Introduction Oesophageal duplication cysts are rare congenital oesophageal anomalies in adults and...
1
Introduction Oesophageal duplication cysts are rare congenital oesophageal anomalies in adults and are mostly asymptomatic. Diagnosis of an oesophageal duplication cyst is usually made in infancy and childhood while investigating for respiratory distress or feeding difficulty. Complications are known to occur during the natural course of the disease due to bleeding, infection and mass effect. We describe the diagnostic pitfalls and management of a case of oesophageal duplication cyst simulating oesophageal GIST, causing retro- sternal pain, gastro oesophageal reflux and intermittent dysphagia. Tarek I. El-Houssari, Amir Kambal, Haythem Ali, Ashraf Rasheed Oesophageal Duplication Cyst Masquerading as a Gastrointestinal Stromal Tumour Gwent Institute for Minimal Access Surgery Case Report A 40-year-old man, previously asymptomatic, presented with nocturnal heartburn, progressive dysphagia and retro-sternal pain. His past history was un-remarkable. The upper endoscopy revealed a distal sub-mucosal oesophageal lesion and the barium swallow confirmed the large extrinsic impression along the right side of the distal oesophagus. Contrast enhanced computed tomography (CT) showed a well-circumscribed pre- vertebral thin-wall mass measuring 50 mm in diameter. Endoscopic ultrasonography (EUS) concurred with CT findings and suggested it to be GIST in nature. A laparoscopic distal oesophagectomy and proximal gastrectomy was carried out for the presumed symptomatic oesophageal GIST to an excellent effect. The histology confirmed it to be a duplication cyst. Discussion The case demonstrates the clinical and the radiological features of oesophageal duplication cyst and highlights the need for a strong index of suspicion if one has to diagnose oesophageal duplication cyst preoperatively. Figure 1. CT Images of the Oesophageal Duplication Cyst • Oesophageal duplication cysts are rare entities that are usually found incidentally during the early years while investigating for respiratory or poor feeding complaints. Surgical excision of these cysts is the mainstay treatment modality for these cysts for fear of complications. These complications range from aspiration, infection, and bleeding to perforation. • In our case, a 39 years old gentleman presented with cough, progressive dysphagia, retro-sternal pain and nocturnal heartburn. He proceeded to have an upper endoscopy and a CT of the chest revealing an opacity at the origin of the left upper lobe of the lung and 5.7 x 3.9 cm oval soft tissue mass on the right side of the lower oesophagus just above the gastro-oesophageal junction. •Bronchoscopy was performed and was normal and a diagnosis of either leiomyoma or an oesophageal GIST was entertained based on the endoscopy and the imaging. • The patient was referred then to us when we organised an endoscopic ultrasound revealing a 4.5 cm sub-mucosal lesion at the level of the left atrium. This hypo-echoic lesion had a well defined capsule and was described to be non-cystic. No fine needle aspiration (FNA) was attempted in fear of the risk of dissemination of this presumed oesophageal GIST (Gastrointestinal Stromal Tumour) and we proceeded to minimal access resection of the lesion (Laparoscopic Gastro-oesophagectomy). Figure 3. EUS showing the submucosal lesion Figure 2. Endoscopic view of the submucosal oesophageal mass Figure 4. Gastro- Oesophagectomy Specimen Figure 5. Incision of the lesion confirmed it to be cystic in nature
-
Upload
neil-heath -
Category
Documents
-
view
223 -
download
1
Transcript of Introduction Oesophageal duplication cysts are rare congenital oesophageal anomalies in adults and...

IntroductionOesophageal duplication cysts are rare congenital oesophageal anomalies in adults and are mostly asymptomatic. Diagnosis of an oesophageal duplication cyst is usually made in infancy and childhood while investigating for respiratory distress or feeding difficulty. Complications are known to occur during the natural course of the disease due to bleeding, infection and mass effect. We describe the diagnostic pitfalls and management of a case of oesophageal duplication cyst simulating oesophageal GIST, causing retro-sternal pain, gastro oesophageal
reflux and intermittent dysphagia.
Tarek I. El-Houssari, Amir Kambal, Haythem Ali, Ashraf Rasheed
Oesophageal Duplication Cyst Masquerading
as a Gastrointestinal Stromal Tumour
Gwent Institute for Minimal Access Surgery
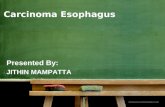
Case ReportA 40-year-old man, previously asymptomatic, presented with nocturnal heartburn, progressive dysphagia and retro-sternal pain. His past history was un-remarkable. The upper endoscopy revealed a distal sub-mucosal oesophageal lesion and the barium swallow confirmed the large extrinsic impression along the right side of the distal oesophagus. Contrast enhanced computed tomography (CT) showed a well-circumscribed pre-vertebral thin-wall mass measuring 50 mm in diameter. Endoscopic ultrasonography (EUS) concurred with CT findings and suggested it to be GIST in nature. A laparoscopic distal oesophagectomy and proximal gastrectomy was carried out for the presumed symptomatic oesophageal GIST to an excellent effect. The histology confirmed it to be a duplication cyst.
DiscussionThe case demonstrates the clinical and the radiological features of oesophageal duplication cyst and highlights the need for a strong index of suspicion if one has to diagnose oesophageal duplication cyst preoperatively.
Figure 1. CT Images of the Oesophageal Duplication Cyst
• Oesophageal duplication cysts are rare entities that are usually found incidentally during the early years while investigating for respiratory or poor feeding complaints. Surgical excision of these cysts is the mainstay treatment modality for these cysts for fear of complications. These complications range from aspiration, infection, and bleeding to perforation. • In our case, a 39 years old gentleman presented with cough, progressive dysphagia, retro-sternal pain and nocturnal heartburn. He proceeded to have an upper endoscopy and a CT of the chest revealing an opacity at the origin of the left upper lobe of the lung and 5.7 x 3.9 cm oval soft tissue mass on the right side of the lower oesophagus just above the gastro-oesophageal junction.
•Bronchoscopy was performed and was normal and a diagnosis of either
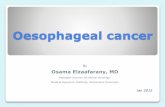
leiomyoma or an oesophageal GIST was entertained based on the endoscopy and the imaging. • The patient was referred then to us when we organised an endoscopic ultrasound revealing a 4.5 cm sub-mucosal lesion at the level of the left atrium. This hypo-echoic lesion had a well defined capsule and was described to be non-cystic. No fine needle aspiration (FNA) was attempted in fear of the risk of dissemination of this presumed oesophageal GIST (Gastrointestinal Stromal Tumour) and we proceeded to minimal access resection of the lesion (Laparoscopic Gastro-oesophagectomy).
• The procedure was followed by uneventful recovery and the histology confirmed it to be duplication cyst.
• Careful pre-operative EUS interrogation of oesophageal sub-mucosal lesions and entertainment of the possibility of oesophageal duplication cyst as a differential diagnosis is necessary to allow better therapeutic planning.
Figure 3. EUS showing the submucosal lesion
Figure 2. Endoscopic view of the submucosal oesophageal mass
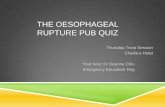
Figure 4. Gastro-Oesophagectomy Specimen
Figure 5. Incision of the lesion confirmed it to be
cystic in nature