Insomnia in depression: Differences in objective and … Trittico sleep.pdf · Insomnia in...
12
~In Neuro-Psychophannacoiogy &lological Psychiatr't ELSEVIER Progress in Neuro-Psychopharmacology &. Biological Psychially 26 (2002) 249-260 Insomniain depression: Differences in objective and subjective sleepand awakening quality to nonnal controls and acuteeffects of trazodone GerdaMaria Saletu-Zyhlarza, Manal Hassan Abu-Bakrb,PeterAndere~, Georg Grub~, Magdalena Mandla, Roland Strobla, Dietmar Golln~, Wolfgang Prausea, Bernd Saletu&.* .Department of Psyclriatly. University of V'1e1I1Ia,W4hringer GIirte//8-20, JienNJ A-1090, Austria bDeparimenI of Psychiatry, University of Alexandria, A/aandria, Egypt Abstract Utilizing polysomnography (pSG) and psychometry, objectiveand subjective sleepand awakening quality was investigated in II drog- free patients (five females, six males)aged35- 75 years(meanage 54.1% 11.4) suffering from nonorganic insomnia(F 51.0) relatedto a depressive episode (F 32) or recun-ent dep~ssive disorder (F 33), as compared with II age-and sex-matched nonna! controls(five females, six males) aged 36- 75 years (mean age53.0% 13.5). PSGdemonstrated decreased sleep efficiency, total sleep time (TST), total sleep period (TSP) andsleep stage S2,aswell as increased wakefulness during TSP, early moming awakening, sleep latency to SI, S2, S3 and sleep stage SI in depressed patients. Subjective sleep quality and the total scoreof die Self-Assessment of Sleep and AwakeningQuality Scale (SSA) were deteriorated aswere moming and eveningwell being, drive, mood and fine motor activity right. Eveningand moming blood pressure, the ~ desaturation index and periodic leg movement (pLM) index were increased. In a subsequent acute, placebo-controlled cross-<lver designstudy, the acute effectsof 100mg oftrazodone, a serotonin reuptake inhibitor with a sedative action due to 5-HT2 and 0,1 receptor blockade,were investigated in the patients. As compared with placebo,trazodone inducedan increase in sleepefficiency (primary target variable), TST,TSPandSWS(S3+ 84), aswell asa decrease in wakefulness during the TSP, early moming awakening and S2. There wasno rhanv~ in ~nili ~e mnvPmPnt (Rf':~.() ~1ef'n with th~ ~r"","nn nf 1'n ;"t'rPA~P in tl,p QPM r4",",,"nn ;n mm'tt T nr4...n~ "lcn ,...,'c~A An - ,- . . - . - - -- -, - -, -. ,. improvement in subjective sleepquality, affectivity, numerical memory and somaticcomplaints. All respiratory variables remained within nonna! limits. Critical flicker frequency and moming diastolic blood pressurewere decreased. The present study demonstrated that depression inducedsignificant changes in objective and subjective sleepand awakeningquality, which were counteracted by 100 mg of trazodone, thus suggesting a key-lock principle in the treatment of depression. (:)2001 Elsevier Science Inc. All rights reserved. Introduction The complaint of sleep disturbance has always been a defining feature of mood disorders. Epidemiological studies showed that insomnia was twice and up to three times as prevalentin depressed individuals as in nondepressed ones (Liljenberg et aI., 1989; Livingston et al., 1990; Quera-Saiva et aI., 1991). In die World Health Organization (WHO) collaborative study on psychologicalproblems in general healdi care, 5438 persons from different cultures were examinedin primary care settings. Approximately half of thepatients sufferingfrom sleep disorders hada well-defined InternationalClassificationof Diseases (ICD)-10 diagnosis of mental disorders; 31.1% of them met the criteria for current depressive disorder(Ostiin et aI., 1996). This is in AbbreviatiollS: AID, apnea-hypopnea index; AI, apnea index; CFF, critical flicker frequency; DDA. descriptive data analysis; DSM, Diagnostic aDd Statistical Manual of Mental Disorders; BEG, electroencephalogram; EMG, electromyogram; EOG, electrooculogram; lCD, International ClassificatXln of Diseases; ICSD, International Classification of Sleep Disorders; LORETA, low-resolution brain electromagnetic tomography; PLM, periodic leg movenlent; PSG, polYSOlmOgram; PSQI, PittsbuJgh SleepQua1ity IOOex; Qu, Quality of Life Index; REM, rapid eye movement; SSA. Self-Assessment of Sleep and Awakening Quality Scale; S-HT, serotonin=S-hydroxytryptamine; S, sleep stage; SWS, slow-wave sleep; TIB, time in bed; TSP, total sleep period; TST, total sleep time; WHO, World Health Organization; SAg, Zung Anxiety Score; SDS, Zung Depression Score . Comsponding author. Tel.: +43-1-40-400-3637/83; fax: +43-1-40- 25-909. E-mail address: [email protected] (B. Sa1etu). 0278-584&'02/$ - see ftont ID81ta' C 2001 EJaevier Science mc. All rights reserved. Pll: S0278-S846{0 I )00262- 7
Transcript of Insomnia in depression: Differences in objective and … Trittico sleep.pdf · Insomnia in...

~InNeuro-Psychophannacoiogy
& lological Psychiatr't
ELSEVIER Progress in Neuro-Psychopharmacology &. Biological Psychially 26 (2002) 249-260
Insomnia in depression:Differences in objective and subjective sleep and awakening quality to
nonnal controls and acute effects of trazodone
Gerda Maria Saletu-Zyhlarza, Manal Hassan Abu-Bakrb, Peter Andere~, Georg Grub~,Magdalena Mandla, Roland Strobla, Dietmar Golln~, Wolfgang Prausea, Bernd Saletu&.*
.Department of Psyclriatly. University of V'1e1I1Ia, W4hringer GIirte//8-20, JienNJ A-1090, Austria
bDeparimenI of Psychiatry, University of Alexandria, A/aandria, Egypt
Abstract
Utilizing polysomnography (pSG) and psychometry, objective and subjective sleep and awakening quality was investigated in II drog-free patients (five females, six males) aged 35- 75 years (mean age 54.1 % 11.4) suffering from nonorganic insomnia (F 51.0) related to adepressive episode (F 32) or recun-ent dep~ssive disorder (F 33), as compared with II age- and sex-matched nonna! controls (five females,six males) aged 36- 75 years (mean age 53.0% 13.5). PSG demonstrated decreased sleep efficiency, total sleep time (TST), total sleep period(TSP) and sleep stage S2, as well as increased wakefulness during TSP, early moming awakening, sleep latency to SI, S2, S3 and sleep stageS I in depressed patients. Subjective sleep quality and the total score of die Self-Assessment of Sleep and Awakening Quality Scale (SSA)were deteriorated as were moming and evening well being, drive, mood and fine motor activity right. Evening and moming blood pressure,the ~ desaturation index and periodic leg movement (pLM) index were increased. In a subsequent acute, placebo-controlled cross-<lverdesign study, the acute effects of 100 mg oftrazodone, a serotonin reuptake inhibitor with a sedative action due to 5-HT2 and 0,1 receptorblockade, were investigated in the patients. As compared with placebo, trazodone induced an increase in sleep efficiency (primary targetvariable), TST, TSP and SWS (S3 + 84), as well as a decrease in wakefulness during the TSP, early moming awakening and S2. There was norhanv~ in ~nili ~e mnvPmPnt (Rf':~.() ~1ef'n with th~ ~r"","nn nf 1'n ;"t'rPA~P in tl,p QPM r4",",,"nn ;n mm'tt T nr4...n~ "lcn ,...,'c~A An- ,- . . - . - - -- -, - -, -. ,.improvement in subjective sleep quality, affectivity, numerical memory and somatic complaints. All respiratory variables remained withinnonna! limits. Critical flicker frequency and moming diastolic blood pressure were decreased. The present study demonstrated thatdepression induced significant changes in objective and subjective sleep and awakening quality, which were counteracted by 100 mg oftrazodone, thus suggesting a key-lock principle in the treatment of depression. (:)2001 Elsevier Science Inc. All rights reserved.
Introduction
The complaint of sleep disturbance has always been adefining feature of mood disorders. Epidemiological studiesshowed that insomnia was twice and up to three times asprevalent in depressed individuals as in nondepressed ones(Liljenberg et aI., 1989; Livingston et al., 1990; Quera-Saivaet aI., 1991). In die World Health Organization (WHO)collaborative study on psychological problems in generalhealdi care, 5438 persons from different cultures wereexamined in primary care settings. Approximately half ofthe patients suffering from sleep disorders had a well-definedInternational Classification of Diseases (ICD)-10 diagnosisof mental disorders; 31.1% of them met the criteria forcurrent depressive disorder (Ostiin et aI., 1996). This is in
AbbreviatiollS: AID, apnea-hypopnea index; AI, apnea index; CFF,critical flicker frequency; DDA. descriptive data analysis; DSM, DiagnosticaDd Statistical Manual of Mental Disorders; BEG, electroencephalogram;
EMG, electromyogram; EOG, electrooculogram; lCD, InternationalClassificatXln of Diseases; ICSD, International Classification of SleepDisorders; LORETA, low-resolution brain electromagnetic tomography;
PLM, periodic leg movenlent; PSG, polYSOlmOgram; PSQI, PittsbuJghSleep Qua1ity IOOex; Qu, Quality of Life Index; REM, rapid eyemovement; SSA. Self-Assessment of Sleep and Awakening Quality Scale;S-HT, serotonin=S-hydroxytryptamine; S, sleep stage; SWS, slow-wavesleep; TIB, time in bed; TSP, total sleep period; TST, total sleep time;WHO, World Health Organization; SAg, Zung Anxiety Score; SDS, ZungDepression Score
. Comsponding author. Tel.: +43-1-40-400-3637/83; fax: +43-1-40-
25-909.E-mail address: [email protected] (B. Sa1etu).
0278-584&'02/$ - see ftont ID81ta' C 2001 EJaevier Science mc. All rights reserved.
Pll: S0278-S846{0 I )00262- 7
G.M. SaJetu-Zyhlan et al. / Progress ill Neuro-PsychopltOmlllCOlogy &; Biological Psychiatry 26 (2002) 249-2~250
line with the results of Schramm et at. (1995), who foundthat in general practice, affective disorders were the mostcommon mental illness comorbid with chronic insomnia, aswell as with our findings of 31 % of affective disorders as acomorbid condition in our sleep outpatient clinic (Saletuet al., 1997a). Balan et al. (1998) evaluated psychiatrically100 subjects referred to a sleep laboratory because of sleepcomplaints, mostly insomnia. Forty-three percent receivedaxis-I DSM-ill-R diagnoses (American Psychiatric Asso-ciation, 1987); 8% was suffering from major depression, 5%from dysthymia and 9% from adjustment disorder withdepressed mood. A new semi structured interview for sleepdisorders was used to detennine the prevalence of sleepcomplaints and insomnia in 1253 patients with majordepressive disorders, both single episode and recurrent.Sleep complaints lasting at least 6-7 days/week were asfollows: 33.7% of the patients had difficulties initiatingsleep, 27% maintaining sleep, 37.5% showed a nonrestor-ative sleep, 30.3% early awakening and 11.1 % excessivesleepiness. A strong association was found between theseverity of depression and insomnia (Bobes et al., 1998).
Insomnia might not only be a symptom of depression, butalso occur prior to and even presage the development of afull clinical syndrome (Dryman and Eaton, 1991; Breslauet al., 1996; Roberts et al., 2000). Perlis et at. (1997) assessedthe sleep disturbance complaints in patients suffering fromrecurrent depression. They found that sleep progressivelyworsened prior to acute recurrence, i.e., the sleep disturbancenot only predicts but also varies with the clinical state.
The sleep patterns of depressed patients have been studiedextensively. Depressed patients were found to usually exhibitreduced sleep efficiency, prolonged sleep latency, frequentbnef awakenings, an mcrease in light sleep, reduced slow-wave sleep (SWS), as well as rapid eye movement (REM)sleep abnormalities (Kupfer and Foster, 1972; Kupfer et al.,1978; Feinberg et al., 1982; Reynolds et al., 1983; Rush et al.,1982; Borbely et al., 1984; Dietzel et al., 1986; Thase et al.,1986). Changes in REM sleep, such as decreased REMlatency, a prolonged first REM period, increased REMdensity and an increased amount of REM sleep, have beenin focus of research and were thought to be rather specific todepression-particularly shortened REM latency (Akiskal etal., 1982; Reynolds and Kupfer, 1987; Rush et al., 1989).However, a meta-analysis of sleep and psychiatric disorderscame to the conclusion that none of these REM sleepabnormalities was unique to depression (Benca et al., 1992).
REM sleep parameters were found to become increas-ingly abnormal with repetitive episodes of depression; apronounced shortening of REM latency, an increase in theREM sleep percentage and higher numbers of REM periodsand REM activity were observed at the time of recurrence(Kupfer et al., 1988, 1991). Moreover, depressed outpatientsdiffered from depressed inpatients in having shortened REMlatency at a somewhat lower percentage. Also the shift ofREM activity to earlier in the night was of lower magnitudein the outpatient sample (Reynolds and Kupfer, 1987).
Although antidepressants are similar in their abilities totreat depression, many of them fail to treat preexistinginsomnia, exacerbate insomnia or cause insomnia (Obem-dorfer et aI., 2000). Trazodone was found to be effective intreating insomnia associated with depression (Brooks et aI.,1984; Wheatley, 1984; Fabre, 1990), as well as insomnia dueto activating antidepressants (Jacobsen. 1990; Nierenberget aI., 1994). Trazodone hydrochloride is a triazolopyridinederivative possessing an antidepressant effect and possiblyantianxiety activity. Phannacologically, it blocks 0.1 adre-nergic receptors, presynaptic 0.2 receptors and 5-HT 2a/2creceptors. Its active metabolite, meta-chlorophenylpipera-zine, is a direct 5-HT receptor agonist (Frazer, 1997). I~sedating effect seems to be related to 5-HT2a and 0.1 receptorblockade (Delini-Stula, 1993; Ware et al., 1994). Someresearchers found that a single nighttime dose of trazodonehad the same hypnotic effect as a divided daily dosageregimen (Brooks et al., 1984), while others found thatnighttime dosage was better than divided dosage as regardssleep latency, number of awakenings, sleep quality, dream-ing and feeling on wakening (Wheatley, 1984; Mashikoet aI., 1999).
Neurophysiologically, the sedative effect of trazodonewas already reported by us in 1982, utilizing pharmaco-
electroencephalogram (BEG) analyses (Saletu, 1982, 1987).This was confinned by Yamadera et al. (1998, 1999), who,in polysomnography (pSG) studies in nonnals, showed anincrease in SWS and a decrease in SI and S2.
Findings on the effect of trazodone on PSG variables inpatients are ambiguous. Mouret et al. (1988) found anincrease in total sleep time (TST), S2, S3 + S4 and REMlatency, as well as a decrease in sleep latency and intrasleepawakening, while Van Remmel et al. (1992) noted onlysuppressed REM sleep and increased REM latency, whichwas also described in elderly nondepressed insomniacpatients (Montgomery et aI., 1983), as well as in normalhealthy volunteers (Ware et aI., 1994).
Thus, the aim of the present study was threefold: (1) toinvestigate objective and subjective sleep and awakeningquality of 11 patients with nonorganic insomnia related tomajor depressive disorder; (2) to detennine whether-like inother sleep disorders-also in insomnia related to depres-sion, one adaptation night would be necessary, which maybe of importance for insurance reimbursements; and (3) tomeasure the acute effect of trazodone, 100 mg, as comparedto placebo on objective and subjective sleep and awakeningquality of depressed patients.
2. Methods
2.1. Patients, inclusion and exclusion criteria
Eleven drug-free patients (five females, six males) aged35 - 75 years (mean age 54.1 of: 11.4 years) with the dia-gnosis of nonorganic insomnia (F 51.0) related to a
GM. Sa/etll-Zyhlan et al. / Progms i" Neuro-Psychopilamlacology &; Biological Psychiatry 26 (2002) 249-260 2$1
depressive episode (F 32) or recurrent depressive disorder(F 33) were included in this study. Infonned consent wasobtained. Eleven matched nonnal subjects (five females,six males) aged 36-75 years (mean age 53.0:i:13.5 years)were studied as a control group (Z 00.6).
2.1.1. Inclusion criteriaThey called for patients of either sex, aged 18 - 7 5 years,
satisfying the ICD-IO diagnostic criteria (World HealthOrganisation, 1992) of nonorganic insomnia related to adepressive episode or recurrent depressive disorder. Clin-ically, these patients had difficulties falling asleep, maintain-ing sl~ep or a poor quality of sleep. The complaint of sleepdisturbance occurred at least three times a week for at least1 month. There was preoccupation with the sleeplessness andexcessive concern over its consequences at night and duringthe day. The unsatisfactory quality of sleep either causedmarked distress or interfered with social and occupationalfunctioning. According to a polydiagnostic approach, thepatients were also required to meet the criteria of the DSM-IV (American Psychiatric Association, 1994) diagnosis ofnonorganic insomnia related to major depressive disorderand the International Classification of Sleep Disorders(ICSD) (American Sleep Disorders Association, 1997) dia-gnosis of sleep disorder associated with mood disorder.
In patients, the Pittsburgh Sleep Quality Index (PSQI)(Buysse et al., 1989) on admission was 13.2 %.4.1 (normals:2.7%. 1.7), the Quality of Life Index (QLI) (Mezzich andCohen, 1996; Mezzich et al., 2000) 6.0%. 1.4 (normals:8.5 %. 0.6), the Zung Depression Score (SDS) (Zung, 1965)52.1 %.10.0 (normals: 25.4%.2.6), the Zuni Anxiety Score(SAS) (Zung, 1976) 47.7%.9.0 (normals: 25.4%.2.6).
bearing period who were not applying adequate contracep-tive methods, patients with insomnia secondary to otherconditions, e.g., nocturia, pain, etc.; patients with a historyof drug abuse or habituation including alcohol; patients witha history of trazodone hypersensitivity; patients with anysignificant medical disorder; patients requiring psychoactivemedication or any other drug, which might interfere with thestudy assessments; patients who worked at night andpatients with narrow angle glaucoma.
The study was perfonned in accordance with the rulesand regulations for the conduct of clinical trials, stated inthe declaration of Helsinki, as revised by the WorldMedical Assembly in Somerset West (World MedicalAssembly, 1996).
2.2. Study design
In the single-blind, placebo-controlled cross-over study,the patients were investigated for three nights:
I. Adaptation night (A)2. Baseline/placebo night (P)3. Trazodone, 100 mg, at night <T:
The decision to choose a dosage of 100 mg was based ona meta-analysis on sleep studies in both nonna! volunteersand patients (Oberndorfer et aI., 2000).
At the time of admission, the patients were required tohave been free of psychophannacoiogical treatment for fivetimes the half-life of the psychopharmacological agentgiven last. The concomitant use of sedatives, propranolol,a-methyldopa, other antidepressants, tranquilizers, antihist-ammes, amphetamme-containing compounds, narcoticanalgesics, anticholinergics or alcohol was prohibited dur-ing the study. Aspirin or acetammophen could be taken, butthe patients were instructed to reftain from doing so after
2.1.2. Exclusion criteriaThe following groups of people were excluded from the
study: pregnant or lactating women; women in the child-
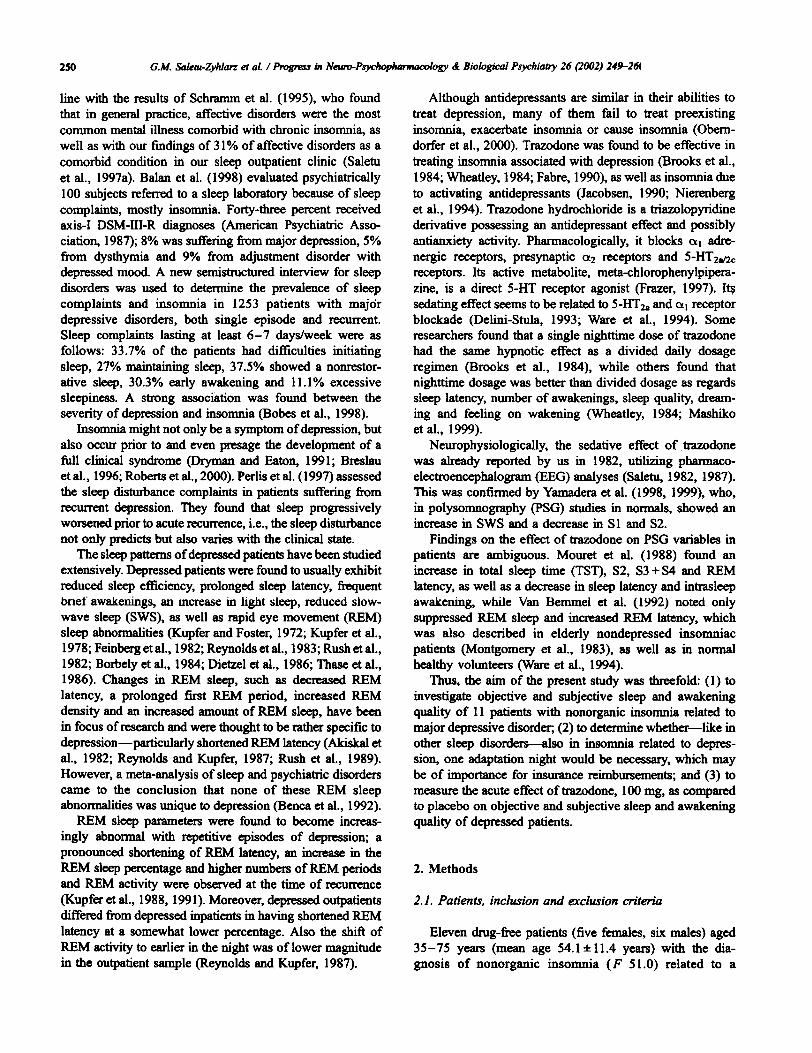
Table IInsomnia (F 51.0) in deIH'e88iOD (F 32, F 33): differences to nomJal controls (q and 8CUte eff«:t8 of 100 mg of trazodone (l) aIM! plKebo (P) after an
adaptation night (A)
212777B49S3304
428375B4
A:p..A:p. P:~P:~A:p. P:~P:~P:~
P:C'.P:C.P:C..P:C..P:C..
Latency to SI (min)!Latency to S2 (min)!Latency to S3 (min)!Latency to S4 (min)!Latency to REM (min)!Wake within TSP (min)!Wake before buzzer (min)!
Awakenings (N)!TSP (min)fTST (min)f
Sleep effi~ (%)1
['t!) DirectKJn of improvement.. P< .OS... P<.Ol.
252 GM SaIetu-Zyhlarz et al. / Progress in Neuro-PsychopilanllaCOlogy &; Biological Psychiatry 26 (2002) 249-260
1700 h during the study. In addition, meals, coffee, tea,Coca-Cola or other caffeine-containing beverages were tobe avoided within 8 h of retiring. No other medication wasallowed after the study treatment had been taken at bed-time. The patients were required not to nap during the dayor evening for the duration of the study.
proportion of sleep in the recorded period and is calculatedby dividing TST by the total TIB (fixed in our study)multiplied by 100.
2.4. Subjective sleep and awakening quality
After the morning toilet. the patients completed theSelf-Assessment of Sleep and Awakening Quality Scale(SSA) (Saletu et al., 1987). Thymopsychic variablesincluded subjective well-being in the evening and morning,based on the Yon Zerssen Bf-S Scale (Yon Zerssen et al.,1970), as well as drive, mood, affectivity and drowsinessin the morning, measured by means of 100-mm visual-analog scales. '
2.3. Evaluation of objective sleep quality
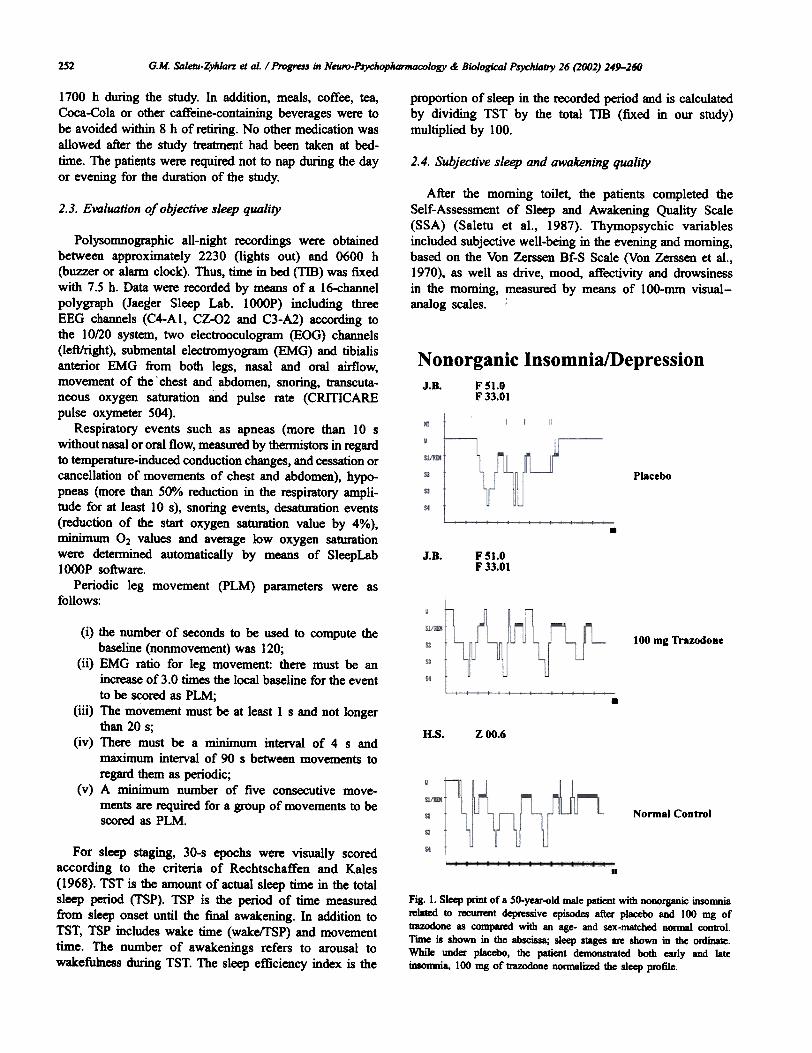
N onorganic Insomnia/Depression
Placebo
.J.B. FS1.0
F 33.01
Polysomnographic all-night recordings were obtainedbetween approximately 2230 (lights out) and 0600 h(buzzer or al8rD1 clock). Thus, time in bed (TIB) was fixedwith 7.5 h. Data were recorded by means of a 16-channelpolygraph (Jaeger Sleep Lab. 1000P) including threeEEG channels (C4-A1, CZ-Q2 and C3-A2) according tothe 10/20 system, two electrooculogram (BOG) channels(left/rigbt), submental electromyogram (BMG) and tibialisanterior EMG from both legs, nasal and oral airflow,movement of the chest and abdomen, snoring, transcuta-neous oxygen saturation and pulse rate (CRIllCARE
pulse oxymeter 504).Respiratory events such as apneas (more than 10 s
without nasal or oral flow, measured by thermistors in regardto temperature-induced conduction changes, and cessation orcancellation of movements of chest and abdomen), hypo-pneas (more than 50% reduction in the respiratory ampli-tude for at least 10 s), snoring events, desaturation events(reduction of the start oxygen saturation value by 4%),minimum O2 values and average low oxygen saturationwere detetmined automatically by means of SleepLab1000P software.
Periodic leg movement (PLM) parameters were asfollows:
100 mg TrazodoDe
.B.s. ZOO.6
(i) the number of seconds to be used to compute thebaseline (nonmovement) was 120;
(ii) EMG ratio for leg movement: there must be anincrease of 3.0 times the local baseline for the eventto be scored as PLM;
(ill) The movement must be at least 1 s and not longerthan 20 s;
(iv) There must be a minimum interval of 4 s andmaximum interval of 90 s between movements toregard them as periodic;
(v) A minimum number of five consecutive move-ments are required for a group of movements to bescored as PLM. Normal Control
For sleep staging, 30-s epochs were visually scoredaccording to the criteria of Rechtschaffen and Kales(1968). TST is the amount of actual sleep time in the totalsleep period (fSP). TSP is the period of time measuredfrom sleep onset until the final awakening. In addition toTST, TSP includes wake time (waketrSP) and movementtime. The number of awakenings refers to arousal towakefulness during TST. The sleep efficiency index is the
II
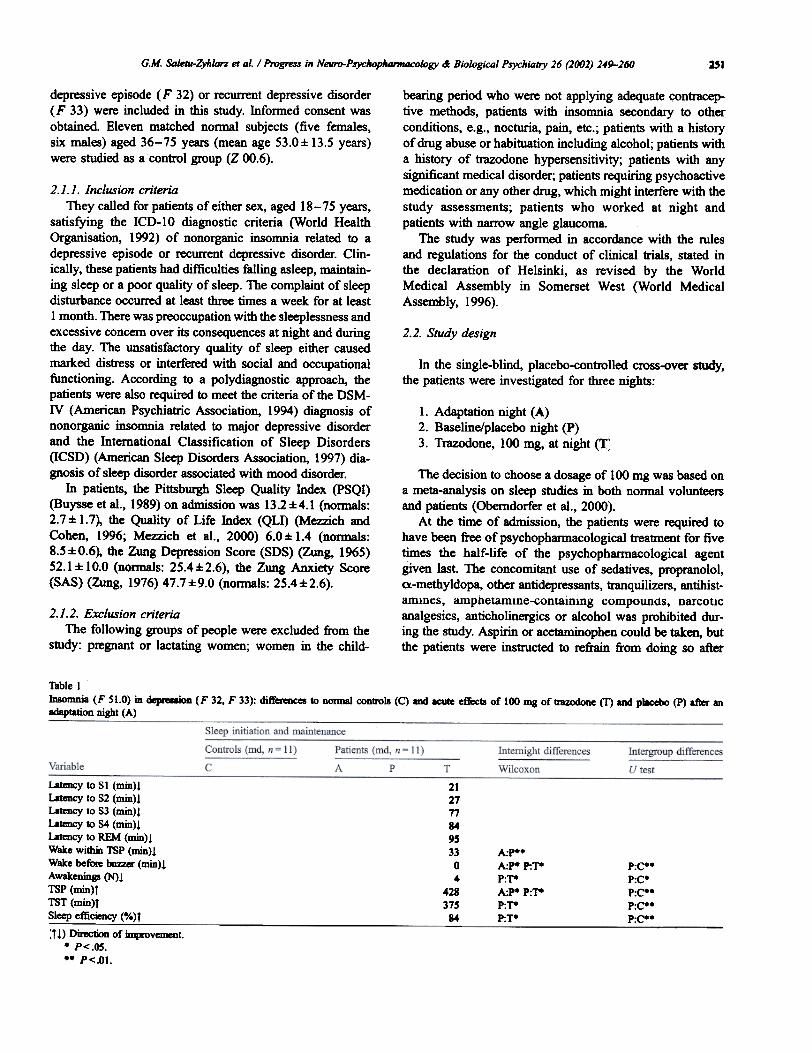
Fia. 1. Sleep print of a 50-year-old male patient with nooorganic insomniarelated to recunent depressive episodes after placebo and 100 mg oftIazoOOne as compared with an age- and sex-matched nomIal control.Time is shown in the abscissa; sleep stages are shown in the ordinate.While under placebo, the patient demonstrated both early and lateinsomnia, 100 mg of trazodone normalized the sleep profile.
J.B. F 51.0F 33.01
G.M. SaJetu-Zyh/arz et al. / Progress in Neuro-Psychopharmacolagy &; Biological Psychiatry 26 (2002) 249'-260
Statistical analysis was based on the concept of descript-ive data analysis (DDA) as proposed by Abt (1988) forcontrolled clinical trials. The predetennined null hypothesisfor the confinnatory statement was: There is no differencebetween trazodone and placebo in regard to sleep efficiency(maximum error probability a = .05). Normal distributionwas tested by means of the one-sample Kolmogorov-Smir-nov Test In case of a violation of the assumption of nonnaldistribution, a Wilcoxon test was used for within-groupcomparisons and a Mann - Whitney U test for intergroupcomparison. All other effects were tested descriptively.
2.5. Objective awakening quality (psychometry)
Noopsychic tests included the Griinberger AlphabeticalCancellation Test for quantification of attention (total score),concentration (errors in percentage of the total score) andattention variability (difference between extreme scores)(Griinberger, 1977), the Numerical Memory Test (Griin-berger, 1977), as well as the Griinberger Fine MotorActivity Test (right and left hands) for evaluation of changesin psychomotor activity and drive (Griinberger, 1977).Reaction time, reaction time variability (ms) and errors ofomission and commission were determined by the com-puter-assisted reaction time apparatus.
3. Results2.6. Psychophysiological investigations
3.1. Objective sleep qualityThese included the critical flicker frequency (CFF;
descending threshold) after awakening, muscular strengthof the right and left hands, as well as of the right and leftindex fingers and thumbs evaluated by means of a vigori-meter (kp/cm1 (FUnfgeld, 1966). The evening and morningpulse rate, as well as systolic and diastolic blood pressurewere also recorded.
2.7. Biometric planning and evaluation
The sample size was based on the meta-analysis study onsleep in psychiatric disorders by Benca et al. (1992).
The primary target variable was sleep efficiency (%). Animprovement by 1 S.D. (4%) from our nonnative databasefor subjects aged between 40 and 60 years (Saletu et al.,1991) was considered as clinically relevant
3.1.1. Sleep initiation and maintenanceMajor depression patients showed a first-night effect in
regard to wakefulness within TSP, which was significantlylonger in the first night than in the second night, while waketin1e before the buzzer was shorter and TSP was signific-antly longer (Table 1).
As compared with nonnal controls, insomniac depressivepatients showed a significantly lower sleep efficiency (77%vs. 92%, P< .01), further, a significantly longer sleeplatency to Sl, S2 and S3, a higher number of awakeningsand shorter TST and TSP, as well as more early morningawakening (Table l).
Acute treatment with trazodone, lOO mg, resulted in asignificant increase in sleep efficiency from 77% to 84%(P< .OS), a significant improvement in TST, TSP, the
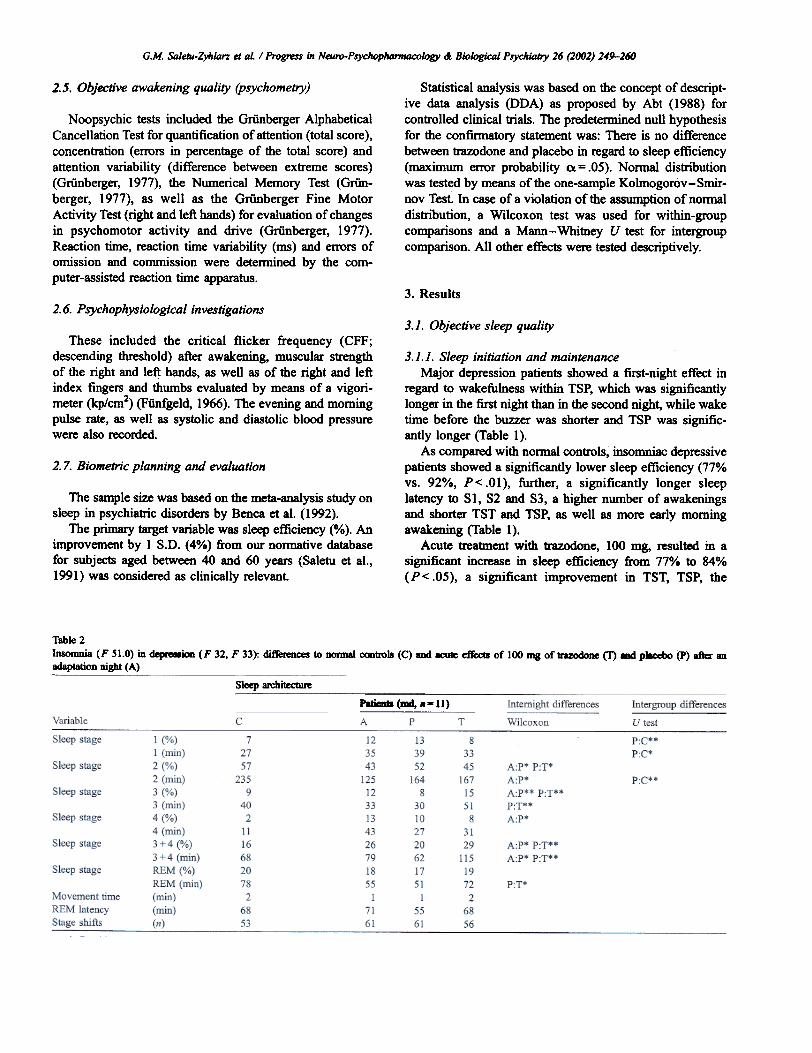
Table 2Insomnia (F 51.0) in d.-ioD (F 32, F 33): differences to norma1 controls (q aDd acute effects of 100 InS of trazodone (T) -' pllcebo (P) after anadaptation night (A)---
Sleep architecture
P8tieaI8 (aMI, . - II)
254 G.M. Sa/etll-Zyhlarz et aI. / Progress in Neuro-PsychopAamracology &; Biological Psychiatry 26 (2002) 249-260
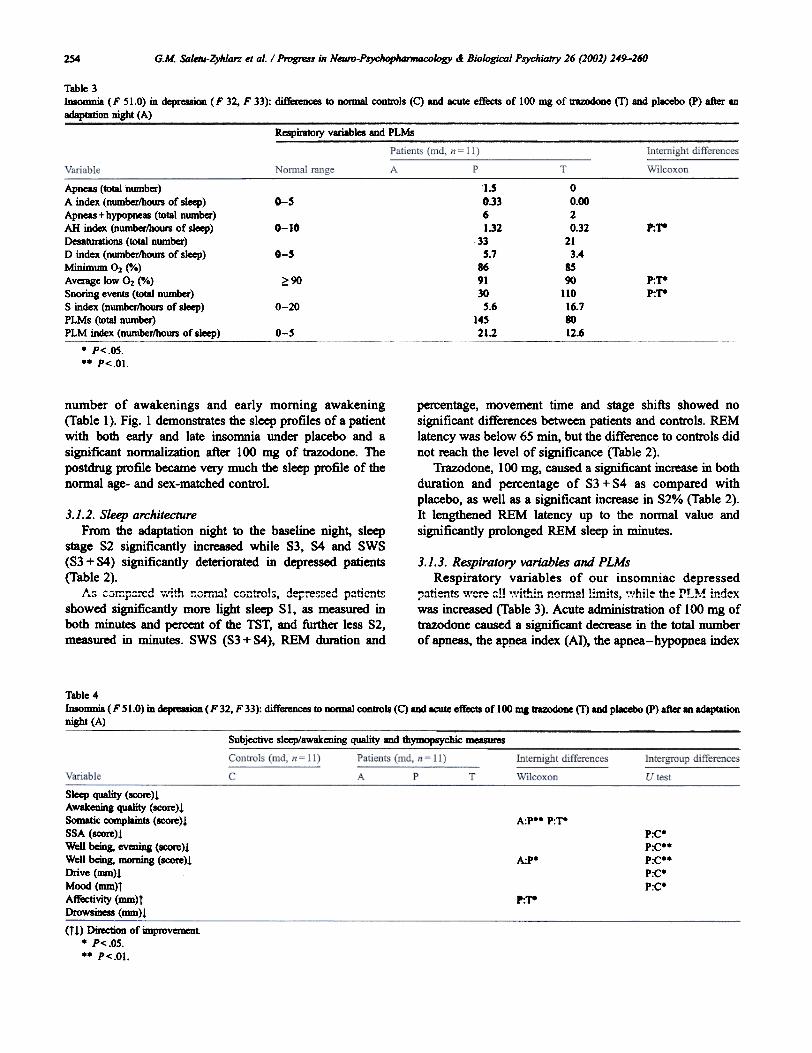
Table 3lDSOmnia (F 51.0) in depression (F 32, F 33): differences to normal controls (C) and acute effects of 100 mg oftrazodone (T) and placebo (P) after anadaptation night (A)
Respiratory variables and PLMs
1.50.3361.32
335.7
869130S.6
14S21.2
00.0020.32
213.4
8590
11016.78012.6
G-S
0-10 r-.T-
0-5
?;90 P:1"-P:1"-
0-20
0-5
Apneas (total nwnber)A index (number/hours of sleep)
Apneas+hypopneas (total number)AH index (number/hours of sleep)Desatlmtions (total nwnber)D index (nwnber/hoUrs of sleep)Minimum O2 (0;.)Average low O2 (0;.)Snoring events (total nwnber)S index (nwnber/hours of sleep)PLMs (total number)PLM index (numberlhqurs of sleep)
. P<.os... P<.Ol
number of awakenings and early morning awakening(Table I). Fig. 1 demonstrates the sleep profiles of a patientwith both early and late insomnia under placebo and asignificant normalization after 100 mg of trazodone. Thepostdmg profile became very much the sleep profile of thenormal age- and sex-matched control.
percentage, movement time and stage shifts showed nosignificant differences between patients and controls. REMlatency was below 65 min, but the difference to controls didnot reach the level of significance (Table 2).
Trazodone, 100 mg, caused a significant increase in bothduration and percentage of 83 + 84 as compared withplacebo, as well as a significant increase in 82% (Table 2).It lengthened REM latency up to the normal value andsignificantly prolonged REM sleep in minutes.
3,1.3, Respiratory variables and PLMsRespiratory variables of our insomniac depressed
.."+: t.. ""-- ftl } "' l't"", .,nnnQI 1, ,ts "' hl' Ie th~ PT ~K ," d"xi-'..Ll~...~ ., ...,~.., .. ...~. ,.~ .,.. ,."li , .. ~ -, , '-
was increased (Table 3). Acute administration of 100 mg oftrazodone caused a significant decrease in the total numberof apneas, the apnea index (AI), the apnea-hypopnea index
3.1.2. Sleep architectureFrom the adaptation night to the baseline night. sleep
stage 82 significantly increased while 83, 84 and 8W8(83 + 84) significantly deteriorated in depressed patients(Table 2).
".. ~~ ~ ,", ..';+L -~ rm '" C~-"' OI~ d-"""~ e'"' P.,ticn." i"", """.t'~"'" .. ,..1 ..v, vuu ,~, ~r ,"J"'" """..:.
showed significantly more light sleep 8 I, as measured inboth minutes and percent of the T8T, and further less 82,measured in minutes. 8W8 (83 + 84), REM duration and
Table 4Insomnia (F 51.0) in depreasiOD (F 32, F 33): ~ to normal oontrols (C) and acute ctJect8 of 100 mg ~ (T) and placebo (P) after an adaptationnight (A)
Subjective sleep/awakening qua1ity and dlymopsychic ~
A:P.. P:~P:C'P:C..P:C..P:C.P:C.
Sleep quality (score)!Awakening quality (score)!Somatic complaints (~)!SSA (scaR)!Well being, evening (score)!Well being, morning (score)!Drive (mm)!Mood (mm)T
Affectivity (mm)TDrowsiness (mm)!
A:P.
P:T-
(t!) DiIection of 'unpro~t. P<.os... P<.Ol.
GM Saletu-ZyiI/an et aI. I Progrus ill Neuro-Psychop1lanPlDcoiogy .I Biological Psychiatry 26 (2002) 249-260 25S
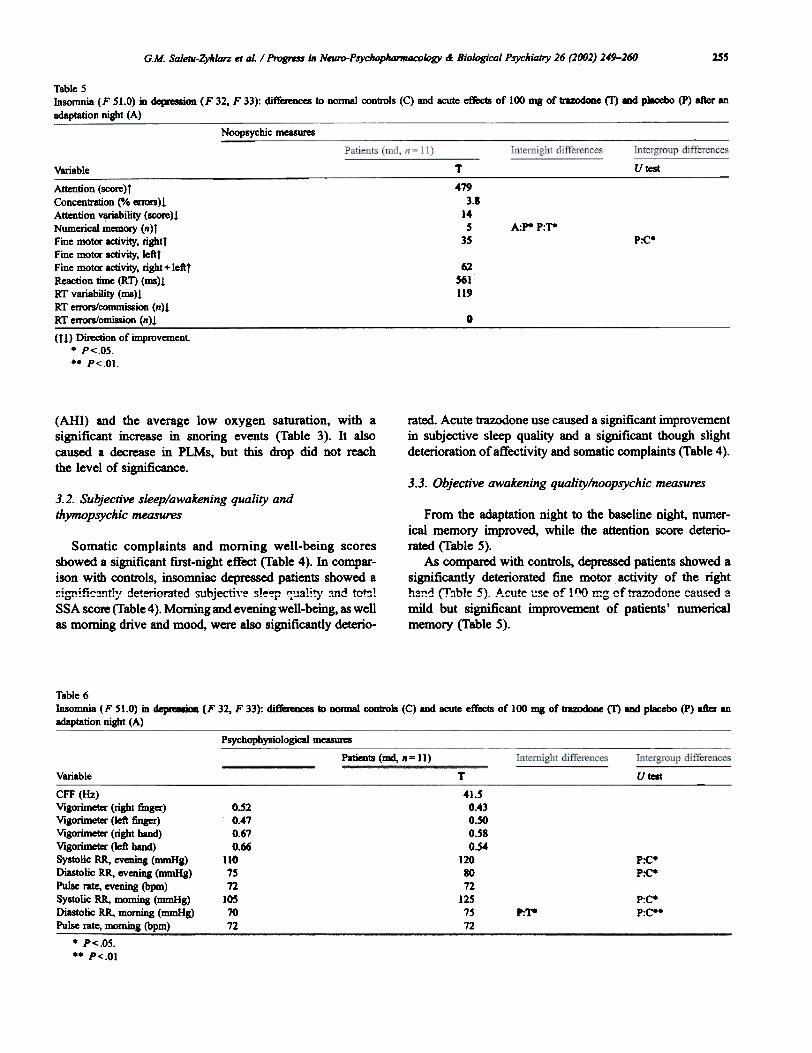
Table 5Insomnia (F 51.0) in depIaaion (F 32, F 33): differences to nonnal controls (C) and acute effects of 100 DIg of tn%OdOIIe (f) and p1ll:ebo (P) after an
adaptation night (A)
Noopsychic measures
T UtestVariable
4793.1
14S
3SA:p. P:T-
P:C'
Attention (score)r
Concentration (0/0 errors)!Attention variability (score)!Numerical mmlory (n)rFine motor activity, rightrFine motor activity, leftrFine motor activity, right + leftr
Reaction time (RT) (ms)!RT variability (ms)!RT errors/commission (n)1RT enors/omission (n)!
6256111'
0
(t!> Direction of improvement.. P<.OS... P<.Ol.
(AHI) and the average low oxygen saturation, with asignificant increase in snoring events (Table 3). It alsocaused a decrease in PLMs, but this drop did not reachthe level of significance.
rated. Acute trazodone use caused a si~cant improvementin subjective sleep quality and a significant though slightdeterioration ofatfectivity and somatic complaints (Table 4).
3.3. Objective awakening quality/noopsychic measures3.2. Subjective sleep/awakening quality andthymopsychic measures
Somatic complaints and morning well-being scoresshowed a significant first-night effect (Table 4). In compar-ison with controls, insomniac depressed patients showed a";""; fi ,",-.n t'" d-+ ; orated sub,ie"+; ,'" SIP""r'! ""' a';'" "nA to""~.O'-_L -~., '" ~,~.. J ...,. ~ ---1' .'. ".J .." ",.
SSA score (Table 4). Morning and evening well-being, as wellas morning drive and mood, were also significantly deterio-
From the adaptation night to the baseline night, numer-ical memory improved, while the attention score deterio.-rated (Table 5).
As compared with controls, depressed patients showed asignificantly deteriorated fine motor activity of the rightha!!d (T~ble 5). ,A.cute l:se of 1 ~ m~ of trazodone caused amild but significant improvement of patients' numericalmemory (Table 5).
Table 6Insomnia (F SI.O) in ~ (F 32, F 33): ~ to DOImal controls (C) and acute effects of 100 mg of trazodone (T) and placebo (P) after anadaptation night (A)
Psychophysiological measures
Patients (md, 11= 11)
Variable T Utest
41.50.430.500.580.54
1208012
1251572
o.o.o.O.
1107'72
1M7072
CFF (Hz)
Vigorimeter (right finger)Vigorimeter (left finger)Vigorimecer (right hand)Vigorimeter (left band)Systolic RR, eveDing (mmHg)Diastolic RR, evening (mmHg)Pulse me, evening (bpm)
Systolic RR, morning (mmHg)Diastolic RR, morning (mmHg)Pulse rate, morning (bpm)
P:C.P~
P:C-P:C..P:T-
. P<.os... P<.OI
'2476766

256 G.M. SaIem-ZyiI/Qrz et aL / Progress ill Neuro-PsyciIophamlocology &: Biological Psychiatry 26 (1002) 249-260
3.4. Psychophysiological measures
There was no significant first-night effect in psychophy-siological measures (Table 6). Evening and morning bloodpressure were significantly higher in depressed patients thanin normals (Table 6). Trazodone significantly reduced theCFF as compared with placebo and also significantlydecreased morning diastolic blood pressure (Table 6).
4. Discussion
4.1. Sleep initiation and maintenance
The polysomnographic investigations in depressedinsomniac patients demonstrated a disturbed sleep initiationand maintenance characterized by prolonged sleep latency,as well as by a decreased sleep efficiency, TSP and TST,and an increased number of nocturnal awakenings. Thisconfirmed previous PSG findings of sleep disturbances indepressed patients (Gillin et al., 1979; Reynolds andKupfer, 1987; Rush et al., 1989). There was also adeterioration of subjective sleep qUality in our depressedpatients as compared with controls, which is in line withthe fact that sleep disturbance is one of the main complaintsof depressed patients (Ford and Kamerow, 1989). Acuteadministration of 100 mg of trazodone at night resulted in asubjective and objective improvement of sleep quality, asindicated by the patients' rating of sleep quality and PSGsleep maintenance variables. However, trazodone showedno effect on sleep latency. Nierenberg et al. (1994) foundthat trazodone 50 mg at night improved patients' sleepduratiun and theil tuti1l PSQI s~ur~~ and ~au~ed i1nimprovement in early morning awakening in patients withantidepressant-associated insomnia. The authors alsodescribed a trend towards an improvement in subjectivesleep latency, but no significant difference in difficultyfalling asleep between patients treated with trazodone andplacebo. Mouret et al. (1988) also noted an increase in thetotal d\n'ation of sleep and a decrease in nocturnal awak-enings, but also a shortened sleep latency in the first nightof administration of 100 mg of trazodone to depressedpatients. On the other hand, Muratorio et al. (1974)reported that a single 50-mg dose of trazodone had nodetectable effect on sleep, while repeated administration of300-600 mg increased TST and decreased the number andduration of awakenings. However, Van Bemmel et al.(1992) found that trazodone, 300-400 mg, in divided dosesafter 5 weeks had no significant effect on any indicator ofsleep continuity.
difference between depressed patients and normal controlsregarding SWS (S3 + S4). Depressed patients usually exhibitan increase in light sleep and a decrease in deep sleep(Coble et aI., 1976; Hawkins and Mendels, 1966; Ansseauet aI., 1984). REM latency tended to be shorter in depressedinsomniacs than in nonnaI controls. Shortened REM latencywas considered the "psychobiologic marker" for primarydepression (Kupfer, 1976). Borbely et aI. (1984) hypothe-sized that a reduction of the generation of SWS in depres-sion (which especially occurred in the first third of the night)was the reason for the advance of REM sleep. In our study,acute oral administration of trazodone, 100 mg, caused asignificant increase in SWS, which confirmed previousfindings of Yamadera et aI. (1998, 1999) in normals andof Mouret et aI. (1988) in depressed patients, as well as anormalization of REM latency and had an ambiguous effecton S I and S2. Trazodone was found to increase SWS andproduce a negative rebound on withdrawaI in elderly poorsleepers (Montgomery et aI., 1983), as well as in healthyyoung adults (Ware and Pittard, 1990). The prolongation ofSWS seems to be related to the effect of trazodone on s-IlT 2A/2c receptors, which playa criticaIrole in the regulationof SWS (Sharpley and Cowen, 1995).
Like ours, all available PSG studies on the effect oftrazodone in depressed patients found that it increased REMlatency (Montgomery et aI., 1983; Mouret et al., 1988; VanBemmel et aI., 1992; Ware et al., 1994). While we observeda prolongation of REM sleep time but no change in REM%,some studies noted no effect for trazodone on REM sleep(Mouret et aI., 1988; Scharf and Sachais, 1990) and othersfound that 1I'azodone did suppress REM sleep (Montgomeryet aI., 1983; Van Bemmel et aI., 1992; Ware et aI., 1994).
4.3. Respiration and PLMs
Regarding respiratory variables, our patients were withinnormal limits with the exception of a marginal increase inthe desaturation index. Trazodone did not deteriorate thesevariables. On the contrary, it decreased the number ofapneas, the AI and the Am. The PLM index was increasedat baseline and improved under trazodone, 100 mg. Weconsider these findings of interest, as drug treatment mayimprove certain aspects of sleep disorders while othersdeteriorate, and different substances of the same psycho-phannacological class may have different effects on sleep. Itis well known that certain drugs may improve nonorganicinsomnia, while at the same time deteriorate snoring andsleep-related breathing disorders or a restless legs syndrome(Mendelson et aI., 1981; Cirignotta et aI., 1988; Ferry, 1993;Robinson and Zwillich, 2000; Ware et aI., 1984; Paik et aI.,1989; Bakshi, 1996).
4.2. Sleep architecture
4.4. Subjective sleep and awakening qualityIn regard to sleep architecture, our depressed patients
showed increased 81 and decreased 82 sleep as compared tonormal controls, while there was no significant intergroup
While in our depressed patients subjective sleep qualitywas deteriorated, as discussed before, concerning awaken-
G.M. Saletll-Zyhlarz et aI. / Progress in Neuro-PSychopilQrlllacology &; Biological Psychiatly 26 (2002) 249-260
1981; Perry et al., 1989). Due to its 0.1 adrenergic block-age, trazodone is also liable to produce postural hypoten-sion (Silvestrini, 1988), which is also the reason why aretard fonnulation avoiding steep blood level peaks wasdeveloped. Indeed. in a recent field study with such aretard fonnulation, we found only slight side effects(Saletu et al., in preparation).
5. Conclusion
ing quality, they showed no difference when comparedwith normal controls. At the same time, the patients' totalSSA score was worse than that of the controls. Trazodonecaused a mild but nonsignificant improvement in the totalSSA score and had no effect on awakening quality.Moreover, it did not affect well-being in the evening orin the morning. Moon and Davey (1988) found thattrazodone, 150 mg hs, improved sleep quality but wors-ened the ease of awakening in the morning and thefeelings on and after awakening during the first 15 days.After day 16, the latter two variables also began toimprove. Blacker et al. (1988) also observed the initialworsening regarding the ease of awakening and feelingsafter awakening. However, they, also noted an improve-ment after day 7. Trazodone, 100 mg, was found tominimally increase the somatic complaints of our patients,which may be due to 0,1 adrenalytic effects. Anyhow,continuous use of trazodone for 3 weeks was found todecrease somatic fmdings among depressed patients (Klieserand ub_m~J1n, 1988).
Utilizing l00-rom visual-analog scales, we found driveand mood scales deteriorated in patients, while affectivityand drowsiness were not different from controls. Acute useof 100 mg of trazodone caused a mild but significantdeterioration of affectivity.
From our results, we may conclude that patients withnonorganic insomnia due to depressive episodes or recUITentdepressive disorder exhibit a significant deterioration inobjective and subjective sleep and awakening quality ascompared widt normal controls. Moreover, they also show afirst-night effect, just like patients suffering from other sleepdisorders such as nonorganic insomnia due to generalizedanxiety disorder (Saletu et al., 1996), panic disorder (Saletu-Zyhlarz et al., 2000a), dysdtymia (Saletu-Zyhlarz et al.,2001) or organic sleep disorders such as restless legssyndrome (Saletu et al., 2000b,c), periodic limb movementdisorder (Saletu et al., 2001), snoring and sleep-relatedbreathing disorders (Saletu et al., 1998).
In regard to the psychophannacological aspects of dlestudy, we can conclude that trazodone possesses a goodhypnotic effect in patients with nonorganic insomniarelated to depressive episodes and recUITent depression,as it improved subjective and objective sleep quality andoilier sleep measures already after a single dose. This isalso in line widl our recent findings on the acute effects oftrazodone in nonorganic insomnia related to dysdlymia'Salc"UZ ..1-1" -, a' 20"" 'T'-.,7-do-- n""" 1--Cll ,"-oveu\ .. ,y"""L 1;;. !., vij- i!ULoV ill;; ut; r'
to be as effective as oilier antidepressants and superior tothem in improving sleep disturbances (Mann et al., 1981;Davis and Vogel, 1981; Weisler et al., 1994; Cunninghamet al., 1994; KallepaIli et al., 1997). Since the mood-elevating effect of nearly all available antidepressantsusually does not become apparent before 10-14 days, arapid improvement in sleep patterns at the onset oftreatment can be psychologically beneficial, particularlyin regard to the patient's future compliance. Most import-ant seems to us the fact that the changes in sleep variablesinduced by trazodone were opposite to the differencesbetween untreated depressed patients and age- and sex.matched normal controls. This supports a key-lock prin-ciple in dle diagnosis and treatment of nonorganic sleepdisorders, as recently described by us for nonorganicinsomnia due to generalized anxiety disorder (Saletu etal., 1 997b; Saletu-Zyhlarz; et al., 1997), panic disorder(Saletu-Zyhlarz et aL, 2000a) and dysdtymia (Saletu-Zyh-1arz et al., 2001). Moreover, such a key-lock principle wasalso demonstrated utilizing EEG mapping and EEG tomo-graphy by low-resolution brain electromagnetic tomo-graphy (LORETA) (Saletu, 1997, 2000; Saletu et al.,1997b, 2000a; Saletu-Zyhlarz et al., 1997, 2000b).
4.5. Objective awakening quality
Regarding noopsychic measures, our patients did notdiffer from controls except for a deteriorated right-handfine motor activity. Trazodone, 100 mg, did not affectthese noopsychic measures except for a mild improvementof ~ U ~";~~I mcmo "'" ~T- ~-+~-: o ~~ ti.on :,., cogn ; ti'. c ~. n -ti ...'" ~. .. 'J. "... u,", ..., ... . v ."..-tions was observed in normal geriatric subjects whenassessed 4 h after acute atimini~tration of 100 mg oftrazodone (Branconnier and Cole, 1981). Meanwhile,Newton (1981) found that continuous treatment withtrazodone caused some behavior changes, including inde-cision, loss of interest, poor memory, difficulty in concen-tration, forgetfulness and confusion. Our patients showed adecrease in CFF, but no change of muscular strength ontrazodone, 100 mg. The critical flicker fusion thresholdwas described to decrease after the first dose of trazodone,150 mg, with performance improving very graduallythereafter (Moon and Davey, 1988). When comparing theself-rated adverse clinical effects of trazodone and fluox-etine, a high frequency of muscle weakness was foundwith trazodone, which had not been anticipated (Fisheret al., 1993). On assessing morning and evening bloodpressure and pulse rate, we noted that 100 mg of trazodonelowered only the morning diastolic blood pressure. Acuteuse of 100 mg of trazodone had no effect on erect orsupine pulse rate and systolic or diastolic blood pressure ina normal geriatric population (Branconnier and Cole,1981), while continuous use tended to produce a signific-ant decrease in pulse rate and blood pressure (Cole et al.,
G.M. Saletll-Zyh/on et aI. / Progress in Neuro-Psychopilarmacology &; Biological Psychiotry 26 (2002) 249-260258
Acknowledgments
The aud1ors would like to express dieir thanks to Mag.Elisabeth Gtitzhofer for editorial assistance, to Ms. BettinaSchrOckenfuchs from CSC Pharmaceuticals and to die entirestaff of die Section of Sleep Research and Pharmaco-psychiatry for dieir valuable assistance in this project.
References
Abt, K., 1988. Descriptive data aDalysis (DDA) in quantitative EEG stud-ies. In: Samson-Dollfus, D., Guieu, J.D., Gotman, J., Etevenon, P.(Eds.), Statistics and Topography in Quantitative EEG. Elsevier, Am-
sterdam, pp. 150-160.Akiskal, H.S., Lennni, H., Yerevanian, B., King, D., Belluomini. J., 1982.
The usefulness of the REM lateDCy test in psychiatric diagnosis: a studyof 81 depressed oulpatimta. Psychiatr. Res. 7, 101-110.
American Psychiatric Association. 1987. Diagnostic and Statistical Manualof Mental ~ 3rd ed., revised. American Psychiatric Associa-tion, Washington, DC.
American Psychiatric Association, 1994. Diagnostic and Statistical Manualof Mental Disorders, 4th cd. American Psychiatric Association, Wash-ington, DC.
American Sleep Disorden Association, 1997. ICSD-lntem8tiOIIal Classi-fication of Sleep Disorders (Revised): Diagnostic and Coding Manual.American Sleep Disorders AJsoci8tion, Rochester, MN.
Ansseau, M., Kupfer, DJ., Reynolds, C.F., McEacbran, A.B., 1984. REMlatency distribution in major depression: clinical characteristics 8SSOci-ated with sleep-o~ REM periods. Bioi. Psychiatry 19, 1651-1666.
Bakshi, R., 1996. Fluoxetine and resdeas legs syndrome. J. N~l. sa.142,151-152.
Balan, S., Spivak, B., Mester, R., Letbovitz, A., Rabat, B., WeiZ1D81. A.,1998. Psychiatric and POIysomnographic evaluation of sleep distwban-~. J. Affective Disord. 49, 27-30.
Bence. R.M.. Obennever. W.H.. Thisted. R.A.. Gillin. J.C.. 1992. Sleep and
psychiatric disorders. Arch. Gen. Psychiatry 49,651-668.Blacker, R., Sbanb, NJ., Chapman, N., Davey, A., 1988. The drug treat-
ment of depression in general practice: a comparison of nocte admin-istration of trazodone with mianserin, dothiepin and amitriptyline.Psycbopharmacology 95 (SuppL), S18-S24.
Bobes, J., Gonzalez, M.P., Ayuso, J.L, GIbert, 1., Saiz, J., Vallejo, J., Rico,F., 1998. Major depreasjon and iDSOmnia assessed through the OviedoSleep QuestiODllaiJe. Eur. Neuropsychophannaool. 8 (Suppl. 2), 162.
Borbely, A.A., Tobler. L, Loepfe, M., KDupfer, DJ., Ulrich, R.F., Grocho-cinsti, U., Doman, J., Matthews, G., 1984. AII-night spectral analysis ofthe sleep EEG in ~ depressives aJMi nomlll controls. Psychiatr.Res. 12,27-33.
BranconDier, R., Cole, J., 1981. Effect of acute adminisUation oftrlzodoneand amitriptyline on cognitive, cardiovlSCUlar functions md SIlivationin normal geriatric subjects. J. Clin. PsychopharmacoL 1 (6),82s-88s.
Breslau, N., Roth, T., Rosenthal, L., Amesk:i. P., 1996. Sleep disturl>anceand psychiatric disorders: a longitudinal epidemiological study ofyoung adults. BioI. Psychiatry 39 (6), 411-418.
Brooks, D., Prothero, W., Bouru, N., Bridles, P.K., Jannan, C., Ankier, S.,1984. T~ coDIP8rison of single nigilt-Ume and divided d0s-age regimens. Psychopb8DlKology 84, 1-4.
Buysse, DJ., Reynolds m. C.F., Monk, T.H., Berman, S.R., Kupfer, D.J.,1989. The Pittsburgh Sleep Quality Index. A new instnIment for psy-chiatric plactice and research. Psychiatr. Res. 28, 193-213.
Cirignotta. F., Mondini. S., Zuceoni. M., Gerardi, R., Farolfi. A., L~E., 1988. Zolpidem-polysomnographic study of the effect of a newhypnotic drug in sleep apnea syndrome. Pharmacal. Biochem. Bebav.29 (4), 807-809.
Coble, P., Foster, F.G., Kupfer, DJ., 1976. BEG sleep diagnosis ofprimarydeprasion. Arch. Gen. Psychiatry 33,1124-1127.
Cole, 1.0., Schatzberg, A.F., Sniffin, C., ZaIner, I., Cole, I.P., 1981. Tra-zodone in treatment-resistant depression: an open study. 1. Clin. Psy-
chopbamlaCol. 1 (6),495-545.Cunningham, L.A., Bori50n, R.L., Carman, I.S., Chouinard, G.,
Crowder, I.E., Diamond, B.I., Fischer, D.E., 1994. A comparison ofven-lafaxine, trazodone, and placebo in major depression. J. CIin. Psychophar-
macol.14 (2), 99-106.Davis, J., Vogel, C., 1981. Efficacy oftrazodone: data from European and
United States studies. J. C1in. PsychophamlacOl. 1 (6),275-34s.Delini-Stula, A., 1993. Experimentelle und Kliniscbe Pham1akologie. In:
Riederer, P., Laux, C., P6ldinger, W. (Eds.), Neuro-Psychopharmaka:Band 3. Antideprasiva und Phasenprophylaktika. Springer-Verlag,Wien, pp. 20-25.
Dietzel, M., Saletu. B., Lesch, O.M., Sieghart, W., Schjerve, M., 1986.Light treatment in depressive illness: polysomnogriphic, psychomet-ric and neuroendocrinological findings. Eur. Neurol. 25 (Suppl. 2),
93-103.Dryman, A., Eaton. D., 1991. Affective symptoms associated with onset of
major depression in the community: finding from the US NationalInstitute of Mental Health Epidemiological Catchment Area Progr8m.Acta Psychiatr. Scand. 84, 1-5.
Fabre, L.F., 1990. Trazodone dosing regimen: experience with single dailyadministration. J. CIin. Psychiatly 51 (Suppl.), 23-26.
Feinberg, M., Gillin, I.C., Caron, BJ., GredeD. I.F., Zis, A.P., 1982. BEGstudies of sleep in the diagnosis of depression. Biol. Psychiatry 17,305-316.
Ferry, M., 1993. Iatrogenic insomnia. In: AJbarede, J.L., Morley, I.E.,Roth, R., Vellas, BJ. (Eds.), Sleep Disorders and Insomnia in the
Elderly. Springer, New Yo.x, pp. 155-164.Fisher, S., Bryant, S.G., Kent, TA, 1993. Postmarketing surveillance by
patient self-monitoring: tra7Ddooe versus fluoxetine. J. Clin. Psycho-pbarmaool. 13 (4),235-242.
FOld, D.E., Kamerow, D.B., 1989. Epidemiological study of sleep distur-bances and psychiatric disorders: an opportunity for prevention?lAMA, 1. Am. Med. Assoc. 262, 1479-1484.
F_, A., 1997. Phannacology ofanUdepressants. J C1in. PsychophamJa-col. 17 (2). 2-18 (SUDOl. 1).
Fiinfgeld, E. W., 1966. Vigorimeter: Zur Krafbnessung der Hand uJJd zurSim~. Deutsch. Med. Wochenschr. 49, 2214-2216.
Gillin, I.C., DuDCan. W.C., PettigJeW, K.D., Frankel, B.L., Snyder, F., 1979.Successful separation of depressed, nomIal, and insomniac subjects byBEG 5leep data. Arch. Gen. Psychiatry 36, 85-90.
Griinberger, J., 1977. Psychodiagoostik des Alkoholmnken. Ein method-ischer Beitrag zur Bestimmung der Organizitit in der Psychiatrie.Maudrich, Wien.
Hawkin8. D.R., Mcndels, J., 1966. Sleep disturbance in depressive syn-dromes. Am. J. Psychiatry 123, 682-690.
llCObsen, F.M., 1990. Low-dose ~ as a hypnotic in patients treatedwith MAOIs and other psycOOtropics: a pilot study. 1. CIin. Psychiatry51, 298-302.
Kallepalli, B.R., Bhatara, V.S., Fogas, B.S., Tervo, R.C., Misra, LK, 1997.Trazodone is only slightly faster than fluoxetine in relieving insomnia inadolescents with depressive disonIen. J. Child Adolesc. Psychophar-macol. 7 (2), 97-107.
Klieser, E., Lehmann, E., 1988. Experimental comparison between the
effect of staIMiardized ~-amitriptyline and placebo ~tin vitalized depressive patients. PsychopharmacoloIY 95 (Suppl.),S3-SS.
Kupfer, DJ., 1976. REM latency: a psychobiologic marker for primary
depressive i1Jnesa. Biol. Psychiatry 11, 159-174.Kupfer, DJ., Foster, F.G., 1972. Interval between onset of sleep aOO rapid
eye mov~t sleep as an indicator of depression. Lancet I, 684-686.Kupfer, DJ., Foster, F.G., Coble, P., McPartland, RJ., Uhich, R.F., 1978.
The application of BEG sleep for the differential diagnosis of affective
disoIden. Am. 1. Psychiatry 135 (1), 69-74.
G.M. Saletu-Zyhial'Z et aL / Pro~ ill N~Payc/8op/lanllacology & Biological Psychiatry 26 (2002) 249-260 259
ogy, Technique and Scoring System for Sleep Stages of Human Sub-jects. Brain Infonnation Service, Brain Re~ Institute, University of
California, 1A>s Angeles.Reynolds, C.F., Kupfer, D.I., 1987. Sleep research in affective illness: state
of the art circa 1987. Sleep 10 (3), 199-215.Reynolds, C.F., Taska, L.S., I~ D.B., Coble, P.A., Kupfer, DJ., 1983.
REM latency in depression: is there one best definition? BioI. Psychia-
try 18 (8), 849-863.Roberts, R.E., Shema, SJ., Kaplan, G.A, Sttawbridge, WJ., 2000. Sleep
complaints and depression in an aging cohort: a prospective peISpec-live. Am. I. Psychiatry 157 (I), 81-88.
Robinson, R. W., Zwillicb, C. W., 2000. Medications, sleep and breathing.In: Kryger, M.H., Roth, T., Dement, W.C. (Eds.), Principles andPractice of Sleep Medicine, 3rd ed. W.B. Saunders, Philadelphia,
pp.797-812.Rush, AI., Giles, D.E., Roffwarg, H.P., Parker, R.C., 1982. Sleep EEG and
dexamethasone supp.-ion test findings in outpatients with unip<>lafand major depressive disorders. Biol Psychiatry 17,327-341.
Rush, AJ., Giles, D.E., Ian'ett, R.B., Feldman-Koffler, F., Debus, I.R.,Weissenburger, I., Orsulak, P.I., Roffwarg, H.P., 1989. Reduced REMlatency predicts response to tricyclic medication in depressed patients.Biol Psychiatry 26 (I), 61-72.
Salem, B., 1982. PhamIaCO-EEG profiles of typical and atypical antidepres-sants. In: Costa, E., Racagni. G. (Eds.), Typical and Atypical Antide-pressants: Clinical Practice. Raven Press, New Yolk, pp. 257 - 268.
Saletu, B., 1987. The use of pharmaco-EEG in drug profiling. In: Hind-JD8I\1h, I., Stonier, P.D. (Eds.), Human Psychopharmacology, M~Ind Methods, vol I. Wiley, Chichest«, pp. 173-200.
Sa1etu, B., 1997. Visualizing the living human brain. The techniques andpromise of EEG and event-related potentials mapping. In: Iudd, L.,Salem, B., Filip, V. (Eds.), Buic and Clinical Science of Mental andAddjctive Disorders. Bibliotheca Psychiatrica, vol 167. Karger, Basel,pp. 54-62.
Sa1etu, B., 2000. ~nics and EEG: I. From single-lead phar-DWCO-EEG to EEG mapping. In: Saletu, B., Krijzer, F., Ferber, G.,Anderer, P. (Eds.), Electrophysiological Brain ~ in Preclinicaland Clinical Pharmacology and Related Fields - An Update. Facultas
Universititsverlag, Wien, pp. 139-156.Saietu,B., Wesscty, P., Grilnberger, I., Schultes, M., 1987. Erste k1inisclle
Ut8!Icungen Dlll emem neuen tiChlaJanslO!jeOOeB lienzod!azepm, (.;mo-Ia7q)am. mittels eines Selbstbeurtcihmgsbogens fiir Schlaf- und Auf-wai:hqualitit (SSA). Neuropsychiatrie I (4), 169-176.
Saletu, B., Anderer, P., Frey, R., K1Upka, M., KlOscb, G., 1991. Zur Neuro-physiologie des Scblafes. Some remaJb about the neurophysiology ofsleep. Psychiatr. Danubina 3 (1-2), 31-58.
Sa1etu, B., KlOscb, G., Gruber, G., Anderer, P., UdoDntD, P., Frey, R.,1996. First-night-effects on g~ anxiety disorder (GAD}-b88edinsomnia: laboratory versus home sleep recordings. Sleep 19 (9),691-697.
Saletu, B., BJandstitter, N., Frey, R., SIletu-Zyhtarz;, G., Dantendor:&:r, K.,8erg«, P., r.offler, H., 1997L Klinik von SchlafstOnmgm-Erfatmm-gen dber 817 Patieoten einer Schta&mbulanz. Wien. Ktin. WochenlCbr.109 (11), 390-399.
Saletu, B., Saletu-Zyhlsn, G., Anderer, P., BJandstitter, N., Frey, R., Grub-er, G., Kl6scb, G., Mandl, M., GrOnberger, I., Liozmayer, L., 1997b.NooolIBnic insomnia in generalized anxiety disorder: 2. Comp6.-8&i-.restudies on sleep, awakening, daytime vigilance Ind anxiety under Ior-azepam plus diphenhydramine (SomniumR.) versus lorazep8m alone,utilizing clinical. polysomnographic and EEG mappm, methods. Neu-ropsychobiology 36, 130-152.
Salem, A., Gritscb, F., Salem, B., Gruber, G., Anderer, P., Maitath-Pokorny, G., Slavicek, R., 1998. Therapie von Schnarchen undsch-\afbezogenen Atmungsst6nmgen mittels eines ProtnISionsbdlelfs(Noiselezze). Stomatologie 95 (5), 203-218.
Salem, B., Anderer, P., Pascual-Marqui, R.D., 2000a. 1A>w-resolution elQ:-tromagnetic tomography (LORETA) in psychopharmacology. Eur.Amb. Psychiatry: Clin. Neurosci. 250 (Suwlt), 9.
Kupfer, D.J., Frank, E., Grochocinski, V.J., Gregor, M., McEachran, A.B.,1988. Electroencephalographic sleep profiles in ~t depression: a
longitudinal investigation. Arch. Gen. Psychiatty 45,678-681.
Kupfer, DJ., Ehlers, C.L., Frank, E., Grochocinski, VJ., McEachran, A.B.,1991. EEG sleep and recurrent depression. Bioi. Psychiatry 30,
641-655.Li1jen~ B., Almwvist, M., Hetta, J., Roos, B.E., Agren, H., 1989. Af-
fective disturbance and insomnia: a population study. Eur. J. Psychiatty
3(2),91-98.Livingston, G., Hawkins, A., Graham, N., Blizard, B., Mann, A., 1990. The
Gospel Oak Study: prevalence rates of dementia, ~ion and timi-tation among elderly residents in Inner Lonckln. PsyclIOI. Med. 20,
137-146.Mann, J.J., Georgotas, A., Newton, R., Gershon, S., 1981. A controlled
study of trazodone, imipramine, and placebo in outpatients widl endog-
enous depression. J. Clin. PSYchophannacoL 1 (2),75-80.
Mashiko, H., Niwa, S., Kumashiro, H., Kaneko, Y., Suzuki, S., Numata, Y:,Horikoshi, R., WataDabe, Y., 1999. Effect of~ in a single dosebefore bedtime for sleep di~ accon1)anied by a depressive state:dose-finding study widl no concomitant use ofhypnoti<: agent. Psychia-try C1in. Neurosci. 53 (2), 193-194.
Mendelson, W.B., Garnett, D., Gillin, C., 1981. ~induced sleepapnea syndrome in a patient widl insomnia and mild sleep-related res-piratory changes. J. Nerv. Ment. Dis. 169, 261-264.
Mezzich, J.E., Cohen, N.L., 1996. Towards a Quality of Life Index: effi-cacy and cultural sensitivity. Paper presented at d1e International Con-gress of dIe International Federation for Psychiatric Epidemiology,Santiago de Compostela, Spain.
Mezzich, J.E., Rui~ M.A., Perez, C., Yoon, G., Liu, J., Mahmud, S.,2000. The Spenish version of d1e Quality of Life Index: presentationand validation. Nerv. Ment. Dis. 188 (5), 301-305.
Montgomery, J., Oswald, 1, Morgan, K., 1983. Traw<kme enhances sleepin subjective quality but not in objective duration. J. Clin. PbarmacoL16, 139-144.
Moon, CA., Davey, A., 1988. The efficacy and residual effects oftruodone (ISO mg nocte) and mianserin in dIe treatment of de-pressed general practice patients. Psycbopbaml8Cology 95 (Supp1.),87-S13.
Mouret, J., Lemoine, P., Minuit, M.P., Benkelfat, C., Ren8Idet, M., 1988.ElleclS of lrazOOone un Ule sleep ut depressed subjects - a polygrapQ1c
study. Psychopbaml8Cology 9S (SuppL), S37-S43.Muratorio, A., Maggini, C., CoccagDa, G., Guazzelli, M., 1974. Poly-
graphic study of the all-night sleep pattern in neurotic and depressedpatients treated widl trazodone. In: Ban, ThA, Siivestrini, B. (Eds.),TrazoOOne. Proceedings of the First International SymposilDD, Mon-treal, Quebec, October 1973. Modern Problems of ~sychia-try 9, 182-189.
Newton, R., 1981. The side effect profile oftramdone in compariIOO to an8Ctive ~trol and placebo. J. C1in. PsychopbanDBCOl. I (65), 898-93S.
Nierenberg. A.A., Adler, LA, Pese1ow, E., Zombag, G., Rosendlal, M.,1994. Tramdone for lDtidepIasant-associated insomnia. Am. J. Psy-chiatry 151 (7), 1069-1072.
Obemdorfer, S., Saletu-ZYhlan. G., 8aietu, B., 2000. Effects of selectiveserotonin ~ inhibitors on objective and subjective sleep~.Neuropsychobiology 42, 69-81.
Paik, 1H., Lee, C., Choi, B.M., Chne, YoL, NiDI, C.E., 1989. Mianserin-induced restless legs syndrome. Br. J. Psychiatty 155, 41S.
Perlis, ML., Giles, D.E., Buysse, D.J., Kupfer, DJ., 1997. Self-repoi1edsleep disturbance as a prOOromal symptotn in ~t depression.J. Affective DisOItl. 42, 209-212.
Perry, PJ., Garvey, M., Kelly, M., Cook, B., Dunner, F., Winokur, G., 1989.A comparative trial of tluoxetine v~ ~ in outpatients withmajor deprasion. J. C1in. Psychiatry SO (8), 290-294.
Quera-Salva, M.A., OrIuc, A., Goldenberg, F., Guilleminault, C., 1991.Insomnia and use of hypnotics: study of a F~ popuJation. Sleep14 (5), 386-391.
Rechtscbaft'en, A., Kales, A., 1968. A Manual of StaDdardizm Tenninol-
G.M. Saletll-Zyhlan et aL / Progress ill Neuro-PSYChophannacology '" Biological Psychiatry 26 (2002) 249-260260
Thase, M.E., Kupfer, D.J., Ulrich, R.F., 1986. EEG sleep in psychoticdepression: "a valid subtype". Arch. Gen. Psychiatry 43, 886-893.
Usti1n, T.B., Privett, M., Lecrobi«, Y., Weill«, E., Simon, G., KorteD, A.,Bassett, S.S., Maier, W., Sartorius, N., 1996. ForDl, ~uency andburden of sleep problems in general health care: a report from theWHO collaborative study on psychological problems in Genen1 HealthCare. Em. J. Psychiatry II (Supp1. 1),5-10.
Van Bemmel. A.L.., Havermans, R.G., Van Diest, R., 1992. Effects of
tr8zodoDe on EEG sleep and clinical state in major depression. Psycho-pharmacology 107, 569-574.
Yon Zcrssen, D., Koeller, D.M., Rey, E.R., 1970. Die Befindlichkeitsskala(B-S)-ein einfaches InstnIment zur Objektivienmg von Betindlich-keitssronmgen,insbesondere im Rahmen von Lingsschnittuntemlchun-gen. Arzneim.-F~. Drug Res. 20, 915-918.
Ware, l.C., Piuard, J., 1990. Inaeased deep sleep after tra7X>done use: adouble-blind placebo-controlled study in healthy young adults. J. Clin.Psychiatry 51 (Suppl.9), 18-22.
Ware: l.C., Brown, F.W., Moorad, PJ., et aI., 1984. Nocturnal myoclonusand tricycljc antideprasants.Sleep Res. 13,72.
Ware, l.C., Rose, F.V., McBray«, R.H., 1994. The acute effects ofllefam-done, trazodone and buspirone on sleep IIxI sleep-related penile tuua-cence in nonnal subjects. Sleep 17 (6), 544-550.
Weisler, R.H., Johnston, J.A., Lineberry, C.G., Samara, B., Bran-conni«, RJ., Billow, A.A., 1994. Comparison ofbubropion and trazo-done for die treatment of major depression. J. am. PsychopblJmlcol.14 (3), 170-179.
Wheatley, D., 1984. Trazodone: alternative dose ~ andsieep. Phar-matberapeuUca 9 (3), 607-612.
World Health Organisation, 1992. international Statistical Classification ofDiseases and Related Health Problems, 1001 ed. WHO, Geneva.
World Medical Assembly, 1996. WMA Recommendations Guiding Physi-cians in Biomedical Research involving Human Subjects. World Med-ical Association, Ferney-Voltaire.
YImadera, H., NakamW'I, So, Suzuki, H., Endo, S., 1998. Efrecu oftrazo-done hydrochloride and imipramine on po1ysomnography in healthysubjects. Psychiatry Clin. Neuroaci. 52 (4), 439-443.
Yamadera, H., Suzuki, H., Nakamura, S., EnOO, S., 1999. Effects oftr8ZA)mne on poiysomnography, blood concentIation and core bodytemperature in healthy volunteers. Psychiatry am. Neuroaci. 53 (2),189-191.
Zung, W. W.K., 1965. A self-rating depression scale. Arch. OeD. Psychiatry
12,63-70.Zung, W.W.K., 1976. SAS, self-rating anxiety BCale. in: Guy, W. (Ed.),
ECDEU Assessment Manual for PSYChophannlCOlogy, revised ed.,Nation8l Institute of Mental Health, Rockville, MD, pp. 337-340.
Salem, B., Grober, G., Salem, M., Brandstitter, N., Hauer, C., Prause, W.,Ritter, K., Saletu-ZyhIarz;, G., 2000b. Sleep laboratory studies in restlesslegs syndrome patients as compaJed with normals and acute effects ofropinirole: I. Findings on objective and subjective sleep and awakening
quality. Neuropsycbobiology 41, 181-189.
Salem, M., Anderer, P., Salem, B., Hauer, C., Mandl, M., Obemdorfer, S.,Zogblami, A., Saletu-Zyb1arz, G., 2000c. Sleep laboratory studies inrestless legs syndrome patients as compared with nonna1s and acuteeffects of ropinirole: 2. Findings on periodk: leg movements, arousalsand respiratory variables. Neuropsychobiology 41, 190-199.
Salem, Mo, Anderer, P., Salem, B., Hauer, C., M8nd1, M, Semler, B., Saletu-ZyhIarz;, G., 2001. Sleep laboratory studies in periodic limb movementdisorder (pLMD) as compared with nonna1s and acute effects of ropi-nirole. Hum. Psychopbalmacol. Clin. Exp. 16 (2), 177-187.
Salem, B., Priemer, Y., and ScbrOckenfuchs, B., in preperation. C1inicalinvestigations on the efficacy and tolerabilitY of a retard fOIDlulationof trazodone in the psychiatric practice.
Saletu-Zyblarz, G., Salem, B., Anderer, P., Brandstitter, N., FIey, R., Grober,G., KlOsch, G., Mandl, M., Griinberger, J., Linzmayer, L., 1997. Non-organic insomnia in g~ anxiety disorder: 1. ConIroDed sbldieson sleep, awak~ and daytime vigilance utilizing polysomnoglapbyand EEG mapping. Neumpsychobiology 36, 117-129.
Saletu-Zyblarz, G.M.;Anderer, P., Berga', P., Grober, G., Obemdorfel', S.,Saletu, B., 2000a. Nonorganic insomnia in panic disorder: COmp8rativesleep laboratory sbldies with normal controls and pllcebo-controUedtrials with alprazolam. Hum. Psychopharmacol15, 241-254.
Saletu-Zyb1arz, G., Anderer, P., Gruber, G., Mandl, M, Saietu, B., 2000b.Polysoumography, EEG-mapping and EEG-tomography in diagnosisand therapy of nonorganic insomnia in anxiety disorders. Em. An:h.Psychiatry: C1in. Neurosci. 250 (Suppl 1), 2.
Saletu-ZyhilrZ, G.M., Hassan Abu-Ban, M., Ander«, P., Semler, B., Deck-er, K., P8r8patics, S., Tscbjda, U., Winkler, A., Salem, B., 2001. in-somnia related to dysthymia: polysomnographic and psychometriccom.-nson with nonnal controls and acute theIapeutic ttia1s with tIa-zodale. Neuropsycbobioiogy 44 (3), 142-150.
Scharf, M.D., Sacbais, B.A., 1990. Sleep laboratory evaluation of the ef-fects and efficacy of ~ in depreaecI insomDiac patients. J. Clin.Psychiatry 51 (Suppl), 13-17.
Schramm, E., Hohagen, F., Kappler, C., Gnashoff, U., Berger, M., 1995.Mental COInOriJidity of chronic insomnia in general practice atfendersusina DSM-m-R. Acta Psychiatr. Scand. 91, 10-17.
Sharpley, A.L., Cowen, P J., 1995. Effect of pbalmacologic treatments onthe sleep of depressed patients. Biol Psychiatry 37 (2), 85-98.
SilveslriDi, B., 1988. Beyond the limits of typical anti~ Psycho-pharmacology 95 (Suppl), Sl-S2.