Journal club oesophageal motility disorders and manometry
48
Journal Club Esophageal Manometry and Motility disorders By Dr G Madhu Kumar Under Guidance of Dr L Hari Prasad MS Dr Kishore Babu MS Dr Ramachandram DNB Dr Venkat Reddy MS
-
Upload
aravind-endamu -
Category
Health & Medicine
-
view
133 -
download
3
Transcript of Journal club oesophageal motility disorders and manometry

Journal ClubEsophageal Manometry and Motility disorders
ByDr G Madhu Kumar
Under Guidance of Dr L Hari Prasad MS Dr Kishore Babu MS
Dr Ramachandram DNB Dr Venkat Reddy MS

Anatomy
• Oesophagus is a muscular tube, approximately 25 cm long, mainly occupying the posterior mediastinum and extending from the upper oesophageal sphincter (the cricopharyngeus muscle) inthe neck to the junction with the cardia of the stomach
• It has striated muscles, a transition zone and only smooth muscles in lower oesophagus
• Lined throughout with squamous epithelium

• Important distances 15, 25 and 40 cm for anatomical location during endoscopy

Physiology
• The upper oesophageal sphincter is normally closed at rest and is a protective mechanism against regurgitation of oesophageal contents into the respiratory passages
• The Lower oesophageal sphincter (LOS) is a zone of relatively high pressure that prevents gastric contents from refluxing into the lower oesophagus

• The normal LOS is 3–4 cm long and has a pressure of 10–25 mmHg
• LOS pressure is measured by perfused tubes or microtransducers.
• Accurate measurement of sphincter relaxation is achieved using a device (Dent sleeve) that straddles the highpressure zone.

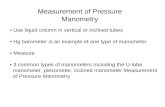
Oesophageal manometry• Done by passing a multi lumen
catheter with three to eight recording orifices at different levels down the oesophagus and into the stomach.
• Electronic microtransducers that are not influenced by changes in patient position during the test have gradually supplanted perfusion systems
• Catheter is withdrawn progressively up the oesophagus, and recordings are taken at intervals of 0.5–1.0 cm to measure the length and pressure of the LOS and assess motility in the body of the oesophagus during swallowing

Indications• Evaluation of noncardiac chest pain or esophageal symptoms not
diagnosed by endoscopy (or after GERD has been excluded) • Evaluation for achalasia or another type of nonobstructive
dysphagia • Preoperative evaluation for patients undergoing corrective
surgery for GERD, particularly if an alternative diagnosis like Scleroderma or achalasia is being considered
• Postoperative evaluation of dysphagia in patients who underwent corrective surgery for reflux or after treatment of achalasia
• Prior to esophageal pH monitoring to assess the location of the lower esophageal sphincter for proper electrode positioning
• Evaluation of esophageal motility problems associated with systemic diseases

Contraindications
• Patients with altered mental status or obtundation • Patients who cannot understand or follow
instructions • Suspicion or known pharyngeal or upper
esophageal obstruction (eg, tumors) • Patients with severe clotting disorders • Patients with known esophageal problems such as
deep ulcers, varices, Zenker's diverticula, and strictures

• Anesthesia – topical lidocaine spray for the pharynx
• Position – – Sitting upright, catheter is passed through the
nose, down the throat, and through the oesophagus into the stomach while the patient takes small sips
– Latter patient is asked to lay down


Complications
• Mild complications like gagging durring the catheter insertion, sore throat, rhinorrhea, and epistaxis.
• Although rare in occurrence, more severe complications include arrhythmias, vasovagal episodes, bronchospasm, aspiration, and oesophageal perforation,

Motility Disorders
• Primary oesophageal motility disorders (PEMDs)– Spastic disorders – Achalasia
• Spastic disorders include – Nutcracker esophagus, – Diffuse esophageal spasm(DES),– Hypertensive lower esophageal sphincter (HLES)
• Secondary causes of esophageal motility diabetes mellitus, Chagas’ disease, collagen vascular diseases, and multiple sclerosis

Spastic Motility Disorders
• Spastic disorders include – Nutcracker esophagus, – Diffuse esophageal spasm(DES),– Hypertensive lower esophageal sphincter (HLES)
• GERD is a significant cause of esophageal dysmotility and should be evaluated for its presence.
• Its successful treatment, medically or surgically, often mitigates the symptoms suffered by many patients

Diffuse Esophageal Spasm• First described by Osgood in 1889• Found only in 3–5% of patients evaluated for Esophageal motility
disorders • Symptoms - chest pain and dysphagia, and functional obstructive
symptom• Difficult to differentiate from GERD• Investigations - pH and manometry• Abnormal reflux is found – treat GERD• Manometry –
– Greater than 10% (but <100%) of wet swallows that are followed by simultaneous esophageal contractions of amplitude 30 mm Hg or greater
– LES dysfunction, manifested by improper relaxation and/or hypertensive state
– Intermittent peristalsis and prolonged contractions


• Small series have shown good results for relief of dysphagia after esophageal myotomy in up to 80% of highly selected patients,
• Chest pain is more difficult to cure.• A careful, thorough workup and exclusion of GERD
as a confounding factor should be done before attempting to diagnose and surgically treat DES.
• Medical management is an appropriate initial approach

Nutcracker Esophagus
• First described by Brand and associates in 1977• Symptoms - chest pain and dysphagia• Association with GERD may be present• Manometry - hypertensive esophageal
contractions of greater than 180 mm Hg• Management –– Calcium channel– Tricyclic antidepressants


Hypertensive Lower Esophageal Sphincter
• Defined as having a resting LES pressure of greater than 45 mm Hg with intact, normal peristalsis
• Symptoms - chest pain and/or dysphagia• Association with GERD may be present


• Management– Medical management to reduce LES pressures• Calcium channel blockers,• Botulinum toxin, • Phosphodiesterase inhibitors
– Associated with GERD• Nissen fundoplication – Good results – GERD cause of
HLES– Not associated with GERD• Myotomy and partial fundoplication – primary
sphincter problem

Achalasia
• Idiopathic achalasia is a primary motor disorder affecting the esophagus.
• Has complete aperistalsis of the esophagus, • Frequently encountered motility disorder seen
by surgeons• Incidence of 1–3 per 100,000 population• Most common PEMD

• Due to result of injury and fibrosis of these cells and myenteric nerves
• Autoimmune disorder - immunohistochemical markers - CD3/CD8 lymphocyte found
• Histopathologic hallmark of the disease remains near complete or total loss of the myenteric plexus ganglion cells
• By above two mechanisms which result in loss of peristalsis and impaired relaxation of the LES -Pathophysiologic findings of impaired esophageal emptying - aperistalsis, and a nonrelaxing LES.

• Symptoms– Dysphagia, – Regurgitation of indigested food,– Complaints of food “sticking” in the chest– worsen after lying supine– Cold liquids exacerbate symptoms– Frequent regurgitation and aspiration can lead to
pulmonary complications. – Weight loss

• Evaluation– Barium esophagram- “bird’s beak” appearance– Manometry
• Aperistalsis of the esophageal body and impaired relaxation of the LES• Waveforms are typically low amplitude and
simultaneous – Endoscopy – Inspect mucosa and GE junction– CT and/or endoscopic ultrasound – R/O
Pseudoachlasia


Treatment• Involve pharmacologic, endoscopic, and surgical
therapies• Medical therapy - Drugs that relaxsmooth
muscle and decrease LES pressure.– Nitrates– Calcium channel blockers– Phosphodiesterase inhibitor
• Endoscopic therapies– Balloon dilation– Botulinumtoxin injection

Surgical therapies
• Surgical myotomy was first described by Ernst Heller in 1913.
• Myotomy for achalasia is associated with good longterm results and relief from dysphagia.
• Long-term follow-up studies have demonstrated symptom relief in nearly 75% of patients

• Shimi et al reported the first laparoscopic Heller myotomy in 1991
• Pellegrini et al reported the first thoracoscopic approach in 1992
• Laparoscopic performance of myotomy, when compared with thoracoscopic technique, has better symptomatic improvement (89.3 vs 77.6%) and a lower incidence of reflux symptoms when combined with a partial fundoplication (14.9 vs 28.3%).

• Myotomy should extend 6–7 cm above the GE junction and 0.5–1.5 cm below the GE junction
• Addition of an antireflux procedure to a standard Heller myotomy has been thought to reduce these symptoms and improve outcomes
• Still being Studing

Journals

• Diagnosis of Esophageal Motility Disorders: Esophageal Pressure Topography vs. Conventional Line Tracing
• by Dustin A Carlson MD et al• Published in Am J Gastroenterol 2015• Aim –– To investigate whether the inter-rater agreement
and/or accuracy of esophageal motility diagnosis differed between EPT and CLT.

• Methods– Forty previously completed patient HRM studies
were selected for analysis – Six experienced gastroenterologists and six
gastroenterology trainees interpreted each of the 40 studies using both EPT and CLT formats.
– Rater diagnoses were assessed for inter-rater agreement and diagnostic accuracy, both for exact diagnosis and for correct identification of a major esophageal motility disorders

• Results– Among all raters, the odds of an incorrect exact
esophageal motility diagnosis were 3.3 times higher with CLT assessment than with EPT (OR: 3.3; 95% CI: 2.4–4.5; P<0.0001), and the odds of incorrect identification of a major motility disorder were 3.4 times higher with CLT than with EPT (OR: 3.4; 2.4–5.0; P<0.0001).
• Conclusions– Superior inter-rater agreement and diagnostic accuracy
of esophageal motility diagnoses were demonstrated with analysis using EPT over CLT among our selected raters. On the basis of these findings, EPT may be the preferred assessment modality of esophageal motility

• How the Body Position Can Influence High-resolution Manometry Results in the Study of Esophageal Dysphagia and Gastroesophageal Reflux Disease
• By Constanza Ciriza-de-los-Ríos et al• Published in J Neurogastroenterol Motil. 2015
Jul• Aim– To examine whether the body position influences
HRM diagnoses in patients with esophageal dysphagia and gastroesophageal reflux disease (GERD).

• Method– HRM (Manoscan) was performed in 99 patients in the sitting and
supine positions. HRM plots were analyzed according to the Chicago classification.]
• Results– HRM results varied in the final diagnoses of the esophageal body
(EB) in patients with dysphagia (P = 0.024), the result being more distal spasm and weak peristalsis while sitting. In patients with GERD,
– HRM diagnoses of the lower esophageal sphincter (LES), the esophagogastric junction (EGJ) morphology, and EB varied depending on the position; (P = 0.063, P = 0.017, P = 0.041 respectively).
– Hypotensive LES, EGJ type III (hiatal hernia), and weak peristalsis were more frequently identified in the sitting position.
– The reliability (kappa) of the position influencing HRM diagnoses was similar in dysphagia and GERD
– The reliability in “EGJ morphology” studies was higher in dysphagia 0.81 (0.68–0.94) than in GERD 0.55 (0.37–0.73), P = 0.020

• Conclusions– HRM results varied according to the position in
patients with dysphagia and GERD. – Weak peristalsis was more frequently diagnosed
while sitting in dysphagia and GERD.– Hypotensive LES and EGJ type III (hiatal hernia)
were also more frequently diagnosed in the sitting position in patients with GERD.

• Botulinum Toxin Reduces Dysphagia in Patients With Nonachalasia Primary Esophageal Motility Disorders
• By Tim Vanuytse et al• Published in Clinical Gastroenterology and Hepatology
September 2013• Background & Aims– Endoscopic injection of botulinum toxin (BTX) has shown
benefits for patients with diffuse esophageal spasm (DES) and nutcracker esophagus (NE) in small uncontrolled trials.
– We investigated the effect of BTX on symptoms of patients with DES or NE and assessed manometry findings in a prospective, double-blind, randomized, controlled study

• Methods– We assessed 22 patients with dysphagia-predominant, manometry-
confirmed DES or NE (6 men; age, 63 ± 2 y) at a tertiary care medical center.
– Patients were given injections of BTX (8 × 12.5 U) or saline (8 × 0.5 mL) in 4 quadrants, at 2 and 7 cm above the esophagogastric junction.
– After 1 month, patients crossed over between groups and received endoscopic injections of BTX or saline. When the study began and 4 weeks after each injection, the patients were assessed by esophageal manometry and completed a symptom questionnaire (to determine solid and liquid dysphagia, chest pain, and regurgitation and heartburn; all scored 0–4).
– Responders were defined based on modified Vantrappen criteria for achalasia.

• Results– After BTX injections, patients had significant decreases in total
symptom scores (sum of solid and liquid dysphagia and chest pain; from 7.6 ± 0.7 to 4.8 ± 0.8; P = .01); this decrease was not observed in patients who received saline injections.
– Moreover, BTX injection stabilized unintentional weight loss (weight gain of 0.3 ± 0.3 after BTX injection vs further weight loss of 1.6 ± 0.5 kg after saline injection; P = .01).
– Fifty percent of patients had a response 1 month after BTX injection, compared with 10% after saline injection (P = .04); 30% still had a response 1 year after BTX injection.
– BTX injection also caused a significant decrease in the mean esophagogastric junction pressure, compared with baseline (15.8 ± 1.7 vs 24.0 ± 2.8 mm Hg; P = .02).
• Conclusions– In a prospective controlled study of patients with DES and NE,
injections of BTX reduced symptoms and stabilized unintentional weight loss

• A utility of peroral endoscopic myotomy (POEM) across the spectrum of esophageal motility disorders
• By Toshitaka Hoppo et al• Published in Surgical Endoscopy April 2015• Background– Peroral endoscopic myotomy (POEM) has been
performed as a novel endoscopic procedure to treat achalasia with favorable outcome.
– The objective of this study was to assess the outcome of POEM in our initial series and to assess the safety and efficacy of POEM in a variety of esophageal motility-related clinical problems

• Methods– This is a retrospective cross-sectional study involving all patients with
esophageal motility disorders defined by the Chicago classification, who had undergone consideration for POEM at our institution.
– Validated questionnaires such as gastroesophageal reflux disease health-related quality of life (GERD-HRQL), reflux symptom index (RSI) and achalasia disease-specific health-related quality of life were obtained pre- and postoperatively.
• Results– A total of 35 POEMs (achalasia n = 25, non-achalasia n = 10) were
performed on 33 patients (female n = 20, male n = 13, mean age 56.9 years).
– During a mean follow-up period of 7 months (range 0.5–17), 92 % of patients with achalasia and 75 % of those with non-achalasia motility disorders had a symptomatic improvement in dysphagia.
– Chest pain was completely resolved in all patients with achalasia (8/8) and 80 % of patients with non-achalasia (4/5). The GERD-HRQL, RSI and dysphagia scores significantly improved after POEM in patients with achalasia.
– There was a significant improvement in GERD-HRQL and RSI scores, and a trend toward lower dysphagia score in patients with non-achalasia.

• Conclusions– The outcome of POEM to treat achalasia and non-
achalasia motility disorders is consistent with previous studies.
– Potential benefit of POEM includes not only its flexibility to adjust the length and location of myotomy but also the ability to extend myotomy proximally without thoracoscopy or thoracotomy.
– POEM can be combined with laparoscopic procedures and used as “salvage” for localized esophageal dysmotility

• Laparoscopic Dor versus Toupet fundoplication following Heller myotomy for achalasia: results of a multicenter, prospective, randomized-controlled trial
• By Arthur Rawlings• Published in Surgical Endoscopy January 2012,• Background– The type of fundoplication that should be performed in
conjunction with Heller myotomy for esophageal achalasia is controversial.
– We prospectively compared anterior fundoplication (Dor) with partial posterior fundoplication (Toupet) in patients undergoing laparoscopic Heller myotomy.

• Methods– A multicenter, prospective, randomized-controlled
trial was initiated to compare Dor versus Toupet fundoplication after laparoscopic Heller myotomy.
– Outcome measures were symptomatic GERD scores (0–4, five-point Likert scale questionnaire) and 24-h pH testing at 6–12 months after surgery. Data are mean ± SD.
– Statistical analysis was by Mann–Whitney U test, Wilcoxon signed rank test, and Freidman’s test.

• Results– Sixty of 85 originally enrolled and randomized patients who underwent
36 Dor and 24 Toupet fundoplications had follow-up data per protocol for analysis.
– Dor and Toupet groups were similar in age (46.8 vs. 51.7 years) and gender (52.8 vs. 62.5% male).
– pH studies at 6–12 months in 43 patients (72%: Dor n = 24 and Toupet n = 19) showed total DeMeester scores and % time pH < 4 were not significant between the two groups.
– Abnormal acid reflux was present in 10 of 24 Dor group patients (41.7%) and in 4 of 19 Toupet patients (21.0%) (p = 0.152).
– Dysphagia and regurgitation symptom scores improved significantly in both groups compared to preoperative scores.
– No significant differences in any esophageal symptoms were noted between the two groups preoperatively or at follow-up.
– SF-36 quality-of-life measures changed significantly from pre- to postoperative for five of ten domains in the Dor group and seven of ten in the Toupet patients (not significant between groups).

• Conclusion– Laparoscopic Heller myotomy provides significant
improvement in dysphagia and regurgitation symptoms in achalasia patients regardless of the type of partial fundoplication.
– Although a higher percentage of patients in the Dor group had abnormal 24-h pH test results compared to those of patients who underwent Toupet, the differences were not statistically significant.

THANK YOU