TA152 Coronary artery disease - drug-eluting stents: guidance ...
Upload
beverly-lambCategory
view
221download
0
Is Coronary Artery Bypass Surgery Is Coronary Artery Bypass Surgery Really Better than Coronary Really Better than Coronary
Stents?Stents?A look at the risks and benefitsA look at the risks and benefits
Sarah SmithSarah SmithAdvisor: Dr. GrimesAdvisor: Dr. Grimes

Why is this important?Why is this important?
The leading cause of death in the United The leading cause of death in the United States is coronary heart diseaseStates is coronary heart disease
It accounts for about 1 million deaths per It accounts for about 1 million deaths per yearyear
About 43% of heart disease deaths are About 43% of heart disease deaths are related to coronary artery diseaserelated to coronary artery disease
Heart disease is the leading cause of death Heart disease is the leading cause of death of American women, accounting for 32% of of American women, accounting for 32% of all deaths per year.all deaths per year. One in three women will die from heart disease, One in three women will die from heart disease,
while one in 25 will die from breast cancerwhile one in 25 will die from breast cancer Trends in the United States suggest that half Trends in the United States suggest that half
of healthy 40-year-old males will develop of healthy 40-year-old males will develop CAD in the future, and one in three healthy CAD in the future, and one in three healthy 40-year-old women40-year-old women

PathophysiologyPathophysiology
CAD is a chronic CAD is a chronic disease in which the disease in which the coronary arteries coronary arteries gradually harden and gradually harden and narrownarrow
Limitation of blood flow Limitation of blood flow to the heart causes to the heart causes ischemia of the ischemia of the myocardial cells, myocardial cells, leading to a myocardial leading to a myocardial infarctioninfarction
This leads to heart This leads to heart muscle damage, heart muscle damage, heart muscle death and later muscle death and later scarring without heart scarring without heart muscle regrowthmuscle regrowth

Pathophysiology Cont.Pathophysiology Cont.
CAD can be thought of as a wide spectrum of CAD can be thought of as a wide spectrum of disease of the heartdisease of the heart
At one end is the asymptomatic individual with At one end is the asymptomatic individual with fatty streaks within the walls of the coronary fatty streaks within the walls of the coronary arteriesarteries Over time these streaks will increase in thickness and Over time these streaks will increase in thickness and
may affect the flow of blood through the arteriesmay affect the flow of blood through the arteries As the plaque continues to grow and obstruct the As the plaque continues to grow and obstruct the
vessel to more than 70% the patient typically vessel to more than 70% the patient typically develops symptoms of obstructive coronary artery develops symptoms of obstructive coronary artery diseasedisease
At this stage the patient is said to have At this stage the patient is said to have ischemic heart disease, meaning the patient’s ischemic heart disease, meaning the patient’s heart is experiencing an increased workload, heart is experiencing an increased workload, thus reduced blood supply to the heart wallsthus reduced blood supply to the heart walls

PathophysiologyPathophysiology
As CAD progresses, there may be As CAD progresses, there may be nearly complete obstruction of the nearly complete obstruction of the lumen of the coronary arterylumen of the coronary artery
Patients at this level have typically Patients at this level have typically suffered from 1 or more myocardial suffered from 1 or more myocardial infarctions, and may have angina at infarctions, and may have angina at rest and pulmonary edemarest and pulmonary edema
An individual may develop a rupture An individual may develop a rupture of a plaque at any stage of the of a plaque at any stage of the spectrum.spectrum. The acute rupture a plaque may lead to The acute rupture a plaque may lead to
an acute MIan acute MI

Risk FactorsRisk Factors
Family history of premature CADFamily history of premature CAD SmokingSmoking Diabetes mellitusDiabetes mellitus HTNHTN HyperlipidemiaHyperlipidemia obesityobesity

Presentation/DiagnosisPresentation/Diagnosis
Generally patients present with stable Generally patients present with stable angina, unstable angina, or a angina, unstable angina, or a myocardial infarctionmyocardial infarction
Coronary angiogram is currently golden Coronary angiogram is currently golden standard for determining the presence standard for determining the presence of obstructive coronary artery diseaseof obstructive coronary artery disease Yields a 2D picture of coronary arteriesYields a 2D picture of coronary arteries A catheter is inserted into the coronary A catheter is inserted into the coronary
arteries and injected with dyearteries and injected with dye The dye allows the physician to pinpoint The dye allows the physician to pinpoint
the number and location of blockages in the number and location of blockages in the coronary arteriesthe coronary arteries

Treatment OptionsTreatment Options
There are many different treatment There are many different treatment options availableoptions available
A physician will look into the patients’ A physician will look into the patients’ individual risk factors, severity of the individual risk factors, severity of the blocked artery, and analyze the blocked artery, and analyze the benefits and risks for possible benefits and risks for possible proceduresprocedures
Two popular procedures are PCTA/stent Two popular procedures are PCTA/stent implantation and CABG surgeryimplantation and CABG surgery
Medical therapy is also available for a Medical therapy is also available for a more conservative treatmentmore conservative treatment

Overview of StentsOverview of Stents
1/3 of patients with CAD will undergo coronary 1/3 of patients with CAD will undergo coronary angioplasty with stents or Percutaneous Transluminal angioplasty with stents or Percutaneous Transluminal Coronary Angioplasty (PCTA)Coronary Angioplasty (PCTA)
Angioplasty involves temporarily inserting and Angioplasty involves temporarily inserting and expanding a tiny balloon at the site of blockage to expanding a tiny balloon at the site of blockage to help widen the narrowed arteryhelp widen the narrowed artery
Usually combined with stent implantation in the Usually combined with stent implantation in the artery to help prop it open and decrease the chance artery to help prop it open and decrease the chance of it narrowing again or restenosisof it narrowing again or restenosis
Performed in cardiac catheterization lab and are non-Performed in cardiac catheterization lab and are non-surgical treatmentsurgical treatment
Usually last about 1-2 hours and most patients are Usually last about 1-2 hours and most patients are usually discharged in 1-2 days after a procedureusually discharged in 1-2 days after a procedure
Stents are a stainless or nytinol mesh like deviceStents are a stainless or nytinol mesh like device Angioplasty and StentsAngioplasty and Stents YouTubeYouTube Stent Stent

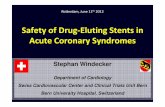
StentsStents
A stent is a stainless tube with A stent is a stainless tube with slots. It is mounted on a balloon slots. It is mounted on a balloon catheter in a collapsed state. catheter in a collapsed state. When the balloon is imflated, the When the balloon is imflated, the stent expands and pushes itself stent expands and pushes itself against the inner wall of the against the inner wall of the coronary artery.coronary artery.
The risk of emergency referral for The risk of emergency referral for CABG and need for subsequent CABG and need for subsequent revascularization procedures has revascularization procedures has reduced by more than 50% reduced by more than 50% because of coronary stentsbecause of coronary stents
Stent implantation has shown to Stent implantation has shown to reduce restenosis in vessels with reduce restenosis in vessels with reference diameter >3mm, reference diameter >3mm, however in-stent restenosis still however in-stent restenosis still occurs in about 10-40% of patientsoccurs in about 10-40% of patients
According to the American Heart According to the American Heart Association stents can be Association stents can be considered for use in patients who considered for use in patients who have significant disease of left have significant disease of left main and left anterior descending main and left anterior descending coronary artery. Also patients with coronary artery. Also patients with 2 or 3-vessel disease should be 2 or 3-vessel disease should be consideredconsidered
In previous years these In previous years these patients were only candidates patients were only candidates for bypass surgeryfor bypass surgery

Risks/Benefits of StentsRisks/Benefits of Stents
Benefits:Benefits: Shorter procedural Shorter procedural
and recovery time and recovery time than CABGthan CABG
Angina relief about Angina relief about 75% of the time75% of the time
Decreases the risk Decreases the risk for heart attackfor heart attack
Increases blood flow Increases blood flow to the heartto the heart
Risks and Risks and Limitations:Limitations: Risk of death <1%Risk of death <1% Risk of heart attack, Risk of heart attack,
thrombosis and thrombosis and bleeding <4%bleeding <4%
Major limitation of Major limitation of procedure is a high procedure is a high rate of restenosis and rate of restenosis and need for need for revascularizationrevascularization
Scar tissue formationScar tissue formation Not a cure to the Not a cure to the
disease, still need to disease, still need to reduce risk factors reduce risk factors and make lifestyle and make lifestyle changes to prevent changes to prevent future disease future disease progressionprogression

Research…Research…
Patients receiving stents had lower incidence Patients receiving stents had lower incidence of death, MI, and stroke at 30-day follow-up of death, MI, and stroke at 30-day follow-up compared to CABG.compared to CABG.
However, patients receiving stents had a However, patients receiving stents had a higher incidence of repeat revascularization higher incidence of repeat revascularization proceduresprocedures 25% of patients at 1 year and 47% at 5 years25% of patients at 1 year and 47% at 5 years
This high risk of restenosis is one of the This high risk of restenosis is one of the major reasons for patients refusing major reasons for patients refusing angioplasty and opting for other treatment angioplasty and opting for other treatment modalities like surgerymodalities like surgery
The introduction of drug-eluting stents may The introduction of drug-eluting stents may shift patients from surgical procedures back shift patients from surgical procedures back to angioplasty and stent use.to angioplasty and stent use.

Drug-eluting StentsDrug-eluting Stents
These are stents that are coated with These are stents that are coated with a drug that is known to interfere with a drug that is known to interfere with the process of restenosisthe process of restenosis
As of December 2007, the FDA has As of December 2007, the FDA has approved of 2 DES: sirolimus-eluting approved of 2 DES: sirolimus-eluting stents and paclitaxel-eluting stentsstents and paclitaxel-eluting stents
Studies show that there is a 70-90% Studies show that there is a 70-90% reduced rate of restenosis when reduced rate of restenosis when compared with bare-metal stentscompared with bare-metal stents
DES were first introduced in April DES were first introduced in April 2003, and just 9 months later made 2003, and just 9 months later made up 35% of all stent implantations in up 35% of all stent implantations in the United Statesthe United States

Problem with DES?Problem with DES?
1. They are expensive1. They are expensive It costs about $2200 for a DES, when compared to bare-It costs about $2200 for a DES, when compared to bare-
metal stents which costs about $600.metal stents which costs about $600. In one study they looked at the cost-effectiveness of In one study they looked at the cost-effectiveness of
DES. They took into account the fact that there will be DES. They took into account the fact that there will be reduced repeat revascularization procedures, and reduced repeat revascularization procedures, and discovered that there was still an increase in $600 per discovered that there was still an increase in $600 per patient, and with an estimated 1 million procedures patient, and with an estimated 1 million procedures done a year, about $600 million increased in annual done a year, about $600 million increased in annual healthcare spendinghealthcare spending
2. The drug agents can interfere with the healing 2. The drug agents can interfere with the healing process and found to hamper natural vascular healing process and found to hamper natural vascular healing processprocess In 2007, the FDA has cautioned the use of DES, because In 2007, the FDA has cautioned the use of DES, because
they are associated with increased risks of both early they are associated with increased risks of both early and late stent thrombosis, as well as death, and and late stent thrombosis, as well as death, and myocardial infarctionmyocardial infarction
DES are still a novel idea; it will be interesting to see DES are still a novel idea; it will be interesting to see the research that comes out in the next couple years the research that comes out in the next couple years looking at their effectiveness and future indicationslooking at their effectiveness and future indications

Overview of CABGOverview of CABG
CABG is still the best therapy for CABG is still the best therapy for reintervation for most patients reintervation for most patients with proximal left anterior with proximal left anterior descending, multivessel, and left descending, multivessel, and left main-stem coronary artery main-stem coronary artery diseasedisease
Of the patients with CAD, about Of the patients with CAD, about 10% will undergo CABG surgery10% will undergo CABG surgery
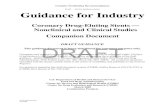
CABG is a surgery that increases CABG is a surgery that increases blood flow to the heart by blood flow to the heart by creating a detour and re-routing creating a detour and re-routing the blood flow around the blocked the blood flow around the blocked portion of the artery. portion of the artery.
A section of a blood vessel from A section of a blood vessel from another part of the body is another part of the body is removed and grafted above and removed and grafted above and below the damaged portion of the below the damaged portion of the coronary artery to form an un-coronary artery to form an un-blocked arteryblocked artery
Most commonly used are the Most commonly used are the saphenous vein and internal saphenous vein and internal thoracic arterythoracic artery
This procedure is performed with This procedure is performed with assistance of a heart-lung assistance of a heart-lung machine, which supports the machine, which supports the patient’s blood during surgerypatient’s blood during surgery
CABG SurgeryCABG Surgery

Risks/Benefits CABG Risks/Benefits CABG surgerysurgery
CABG was introduced about 50 years ago CABG was introduced about 50 years ago and is now performed in 1 million patients and is now performed in 1 million patients at a cost exceeding $20 billion annuallyat a cost exceeding $20 billion annually
Many benefits such as decrease in angina, Many benefits such as decrease in angina, improved life-span, and providing an improved life-span, and providing an effective route for blood with prevention of effective route for blood with prevention of new plaques to formnew plaques to form
Surgery is however a much more serious Surgery is however a much more serious operation that lasts a long time, with a long operation that lasts a long time, with a long recovery timerecovery time
Some complications seen after surgery are Some complications seen after surgery are atrial fibrillation, increased risk of stroke, atrial fibrillation, increased risk of stroke, and cognitive dysfunctionand cognitive dysfunction

Research…Research…
Less than 5% chance of heart damage and less than Less than 5% chance of heart damage and less than 2% chance of death2% chance of death
Stroke or other neurological injury occurs in 5% Stroke or other neurological injury occurs in 5% patientspatients
Atrial fibrillation occurs in 20-40% of patients after Atrial fibrillation occurs in 20-40% of patients after CABGCABG
2 reasons as to why CABG offers survival advantages 2 reasons as to why CABG offers survival advantages for multivessel and left main-stem coronary artery for multivessel and left main-stem coronary artery diseasedisease 1. Bypass grafts are placed on the midcoronary vessel, 1. Bypass grafts are placed on the midcoronary vessel,
CABG not only protects the culprit lesion, but also offers CABG not only protects the culprit lesion, but also offers prophylaxis against new lesions in diseased prophylaxis against new lesions in diseased endotheliumendothelium
Where stents only treat immediate culprit lesion, with no Where stents only treat immediate culprit lesion, with no protective effect against the development of new diseaseprotective effect against the development of new disease
2. failure of stents to achieve complete 2. failure of stents to achieve complete revascularization in most patients with multivessel revascularization in most patients with multivessel disease reduces survival proportional to the degree of disease reduces survival proportional to the degree of incomplete revascularizationincomplete revascularization

Isolated LAD and Left-main Isolated LAD and Left-main stem CADstem CAD
CAD in LAD has been reported as high as CAD in LAD has been reported as high as 50% among patients who undergo CABG50% among patients who undergo CABG
CABG is regarded as an accepted golden CABG is regarded as an accepted golden standard for left main coronary artery standard for left main coronary artery diseasedisease
CABG has generally been considered the CABG has generally been considered the golden standard of therapy for left-main stem golden standard of therapy for left-main stem stenosis for the last decade.stenosis for the last decade. However, there are recent studies out that show However, there are recent studies out that show
patients underwent PCI more than CABG for this patients underwent PCI more than CABG for this type of disease. This artery has a relatively large type of disease. This artery has a relatively large diameter, making it an attractive site for PCIdiameter, making it an attractive site for PCI
Restenosis rates in a study were 30.3% in bare-Restenosis rates in a study were 30.3% in bare-metal stents, 7.4% in DES group, and 3.7% in CABG metal stents, 7.4% in DES group, and 3.7% in CABG groupgroup

Multivessel CADMultivessel CAD
MVD accounts for approximately 60% of the MVD accounts for approximately 60% of the CAD patientsCAD patients
The use of stents in these patients has The use of stents in these patients has resulted in higher restenosis and repeat resulted in higher restenosis and repeat vascularization rates than in patients treated vascularization rates than in patients treated with surgerywith surgery Stents group had 16.8% restenosis rate as Stents group had 16.8% restenosis rate as
compared with 3.5% who underwent surgerycompared with 3.5% who underwent surgery CABG patients also experience fewer MI and CABG patients also experience fewer MI and
major adverse cardiovascular eventsmajor adverse cardiovascular events DES have decreased the difference between DES have decreased the difference between
CABG and bare-metal stentsCABG and bare-metal stents In order for PCI to replace CABG as the In order for PCI to replace CABG as the
preferred therapy in MVD, clinical trials must preferred therapy in MVD, clinical trials must demonstrate long-term outcomes that are demonstrate long-term outcomes that are equivalentequivalent

What about the Diabetic What about the Diabetic Patient?Patient?
The diabetic patient is a high risk for coronary artery The diabetic patient is a high risk for coronary artery disease, the incidence and severity of the disease disease, the incidence and severity of the disease are higher as compared to nondiabetic patientare higher as compared to nondiabetic patient
Revascularization of diabetic patients has been a Revascularization of diabetic patients has been a huge dilemma and a great challengehuge dilemma and a great challenge
A study confirmed that even a low-risk diabetic A study confirmed that even a low-risk diabetic patient there is a survival advantage at 10 years for patient there is a survival advantage at 10 years for CABG in comparision with PCI of 58% vs. 46%CABG in comparision with PCI of 58% vs. 46% Also found that there is a huge difference in the need Also found that there is a huge difference in the need
for revascularization in both; 18% of CABG patients and for revascularization in both; 18% of CABG patients and 80% of PCI80% of PCI
Studies state that the preferred revascularization Studies state that the preferred revascularization strategy in the diabetic patient with MVD is CABG strategy in the diabetic patient with MVD is CABG surgerysurgery Lower mortality in CABG patients vs. PCI patients (1.4% Lower mortality in CABG patients vs. PCI patients (1.4%
vs. 12.8%)vs. 12.8%) Lower major adverse cardiovascular events (8.6% vs. Lower major adverse cardiovascular events (8.6% vs.
26.6%)26.6%)

The FutureThe Future
Minimally invasive direct coronary artery bypass Minimally invasive direct coronary artery bypass (MIDCAB) is on the rise(MIDCAB) is on the rise
It is performed on a beating heart with use of stabilizing It is performed on a beating heart with use of stabilizing devices or using minimal access bypass system with devices or using minimal access bypass system with endo-aortic clamping and cardioplegic arrestendo-aortic clamping and cardioplegic arrest
Yields shorter hospital stay with lower postoperative Yields shorter hospital stay with lower postoperative complications and better quality of life with similar complications and better quality of life with similar safety and long-term efficacy as conventional CABGsafety and long-term efficacy as conventional CABG
Robotic instrumentation is also developingRobotic instrumentation is also developing Surgery does not have a single chest incision of any kind, Surgery does not have a single chest incision of any kind,
this surgery requires 3 pencil-sizes holes made between this surgery requires 3 pencil-sizes holes made between the ribsthe ribs
2 robotic arms and an endoscope gain access to the heart, 2 robotic arms and an endoscope gain access to the heart, making surgery possible without opening the chestmaking surgery possible without opening the chest
Has been proven that these patients get out of the Has been proven that these patients get out of the hospital 1-2 days earlierhospital 1-2 days earlier
This technique may develop into new technology that This technique may develop into new technology that might be used more often in the future and may replace might be used more often in the future and may replace open heart surgeryopen heart surgery

ConclusionConclusion
CABG still remains that best therapy in CABG still remains that best therapy in terms of superior survival and decreased terms of superior survival and decreased need for reintervention for most patients need for reintervention for most patients with proximal LAD, multivessel, and left with proximal LAD, multivessel, and left main-stem CAD.main-stem CAD.
These affects are magnified in the diabetic These affects are magnified in the diabetic patientpatient
PCI with stent is still chosen as treatment PCI with stent is still chosen as treatment option for single-vessel disease, and now option for single-vessel disease, and now considered for 2 or 3-vessel diseaseconsidered for 2 or 3-vessel disease
Each patient is evaluated for the best Each patient is evaluated for the best treatment option based on their own risk treatment option based on their own risk factors and progression of diseasefactors and progression of disease

ReferencesReferences
REFERENCES:REFERENCES: Anderson, H. Vernon, Richard E. Shaw, Ralph G Brindis, Kathleen Hewitt, Ronald Krone, Peter C. Block, Charles R. McKay, Anderson, H. Vernon, Richard E. Shaw, Ralph G Brindis, Kathleen Hewitt, Ronald Krone, Peter C. Block, Charles R. McKay,
Williams S. Weintraub. “A contemporary overview of percutaneous coronary interventions: The American College of Williams S. Weintraub. “A contemporary overview of percutaneous coronary interventions: The American College of Cardiology-National Cardiovascular Registry.” Cardiology-National Cardiovascular Registry.” Journal of the American College of Cardiology.Journal of the American College of Cardiology. 39 (2002): 1096-1103. 39 (2002): 1096-1103.
Aziz, Omer, Christopher Rao, Sukhmeet Singh Panesar, Catherine Jones, Stephen Morris, Ara Darzi, Thanos Athanasiou. Aziz, Omer, Christopher Rao, Sukhmeet Singh Panesar, Catherine Jones, Stephen Morris, Ara Darzi, Thanos Athanasiou. “Meta-analysis of minimally invasive internal thoracic artery bypass versus percutaneous revascularization for isolated “Meta-analysis of minimally invasive internal thoracic artery bypass versus percutaneous revascularization for isolated lesions of the left anterior descending artery.”lesions of the left anterior descending artery.”
Bair, Tami L., Joseph B. Muhlestein, Heidi T. May, Kent G. Meredith, Benjamin D. Horne, Robert R. Pearson, Qunyu Li, Kurt Bair, Tami L., Joseph B. Muhlestein, Heidi T. May, Kent G. Meredith, Benjamin D. Horne, Robert R. Pearson, Qunyu Li, Kurt R. Jensen, Jeffrey L. Anderson, and Donald L. Lappe. “ Surgical Revascularization is associated with improved long-term R. Jensen, Jeffrey L. Anderson, and Donald L. Lappe. “ Surgical Revascularization is associated with improved long-term outcomes compared with percutaneous stenting in most subgroups of patients with multivessel coronary artery disease: outcomes compared with percutaneous stenting in most subgroups of patients with multivessel coronary artery disease: results from the intermountain heart registry.” results from the intermountain heart registry.” Journal of the American Heart Association.Journal of the American Heart Association. 116 (2007): 226-231. 116 (2007): 226-231.
Bravata, Dena M., Allison L. Glenger, Kathryn M. McDonald, Vandana Sundaram, Marco V. Perez, Robin Varghese, John R. Bravata, Dena M., Allison L. Glenger, Kathryn M. McDonald, Vandana Sundaram, Marco V. Perez, Robin Varghese, John R. Kapoor, Reza Ardehall, Douglas Owens, and Mark A. Hlatky. “The Comparative effectiveness of Percutaneous Coronary Kapoor, Reza Ardehall, Douglas Owens, and Mark A. Hlatky. “The Comparative effectiveness of Percutaneous Coronary Interventions and Coronary Artery Bypass Graft Surgery.” Interventions and Coronary Artery Bypass Graft Surgery.” American College of Physicians.American College of Physicians. 147 (2007): 1-15. 147 (2007): 1-15.
Davies, MJ. “Coronary Disease: The Pathophysiology of acute coronary syndromes.” Davies, MJ. “Coronary Disease: The Pathophysiology of acute coronary syndromes.” HeartHeart. 83 (2000): 361-3666. 83 (2000): 361-3666 Daemen, Joost, Patrick W. Serruys. “Drug-Eluting stent update 2007: Part I: A survey of current and future generation Daemen, Joost, Patrick W. Serruys. “Drug-Eluting stent update 2007: Part I: A survey of current and future generation
drug-eluting stents: meaningful advances or more of the same?” drug-eluting stents: meaningful advances or more of the same?” Circulation.Circulation. 116 (2007): 316-328. 116 (2007): 316-328. Daemen, Joost, Pattrick W. Serruys. “Drug-eluting stent update 2007: Part II Unsettled issues” Daemen, Joost, Pattrick W. Serruys. “Drug-eluting stent update 2007: Part II Unsettled issues” Circulation.Circulation. 116 (2007): 961- 116 (2007): 961-
968.968. Elsasser, A. H. Mollmann, H.M. Nef, C.W. Hamn. “How to revascularize patients with diabetes mellitus- Bypass or stents Elsasser, A. H. Mollmann, H.M. Nef, C.W. Hamn. “How to revascularize patients with diabetes mellitus- Bypass or stents
and drugs?” and drugs?” Clinical Research in Cardiology.Clinical Research in Cardiology. 95.4 (2006): 193-202. 95.4 (2006): 193-202. Eisenberg, Mark J. “Drug-Eluting Stents, The price is not right.” Eisenberg, Mark J. “Drug-Eluting Stents, The price is not right.” Circulation.Circulation. 114 (2006): 1745-1754. 114 (2006): 1745-1754. Farb, A. Boam MS. “Stent Thrombosis Redux- the FDA perspective.” Farb, A. Boam MS. “Stent Thrombosis Redux- the FDA perspective.” New England Journal of Medicine. New England Journal of Medicine. 356 (2007): 984-356 (2007): 984-
987.987. Gupta, S., and Brig MM Gupta. “Coronary Artery Bypass Surgery or Drug Eluting Stent for Unprotected Left Main Coronary Gupta, S., and Brig MM Gupta. “Coronary Artery Bypass Surgery or Drug Eluting Stent for Unprotected Left Main Coronary
Artery Disease. Artery Disease. Journal of The Association of Physicians of India.Journal of The Association of Physicians of India. 55 (2007): 287-291. 55 (2007): 287-291. Harmon DC, Ghori KG, Eustace NP, O’Callaghan SJF, O’Donnell AP, Shorten GD. “Aprotinin decreases the incidence of Harmon DC, Ghori KG, Eustace NP, O’Callaghan SJF, O’Donnell AP, Shorten GD. “Aprotinin decreases the incidence of
cognitive deficit following CABG and cardiopulmonary bypass: a pilot randomized controlled study.” cognitive deficit following CABG and cardiopulmonary bypass: a pilot randomized controlled study.” Canadian Journal of Canadian Journal of Anethesia Anethesia 51 51 ((2004)51:10.2004)51:10.
Jaffery, Zehra, Marcin Kowalski, W. Douglas Weaver, Sanjaya Khanal. “A meta-alysis of randomized control trials Jaffery, Zehra, Marcin Kowalski, W. Douglas Weaver, Sanjaya Khanal. “A meta-alysis of randomized control trials comparing minimally invasive direct coronary bypass grafting versus percutaneous coronary intervention for stenosis of comparing minimally invasive direct coronary bypass grafting versus percutaneous coronary intervention for stenosis of the proximal left anterior descending artery.” the proximal left anterior descending artery.” European Journal of Cardio thoracic Surgery.European Journal of Cardio thoracic Surgery. 31 (2007): 691-697. 31 (2007): 691-697.
Javaid, Aamir, Daniel H. Steinberg, Ashlesh N. Buch, Paul J. Corson, Steven W. Boyce, Tina L. Pinto Slottow, Probal K, Peter Javaid, Aamir, Daniel H. Steinberg, Ashlesh N. Buch, Paul J. Corson, Steven W. Boyce, Tina L. Pinto Slottow, Probal K, Peter Hill, Teruo Okabe, Rebecca Torguson, and et. “Outcomes of Coronary Artery Bypass Grafting versus Percutaneous Hill, Teruo Okabe, Rebecca Torguson, and et. “Outcomes of Coronary Artery Bypass Grafting versus Percutaneous Coronary Intervention with Drug-Eluting Stents for patients with Mulitivessel Coronary Artery Disease.” Coronary Intervention with Drug-Eluting Stents for patients with Mulitivessel Coronary Artery Disease.” Circulation.Circulation. 116 116 (2007): I-200-I-206.(2007): I-200-I-206.
Kaiser, Christopher, Hans Peter Brunner-LaRocca, Peter T Buser, Piero O Bonneti, Stefan Osswald, Andre Linka, Andreas Kaiser, Christopher, Hans Peter Brunner-LaRocca, Peter T Buser, Piero O Bonneti, Stefan Osswald, Andre Linka, Andreas Zutter, Michael Zellweger, Leticia Grize, Matthias E Pfisteter. “Incremental cost-effectiveness of drug-eluting stents Zutter, Michael Zellweger, Leticia Grize, Matthias E Pfisteter. “Incremental cost-effectiveness of drug-eluting stents compared with a third generation bare-metal stent in a real world setting: randomized Basel Stent Kosten Effectivitats compared with a third generation bare-metal stent in a real world setting: randomized Basel Stent Kosten Effectivitats Trial” Trial” Lancet.Lancet. 366 (2005): 921-929. 366 (2005): 921-929.

ReferencesReferences
Kappert U, Schneider J, Cichon R, Gulielmos V, Tugtekin SM, Nicolai J, Matschke K, Schueler S. “Development of Kappert U, Schneider J, Cichon R, Gulielmos V, Tugtekin SM, Nicolai J, Matschke K, Schueler S. “Development of Robotic Enhanced Endoscopic Surgery for the treatment of Coronary Artery Disease.” Robotic Enhanced Endoscopic Surgery for the treatment of Coronary Artery Disease.” CirculationCirculation. 104 (2001): . 104 (2001): 102-107.102-107.
Lee MS, Kapoor N, Jamal F, Czer L, Aragon J, Forrester J, Kar S, Donhad S, Kass R, Eigler N, Trento A, Shah PK, Lee MS, Kapoor N, Jamal F, Czer L, Aragon J, Forrester J, Kar S, Donhad S, Kass R, Eigler N, Trento A, Shah PK, Makkar RR. “Comparison of coronary artery bypass surgery with percutaneous coronary intervention with drug Makkar RR. “Comparison of coronary artery bypass surgery with percutaneous coronary intervention with drug eluting stents for unprotected left main coronary artery disease.” eluting stents for unprotected left main coronary artery disease.” Journal of American College of Cardiology.Journal of American College of Cardiology. 47 47 (2006): 864-870.(2006): 864-870.
Legrand, Victor M.G., Patrick W. Serruys, Felix Unger, Ben A. van Hout, Mathias C.M. Vrolix, Geert M.P. Fransen, Legrand, Victor M.G., Patrick W. Serruys, Felix Unger, Ben A. van Hout, Mathias C.M. Vrolix, Geert M.P. Fransen, Torsten Toftegaard Nielsen, Peter Kildeberg Paulsen, Ricardo Seabra Gomes and et. “Three-year outcomes after Torsten Toftegaard Nielsen, Peter Kildeberg Paulsen, Ricardo Seabra Gomes and et. “Three-year outcomes after coronary stenting versus bypass surgery for the treatment of multivessel disease” coronary stenting versus bypass surgery for the treatment of multivessel disease” Circulation.Circulation. 109 (2004): 1114- 109 (2004): 1114-1120.1120.
Lemos, Pedro, Patrick Serruys, Edurdo Sousa. “Drug-Eluting Stents; Cost versus clinical benefit.” Lemos, Pedro, Patrick Serruys, Edurdo Sousa. “Drug-Eluting Stents; Cost versus clinical benefit.” Circulation.Circulation. 107 107 (2003): 3003-3007.(2003): 3003-3007.
Libby P, Theroux P. “Pathophysiology of Coronary Artery Disease.” Libby P, Theroux P. “Pathophysiology of Coronary Artery Disease.” Circulation.Circulation. 111 (2005): 3481-3488. 111 (2005): 3481-3488. Medline Plus: Heart Bypass Surgery. Retrieved August 16, 2008 from Medline Plus: Heart Bypass Surgery. Retrieved August 16, 2008 from
http://www.nlm.nih.gov/medlineplus/ency/article/002946.htmhttp://www.nlm.nih.gov/medlineplus/ency/article/002946.htm.. Mercado, Nestor, William Wijns, Patrick W. Serruys, Ulrich Sigwart, Marcus D. Flather, Rodney H. Stables, William Mercado, Nestor, William Wijns, Patrick W. Serruys, Ulrich Sigwart, Marcus D. Flather, Rodney H. Stables, William
W. O’Neil, Alfredo Rodriguez, Pedro A. Lemos, Whady A. Hueb, Bernard J. Gersh, Jean Booth, and Eric Boersma. W. O’Neil, Alfredo Rodriguez, Pedro A. Lemos, Whady A. Hueb, Bernard J. Gersh, Jean Booth, and Eric Boersma. “One-year outcomes of coronary artery bypass graft surgery versus percutaneous coronary intervention with “One-year outcomes of coronary artery bypass graft surgery versus percutaneous coronary intervention with multiple stenting for multisystem disease: A meta-analysis of individual patient data from randomized clinical multiple stenting for multisystem disease: A meta-analysis of individual patient data from randomized clinical trials.” trials.” The Journal of Thoracic and Cardiovascular SurgeryThe Journal of Thoracic and Cardiovascular Surgery. 130.2 (2005): 512-519.. 130.2 (2005): 512-519.
Michaels AD, Chatterjee K. “Angioplasty versus bypass surgery for Coronary Artery Disease.” Michaels AD, Chatterjee K. “Angioplasty versus bypass surgery for Coronary Artery Disease.” CirculationCirculation. 106 . 106 (2000): 187-190.(2000): 187-190.
Morrison DA, Sethi G, Sacks J, et al. “Percutaneous coronary intervention versus coronary artery bypass graft Morrison DA, Sethi G, Sacks J, et al. “Percutaneous coronary intervention versus coronary artery bypass graft surgery for patients with medically refractory myocardial ischemia and risk factors for adverse outcome with surgery for patients with medically refractory myocardial ischemia and risk factors for adverse outcome with bypass: a multicenter, randomized trial.” bypass: a multicenter, randomized trial.” Journal of the American College of Cardiology.Journal of the American College of Cardiology. 38 (2001): 143-149. 38 (2001): 143-149.
Morton, A.C., R.D. Walker, and J. Gunn. “Current Challenges in coronary stenting: from bench to bedside.” Morton, A.C., R.D. Walker, and J. Gunn. “Current Challenges in coronary stenting: from bench to bedside.” Biochemical society transations.Biochemical society transations. 35.5 (2007): 900-904. 35.5 (2007): 900-904.
O’Keefe, James H., Thomas R. Kreamer, Philip G. Jones, James L. Vacek, Michael E. Gorton, Gregory F. O’Keefe, James H., Thomas R. Kreamer, Philip G. Jones, James L. Vacek, Michael E. Gorton, Gregory F. Muehlebach, Barry D. Rutherford, Ben D. McCallister. “Isolated Left Anterior Descending Artery Disease: Muehlebach, Barry D. Rutherford, Ben D. McCallister. “Isolated Left Anterior Descending Artery Disease: Percutaneous Transluminal Coronary Angioplasty versus Stenting versus Left Internal Mammary artery bypass Percutaneous Transluminal Coronary Angioplasty versus Stenting versus Left Internal Mammary artery bypass Grafting.” Grafting.” Circulation.Circulation. 100 (1999): II114-II118. 100 (1999): II114-II118.
O’Neil, William W., Martin B. Leon. “Drug-Eluting stents: Cost versus clinical benefit.” O’Neil, William W., Martin B. Leon. “Drug-Eluting stents: Cost versus clinical benefit.” Circulation.Circulation. 107 (2003): 107 (2003): 3008-3011.3008-3011.
Ott, Elizabeth, David Mazer, Iulia Tudor, Linda Shore-Lesserson, Stephanie Snyder-Ramos, Barry Finegan, Patrick Ott, Elizabeth, David Mazer, Iulia Tudor, Linda Shore-Lesserson, Stephanie Snyder-Ramos, Barry Finegan, Patrick Mohnle, Charles Hantler, Bernd Bottiger, Ray Latimer, Warren Browner, Jack Levin, Dennis Mangano. “Coronary Mohnle, Charles Hantler, Bernd Bottiger, Ray Latimer, Warren Browner, Jack Levin, Dennis Mangano. “Coronary artery bypass graft surgery- care globalization: The impack of national care on fatal and nonfatal outcome.” artery bypass graft surgery- care globalization: The impack of national care on fatal and nonfatal outcome.” The The Journal of Thoracic and Cardiovascular Surgery.Journal of Thoracic and Cardiovascular Surgery. 133 (2007): 1242-1251. 133 (2007): 1242-1251.

ReferencesReferences
Patil, CV., E. Nikolsky, M. Boulos, E. Grenadier, R. Beyar. “Multivessel coronary artery disease: current revascularization strategies.” Patil, CV., E. Nikolsky, M. Boulos, E. Grenadier, R. Beyar. “Multivessel coronary artery disease: current revascularization strategies.” European Heart Journal.European Heart Journal. 22 (2001): 1183-1197. 22 (2001): 1183-1197.
Rao, Christopher, Omer Aziz, Sukhmeet Singh Panesar, Catherine Jones, Stephen Morris, Ara Darzi, Thanos Athanasiou. “Cost Rao, Christopher, Omer Aziz, Sukhmeet Singh Panesar, Catherine Jones, Stephen Morris, Ara Darzi, Thanos Athanasiou. “Cost Effectiveness analysis of minimally invasive internal thoracic artery bypass versus percutatneous revascularization for isolated Effectiveness analysis of minimally invasive internal thoracic artery bypass versus percutatneous revascularization for isolated lesions of the left anterior descending artery.” lesions of the left anterior descending artery.” British Medical Journal.British Medical Journal. 334 (2007): 621-628. 334 (2007): 621-628.
Rihal, Charanjit, Dominic L. Raco, Bernard J. Gersh, Salim, Yusuf. “Indications for Coronary Artery Bypass Surgery and Percutaneious Rihal, Charanjit, Dominic L. Raco, Bernard J. Gersh, Salim, Yusuf. “Indications for Coronary Artery Bypass Surgery and Percutaneious Coronary Intervention in Chronic Stable Angina: Review of the Evidence and Methodological Considerations.” Coronary Intervention in Chronic Stable Angina: Review of the Evidence and Methodological Considerations.” Circulation.Circulation. 108 (2003): 108 (2003): 2439-2445.2439-2445.
Rodriguez, Alfredo E., Andrew O. Maree, Juan Mieres, Daniel Berrocal, Lilliana Grinfeld, Carlos Fernandez-Pereira, Valeria Curotto, Rodriguez, Alfredo E., Andrew O. Maree, Juan Mieres, Daniel Berrocal, Lilliana Grinfeld, Carlos Fernandez-Pereira, Valeria Curotto, Alfredo Rodriguez-Granillo, William O’Neill, and Igor F. Palacios. “Late loss of early benefit from drug-eluting stents when compared Alfredo Rodriguez-Granillo, William O’Neill, and Igor F. Palacios. “Late loss of early benefit from drug-eluting stents when compared with bare-metal stents and coronary artery bypass surgery: 3 years follow-up of the ERACI III registry.” with bare-metal stents and coronary artery bypass surgery: 3 years follow-up of the ERACI III registry.” The European Society of The European Society of Cardiology.Cardiology. 28 (2007): 2118-2125 28 (2007): 2118-2125
Ryan, Jason, David Cohen. “Will drug-eluting stents bankrupt the healthcare system? Are drug-eluting stents cost-effective? It Ryan, Jason, David Cohen. “Will drug-eluting stents bankrupt the healthcare system? Are drug-eluting stents cost-effective? It depends on who you ask.” depends on who you ask.” Circulation.Circulation. 114 (2006): 1736-1744. 114 (2006): 1736-1744.
Schaar, Johannes A., James E. Muller, Erling Falk, Renu Virmani, Valentin Fuster, Patrick Serruys, Antonio Colombo, Christodoulos Schaar, Johannes A., James E. Muller, Erling Falk, Renu Virmani, Valentin Fuster, Patrick Serruys, Antonio Colombo, Christodoulos Stefanadis, S. Ward Casscells, Pedro R. Moreno, Attilio Maseri, Anton van der Steen. “Terminology for high-risk and vulnerable Stefanadis, S. Ward Casscells, Pedro R. Moreno, Attilio Maseri, Anton van der Steen. “Terminology for high-risk and vulnerable coronary artery plaques.” coronary artery plaques.” European Heart Journal.European Heart Journal. 25 (2004): 1077-1082. 25 (2004): 1077-1082.
Serruys, Patrick W., Felix Unger, J. Eduardo Sousa, Adib Jatene, Hans J.R.M. Bonnier, Jacques P.A.M Schonberger, Nigel Buller, Robert Serruys, Patrick W., Felix Unger, J. Eduardo Sousa, Adib Jatene, Hans J.R.M. Bonnier, Jacques P.A.M Schonberger, Nigel Buller, Robert Bonser, Marcel J.B. VAN DEN Brand, Lex A. VAN Herwerden, Marie-Angele M. Morel, and Ben A. VAN HOUT. “Comparison of Coronary-Bonser, Marcel J.B. VAN DEN Brand, Lex A. VAN Herwerden, Marie-Angele M. Morel, and Ben A. VAN HOUT. “Comparison of Coronary-Artery Bypass Surgery and Stenting for the Treatment of Multivessel Disease.” Artery Bypass Surgery and Stenting for the Treatment of Multivessel Disease.” New England Journal of MedicineNew England Journal of Medicine. 344.15 (2001): . 344.15 (2001): 1117-1124.1117-1124.
Serruys, Patrick W., Andrew T. L. Ong, Lex A. van Herwerden, Eduardo Sousa, Adib Jantene, Johannes Bonnier, Jacque Schoenberger, Serruys, Patrick W., Andrew T. L. Ong, Lex A. van Herwerden, Eduardo Sousa, Adib Jantene, Johannes Bonnier, Jacque Schoenberger, Nigel Buller, Robert Bonser, Clemens Disco, Bianca Backx, Paul Hugenholtz, Brian Firth, Felix Unger. “Five-year outcomes after Nigel Buller, Robert Bonser, Clemens Disco, Bianca Backx, Paul Hugenholtz, Brian Firth, Felix Unger. “Five-year outcomes after coronary stenting versus bypass surgery for the treatment of mulivessel disease.” coronary stenting versus bypass surgery for the treatment of mulivessel disease.” Journal of American College of Cardiology.Journal of American College of Cardiology. 46 46 (2005): 575-581.(2005): 575-581.
Spiess, B, et al. “Platelet transfusions during coronary artery bypass graft surgery are associated with serious adverse outcomes.” Spiess, B, et al. “Platelet transfusions during coronary artery bypass graft surgery are associated with serious adverse outcomes.” TransfusionTransfusion 44 (2004):1143-48. 44 (2004):1143-48.
Stephenson, Larry W. Mercedes K. C. Dullum. “Coronary Artery Bypass Surgery.” Available at: Stephenson, Larry W. Mercedes K. C. Dullum. “Coronary Artery Bypass Surgery.” Available at: http://www.heartcenteronline.com/myheartdr/common/articles.cfm?ARTID=332, December 2004. Retrieved February 7, 2008.http://www.heartcenteronline.com/myheartdr/common/articles.cfm?ARTID=332, December 2004. Retrieved February 7, 2008.
Sundt, Thoralf M. “Adult Cardiac Surgery: Coronary Artery Bypass Grafting Surgery.” Retrieved February 7, 2008 from Sundt, Thoralf M. “Adult Cardiac Surgery: Coronary Artery Bypass Grafting Surgery.” Retrieved February 7, 2008 from http://www.sts.org/doc/3706http://www.sts.org/doc/3706
Taggart, DP. “Coronary artery bypass graft vs. percutaneous coronary angioplasty: CABG on the rebound?” Taggart, DP. “Coronary artery bypass graft vs. percutaneous coronary angioplasty: CABG on the rebound?” Lippincott Williams and Lippincott Williams and Wilkins, Inc.Wilkins, Inc. 22 (2007): 517-523. 22 (2007): 517-523.
Villareal, Rollo P., Vei-Vei Lee, MacArthur A. Elayda, and James M. Wilson. "Coronary Artery Bypass Surgery versus Coronary Villareal, Rollo P., Vei-Vei Lee, MacArthur A. Elayda, and James M. Wilson. "Coronary Artery Bypass Surgery versus Coronary Stenting." Stenting." Texas Heart Institute JournalTexas Heart Institute Journal 29.1 (2002): 3-9. 29.1 (2002): 3-9.
Virmani, R, Farb A., “Pathology of in-stent restenosis.” Virmani, R, Farb A., “Pathology of in-stent restenosis.” Curropin Lipidol.Curropin Lipidol. 10(1999): 499-506. 10(1999): 499-506. Yang, Zhen Kun, Wei Feng Shen, Rui Yan Zhang, Ye Kong, Jian Sheng Zhang, Jian Hu, Qi Zhang, and Feng Hua Ding. "Coronary Artery Yang, Zhen Kun, Wei Feng Shen, Rui Yan Zhang, Ye Kong, Jian Sheng Zhang, Jian Hu, Qi Zhang, and Feng Hua Ding. "Coronary Artery
Bypass Surgery Versus Percutaneous Coronary Intervention with Drug-Eluting Stent Implantatio in Patinets with Multivessel Coronary Bypass Surgery Versus Percutaneous Coronary Intervention with Drug-Eluting Stent Implantatio in Patinets with Multivessel Coronary Disease." Disease." Journal of Interventional CardiologyJournal of Interventional Cardiology 20.1 (2007): 10-16. 20.1 (2007): 10-16.
Zaman, Azfar G., Andrew Archbold, Gerard Helft, Elizabeth A. Paul, Nicholas P. Curzen, Peter G. Mills. “Atrial fibrillation after coronary Zaman, Azfar G., Andrew Archbold, Gerard Helft, Elizabeth A. Paul, Nicholas P. Curzen, Peter G. Mills. “Atrial fibrillation after coronary artery bypass surgery: A model for Preoperative Risk Stratification artery bypass surgery: A model for Preoperative Risk Stratification Circulation.Circulation. 101 (2000): 1403-1408. 101 (2000): 1403-1408.