Intestinal Obstruction
52
Intestinal Obstruction By Dr. Asfand PGR S.U IV
-
Upload
asfandyar-khan -
Category
Documents
-
view
42 -
download
0
description
Intestinal Obstruction presentation
Transcript of Intestinal Obstruction

Intestinal Obstruction
By Dr. AsfandPGR S.U IV

Is a partial or complete blockage of forward progression of intestinal contents (chyle) due to mechanical or functional causes
can occur at any level distal to the duodenum
Is a medical emergency (20% of acute surgical admissions & 5-10 % of acute abdomen patients)
Complications include bowel ischemia & Perforation
Introduction

Mechanical/Functional congenital/acquired; partial(incomplete or subacute)/complete; acute/acute on chronic/or chronic; simple/closed loop/strangulated; proximal/distal
Classification

EtiologyDynamic (Mechanical) Adynamic (Functional)
Intraluminal:Gallstones, Foreign Body, Round worms, impacted faeces, Bezoars, Meconium ileus
Intramural:TB stricture, IBD, Malignancy
Extraluminal:Bands/Adhesions, Hernia, Intussusception, Volvulus
Paralytic Ileus◦ Post Surgery/trauma◦ Electrolyte imbalance◦ Diabetes mellitus (DKA)◦ Uremia
Drugs – Narcotics, Anticholinergics
Mesenteric ischaemia Pseudo-obstruction

80% in small bowel – usually ileum20% in colon – usually sigmoid colon (70% CA, 30% due to diverticulosis, volvulus & inflammatory causes)
Incidence

Direct External compression◦ Adhesions◦ Hernia
Interruption of mesenteric blood flow
◦ Intussussception◦ Volvulus
Primary occlusion of mesentric blood vessles :
acute mesentric ischemia
Closed Loop Obstruction◦ Hernia◦ Adhesions
Strangulated intestinal obstruction(interference of mesenteric blood supply)

Continuous severe pain
Shock indicates underlying ischemia
Symptoms commence suddenly and recur regularly
Local tenderness associated with rigidity and rebound tenderness ( Blumbergs sign )
Features of Strangulation

Acute colonic pseudo-obstruction
It is massive colonic dilatation affecting caecum and Rt. colon with presentation of colonic obstruction without any mechanical blockage
It likely results from imbalance of autonomic regulation of colonic motility with excessive parasympathetic suppression causing atony to distal colon causing functional obstruction
The vast majority of patients are Elderly hospitalized patients with major TRAUMA; ILLENESS; MAJOR NON-INTESTINAL SURGERY
(Stress)

Afferent & Efferent limbs of bowel are obstructed
The rich bacterial flora w/in the loop adds to the production of gases causing rapid distension
Closed Loop Obstruction

Rapid distension inc luminal pressure Impaired circulation bowel necrosis & perforation fulminant peritonitis
Typically seen in colon with competent ileocaecal valve
Hernia, Adhesions, Volvulus
Closed Loop Obstruction

Pathophysiology/Features
Fluid & Gas accumulates
Further Distention of Intestine
Vigorous Contractions
Severe Colicky Abdominal
pain
BorborygmiVomiting/ Metabolic Alkalosis
High pitched Bowel Sounds

Inc contractions &Distention
Inc Intra-luminal Pressure
Defective absorption/Inc intestinal secretion
Inc venous pressureHence venous return impairs
Congestion, Edema --- jeopardizes Arterial supply – ischemia & Gangrene
Perforation Bacterial / toxintranslocation
Peritonitis/Bacteremia, Septicemia
Multiple air fluid levels
Severe Dehydration
Fluid & Electrolyte Imbalance
Dec Bowel Sounds
Shock Death

History Physical Examination Lab Tests Imaging• X-Ray (Abdomen & Chest)• Contrast enhanced CT Scan◦ Barium Studies◦ U/S◦ MRI
Diagnosis

These clinical features and also the clinical course vary according to the LEVEL & CAUSE of obstruction
History
Cardinal features
Abdominal pain
Distension Vomiting
Absolute constipation

Proximal small bowel
Distal small bowel
Large bowel
Severe vomiting Moderate vomiting Late vomiting
Less distension Central distension Early distension , pronounced
Colicky pain Central abdominal pain Less pain
Constipation late Varies in appearance Constipation is early feature
Severe dehydration Moderate Less dehydration
Comparison of clinical aspects

Distension - minimal /absent in mesenteric vascular occlusion
Fever signifies inflammation in bowel wall / ischemia / perforation
Hypothermia -- when septicemia due to poor pyrogenic response
Specific Points

Physical ExaminationOthers
Systemic examination If deemed necessary.•CNS•Vascular•Gynaecological•Muscuoloskeltal
Abdominal
•Abdominal distension and it’s pattern•Hernial orifices•Visible peristalsis•Tympanitic Abdomen•Cecal distension•Tenderness, guarding and rebound•Organomegaly•Bowel sounds
–High pitched–Absent
•Rectal examination
General
•Vital signs: P, BP, RR, T, Sat•dehydration•Anaemia, jaundice, LN•Assessment of vomitus if possible•Full lung and heart examination

visible peristalsis seen in obstruction

CBC Anemia, Leukocytosis Urea/ Creatinine Dehydration Serum Electrolytes
Random Blood Sugar - DM Coagulation Screen - DIC LFTs - Bilirubin & Alk Phosphatase Serum Amylase - non-specific
Lab Tests

Radiological EvaluationPlain X-Ray
Always request: Supine, Upright, lateral and CXR(Obstructive Series)
Diagnostic in 60% of cases but further evaluation (CT or barium studies) may be necessary in rest of the cases

Findings
Supine Film: Gas Distended Bowel Loops
Supine Film:◦ Gas distended Bowel
Loops
SBO LBO

Contd…… Upright Film
◦ Multiple Air Fluid levels “Stepladder pattern”
Flat surfaces at the Air Fluid interface

Difference Between Large & Small Bowel Obstruction
Small Bowel Large bowel
•Central (diameter 2.5cm to 5cm)•Vulvulae conniventes
•Peripheral ( diameter 5cm+) •Presence of haustration•Presence of solid faeces
vulvulae conniventes
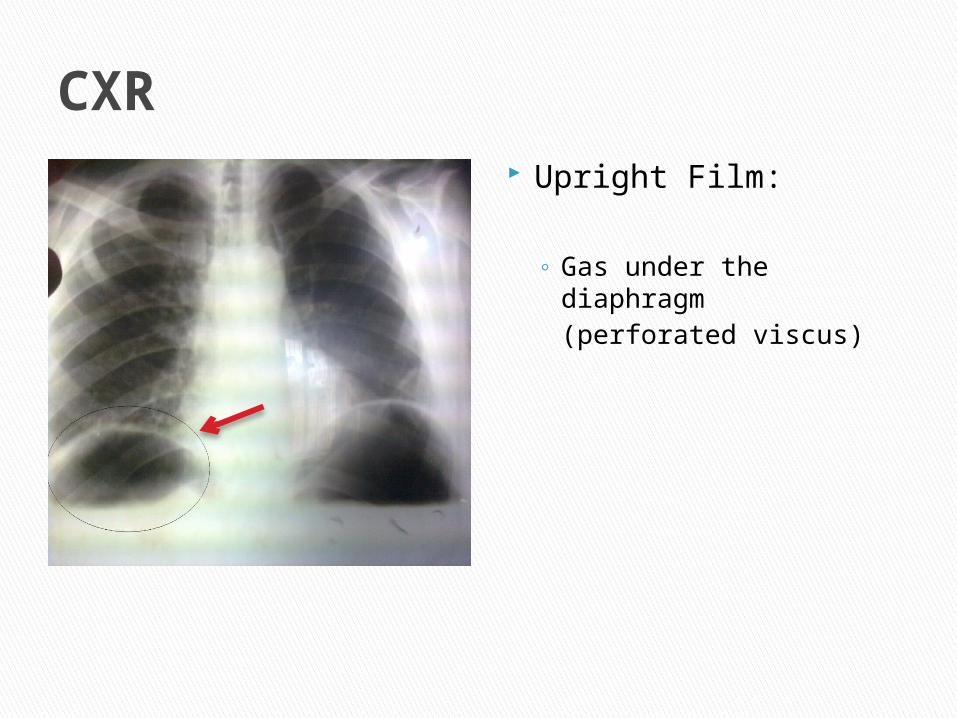
CXR Upright Film:
◦ Gas under the diaphragm(perforated viscus)

Other Causes
IBDGall stone IleusIntussusception
Claw hand sign

Other causes
Paralytic Ileus
Massive Gastric Dilatation
Carcinoma (desc left colon)

Useful in patients with Hx of Abd CA & postsurgical pts
Role/Advantages:◦ Level of obstruction◦ Degree of obstruction & ischemia◦ Cause : volvulus, hernia, luminal & mural causes◦ Free fluid & Gas (perforated viscus)◦ Can detect closed loop obstruction & early
strangulation
CT Scan

SBO - Air Fluid level seen Adhesive Small Bowel Obstruction

Sigmoidoscopy (Rigid or flexible)◦ Performed when on Abd X-Ray large amounts of
colonic air extends down to the rectum◦ To rule out rectal or distal sigmoid obstruction
Barium Studies (follow through, Enema)◦ Performed if there is history of recurring obstruction or distal partial colonic obstruction (via sigmoidoscopy)◦ Gastrografin or Barium Sulphate◦ Limited use in acute setting
Adjunctive Tests

U/S, fast MRI ◦ They are performed if the clinical profile &
Physical Ex is consistent with Intestinal Obstruction despite Normal Abdominal Radiographs
◦ Also capable off detecting the cause of the obstruction
◦ Not routinely performed


Keep patient NPO
1. Nasogastric Intubation/Aspiration Reduce bowel distension Improve pulmonary ventilation Reduce risk of subsequent aspiration during
induction of anesthesia and post extubation• Non-vented Ryle’s tube• Vented Salem tube • Bakers Intestinal tube
2. Fluid and electrolyte replacement
General Management

3. Parenteral antibiotics Broad spectrum antibiotics- Ampicillin, Gentamycin,
Metronidazole, Cephalosporins To correct bacterial infection Mandatory for all patients undergoing small or large bowel
resection
4. Analgesia
5. Blood Transfusion FFP or platelet transfusions Often needed in critical patients
6. Indwelling Catheter Hourly Urine output monitoring

7. CVP For Fluid And Monitoring
PCWP (pulmonary capillary wedge pressure) monitoring
Needed in haemodynamically unstable patients
Follow Up
IMPROVEMENTConservative treatment is carried on.
DETERIORATIONSurgery indicated if no improvement occurs with in 24-48 hours
Specific Surgery:Therapy directed at underlying disease

Exploratory Laparotomy (emergent in critically ill patients)
Wide Midline Incision Revision of intestine & detection of level and
cause of obstruction Decompression of proximal obstruction Assess viability of bowel (peristalsis, colour,
vessel pulsations) Removal of obstruction
Operative procedures vary according to cause of obstruction
Surgical Treatment

Specific Management

Post operative adhesion obstruction usually resolves on conservative measures.
In adhesive obstructed cases, laparoscopic adhesiolysis (adhesive band lysis) maybe performed in selected patients or using open procedure
Adhesions

Investigations- Plain X-ray Duodenal obstruction- stomach & proximal
duodenum are distended- “double bubble” Jejunal & ileal obstruction- air fluid levels
present
Congenital atresia/stenosis

Treatment: Correct electrolyte & fluid deficits Duodenal atresia requires
duodenojejuostomy & spliting of the anastomosis with a feeding tube.
Congenital atresia/stenosis

Investigation: Plain x-ray of the small bowel - gas shows
malrotation & level of obstruction + A/F levels.
Barium meal (inv of choice)
Malrotation & neonatal volvulus

Treatment: The volvulus is reduced, the
transduodenal band (Ladd’s band) divided, the duodenum mobilised & the mesentry freed.
Appendicectomy is routinely performed to avoid diagnostic difficulty with appendicitis in the future (ladds operation)
Infarcted bowel necessitates resection.
Malrotation & neonatal volvulus

Investigation white cell count is raised A Merkel’s radioisotope scan will reveal acid
producing gastric mucosa.
Merkel’s diverticulum

Treatment: Excision of the inflammed diverticulum Presence of gastric mucosa requires the
resection of the ileal loop containing the diverticulum to ensure complete excision of all acid producing mucosa.
Merkel’s diverticulum

Plain x-ray Shows small dilated bowel loops Gastrograffin enema (in the absence of
acute obstruction) shows up the meconium
Meconium Ileus

Treatment: Colonic gastrograffin (enema) washouts
may restore patency Proximal ileum is anastomosed end to side
to the colon with a distal ileostomy to clear the obstruction.
Meconium Ileus

Investigations: Gastrograffin enema (‘claw sign’ of ileocolic
intussusception) In adults, a contrast CT scan of the
abdomen or barium enema is confirmatory.
Intussusception

Rx: Reduction of the intussusception by
hydrostatic pressure (in children) – done w/in 24 hrs
Surgical reduction by milking out the ISS; bowel resection if there is gross edema preventing reduction or vascular compromise.
Reduction via laparosopic approach
Intussusception

Investigations: Plain x-ray may be diagnostic ‘kidney bean-shaped’ shadow in the right
upper zone: Sigmoid volvulus ‘kidney bean-shaped’ shadow in the left lower zone: Caecal volvulus.
Volvulus of the bowel

Rx: Sigmoid volvulus may be relieved at right
sigmoidoscopy – if not then laparotomy & sigmoidopexy performed
Emergency laparotomy & resection of the volvulus for strangulated or recurrent cases.
Gangrenous bowel is exteriorised & resected, with the formation of a ‘double barrel’ colostomy (Paul-Mikulicz procedure).
Volvulus of the bowel

Investigations: White cell count: >20×109 /L Serum amylase: slightly raised (>200IU)Mesentric angiography
Rx: Laparotomy: superior mesentric
embolectomy; Resection of areas of non-viable bowel.‘second look’ laparotomy at 24 hours for
further resection of non-viable bowel.
Intestinal ischaemia (Acute)

In cases of strangulated Inguinal/femoral hernias the standard groin incision is given & the weakness repaired using hernioplasty or herniorrhaphy, with bowel resection if required.
Hernia

Thank You