Infection Control Training - Advance · Prevention and management of infectious or communicable...
30
1 Infection Control Training New York State Department of Health State Education Department 2001 Syllabus Revised July 2007, November 2008 Developed by Robin Haag, RNC, MA Infection Control Director, Coney Island Hospital Presented by Barbara A. Smith, MPA, CIC St. Luke’s Roosevelt Medical Center 1 Background • Chapter 786 of the Laws of 1992 established a requirement that certain health care professionals licensed in NYS receive training on infection control and barrier precautions by July 1994 and every four years thereafter unless otherwise exempted 2 Statute Applies To: • Dental hygienists • Dentists • Licensed practical nurses • Optometrists • Physicians • Physician assistants • Podiatrists • Registered professional nurses • Specialist assistants • New as of 11/08 – Medical & PA students 3 Documentation • Submit certification of training to hospital/facility that maintains credentials for granting professional privileges to practice • If not employed by a State regulated facility submit form to NYSDOH attesting to completion of required training 4 Goals of Infection Control Training • Assure the understanding of how bloodborne pathogens (BBP) may be transmitted in the work environment : – patient to healthcare worker: hepatitis B Occupational cases of HBV in HCWNIOSH- Worker Health Chart book - 2004 5 Transmission in the Workplace – Healthcare worker to patient : NEW YORK CITY – 3/15/07 15, 2007 – patient to patient: Hepatitis C – NY and Nevada Acute Hepatitis C Virus Infections Attributed to Unsafe Injection Practices at an Endoscopy Clinic --- Nevada, 2007 May 16, 2008/ 57(19);513-517 HEALTH DEPARTMENT AND ST. BARNABAS HOSPITAL NOTIFY PATIENTS OF POTENTIAL TUBERCULOSIS EXPOSURE Mothers, Babies, Patients, and Staff who Were in the Maternity, Neonatal, or Psychiatric Units at St. Barnabas Hospital in the Bronx from November 1, 2006 – January 24, 2007 May Have Been Exposed and Should be Screened Immediately
Transcript of Infection Control Training - Advance · Prevention and management of infectious or communicable...
1
Infection Control Training
New York State Department of Health
State Education Department
2001 Syllabus Revised July 2007, November 2008
Developed by Robin Haag, RNC, MA
Infection Control Director, Coney Island Hospital
Presented by Barbara A. Smith, MPA, CIC
St. Luke’s Roosevelt Medical Center 1
Background
• Chapter 786 of the Laws of 1992
established a requirement that certain health
care professionals licensed in NYS receive
training on infection control and barrier
precautions by July 1994 and every four
years thereafter unless otherwise exempted
2
Statute Applies To:
• Dental hygienists
• Dentists
• Licensed practical
nurses
• Optometrists
• Physicians
• Physician assistants
• Podiatrists
• Registered
professional nurses
• Specialist assistants
• New as of 11/08
– Medical & PA students
3
Documentation
• Submit certification of training to
hospital/facility that maintains credentials
for granting professional privileges to
practice
• If not employed by a State regulated facility
submit form to NYSDOH attesting to
completion of required training
4
Goals of Infection Control Training
• Assure the understanding of how bloodborne pathogens
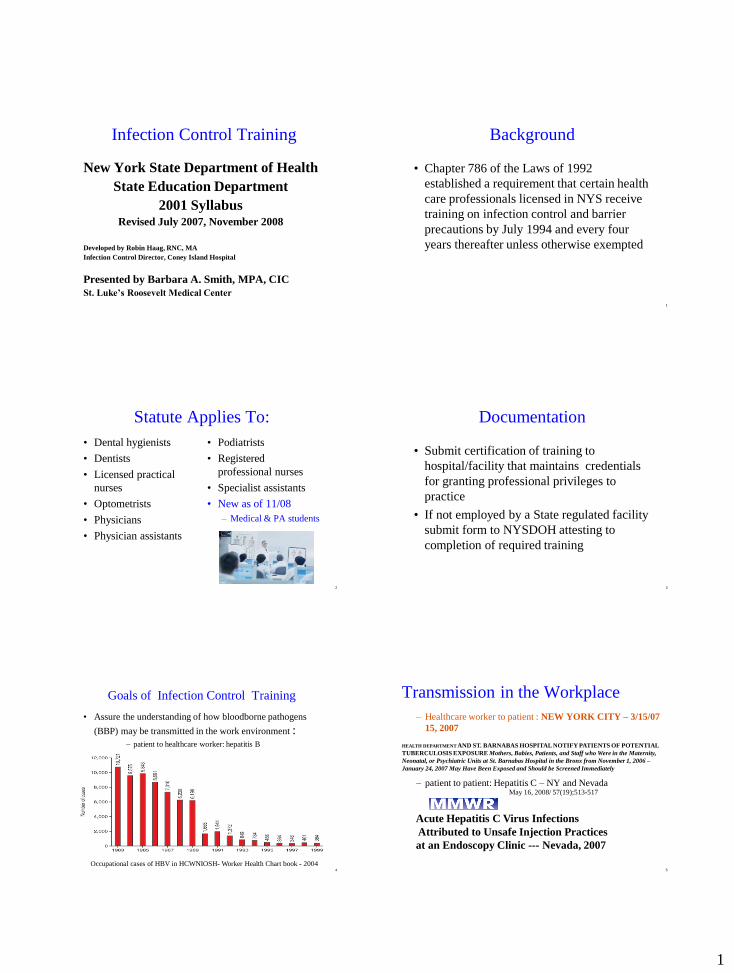
(BBP) may be transmitted in the work environment : – patient to healthcare worker: hepatitis B
Occupational cases of HBV in HCWNIOSH- Worker Health Chart book - 2004 5
Transmission in the Workplace
– Healthcare worker to patient : NEW YORK CITY – 3/15/07
15, 2007
– patient to patient: Hepatitis C – NY and Nevada
Acute Hepatitis C Virus Infections
Attributed to Unsafe Injection Practices
at an Endoscopy Clinic --- Nevada, 2007
May 16, 2008/ 57(19);513-517
HEALTH DEPARTMENT AND ST. BARNABAS HOSPITAL NOTIFY PATIENTS OF POTENTIAL
TUBERCULOSIS EXPOSURE Mothers, Babies, Patients, and Staff who Were in the Maternity,
Neonatal, or Psychiatric Units at St. Barnabas Hospital in the Bronx from November 1, 2006 –
January 24, 2007 May Have Been Exposed and Should be Screened Immediately

2
•NYC – Sept ’08
•2 women rec’d epidural – S. salivarius meningitis
•Ohio - May ’09
•3 women rec’d epidural- S. salivarius meningitis
•One fatal
6
Bacterial Meningitis After Intrapartum Spinal
Anesthesia --New York and Ohio, 2008- 2009 MMWR January 29, 2010 / 59(03)
7
Goals Continued:
• Apply current scientifically accepted infection
control principles, as appropriate for the specific
work environment
• Minimize opportunity for transmission of
pathogens to patients and healthcare workers
• Familiarize professionals with the law requiring
this training and the professional misconduct
charges that may be applicable for not complying
with the law.
8
New York State Public Health Law
• Section 2819 enacted in 2005
• Effective January 1, 2007
• Mandates reporting of:
– Central Line Associated Blood Stream Infections in ICUs
– Coronary Artery Bypass Surgical Infections
– Colon Surgical Site Infections
– Hip Replacements Surgical Site Infections
– C. difficile
9
MDRO Guidelines
• Management of Multidrug-Resistant Organisms in
Healthcare Settings, 2006. Jane D. Siegel, MD; Emily
Rhinehart, RN MPH CIC; Marguerite Jackson, PhD; Linda Chiarello,
RN MS; the HICPAC
• JCAHO expectation
• Designed to:
– halt the rising rates of drug-resistant infections
10
MRSA Guidelines
• Guide to the Elimination of MRSA Transmission
in Hospital Settings. March 2007
• www.apic.org
– Click on implementation guide
– Risk assessments
– Surveillance cultures
– Contact isolation
• Pending NYS legislation
– Reporting all MRSA infections
11

3
Six Core Elements
• Element I
The responsibility to adhere
to scientifically accepted
principles and practices of
infection control and to
monitor the performance
of those for whom the
professional is responsible
• Element II
Modes and mechanisms of
transmission of pathogenic
organisms in the
healthcare setting and
strategies for prevention
and control
12
Elements continued
• Element III
Use of engineering and work
practice controls to reduce
the opportunity for patient
and healthcare worker
contact with potentially
infectious material for
bloodborne pathogens.
• Element IV
Selection and use of barriers
and/or personal protective
equipment for preventing
patient healthcare worker
contact with potentially
infectious material
13
Final 2 Elements
• Element V
Creation and maintenance of
a safe environment for
patient care through
application of infection
control principles and
practices for cleaning,
disinfection, and
sterilization
• Element VI
Prevention and management
of infectious or
communicable diseases in
healthcare workers
14 15
Element I
• The responsibility to adhere to scientifically
accepted principles and practices of
infection control and to monitor the
performance of those for whom the
professional is responsible
16
Learning Objectives
• Recognize the benefit to patients and HCWs of
adhering to scientifically accepted principles and
practices of IC
• Recognize the professional’s responsibility to
adhere to scientifically accepted IC practices and
consequences of failing to comply
• Recognize the professional’s responsibility to
monitor IC practices of those for whom she/he is
responsible and intervene as necessary for
compliance and safety
17
Source of Standards
• NYS Education Department, Board of
Regents, Section 29.2 (A) (13) defines
unprofessional conduct as “failure to use
scientifically accepted infection prevention
techniques.”
• Part 92 of Title 10 (Health) of the Official
Compilation of Codes, Rules and
regulations of New York
• Statements of relevant professional and
national organizations

4
18
NYS DOH Mandates
• Infection control training for health professionals
• Enforcement of infection control standards in licensed health facilities
• Protection of HCWs from exposure to infection as per OSHA
• Processes and procedures to evaluate infected HCWs
• Policies to protect confidentiality of HCWs
• Policies for prevention and transmission within a facility
19
Implication of Professional
Conduct Standards
• Professional responsibility to adhere to
infection control standards
• Professional responsibility for monitoring
others
20
Monitoring Compliance of
Regulations
• New York State Public Health Law Article 28
inspections
• JCAHO Surveys and other accreditation bodies
– Patient Safety Goals
• OSHA and PESH inspections
• Inter-agency sharing of findings
• Penalties and fines for failure to comply with
standards
Consequences of Failing to Apply IC
Standards
• Increase risk of
adverse health
outcomes for patients
and healthcare
workers
• Subject to charges of
professional misconduct if
managers: – fail to report misconduct
– fail to conduct complaint
investigation
• Possible outcomes – professional liability
– disciplinary action
– revocation of professional
license
21
22
Methods of Compliance
• Participation in required infection control
training
• Adherence to accepted principles and
practices of infection control
23
Element II
• Modes and mechanisms of transmission of
pathogenic organisms in the healthcare
setting and strategies for prevention and
control
5
24
Learning Objectives
• Describe how pathogenic organisms may be
spread in healthcare settings
• Identify the factors which influence the
outcome exposure
• List the strategies for preventing
transmission of pathogenic organisms
• Describe how infection control concepts are
applied in professional practice
25
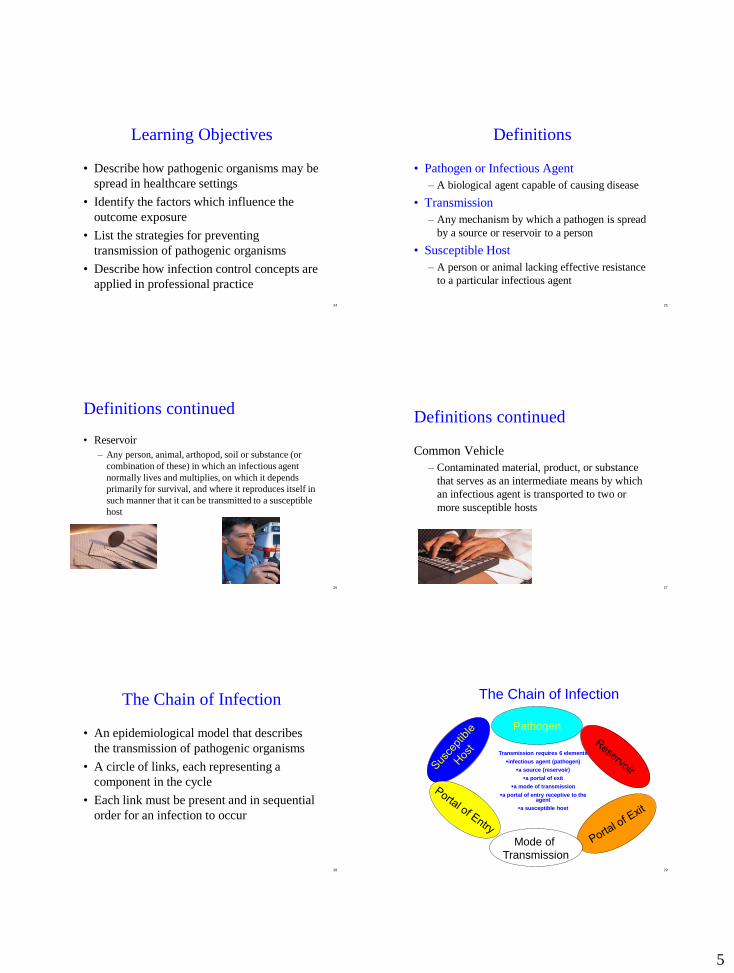
Definitions
• Pathogen or Infectious Agent
– A biological agent capable of causing disease
• Transmission
– Any mechanism by which a pathogen is spread
by a source or reservoir to a person
• Susceptible Host
– A person or animal lacking effective resistance
to a particular infectious agent
Definitions continued
• Reservoir
– Any person, animal, arthopod, soil or substance (or
combination of these) in which an infectious agent
normally lives and multiplies, on which it depends
primarily for survival, and where it reproduces itself in
such manner that it can be transmitted to a susceptible
host
26 27
Definitions continued
Common Vehicle
– Contaminated material, product, or substance
that serves as an intermediate means by which
an infectious agent is transported to two or
more susceptible hosts
28
The Chain of Infection
• An epidemiological model that describes
the transmission of pathogenic organisms
• A circle of links, each representing a
component in the cycle
• Each link must be present and in sequential
order for an infection to occur
29
Pathogen
Mode of
Transmission
The Chain of Infection
Transmission requires 6 elements
infectious agent (pathogen)
a source (reservoir)
a portal of exit
a mode of transmission
a portal of entry receptive to the agent
a susceptible host

6
30
Presence of a Pathogen
• Bacteria
• Viruses
• Fungi
• Parasites (protozoa and helminths)
• Prions
– small proteinaceous particles
– resists inactivation procedures
Reservoirs
• Animate
– Human reservoirs may
be symptomatic of
infection or may be
non- symptomatic
carriers
• Inanimate
– Objects (fomites) may
also be reservoirs for
infection
• Contaminated
equipment or supplies
31
32
Portals of Exit
• Mechanism by which pathogens leave the
reservoir
• Allows for the pathogen to be transmitted to
a susceptible host
– drainage of blood and other body substances
– coughing, sneezing respiratory / oral secretions
– draining lesions
– feces
33
Modes of Pathogen Transmission • Direct contact with the source
– Airborne (TB)
– Droplet spread (Meningitis)
• Direct physical contact
– or indirect contact with a fomite
• Common vehicle by an intermediate means of transmission
to multiple susceptible hosts
– Food borne pathogens (E Coli)
• Vectorborne transmission through a pathogen carrying
organism
– Insects (Malaria, WNV, Lyme Disease)
34
Portals of Entry
• Sites and mechanisms by which pathogens
are introduced to a susceptible host
• Susceptible host
– lacks effective resistance to infectious agent
– entry sites (mucous membranes, non-intact
skin, gastrointestinal, respiratory, gentourinary
tracts)
– mechanism of introduction (percutaneous
injury, vascular access, other invasive devices,
surgical incision)
35
Host Factors that Influence the
Outcome of Exposures
• Natural barriers – intact skin
– respiratory cilia
– gastric acid
– tears
– normal flora
• Extremes of age
• Underlying pathology
• Nutrition
• Lifestyle
• Invasive procedures or
devices
• Medication (steroids,
chemotherapy, antibiotics)
• Immune System
– inflammatory response
– humoral immunity
– cell-mediated
immunity

7
36
Agent Factors that Influence the
Outcome of Exposures
• Agent Factors
– Infectivity
– Pathogenicity
– Virulence
– Size of inoculum: How big
– Route and site of exposure: Entry
– Duration of exposure: Time
37
Environmental Factors that
Influence the Outcome of
Exposures
• Contamination of environment
• Contamination of equipment
• Guideline for Environmental Infection Control in Health-Care Facilities. – MMWR. June 2003
– Recommendations of the Advisory Committee on Immunization Practices (ACIP)
38
How We Break The Links
• Eliminate the agent by reducing the number of organisms
– Sterilization / Disinfection
• Remove the means of transmission
– Cleaning Blood Spills Properly
• Limit the susceptibility of the host
– Wearing a PFR 95 Particulate Respirator
39
Prevention Strategies
• Standard Precautions
– Consider all patients to be potentially infected
with a bloodborne pathogen (BBP)
• Non BPP
– Early identification
– Prompt isolation
– Appropriate treatment
40
Hand Hygiene
• The single most important measure in breaking the
chain of infection
• Compliance is poor
• CDC Guidelines
– Guideline for hand hygiene in health-care settings:
recommendations of the Healthcare Infection Control
Practices Advisory Committee and the
HICPAC/SHEA/APIC/IDSA Hand Hygiene Task
Force. MMWR. 2002;51(RR-16):1-44.
41

8
42
Hand Flora
• Resident Flora
– AKA colonizing flora
– Can be isolated on hands of most people
– Not readily removed by mechanical friction
• Transient Flora
– AKA contaminating or non-colonizing flora
– Readily transmitted unless removed by hand
hygiene
43
44
Selection Of Products
• Antiseptic soaps
• Scrubs
• Waterless hand sanitizers
• Selection of product based on: – Desired characteristics
• Rapidity of flora reduction, persistence of action, absorption, spectrum
– Staff acceptance
– Where product will be used
– Cost
– Safety and efficacy
– Potential contamination of soaps
45
Antimicrobial Products
• Use where invasive procedures are performed
• Use in special care units
• Use in areas where patients have resistant organisms
• CHG: Chlorhexadine gluconate – Remains active for 6 hrs on skin
– Neutralized by hand creams
• PCMX: Para-chloro meta-xylenol – Less active than CHG
– Neutralized by hand creams
• Iodophor – Slightly less effective than CHG
– Inactivated by organic material
• Triclosan: Dichlorophenoxyl – Absorbed through intact skin
– Commonly used in commercial soaps
46
Antimicrobials continued
• Waterless Alcohol Based hand sanitizers
– 60 - 70% alcohol solutions kill 99% of most
common organisms including MRSA,
Acinetobacter and VRE
– Emollients reduce dryness
– Takes less than 30 seconds to use
– Can be carried in pockets or wall mounted
– Use where non-anti-microbial soaps are used
47
Non-Antimicrobial Soap
• Standard hand soap
– No antimicrobial activity
– Use in visitors areas
– Use in bathrooms
– Use in conjunction with hand sanitizers
– Bar soap must be placed on racks that permit drainage
• Organisms collect in pools of water and then become reservoirs for soap.

9
48
Hand Washing Instructions
• Wet hands with warm
water
• Apply soap
• Lather hands well
• Vigorously rub
together all hand
surfaces for 10 - 15
seconds
• Thoroughly rinse
hands under a stream
of water
• Completely dry hands
with a clean paper
towel
• Use a clean dry paper
tower to turn off the
faucet
49
50
Hand Sanitizing Instructions
• Hold one hand under dispenser spout and press
• the lever once or twice with your other hand
• Use enough alcohol to wet all surfaces of your hands
• Spread the alcohol thoroughly over your hands and
fingers
• Rub your hands together until the alcohol is dry
• Do Not rinse with water
• Do Not use a source of electricity or flame until dry
• Do Not drink!
51
ABHR really works!
52
Fingernails
• Natural Nails
• No artificial fingernails or extenders
– For direct care providers with patients at high
risk for infection (OR, ICU, Transplant)
– Hospital policy
• No chipped nail polish
• ¼ inch beyond fingertip
53
Control of Transmission Routes
• Standard precautions for all patients
• Use of appropriate barriers
• Sterilization or disinfection of patient care
equipment
• Isolation/cohorting communicable
individuals – Who is in the next bed?
“If you’re in a two, three or four-bedded
room, each time you get a new roommate
your risk of acquiring these serious
infections increases by 10 per cent,” says
Dr. Zoutman

10
54
Standard Precautions
• Apply to ALL patients
• Use Personal Protective Equipment (PPE)
• Wear gloves before touching:
– body fluids
– mucous membranes
– non-intact skin
• Change gloves between patients
• Wash hands after removing gloves
55
Transmission Based Precautions
• Guideline for Isolation Precautions: Preventing
Transmission of Infectious Agents in Healthcare Settings, June 2007, Siegel JD, Rhinehart E, Jackson M, Chiarello L, and the
Healthcare Infection Control Practices Advisory Committee, 2007
• Isolation based on route of transmission
• Airborne precautions
• Droplet precautions
• Contact precautions
• Protective isolation
Airborne Precautions
• Use for:
– TB
– Varicella (with contact)
– Measles
– Variola
– SARS
– Avian flu
56 57
Airborne Pathogens
Prevention and Control Early Identification of Suspect Cases
– Triage and separate possibly infectious individuals from others
– Respiratory Etiquette
• Signage
• Instruct patient to wear surgical mask
• Instruct patient to cover mouth with tissue
• when coughing or sneezing
• Garbage cans
• Hand sanitizer availability
58
Airborne Pathogens continued
• Engineering Controls to Prevent Transmission
– Negative Pressure Isolation Rooms
• Air currents prevented from entering corridor
• Monitor effectiveness of negative pressure
– Air Exchanges
• New Construction: 12 per hour
• Old Construction: 6 per hour
– Alarms and Physical Testing
• Smoke or tissue tests
• Logs
HEPA filtration
UV irradiation 59
Airborne Pathogens continued
• Personal Protective Equipment (Element IV)
• Special Considerations
– Operating suites
• all have positive pressure
• air flows from room into the corridor
– Procedures associated with transmission of
extrapulmonary TB
– Limit transportation of potentially infectious
patients

11
60
Droplet Precautions
• Standard procedure mask required when within 3 - 6 feet of the patient
• Private room
• Use for:
– Pneumonic Plague
– Influenza
– Rubella
– Adenovirus
– Meningococcal meningitis
– Pertussis 61
Contact Precautions
• Gloves for contact with infective material
• Change gloves when contaminated
• Gowns for close contact with patient
• May or may not require a private room
• Patients with like organisms and sites
may be cohorted
• Used for resistant organisms, Scabies, C Difficile
Respiratory etiquette
Necessary because unable to identify all infectious sources immediately
and consistently
Implemented at first point of contact and in conjunction with standard
precautions
• 1. Visual alerts to patients to report symptoms of
respiratory illness.
• 2. Respiratory hygiene
– Cover your mouth and nose with a tissue when
coughing or sneezing
– Use the nearest waste receptacle to dispose of the tissue
after use.
– Perform hand hygiene after having contact with
respiratory secretions.
• 3. Masking and separation of patients with
respiratory symptoms.
Key components
Resources: http://www.cdc.gov/flu/professionals/infectioncontrol/resphygiene.htm
Cover your cough multiple
languages
Symptoms alert
65
Environmental Control Measures
• Environmental cleaning
• Appropriate ventilation
• Waste management
• Linen and laundry management

12
66
Additional Controls
• Support and Protection of the Host
– Vaccination
– Pre and post exposure prophylaxis
– Protecting skin and immune system integrity
• Training and Education of HCWs
67
Element III
• Use of engineering and work practice
controls to reduce the opportunity for
patient and healthcare worker contact with
potentially infectious material for
bloodborne pathogens.
68
Learning Objectives
• Define “engineering controls” and “work”
practice controls”
• Describe specific practices and settings
which increase the opportunity for exposure
to healthcare workers and patients
• Identify where engineering or work practice
controls can be utilized to prevent exposure
69
Definitions
• Engineering Controls
– Equipment, devices or instruments that remove
or isolate a hazard
• Work Practice Controls
– Controls that reduce or eliminate the
likelihood of exposure by altering the manner
in which a task is performed
• Personal Protective Equipment (PPE)
– Equipment or clothing worn to reduce the
exposure to hazards
70
High Risk Practices and
Procedures
• Percutaneous Exposures
– Injury through
handling/disassembly/disposal/reprocessing of
needles and other sharps
• manipulating needles and other sharps by hand
• recapping using a two-handed technique
• removing scalpel blades
71
High Risk Practices and Procedures continued
Procedures in which there is opportunity for
injury, particularly where there is poor
visualization
• blind suturing
• non-dominant hand opposing next to a sharp
• bone spicules or metal fragments
• passing sharp instruments
13
72
High Risk Practices and Procedures continued
• Mucous membrane and non-intact skin
exposures
– Direct contact with blood or body fluid
• contaminated hand in contact with eyes, nose
or mouth
• open skin lesions on hands/dermatitis
– Splashes or sprays of blood or body fluid
• irrigation/suctioning
73
High Risk Practices and
Procedures continued
• Parenteral Exposures
– Injection with infectious material
– Infusion of contaminated blood products or
fluids
– Multidose vials
74
Evaluation/Surveillance of
Exposure Incidents
• Identification of those at risk for exposure
(who)
• Identification of devices causing exposure
(what)
– Devices with higher disease transmission risk
(hollow bore)
– Devices with higher injury rates (butterflies
recoil action)
– Devices by name brand 75
Evaluation/Surveillance of
Exposure Incidents continued
• Identification of areas/settings where
exposures are occurring
• Circumstances by which exposures are
occurring
• Identify trends and hazards for the purpose
of minimizing future exposures
76
Engineering Controls Which
Eliminate or Isolate the Hazard
• Use safer devices whenever possible to
prevent sharps injuries – proper evaluation and selection of safer devices
– passive vs. active safety devices
– mechanisms that provide continuous protection immediately
– integrated safety equipment vs. accessory devices
http://www.healthsystem.virginia.edu/internet/EP
INet/safetydevice.cfm
77
Engineering Controls continued
• Proper education and training on safer devices
• Eliminating the traditional or non-safety
alternative whenever possible
• Puncture resistant containers for transport and
disposal of needles and other sharps
– NIOSH guidelines for selecting containers
– Location and accessibility
• Splatter shields on medical equipment with risk
prone procedures
– Locking centrifuge lids

14
78
Work Practice Controls
• General Practices
– Handwashing
– Prompt cleaning of blood and body fluid spills
with appropriate disinfectant
– Proper disposal/handling of blood and body
fluid, including contaminated patient care items
– Use of personal protective equipment (PPE)
• Element IV
79
Work Practice Controls continued
• Percutaneous Exposures
– Avoiding unnecessary use of needles and other
sharps
– Using care in handling/disposal of needles and
other sharps
• No recapping unless absolutely medically necessary
and then only using one-hand technique or safety
device
• Passing sharps by use of designated “safe zones”
• Disassembling sharp equipment with forceps or
other devices
80
Work Practice Controls continued
• Modifying Procedures to Avoid Injury
– Using forceps, suture holder or other
instruments for suturing
– Not holding tissue with fingers when suturing
or cutting
– Not leaving sharps on a field
– Cleaning up after yourself
– Checking linen for sharps/trash before disposal
– Asking for assistance with procedures 81
Work Practice Controls continued
• Appropriate Use of Safety Devices
– Attend the inservice
– Always activate the safety feature
– Never circumvent the safety feature
– Give the safer device a chance
• learning curve
82
Safe injection practices
Pathogens can be present in sufficient quantities to produce infection in the absence of visible blood
Unsafe injection practices have resulted in:
• Transmission of bloodborne viruses, including hepatitis B and C viruses to patients;
• Notification of thousands of patients of possible exposure to bloodborne pathogens
• Referral of providers to licensing boards for disciplinary action; and
• Malpractice suits filed by patients.
83
Acute Hepatitis C Virus Infections Attributed
to Unsafe Injection Practices at an Endoscopy
Clinic --- Nevada, 2007 MMWR 5/16/2008

15
84
MMWR 5/2008 continued
85
Highlights of safe injection practice
• Medications should be drawn up in a designated "clean" area
• If a medication vial has already been opened, the rubber septum should be disinfected with alcohol prior to piercing it.
• Never leave a needle or “spikes” inserted into a medication vial septum or IV bag/bottle for multiple uses
• Never administer medications from the same syringe to more than one patient, even if the needle is changed
• Never use bags or bottles of intravenous solution as a common source of supply for more than one patient.
Safe Injection Practices Coalition
www.oneandonlycampaign.org
Nineteen of 67 ASCs that were evaluated
in this study administered injections or
handled medications in an unsafe
manner, primarily through the use of
single-dose vials for more than one
patient.
Infection Control Assessment of
Ambulatory Surgical Centers” and
authored by Melissa K. Schaefer, M.D.
JAMA June , 2010
87
Element IV
• Selection and use of barriers and/or
personal protective equipment for
preventing patient healthcare worker
contact with potentially infectious material.
88
Learning Objectives
• Describe circumstances requiring use of
barriers and PPE to prevent patient or HCW
contact with potentially infectious material
• Identify specific barriers or PPE for patients
and HCW protection from exposure to
potentially infectious material
89
Definitions
• Personal Protective Equipment (PPE)
– Specialized clothing or equipment worn by a
HCW for protection against a hazard
• Barrier
– A material object that separates a person from a
hazard

16
90
Selection Criteria
• Selection of PPE
– Wide variety of PPE available
– Selection of equipment is situation based
– Dependent on type and amount of contact
91
Glove Selection
• Sterile
– Barrier device to reduce transmission of
infection to the patient
– For procedures involving direct contact with
sterile body parts
• Surgery
– For procedures requiring the entry of sterile
devices into sterile areas
• Foley Catheter and Central Line Insertions
92
Glove Selection continued • Non-sterile Gloves for:
– procedures having contact with patient’s body
fluids, mucous membranes or non-intact skin
– decontaminating equipment
– cleaning the environment
– removing medical waste
• Material • latex
• vinyl
• Nitrile
• rubber (utility)
93
Types of PPE/Barriers
Selection Criteria
• Allergies
– Latex allergy in personnel or patients
• Select hypo-allergenic/ non-latex gloves
• Must be made available
– Powder
• Powderless gloves available for powder allergy
• Powderless gloves reduce release of latex into
environment
94
Glove Basics
• Wear for potential contact with
– body fluids or fluid contaminated items
– mucous membranes
– non-intact skin
• Remove immediately after need to wear
• Hand hygiene immediately after removing
• Double gloving for procedures with large quantities of blood
• Don’t wear gloves unnecessarily
– Moist skin: conducive to bacterial growth
• Gloves develop microscopic holes
95
Cover Garb
• Types
– gowns
– aprons
– lab coats
• Characteristics
– impervious: Fluid will not soak through to skin
– fluid resistant: If saturated, fluid can soak
through
– permeable: Protect against small splashes, will
soak through
17
96
When To Wear Cover Garb
• When there is a risk that clothing, arms or legs
may be contaminated with body fluids
• Use impervious gowns when there may be an
exposure to large quantities of body fluid (OR,
Trauma ER)
• Wear a fluid resistant gown when less fluids are
expected (linen removal, dental procedures)
• Wear a lab coat when minimal exposure is
expected (drawing blood)
• Wear a sterile gown during to protect the patient
during procedures 97
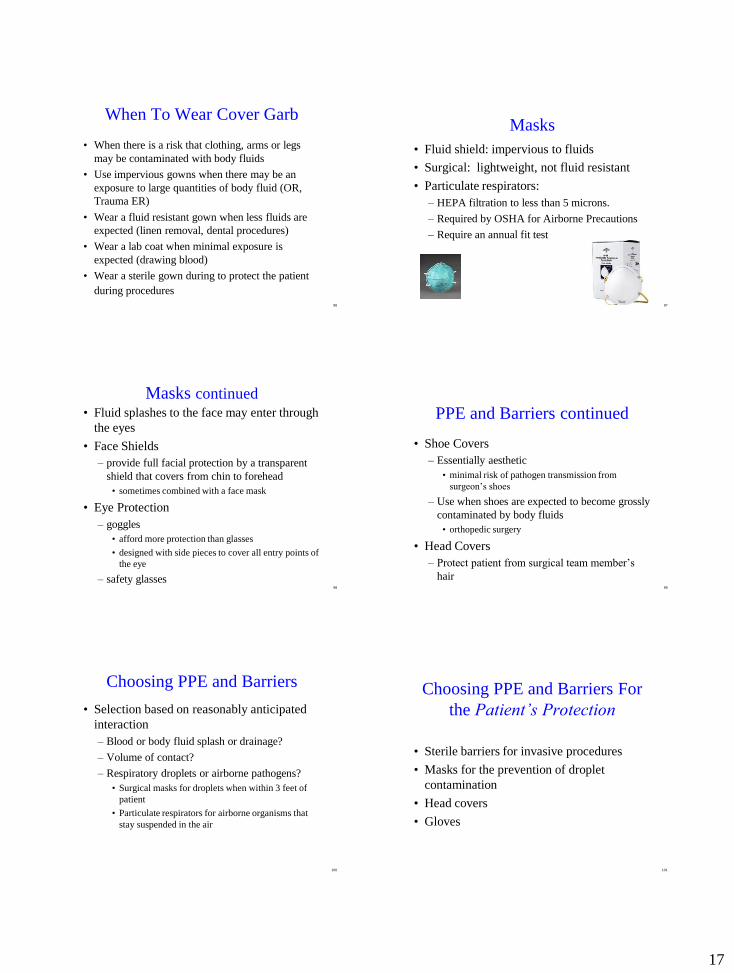
Masks
• Fluid shield: impervious to fluids
• Surgical: lightweight, not fluid resistant
• Particulate respirators:
– HEPA filtration to less than 5 microns.
– Required by OSHA for Airborne Precautions
– Require an annual fit test
98
Masks continued
• Fluid splashes to the face may enter through
the eyes
• Face Shields
– provide full facial protection by a transparent
shield that covers from chin to forehead
• sometimes combined with a face mask
• Eye Protection
– goggles
• afford more protection than glasses
• designed with side pieces to cover all entry points of
the eye
– safety glasses
99
PPE and Barriers continued
• Shoe Covers
– Essentially aesthetic
• minimal risk of pathogen transmission from
surgeon’s shoes
– Use when shoes are expected to become grossly
contaminated by body fluids
• orthopedic surgery
• Head Covers
– Protect patient from surgical team member’s
hair
100
Choosing PPE and Barriers
• Selection based on reasonably anticipated
interaction
– Blood or body fluid splash or drainage?
– Volume of contact?
– Respiratory droplets or airborne pathogens?
• Surgical masks for droplets when within 3 feet of
patient
• Particulate respirators for airborne organisms that
stay suspended in the air
101
Choosing PPE and Barriers For
the Patient’s Protection
• Sterile barriers for invasive procedures
• Masks for the prevention of droplet
contamination
• Head covers
• Gloves

18
102
Element V
• Creation and maintenance of a safe
environment for patient care through
application of infection control principles
and practices for cleaning, disinfection, and
sterilization
103
Learning Objectives
• Recognize importance of correct application
of reprocessing methods for assuring the
safety and integrity patient care equipment
• Identify the individual’s professional
responsibility for maintaining a safe patient
care environment
• Recognize strategies for effective pre-
cleaning, chemical disinfection and
sterilization of instruments and devices
104
Definitions
• Contamination
– The presence of microorganisms on inanimate objects (surgical
instruments) or in substances (water, food, milk)
• Cleaning
– The removal of all foreign material (dirt, fluids, organic debris)
from objects
• Decontamination
– Process of removing disease-producing microorganisms and
rendering the object safe for handling
• Disinfection
– Process that results in the elimination of many or all pathogenic
microorganisms on inanimate objects with the exception of
bacterial endospores
105
Definitions continued
Sterilization – Process that completely eliminates or destroys all forms of microbial life
High Level Disinfection – Kills bacteria, mycobacteria (TB), fungi, viruses and some bacterial
spores.
Intermediate Level Disinfection – Kills bacteria, mycobacteria (TB), most fungi and most viruses. Does not
kill resistant bacterial spores.
Low Level Disinfection – Kills most bacteria, some fungi and some viruses.
– Will not kill bacterial spores, MTb, and is less active against some gram
negative rods (pseudomonas)
106
Potential For Contamination
• Degree of frequency of hand contact
• Potential for contamination with body
substances or environmental sources of
microorganisms
• Level of contamination
– Types of microorganisms
– Number of microorganisms
• Potential for cross-contamination
107
Potential For Contamination
• Type of device, equipment or
environmental surface
– External contamination
• surface
– Internal contamination
• channels
– Composition of the device, equipment,
environmental surface being contaminated
• Manufacturer’s recommendations

19
108
Contributing Factors to
Contamination
• Inadequate cleaning
– most important step in disinfection or
sterilization
– Physically eliminates many microbes
– Organic matter prevents surface exposure to
disinfectant or sterilant
– Residual detergent may inactivate disinfectant
or sterilant: rinse well
109
Contributing Factors to
Contamination cont.
• Contamination of disinfectant or rinse
solutions
• Improper storage and handling
• Failure to reprocess or dispose of equipment
between patients
• FDA reprocessing standards for single use
devices (SUDs)
110
Efficacy of Disinfection/Sterilization
Influencing Factors
• Cleaning of the object
• Organic and inorganic load present
• Type and level of microbial contamination
• Concentration of and exposure time to
disinfectant/sterilant used
• Nature of object
• Temperature and relative humidity
111
Reprocessing Points That Can Compromise
Equipment/Device Integrity
• Handling and cleaning contaminated items
– internal and external surfaces
• endoscopy equipment
– right chemical or process
– timing
• right amount of time
• rinse/pre-soak
– immediate transport for reprocessing
112
Cleaning Methods
• Manual
– Soaking (i.e.: Glutaraldehyde, OPA)
• Mechanical (Automated)
– Reduces employee contact with potentially
infectious material or equipment
• Washer-sterilizer: Item immersed and agitated
in detergent bath. Usually put through a steam heat
cycle to sterilize.
• Ultrasonic cleaner: Sonic waves produce tiny
bubbles from gas nuclei. Imploding bubbles
dissolve organic material from equipment surface.
113
EH Spaulding’s Principles
• How an object will be disinfected depends on the object’s intended use.
• Critical – Objects which enter normally sterile tissue or the vascular system
or through which blood flows should be sterile
• Semicritical – Objects that touch mucous membranes or skin that is
not intact require high level disinfection
• Noncritical – Objects that touch only intact skin require low level disinfection
20
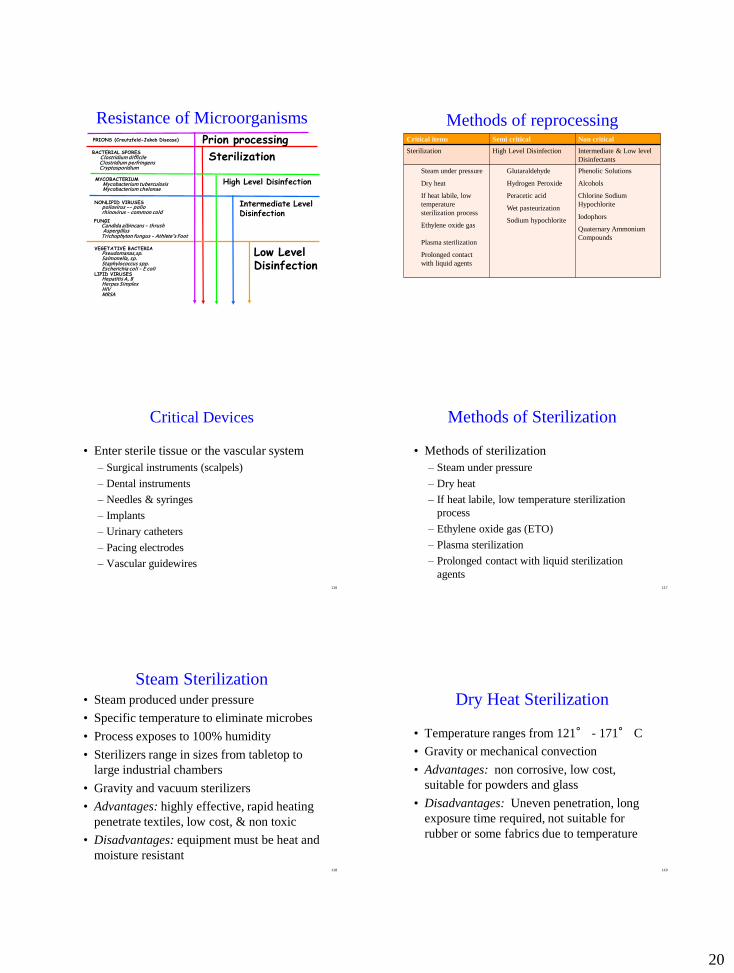
Resistance of Microorganisms
Low Level Disinfection
LIPID VIRUSES Hepatitis A, B Herpes Simplex HIV
High Level Disinfection
Intermediate Level Disinfection
BACTERIAL SPORES Clostridium difficile Clostridium perfringens Cryptosporidium
MYCOBACTERIUM Mycobacterium tuberculosis Mycobacterium chelonae
NONLIPID VIRUSES poliovirus -- polio rhinovirus – common cold
FUNGI Candida albincans – thrush Aspergillus Trichophyton fungus – Athlete’s Foot
VEGETATIVE BACTERIA Pseudomanas,sp. Salmonella, sp. Staphylococcus spp. Escherichia coli – E coli MRSA
Sterilization
PRIONS (Creutzfeld-Jakob Disease) Prion processing Critical items Semi critical Non critical
Sterilization High Level Disinfection Intermediate & Low level
Disinfectants
Steam under pressure
Dry heat
If heat labile, low
temperature
sterilization process
Ethylene oxide gas
Plasma sterilization
Prolonged contact
with liquid agents
Glutaraldehyde
Hydrogen Peroxide
Peracetic acid
Wet pasteurization
Sodium hypochlorite
Phenolic Solutions
Alcohols
Chlorine Sodium
Hypochlorite
Iodophors
Quaternary Ammonium
Compounds
Methods of reprocessing
116
Critical Devices
• Enter sterile tissue or the vascular system
– Surgical instruments (scalpels)
– Dental instruments
– Needles & syringes
– Implants
– Urinary catheters
– Pacing electrodes
– Vascular guidewires
117
Methods of Sterilization
• Methods of sterilization
– Steam under pressure
– Dry heat
– If heat labile, low temperature sterilization
process
– Ethylene oxide gas (ETO)
– Plasma sterilization
– Prolonged contact with liquid sterilization
agents
118
Steam Sterilization • Steam produced under pressure
• Specific temperature to eliminate microbes
• Process exposes to 100% humidity
• Sterilizers range in sizes from tabletop to
large industrial chambers
• Gravity and vacuum sterilizers
• Advantages: highly effective, rapid heating
penetrate textiles, low cost, & non toxic
• Disadvantages: equipment must be heat and
moisture resistant
119
Dry Heat Sterilization
• Temperature ranges from 121° - 171° C
• Gravity or mechanical convection
• Advantages: non corrosive, low cost,
suitable for powders and glass
• Disadvantages: Uneven penetration, long
exposure time required, not suitable for
rubber or some fabrics due to temperature

21
120
Plasma Sterilization
• Gas plasma created in vacuum chamber through
radio waves and hydrogen peroxide
• Free elements generated that eliminate all
microorganisms and spores
• Marketed as STERRAD by J&J
• Advantages: highly sporicidal, non corrosive,
good for heat and moisture resistant items
• Disadvantages: Requires special packing
material, doesn’t penetrate foreign material,
unable to enter small and long lumens
121
Ethylene Oxide Gas
• Chamber filled with Ethylene Oxide (ETO)
• Gas inhibits microorganism’s metabolism
• Must comply with EPA standards for safe
exhaust of gas
• Advantages: Very effective, safe for heat
sensitive items
• Disadvantages: Toxic gas, special
ventilation required
122
Peracetic Acid (Cidex PA)
• Submerge instruments in peracetic acid liquid or
in a computerized processing unit
• Connectors direct fluid through lumens Marked as
Steris system by Steris
• Advantages: rapid cycle, fully automated,
decomposes into water, hydrogen peroxide and
acetic acid, effective in presence of organic matter,
can be used without Steris
• Disadvantages: For immersible items only,
inactivated by blood, unstable when diluted,
corrosive
123
Ortho-phthaladehyde (Cidex-OPA )
• Liquid disinfectant/sterilant
• Advantages: 12 – 20 minute process, no
activation, not a known irritant to eyes or
nasal passages, no special ventilation
• Disadvantages: Cost, stains protein gray
(including skin)
124
Glutaraldehyde (Cidex)
• Excellent high level disinfectant /sterilant
• Advantages: Active in the presence of
organic matter, compatible with lensed
instruments
• Disadvantages: Toxic and caustic, requires
copious rinsing, requires special ventilation
125
Hydrogen Peroxide
• Can be used to achieve disinfection or
sterilization
• Environmentally friendly
• Advantages: Decomposes into hydrogen
and water
• Disadvantages: Oxidizing may be harmful
to scopes, copious rinsing required

22
126
Semi-Critical Devices
• Touches mucous membranes or non-intact skin
• Require cleaning and high level disinfection
• Use for: – Vaginal sonography probes
– Diaphragm fitting rings
– Flexible endoscopes
– Themometers
– Tonometers
– Laryngoscopes
– Anesthesia/respiratory equipment
127
Methods of Reprocessing
Semi-Critical Items
• High Level Disinfection (HLD)
– Glutaraldehyde
– Hydrogen Peroxide
– Peracetic acid
– Wet pasteurization (HLD with hot water)
• anesthesia/respiratory equipment
– Sodium hypochlorite (household bleach)
128
Non-Critical Devices
• Touch intact skin
• Require cleaning and low level disinfection
• Examples: – BP cuffs
– Stethescopes
– EKG leads
– Crutches
– Furniture
– Mattresses
– Walls
– Floors
The Inanimate Environment
Can Facilitate Transmission
Green X’s show areas of contamination in a patient’s room
Pathogen HCW Hand
Contamination
Persistence
(Hands)
Persistence
(Environmental)
Acinetobacter 3-15 % >150 min 3 days-5 mo
C. difficile 14-59 % ? 24 h (vegetative
cells), up to 5 mo
(spores)
Klebsiella spp. 17% 2 h 2 h-30 mo
MRSA Up to 16.9 % ? 4 wk-7 mo
(* 1 yr in dust)
VRE Up to 41% 60 min 5 days-4 mo
Adapted from Kampf G, Kramer A. Clinical Microbiology Reviews (2004) 17:863-893
*JH Wagenvoort, W Sluijsmans, RJ Penders, Better environmental survival of outbreak
vs sporadic MRSA isolates. , J Hosp Infect 45 (2000), pp. 231–234
131
Intermediate & Low level
Disinfectants
Alcohol
– Requires wet contact for 5 minutes
– Evaporation may diminish disinfection
– Flammable
– Inactivated by organic matter
– Damaging to lensed instruments
– Uses: thermometers, external surfaces of
equipment, skin antisepsis
23
132
Intermediate & Low level
Disinfectants
Chlorine Sodium Hypochlorite
• Must dilute to be effective
– Dilution determines level of disinfection
• Corrosive to metals
• Cannot combine with detergents
• Inactivated by organic matter
• Uses: disinfect dialysis equipment, hydrotherapy tanks,
CPR mannequins, toilets, blood spills
133
Intermediate & Low level
Disinfectants
Iodophors (Iodine Based)
• Relatively non-toxic and non-irritating
• Excellent detergent action
• May stain fabrics, plastic an other synthetics
• Inactivated by organic material
• Not suitable for hard surface disinfection
• Uses: Disinfect thermometers, hydrotherapy tanks
134
Intermediate & Low level
Disinfectants
Phenolic Solutions
• Leave residue film on environmental surfaces
• May cause skin irritation
• Affected by organic matter
• Corrosive to rubber and plastic
• Never use in a nursery setting
– Cause hyperbilrubinemia
• Uses: environmental cleaning
135
Low level Disinfectants
Quaternary Ammonium Compounds
• Good detergents
• Good germicides
• Affected by organic matter
• Uses: environmental cleaning (floors, walls,
furniture)
136
Reprocessing Summary
• Choose reprocessing method based on:
– Desired level of antimicrobial activity
• High, intermediate or low
– Manufacturer’s recommendations
• Heat/pressure/temperature tolerance, time
– Effectiveness of process
• Surface, channels, immersible, stability of product
137
Sterilization Process Summary
• Selection and use of sterilization methods
– compatibility with equipment components and
materials
– heat and pressure tolerance
– time requirements for reprocessing
– temperature requirements for reprocessing

24
138
Process Monitoring
• Monitoring the sterilization process
– biologic monitors
– indicator strips
– pressure, temperature gauges
• Post-sterilization handling and storage
– package integrity
– shelf-life or event related sterility criteria
139
Event Related Sterility
• Based on concept that specific events, not
time, causes contamination
• Event is an incident that compromises
package integrity
– wetness
– holes or tears
– dropped on floor
– improperly transported
– improperly stored
140
Storing Sterile Items
• Limited access areas
• Closed cabinets
• Clean, dry and dust free
• 65° - 72° degrees F
• Relative humidity of 35 – 50 %
• 18 - 20 inches below ceiling
• 6 - 2 inches from walls
141
Equipment Users
• Must Know:
– Basic concepts and principles of cleaning,
disinfection and sterilization
– Appropriate application of safe practices for
handling devices and equipment
142
Reprocessing Managers/Workers
• Must Know:
– Core concepts of cleaning, disinfection and sterilization
– Appropriate application of safe practices for handling devices and equipment
– Residual Effect/Toxicity
– Antibacterial residual
– Staff/patient toxicity
– Monitoring exposures
– Abatement procedures
– Ease of Use
– Need for special equipment
– Training requirements
– FDA rules for reuse of SUDs
– Cost
143
Element VI
• Prevention and management of infectious or
communicable diseases in healthcare
workers
• 5/2010 – OSHA issued RFI re: workpalce
exposure to air, droplet contact routes – all
HC settings
25
144
Learning Objectives
• Recognize the role of occupational health
strategies in protecting healthcare workers and
patients
• Recognize non-specific disease findings which
should prompt evaluation of healthcare workers
• Identify strategies for preventing BBP and other
communicable diseases in HCWs
• Identify resources for evaluation of HCWs
infected with HIV, HBV, and/or HCV
145
Definitions
• Infectious Disease
– A clinically manifest disease of
man resulting from infection
• Communicable Disease
– An illness due to a specific infectious agent
which arises through transmission of that agent
from an infected person, animal, or inanimate
reservoir to a susceptible host
• Occupational Health Strategies
– A set of activities intended to assess, prevent,
and control infections
146
Pre-Employment & Periodic
Health Assessments
• Prevent the HCW from transmitting
diseases to patients and co-workers
• Protect HCWs from acquiring
communicable diseases at work
• Annual health assessments
• Follow-up for potential communicable
diseases
147
Immunization/Screening Program
• Rubella
• Measles
• Varicella
• Hepatitis B
• Influenza
• Any other additional/mandated
requirements - Pertussis
148
Recommended Immunizations
• Recommended Adult Immunization Schedule---United States
• Mandated immunizations for school
• Foreign born HCWs
• If immunization or serologic evidence of immunity cannot be established, vaccination for these diseases is strongly recommended
149
Boosters
• Tetanus
– 0.5 ml every 10 years
• Diphtheria and Polio boosters
– recommended for travel where diseases prevail
• Pertussis
– Tdap

26
In 2010, 9,143 cases of pertussis (including ten infant deaths) were
reported throughout California. This is the most cases reported in
63 years when 9,394 cases were reported in 1947.
In Michigan, an increase in pertussis was first observed in 2008. In
2010 there were 1,564 cases. In 2009 there were 902 cases reported.
In 2008 there were 315 cases reported.
In Ohio, in 2010, there were 964 cases reported by Columbus and
Franklin Counties. This is the most cases reported in 25 years.
Outbreaks of pertussis-not uncommon
• The ACIP recommends that all healthcare personnel
(HCP), regardless of age, should receive a single dose of
Tdap as soon as feasible if they have not previously
received Tdap and regardless of the time since last Td
dose.•
• Hospitals and ambulatory-care facilities should provide
Tdap for HCP and use approaches that maximize
vaccination rates (e.g., education about the benefits of
vaccination, convenient access, and the provision of Tdap
at no charge).
Tdap in healthcare personnel
January 27, 2010
CONFIRMED CASE OF MEASLES IN
NASSAU COUNTY Uniondale, NY
The Nassau County Department of Health today
announced that a case of measles has been
confirmed in a 12 month old child who resides in
Nassau County. The child recently traveled
internationally to a location with known measles
152
www.nassaucountyny.gov/agencies/Health/NewsRelease/2010/01272010.html
153
Hepatitis B Vaccine
• OSHA Bloodborne Pathogen Standard
requires:
– Offering to HCWs at no charge
– For employees at risk for exposures to blood
and body fluids which may contain blood
– If refused, employee must sign a statement
acknowledging potential consequences
– Employees may request vaccination at future
date during employment
154
Influenza
• Up to 20 % or more of the population becomes infected with the flu each season
• Viral shedding occurs before symptoms
• Some people are so mildly sick they don’t realize they are sharing their flu virus
• Prevention and Control of Seasonal Influenza with Vaccines – MMWR Recommendations and Reports

27
Cumulative percentages of health-care personnel* who
received seasonal influenza vaccine, influenza A (H1N1)
2009 monovalent vaccine, or both United States, August 2009--January 2010†
Fundamental Elements to Prevent Influenza
Transmission
• administration of influenza vaccine
• implementation of respiratory hygiene and cough
etiquette
• appropriate management of ill HCP
• adherence to infection control precautions
– Standard precautions for all patient-care activities
– Droplet – separate patient & HCP use mask
– Upgrade for aerosol-generating procedures
• implementing environmental and engineering
infection control measures
2010-11 Influenza Prevention & Control Recommendations
• All persons aged 6 months and older should be vaccinated annually
If limited supply, vaccination efforts should focus on :
• aged 6 months--4 years (59 months)
• aged 50 years and older
• have chronic pulmonary (including asthma), cardiovascular (except hypertension), renal,
hepatic, neurologic, hematologic, or metabolic disorders (including diabetes mellitus);
• immunosuppressed (medications or by human immunodeficiency virus)
• will be pregnant during the influenza season
• aged 6 months--18 years and receiving long-term aspirin therapy and who therefore might be
at risk for experiencing Reye syndrome after influenza virus infection;
• residents of nursing homes and other chronic-care facilities;
• American Indians/Alaska Natives
• morbidly obese
• health-care personnel
• household contacts and caregivers of – children aged younger than 5 years, esp. younger than 6 months NYS requirement to offer vaccine to caregivers of
NICU babies
– adults aged 50 years and older, with particular emphasis on vaccinating contacts of children aged younger than 6
months
– persons with medical conditions that put them at higher risk for severe complications from influenza.
161
28
162
Varicella Vaccine
• Prevention of Varicella
– MMWR June 22, 2007/ Vol.56/ No. RR-4.
– Recommendations of the Advisory Committee on Immunization
Practices (ACIP) 2007
• Available for children and adults in the USA
• Varicella titers drawn for those who are unsure of
history
• If susceptible to varicella, the vaccine should be
offered
• HCWs refusing immunization sign
acknowledgment of potential consequences
• Re-offered an annual physical exam 163
Tuberculosis Screening
• QuantiFeron Gold: blood test
• 2 step TST (PPD) placed at time of hire
• Annual screening thereafter
• Semi-annual screening for high risk employees
• Exposures referred for follow-up
• TST conversions tracked and trended annually
• Positive TST HCWs screened for signs and
symptoms of active disease: bloody sputum,
weight loss, night sweats
164
Symptoms Requiring Immediate
Medical Evaluation
• Fever
• Cough
• Rash
• Vesicular lesions
• Draining wounds
• Vomiting
• Diarrhea
165
Management of Exposures
• Prompt evaluation and treatment as needed
• Limiting contact with susceptibles
• Furlough until non-infectious
• Prophylaxis if indicated
166
Exposure Prophylaxis
• Diphtheria: Contact with respiratory
secretions
– Penicillin, Erythromycin, Td vaccine
• Hepatitis A: Contact with feces
– Immune globulin within 2 weeks
• Hepatitis B: Contact with infected blood
or body fluid via needlestick, splash to eyes,
non-intact skin, or mucous membrane
– Hepatitis B Immune Globulin
– Hepatitis B Vaccine
167
Hepatitis B
• 6 -30% risk of seroconversion
• Conversion risk influenced by source’s viral
titer
• Correlation with presence of hepatitis B
antigen
• 10% HBV infections become chronic
• CDC prophylaxis recommendations based
on exposed persons immunization status
– Detailed CDC recommendation

29
168
Hepatitis C
• 1 - 10 % seroconversion rate post exposure
• Estimated 4 million Americans infected
• 60 -70 % have no symptoms
• 80 % develop chronic liver disease
• No recommended post-exposure treatment
• Following exposure, HCWs should be
tested for HCV antibodies (anti-HCV) or
PCR at baseline, 4 weeks, 6 and 12 months
• Source patient should be tested if possible
169
HIV
• 0.3% risk of seroconversion from needlestick
• 0.09% risk from mucous membrane exposure
• Old data
– 56 HCWs infections since 1985
– 138 “possible” occupational transmissions
• Percutaneous injury associated with 89%
transmissions
170
HIV PEP
• NYS guidelines more aggressive than CDC
• Maximally suppress any limited viral
replication with HAART
– Highly active anti-retroviral therapy
• Assess exposure within 2 hours
– percutaneous exposure
– bite with blood in source’s mouth
– splash to mucous membrane or non-intact skin
– source patient’s HIV status or risk factors
– confidential consented HIV testing of source
171
HIV PEP cont.
• Initiate Pep within 2 hours of exposure, no
longer than 36 hours
• HAART (2 nucleoside analogues with
either a PI or NNRTI) for four weeks
• Baseline CBC, liver enzymes, Hep B & C
serologies
• Confidential HIV baseline within 72 hours
and at 6, 12 and 26 (52 weeks option)
172
BBP Source is a HCW
• Professional obligation to inform patients or
other HCWs
• Post exposure management must be offered
to exposed
• Evaluation of HCWs compliance with IC
Standards
• Assessment of HCWs physical health status
and cognitive function
• Ethical panel for evaluation when needed
www.cdc.gov/HAI/settings/outpatient/checklist/outpat
ient-care-checklist-observations.html
Ten point checklist
1. Hand hygiene
2. Use of PPE
3. Injection safety
4. Point of care testing
5. Environmental cleaning
6. Reprocessing of instruments
7. Sterilization of instruments
8. High level disinfection of
instruments
9. Policies
10.Training

30
Hope You Learned Something
New Today
Special thanks to my colleague- Robin Haag
Barbara A. Smith [email protected]
Resources
• APIC www.apic.org
• CDC www.cdc.gov
• Institute for Healthcare Improvement www.ihi.org
• SHEA www.shea-online.org
• TJC www.jointcommission.org
• AHRQ www.ahrq.gov
• CMS Hospitalcompare.hhs.gov
• New York State - search for HAI report
• ADVANCE http://nursing.advanceweb.com
– Look for infection control center
• Articles, references, blogs and quizzes
• Barbara A. Smith, [email protected]