LESSONS FROM THE BEDSIDE - VAGADIA- BREATHING EASIER (SLIDES)
63
Case Presentation Case Presentation October 13 October 13 th th , 2009 , 2009 Breathing Easier Breathing Easier Neha R. Vagadia, D.O. Neha R. Vagadia, D.O. Fellow in Pulmonary/Critical Care Fellow in Pulmonary/Critical Care Medicine Medicine Tufts Medical Center Tufts Medical Center
Transcript of LESSONS FROM THE BEDSIDE - VAGADIA- BREATHING EASIER (SLIDES)

Case PresentationCase Presentation
October 13October 13thth, 2009, 2009Breathing Easier Breathing Easier Neha R. Vagadia, D.O.Neha R. Vagadia, D.O.Fellow in Pulmonary/Critical Care MedicineFellow in Pulmonary/Critical Care MedicineTufts Medical CenterTufts Medical Center

History and PhysicalHistory and Physical
CC: Shortness of BreathCC: Shortness of Breath HPI: Pt is a 31 year old male with history of HPI: Pt is a 31 year old male with history of
Hypertrophic Cardiomyopathy, IgA Deficiency Hypertrophic Cardiomyopathy, IgA Deficiency who presents to OSH with 5 days of worsening who presents to OSH with 5 days of worsening shortness of breath. States that began to shortness of breath. States that began to have symptoms of cough, fever/chills 3 days have symptoms of cough, fever/chills 3 days prior to admission. Symptoms similar to prior to admission. Symptoms similar to pneumonias in past, but this is significantly pneumonias in past, but this is significantly worse. worse.
ROS: No significant wt changes. Generalized ROS: No significant wt changes. Generalized fatigue. No chest pain. Some mild chest fatigue. No chest pain. Some mild chest tightness. Positive dyspnea, particularly on tightness. Positive dyspnea, particularly on exertion. No abdominal pain. No N/V/D. No exertion. No abdominal pain. No N/V/D. No rashes. No lower extremity edema. rashes. No lower extremity edema.

HistoryHistory
Past Medical History:Past Medical History:– Hypertrophic Hypertrophic
CardiomyopathyCardiomyopathy Gradient of 25%Gradient of 25%
– IgA deficiencyIgA deficiency– 2 previous 2 previous
pneumoniaspneumonias
Social History:Social History:– No smoking historyNo smoking history– No IVDA or ETOH useNo IVDA or ETOH use– Lives with wife – who is Lives with wife – who is
a nurse. Newborn child a nurse. Newborn child of 8 weeks. of 8 weeks.
MedicationsMedications::– NoneNone
AllergiesAllergies:: – NKDANKDA
Family HistoryFamily History:: – CAD, DMCAD, DM

Physical ExamPhysical Exam
Vital Signs: T: 101.3, P: 100, BP: 92/60, RR: 40 Vital Signs: T: 101.3, P: 100, BP: 92/60, RR: 40 85% on a Non-rebreather.85% on a Non-rebreather. General: Young male, WD, WN male in apparent General: Young male, WD, WN male in apparent
distress. distress. Skin: Diaphoretic, no rash obvious. Clearly flushed. Skin: Diaphoretic, no rash obvious. Clearly flushed. HEENT: Non-icteric, EOMI. PERLA. Oropharynx HEENT: Non-icteric, EOMI. PERLA. Oropharynx
negative for erythema or exudate. negative for erythema or exudate. Neck: Supple. No LAD. No JVDNeck: Supple. No LAD. No JVD Lungs: Diffuse ronchi in the RUL. Diminished breath Lungs: Diffuse ronchi in the RUL. Diminished breath
sounds on the Left > right. No wheezes or rales. sounds on the Left > right. No wheezes or rales. CVS: S1, S2 normal with RRR. CVS: S1, S2 normal with RRR. Abdomen: Positive BS. Mildly obese. NT, ND. No Abdomen: Positive BS. Mildly obese. NT, ND. No
hepatosplenomegalyhepatosplenomegaly Extremities: No edema, no cyanosis, or clubbing.Extremities: No edema, no cyanosis, or clubbing.

DiagnosticsDiagnostics
15.6 13
37.5
168Segs 72
Bands 26
134
4.7
97
28
20
1.05214
Ca – 8.9, Mg – 2.0, Phos – 2.4,
CK: 1016, Troponin: 0.10
Lactate: 1.9, LDH: 1521
LFT’s: AST -115, AP – 60, ALT – 37, TB: 0.8
Amylase: 135, Lipase: 38
IgA and IgG levels were confirmed low. IgA and IgG levels were confirmed low.
EKG: Sinus Tachycardia. Regular rhythm

Hospital CourseHospital Course
Patient arrived here in clear Patient arrived here in clear respiratory distress. respiratory distress.
ABG done and finally due to ABG done and finally due to increased work of breathing and increased work of breathing and clear hypoxia clear hypoxia patient patient intubated.intubated.
ABG: 7.47/36/66/26/ on non-rebreather. 7.33/51/79/26 on 100% Fi02

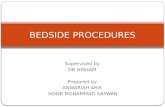
Diagnostic Data - CXRDiagnostic Data - CXR
CXR - CXR -

What next?What next?
Bronchoscopy Bronchoscopy
Chest CT Chest CT

Bronchoscopy 6/10Bronchoscopy 6/10
BAL fluid differential sent but BAL fluid differential sent but nothing remarkable.nothing remarkable.
Gram stain was negative.Gram stain was negative. Rest of Microbiology – pendingRest of Microbiology – pending

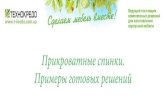
Chest CT – 6/10Chest CT – 6/10

Chest CT – 6/10Chest CT – 6/10

Chest CT – 6/10Chest CT – 6/10

Chest CT – 6/10Chest CT – 6/10

Chest CT – 6/10Chest CT – 6/10

Chest CT – 6/10Chest CT – 6/10

Chest CT – 6/10Chest CT – 6/10

Chest CT – 6/10Chest CT – 6/10

Chest CT – 6/10Chest CT – 6/10

Chest CT – 6/10Chest CT – 6/10

Chest CT – 6/10Chest CT – 6/10

Chest CT – 6/10Chest CT – 6/10

Chest CT – 6/10Chest CT – 6/10

Chest CT – 6/10Chest CT – 6/10

Chest CT – 6/10Chest CT – 6/10

Chest CT – 6/10Chest CT – 6/10

Chest CT – 6/10Chest CT – 6/10

Chest CT – 6/10Chest CT – 6/10
Extensive areas of pulmonary Extensive areas of pulmonary parenchymal opacification, with only a parenchymal opacification, with only a small portion of the upper lobes small portion of the upper lobes remaining aerated. Consistent with remaining aerated. Consistent with extensive collapse and/or pneumonia, extensive collapse and/or pneumonia, involving both lower lobes and much of involving both lower lobes and much of the right middle lobe and both upper the right middle lobe and both upper lobeslobes with hemorrhage not excluded. with hemorrhage not excluded.
Mildly prominent mediastinal lymph Mildly prominent mediastinal lymph nodes, perhaps reactive. nodes, perhaps reactive.

Things to consider in Things to consider in this patient’s this patient’s management…management…

IgA DeficiencyIgA DeficiencyPrevalencePrevalence
United StatesUnited States Selective IgA deficiency Selective IgA deficiency most most
common primary common primary immunodeficiency, immunodeficiency,
Prevalence ranging from 1 in 223-Prevalence ranging from 1 in 223-30003000

Clinical ManifestationsClinical Manifestations
Vast majority of IgA deficient individuals (85 to 90 Vast majority of IgA deficient individuals (85 to 90 percent) are asymptomatic percent) are asymptomatic
Some are predisposed to develop one or more of the Some are predisposed to develop one or more of the following: following: – Recurrent Sino pulmonary infections (those with Recurrent Sino pulmonary infections (those with
concurrent IgG deficiency) concurrent IgG deficiency) – Autoimmune antibodies and/or disorders Autoimmune antibodies and/or disorders – Gastrointestinal infections and disorders (those with Gastrointestinal infections and disorders (those with
absent secretory IgA) absent secretory IgA) – Anaphylactic transfusion reactions (those with anti-IgA Anaphylactic transfusion reactions (those with anti-IgA
antibodies) antibodies) Those with concomitant IgM or IgG subclass deficiency Those with concomitant IgM or IgG subclass deficiency
present more frequently with recurrent infections. present more frequently with recurrent infections.

IgA DeficiencyIgA DeficiencyDefectDefect Humoral immune deficiencyHumoral immune deficiency
– Impaired molecular defect intrinsic to B cells or a Impaired molecular defect intrinsic to B cells or a failure of interactions between B and T cells. failure of interactions between B and T cells.
Helps the phagocytic arm of the immune Helps the phagocytic arm of the immune system located in the mucosal areas, which system located in the mucosal areas, which is why thought to prevent against recurrent is why thought to prevent against recurrent respiratory and gastrointestinal infections.respiratory and gastrointestinal infections.
Binds foreign antigens which then binds to a Binds foreign antigens which then binds to a receptor located on neutrophils, eosinophils, receptor located on neutrophils, eosinophils, and macrophages. The organism is then and macrophages. The organism is then ingested and destroyed. ingested and destroyed.


Bronchoscopy resultsBronchoscopy results

The Flu and IgA The Flu and IgA DeficiencyDeficiency Bernard P. Arulanandam, et al: Bernard P. Arulanandam, et al:
– The Journal of Immunology, The Journal of Immunology, 2001, 166: 226–2001, 166: 226–231.231.
IgA deficient mice displayed impaired T cell IgA deficient mice displayed impaired T cell priming to the H1N1 subunit vaccine, with priming to the H1N1 subunit vaccine, with concomitant reduction in recall memory concomitant reduction in recall memory responses due to a defect in APC function. responses due to a defect in APC function.
Provided evidence that a major role of IgA is to Provided evidence that a major role of IgA is to facilitate presentation of Ag to mucosal T cells. facilitate presentation of Ag to mucosal T cells.
IL-12 treatment can overcome IgA deficiency by IL-12 treatment can overcome IgA deficiency by providing adequate T cell priming during providing adequate T cell priming during vaccinationvaccination

TreatmentTreatment
For those with recurrent For those with recurrent infections: General focus is infections: General focus is management of infections. management of infections.
Six month course of daily Six month course of daily prophylactic antibiotics can be prophylactic antibiotics can be used for those with continued used for those with continued infections. infections.
If this fails trial of gamma globulin If this fails trial of gamma globulin replacement therapy may be replacement therapy may be warranted. warranted.



InfluenzaInfluenza
Influenza A and B are two types of influenza Influenza A and B are two types of influenza viruses that cause epidemic diseaseviruses that cause epidemic disease
Influenza A Influenza A – HemagglutininHemagglutinin– NeuraminidaseNeuraminidase– H1N1, H3N2, reassortment H1N2,H1N1, H3N2, reassortment H1N2,
Influenza B Influenza B – Yamagata and VictoriaYamagata and Victoria
Antigenic shift occurs when a new subtype of Antigenic shift occurs when a new subtype of influenza A virus appears and can result in the influenza A virus appears and can result in the emergence of a novel influenza A virus i.e.. emergence of a novel influenza A virus i.e.. H1N1H1N1

H1N1H1N1
This novel virus is This novel virus is derived partly from derived partly from influenza A viruses influenza A viruses that circulate in that circulate in swine and is swine and is antigenically distinct antigenically distinct from human from human influenza A (H1N1) influenza A (H1N1) viruses in circulation viruses in circulation since 1977.since 1977.
First detected in First detected in people in the United people in the United States in April 2009States in April 2009

Treatment Treatment
Most people who get the flu (either seasonal or 2009 Most people who get the flu (either seasonal or 2009 H1N1) will have mild illness and will recover in less H1N1) will have mild illness and will recover in less than 2 weeks. They do not need medical care or than 2 weeks. They do not need medical care or antiviral drugs. antiviral drugs.
Empiric therapy and therapy should be considered in Empiric therapy and therapy should be considered in those with suspected influenza and either severe those with suspected influenza and either severe symptoms or potential for complications. symptoms or potential for complications.
Those at higher risk for complications including: Those at higher risk for complications including: – Children younger than 2 years old; Children younger than 2 years old; – Persons aged 65 years or older Persons aged 65 years or older – Pregnant women Pregnant women – Persons of any age with certain chronic medical or Persons of any age with certain chronic medical or
immunosuppressive conditions (blood disorders, kidney immunosuppressive conditions (blood disorders, kidney disease, cancer, chronic lung disease, liver disease, heart disease, cancer, chronic lung disease, liver disease, heart disease, neurologic disorders, or weakened immune disease, neurologic disorders, or weakened immune systems)systems)

TreatmentTreatment
When indicated, should be initiated as early When indicated, should be initiated as early as possible as possible within 48 hours of illness for within 48 hours of illness for most benefit. most benefit.
Treatment should not wait for laboratory Treatment should not wait for laboratory confirmation of influenza. confirmation of influenza.
Laboratory testing can delay treatment and a Laboratory testing can delay treatment and a negative rapid test for influenza does not rule negative rapid test for influenza does not rule out influenza. out influenza. – The sensitivity of rapid tests in detecting 2009 The sensitivity of rapid tests in detecting 2009
H1N1 has ranged from 10% to 70%. H1N1 has ranged from 10% to 70%. Antiviral chemoprophylaxis Antiviral chemoprophylaxis
– Persons at higher risk for influenza-related Persons at higher risk for influenza-related complications complications
– Those who have had contact with someone likely to Those who have had contact with someone likely to have been infected with influenza.have been infected with influenza.

Treatment Treatment
H1N1 influenza viruses likely will be the most H1N1 influenza viruses likely will be the most common influenza viruses circulating this common influenza viruses circulating this season, but circulation of seasonal influenza season, but circulation of seasonal influenza viruses is also expected. viruses is also expected.
Currently circulating 2009 H1N1 viruses Currently circulating 2009 H1N1 viruses susceptible to oseltamivir and zanamivir, but susceptible to oseltamivir and zanamivir, but resistant to amantadine and rimantadine;resistant to amantadine and rimantadine;
Antiviral treatment regimens might change Antiviral treatment regimens might change according to new antiviral resistance or viral according to new antiviral resistance or viral surveillance information. surveillance information.

Prevention: Prevention:
Influenza vaccination is the most effective Influenza vaccination is the most effective method for preventing influenza virus method for preventing influenza virus infection. infection.
Beginning each September, or even earlier if Beginning each September, or even earlier if vaccine is available, the flu vaccine should vaccine is available, the flu vaccine should be offered be offered
Both the Both the Live, Intranasal Influenza Vaccine (LAIV) and and Trivalent Inactivated Influenza Vaccine (TVIV) contain strains of influenza (TVIV) contain strains of influenza viruses that are antigenically equivalent to viruses that are antigenically equivalent to the annually recommended strains: one the annually recommended strains: one influenza A (H3N2) virus, one influenza A influenza A (H3N2) virus, one influenza A (H1N1) virus, and one influenza B virus.(H1N1) virus, and one influenza B virus.

Seasonal VaccinationSeasonal Vaccination
Trivalent Inactivated Influenza Vaccine Trivalent Inactivated Influenza Vaccine (TIV)(TIV)– TIV is injected into the muscle of the upper arm or TIV is injected into the muscle of the upper arm or
thigh. thigh. – It can be used for people 6 months of age or older, It can be used for people 6 months of age or older,
including healthy people, those with chronic medical including healthy people, those with chronic medical conditions, and pregnant women. conditions, and pregnant women.
– The viruses in the injectable influenza vaccine are The viruses in the injectable influenza vaccine are inactivated so they do not cause influenza.inactivated so they do not cause influenza.
Live, Intranasal Influenza Vaccine (LAIV)Live, Intranasal Influenza Vaccine (LAIV) – LAIV is given as a nasal spray. It can be used for LAIV is given as a nasal spray. It can be used for
healthyhealthy people 2-49 years of age who are not people 2-49 years of age who are not pregnant. pregnant.

Summary of seasonal influenza Summary of seasonal influenza vaccination recommendations vaccination recommendations 2009: Adults2009: Adults People recommended for vaccination based on their People recommended for vaccination based on their
risk of complications from influenza or because they risk of complications from influenza or because they are in close contact with someone at higher risk of are in close contact with someone at higher risk of influenza complications include: influenza complications include:
– Children aged 6 months until their 5th birthday, Children aged 6 months until their 5th birthday, – Pregnant women, Pregnant women, – People 50 years of age and older, People 50 years of age and older, – People of any age with certain chronic health conditions (such as People of any age with certain chronic health conditions (such as
asthma, diabetes, or heart disease), asthma, diabetes, or heart disease), – People who live in nursing homes and other long-term care People who live in nursing homes and other long-term care
facilities, facilities, – Household contacts of person at high risk for complications from Household contacts of person at high risk for complications from
influenza, influenza, – Household contacts and out of home caregivers of children less Household contacts and out of home caregivers of children less
than 6 months of age, and than 6 months of age, and – Health care workers.Health care workers.
http://www.cdc.gov/flu/professionals/vaccination/vax-summary.html

VaccinationVaccination
People who should NOT be vaccinated People who should NOT be vaccinated include: include: – People who have a severe allergy to chicken eggs, People who have a severe allergy to chicken eggs, – People who have had a severe reaction to an People who have had a severe reaction to an
influenza vaccination, influenza vaccination, – People who have developed Guillian-Barré People who have developed Guillian-Barré
syndrome within 6 weeks of getting an influenza syndrome within 6 weeks of getting an influenza vaccine, vaccine,
– Children less than 6 months of age (influenza Children less than 6 months of age (influenza vaccine is not approved for this age group), and vaccine is not approved for this age group), and
– People who have a moderate to severe illness with People who have a moderate to severe illness with a fever (they should wait until they recover to get a fever (they should wait until they recover to get vaccinated). vaccinated).
http://www.cdc.gov/flu/professionals/vaccination/vax-summary.htm

2009 H1N1 Influenza 2009 H1N1 Influenza VaccineVaccine Pregnant womenPregnant women Persons who live with or provide care for Persons who live with or provide care for
infants aged <6 months (e.g., parents, infants aged <6 months (e.g., parents, siblings, and daycare providers)siblings, and daycare providers)
Health-care and emergency medical services Health-care and emergency medical services personnelpersonnel
Children and young adults aged 6 months-24 Children and young adults aged 6 months-24 yearsyears
Persons aged 25--64 years who have medical Persons aged 25--64 years who have medical conditions that put them at higher risk for conditions that put them at higher risk for influenza-related complications.influenza-related complications.

2009 H1N1 Influenza 2009 H1N1 Influenza VaccineVaccine A 2009 H1N1 "flu shot"A 2009 H1N1 "flu shot" — —
– Inactivated vaccine (containing killed virus) muscle Inactivated vaccine (containing killed virus) muscle injection. injection.
– The indications are the same as for seasonal flu shots. The indications are the same as for seasonal flu shots. – Approved for use in people 6 months of age and older, Approved for use in people 6 months of age and older,
including healthy people, people with chronic medical including healthy people, people with chronic medical conditions and pregnant women. conditions and pregnant women.
The 2009 H1N1 nasal spray flu vaccineThe 2009 H1N1 nasal spray flu vaccine — — – live attenuated influenza vaccine (live, weakened live attenuated influenza vaccine (live, weakened
viruses) . viruses) . – The indications are the same as for seasonal nasal The indications are the same as for seasonal nasal
spray vaccine. LAIV is approved for use in healthy* spray vaccine. LAIV is approved for use in healthy* people 2 years to 49 years of age who are not people 2 years to 49 years of age who are not pregnant.. pregnant..

What to look out forWhat to look out for
The symptoms of novel H1N1 and seasonal influenza are similar: Fever, cough, headache, sore throat, anorexia, myalgias, lethargy, and sometimes vomiting and diarrhea. However, 10% to 40% of persons with novel H1N1 influenza may not be febrile
Of Boston residents hospitalized with confirmed novel H1N1 influenza, 49% had underlying asthma and 37% required ICU care
One thing that appears to be different from seasonal One thing that appears to be different from seasonal influenza is that adults older than 64 years do not yet influenza is that adults older than 64 years do not yet appear to be at increased risk of 2009 H1N1-related appear to be at increased risk of 2009 H1N1-related complications thus far about one-third of adults older complications thus far about one-third of adults older than 60 may have antibodies against this virusthan 60 may have antibodies against this virus

Hospital Course Hospital Course ContinuedContinued Patient treated with empiric antibiotics – Patient treated with empiric antibiotics –
broad spectrum. Then placed on oseltamivir broad spectrum. Then placed on oseltamivir for 5 days with the results of the for 5 days with the results of the bronchcoscopy.bronchcoscopy.
Flu swab was negative but culture was Flu swab was negative but culture was positive for Influenza A and presumed H1N1.positive for Influenza A and presumed H1N1.
Patient remained on the vent for 4 weeks.Patient remained on the vent for 4 weeks. Went on to get trach and peg transferred out Went on to get trach and peg transferred out
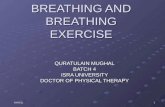
to an LTAC. to an LTAC. Now awake, walking, decannulated and able Now awake, walking, decannulated and able
to hold his 4 month old child.to hold his 4 month old child.

Follow up CT scan 6/28Follow up CT scan 6/28

Follow up CT scan 6/28Follow up CT scan 6/28

Follow up CT scan 6/28Follow up CT scan 6/28

Follow up CT scan 6/28Follow up CT scan 6/28

Follow up CT scan 6/28Follow up CT scan 6/28

Follow up CT scan 6/28Follow up CT scan 6/28

Follow up CT scan 6/28Follow up CT scan 6/28

Follow up CT scan 6/28Follow up CT scan 6/28

Follow up CT scan 6/28Follow up CT scan 6/28

Follow up CT scan 6/28Follow up CT scan 6/28

Follow up CT scan 6/28Follow up CT scan 6/28

Thank you.Thank you.
Special thanks to:Special thanks to: Dr. Alex WhiteDr. Alex White Dr. Heidi O’ConnorDr. Heidi O’Connor Dr. Geraldine Finlay Dr. Geraldine Finlay Dr. Eric GarpestadDr. Eric Garpestad
Please remember to HANDWASH!!Please remember to HANDWASH!!

ReferencesReferences
IgA deficiency: clinical correlates and responses to IgA deficiency: clinical correlates and responses to pneumococcal vaccine E. Edwards et al. / Clinical pneumococcal vaccine E. Edwards et al. / Clinical Immunology 111 (2004) 93–97Immunology 111 (2004) 93–97
Bernard P. Arulanandam, et al. IgA Immunodeficiency Leads to Inadequate Th Cell Priming and Increased Susceptibility to Influenza Virus Infection. Journal of Immunology. 2001 226-229
Frederick M. Schaffer, MD. Clinical assessment and management of abnormal IgA levels. Annals Of Allergy, Asthma & Immunology. Volume 100, March, 2008.
http://www.cdc.gov/flu/weekly/ BOSTON PUBLIC HEALTH COMMISSION ▪
INFECTIOUS DISEASE BUREAU Communicable Disease Control Division 1010 Massachusetts Avenue ∙ Boston, MA 02118