
Kuliah Ekg Unwar 2013
151
ECG Interpretation UNWAR Medical Student Lecture A.A.Gede Budhitresna MD,Int,Ph.D,FINASIM
description
kardio
Transcript of Kuliah Ekg Unwar 2013

ECG InterpretationUNWAR Medical Student Lecture
A.A.Gede Budhitresna MD,Int,Ph.D,FINASIM

Objectives The Basics Interpretation Clinical Pearls Practice
Recognition

3
QUICK REVIEW OF HEART
Purpose Pumps bloodBasic Anatomy 4 chambers 2 sides 4 valves

Circulatory System Three basic components
Heart Serves as pump that establishes the pressure
gradient needed for blood to flow to tissues Blood vessels
Passageways through which blood is distributed from heart to all parts of body and back to heart
Blood Transport medium within which materials
being transported are dissolved or suspended

Circulatory System Pulmonary
circulation Closed loop of vessels
carrying blood between heart and lungs
Systemic circulation Circuit of vessels
carrying blood between heart and other body systems

Functions of the Heart Generating blood pressure Routing blood
Heart separates pulmonary and systemic circulations
Ensuring one-way blood flow Regulating blood supply
Changes in contraction rate and force match blood delivery to changing metabolic needs

Blood Flow Through and Pump Action of the Heart

Blood Flow Through Heart

Sel otot jantung 2 macam sel :
Sel autoritmik (1%) Potential pace maker Hanya terdapat pada NSA – NAV – berkas
his cabang kanan dan kiri – serabut purkinye
Sel kontraktil (99%) Sel yang berkontraksi sebagai respon thd
impuls dari sel autoritmik

Muatan listrik sel otot jantungKeadaan sel otot jantung
Muatan listrik
intraseluler ekstraseluler
Istirahat/repolarisasi
- (relatif lebih negatif)
+ (relatif lebih positif)
depolarisasi + (relatif lebih positif)
- (relatif lebih negatif)

Sel istirahat
+ + + + + + +
Sel sedang depolarisasi
--- --- --- + + + +
-- -- -- --- --- ---
--- --- --- --- ---
+ + + +
+ + + +
--- --- ---
--- --- ---
+ + + + + + +
Sel telah depolarisasi
--- --- --- --- ---
--- --- --- + + + + +
Sel mulai repolarisasi
--- --- --- + + + +
+ + + + + + +
+ + + + + + +
+ + + +
+ + + +
--- --- ---
--- --- ---
--- --- --- --- --- --- --- + + + +

Elektrokardiogram Fase depolarisasi (SISTOLE)
bagian yang terjadi akibat penyebaran impuls
Fase repolarisasi (DIASTOLE) bagian yang terjadi bila sel otot
jantung kembali istrirahat Arah defleksi , ditentukan :
Arah penyebaran impuls depolarisasi Letak elektroda

Hubungan arah impuls – defleksi elektrokardiogram
Arah impuls depolarisasi
Arah defleksi Gambar
Menuju elektroda +
Positif (ke atas)
Menuju - meninggalkan
Bifasik
Meninggalkan elektroda +
Negatif (ke bawah)

The Normal Conduction System

CONDUCTION SYSTEM

Normal Impulse Conduction
Sinoatrial node
AV node
Bundle of His
Bundle Branches
Purkinje fibers


18
RELATIONSHIP

Putting the A&P with the EKG

Normal Adult ECG

CARDIAC CYCLES


SANDAPAN (LEAD) EKG Sandapan rutin 12 leads
3 bipolar standard leads ( I, II, III) 3 unipolar lead ekstremitas (aVR, aVL, aVF) 6 unipolar chest leads (V1, V2, V3, V4, V5, V6)
Bipolar standard lead & unipolar lead ekstremitas menggambarkan keadaan medan bioelektrik aktivitas jantung pada bidang frontal
Chest lead Bidang horizontal

Lead Placement
aVF

All Limb Leads

12 Lead Placement

Precordial Leads

Precordial Leads

I and AVL
II, III and AVF
V3 & v4
V1 & v2
V5 & v6 Where the positive
electrode is positioned, determines what part of the heart is seen!

Electrode Placement
Lead V1 is placed over the 4th intercostal space, to the right of the sternum
Lead V2 is placed over the 4th intercostal space, to the left of the sternum
Lead V4 is placed over the 5th intercostal space in the mid-clavicular line
Lead V3 is placed midway between V2 and V4 Lead V5 is placed on the same horizontal level
as V4 but at the anterior axilliary line Lead V6 is placed on the same horizontal level
as V4 and V5 but on the mid axilliary line

EKG Distributions
Anteroseptal: V1, V2, V3, V4 Anterior: V1–V4 Anterolateral: V4–V6, I, aVL Lateral: I and aVL Inferior: II, III, and aVF Inferolateral: II, III, aVF, and
V5 and V6

2004 Anna Story
The ECG Tracing: Waves P- wave
Marks the beginning of the cardiac cycle and measures the electrical impulse that causes atrial depolarization and mechanical contraction
QRS- Complex Measures the impulse that causes ventricular
depolarization Q-wave- may or may not be evident on the ECG R-wave- first upward deflection following P wave S-wave- the first downward deflection following the
R-wave T- wave
Marks ventricular repolarization that ends the cardiac cycle

Intervals and Segments P-R interval-
Time interval for impulse to go from the SA to the AV node
normal 0.12-0.20 secs QRS Interval
Time interval for impulse to go from AV node to stimulate Purkinjie fibers
Less than 0.12 secs QT Interval
Time interval from beginning of depolarization to the end of repolarization
Should not exceed ½ the length of the R-R ST segment
end of the S to the beginning of the T

Waveforms

Interpretation Develop a systematic approach to
reading EKGs and use it every time The system we will practice is:
Rate Rhythm (including intervals and
blocks) Axis Hypertrophy Ischemia

RATE2 More Methods to Count Rate
1. When the rhythm is regular, the heart rate is 300 divided by the number of large squares between the QRS complexes.
For example, if there are 4 large squares between regular QRS complexes, the heart rate is 75 (300/4=75).
2. The second method can be used with an irregular rhythm to estimate the rate. Count the number of R waves in a 6 second strip and multiply by 10.
For example, if there are 7 R waves in a 6 second strip, the heart rate is 70 (7x10=70).

Heart Rate: 300, 150, 100, 75, 60, 50, 43, 37 bpm

Rate
HR of 60-100 per minute is normal HR > 100 = tachycardia HR < 60 = bradycardia

Differential Diagnosis of Tachycardia
Tachycardia
Narrow Complex Wide Complex
Regular STSVTAtrial flutter
ST w/ aberrancySVT w/ aberrancy
VT
Irregular A-fibA-flutter w/ variable conductionMAT
A-fib w/ aberrancy
A-fib w/ WPWVT

What is the heart rate?
(300 / 6) = 50 bpm
www.uptodate.com


Asystole V-Tach to V-Fib
can lead to….
Asystole

Rhythm
Sinus Originating
from SA node P wave before
every QRS P wave in same
direction as QRS

What is this rhythm?Normal Sinus Rythm


Normal Intervals PR
0.20 sec (less than one large box)
QRS 0.08 – 0.10 sec (1-2
small boxes) QT
450 ms in men, 460 ms in women
Based on sex / heart rate
Half the R-R interval with normal HR

Prolonged QT Normal
Men 450ms Women 460ms
Corrected QT (QTc) QTm/√(R-R)
Causes Drugs (Na channel blockers) Hypocalcemia, hypomagnesemia, hypokalemia Hypothermia AMI Congenital Increased ICP

Blocks AV blocks
First degree block PR interval fixed and > 0.2 sec
Second degree block, Mobitz type 1 PR gradually lengthened, then drop QRS
Second degree block, Mobitz type 2 PR fixed, but drop QRS randomly
Type 3 block PR and QRS dissociated

What is this rhythm?
First degree AV block PR is fixed and longer than 0.2 sec

What is this rhythm?
Type 1 second degree block (Wenckebach)

What is this rhythm?
Type 2 second degree AV block Dropped QRS

What is this rhythm?
3rd degree heart block (complete)

Bundle Branch Block - BBB



The QRS Axis
Represents the overall direction of the heart’s activity
Axis of –30 to +90 degrees is normal

The Quadrant Approach
QRS up in I and up in aVF = Normal

What is the axis?
Normal- QRS up in I and aVF

Hypertrophy Add the larger S wave of V1 or V2
in mm, to the larger R wave of V5 or V6.
Sum is > 35mm = LVH

Ischemia
Usually indicated by ST changes Elevation = Acute infarction Depression = Ischemia
Can manifest as T wave changes Remote ischemia shown by q
waves

Acute Coronary Syndrome

PEMBULUH DARAH PEMBULUH DARAH KORONERKORONER
RCA
LM
LAD LCx



Normal : Isoelektris
Kepentingan : Elevasi Pada injuri/infark akutDepresi Pada iskemia
Segmen STDiukur dari akhir QRS s/d awal gel
T

NSTEMI dan STEMI

ECG Changes : Ischemia T-wave inversion ( flipped T) ST segment depression T wave flattening Biphasic T-waves
Baseline

ECG Changes: Injury ST segment elevation of greater than 1mm in
at least 2 contiguous leads Heightened or peaked T waves Directly related to portions of myocardium
rendered electrically inactive
Baseline

ECG Changes: Infarct Significant Q-wave where none previously existed
Why? Impulse traveling away from the positive lead Necrotic tissue is electrically dead
No Q-wave in Subendocardial infarcts Why?
Not full thickness dead tissue But will see a ST depression Often a precursor to full thickness MI
Criteria Depth of Q wave should be 25% the height of the R
wave Width of Q wave is 0.04 secs Diminished height of the R wave


Evolving MI and Hallmarks of AMI
1 year
Q wave
ST Elevation
T wave inversion


INFERIOR INFARCTION

Color Coding ECG- Inferior
Blue indicates leads II, III, AVF
Inferior Infarct with ST elevations
Right Coronary Artery (RCA)
1st degree Heart Block
2nd degree Type 1, 2 3rd degree Block N/V common, Brady

Inferior MI

Inferior myocardial infarction

Small inferior distal RCA occlusion
ECG changes in leads II, III, and aVF

ANTERIOR INFARCTION

ECG demonstrates large anterior infarction

Color Coding ECG’s Anterior
Yellow indicates V1, V2, V3, V4
Anterior infarct with ST elevation
Left Anterior Descending Artery (LAD)
V1 and V2 may also indicate septal involvement which extends from front to the back of the heart along the septum
Left bundle branch block Right bundle branch block 2nd Degree Type2 Complete Heart Block

Anterior MI

Mid LAD occlusion after the first septal perforator (arrow)
ECG : large anterior MI

2004 Anna Story 83
Color Coding ECG- Lateral Red indicates leads
I, AVL, V5, V6 Lateral Infarct
with ST elevations
Left Circumflex Artery
Rarely by itself Usually in combo

Lateral MI

Color Coding ECG- Posterior
Green indicates leads V1, V2
Posterior Infarct with ST Depressions and/ tall R wave RCA and/or LCX Artery
Understand Reciprocal changes The posterior aspect of the
heart is viewed as a mirror image and therefore depressions versus elevations indicate MI
Rarely by itself usually in combo

Posterior MI

Putting it ALL together


2004 Anna Story 89
Practice 1
Anterior MI with lateral involvement
ST elevations V2, V3, V4
ST elevations II, AVL, V5
Click for answer

Practice 2
Anteroseptal MI
ST elevations V1, V2, V3, V4
Click for answer

Practice 3
Click for answer
Inferior MI
ST elevation 2,3 AVF

Practice 4
Click for answer
Inferior lateral MI
ST elevations 2, 3, AVF
ST elevations V5

Practice 5
•Acute inferior MI
•Lateral ischemia
Click for answer

Cardiac Enzymes Indicating Infarct Normals
CPK- 10-155u/liter begin rise 3-6 hours and peaks 12-24 with return
to norm 3-5 days CPK-MB < than 5% IU/liter LDH 85-200 IU/liter
Begin rise 12 hours, peaks 36-72 and normal around 10 days
LDH 1- 18.1% - 29% of total LDH 2- 27.4% to 37.5% of total

Cardiac Enzymes Indicating Infarct
Troponins- Now the Gold Standard! Rises after 3-6
hours Negative Troponin
within 6 hours of onset of S&S rules out the MI
Peaks at about 20 hours
May be raised for 14 days

Cardiac Enzymes Indicating Infarct Troponin T
84% sensitivity for MI 8 hours after onset of symptoms
22% for unstable angina Advantages
Highly sensitive for detecting myocardial ischemia Levels may help to stratify risks
Disadvantages Less specific than Troponin I Increased in angina Increased in chronic renal failure

Cardiac Enzymes Indicating Infarct Troponin I
90% sensitivity for MI 8 hours after onset of S&S and 95% specificity
Level greater than 1.2 suggest MI Negative rules out MI Obtain two negative troponin values 4 hours
apart Normally exceedingly low Even a small elevation indicates
myocardial damage


DISKUSI KASUS

Normal Sinus Rhythm
Mattu, 2003

First Degree Heart Block
PR interval >200ms

Junctional Rhythm
Rate 40-60, no p waves, narrow complex QRS

Hyperkalemia
Tall, narrow and symmetric T waves

Premature Atrial Contractions
Trigeminy pattern

Atrial Flutter with Variable Block
Sawtooth waves Typically at HR of 150

Torsades de Pointes
Notice twisting pattern
Treatment: Magnesium 2 grams IV

Digitalis
Dubin, 4th ed. 1989

Lateral MI
Reciprocal changes

Inferolateral MI
ST elevation II, III, aVF
ST depression in aVL, V1-V3 are reciprocal changes

Anterolateral / Inferior Ischemia
LVH, AV junctional rhythm, bradycardia

Left Bundle Branch Block
Monophasic R wave in I and V6, QRS > 0.12 secLoss of R wave in precordial leadsQRS T wave discordance I, V1, V6Consider cardiac ischemia if a new finding

Right Bundle Branch Block
V1: RSR prime pattern with inverted T waveV6: Wide deep slurred S wave

First Degree Heart Block, Mobitz Type I (Wenckebach)
PR progressively lengthens until QRS drops

Supraventricular Tachycardia
Narrow complex, regular; retrograde P waves, rate <220
Retrograde P waves

Right Ventricular Myocardial Infarction
Found in 1/3 of patients with inferior MI
Increased morbidity and mortality
ST elevation in V4-V6 of Right-sided EKG

Ventricular Tachycardia

Second Degree Heart Block, Mobitz Type II
PR interval fixed, QRS dropped intermittently

Acute Pulmonary Embolism
SIQIIITIII in 10-15%
T-wave inversions, especially occurring in inferior and anteroseptal simultaneously
RAD

Hypokalemia
U wavesCan also see PVCs, ST depression, small T waves

LVH with ‘strain’

Sinus arrhythmia
Perempuan 26 th, MCU penerimaan karyawan

Lateral myocardial infarction
Perempuan 46 th, DM, Nyeri dada 10 jam yg lalu, mendadak, Trop T (+)

Acute inferoposterior myocardial infarction
Laki-laki 36 th, perokok, nyeri dada 1 jam yg lalu, mendadak, Trop T (-)

Atrial fibrillation dan STEMI inferior
Laki-laki 76 th, perokok, stroke ischemik berulang, nyeri dada memberat

Atrial flutter
Laki-laki 76 th, perokok, keluhan (-), akan operasi reseksi kolon ok tumor

premature ventricular contraction
Laki-laki 32 th, gemuk, tidak nyaman di dada hilang timbul, terutama kalau cape.

Wide complex tachycardia
Laki-laki 66 th, perokok, DM, nyeri dada 8 jam yg lalu, tiba2 kolaps

Supraventricular tachycardia
Perempuan 36 th, HT, berdebar-debar sejak 2 jam yll, hilang-timbul

Ventricular flutter
Laki-laki 36 th, dyslipidemia, nyeri dada 6 jam yg lalu, mendadak, Trop T (+), tiba-tiba kolaps di IGD

KASUS 1

EKG

Interpretasi EKG ?
Jawaban: D

Kasus 2 Pria 50 thn, CAD post PTCA, Hipertensi Berdebar & lemas 3 jam SMRS, hemodinamik
stabil

Diagnosis EKG
A. Supraventricular Tachycardia (AVNRT)
B. Atrial TachycardiaC. Atrial FlutterD. Atrial Fibrillasi
Jawaban: A

KASUS 3
Pria 67 tahun, anggota DPR Berdebar dan sesak nafas sejak 2 jam Hipertensi dan PPOK Tidak ada bukti klinis CAD


Apa diagnosis EKG ?
A. Atrial fibrillationB. Atrial TachycardiaC. Sinus arrhythmiaD. Atrial flutter
Jawaban: D

Kasus 4 Wanita 45 tahun Lemas, lekas capek dan sesak nafas
bila aktivitas

Diagnosis EKG
A. Sick Sinus Syndrome
B. AV blok derajat 2 Mobitz II
C. Sinus arrest
D. AV blok derajat 3
Jawaban: D

Kasus 5 : Laki-laki, 50 thn. Chest pain dengan Troponin T (+)

A. UAPB. STEMI Anteroseptal (fase evolusi)C. NSTEMI AnteroseptalD. NSTEMI Anterior Ekstensif
Jawaban : B
JAWABAN :

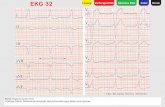
KASUS 6

EKG

Interpretasi EKG ?
Jawaban : C

KASUS 7

EKG

Interpretasi EKG ?
Jawaban : D

KASUS 8

EKG

Interpretasi EKG ?
Jawaban : B

151
THANK YOU- ANY QUESTION?





![RENSTRA UNWAR 2015 - 2018 - WordPress.com · 2020. 1. 8. · [RENSTRA UNWAR] 2015 - 2018 3 1.3 Manfaat Rencana Strategis Universitas Warmadewa akan memberikan manfaat kepada pihak](https://static.fdocuments.net/doc/165x107/6090fa1ef1d2296be273ab84/renstra-unwar-2015-2018-2020-1-8-renstra-unwar-2015-2018-3-13-manfaat.jpg)









![KULIAH CARDIO1 baru.ppt [Read-Only] - ocw.usu.ac.idocw.usu.ac.id/.../kesehatan_anak_slide_kardiologi_anak1.pdf · EKG / Ro N AUSKULTASI JANTUNG A. B.JTG I :PENUTUPAN KATUP MITRAL](https://static.fdocuments.net/doc/165x107/5b0e15c67f8b9a8b038e9e2d/kuliah-cardio1-baruppt-read-only-ocwusuacidocwusuacidkesehatananakslidekardiologianak1pdfekg.jpg)
