heart and skeletal muscle), transferrin receptor 2 (from hepatocytes), HFER the product of the hemochromatosis gene.
9. What are the normal ranges of total body iron? What is the number for patients with hemochromatosis? When do symptoms occur (refer to lectures titled “Pathology of Liver Disease I-IV and Robbins)? Normal: 2-6gr (98% in hepatocytes). In hemochromatosis total iron accumulation >50gr (1/3 in liver). Symptoms at >20gr
10. What are the Iron mechanisms of toxicity? (Robbins) • Lipid peroxidation via iron-catalyzed free radical reactions • Stimulation of collagen formation by activation of hepatic stellate cells • Interaction of reactive oxygen species and of iron itself with DNA, leading to lethal cell injury
or predisposition to hepatocellular carcinoma. 11. What are the causes of secondary hemochromatosis (refer to lectures titled “Pathology of Liver Disease
I-IV)? • Anemia with ineffective erythropoiesis (thalassemia major, aplastic anemia, sideroblastic
anemia). • Multiple blood transfusions, chronic liver disease, high-oral iron intake (excessive medicinal
iron). 12. What special stain is used to better see the hemosiderin granules (see special stain picture below)?
(Robbins) Prussian Blue
13. Can you tell the difference between hepatocellular pigment of cholestasis and hepatocellular pigment of hemochromatosis on H&E? No. They both show accumulation of pigment in the hepatic parenchyma. Cholestasis tends to show brown plugs of bile within bile canaliculi.
14. What is the main difference between hemochromatosis and hemosiderosis? Hemochromatosis is hereditary; hemosiderosis (secondary hemochromatosis) is acquired
15. What are the changes in other organs like pancreas, heart, skin, endocrine glands and joints?

12
• Pancreas: hemosiderin deposits in islet cells and acinar cells. • Heart: enlarged brown color, hemosiderin deposits in myocytes, interstitial fibrosis • Endocrine (pituitary, adrenal, thyroid and parathyroid) glands: Low gonadotropin gonadal
insufficiency (testicular atrophy). • Joints: Hemosiderin deposits in synovium, pyrophosphate deposition with damage to
articular cartilage and pseudogouty arthritis. • Skin: Increased melanin in basal melanocytes. Only about 50% of patients will have
detectable iron deposits in dermis.
16. What do patients with hemochromatosis usually die of? (Robbins) Cirrhosis or cardiac disease 17. What are the screening labs for suspicious cases? (Robbins) Serum iron and ferritin, liver biopsy if
indicated with biochemical determination of hepatic tissue iron concentration. 18. What is the treatment? Regular phlebotomy

13
3) Alpha-1 ANTITRYPSIN DEFICIENCY A 32-year-old woman presents to her physician’s office with jaundice present for a few weeks.
She has no history of liver disease, drug use or abuse, transfusion, foreign travel, exposure to jaundiced persons or alcohol abuse. She has no abdominal pain, fever or chills.
Physical examination reveals a jaundiced woman who appears in no distress. Physical examination is otherwise normal except for icteric sclera and detection of a non-tender liver edge 3 cm below the right costal margin.
Laboratory tests and sonogram of the abdomen are ordered.
Laboratory tests:
CBC: Hemoglobin 12.5 g/dL, hematocrit 38%, WBC 8,000 with 60% segmented neutrophils, 28% lymphocytes, 8% monocytes, 4% basophils. Platelet count 150,000. Reticulocyte count 1%.
CMP: Sodium 140 mmol/L, potassium 4.5 mmol/L, chloride 100 mmol/L, bicarbonate 26 mmol/L, BUN 8 mg/dL, creatinine. 0.9 mg/dL, ALT 1200 units/L, AST 140 units/L, alkaline phosphatase 90 units/L, bilirubin level 4.5 mg/dL.
Hepatitis A, hepatitis B and hepatitis C serologic tests were negative except for positive hepatitis B surface antibody (previously immunized).
Iron level, total iron binding capacity, and ferritin were normal.
Antinuclear antibodies, antimitochondrial antibodies, and serum globulin levels were normal.
Serum ceruloplasmin level was normal.
Serum alpha-1 antitrypsin level was 52 mg/dL (normal range: 100 – 300 mg/dL) and phenotype was PiMZ (normal phenotype: PiMM).
SLIDE TO REVIEW: Aperio slide # 671.
ORIENTATION TO SLIDE: Sections show a cirrhotic liver. Mild chronic inflammation is seen within the fibrous connective bands surrounding the cirrhotic nodules.
ABNORMAL CHANGES: At low power there is a pattern of micronodular cirrhosis with expansile as well as bridging fibrosis of portal tracts. At high power some hepatocytes are enlarged and contain bright eosinophilic (pink) intracytoplasmic globules. These globules can be highlighted by periodic acid-Schiff “PAS” or immunostain (not available for this Aperio case, see picture below). No histologic evidence of inflammation is seen, including, necrotic hepatocytes, lymphocytes or neutrophils.
Checklist (have you seen the following structures):
__ Round cytoplasmic eosinophilic (pink) globular inclusions on hepatocytes.

14
QUESTIONS:
1. Where is the enzyme alpha-1 antitrypsin produced? What is the protein’s main function? (Robbins) • Is a plasma glycoprotein synthesized by hepatocytes. • The major function is the inhibition of proteases (neutrophil elastase, cathepsin G, and
proteinase) which are normally released from neutrophils at sites of inflammation. 2. What are the main organs involved by the disease? (Robbins) Lungs and liver 3. What is the inheritance of the disease? Autosomal recessive 4. What is the most common alpha-1 antitrypsin genotype? (Robbins) PiMM (90%) 5. What is the most common clinically significant mutation? (Robbins) Homozygotes PiZZ 6. What special stain is used to highlight the inclusions (stain shown in these pictures)? Periodic acid
Schiff (PAS)
7. Are inclusions “pathognomonic of alpha-1-antitrypsin disease? What other tests/labs should be ordered? No, get serum alpha-1 antitrypsin levels and phenotype (also get other labs to exclude other liver diseases- see clinical vignette)
8. What percentage of PiZZ adults develops Hepatocellular carcinoma? (Robbins) 2-3% 9. What type of emphysema is present in patients with alpha-1 antitrypsin deficiency? (Respiratory block)
Panacinar emphysema.

15
4) HEPATOCELLULAR CARCINOMA A 30-year-old woman presents to the doctor’s office for follow-up of hepatitis B.
She immigrated from China to the United States at age 3. Her mother had hepatitis B and the patient was tested for hepatitis at age 15 when her mother died from complications of cirrhosis. She was given treatment with antiviral therapy, but she failed to respond. Her doctor suggested that she come in yearly for follow-up. Each year she had liver and viral tests and sonogram testing. Tests showed modest elevation of ALT and AST, normal albumin and prothrombin time (INR), normal alpha-fetoprotein level, persistent viremia, and stable nodularity of the liver consistent with cirrhosis.
At the time of this year’s visit, she related no symptoms or change in functional status. Physical examination is stable.
Laboratory tests:
CBC: Hemoglobin 11.5 g/dL, hematocrit 34%, WBC 10,000 with a normal differential. Platelet count 90,000.
CMP: Sodium 142 mmol/L, potassium 3.8 mmol/L, chloride 107 mmol/L, bicarbonate 28 mmol/L, BUN 7 mg/dL, creatinine 0.8 mg/dL, ALT 95 units/L, AST 100 units/L, alkaline phosphatase 120 units/L, bilirubin level 1.5 mg/dL.
Alpha-fetoprotein level: 450 ng/mL (normal: <10 ng/mL)
Imaging:
Abdominal sonography: Small liver with coarse texture, more prominent nodule in right lobe. CT scan to evaluate further.

16
GROSS: Different patterns of HCC Explanations on gross guide (posted on e-campus)
GROSS QUESTIONS
1. What is the most common “malignant tumor” seen in the liver (refer to lectures titled “Pathology of Liver Disease I-IV)? Metastatic carcinoma (GI tract, breast, lung, pancreas).
2. What are the two main carcinomas that arise in the liver? (Robbins) HCC, cholangiocarcinoma 3. According to Robbins what are the four major etiologic factors associated with Hepatocellular
carcinoma (HCC)? • Chronic viral infection (HBV,HCV) • Chronic alcoholism • Non-alcoholic steatohepatitis (NASH) • Food contaminants (aflatoxins)
4. What virus is strongly associated with the development of HCC in eastern countries versus western
countries? Eastern- HBV, Western- HCV 5. What percentage of HCC occurs in cirrhotic livers (western world)? (refer to lectures titled “Pathology of
Liver Disease I-IV) 75-90% 6. According to Robbins what are the three gross patterns of presentation of HCC? See gross images above
• Unifocal • Multifocal • Diffusely infiltrate

17
7. What is the primary metastatic route (outside liver)? Vascular invasion (hepatic vein) but hematogenous metastasis (lung) occur later in the disease.
SLIDE TO REVIEW: Aperio slide #142.
ORIENTATION TO SLIDE: This is a section of abnormal liver including liver capsule on top. Almost the entire slide is composed of tumor. A few strands of compressed non-neoplastic liver parenchyma are present on the left side.
ABNORMAL CHANGES: Large nodules of altered hepatocytes comprise most of the section. Tumoral hepatocytes are arranged in cords, 3-4 cells thick (normal hepatocytes do not show more than 2 to 3 cell thickness). Tumor cells show clear cytoplasm (have less granulation than normal hepatocytes), irregular nuclei shape and prominent nucleoli. Mitoses can be seen occasionally. Bile plugs can be found in canaliculi-like locations.
Check list (have you seen the following structures):
__ Tumor cells with “hepatocyte-like” appearance, clear cytoplasm and increased nucleo-cytoplasmic ratio.
QUESTIONS:
8. Histologically how are the tumor cells arranged on well to moderately differentiated tumors? (Robbins) Trabecular, acinar or glandular pattern (example: the aperio case).
9. Describe the variant “fibrolamellar HCC”? Age of presentation, association with chronic liver disease and prognosis. 5% of HCC. It occurs in young males and female adults (20-40y/o). Patients usually do not have underlying chronic liver disease, and the prognosis is better than conventional HCC.
10. Levels of what serum marker are elevated in patients with HCC? What other tumors can show elevated levels of the same marker? Serum alpha-fetoprotein can be present in yolk sac tumors.
11. What is the overall prognosis of patients with this tumor (5-year survival)? The majority of patients die within 2 years.
Main HCC types:
1) “Classic type”:

18
2) Fibrolamellar type:

19
5) ACUTE AND CHRONIC CHOLECYSTITIS/ CHOLELITHIASIS A 48-year-old-woman presents to the emergency department at 1 AM with the acute onset of right-upper-quadrant abdominal pain.
The pain started at 10 PM and was mild initially, “like bad indigestion,” but rapidly intensified. It is associated with nausea, but she has not vomited. She has had no fever or chills.
Physical examination shows a middle-aged woman who seems uncomfortable. Temperature 99 oF, pulse 104, respirations 18 and shallow, BP 130/85, height 66 inches, weight 150 pounds. Skin: warm and dry. HEENT: not icteric, mucosae moist. Chest: clear. Heart: regular rhythm, no murmur. Abdomen: soft, no organomegaly. Tender in RUQ with inspiratory arrest during palpation (Murphy’s sign), modest rebound tenderness in RUQ. Bowel sounds quiet. Extremities: no edema.
Laboratory testing:
CBC: Hemoglobin 13.5 g/dL, hematocrit 39%, WBC 12,000 with 70% segmented neutrophils, 10% bands, 20% lymphocytes. Platelet count 150,000.
CMP: Sodium 142 mmol/L, potassium 4 mmol/L, chloride 105 mmol/L, bicarbonate 24 mmol/L, BUN 12 mg/dL, creatinine 1.1 mg/dL, ALT 30 units/L, AST 40 units/L, alkaline phosphatase 110 units/L, bilirubin level 1.0 mg/dL, lipase 80 U/L (normal: 0 – 160 U/L).
Imaging:
Abdominal sonography: Enlarged gallbladder with thickening of its wall, pericholecystic fluid, cholelithiasis with stone in neck of gallbladder, extrahepatic bile duct not enlarged.

20
Gross: Explanations on gross guide (posted on e-campus)
GROSS QUESTIONS:
1. Describe the morphology of both pictures ( two types of stones) shown in the above pictures. • Cholesterol stones (top): light yellow to brown, rather large • Pigment stones (below): black or brown, small
2. What percentage of adults have gallstones in developed countries? (Robbins)10-20% 3. What percentage of gallstones are “symptomatic”? (Robbins) 20% only (80% asymptomatic) 4. When symptomatic how do patients present clinically? (Robbins) Biliary pain: constant or colicky,
radiating into right shoulder. 5. What are the two main types of stones? What are they composed of? What are the main risk factors of
one vs the other one? • Cholesterol Stones: western countries, females, oral contraceptive use, pregnancy. Obesity,
rapid weight loss. Hyperlipidemia. • Pigment Stones: Asians more than western. Biliary infections. Chronic hemolysis.
6. How do stones look on radiology? (Robbins) • Stones composed largely of cholesterol are radiolucent; sufficient calcium carbonate is found
in 10% to 20% of cholesterol stones to render them radiopaque. • 50-75% of blackstones are radiopaque.

21
7. If you see black/brown pigmented stones, what diseases should be included in your differential diagnosis? Disorders that are associated with elevated levels of unconjugated bilirubin, such as hemolytic syndromes
SLIDES TO REVIEW: Aperio slide # 753 (acute cholecystitis)
ORIENTATION TO SLIDE: This is a full- thickness section of the wall of the gallbladder.
ABNORMAL CHANGES: The normal gallbladder architecture is entirely replaced by necrosis, acute inflammation (with neutrophils) and fibrosis. The inflammation is transmural (involving the entire wall from mucosa to serosa). This is a severe case of acute cholecystitis with a high risk of organ perforation and secondary peritonitis.
Check list (have you seen the following structures):
__ Inflammatory cells (neutrophils) within the entire gallbladder thickness
_______________________________________________________________________________________
SLIDES TO REVIEW: Aperio slide # 754 (chronic cholecystitis)
ORIENTATION TO SLIDE: This is a full- thickness section of the wall of the gallbladder
ABNORMAL CHANGES: This case shows mild inflammation in comparison with previous one. Here the inflammation is due to lymphocytes and plasma cells within lamina propria. The reactive mucosa causes outpunching of the epithelium with invagination into the lamina propria and muscularis (Rokitansky Aschoff sinuses). Within the lamina propria you will see foamy histiocytes containing intracellular fat. This process is called cholesterolosis and is an indication that calculi were probably present within the lumen of the gallbladder.
Check list (have you seen the following structures):
__ Inflammatory cells (lymphocytes and plasma cells) within lamina propria
__ Rokitansky-Aschoff sinuses (outpunching of the mucosa)
QUESTIONS:
8. What percentage of cholecystitis is not associated with stones “acalculous cholecystitis”? What are the risk factors for “acalculous cholecystitis”? (Robbins) 10%. Ischemia (inflammation and edema of the wall comprising slow flow) gallbladder stasis, accumulation of microcrystals of cholesterol, viscous bile.
9. What are the most common risk factors for cholelithiasis (Rule 4 F’s): Female, forty, fertile, fat. 10. How do patients with acute/chronic cholecystitis usually present? (Robbins) Right upper quadrant or
epigastric pain, mild fever, anorexia, tachycardia, nausea/vomiting 11. Name the components of Charcot’s triad of cholangitis:
• Biliary pain

22
• Spiking fevers • Jaundice
12. What are the complications of acute cholecystitis? Acute cholangitis (infection of biliary tract), emphyema, perforation, fistulas, acute pancreatitis, galbladder CA.

23
6) ACUTE AND CHRONIC PANCREATITIS
A 50-year-old man presents to the emergency department with epigastric pain and vomiting.
The pain began about 4 hours before he presented, approximately 4 hours after a meal of chili. Emesis started soon after the pain and consisted of old food without blood. He reports that he is a relapsing alcoholic and has consumed 12 ounces of whiskey and two six-packs of beer daily for the last 6 months since relapse of his alcoholism. He smokes two packs of cigarettes daily.
He has had similar episodes previously and has been hospitalized six times before. He has no history of gallstones and has not had previous surgeries. He has lost about 20 pounds over the last 6 months.
Physical examination shows a thin middle-aged man who appears older than his stated age. Temperature 99.6 oF, pulse 110, respirations 22, BP 110/75, height 70 inches, weight 140 pounds. Skin: warm and dry. HEENT: not icteric, mucosae dry. Chest: clear. Heart: regular tachycardia, no murmur. Abdomen: soft, no organomegaly. Tender in epigastrium, no rebound tenderness in RUQ. Bowel sounds quiet. Extremities: no edema, some muscle wasting.
Laboratory testing:
CBC: Hemoglobin 14.5 g/dL, hematocrit 45%, WBC 12,000 with 70% segmented neutrophils, 10% bands, 20% lymphocytes. Platelet count 120,000.
CMP: Sodium 138 mmol/L, potassium 2.5 mmol/L, chloride 98 mmol/L, bicarbonate 18 mmol/L, BUN 25 mg/dL, creatinine 1.4 mg/dL, ALT 30 units/L, AST 40 units/L, alkaline phosphatase 110 units/L, bilirubin level 0.9 mg/dL, lipase 1205 U/L (normal: 0 – 160 U/L).
GROSS: Explanations on gross guide (posted on e-campus)

24
GROSS QUESTIONS:
1. What are the three main types of acute pancreatitis? • Acute interstitial pancreatitis: edema, fat necrosis and perinephric fat • Acute necrotizing pancreatitis: parenchymal necrosis, areas of hemorrhage, fat necrosis in
peripancreatic fat as well as in momentum, mesentery and subcutaneous fat • Acute hemorrhagic pancreatitis: extensive parenchymal necrosis and hemorraghe, with near
total destruction of pancreas. 2. What are the basic alterations of acute pancreatitis? (Robbins)
• Microvascular leakage causing edema • Necrosis of fat by lipolytic enzymes • Acute inflammation • Proteolytic destruction of pancreatic parenchyma • Destruction of blood vessels and subsequent interstitial hemorrhage
3. What are the main gross differences between acute and chronic pancreatitis? • Acute: Depends on type of acute pancreatitis. • Chronic: Numerous yellow/white foci of fat necrosis
SLIDE TO REVIEW: Aperio slide #603 (Acute pancreatitis)
ORIENTATION TO SLIDE: Section of pancreas surrounded by fat. Main pancreatic duct is within the middle.

25
ABNORMAL CHANGES: Focus on the pancreatic duct, just above it you can see an area of fat necrosis with saponification of fat. A few lymphocytes and neutrophils are present within the periphery of necrosis. Focus again on the pancreatic duct just left to it, observe an area of acini that is replaced by fibrosis, inflammation and congestion. This is a case of early acute pancreatitis, the majority of tissue (pancreatic acini) is still viable.
Check list (have you seen the following structures):
____ Necrosis (saponification of fat)
____ Inflammation (neutrophils and lymphocytes)
_____________________________________________________________________________________________
SLIDE TO REVIEW: Aperio slide #149 (Chronic pancreatitis)
ORIENTATION TO SLIDE: Section of pancreas almost entirely replaced by fibrosis.
ABNORMAL CHANGES: This section is almost entirely replaced by fibrosis. No residual acini are present. The only original pancreatic tissue left is consistent with isolated islets of Langerhans, pancreatic ducts and blood vessels.
Check list (have you seen the following structures):
____ Fibrosis and residual isolated islets of Langerhans.
QUESTIONS:
4. What are the two main causes of pancreatitis in Western countries? Alcohol and gallstones 5. Name other causes of acute pancreatitis besides the two above. (Robbins)
• Obstructive: tumors, choledochocele, parasites (ascaris lumbricoides and Clonorchis sinenesis)
• Metabolic: hyperlipoproteinemia, hypercalcemia • Drugs: >80 drugs • Genetics: Mutations of PRSS1 gene encoding cationic trypsinogen. SPINK1 encoding trypsin
inhibitor. • Mechanical: Trauma, surgery, endoscopic procedures with dye injection (ERCP) • Vascular: shock, embolism, vasculitis • Infections: Mumps, coxackievirus, mycoplasma
6. What percentage of pancreatitis are hereditary (no known associated processes)? 10-20% 7. Most hereditary cases are associated with mutations on: germline mutations in the cationic
trypsinogen gene (also known as PRSS1) 8. How do patients with acute pancreatitis usually present? Abdominal pain: constant and intense and is
often referred to the upper back. Anorexia, nausea and vomiting. 9. What labs do you order in a case suspicious for acute pancreatitis? Elevated plasma levels of amylase
and lipase. Glycosuria in 10% of cases. Hypocalcemia from precipitation of calcium soaps in necrotic fat.
10. Why is full-blown acute pancreatitis a medical emergency? (Robbins) It can develop leukocytosis, hemolysis, disseminated intravascular coagulation, fluid sequestration, acute respiratory distress

26
syndrome (ARDS) and diffuse fat necrosis. Peripheral vascular collapse and shock with acute renal tubular necrosis may occur
11. Why can patients with acute pancreatitis present with hypocalcemia? Hypocalcemia from precipitation of calcium soaps in necrotic fat.
12. What is the treatment for acute pancreatitis? “Resting the pancreas”, total restriction of oral intake, supportive therapy with intravenous fluids and analgesia.
13. What percentage of patients with acute pancreatitis die from shock during the first week of illness? 5% due to ARDS and Acute Renal Failure.
14. What percentage of patients with chronic pancreatitis die? 20 to 25 year mortality rate of 50% 15. What are the main sequela of acute pancreatitis? Pancreatic abscess and pancreatic pseudocyst.

27
7) PANCREATIC ADENOCARCINOMA A 58-year-old woman presents to her family doctor’s office because of jaundice.
She was in good health until 4 weeks prior to this visit when she noted the whites of her eyes turning yellow and her urine becoming darker. She lost about 5 pounds since the onset of the jaundice. She has no abdominal pain, no nausea or vomiting. Her stools have become lighter in color. She has no history of pancreatitis, gallstones or liver disease, and no history of anemia.
Physical examination shows a jaundiced middle-aged woman who is in no acute distress. Temperature 98 oF, pulse 86/min and regular, respirations 16/min, BP 125/80. Skin: jaundiced. HEENT: icteric sclerae, mucosae moist. Neck: supple, no adenopathy. Chest: clear. Heart: regular rhythm, no murmur. Abdomen: soft, not distended, bowel sounds active, liver span 10 cm in midclavicular line, spleen not palpable, no tenderness or mass. Extremities: no edema.
Laboratory testing:
CBC: Hemoglobin 11.5 g/dL, hematocrit 33%, WBC 8,000 with 70% segmented neutrophils, 30% lymphocytes. Platelet count 150,000.
CMP: Sodium 142 mmol/L, potassium 4 mmol/L, chloride 105 mmol/L, bicarbonate 24 mmol/L, BUN 12 mg/dL, creatinine 1.1 mg/dL, ALT 30 units/L, AST 40 units/L, alkaline phosphatase 110 units/L, bilirubin level 8.0 mg/dL, lipase 50 U/L (normal: 0 – 160 U/L).
Imaging:
Abdominal sonography: Dilated intra- and extrahepatic bile ducts and dilated pancreatic duct.
Magnetic resonance cholangiopancreatography (MRCP): Classic double duct sign.

28
GROSS: Explanations on gross guide (posted on e-campus)
1. Can you delineate tumor on this gross specimen? Yes 2. Where are pancreatic carcinomas usually located? (Head vs. body vs. tail) Head
SLIDES TO REVIEW: Aperio slide #604 and #602.
ORIENTATION TO SLIDE: Section including duodenum on top and underneath pancreas.
ABNORMAL CHANGES: Normal pancreas is located within the bottom of the slide. A tumor is almost entirely replacing the pancreatic lobules. At high power tumor is composed of glands with a central lumen. Towards the bottom of the slide you can see a large nerve entirely surrounded by tumor glands “perineural invasion”. Perineural invasion is a particular histologic characteristic of pancreatic adenocarcinomas.
MICROSCOPIC DESCRIPTION AND ORIENTATION TO SLIDE #602.
ORIENTATION TO SLIDE: No normal pancreatic tissue present. This slide contains tumor on the right , on the left there is a lymph node (peripancreatic lymph node).
ABNORMAL CHANGES: Similar to previous slide tumor is mainly composed of glands. Focus on the lymph node next to it and observe the sub capsular metastasis into lymph node.
Check list (have you seen the following structures):
____ Tumor cells
____ Perineural invasion
QUESTIONS:

29
3. Pancreatic carcinoma progresses from normal epithelium to precursor lesions to invasive carcinoma. How are the precursor lesions called? Pancreatic intraepithelial neoplasia (PanIN)
4. What are the most common pancreatic adenocarcinoma genetic associations: • KRAS • CDKN2A (p16) • SMAD4 • P53
5. Epidemiology of pancreatic cancer: • Age: elderly, 80% between the ages of 60 and 80 years. • Race: Blacks • Environmental factor associated: Cigarrette smoking
6. What are the main clinical manifestations? They remain silent until they invade into adjacent structures. Pain, obstructive jaundice, weight loss, anorexia, generalized malaise and weakness.
7. What is Trousseau’s sign? Migratory thrombophlebitis due to elaboration of platelet-aggregating factors and procoagulants from the carcinoma or its necrotic products.
8. Serum levels of what marker are usually elevated? CA 19-9

30
Aperio Spectrum Website http://aperio.ad.tamhsc.edu
Login: student1 (or sudent2/3/4) the number corresponds to the workstation number
Password: tamhsc1 (or 2/3/4) also according to work-station number
- Content - Check the box on the left for pathology - Open data (top) - Check the box on the left for Liver, biliary tract and pancreas - Open data(top) - Check the box on the selected slide from manual - Open digital slide (top)
Liver, biliary tract and pancreas, CPC-2, Aperio Slides to review:
1) Aperio #605 (Histology) Normal liver 2) Aperio #755, H&E (Liver biopsy) Cirrhosis 3) Aperio # 756, Thrichrome special stain (liver biopsy) Cirrhosis 4) Aperio #141, H&E (Liver resection) Cirrhosis 5) Aperio #140, Thrichrome special stain (Liver resection) Cirrhosis 6) Aperio #143, H&E (Liver resection) Hemochromatosis 7) Aperio #671, H&E (Liver resection) Alpha-1 antitrypsin deficiency 8) Aperio #142, H&E (Liver resection) Hepatocellular carcinoma 9) Aperio #753, H&E (Gallbladder) acute cholecystitis 10) Aperio #754, H&E (Gallbladder) chronic cholecystitis 11) Aperio #603, H&E (Pancreas) Acute pancreatitis 12) Aperio #604 and #602 (Pancreas) Pancreatic adenocarcinoma
INSTRUCTIONS FOR APERIO USE

31
SELF REVIEW IMAGES QUIZ (FROM APERIO)
Question 1:
Intracellular substance/yellow arrow: Hepatocellular Iron
Special stain (blue): Prussian Blue stain (Robbins/handout)

32
Question 2: Name the process involving this gallbladder: Acute necrotizing cholecystitis
Question 3:
Normal (A or B?): A
Tumor (A or B): B

33
Question 4:
Diagnosis: Cirrhosis
Name the Special Stain: Trichrome stain

34
Question 5: The phenomenon shown on this picture that is highly associated with pancreatic adenocarcinoma is called: perineural invasion

35
Question 6: Name for this special type of liver tumor: Fibrolamellar, hepatocellular carcinoma
Question 7:
Normal (A or B?): A
Tumor (A or B): B (Pancreatic adenocarcinoma)

36
Question 8: Name the process involving this gallbladder: Cholesterolosis

37
Question 9: (see inside box below):
Inclusions within hepatocytes: Intracytoplasmic globular inclusions (acidophilic on H&E)
Special stain: PAS (granules are PAS positive)

38
Question 10: Name the process involving this pancreas: Fat necrosis (saponification of fat) from enzymatic activity of lipase.