elearning.rcog.org.uk in... · ManagementofCancerDuringPregnancy Donald C. Doll, MD; Q. Scott...
7
Management of Cancer During Pregnancy Donald C. Doll, MD; Q. Scott Ringenberg, MD; John W. Yarbro, MD, PhD \s=b\ Although cancer during pregnancy is Infrequent, its man- agement is difficult for patients, their families, and their physicians. When termination of the pregnancy is unaccept- able, decisions regarding the use of Irradiation and chemo- therapy are complicated by the well-known high risks of abortion and fetal malformation. This risk is concentrated in the first trimester and varies with the choice of chemothera- peutic agents or combinations of agents. There is only minimal evidence of increased risk of malformation or abortion in the second or third trimester. Recent progress in cancer therapy has made cure a reasonable goal, and for some malignant neoplasms, cure is still possible even when initial therapy is modified or delayed. When cure is a reasonable goal, curative therapy should not be compromised by modification or delay. When treatment for cure or significant palliation is not possi- ble, however, the goal should shift to protection of the fetus from damage by the injudicious use of teratogenic cancer therapy. This report will review the available data that may assist in these difficult decisions. (Arch Intern Med 1988;148:2058-2064) fiancer is a leading cause of death in women of childbear- ^ ing age,1 but its simultaneous occurrence with preg¬ nancy is uncommon, with a reported incidence of 0.07% to 0.1%.2·3 The malignant neoplasms complicating pregnancy are those most frequently seen in young women: lym¬ phoma, leukemia, melanoma, and cancers of the breast, cervix, ovary, thyroid, and colon.4-7 There is no evidence of an increased incidence of malignant neoplasms in pregnant patients. In the past, pregnancy has been thought to have a deleterious effect on some cancers, but except for delay in diagnosis, no convincing data exist that pregnancy per se adversely influences the prognosis or biology of maternal cancer, including breast cancer. No firm data exist that there is a greater likelihood of reactivation of cancer during pregnancy. Conversely, there are only a few reports indi¬ cating that cancer per se adversely affects pregnancy. Metastasis to the placenta and fetus is rare, with 44 cases reported and only 12 infants with cancer at birth (seven melanoma, two leukemia, two lymphoma, and one ethmoid carcinoma); two with melanoma had regressions, and the other infants died.8·9 The immediate and delayed effects of diagnostic and therapeutic interventions, however, are potentially deleterious to the fetus and mother. It is well established that irradiation and cytotoxic drugs during pregnancy are associated with a significant risk of abortion and teratogenesis. Similarly, delay or modification of cancer therapy to ensure the birth of a healthy infant may adversely affect maternal prognosis. Hence, the deci¬ sion to initiate therapy in a pregnant patient is usually a difficult one for all concerned and may be complicated by heightened emotions, ethical issues, and religious beliefs. Accepted for publication March 30, 1988. From the Division of Hematology/Medical Oncology, Department of Medicine, Harry S Truman Memorial Veterans Hospital (Dr Doll) and the University of Missouri\p=m-\Columbia (Drs Doll, Ringenberg, and Yarbro). Reprint requests to Department of Medicine, Harry S Truman Memorial Veterans Hospital, Columbia, MO 65201 (Dr Doll). This article discusses the effects of cancer diagnosis and treatment on the fetus and makes recommendations re¬ garding management. DRUG METABOLISM DURING PREGNANCY Drug metabolism is altered by the physiologic changes of pregnancy. The stomach empties more slowly,1011 which may affect the rate of drug absorption. Plasma volume increases by approximately 50%,12 resulting in a larger space for drug dilution. Albumin concentration decreases while plasma protein levels increase, which alters plasma unbound drug concentration.13 Hepatic oxidation by the mixed function oxidase system is enhanced and renal plasma flow and glomerular filtration rate are increased.14 Changes in drug distribution volume, peak drug concen¬ tration, renal and hepatic excretion, and half-life alter the concentration and time relationship that is so important for chemotherapeutic drugs.15 The possibility exists that these changes alter the efficacy of cancer chemotherapy regimens, although there are no data on this question (to our knowledge). Whether the amniotic fluid functions as a pharmacologie third space is not reported, but this would be especially relevant to methotrexate, where distribution into a third space such as ascitic fluid or pleural effusion delays elimination and increases toxicity.16 Drug characteristics that enhance entry into the fetus across the placenta are low molecular weight, high lipid solubility, nonionization, and loose binding to plasma pro¬ tein.1314 Multiple drugs, including most antineoplastic agents, possess these qualities. The immature fetal liver and kidney are functional to a variable degree as the fetus develops, and chemotherapeutic agents may be excreted via bile and urine. Since the fetus ingests amniotic fluid, agents excreted in active form may have their activity enhanced. ADVERSE EFFECTS OF ANTINEOPLASTIC AGENTS ON THE FETUS AND NEONATE The timing of exposure to cytotoxic agents is critical, since their effects are different during each trimester. During the first trimester, when organogénesis occurs, drugs can produce congenital malformation or abortion.17 After the first trimester, drugs rarely cause congenital malformations but can impair fetal growth and functional development, particularly that of the brain. The back¬ ground incidence of major congenital malformations is about 3% of all births,18 and radiation treatment and chemotherapeutic drugs increase this incidence. The ter¬ atogenic and mutagenic potentials of chemotherapeutic agents have been clearly demonstrated in animals,19-21 but extrapolation to humans is tenuous.22 Many drugs that produce defects in animals seem to be harmless to the human embryo, eg, aspirin. Conversely, the absence of teratogenicity in animals is no guarantee of safety in humans, eg, thalidomide. The probability of teratogenesis is influenced by the trimester of exposure, drug dose, frequency of administra¬ tion, and duration of treatment. To be teratogenic it seems on May 7, 2010 www.archinternmed.com Downloaded from
Transcript of elearning.rcog.org.uk in... · ManagementofCancerDuringPregnancy Donald C. Doll, MD; Q. Scott...

Management of Cancer During PregnancyDonald C. Doll, MD; Q. Scott Ringenberg, MD; John W. Yarbro, MD, PhD
\s=b\Although cancer during pregnancy is Infrequent, its man-agement is difficult for patients, their families, and theirphysicians. When termination of the pregnancy is unaccept-able, decisions regarding the use of Irradiation and chemo-therapy are complicated by the well-known high risks ofabortion and fetal malformation. This risk is concentrated inthe first trimester and varies with the choice of chemothera-peutic agents or combinations of agents. There is only minimalevidence of increased risk of malformation or abortion in thesecond or third trimester. Recent progress in cancer therapyhas made cure a reasonable goal, and for some malignantneoplasms, cure is still possible even when initial therapy ismodified or delayed. When cure is a reasonable goal, curativetherapy should not be compromised by modification or delay.When treatment for cure or significant palliation is not possi-ble, however, the goal should shift to protection of the fetusfrom damage by the injudicious use of teratogenic cancer
therapy. This report will review the available data that mayassist in these difficult decisions.
(Arch Intern Med 1988;148:2058-2064)
fiancer is a leading cause of death in women of childbear-^ ing age,1 but its simultaneous occurrence with preg¬nancy is uncommon, with a reported incidence of 0.07% to0.1%.2·3 The malignant neoplasms complicating pregnancyare those most frequently seen in young women: lym¬phoma, leukemia, melanoma, and cancers of the breast,cervix, ovary, thyroid, and colon.4-7 There is no evidence ofan increased incidence of malignant neoplasms in pregnantpatients. In the past, pregnancy has been thought to havea deleterious effect on some cancers, but except for delayin diagnosis, no convincing data exist that pregnancy perse adversely influences the prognosis or biology of maternalcancer, including breast cancer. No firm data exist thatthere is a greater likelihood of reactivation of cancer duringpregnancy. Conversely, there are only a few reports indi¬cating that cancer per se adversely affects pregnancy.Metastasis to the placenta and fetus is rare, with 44 cases
reported and only 12 infants with cancer at birth (sevenmelanoma, two leukemia, two lymphoma, and one ethmoidcarcinoma); two with melanoma had regressions, and theother infants died.8·9 The immediate and delayed effects ofdiagnostic and therapeutic interventions, however, are
potentially deleterious to the fetus and mother.It is well established that irradiation and cytotoxic drugs
during pregnancy are associated with a significant risk ofabortion and teratogenesis. Similarly, delay or modificationof cancer therapy to ensure the birth of a healthy infantmay adversely affect maternal prognosis. Hence, the deci¬sion to initiate therapy in a pregnant patient is usually adifficult one for all concerned and may be complicated byheightened emotions, ethical issues, and religious beliefs.
Accepted for publication March 30, 1988.From the Division of Hematology/Medical Oncology, Department of
Medicine, Harry S Truman Memorial Veterans Hospital (Dr Doll) and theUniversity of Missouri\p=m-\Columbia(Drs Doll, Ringenberg, and Yarbro).
Reprint requests to Department of Medicine, Harry S Truman MemorialVeterans Hospital, Columbia, MO 65201 (Dr Doll).
This article discusses the effects of cancer diagnosis andtreatment on the fetus and makes recommendations re¬
garding management.DRUG METABOLISM DURING PREGNANCY
Drug metabolism is altered by the physiologic changesof pregnancy. The stomach empties more slowly,1011 whichmay affect the rate of drug absorption. Plasma volumeincreases by approximately 50%,12 resulting in a largerspace for drug dilution. Albumin concentration decreaseswhile plasma protein levels increase, which alters plasmaunbound drug concentration.13 Hepatic oxidation by themixed function oxidase system is enhanced and renalplasma flow and glomerular filtration rate are increased.14Changes in drug distribution volume, peak drug concen¬
tration, renal and hepatic excretion, and half-life alter theconcentration and time relationship that is so importantfor chemotherapeutic drugs.15 The possibility exists thatthese changes alter the efficacy of cancer chemotherapyregimens, although there are no data on this question (toour knowledge). Whether the amniotic fluid functions as a
pharmacologie third space is not reported, but this wouldbe especially relevant to methotrexate, where distributioninto a third space such as ascitic fluid or pleural effusiondelays elimination and increases toxicity.16
Drug characteristics that enhance entry into the fetusacross the placenta are low molecular weight, high lipidsolubility, nonionization, and loose binding to plasma pro¬tein.1314 Multiple drugs, including most antineoplasticagents, possess these qualities. The immature fetal liverand kidney are functional to a variable degree as the fetusdevelops, and chemotherapeutic agents may be excretedvia bile and urine. Since the fetus ingests amniotic fluid,agents excreted in active form may have their activityenhanced.
ADVERSE EFFECTS OF ANTINEOPLASTICAGENTS ON THE FETUS AND NEONATE
The timing of exposure to cytotoxic agents is critical,since their effects are different during each trimester.During the first trimester, when organogénesis occurs,drugs can produce congenital malformation or abortion.17After the first trimester, drugs rarely cause congenitalmalformations but can impair fetal growth and functionaldevelopment, particularly that of the brain. The back¬ground incidence of major congenital malformations isabout 3% of all births,18 and radiation treatment andchemotherapeutic drugs increase this incidence. The ter¬atogenic and mutagenic potentials of chemotherapeuticagents have been clearly demonstrated in animals,19-21 butextrapolation to humans is tenuous.22 Many drugs thatproduce defects in animals seem to be harmless to thehuman embryo, eg, aspirin. Conversely, the absence ofteratogenicity in animals is no guarantee of safety inhumans, eg, thalidomide.
The probability of teratogenesis is influenced by thetrimester of exposure, drug dose, frequency of administra¬tion, and duration of treatment. To be teratogenic it seems
on May 7, 2010 www.archinternmed.comDownloaded from

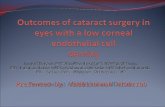
Table 1.—Chemotherapy During First Trimester of Pregnancy
Class
No. ofExposed Patients/
No. ofFetal Malformations Reference No.
Alkylating agentsBusulfanChlorambucilCyclophosphamideMechlorethamine
hydrochlorideTriethylenemelamineTotal (%)
AntimetabolitesAminopterinMethotrexateMercaptopurineCytarabineFluorouracilTotal (%)
Plant alkaloidsVinblastine
sulfateAntibiotics
Daunorubicinhydrochloride
MiscellaneousProcarbazine
hydrochlorideAmsacrineCisplatinTotal (%)
TotalCombinations (%)
22/25/17/3
6/04/0
44/6 (14)
52/103/3
20/01/11/1
77/15 (19)
14/1
1/0
1/11/11/0
18/3 (17)139/24 (17)30/7 (23)
30,32,34-3849-52,9330,32,53,54,94
30,32,52,56-5812,30,59,60
30,32,61-69,72-7470-72
30-32,73-818485
25,30,32,86-89
90
913192
25,96-109
that the required drug dose lies within a narrow rangebetween that which causes death of the fetus and thatwhich has no discernible effect.23 Synergistic teratogenicinteractions may occur with combination chemotherapy,24·25different drugs given sequentially,25·26 and the combinationof chemotherapy and radiotherapy.26-28 Individual and ge¬netic susceptibility may be important but have not beenclearly defined.19
There are many reports of chemotherapy during preg¬nancy.2494 Table 1 shows drug-associated fetal malforma¬tions during the first trimester. In several reported cases,the mothers were also treated with radiation,26·27·53·85 whichis well recognized as a potent teratogen.95 The apparentrate of fetal malformation from combinations of drugs96-109is only slightly higher than that observed with singleagents: six (25%) of 24 cases vs 24 (17%) of 139 cases. Ifone excludes the folate antagonists and those cases involv¬ing the concomitant use of irradiation, however, the inci¬dence for single agents declines to 6%.
In contrast, no evidence of an increased risk of terato-genicity in the second and third trimesters exists (Table2).* In 110 cases, one report of trisomy C was notedfollowing cytarabine and thioguanine administration,126 oneinfant had multiple anomalies following third-trimesterexposure to busulfan,126 and one neonate had adherence ofthe iris to the cornea after combination chemotherapy inthe last trimester.94 One should not assume that suchexposure is safe, however, because there may be delayedeffects. Nonteratogenic effects of antineoplastic agentsinclude low birth weight, intrauterine growth retardation,spontaneous abortion, premature birth, and myocardial
*References 24-30, 94, 100-108, 112-142.
Table 2.—Chemotherapy During Second and Third Trimesterof Pregnancy
No. ofExposed Patients/
No. ofClass Fetal Malformations Reference No.
Alkylating agents 26/1 30,32,126-128Antimetabolites 38/0 30,32,75Antibiotics 1/0 110Plant alkaloids 6/0 25,32,89,94,112,113Combinations 60/1* 25,31,94,104-107,
111-142Total (%) 131/2 (1.5)
*One case of trlsomy C following cytarabine and thioguanine was reported.Autopsy revealed no congenital malformation.
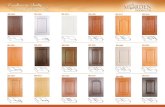
Table 3.—Estimated Average Fetal Dose
Procedure Dose to Fetus, mllliradExtremity 1Shoulder 1Cervical spine 2Skull 4Chest roentgenogram 8Pelvis 40Cholecystography 200Lumbar spine 275Abdomen 290Hip 300Intravenous pyelogram 400Upper gastrointestinal series 560Barium enema 800Lymphangiogram 1100Computed tomography abdomen 1000-5000
toxicity.17·26·30-33·143 Regarding biologic response modifiers,we are not familiar with any data concerning their use inpregnancy.
Little is known about the delayed effects of exposure toantineoplastic agents in utero, but several—impairedmental and physical development, infertility, carcinogen¬esis, and second-generation teratogenesis—have been sug¬gested.17·31-33·144 Transplacental carcinogenesis is well doc¬umented in animals, with the time of greatest susceptibilitynear the end of gestation.146 Second malignant neoplasmsare well-recognized delayed complications of antineoplasticagents in humans,146 but clear evidence of carcinogenesisfrom chemotherapy in utero is lacking. In utero exposureto diethylstilbestrol has been linked to the late develop¬ment of clear-cell vaginal carcinoma in young women,147though the validity of this association has been ques¬tioned.148 Reynoso et al94 recently reported the case of aninfant exposed to cyclophosphamide and prednisonethroughout gestation who developed neuroblastoma at age14 years and thyroid cancer at age 16 years.
ADVERSE EFFECTS OF RADIATION EXPOSUREON THE FETUS AND NEONATE
Radiation effects are related to dose, dose rate, fieldsize, energy of the radiation, and gestational age. Theincidence of malformation is greatest during the period oforganogénesis from the second to the eighth week. Growthretardation, microcephaly, and eye abnormalities have beenthe predominant manifestations. The major unresolvedquestion with radiation is the maximum safe dose. Severalstudies have demonstrated no increase in abortion, growthretardation, or congenital malformations from diagnosticexposures below 0.05 Gy delivered at any time duringgestation.18·149·150 As given in Table 3, the estimated fetal
on May 7, 2010 www.archinternmed.comDownloaded from

dose from many commonly used radiologie diagnosticprocedures is less than 0.01 Gy.161 However, proceduressuch as lymphangiography and computed tomography ofthe pelvis and abdomen may expose the fetus to muchhigher doses (up to 0.05 to 0.1 Gy), and low doses ofradiation potentially could be associated with deleteriouslong-term effects.95 Since diagnostic ultrasound and mag¬netic resonance imaging are not associated with ionizingradiation, these procedures are relatively safe duringpregnancy. However, subdiaphragmatic therapeutic radia¬tion exposure is associated with severe toxic effects to thefetus. The minimal lethal dose increases from approxi¬mately 0.1 Gy at day 1 to greater than 1 Gy after the firsttrimester.161 During the second and third trimesters, thechance of abortion and congenital abnormalities declines,but damage to the central nervous system can occur.
Dekaban152 correlated gestational age with dose and fetaldamage in 26 infants. At 2.5 Gy, more than 50% of theinfants exposed between the third and tenth week ofgestation developed mental retardation, microcephaly, cat¬aracts, retinal degeneration, low birth weight, and skeletaland genital abnormalities. Radiation exposure between 12and 20 weeks was associated with stunted growth, mentalretardation, and microcephaly. Radiation exposure after20 weeks was not associated with any gross malformation,but some infants had evidence of radiation-exposure dam¬age, including erythema, epilation, and hématologie de¬pression. Epidemiologie studies from the Nagasaki andHiroshima (Japan) atomic bombings reported congenitalabnormalities in 28 of 205 infants exposed during the first20 weeks of gestation.153 Abnormalities were not observedbelow an estimated in utero dose of 0.5 Gy in Hiroshima154and 1.5 Gy in Nagasaki.156
In experimental animals, 0.1 to 0.2 Gy does not increasethe incidence of microcephaly.156 To our knowledge, a "safe"dose has not been established, but a commonly repeatedrule is that therapeutic abortion should be considered if adose of 0.1 Gy is exceeded during the first trimester.157 Adose of 0.5 Gy has been associated with a strong possibilityof fetal damage.96
With supradiaphragmatic radiation, substantial scatterto the fetus can occur.60168159 Much of the scatter is internal,but abdominal shielding can reduce the fetal dose signifi¬cantly160 and it may be safe to administer localized radiationto the neck or axilla during the first trimester if absolutelynecessary.60 There are reports of normal infants after full-mantle radiotherapy,96 but one patient with Hodgkin'sdisease had a spontaneous abortion in the first trimesterafter 44 Gy to the chest.50 It is difficult to generalize aboutsafe doses because the size of the uterus varies duringpregnancy and thus its distance from the field of radiationvaries. Sharma et al,160 using a "phantom," validated Clark-son's method of calculating scatter and measured thefraction of mediastinal dose delivered to the uterus atvarious levels below the lower border of the mediastinalportal with and without shielding. They found values of1,2% at 11 cm, 0.6% at 18 cm, and 0.3% at 28 cm whenshielding was used. Thus, the delivery of therapeutic levelsto the mediastinum, ie, 35 to 44 Gy, should scatter lessthan 0.5 Gy to the fetus. In two patients treated withmantle irradiation, fetal doses were measured as 0.04 Gyat the level of the cervix and 0.1 Gy at the level of thefundus at 16 weeks' gestation and 0.08 Gy and 0.3 Gy,respectively, at 25 weeks' gestation.96
The long-term sequelae of fetal radiation exposure areunknown. Chromosomal aberrations have been docu¬mented,161 but to our knowledge, no conclusive data existlinking in utero irradiation to any human mutation or tofuture infertility. The data on carcinogenesis are conflictingwith both positive162165 and negative studies.166167
ADVERSE EFFECTS OF SURGERY ONTHE FETUS AND NEONATE
Of the primary treatment modalities for cancer duringpregnancy, surgery is the type least associated with fetalsequelae. Needle or excision biopsy and surgery underlocal anesthesia are essentially without risk to the fetus.Moreover, if indicated, the ovaries may be safely removedduring the second trimester, since placental progesteroneproduction begins at seven weeks and completely replacesthe corpus luteum by 12 weeks.168 However, pelvic surgeryand cervical conization during the first trimester increasethe risk of abortion.169
Striking physiologic and anatomic changes in manyorgans occur during gestation,170 and such changes may berelevant to the operative management of pregnant patients.For instance, the supine position during late pregnancycauses the uterus to compress the aorta and vena cava171;this may lead to a reduction in uteroplacental perfusionand thus may potentially cause fetal hypoxemia. Since thefetus is sensitive to hypotension and hypoxia, pregnantpatients should not be supine for prolonged periods afterthe first trimester. Also, certain anesthetic drugs andtechniques may compromise blood pressure and cardiacoutput in the gravid patient.170 Knowledge of the variousalterations associated with pregnancy is mandatory for theoptimal management of these patients, and a recent reviewhas discussed this problem in depth.170
ADVERSE EFFECTS OF PREMATURE BIRTH
The risks ofprematurity172 decline rapidly after 28 weeks;in expert neonatal units, the risk of neonatal death forinfants after 32 weeks may not exceed the risk of thoseborn at term.172 Low-birth-weight (^2500 g) infants, andparticularly very-low-birth-weight (<1500 g) infants, areat an increased risk of neonatal death, congenital anoma¬lies, pulmonary complications, and subsequent neurode-velopmental handicaps.173·174 Approximately 90% of theseinfants survive at 1500 g, 80% survive at 1250 g, 60% to75% survive at 1000 g, and 50% survive at 800 to 900 g.174
MANAGEMENT RECOMMENDATIONS
The treatment of cancer occurring during pregnancy iscomplicated, and therapeutic decisions must be individu¬alized. These decisions might best be facilitated by a
multidisciplinary team, including the patient's obstetrician/gynecologist, family physician, oncologist, pediatrician,neonatologist, and other ancillary consultants. Such inter¬action should begin when the patient is initially diagnosedas having cancer. Considerations must be given to theimmediate health of the mother and fetus and to the long-term health of infants exposed to potentially teratogenicand carcinogenic drugs and radiation.
When there is inadvertent chemotherapy or radiationexposure in excess of 0.1 Gy to the uterus during the firsttrimester, the most conservative recommendation is ther¬apeutic abortion. The degree of risk if the pregnancy isnot terminated can be estimated from the data reviewedherein. If the decision is to continue the pregnancy, thenthe question of further therapy should be evaluated as
carefully as if initiating a new therapeutic regimen.If intensive cancer therapy is anticipated early in preg¬
nancy, the conservative approach is to consider therapeuticabortion because of the hazard to the fetus. If the preg¬nancy is to continue and cure is a realistic goal, therapyshould not be modified or delayed to compromise that goal.However, when there is no hope for cure or even significantpalliation, the primary goal should become protection ofthe fetus from the potential harmful effects of chemother-
on May 7, 2010 www.archinternmed.comDownloaded from

apy or irradiation. The most difficult cases are the majorityin which the issues are not so obvious.
When cancer is diagnosed during the first trimester, adecision must be made as to whether treatment can besafely postponed until the second trimester or later. Fortumors encountered after 20 weeks when abortion is notpossible (except as part of the surgical management ofsome tumors), delay of therapy should be considered whenit will not adversely affect maternal prognosis. Earlydelivery may allow a compromise between risk to motherand risk to child by permitting earlier cancer treatment.Ultrasound and laboratory analysis of amniotic fluid canbe helpful in determining the timing and mode of deliveryof a viable fetus.176
When chemotherapy must be given, one should selectdrugs to minimize fetal damage without compromisingtherapeutic benefit to the mother. During the first trimes¬ter, folate antagonists should never be given. At present,methotrexate is not part of any curative regimen for whicha therapeutic equivalent is lacking. This is fortunate sincethe folie acid antagonists, more than any other agents,have been associated with fetal abnormalities when givenduring the first trimester.61-69·72-74 A syndrome of congenitalanomalies has been recognized, the "aminopterin syn¬drome," with the most consistent anomaly being cranialdysostosis.72 Other antimetabolites have rarely been asso¬ciated with fetal malformations. An isolated case of fluo-rouracil-associated congenital abnormality also occurredin a fetus who had received radiotherapy.86 Of 20 patientsexposed to mercaptopurine alone, no fetal anomalies weredocumented.30·32·77-83
There are only two cases of malformation in 44 patientswho received alkylating agents in the first trimester (whenpatients who also received radiotherapy are excluded), so
alkylating agents given alone may be relatively safe. Thereare two potentially curative or significantly palliativeregimens using single alkylating agents: melphalan inovarian cancer176 and the adjuvant breast cancer regimenusing cyclophosphamide reported by Nissen-Meyer et al.177
Although vinblastine sulfate is highly teratogenic inanimal models,178 there has been only one reported abnor¬mality observed in the offspring of 14 women treated withvinblastine in the first trimester.25·30·32·86-89 Therefore, theuse of vinblastine in the first trimester may be relativelysafe. Used alone this agent is only palliative, but it mightbe considered in the patient with Hodgkin's disease whentemporizing chemotherapy is necessary until a curativeregimen becomes safer for the fetus. We found no data onthe closely related vinca alkaloid, vincristine sulfate.
Regarding combination chemotherapy, four of the sevenmalformations seen with combination regimens were inpatients who had received procarbazine hydrochloride.The popular MOPP (mechlorethamine [Mustargen] hydro¬chloride, vincristine sulfate [Oncovin], procarbazine, andprednisone) regimen, one of two regimens curative inHodgkin's disease, contains this drug. The other popularcurative regimen is ABVD (doxorubicin hydrochloride[Adriamycin], bleomycin sulfate, vinblastine, and dacar-bazine), and although no data concerning the use of thisregimen during pregnancy are available (to our knowledge),the drugs in this combination, used singly, have rarely beenassociated with fetal malformations. Insufficient data areavailable to evaluate the CHOP (cyclophosphamide, doxo¬rubicin [Adriamycin], vincristine [Oncovin], and predni¬sone) and BACOP (bleomycin, doxorubicin [Adriamycin],cyclophosphamide, vincristine [Oncovin], and prednisone)regimens curative in intermediate and high-grade lympho¬mas and the PVB (cisplatin [Platinol], vinblastine, andbleomycin) regimen curative in germ cell tumors, but thedrugs in these regimens, used singly, are not unusually
teratogenic based on the human data in Table 1.Single and combination chemotherapy may be adminis¬
tered in the second and third trimester, with a low risk ofteratogenicity. Nevertheless, the least potentially terato¬genic regimen should be selected. The mother and familyshould be informed of the possible early and delayed effectsof cancer therapy.
There are several tumors seen during pregnancy in whichchemotherapy may increase the cure rate: breast cancer,acute leukemia, intermediate and high-grade lymphomas,Hodgkin's disease, and ovarian cancer. Other tumors inwhich radiation therapy may be curative are: carcinoma ofthe cervix, Hodgkin's disease, non-Hodgkin's lymphoma,epithelial and germ cell tumors of the ovary. Surgery maybe curative in melanoma and carcinomas of the breast,cervix, ovary, large bowel, vagina, thyroid.
Breast cancer is best managed surgically rather thanwith the newer breast-sparing procedures that requireirradiation. Patients in this age group are likely to havehormone-receptor-negative, lymph-node-positive diseaseand thus have a poorer prognosis. Survival can be improvedby 20% to 30% in such patients by the use of adjuvantchemotherapy,179 but such therapy is not effective if de¬layed. If adjuvant chemotherapy for breast cancer is usedin the first trimester, the CMF (cyclophosphamide, meth¬otrexate, and fluorouracil) regimen is not the regimen ofchoice. One might consider the CAF (cyclophosphamide,doxorubicin [Adriamycin], and fluorouracil) regimen oreven the regimen of Nissen-Meyer et al177 that utilizes onlycyclophosphamide. In the second or third trimester, CMFmay be utilized.
Acute leukemia requires immediate, intensive, and pro¬longed chemotherapy that may produce fetal damage ifgiven during the first trimester. Delay in therapy willeliminate the very real possibility of cure. During the firsttrimester, if abortion is refused, the therapy may produceabortion or fetal malformation. During the second andthird trimester, despite the intensity of therapy, there arenumerous reports of normal infants.24·94·114115 Because acuteleukemia is potentially curable, particularly in youngerpatients, the best available regimen should be used.
Approximately half the cases of leukemia diagnosedduring pregnancy are chronic myelogenous leukemia.180Often it is possible to observe these patients, withoutprescribing therapy, after the diagnosis is made. If thewhite blood cell count rises to the level where vascularevents are likely, over 250 109/L, or if splenomegalybecomes a problem, leukapheresis may be useful in reduc¬ing the count and decreasing the size of the spleen.181
Lymphoma presents a more complex dilemma. Delayuntil after delivery is almost certainly the best choice innon-Hodgkin lymphoma of the low-grade variety, but thisis uncommon in pregnancy. In the intermediate and high-grade forms, intensive chemotherapeutic regimens are
required to achieve a potential cure rate of about 33% to70%, but delay from the first to the second trimester oruntil after delivery may compromise such results. Inconsidering delay, it should be remembered that withintermediate and high-grade non-Hodgkin's lymphoma,there are no curative salvage regimens, except perhapsintensive chemotherapy coupled with bone marrow trans¬plantation. If therapy is to be given, a first-line regimensuch as CHOP, or one of the newer combination regimens,182should be selected to maximize the possibility of cure.
For Hodgkin's disease, it is probably not possible todeliver full-mantle radiation or one of the curative chemo¬therapy regimens early in pregnancy without a high prob¬ability of fetal damage. Delay, at least until the secondtrimester, seems indicated, and the availability of severalcurative approaches makes delay more reasonable in this
on May 7, 2010 www.archinternmed.comDownloaded from

instance that in high-grade non-Hodgkin's lymphoma. Iftreatment becomes necessary due to disease progressionduring the first trimester, it is reasonable to temporizewith limited radiation to supradiaphragmatic areas andsingle-drug therapy with vinblastine. After the first tri¬mester, it is probably reasonable to begin radiotherapyabove the diaphragm with modification of field and doseand appropriate abdominal shielding. Calculation of esti¬mated fetal dose should be performed. Curative combina¬tion chemotherapy, such as MOPP or ABVD, may be givenduring the second or third trimester with little teratogenicrisk to the fetus. If the disease permits, delay of definitivetherapy until after delivery is an alternative with even lessfetal risk. Staging Hodgkin's disease during pregnancymay be a problem; some have suggested a single 24-hourlymphangiogram as producing the maximum informationfor the least fetal exposure.96 Ultrasound and magneticresonance imaging may be useful and do not expose thefetus to ionizing radiation. If definitive therapy is delayed,staging should also be delayed until after delivery.
Ovarian cancer may be cured by salpingo-oophorectomyalone in stage IA or IB, whether of epithelial183 or germcell184 origin, but more extensive disease requires chemo¬therapy for cure. Because of a high risk of inducingabortion, surgical exploration of an asymptomatic ovarianmass should be delayed until the second trimester unlessthe mass is very large, over 6 cm186 or over 10 cm.186Extensive investigation with multiple biopsy specimens isnecessary. If cure is to be achieved by subsequent chemo¬therapy in cancer of epithelial origin, the usually recom¬mended surgery is total hysterectomy and bilateral sal¬pingo-oophorectomy with omentectomy and debulking ofperitoneal implants over 1 cm in size. In such cases, thequestion of chemotherapy damage to the fetus will notarise. On the other hand, tumors of germ cell origin mayconstitute up to one third of ovarian cancers in pregnancy187;even in the absence of debulking surgery, these seem to becurable with radiation therapy or with intensive chemo¬therapy with PVB,188 with the latter being the treatmentof choice.
Colposcopy should be used to follow up suspicious cer¬vical cytologie specimens; if carcinoma in situ is discovered,careful observation is necessary until after delivery. Ifcolposcopy is unsatisfactory, cone biopsy may be necessary,but this carries substantial risk to the pregnancy. Coniza-tion should be performed during the second trimester, ifpossible.168 When invasive cervical cancer is diagnosed, itmay be possible to delay definitive therapy until afterdelivery; if rapid progression of the disease is observed,however, the best treatment is probably hysterectomy,with appropriate dissection based on stage. Radiotherapygives comparable survival, and the products of conceptionare generally passed after three to six weeks.189 Hysterot-omy or cesarean delivery may precede surgery or radiationafter 20 weeks' gestation in the rare patient in whom delayuntil delivery is not possible. This question has beenextensively reviewed elsewhere.168
Melanoma and cancers of the thyroid, colon, and vaginaare best managed surgically as in the nonpregnant patientexcept that irradiation and radioactive iodine are not used.In none of these cancers—melanoma, thyroid, colon, va¬
gina—does chemotherapy offer sufficient benefit to themother to warrant the risk to the fetus.
If chemotherapy has been given, delivery should beinduced or cesarean section performed as near to term as
possible when maternal blood cell counts are not compro¬mised due to cancer therapy.144 Neonatal cytopenias havebeen noted after exposure to cancer chemotherapy,108 so a
complete blood cell count should be obtained on the new¬born. Antineoplastic agents administered systemically
may reach significant levels in milk,190 and cyclophospha¬mide has produced neutropenia and thrombocytopenia ina breast-fed infant191; therefore, breast-feeding is contra¬indicated if the mother is receiving chemotherapy. A carefulexamination should be made for congenital malformationsand organ dysfunction, and long-term follow-up of theinfant is essential.
Michael C. Perry, MD, Alfred Llorens, MD, and Jerry Murrell, MD,reviewed the manuscript, and Susan E. Brown gave secretarial assistance.
References
1. Silverberg E, Lubera J: Cancer statistics, 1986. CA 1986;36:9-25.2. Orr JW Jr, Shingleton HM: Cancer in pregnancy. Curr Probl Cancer
1983;8:1-50.3. Nieminen V, Remes N: Malignancy during pregnancy. Acta Obstet
Gynecol Scand 1970;49:315-318.4. Barber HRK, Brunschwig A: Gynecologic cancer complicating preg-
nancy. Am J Obstet Gynecol 1963;85:156-164.5. Lutz MH, Underwood PB Jr, Rozier JC, et al: Genital malignancy in
pregnancy. Am J Obstet Gynecol 1977;129:536-542.6. Betson JR, Golden ML: Cancer and pregnancy. Am J Obstet Gynecol
1961;81:718-728.7. Haas JF: Pregnancy in association with a newly diagnosed cancer: A
population-based epidemiologic assessment. Int J Cancer 1984;34:229-235.8. Potter JF, Schoeneman M: Metastasis of maternal cancer to the
placenta and fetus. Cancer 1970;25:380-388.9. Read EJ Jr, Platzer PB: Placental metastasis from maternal carcinoma
of the lung. Obstet Gynecol 1981;58:387-391.10. Davison JS, Davison MC, Hay DM: Gastric emptying time in late
pregnancy and labour. Br J Obstet Gynaecol 1970;77:37-41.11. Parry E, Shields R, Turnbull AC: Transit time in the small intestine
in pregnancy. Br J Obstet Gynaecol 1970;77:900-901.12. Pirani BBK, Campbell DM, MacGillivray I: Plasma volume in normal
first pregnancy. Br J Obstet Gynaecol 1973;80:884-887.13. Mucklow JC: The fate of drugs in pregnancy. Clin Obstet Gynaecol
1986;13:161-175.14. Redmond GP: Physiological changes during pregnancy and their
implications for pharmacological treatment. Clin Invest Med 1985;8:317\x=req-\322.
15. Powis G: Anticancer drug pharmacodynamics. Cancer ChemotherPharmacol 1985;14:177-183.
16. Wan SH, Huffman DH, Azarnoff DL, et al: Effect of route ofadministration and effusions on methotrexate pharmacokinetics. CancerRes 1974;34:3487-3491.
17. Beeley L: Adverse effects of drugs in the first trimester of pregnancy.Clin Obstet Gynaecol 1986;13:177-195.
18. Kalter H, Warkany J: Congenital malformations. N Engl J Med1983;308:424-431.
19. Cahen RL: Experimental and clinical chemoteratogenesis. Adv Phar-macol Chemother 1966;4:263-349.
20. Chaube S, Murphy ML: The teratogenic effects of the recent drugsactive in cancer chemotherapy. Adv Teratology 1968;3:181-237.
21. Sieber SM, Adamson RH: Toxicity of antineoplastic agents in man:Chromosomal aberrations, antifertility effects, congenital malformationsand carcinogenic potential. Adv Cancer Res 1975;22:57-155.
22. Brent RL: Evaluating the alleged teratogenicity of environmentalagents. Clin Perinatol 1986;13:609-613.
23. Beckman DA, Brent RL: Mechanism of known environmental tera-togens: Drugs and chemicals. Clin Perinatol 1986;13:649-687.
24. Antman KH, Mayer RJ, Frei E: Vascular, hormonal, teratogenic andmiscellaneous toxicities of chemotherapeutic agents, in Perry MC, YarbroJW (eds): Toxicity of Chemotherapy. New York, Grune & Stratton, 1984,pp 521-538.
25. Mulvihill JJ, McKeen EA, Rosner F, et al: Pregnancy outcome incancer patients: Experience in a large cooperative group. Cancer 1987;60:1143-1154.
26. Diamond I, Anderson MM, McCreadie SR: Transplacental transmis-sion of busulfan (Myleran) in a mother with leukemia: Production of fetalmalformations and cytomegaly. Pediatrics 1960;25:85-90.
27. Toledo TM, Harper RC, Moser RH: Fetal effects during cyclophos-phamide and irradiation therapy. Ann Intern Med 1971;74:87-91.
28. Abramovici A, Shaklai M, Pinkhas J: Myeloschisis in a six weeksembryo of a leukemic woman treated with busulfan. Teratology 1978;18:241-246.
29. Sokal JE, Lessman EM: Effects of cancer chemotherapeutic agentson the human fetus. JAMA 1960;172:1765-1771.
30. Nicholson HO: Cytotoxic drugs in pregnancy. Br J Obstet Gynaecol1968;75:307-312.
31. Blatt J, Mulvihill JJ, Ziegler JL, et al: Pregnancy outcome followingcancer chemotherapy. Am J Med 1980;69:828-832.
32. Sweet DL Jr, Kinzie J: Consequences of radiotherapy and antineo-plastic therapy for the fetus. J Reprod Med 1976;17:241-246.
33. Barber HRK: Fetal and neonatal effects of cytotoxic agents. Obstet
on May 7, 2010 www.archinternmed.comDownloaded from

Gynecol 1981;58:41S-47S.34. Gilliland J, Weinstein L: The effects of cancer chemotherapeutic
agents on the developing fetus. Obstet Gynecol Surv 1983;38:6-13.35. Izumi HM: Myleran in pregnancy: Report of a case. JAMA 1956;
161:969.36. Sherman JL, Locke RV: Use of busulfan in myelogenous leukemia
during pregnancy. N Engl J Med 1958;259:288-289.37. Ruiz Reyes G, Tamayo Perez R: Leukemia and pregnancy: Observa-
tion of a case treated with busulfan (Myleran). Blood 1961;18:764-768.38. White LG: Busulfan in pregnancy. JAMA 1962;179:973-974.39. Neu LT: Leukemia complicating pregnancy. Mo Med 1962;59:220\x=req-\
222.40. Lee RA, Johnson CE, Hanlon DG: Leukemia during pregnancy. Am
J Obstet Gynecol 1962;84:455-461.41. Dennis LH, Stein S: Busulfan in pregnancy. JAMA 1965;192:715-716.42. Earl JM, May RL: Busulfan therapy of myelocytic leukemia during
pregnancy. Am J Obstet Gynecol 1965;92:580-581.43. Williams DW: Busulfan in early pregnancy. Obstet Gynecol
1966;27:738-740.44. Smalley RV Wall RL: Two cases of busulfan toxicity. Ann Intern Med
1966;64:154-164.45. Dugdale M, Fort AT: Busulfan treatment of leukemia during preg-
nancy. JAMA 1967;199:131-133.46. Frid-de Guttman R: Leukemia and pregnancy: Report of two cases
treated with busulfan. Rev Invest Clin 1968;20:359-367.47. Korbitz BL, Reiquam CW: Busulfan in chronic granulocytic leukemia:
A spectrum of clinical considerations. Clin Med 1969;76:16.48. Nolan GH, Marks R, Perez C: Busulfan treatment of leukemia during
pregnancy: A case report. Obstet Gynecol 1971;38:136-138.49. Shotten D, Monie IW: Possible teratogenic effect of chlorambucil on
a human fetus. JAMA 1963;186:74-75.50. Jacobs C, Donaldson SC, Rosenberg SA, et al: Management of the
pregnant patient with Hodgkin's disease. Ann Intern Med 1981;95:669-675.51. Baynes TLS, Grickmay GF, Vaughn Jones R: Pregnancy in a case of
chronic lymphatic leukemia. Br J Obstet Gynaecol 1968;75:1165-1168.52. Revol L, Viala J, Pelet J, et al: Hodgkin's disease, lymphosarcoma,
reticulosarcoma and pregnancy. Nouv Rev Fr Hematol 1962;2:311-325.53. Greenberg LH, Tanaka KR: Congenital anomalies probably induced
by cyclophosphamide. JAMA 1964;188:423-426.54. Sinkovics JG, Shullenberger CC: Pregnancy and systemic malignant
disease, abstracted. Cancer Chemother Rep 1969;53:94.55. Coates A: Cyclophosphamide in pregnancy. Aust NZ J Obstet Gynae-
col 1970;10:33-34.56. Zoet AG: Pregnancy complicating Hodgkin's disease. Northwest Med
1950;49:373-374.57. Barry RM, Diamond HD, Craver LF: Influence of pregnancy on the
course of Hodgkin's disease. Am J Obstet Gynecol 1962;84:445-454.58. Boland J: Reticuloses: Clinical experience with nitrogen mustard in
Hodgkin's disease. Br JRadiol 1951;24:513-515.59. Smith RBW, Sheehy TW, Rothbert H: Hodgkin's disease and preg-
nancy. Arch Intern Med 1958;102:777-789.60. Dameshek W, Gunz F: Leukemia, ed 2. New York, Grune & Stratton,
1964.61. DeAlvarez RR: An evaluation of aminopterin as an abortifacient. Am
J Obstet Gynecol 1962;83:1467-1477.62. Bourne FM, Freedman SO, Joron GE: Intoxication by aminopterin
used as an abortifacient. Can Med Assoc J 1957;76:473-475.63. Cariati A: A case ofacute hematocytoblastic leukemia and pregnancy.
Riv Ostet Ginecol 1955;10:785-796.64. Emerson DJ: Congenital malformation due to attempted abortion
with aminopterin. Am J Obstet Gynecol 1962;84:356-357.65. Goetsch C: An evaluation of aminopterin as an abortifacient. Am J
Obstet Gynecol 1962;83:1474-1477.66. Harris LJ: Leukemia and pregnancy. Can Med Assoc J 1953;68:234\x=req-\
236.67. Meltzer HJ: Congenital anomalies due to attempted abortion with 4\x=req-\
amino-pteroglutamic acid. JAMA 1956;161:1253.68. Warkany J, Beaudry PH, Hornstein S: Attempted abortion with
aminopterin: Malformations of the child. AJDC 1959;97:274-281.69. Thiersch JB: Therapeutic abortions with a folic acid anagonist 4\x=req-\
aminop-teroyglutamic acid administered by the oral route. Am J ObstetGynecol 1952;63:1298-1304.
70. Powell HR, Eckert H: Methotrexate-induced congenital malforma-tions. Med J Aust 1971;2:1076-1077.
71. Milunsky A, GraefJW, Gaynor MF Jr: Methotrexate-induced congen-ital malformations. J Pediatr 1968;72:790-795.
72. Warkany J: Aminopterin and methotrexate: Folic acid deficiency.Teratology 1978;17:353-358.
73. Schein PS, Winokur SH: Immunosuppressive and cytotoxic chemo-therapy: Long-term complications. Ann Intern Med 1975;82:84-95.
74. Panchalingham S: Post-methotrexate babies. Ceylon Med J 1973;18:93-97.
75. Wegelius R: Successful pregnancy in acute leukemia. Lancet 1975;2:1301.
76. McConnell JB, Bhoola R: A neonatal complication of maternalleukemia treated with 6-mercaptopurine. Postgrad Med J 1973;49:211-213.
77. Frenkel EP, Meyers MC: Acute leukemia and pregnancy. Ann InternMed 1960;53:656-671.
78. Hoover BA, Schumacher HR: Acute leukemia in pregnancy. Am JObstet Gynecol 1966;96:316-320.
79. Freedman HL, Magagnini A, Glass M: Pregnancies following chemi-cally treated choriocarcinoma. Am J Obstet Gynecol 1962;83:1637-1641.
80. Ravenna P, Stein PJ: Acute monocytic leukemia in pregnancy: Reportof a case treated with 6-mercaptopurine in the first trimester. Am J ObstetGynecol 1963;85:545-548.
81. Sinykin MB, Kaplan H: Leukemia in pregnancy. Am J Obstet Gynecol1962;83:220-224.
82. Boggs DR, Wintrobe MM, Cartwright GE: The acute leukemias.Medicine 1962;41:163-226.
83. Mersky C, Rigal W: Pregnancy in acute leukemia treated with 6\x=req-\mercaptopurine. Lancet 1956;2:1268-1269.
84. Wagner VM, Hill JS, Weaver D, et al: Congenital abnormalities inbaby born to cytarabine treated mother. Lancet 1980;2:98-99.
85. Stephens JD, Golbus MS, Miller TR, et al: Multiple congenitalanomalies in a fetus exposed to 5-fluorouracil during the first trimester.Am J Obstet Gynecol 1980;137:747-749.
86. Armstrong JG, Dyke RW, Fouts PJ, et al: Delivery of a normal infantduring the course of oral vinblastine sulfate therapy for Hodgkin's disease.Ann Intern Med 1964;61:106-107.
87. Rosenzweig AI, Crews QE, Hopwood HG: Vinblastine sulfate inHodgkin's disease in pregnancy. Ann Intern Med 1964;61:108-112.
88. Goguel A: Hodgkin's disease and pregnancy. Presse Med 1970;78:1507\x=req-\1510.
89. Nisce LZ, Tome MA, He S, et al: Management of coexisting Hodgkin'sdisease and pregnancy. Am J Clin Oncol 1986;9:146-151.
90. Alegre A, Chunchuretta R, Rodriguez-Alarcon J, et al: Successfulpregnancy in acute promyelocytic leukemia. Cancer 1982;49:152-153.
91. Wells JH, Marshall JR, Carbone PP: Procarbazine therapy forHodgkin's disease in early pregnancy. JAMA 1968;205:119-121.
92. Jacobs A, Marchevsky A, Gordon RE, et al: Oat cell carcinoma of theuterine cervix in a woman treated with cis-diamminedichloroplatinum.Gynecol Oncol 1980;9:405-410.
93. Ioachim HL: Non-Hodgkin's lymphoma in pregnancy: Three casesand review of the literature. Arch Pathol Lab Med 1985;109:803-809.
94. Reynoso E, Shepherd F, Messner H, et al: Acute leukemia duringpregnancy: The Toronto Leukemia Study Group experience with long-termfollow-up of children exposed in utero to chemotherapeutic agents. J ClinOncol 1987;5:1098-1106.
95. Brent RL: The effects of embryonic and fetal exposure to x-ray,microwaves, and ultrasound. Clin Perinatol 1986;13:615-648.
96. Thomas PRM, Peckham MJ: The investigation and management ofHodgkin's disease in the pregnant patient. Cancer 1976;38:1443-1451.
97. Garrett MJ: Teratogenic effects of combination chemotherapy. AnnIntern Med 1974;80:667.
98. Schapira DJ, Chudley AE: Successful pregnancy following continuoustreatment with combination chemotherapy before conception and through-out pregnancy. Cancer 1984;54:800-803.
99. Schafer AI: Teratogenic effects of antileukemic chemotherapy. ArchIntern Med 1981;141:514-515.
100. Newcomb M, Balducci L, Thigpen JT, et al: Acute leukemia inpregnancy: Successful delivery after cytarabine and doxorubicin. JAMA1978;739:2691-2692.
101. Mennuti MT, Shepard TH, Mellman WJ: Fetal renal malformationfollowing treatment of Hodgkin's disease during pregnancy. Obstet Gynecol1975;46:194-196.
102. Dara P, Slater LM, Armentrout SA: Successful pregnancy duringchemotherapy for acute leukemia. Cancer 1981;47:845-846.
103. Lilleyman JS, Hill AS, Anderton KJ: Consequences of acute mye-logenous leukemia in early pregnancy. Cancer 1977;40:1300-1303.
104. Pizzuto J, Aviles A, Noriega L, et al: Treatment of acute leukemiaduring pregnancy Cancer Treat Rep 1980;64:679-683.
105. Jones RT, Weinerman BH: MOPP (nitrogen mustard, vincristine,procarbazine, and prednisone) given during pregnancy. Obstet Gynecol 1979;54:477-478.
106. Falkson HC, Simson IW, Falkson G: Non-Hodgkin's lymphoma inpregnancy. Cancer 1980;45:1679-1682.
107. Lowenthal RM, Funnell CF, Hope DM, et al: Normal infant aftercombination chemotherapy including teniposide for Burkitt's lymphoma inpregnancy. Med Pediatr Oncol 1982;10:165-169.
108. Okun DB, Groncy PK, Sieger L, et al: Acute leukemia in pregnancy:Transient neonatal myelosuppression after combination chemotherapy inthe mother. Med Pediatr Oncol 1979;7:315-319.
109. Murray CL, Reichert JA, Anderson J, et al: Multimodal cancer
therapy for breast cancer in the first trimester ofpregnancy: A case report.JAMA 1984;252:2607-2608.
110. Roboz J, Gleicher N, Wu K, et al: Does doxorubicin cross theplacenta? Lancet 1979;2:1382-1383.
111. Karp GI, von Oeyen P, Valone F, et al: Doxorubicin in pregnancy:Possible transplacental passage. Cancer Treat Rep 1983;67:773-777.
112. Nordlund JJ, DeVita VT, Carbone PP: Severe vinblastine-inducedleukopenia during late pregnancy with delivery of a normal infant. AnnIntern Med 1968;69:581-582.
113. Lacher MJ: Use of vinblastine sulfate to treat Hodgkin's diseaseduring pregnancy. Ann Intern Med 1964;61:106-107.
114. Fassas A, Kartalis G, Klearchou N, et al: Chemotherapy for acuteleukemia during pregnancy. Nouv Rev Fr Hematol 1984;26:19-24.
on May 7, 2010 www.archinternmed.comDownloaded from

115. Catanzarite JA, Ferguson JE: Acute leukemia and pregnancy: Areview of management outcome, 1972-1982. Obstet Gynecol Surv 1984;39:663-678.
116. Haerr RW Pratt AT: Multiagent chemotherapy for sarcoma diag-nosed during pregnancy. Cancer 1985;56:1028-1033.
117. Cantini E, Yanes B: Acute myelogenous leukemia in pregnancy.South Med J 1984;77:1050-1052.
118. Durie BGM, Giles HR: Successful treatment of acute leukemiaduring pregnancy. Arch Intern Med 1977;137:90-91.
119. Doney KC, Kraemer KG, Shepard TH: Combination chemotherapyfor acute myelocytic leukemia during pregnancy: Three case reports. CancerTreat Rep 1979;63:369-371.
120. Taylor G, Blom J: Acute leukemia during pregnancy. South Med J1980;73:1314-1315.
121. Raich PC, Curet LB: Treatment ofacute leukemia during pregnancy.Cancer 1975;36:861-862.
122. Ortega J: Multiple agent chemotherapy including bleomycin of non-
Hodgkin's lymphoma during pregnancy. Cancer 1977;40:2829-2835.123. Garg A, Kochupillai V: Non-Hodgkin's lymphoma in pregnancy.
South Med J 1985;78:1263-1264.124. Hardin JA: Cyclophosphamide treatment of lymphoma during third
trimester of pregnancy. Obstet Gynecol 1972;39:850-851.125. Maurer LH, Forcier RJ, McIntyre OR: Fetal group C trisomy after
cytosine arabinoside and thioguanine. Ann Intern Med 1971;75:809-810.126. Boros SJ, Reynolds JW: Intrauterine growth retardation following
third trimester exposure to busulfan. Am J Obstet Gynecol 1977;129:111\x=req-\112.
127. Finkle HJ, Goldman RL: Burkitt's lymphoma: Gynecologic consid-eration. Obstet Gynecol 1974;43:281-284.
128. Armitage JD, Feagler JR: Burkitt during pregnancy with bilateralbreast involvement. JAMA 1976;237:247-253.
129. Johnson IR, Filshie GM: Hodgkin's disease diagnosed in pregnancy.Br J Obstet Gynecol 1977;84:791-792.
130. Hamer JW, Beard MEJ, Duff GB: Pregnancy complicated by acutemyeloid leukemia. NZ Med J 1979;89:212-213.
131. Lowenthal RM, Marsden KA, Newman NM, et al: Normal infantafter treatment of acute myeloid leukemia in pregnancy with daunorubicin.Aust NZ J Med 1978;8:431-432.
132. Manoharan A, Leyden MJ: Acute non-lymphocytic leukemia in thethird trimester of pregnancy. Aust NZ J Med 1979;9:71-74.
133. Coopland AT, Friesen WJ, Galbraith PA: Acute leukemia in preg-nancy. Am J Obstet Gynecol 1969;105:1288-1289.
134. O'Donnell R, Lostigan C, O'Connell G: Two cases of acute leukemiain pregnancy. Acta Haematol 1979;61:298-300.
135. Khunsid M, Saleem M: Acute leukemia in pregnancy. Lancet1978;2:534-535.
136. Krueger JA, David RB, Field C: Multiple-drug chemotherapy in themanagement of acute lymphocytic leukemia during pregnancy. ObstetGynecol 1976;48:324-327.
137. Gokal R, Durant J, Baum JD, et al: Successful pregnancy in acutemonocytic leukemia. Br J Cancer 1976;34:299-302.
138. Tobias JS, Bloom HJG: Doxorubicin in pregnancy. Lancet 1980;1:776.139. Gstottner M, Frisch H, Dienstl F: Delivery of a normal child after
chemotherapy of acute promyelocytic leukemia during pregnancy. Blut1978;36:171-174.
140. Chapman RM, Crosby WH: Hodgkin's disease and the pregnantpatient. Ann Intern Med 1982;96:681-682.
141. Pawliger DF, McLean FW Noyes WD: Normal fetus after cytosinearabinoside therapy. Ann Intern Med 1971;75:1012.
142. Plows CW: Acute myelomonocytic leukemia in pregnancy: Reportof a case. Am J Obstet Gynecol 1982;143:41-42.
143. Schaison G, Jacquillat C, Auclerc G, et al: Les fisques foeto-embryonnaines des chimiotherapies. Bull Cancer 1979;66:165-170.
144. Sutcliffe SB: Treatment of neoplastic disease during pregnancy:Maternal and fetal effects. Clin Invest Med 1985;8:333-338.
145. Rice JM: An overview of transplacental carcinogenesis. Teratology1973;8:113-126.
146. Kyle RA: Second malignancies associated with chemotherapy, inPerry MC, Yarbro JW (eds): Toxicity of Chemotherapy. New York, Grune& Stratton, 1984, pp 479-506.
147. Herbst AL, Ulfelderlt H, Poskanzer DC: Adenocarcinoma of thevagina: Association of maternal stilbestrol therapy with tumor appearancein young women. N Engl J Med 1971;284:878-881.
148. McFarlane MJ, Feinstein AR, Horwitz RI: Diethylstilbestrol andclear cell vaginal carcinoma: Reappraisal of the epidemiologic evidence.Am J Med 1986;81:855-863.
149. Kinlen LV, Acheson FD: Diagnostic irradiation, congenital malfor-mations, and spontaneous abortion. Br J Radiol 1968;41:648-654.
150. Mole RH: Radiation effects on pre-natal development and theirradiological significance. Br JRadiol 1979;52:89-101.
151. Brent RL: Irradiation in pregnancy, in Gerbie AB, Sciarra JJ (eds):Gynecology and Obstetrics. New York, Harper & Row Publishers Inc, 1981,pp 1-22.
152. Dekaban AS: Abnormalities in children exposed to x-irradiationduring various stages of gestation: Tentative timetable of radiation injuryto the human fetus. J Nucl Med 1968;9:471-477.
153. Plummer G: Anomalies occurring in children exposed in utero tothe atomic bomb in Hiroshima. Pediatrics 1952;10:687-692.
154. Blot WJ, Miller RW: Mental retardation following in utero exposureto the atomic bombs of Hiroshima and Nagasaki. Radiology 1973;106:617\x=req-\619.
155. Blot WJ: Growth and development following prenatal and childhoodexposure to atomic radiation. J Radiat Res 1975;16(suppl):82-88.
156. Brent RL: Radiations and other physical agents, in Wilson JG,Fraser FC (eds): Handbook of Teratology. New York, Plenum Press, 1977,vol 1, pp 153-223.
157. Hammer-Jacobson E: Therapeutic abortion on account of X-rayexamination during pregnancy. Dan Med Bull 1959;6:113-122.
158. Covington EE, Baker AS: Dosimetry of scattered radiation to thefetus. JAMA 1969;209:414-415.
159. Zucali R, Marchesini R, DePolo G: Abdominal dosimetry for supra-diaphragmatic irradiation of Hodgkin's disease in pregnancy: Experimentaldata and clinical considerations. Tumori 1981;67:203-208.
160. Sharma SC, Williamson JF, Khan FM, et al: Measurement andcalculation of ovary and fetus dose in extended field radiotherapy for 10MVX rays. Int J Radiat Oncol Biol Phys 1981;7:843-846.
161. Bloom AD, Neriishi S, Kamada N, et al: Cytogenetic investigationof survivors of the atomic bombings of Hiroshima and Nagasaki. Lancet1966;2:672-678.
162. Stewart A, Webb V, Giles D, et al: Malignant disease in childhoodand diagnostic irradiation in utero. Lancet 1956;2:447.
163. Bithell JF, Stewart AM: Prenatal irradiation and childhood malig-nancy: A review of British data from the Oxford survey. Br J Cancer1975;31:271-287.
164. Shlono PH, Chung CS, Myrianthopoulos NC: Preconception radia-tion, intrauterine diagnostic radiation, and childhood neoplasia. JNCI1980;65:681-686.
165. Harvey EB, Boice JD Jr, Honeyman M, et al: Prenatal x-rayexposure and childhood cancer in twins. N Engl J Med 1985;312:541-545.
166. Count-Brown SM, Soll R, Hill RB: Incidence of leukemia afterexposure to diagnostic radiation in utero. Br Med J 1960;2:1539-1545.
167. Jablon S, Kato H: Childhood cancer in relation to prenatal exposureto atom-bomb radiation. Lancet 1970;2:1000-1003.
168. Csapo AI, Pulkkinen MO, Wiest WG: Effects of luteectomy andprogesterone replacement in early pregnant patients. Am J Obstet Gynecol1973;115:759-765.
169. Hacker NF, Berek JS, Lagasse LD, et al: Carcinoma of the cervixassociated with pregnancy. Obstet Gynecol 1982;59:735-747.
170. Barron WM: The pregnant surgical patient: Medical evaluation andmanagement. Ann Intern Med 1984;101:683-691.
171. Marx GF, Bassell GM: Hazards of the supine position in pregnancy.Clin Obstet Gynaecol 1982;9:255-271.
172. Howie PW, Patel NB: Obstetric management of preterm labor. ClinObstet Gynaecol 1984;11:373-390.
173. McCormick MC: The contribution of low birth weight to infantmortality and childhood morbidity. N Engl J Med 1985;312:82-90.
174. Cashore WJ, Stern L: Neonatal problems of the preterm baby. ClinObstet Gynaecol 1984;11:391-414.
175. Chervenak FA, Isaacson G, Mahoney MV: Advances in the diagnosisof fetal defects. N Engl J Med 1986;315:305-307.
176. Young RC, Chabner BA, Hubbard SP, et al: Advanced ovarianadenocarcinoma: A prospective clinical trial of melphalan (L-PAM) versuscombination chemotherapy. N Engl J Med 1979;299:1261-1266.
177. Nissen-Meyer R, Kjellgren K, Malmio K, et al: Surgical adjuvantchemotherapy: Results with one short course with cyclophosphamide aftermastectomy for breast cancer. Cancer 1978;41:2088-2098.
178. Ferm VJ: Congenital malformation in hamster embryos after treat-ment with vinblastine and vincristine. Science 1963;141:426.
179. Bonadonna G, Valagussa P: Current status of adjuvant chemother-apy for breast cancer. Semin Oncol 1987;14:8-22.
180. O'Dell RF: Leukemia and lymphoma complicating pregnancy. ClinObstet Gynaecol 1979;22:859-870.
181. Fitzgerald D, Rowe JM, Heal J: Leukapheresis for control of chronicmyelogenous leukemia during pregnancy. Am J Hematol 1986;22:213-218.
182. Coleman M, Gerstein G, Topilo WA, et al: Advances in chemotherapyfor large cell lymphoma. Semin Hematol 1987;24(suppl 1):8-20.
183. Richardson GS, Scully RE, Nikrui N, et al: Common epithelialcancer of the ovary. N Engl J Med 1985;312:415-424.
184. Stanhope CR, Smith JP: Germ cell tumors. Clin Obstet Gynaecol1983;10:357-364.
185. Bezjian AA: Pelvic masses in pregnancy. Clin Obstet Gynaecol 1984;27:402-415.
186. Barber HRK: Manual of Gynecologic Oncology. Philadelphia, JBLippincott, 1980.
187. Karlen JR, Akbari A, Cook WA: Dysgerminoma associated withpregnancy. Obstet Gynecol 1979;53:330-335.
188. Taylor MH, Depetrillo AD, Turner AR: Vinblastine, bleomycin andcisplatin in malignant germ cell tumors of the ovary. Cancer 1985;56:1341\x=req-\1349.
189. Bosch A, Marcial VA: Carcinoma of the uterine cervix associatedwith pregnancy. AJR 1966;96:92-98.
190. Sylvester RK, Lobell M, Teresi ME, et al. Excretion of hydroxyureainto milk. Cancer 1987;60:2177-2178.
191. Durodola JI: Administration of cyclophosphamide during late preg-nancy and early lactation: A case report. J Natl Med Assoc 1979;71:165\x=req-\166.
on May 7, 2010 www.archinternmed.comDownloaded from