
Implantable Infusion Pump - Blue Shield of California · An implantable infusion pump is intended...
32
Medical Policy 1 7.01.41 Implantable Infusion Pump Section 7.0 Surgery Effective Date January 30, 2015 Subsection Original Policy Date March 5, 2012 Next Review Date January 2016 Description An implantable infusion pump is intended to provide long-term continuous or intermittent drug infusion. Possible routes of administration include intravenous, intra-arterial, subcutaneous, intraperitoneal, intrathecal, and epidural. The implantable infusion pump is surgically placed in a subcutaneous pocket under the infraclavicular fossa or in the abdominal wall, and a catheter is threaded into the desired position. Intrathecal and epidural catheter positions are both intraspinal; however, the intrathecal position is located in the subarachnoid space, which is past the epidural space and dura mater and through the theca of the spinal cord. A drug is infused over an extended period of time and may be delivered at a constant or variable rate by calibrating the implantable infusion pump per physician specifications. The drug reservoir may be refilled as needed by an external needle injection through a self-sealing septum in the implantable infusion pump. Bacteriostatic water or physiological saline is often used to dilute drugs. A heparinized saline solution may also be used during an interruption of drug therapy to maintain catheter patency. The driving mechanisms may include peristalsis, fluorocarbon propellant, osmotic pressure, piezoelectric disk benders, or the combination of osmotic pressure with an oscillating piston. Implantable infusion pumps can provide long-term drug infusion at constant or variable rates. Primary uses are delivery of chemotherapy agents and analgesics; several devices are commercially available. Related Policies • Continuous or Intermittent Monitoring of Glucose in Interstitial Fluid • Chronic Intermittent Intravenous Insulin Therapy • Pain Medication-Administration Through Pain Pumps Policy Implantable infusion pumps may be considered medically necessary when used to deliver drugs having FDA approval for this route of access and for the related indication for the treatment of patients with any of the following conditions: • Cancer in the following situations: o Primary liver cancer (intrahepatic artery injection of chemotherapeutic agents) o Metastatic colorectal cancer where metastases are limited to the liver (intrahepatic artery injection of chemotherapeutic agents)
Transcript of Implantable Infusion Pump - Blue Shield of California · An implantable infusion pump is intended...
Medical Policy
1
7.01.41 Implantable Infusion Pump Section 7.0 Surgery
Effective Date January 30, 2015
Subsection
Original Policy Date March 5, 2012
Next Review Date January 2016
Description
An implantable infusion pump is intended to provide long-term continuous or intermittent drug infusion. Possible routes of administration include intravenous, intra-arterial, subcutaneous, intraperitoneal, intrathecal, and epidural. The implantable infusion pump is surgically placed in a subcutaneous pocket under the infraclavicular fossa or in the abdominal wall, and a catheter is threaded into the desired position. Intrathecal and epidural catheter positions are both intraspinal; however, the intrathecal position is located in the subarachnoid space, which is past the epidural space and dura mater and through the theca of the spinal cord.
A drug is infused over an extended period of time and may be delivered at a constant or variable rate by calibrating the implantable infusion pump per physician specifications. The drug reservoir may be refilled as needed by an external needle injection through a self-sealing septum in the implantable infusion pump. Bacteriostatic water or physiological saline is often used to dilute drugs. A heparinized saline solution may also be used during an interruption of drug therapy to maintain catheter patency.
The driving mechanisms may include peristalsis, fluorocarbon propellant, osmotic pressure, piezoelectric disk benders, or the combination of osmotic pressure with an oscillating piston.
Implantable infusion pumps can provide long-term drug infusion at constant or variable rates. Primary uses are delivery of chemotherapy agents and analgesics; several devices are commercially available.
Related Policies
• Continuous or Intermittent Monitoring of Glucose in Interstitial Fluid
• Chronic Intermittent Intravenous Insulin Therapy
• Pain Medication-Administration Through Pain Pumps
Policy
Implantable infusion pumps may be considered medically necessary when used to deliver drugs having FDA approval for this route of access and for the related indication for the treatment of patients with any of the following conditions:
• Cancer in the following situations:
o Primary liver cancer (intrahepatic artery injection of chemotherapeutic agents)
o Metastatic colorectal cancer where metastases are limited to the liver (intrahepatic artery injection of chemotherapeutic agents)
Medical Policy
2
o Primary epithelial ovarian cancer (intraperitoneal infusion as component of chemotherapy)
• Severe, chronic, intractable pain (intravenous, intrathecal, and epidural injection of opioids), after a successful temporary trial of opioid or nonopioid analgesics by the same route of administration as the planned treatment. A successful trial is defined as greater than 50% reduction in pain after implementation of treatment. (See Policy Guidelines)
• Severe spasticity of cerebral or spinal cord origin in patients who are unresponsive to or who cannot tolerate oral baclofen therapy (intrathecal injection of baclofen*) (See Policy Guidelines)
Implantable infusion pumps are considered investigational for all other uses (e.g., chemotherapy for patients with head and neck cancers, gastric cancer, bone or soft tissue sarcomas, or skin cancers; heparin for thromboembolic disease; insulin for diabetes; antibiotics for osteomyelitis).
Policy Guidelines
Preliminary Trial of Intrathecal Drug Delivery
A preliminary trial of percutaneous intrathecal (intraspinal) drug delivery may be considered for the treatment of patients with the following conditions:
• Baclofen (Lioresal®) intrathecal therapy for severe, refractory spasticity or chronic intractable dystonia of cerebral* or spinal cord origin when there is failure of, contradiction, or intolerance to at least a 6 week trial of oral antispasticity agents (i.e., baclofen [Lioresal®]) and other less-invasive methods (e.g., physical therapy)
Note: Per the FDA, patients with spasticity due to traumatic brain injury should wait at least one year after the injury before consideration of long-term intrathecal baclofen therapy.
• Intrathecal (intraspinal) opiate or non-opiate medications, specifically approved by the U.S. Food and Drug Administration (FDA), for the treatment of severe, intractable chronic pain when the following exist:
o There is documented pathology (i.e., an objective basis for the pain complaint)
o Further surgical intervention or other treatment is not indicated or likely to be effective
o Patient has a life expectancy of greater than 3 months (less invasive techniques such as external infusion pumps provide comparable pain relief in the short term and are consistent with standard of care)
o Sufficient trial of opioids or other analgesics in adequate doses, with a fixed schedule (not on a PRN basis) dosing which have failed to relieve pain or the patient has developed intolerable side effects to systemic opioids or other analgesics
o Behavioral, psychological and social support stability* have been evaluated and indicate appropriateness of implantable therapy
Medical Policy
3
*Note: Attempts should be made to eliminate physical, psychological, and behavioral contributors to an exaggerated sensation of pain, and no active or untreated drug dependence should exist.
o Malignant pain (pain associated with primary or metastatic cancer) and failure of, or intolerance, or contraindications to non-invasive methods of pain control (e.g., psychological and cognitive/behavioral intervention, physical therapy, pharmacotherapy [e.g., opiate or non-opiates, antidepressants, anticonvulsants], minimally invasive interventions or other alternative therapies)
o Non-malignant pain including all of the following:
Intractable chronic pain, including but not limited to any of the following:
o Failed back surgery syndrome with low back pain and/or radicular pain
o Chronic arachnoiditis
o Visceral pain syndromes
o Complex regional pain syndrome (also known as reflex sympathetic dystrophy)
o Post-herpetic neuralgia and other neuropathic pain syndromes
o Phantom limb pain
o Peripheral neuropathies
o Spinal cord injuries
Documentation of failure of a 6 month trial of other conservative treatment modalities for pain management (e.g., pharmacotherapy [antidepressant, anti-epileptic, anti-inflammatory and analgesia medications]), and minimally invasive interventions such as spinal injections)
Documentation of active participation in a reasonable trial of an aggressive active rehabilitative exercise program (e.g., physical therapy), if appropriate and not contraindicated
Documentation from a primary care physician, neurologist, physiatrist, psychiatrist or psychologist, supports the absence of untreated, underlying psychological conditions or psychosocial issues (e.g., depression, drug and alcohol dependence) as a contributor to chronic pain and that benefit will occur with implantation
The use of a percutaneous intrathecal drug delivery system for other indications, including other chronic pain conditions, will be reviewed on a case-by-case basis for medical necessity.
*Recommended medications are those approved by the FDA for infusion at the site requested (e.g., intrathecal, intravenous, intra-arterial, subcutaneous).
See applicable Blue Shield Pharmacy Policies.
Medical Policy
4
Benefit Application
Benefit determinations should be based in all cases on the applicable contract language. To the extent there are any conflicts between these guidelines and the contract language, the contract language will control. Please refer to the member's contract benefits in effect at the time of service to determine coverage or non-coverage of these services as it applies to an individual member.
Some state or federal mandates (e.g., Federal Employee Program (FEP)) prohibit Plans from denying Food and Drug Administration (FDA) - approved technologies as investigational. In these instances, plans may have to consider the coverage eligibility of FDA-approved technologies on the basis of medical necessity alone.
Rationale
Background
An implantable infusion pump is intended to provide long-term continuous or intermittent drug infusion. Possible routes of administration include intravenous, intra-arterial, subcutaneous, intraperitoneal, intrathecal, and epidural. The implantable infusion pump is surgically placed in a subcutaneous pocket under the infraclavicular fossa or in the abdominal wall, and a catheter is threaded into the desired position. Intrathecal and epidural catheter positions are both intraspinal; however, the intrathecal position is located in the subarachnoid space, which is past the epidural space and dura mater and through the theca of the spinal cord.
A drug is infused over an extended period of time and may be delivered at a constant or variable rate by calibrating the implantable infusion pump per physician specifications. The drug reservoir may be refilled as needed by an external needle injection through a self-sealing septum in the implantable infusion pump. Bacteriostatic water or physiological saline is often used to dilute drugs. A heparinized saline solution may also be used during an interruption of drug therapy to maintain catheter patency.
The driving mechanisms may include peristalsis, fluorocarbon propellant, osmotic pressure, piezoelectric disk benders, or the combination of osmotic pressure with an oscillating piston.
Regulatory Status
Several implantable infusion pumps have been approved by FDA through the premarket approval process, including, but not limited to, the Medtronic SynchroMed® (Fridley, MN) family of pumps; the Medtronic IsoMed® infusion system (Minneapolis, MN); the Flowonix™ Prometra® programmable pump (Mount Olive, NJ); and Shiley Infusaid® pumps (Norwood, MA). In August 2012, FDA approved theMedStream™ Programmable Infusion System (Codman and Shurtleff, a division of DePuy), which includes an implantable pump, for intrathecal delivery of baclofen in patients with spasticity. FDA product code: LKK
Chemotherapy for Cancer Patients
Primary Liver Cancer
No randomized controlled trials (RCTs) have evaluated whether hepatic arterial infusion of chemotherapy in patients with primary liver cancer improves health outcomes. A 2013 comparative effectiveness review by the Agency for Healthcare Research and Quality (AHRQ) evaluated local therapies for unresectable primary hepatocellular carcinoma
Medical Policy
5
(HCC) in patients ineligible for surgical resection or transplantation.1 Treatments reviewed included ablative therapies (e.g., radiofrequency ablation), radiotherapy (e.g., intraluminal brachytherapy), and embolization (e.g., transarterial embolization either with [TACE] or without [TAE] chemotherapy). Although TACE delivers chemotherapy and embolic materials through hepatic arterial infusion, this procedure generally is performed by an interventional radiologist and does not require implantation of an infusion pump. Thus, this AHRQ report does not address the use of implantable infusion pumps for delivery of chemotherapy for primary liver cancer.
Several case series were identified. Most recently, Jarnagin et al (2009) reported on 34 patients with unresectable primary liver cancer who received hepatic arterial infusion of floxuridine and dexamethasone.2 Sixteen of 34 patients (47%) had a partial response (PR) to treatment. Median survival was 29.5 months; the 2-year survival rate was 67%. In addition, Smith et al (1984) studied 11 patients and found a complete response to chemotherapy in 1 patient and PRs in 6 patients.3 Atiq et al found a partial response in 4 of 10 patients (40%) with unresectable liver cancer treated with intrahepatic chemotherapy delivered through an implantable pump.4
This evidence is limited but suggests that some patients, with limited alternative treatment options, may benefit from arterial infusion of chemotherapy.
Liver Metastases from Colorectal Cancer
A 2012 AHRQ comparative effectiveness review evaluated local hepatic therapies for colorectal cancer (CRC) metastases in patients ineligible for systemic chemotherapy.5 Like the AHRQ review previously mentioned, local therapies included ablation, radiotherapy, and embolization. Four case series of chemotherapy delivered via hepatic artery infusion by an indwelling pump were identified. Two retrospective case series assessed a total of 67 patients who were refractory to systemic chemotherapy, and 2 case series assessed a total of 36 patients who received concomitant systemic chemotherapy. Infused chemotherapies were mitomycin plus gemcitabine or 5-fluoruracil; systemic chemotherapy regimens varied. Median overall survival (OS) was 9.7 months and 6.7 months in the refractory group, and 30.1 months and 22.0 months in the systemic chemotherapy group. Grade 3 adverse events (AEs) attributed to hepatic artery infusion included leukocytopenia, hyperbilirubinemia, hypersensitivity reaction, and neuropathy. This evidence was considered insufficient to form any conclusion about the comparative benefits (e.g., OS, quality of life) or harms (i.e., AEs) of hepatic artery infusion for these patients.
For patients who are eligible for systemic chemotherapy, a 2009 Cochrane review compared hepatic arterial infusion versus systemic chemotherapy in patients with unresectable liver metastases from CRC.6 Ten RCTs that evaluated a total of 1277 patients were included. Nine of these provided data on tumor response. The response rate was significantly higher in the hepatic arterial infusion group (198/461 [43%]) than the systemic chemotherapy group (81/440 [18%]). The pooled risk ratio (RR) was 2.26 (95% confidence interval [CI]: 1.80 to 2.84). However, there was not a significantly higher survival rate associated with hepatic arterial infusion chemotherapy. The mean weighted median OS times were 15.9 months with hepatic arterial infusion chemotherapy and 12.4 months with systemic chemotherapy (pooledhazard ratio [HR], 0.90; 95% CI: 0.76 to 1.07). Adverse effects and quality-of-life outcomes were not reported.
Ammori et al (2014) reported on a cohort of 373 patients with unresectable colorectal liver metastases who received hepatic artery infusional chemotherapy and systemic chemotherapy at a single U.S. center.7 The primary outcome was the proportion of patients who converted to complete resection or ablation. Two patients died due to

Medical Policy
6
postoperative complications after pump placement; AEs associated with the pump (e.g., biliary sclerosis, malfunction) occurred in 13% of patients. Ninety-three patients (25%) achieved the primary outcome at a median of 7 months. Median and estimated 5-year survival (from the time of pump placement) was 59 months and 47%, respectively, in patients who underwent resection or ablation, and 16 months and 6%, respectively, in patients who did not (log-rank test, p<0.001).
This evidence suggests that arterial infusion of chemotherapy improves response rates for patients with CRC metastatic to the liver compared with systemic chemotherapy. The impact on survival is uncertain.
Head and Neck Cancers
Several studies have evaluated interventions that combine radiotherapy and concomitant intra-arterial cisplatin (known as RADPLAT) in patients with head and neck cancer. These studies used intra-arterial delivery of cisplatin via an intra-arterial catheter rather than an implantable pump. Although an implantable infusion pump was not used, the principle of treatment is similar, so that these studies have some relevance to the evaluation of infusion pumps.
In 2006, Hoebers et al in The Netherlands randomized patients with stage 3/4 head and neck squamous cell carcinoma to radiotherapy with standard intravenous (IV) cisplatin (n=21) or high-dose intra-arterial cisplatin (n=14).8 Rates of acute mucositis and hematological toxicity did not differ significantly between groups; however, there was a higher rate of acute renal toxicity in the IV group (30%) compared with the intra-arterial group (0%). Over 2 years, there were no significant differences between treatment groups in locoregional control of disease, disease-free survival, or OS.
A study by Ackerstaff et al (2009) examined 17 quality-of-life scales at several time points after treatment with radiotherapy with IV or intra-arterial cisplatin.9 The study included 207 patients with inoperable advanced head and neck cancer. The only statistically significant difference between groups was in the nausea/vomiting scale at 7 weeks, at which time the incidence of symptoms was higher in the IV compared with the intra-arterial group. Otherwise, quality-of-life symptoms were similar in the 2 groups.
Evidence from 2 RCTs did not find a clear advantage of intra-arterial chemotherapy delivered via an intra-arterial catheter compared with IV chemotherapy in combination with radiotherapy for patients with head and neck cancer. Therefore, it is not likely that similar agents delivered via an implantable infusion pump would improve outcomes.
Primary Epithelial Ovarian Cancer
A 2011 Cochrane review examined literature on whether an intraperitoneal component of chemotherapy improves ovarian cancer outcomes compared with IV chemotherapy-only.10 Nine RCTs with a total of 2119 patients were identified; 6 trials were considered high quality. In a pooled analysis of data from 8 trials, there was a significantly lower rate of mortality with an intraperitoneal component of chemotherapy compared with no intraperitoneal component (HR=0.81; 95% CI: 0.72 to 0.90). Moreover, a pooled analysis of data from 5 trials found that an intraperitoneal component of chemotherapy was associated with a significantly longer disease-free interval (HR=0.78; 95% CI: 0.70 to 0.86). However, an intraperitoneal component of chemotherapy was associated with significantly more adverse effects (e.g., infection, fever, pain, gastrointestinal symptoms). For example, a pooled analysis of 3 trials found a significantly higher infection rate when there was an intraperitoneal component of chemotherapy compared with IV-only chemotherapy (relative risk [RR], 3.34; 95% CI: 2.06 to 5.43).

Medical Policy
7
An example of one of the individual RCTs is a high-quality RCT with a relatively large number of patients published by Markman et al in 2001.11 This was a multicenter study conducted in the United States that included women diagnosed with stage 3 epithelial ovarian cancer who entered the study within 6 weeks of surgery. Patients were randomized to receive either standard dose IV cisplatin/paclitaxel for 6 courses or 2 cycles of moderately high-dose carboplatin, followed by 6 courses of IV paclitaxel and intraperitoneal cisplatin. A total of 523 patients entered the trial, and 61 (12%) were subsequently found to be ineligible for reasons including the wrong stage of cancer or inadequate surgery. Of the remaining 462 eligible patients, 227 were in the IV chemotherapy-only group and 235 were in the intraperitoneal chemotherapy component group. At the time of data analysis, 103 (45%) of 227 patients in the IV-only group and 126 (54%) of 235 in the intraperitoneal chemotherapy-component group were still alive. Improvement in survival with intraperitoneal chemotherapy was of borderline statistical significance (RR of death, 0.81 [95% CI: 0.65 to 1.00]). Progression-free survival (PFS) was significantly longer in the intraperitoneal chemotherapy-component group compared with the IV chemotherapy-only group (median time to recurrence, 27.9 months vs. 22.2 months, respectively; p=0.01). Several adverse events occurred more commonly in the intraperitoneal chemotherapy-component group than in the IV chemotherapy-only group. These included grade 3 to 4 gastrointestinal events (37% vs. 17%, respectively) and platelet toxicity (49% vs. 3%, respectively). Two patients in each group died of causes considered to be related to chemotherapy.
Evidence from multiple RCTs, including some of high-quality, and systematic reviews, indicates that intraperitoneal chemotherapy for patients with primary epithelial ovarian cancer has a significant impact on PFS and likely also improves OS. This benefit is accompanied by an increased risk of adverse effects with intraperitoneal infusions, including infections, pain, and gastrointestinal symptoms.
Gastric Cancer
A 2011 systematic review examined RCTs and observational studies of intraperitoneal chemotherapy used to treat gastric cancer.12 The authors identified 14 studies: 2 RCTs, 2 case-control studies, and 10 single cohort studies. One RCT compared groups of patients who did and did not receive intraperitoneal taurolidine after tumor resection and did not find statistically significant differences in outcomes. The other RCT (n=118) found a significantly higher rate of survival in patients who received either intraperitoneal chemotherapy plus intraoperative peritoneal lavage or intraperitoneal chemotherapy only in addition to surgery versus surgery only. (Additionally, all patients in the second study received adjuvant oral 5- fluorouracil derivatives for 2 years.) Authors of the systematic review recommended that future studies evaluate preoperative or intraoperative intraperitoneal chemotherapy in association with systemic chemotherapy. This evidence on intraperitoneal chemotherapy for treating gastric cancer is insufficient to determine whether health outcomes are improved.
Mixed Sarcoma and Skin Cancers
Liu et al (2014) reported on a cohort of 31 patients with ulcerative skin cancers or sarcomas who received intra-arterial chemotherapy at a single center in China.13 Patients had squamous cell skin carcinoma (n=9), synovial sarcoma (n=6), malignant fibrous histiocytoma (n=5), liposarcoma (n=3), osteosarcoma (n=3), malignant melanoma (n=2), epidermoid sarcoma (n=2), or dermatofibrosarcoma protuberans (n=1). Infusion pumps were implanted in subcutaneous tissue near the involved subclavian artery for 10 patients with upper extremity disease and near the involved femoral artery for 21 patients with lower extremity disease. All patients received intra-arterial cisplatin and epirubicin at 2- to 3-week intervals for 2 (n=9) or 3 (n=22) cycles;

Medical Policy
8
patients with squamous cell carcinoma additionally received bleomycin, and patients with melanoma received dacarbazine. Twenty-seven patients (87%) achieved pain remission; 19 patients (61%) had complete remission (no pain), and 8 patients (26%) had partial remission (significantly reduced pain with uninterrupted sleep and normal life). Nineteen patients underwent tumor resection after tumor shrinkage with chemotherapy. Using World Health Organization criteria for chemotherapy response in ulcerating tumors, 22 patients (71%) achieved remission; 7 patients (23%) had complete remission (complete healing without rerupture for >1 month), and 15 patients (48%) had partial remission (50% shrinkage of the ulcer surface without rerupture for >1 month). Three patients had tumor recurrence, and 3 patients underwent lower leg amputation. Among 19 patients who underwent local tumor resection after chemotherapy-induced tumor shrinkage, local chemotherapy reaction by pathologic examination of excised tissue was observed in all patients, half of which were severe. Other AEs included gastrointestinal effects, bone marrow suppression, and visceral injury, which were considered milder than seen with traditional chemotherapy. Due to lack of a control group, relative improvement in net health outcomes in comparison with current treatments is unknown. Therefore, implanted infusion pumps to deliver chemotherapy in patients with sarcoma and ulcerative skin cancers are considered investigational.
Pain
Cancer Pain
One systematic review of the literature was identified; it was published in 2010 by Myers et al.14 They identified 12 RCTs on intraspinal techniques for managing pain in cancer patients; studies were required to report pain as an outcome measure using a validated scale. The investigators did not identify the type or types of cancer addressed in individual studies and did not pool study findings. Two RCTs specifically addressed implantable infusion pumps. One compared intrathecal morphine delivered via an implantable infusion pump plus medical management (n=101) to medical management alone (n=99) in patients with refractory cancer pain. The difference between groups in clinical success (defined as a minimum 20% reduction in pain score and a minimum 20% reduction in drug toxicity at 4 weeks) reached borderline statistical significance, favoring the implantable pump group over the control group (85% vs. 71%, respectively, p=0.05). The proportion of patients who experienced a minimum 20% pain score reduction was 52% in the implantable pain pump group and 39% in the control group; this was not a statistically significant difference (p=0.55). The other RCT on implantable pumps compared epidural morphine delivered as a continuous infusion by the Infusaid pump with intermittent delivery by a Port-a-Cath® (Deltec, St. Paul, MN). The 2 groups did not differ significantly in their pain scores; scores were low in both groups, and the trial, which had only 29 participants, was likely underpowered. Evidence from this systematic review indicates that intraspinal techniques may be appropriate for select cancer patients with intractable cancer pain but there is a shortage of high-quality RCTs.
Noncancer Pain
In 2013, the American Society of Interventional Pain Physicians (Falco et al) published a systematic review of intrathecal infusion for the treatment of chronic noncancer pain.15 The outcome of interest was pain relief, defined as a minimum 50% reduction of pain in at least 40% of patients, or a minimum 3-point reduction in pain scores. Both short-term (<12 months) and long-term (≥12 months) outcomes were considered. Twenty-eight studies were identified, but 21 were excluded for not meeting 1 or more inclusion criteria (e.g., outcomes not related to pain relief; sample size <50; minimum quality assessment). All 7 included studies were retrospective or prospective cohort studies. Six studies that each reported short-term (668 patients) or long-term (637 patients) pain outcomes
Medical Policy
9
indicated reduced pain with intrathecal opioids. The authors concluded that evidence for intrathecal opioid infusion in chronic noncancer pain is limited. Suggested contraindications to intrathecal opioid therapy (e.g., active infection) and indications to proceed with therapy (e.g., oral opioid therapy contraindicated) are provided.
In 2009, Patel et al published a systematic review of intrathecal infusion pumps used to treat chronic noncancer pain.16 Included studies evaluated an intrathecal device (programmable or fixed infusion rate), stated a specific indication and the drug that was injected, followed patients for at least 12 months, and included at least 25 patients. In addition, the investigators rated study quality; included studies scored at least 50 of 100 on a methodologic quality scale. The primary outcome of interest to the systematic review was pain relief. A total of 15 studies on intrathecal infusion for noncancer pain were identified; however, 6 did not have sufficient follow-up, 4 included fewer than 25 patients, and 1 had unacceptably low quality, leaving 4 eligible studies. All of the studies were observational and involved intrathecal opioid administration; sample sizes ranged from 69 to 120. Most patients experienced lumbospinal pain. Two of the 4 studies showed positive results for pain relief, 1 study had negative results, and results were unavailable for the fourth study. The authors of the systematic review acknowledged the paucity of literature and lack of RCTs. Using the grading system developed by Guyatt et al, the authors concluded that a 1C recommendation for the use of intrathecal infusion systems in chronic noncancer pain was appropriate; that is, a strong recommendation based on low-quality or very low-quality evidence in which the benefits outweigh the risks and the recommendation may change when higher quality evidence becomes available.17
In 2012, Hamza et al published a 36-month prospective cohort study of low-dose intrathecal opioids for chronic nonmalignant pain using the SynchroMed II programmable pump.18 Sixty-one patients with severe intractable pain who had failed multiple lines of pain therapy and were referred for intrathecal treatment underwent a blinded trial of intrathecal opioids. Three patients who experienced pain relief in response to saline were excluded. Mean age of the 58 included patients was 59±14 years, and mean duration of symptoms was 6±2 years. Pain syndromes were failed back surgery syndrome in 60% of patients, chronic low back pain in 28%, and chronic complex regional pain syndrome, abdominal pain, or pelvic pain in 12%. All patients were weaned from opioids for 7 to 10 days before pump implantation and participated in a 12-week physical therapy program commencing at 8 weeks post implant. At 36 months, there was a 55% reduction from baseline worst pain score (from 8.91 to 4.02 on the Brief Pain Inventory [BPI] 0-10 scale; p=0.012) and a 54% reduction from baseline average pain score (7.47 to 3.41; p<0.001). Improvements in physical function and behavior (mood, relations, sleep) as measured by the BPI also were statistically significant. Mean intrathecal opioid dose increased 11% from 1.4 to 1.6 morphine equivalents daily. Mean oral opioid dose decreased 97% from 129 to 4 morphine equivalents daily. AEs were reported to be mild and limited (wound infection and pruritus in 3 patients [5%] each; peripheral edema and seroma in 2 patients [3%] each).
Several additional case series were identified in recent literature searches. In 2010, Atli et al published a single-center study conducted in the United States.19 This was a retrospective review of 57 patients referred for pain management who received an implanted intrathecal infusion pump. Twenty-eight of the 57 patients (49%) had failed back surgery syndrome, 16 (28%) had neuropathic pain, and the remaining 13 (23%) had a variety of diagnoses. Preservative-free opioid (usually morphine) was infused, and patients also could receive oral opioid; adjustments in dosage could be made at any time. Forty-nine of 57 patients (86%) completed the 3-year follow-up. At the time of the first pump refill (3-6 months), 23 of 49 study completers (47%) reported having a 50% or greater reduction in pain from baseline, as measured on a 10-point visual analog scale.

Medical Policy
10
The proportion of responders decreased over time; at the 3- year follow-up, 9 of 49 patients (18%) had a 50% or greater reduction in pain from baseline. These 9 patients represented 39% of those who met the 50% reduction threshold at the first refill. The use of oral opioids was significantly less at the 1- and 3-year follow-ups than at baseline (p not reported). Mean baseline oral opioid dose in morphine equivalents was 184 mg/24 hours. At 1 and 3 years, mean oral doses were 44 mg/24 hours and 58 mg/24 hours, respectively. At 3 years, 12 of 49 patients (25%) had ceased all oral opioid use. In contrast, mean dose of intrathecal opioids significantly increased during follow-up compared with the dose at discharge after pump implantation. The mean dose was 6.5 mg/24 hours at discharge; 9.3 mg/24 hours at 1 year; and 12.2 mg/24 hours at 3 years. Complications occurred in 10 of 57 patients (17.5%); these included 5 infections, 3 catheter revisions, 2 seromas at the pump site, and 2 intrathecal granulomas. Another retrospective case series conducted in the U.S. and published in 2011 included 126 noncancer intractable pain patients.20 Patients received intrathecal opioids only (n=72) or opioids and bupivacaine (n=54). Outcomes were evaluated 12 months after pump implantation. Pain intensity was assessed using an 11-point numeric rating scale, ranging from 0 (no pain) to 10 (worst imaginable pain). In the group that began with opioids only, mean (SD) pain intensity score decreased significantly from 7.42 (2.1) at baseline to 5.85 (2.8) at 12 months (p<0.001). In the opioid plus bupivacaine group, the mean pain intensity score decreased from 7.35 (2.1) at baseline to 5.03 (2.4) at 12 months (p<0.001).
In 2012, Duarte et al in the U.K. published a case series with long-term follow-up on 20 patients with chronic nonmalignant pain who received intrathecal delivery of opioid analgesics.21 Patients were followed for a mean of 13.5 years (range, 10.4-17.9 years). At 4- and 13-year assessments, outcomes were significantly improved compared with baseline. However, outcomes did not significantly improve between 4 and 13 years. For example, mean pain intensity (measured on an 11-point scale, ranging from 0 [no pain] to 10 [worst pain]) was 8.65 (SD=0.29) at baseline, 4.95 (SD=0.53) at 4 years post treatment, and 5.30 (SD=0.35) at 13 years post treatment. Similarly, mean quality-of-life score (0 represents no interference with quality of life and 10 represents maximum interference) was 8.45 (SD=0.49) at baseline, 4.95 (SD=0.69) at 4 years, and 4.45 (SD=0.48) at 13 years.
In summary, evidence on the use of infusion pumps for chronic, noncancer pain comprises numerous uncontrolled observational studies. These studies, which are limited methodologically, report that pain and quality of life is improved with the use of infusion pumps.
Severe Spasticity
The evidence base comprises observational studies and 2 systematic reviews of these studies. A 2014 systematic review of intrathecal baclofen for spasticity in patients with traumatic or nontraumatic spinal cord injury identified 8 studies (total N=162).22 At follow-up (range, 2-41 months), reductions in mean Modified Ashworth Scale (scored 0-5) were statistically significant, from 3.1 to 4.5 (limb rigidity or considerable increase in tone) at baseline to 1.0 to 2.0 (slight increase in tone; p<0.005). AEs associated with baclofen, pump/catheter malfunction (e.g., dislodging, kinking, breaking), and infections/seromas at the incision site were reported. Baclofen overdose in 3 patients (2%) and withdrawal seizure in 1 patient (<1%) were attributed to pump malfunction.
The other systematic review, published in 2011 by Pin et al, focused on intrathecal baclofen therapy for spasticity and/or dystonia of cerebral origin in children and adolescents.23 The authors identified 16 uncontrolled studies with a total of 227 participants. All studies were judged to be low quality. Most outcomes were intermediate measures (i.e., at the level of body structures or functions), such as range of motion and
Medical Policy
11
muscle strength; several studies used objective outcomes (e.g., motor function at the level of activities or participation as assessed by the Gross Motor Function Measure [GMFM], laboratory-based gait analysis, or gait assessment tools). Effects of intrathecal baclofen therapy were greater in patients who were ambulatory at baseline compared with those who were nonambulatory. AEs were not consistently defined and reported but appeared to be common. One study that used objective outcomes was published in 2011 by Motta et al in Italy.24 This study found a statistically significant increase in GMFM score after 1 year. Median GMFM score (as a percentage of maximum score) in 30 cerebral palsy patients with spasticity who received intrathecal baclofen increased from 65.0 to 69.4 (p=0.004).
In 2011 (after the Pin et al literature search), Morton et al in the U.K. published findings of a nonrandomized controlled study of intrathecal baclofen therapy in nonambulatory children with severe spastic cerebral palsy.25 Patients who responded to a one-time test dose of 50 mcg intrathecal baclofen were fitted for a pump and placed on a waiting list for surgery. Investigators compared patients who had been on the waiting list between 6 to 12 months (group 1, n=18) with patients who had undergone surgery (group 2, n=20). Mean time between baseline and outcome assessment was 8.5 months in group 1 and 9.5 months in group 2. There was no statistically significant difference between the 2 groups in the primary outcome measure, the Pediatric Evaluation of Disability Inventory. The authors noted, however, that given the small number of patients recruited, the study was underpowered to detect statistically significant differences between groups on this outcome. Several secondary outcomes favored group 2, including scores on the Modified Ashworth Scale (difference between groups, 1.7; p=0.008), scores on the Penn Spasm Scale (difference between groups, -1.3; p=0.001) and the range-of-motion score (difference between groups, 8.3; p=0.005).
A small 2012 study compared mode of administration of intrathecal baclofen in 38 adults with muscle hypertonia due to brain injury or spinal cord disorder who were receiving intrathecal baclofen.26 Pumps were programmed to deliver a single daily bolus of baclofen with low background continuous dose (intervention group) or a continuous equivalent daily dose (controls). For patients receiving 75 to 85 mg of baclofen daily, a neurophysiologic measure of spasticity (H-reflex in the soleus [calf] muscle) improved statistically significantly more in the intervention group than in controls. For patients receiving 100 to 150 mg of baclofen daily, the difference between groups was not statistically significant.
Several authors have reported on long-term (1-14 years) outcomes in patients receiving intrathecal baclofen for treatment of intractable spasticity or dystonia.
• Of 158 adults at a single center in France, 28 (18%) experienced an AE within 12 months of surgical insertion of the pump.27 Most AEs (58%) occurred during the first month after surgery and were commonly related to the insertion site (scar dehiscence, hematoma; 53%), device dysfunction or migration (29%), and adverse effects of baclofen (18%).
• Margetis et al (2014) reported 2-year outcomes of 14 ambulatory adults with hereditary spastic paraplegia.28 All patients experienced a reduction in lower limb spasticity as measured by Modified Ashworth Scale; mean (SD) scores reduced from 2.6 (0.8) (slight-to-moderate increase in tone) to 0.7 (0.9) (no-to-slight increase in tone; paired-samples t test, p=0.000). Walking ability as assessed by a modified pediatric scale (functional walking scale of the Gillette Functional Assessment Questionnaire, scored 1-10) improved from a mean (SD) of 5.9 (1.7) (walks > 15-50 feet outside but uses a wheelchair for community distances) to 7.4 (2.0) (walks community distances but requires moderate assistance on uneven
Medical Policy
12
terrain, e.g., curbs; paired-samples t test, p=0.001). A responder analysis was not reported. Adverse events included catheter fracture in 2 patients. Ghosh et al (2013) reported 3-year experience of 119 children (mean age, 13 years) at a single U.S. center.29 Five patients (4%) underwent pump removal due to lack of efficacy. Mechanical complications requiring pump and/or catheter revision occurred in 19%, infections in 22%, and meningitis in 6%.
• Vles et al (2013) reported long-term (6-9 years) follow-up of 17 nonambulant children (mean age at enrollment: 13 years) with cerebral palsy who had participated in a Dutch trial of continuous intrathecal baclofen.30 Previously observed positive effects on pain, ease of care, and mental health of the child were maintained at follow-up.
• Of 430 children (mean age, 13 years) followed for a mean of 8 years at a single center in Italy, 25% had 1 or more complications: 15% experienced a problem with the catheter (most commonly within 12 months after implant), 9% experienced an infection, 5% a cerebrospinal fluid leak, and 1% a problem related to the pump.31
• At 10 years or more of follow-up, 24 adults at a single U.S. outpatient spasticity clinic reported on average: low levels of pain, moderate life satisfaction, infrequent spasms (mild-to-moderate severity), and few adverse effects (normal sleepiness, low-to-moderate fatigue).32
In summary, evidence from case series and nonrandomized, comparative studies report improvements in spasticity for patients treated via implantable infusion pumps. However, high-quality RCTs to confirm this benefit are lacking.
Implanted Infusion Pumps for Other Indications
Type 1 Diabetes Mellitus
A small body of literature reports on outcomes of continuous peritoneal insulin infusion (CPII) for patients with poorly controlled type I diabetes mellitus (DM), including a few small RCTs and a systematic review that included several RCTs.33-35 These studies reported decreased hypoglycemic episodes, and some reported improved glucose control compared with usual care. However, larger, high-quality trials are needed to determine whether this approach improves outcomes and whether it is equivalent to treatment alternatives for patients with poorly controlled type I DM.
Systematic reviews, meta-analyses, or large RCTs on the use of implanted infusion pumps for other indications were not identified.
Ongoing and Unpublished Clinical Trials
An online search of ClinicalTrials.gov identified 4 ongoing RCTs that are evaluating the use of implantable infusion pumps in a variety of conditions. These are listed next. Additionally, Bonouvrié et al are conducting an RCT in 30 children (age, 4-25 years) with dystonic cerebral palsy.36 Patients will be randomized to 3 months of continuous intrathecal baclofen or placebo, after which all patients will receive intrathecal baclofen for 9 months due to ethical concerns related to placebo treatment for longer than 3 months in this population. The primary efficacy outcome is change in activities of and participation in daily life measured by Goal Attainment Scaling at 3 and 12 months. Individualized goals and definitions of response in Goal Attainment Scaling permits are scored in a standardized way to permit comparisons between groups. Secondary outcomes include changes in dystonia, spasticity, pain, comfort, and sleep related breathing disorders (Netherlands Trial Register: NTR3642).

Medical Policy
13
• SISTERS: Spasticity in Stroke Study (NCT01032239): This RCT compares intrathecal baclofen therapy with best medical treatment for patients with severe spasticity for at least 6 months after stroke. The primary outcome is change in Modified Ashworth Scale. Estimated enrollment is 88 patients, and the expected date of completion is March 2017.
• Regional Versus Systemic Chemotherapy in the Treatment of Unresectable Pancreatic Cancer (NCT01665625): This open-label RCT compares systemic gemcitabine therapy with continuous regional delivery of gemcitabine using an implanted percutaneous left subclavian artery port-catheter drug delivery system in patients with inoperable pancreatic carcinoma. The primary outcome is OS. Estimated enrollment is 90 patients, and the expected date of completion is February 2016.
Clinical Input Received from Physician Specialty Societies and Academic Medical Centers
While various physician specialty societies and academic medical centers may collaborate with and make recommendations during this process, through the provision of appropriate reviewers, input received does not represent an endorsement or position statement by the physician specialty societies or academic medical centers, unless otherwise noted.
2012 Input
In response to requests, input was received through 1 physician specialty society and 3 academic medical centers while this policy was under review in 2012. Clinical input focused on implantable infusion pumps for treating patients with cancer; other potential indications were not addressed. There was consensus that implantable infusion pumps may be considered medically necessary for treating patients with primary liver cancer, metastatic colorectal cancer and epithelial ovarian cancer. Reviewers from 3 of 4 organizations disagreed that implantable infusion pumps are medically necessary for providing chemotherapy in patients with head and neck cancer. There was consensus among reviewers that implantable infusion pumps are investigational for all other uses in cancer patients, e.g., chemotherapy for patients with gastric cancer.
Summary of Evidence
A large body of evidence on the use of infusion pumps exists, but the quality of the literature varies by condition. For patients with primary liver cancer, evidence is limited. However, these patients have few alternative treatment options, and some may benefit from hepatic arterial infusion of chemotherapy.
Clinical input supported the use of implantable infusion pumps for this indication, which is therefore considered medically necessary.
For patients with colorectal cancer metastatic to the liver, a 2009 meta-analysis of randomized controlled trials (RCTs) found that hepatic arterial infusion of chemotherapy with implanted infusion pumps improves tumor control. For women with primary epithelial ovarian cancer, evidence from RCTs and a systematic review of RCTs indicates that an intraperitoneal infusion of chemotherapy can lead to improved survival and progression-free survival compared with intravenous chemotherapy only. Benefits of intraperitoneal chemotherapy must be weighed against the risk of adverse events, which has been found to be higher with an intraperitoneal component of chemotherapy. For patients with chronic cancer pain, a systematic review of RCTs concluded that pain symptoms were reduced in patients who used an infusion pump. For these 3 indications, evidence is
Medical Policy
14
sufficient to conclude that the use of an implantable infusion pump improves outcomes and therefore may be considered medically necessary.
There is insufficient evidence suggesting that chemotherapy delivered through implantable infusion pumps improves health outcomes for patients with head and neck cancer, gastric cancer, bone or soft tissue sarcomas, or skin cancers. Clinical input did not support use of this technology for these types of cancer. Thus, these indications are considered investigational.
For patients with intractable, noncancer pain, evidence comprises uncontrolled studies that report improvements in pain and quality of life with use of an implantable infusion pump. Additionally, guidelines from specialty societies support the use of infusion pumps for this indication. For patients with severe spasticity, evidence from case series and RCTs reports improvements in symptoms, and there is support from specialty society guidelines for use in spasticity. Because of the strong rationale for use, the suggestive evidence, and the support from clinical guidelines, infusion pumps may be considered medically necessary for chronic, intractable noncancer pain and for severe spasticity.
SUPPLEMENTAL INFORMATION
Practice Guidelines and Position Statements
Cancer Treatment
Current guidelines (2014) from the National Comprehensive Cancer Network (NCCN) include the following statements:
• Colon cancer
o “Placement of a hepatic arterial port or implantable pump during surgical intervention for liver resection with subsequent infusion of chemotherapy directed to the liver metastases through the hepatic artery (e.g., hepatic arterial infusion [HAI]) remains an option.”37
• Hepatocellular carcinoma
o Intra-arterial chemotherapy is recommended as a treatment option for patients with unresectable disease who are not transplant candidates (Category 2A recommendation: based on lower level evidence with uniform NCCN consensus that the intervention is appropriate).38
• Intrahepatic cholangiocarcinoma
o For patients with unresectable or metastatic disease, and for patients with residual local disease post-resection, systemic or intra-arterial chemotherapy may be used in a clinical trial or at experienced centers (Category 2A recommendation).38
• Ovarian cancer
o Intraperitoneal chemotherapy is recommended for patients with stage 2-3 disease, with less than 1 cm optimally debulked tumor (Category 1 recommendation for stage 3 disease: based on high-level evidence, there is uniform NCCN consensus that the intervention is appropriate; Category 2A recommendation for stage 2 disease).39
Current NCCN guidelines for head and neck cancers40, soft tissue sarcoma41, bone cancer42, basal and squamous cell skin cancers43, and melanoma44, do not include implantable infusion pumps. Isolated limb perfusion/infusion, which is a treatment option
Medical Policy
15
for select patients with unresectable soft tissue sarcoma41 and melanoma44 does not involve insertion of an infusion pump.
The 2014 information summaries from the National Cancer Institute state the following:
• Colon cancer
o For patients with Stage 4 and recurrent colon cancer with liver metastases, hepatic intra-arterial chemotherapy with floxuridine has had higher overall response rates but not a consistent improvement in survival when compared with systemic chemotherapy.45
• Primary liver cancer
o For patients with localized and locally advanced unresectable adult primary liver cancer, infusion of chemotherapeutic agents with a subcutaneous portal or implantable pump via a catheter placed in the hepatic artery is described as a standard treatment option.46
Cancer Pain
Current NCCN guidelines (version 2.2014) for treatment of adult cancer pain recommend placement of epidural, intrathecal, or regional infusion pumps to deliver analgesic or anesthetic drugs as indicated.47
Noncancer Pain
Publications from the American Society of Interventional Pain Physicians include:
• Evidence-based guidelines (updated in 2009) on interventions for managing chronic spinal pain.48 The guidelines state that there is strong evidence to support the use of implantable intrathecal drug administration systems with proper patient selection criteria.
• A 2013 systematic review of intrathecal infusion systems for long-term management of chronic noncancer pain, as previously reviewed.15 The authors concluded that the evidence for intrathecal opioid infusion in this setting is limited. Intrathecal opioid therapy may be indicated in select patients, e.g., those with contraindications to oral opioid therapy.
Spasticity
In July 2012, Britain’s National Institute for Health and Care Excellence published an evidence-based clinical guideline on the management of spasticity in children and young people with nonprogressive brain disorders.49 Intrathecal baclofen may be considered for children and young people with spasticity or dystonia that causes difficulty with pain or muscle spasms; posture or function; or self-care or ease of care by parents or caregivers. Additional recommendations include:
• Consideration of potential adverse effects of reducing spasticity when spasticity may support function, e.g., by compensating for muscle weakness. A trial of intrathecal baclofen to assess efficacy and adverse events before deciding to implant the intrathecal pump.
In 2010, the European Working group for Spasticity in Children published a consensus statement on the use of intrathecal baclofen therapy in children with spasticity.50 For children with spasticity that interferes with function or quality of life, they recommended conservative treatment and a trial of oral medication before use of a pump to deliver intrathecal baclofen. They also recommended individuation of treatment and
Medical Policy
16
involvement of parents and caregivers. The group received an unrestricted educational grant from Medtronic (Minneapolis, MN).
U.S. Preventive Services Task Force Recommendations
Not applicable.
Medicare National Coverage
Medicare provides coverage for implantable infusion pumps for the following indications51:
1. Intra-arterial infusion of 5-FUdR (5-fluorouracil deoxyribose) for the treatment of liver cancer for patients with primary hepatocellular carcinoma or Duke's Class D colorectal cancer, in whom metastases are limited to the liver and where the disease is unresectable or the patient refuses surgical excision of the tumor.
2. Administration of antispasmodic drugs intrathecally (e.g., baclofen) to treat chronic intractable spasticity in patients who have proven unresponsive to less invasive medical therapy as determined by the following criteria:
• As indicated by at least a 6-week trial, the patient cannot be maintained on noninvasive methods of spasm control, such as oral antispasmodic drugs, either because these methods fail to control adequately the spasticity or produce intolerable side effects, and
• Before pump implantation, the patient must have responded favorably to a trial intrathecal dose of the antispasmodic drug.
3. Administration of opioid drugs (e.g., morphine) intrathecally or epidurally for treatment of severe chronic intractable pain of malignant or nonmalignant origin in patients who have a life expectancy of at least 3 months and who have proven unresponsive to less invasive medical therapy as determined by the following criteria:
• The patient's history must indicate that he/she would not respond adequately to noninvasive methods of pain control, such as systemic opioids (including attempts to eliminate physical and behavioral abnormalities that may cause an exaggerated reaction to pain); and
• A preliminary trial of intraspinal opioid drug administration must be undertaken with a temporary intrathecal/epidural catheter to substantiate adequately acceptable pain relief and degree of side effects (including effects on the activities of daily living) and patient acceptance.
4. Other uses of implanted infusion pumps if:
• The drug is reasonable and necessary for the treatment of the individual patient;
• It is medically necessary that the drug be administered by an implanted infusion pump; and
• The FDA-approved labeling for the pump must specify that the drug being administered and the purpose for which it is administered is an indicated use for the pump.
References
1. Belinson S, Yang Y, Chopra R, Shankaran V, Samson D, Aronson N. Local Therapies for Unresectable Primary Hepatocellular Carcinoma. Comparative Effectiveness Review No. 114. (Prepared by the Blue Cross Blue Shield Association Technology
Medical Policy
17
Evaluation Center Evidence-based Practice Center under Contract No. 290-2007-10058-I.) AHRQ Publication No. 13-EHC069-EF. Rockville, MD: Agency for Healthcare Research and Quality. May 2013. Retrieved on December 31, 2014 from http:// www.effectivehealthcare.ahrq.gov/reports/final.cfm.
2. Jarnagin WR, Schwartz LH, Gultekin DH, et al. Regional chemotherapy for unresectable primary liver cancer: results of a phase II clinical trial and assessment of DCE-MRI as a biomarker of survival. Ann Oncol. Sep 2009;20(9):1589-1595. PMID 19491285
3. Smith GW, Bukowski RM, Hewlett JS, et al. Hepatic artery infusion of 5-fluorouracil and mitomycin C in cholangiocarcinoma and gallbladder carcinoma. Cancer. Oct 15 1984;54(8):1513-1516. PMID 6089991
4. Atiq OT, Kemeny N, Niedzwiecki D, et al. Treatment of unresectable primary liver cancer with intrahepatic fluorodeoxyuridine and mitomycin C through an implantable pump. Cancer. Feb 15 1992;69(4):920-924. PMID 1370918
5. Belinson S, Chopra R, Yang Y, Shankaran V, Aronson N. Local Hepatic Therapies for Metastases to the Liver From Unresectable Colorectal Cancer. Comparative Effectiveness Review No. 93. (Prepared by Blue Cross Blue Cross Blue Shield Association Technology Evaluation Center under Contract No. 290-2007-10058-I.) AHRQ Publication No.13-EHC014-EF. Rockville, MD: Agency for Healthcare Research and Quality. December 2012. Retrieved on December 31, 2014 from http:// www.effectivehealthcare.ahrq.gov/reports/final.cfm.
6. Mocellin S, Pasquali S, Nitti D. Fluoropyrimidine-HAI (hepatic arterial infusion) versus systemic chemotherapy (SCT) for unresectable liver metastases from colorectal cancer. Cochrane Database Syst Rev. 2009(3):CD007823. PMID 19588444
7. Ammori JB, Kemeny NE, Fong Y, et al. Conversion to complete resection and/or ablation using hepatic artery infusional chemotherapy in patients with unresectable liver metastases from colorectal cancer: a decade of experience at a single institution. Ann Surg Oncol. Sep 2013;20(9):2901-2907. PMID 23771246
8. Hoebers FJ, Pluim D, Verheij M, et al. Prediction of treatment outcome by cisplatin-DNA adduct formation in patients with stage III/IV head and neck squamous cell carcinoma, treated by concurrent cisplatin-radiation (RADPLAT). Int J Cancer. Aug 15 2006;119(4):750-756. PMID 16550603
9. Ackerstaff AH, Balm AJ, Rasch CR, et al. First-year quality of life assessment of an intra-arterial (RADPLAT) versus intravenous chemoradiation phase III trial. Head Neck. Jan 2009;31(1):77-84. PMID 18972429
10. Jaaback K, Johnson N, Lawrie TA. Intraperitoneal chemotherapy for the initial management of primary epithelial ovarian cancer. Cochrane Database Syst Rev. 2011(11):CD005340. PMID 22071822
11. Markman M, Bundy BN, Alberts DS, et al. Phase III trial of standard-dose intravenous cisplatin plus paclitaxel versus moderately high-dose carboplatin followed by intravenous paclitaxel and intraperitoneal cisplatin in small volume stage III ovarian carcinoma: an intergroup study of the Gynecologic Oncology Group, Southwestern Oncology Group, and Eastern Cooperative Oncology Group. J Clin Oncol. Feb 15 2001;19(4):1001-1007. PMID 11181662
12. Matharu G, Tucker O, Alderson D. Systematic review of intraperitoneal chemotherapy for gastric cancer. Br J Surg. Sep 2011;98(9):1225-1235. PMID 21644239
13. Liu C, Cui Q, Guo J, et al. Intra-Arterial Intervention Chemotherapy for Sarcoma and Cancerous Ulcer Via an Implanted Pump. Pathol Oncol Res. Jan 21 2014. PMID 24446082
Medical Policy
18
14. Myers J, Chan V, Jarvis V, et al. Intraspinal techniques for pain management in cancer patients: a systematic review. Support Care Cancer. Feb 2010;18(2):137-149. PMID 19943068
15. Falco FJ, Patel VB, Hayek SM, et al. Intrathecal infusion systems for long-term management of chronic noncancer pain: an update of assessment of evidence. Pain Physician. Apr 2013;16(2 Suppl):SE185-216. PMID 23615891
16. Patel VB, Manchikanti L, Singh V, et al. Systematic review of intrathecal infusion systems for long-term management of chronic non-cancer pain. Pain Physician. Mar-Apr 2009;12(2):345-360. PMID 19305484
17. Guyatt G, Gutterman D, Baumann MH, et al. Grading strength of recommendations and quality of evidence in clinical guidelines: report from an american college of chest physicians task force. Chest. Jan 2006;129(1):174-181. PMID 16424429
18. Hamza M, Doleys D, Wells M, et al. Prospective study of 3-year follow-up of low-dose intrathecal opioids in the management of chronic nonmalignant pain. Pain Med. Oct 2012;13(10):1304-1313. PMID 22845187
19. Atli A, Theodore BR, Turk DC, et al. Intrathecal opioid therapy for chronic nonmalignant pain: a retrospective cohort study with 3-year follow-up. Pain Med. Jul 2010;11(7):1010-1016. PMID 20492572
20. Veizi IE, Hayek SM, Narouze S, et al. Combination of intrathecal opioids with bupivacaine attenuates opioid dose escalation in chronic noncancer pain patients. Pain Med. Oct 2011;12(10):1481-1489. PMID 21943351
21. Duarte RV, Raphael JH, Sparkes E, et al. Long-term intrathecal drug administration for chronic nonmalignant pain. J Neurosurg Anesthesiol. Jan 2012;24(1):63-70. PMID 21904220
22. McIntyre A, Mays R, Mehta S, et al. Examining the effectiveness of intrathecal baclofen on spasticity in individuals with chronic spinal cord injury: a systematic review. J Spinal Cord Med. Jan 2014;37(1):11-18. PMID 24089997
23. Pin TW, McCartney L, Lewis J, et al. Use of intrathecal baclofen therapy in ambulant children and adolescents with spasticity and dystonia of cerebral origin: a systematic review. Dev Med Child Neurol. Oct 2011;53(10):885- 895. PMID 21635230
24. Motta F, Antonello CE, Stignani C. Intrathecal baclofen and motor function in cerebral palsy. Dev Med Child Neurol. May 2011;53(5):443-448. PMID 21480874
25. Morton RE, Gray N, Vloeberghs M. Controlled study of the effects of continuous intrathecal baclofen infusion in non-ambulant children with cerebral palsy. Dev Med Child Neurol. Aug 2011;53(8):736-741. PMID 21707598
26. Stokic DS, Yablon SA. Effect of concentration and mode of intrathecal baclofen administration on soleus H-reflex in patients with muscle hypertonia. Clin Neurophysiol. Nov 2012;123(11):2200-2204. PMID 22595326
27. Borrini L, Bensmail D, Thiebaut JB, et al. Occurrence of adverse events in long-term intrathecal baclofen infusion: a 1-year follow-up study of 158 adults. Arch Phys Med Rehabil. Jun 2014;95(6):1032-1038. PMID 24407102
28. Margetis K, Korfias S, Boutos N, et al. Intrathecal baclofen therapy for the symptomatic treatment of hereditary spastic paraplegia. Clin Neurol Neurosurg. Aug 2014;123:142-145. PMID 24973568
29. Ghosh D, Mainali G, Khera J, et al. Complications of intrathecal baclofen pumps in children: experience from a tertiary care center. Pediatr Neurosurg. 2013;49:138-144. PMID 24577095
30. Vles GF, Soudant DL, Hoving MA, et al. Long-term follow-up on continuous intrathecal Baclofen therapy in nonambulant children with intractable spastic Cerebral Palsy. Eur J Paediatr Neurol. Nov 2013;17(6):639-644. PMID 23871360
Medical Policy
19
31. Motta F, Antonello CE. Analysis of complications in 430 consecutive pediatric patients treated with intrathecal baclofen therapy: 14-year experience. J Neurosurg Pediatr. Mar 2014;13(3):301-306. PMID 24404968
32. Mathur SN, Chu SK, McCormick Z, et al. Long-term intrathecal baclofen: outcomes after more than 10 years of treatment. PM R. Jun 2014;6(6):506-513 e501. PMID 24355547
33. Spaan N, Teplova A, Stam G, et al. Systematic review: continuous intraperitoneal insulin infusion with implantable insulin pumps for diabetes mellitus. Acta Diabetol. Jun 2014;51(3):339-351. PMID 24595518
34. van Dijk PR, Logtenberg SJ, Groenier KH, et al. Report of a 7 year case-control study of continuous intraperitoneal insulin infusion and subcutaneous insulin therapy among patients with poorly controlled type 1 diabetes mellitus: Favourable effects on hypoglycaemic episodes. Diabetes Res Clin Pract. Sep 30 2014. PMID 25305134
35. van Dijk PR, Logtenberg SJ, Groenier KH, et al. Continuous intraperitoneal insulin infusion in type 1 diabetes: a 6-year post-trial follow-up. BMC Endocr Disord. 2014;14:30. PMID 24708696
36. Bonouvrie LA, Becher JG, Vles JS, et al. Intrathecal baclofen treatment in dystonic cerebral palsy: a randomized clinical trial: the IDYS trial. BMC Pediatr. 2013;13:175. PMID 24165282
37. National Comprehensive Cancer Network (NCCN). Clinical practice guidelines in oncology: Colon Cancer, version 2.2015. Retrieved on December 31, 2014 from http://www.nccn.org/professionals/physician_gls/PDF/colon.pdf.
38. National Comprehensive Cancer Network (NCCN). Clinical practice guidelines in oncology: Hepatobilliary Cancer, version 1.2015. Retrieved on December 31, 2014 from http://www.nccn.org/professionals/physician_gls/PDF/hepatobilliary.pdf.
39. National Comprehensive Cancer Network (NCCN). Clinical practice guidelines in oncology: Ovarian Cancer Including Fallopian Tube Cancer and Primary Peritoneal Cancer, version 3.2014. Retrieved on December 31, 2014 from http://www.nccn.org/professionals/physician_gls/pdf/ovarian.pdf.
40. National Comprehensive Cancer Network (NCCN). Clinical practice guidelines in oncology: Head and Neck Cancers, version 2.2014. Retrieved on December 31, 2014 from http://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf.
41. National Comprehensive Cancer Network (NCCN). Clinical practice guidelines in oncology: Soft Tissue Sarcoma, version 2.2014. Retrieved on December 31, 2014 from http://www.nccn.org/professionals/physician_gls/pdf/sarcoma.pdf.
42. National Comprehensive Cancer Network (NCCN). Clinical practice guidelines in oncology: Bone Cancer, version 1.2015. Retrieved on December 31, 2014 from http://www.nccn.org/professionals/physician_gls/pdf/bone.pdf.
43. National Comprehensive Cancer Network (NCCN). Clinical practice guidelines in oncology: Basal Cell Skin Cancer, version 1.2015. Retrieved on December 31, 2014 from http://www.nccn.org/professionals/physician_gls/pdf/nmsc.pdf.
44. National Comprehensive Cancer Network (NCCN). Clinical practice guidelines in oncology: Melanoma, version 1.2015. Retrieved on December 31, 2014 from http://www.nccn.org/professionals/physician_gls/pdf/melanoma.pdf.
45. National Cancer Institute (NCI). Colon Cancer Treatment (PDQ®). Retrieved on December 31, 2014 from http://www.cancer.gov/cancertopics/pdq/treatment/colon/HealthProfessional.
46. National Cancer Institute (NCI). Adult Primary Liver Cancer Treatment (PDQ®). Retrieved on December 31, 2014 from
Medical Policy
20
http://www.cancer.gov/cancertopics/pdq/treatment/adult-primary-liver/HealthProfessional.
47. National Comprehensive Cancer Network (NCCN). Clinical practice guidelines in oncology: Adult Cancer Pain, version 2.2014. Retrieved on December 31, 2014 from http://www.nccn.org/professionals/physician_gls/pdf/pain.pdf.
48. Manchikanti L, Boswell MV, Singh V, et al. Comprehensive evidence-based guidelines for interventional techniques in the management of chronic spinal pain. Pain Physician. Jul-Aug 2009;12(4):699-802. PMID 19644537
49. National Institute for Health and Care Excellence (NICE). Spasticity in children and young people with nonprogressive brain disorders: Management of spasticity and co-existing motor disorders and their early musculoskeletal complications, July 2012. Retrieved on December 31, 2014 from http://guidance.nice.org.uk/CG145.
50. Dan B, Motta F, Vles JS, et al. Consensus on the appropriate use of intrathecal baclofen (ITB) therapy in paediatric spasticity. Eur J Paediatr Neurol. Jan 2010;14(1):19-28. PMID 19541514
51. Centers for Medicare and Medicaid Services. Infusion pumps (280.14). Retrieved on December 31, 2014 from www.cms.gov.
52. Blue Cross Blue Shield Association. Medical Policy Reference Manual, No. 7.01.41 (November 2014).
Documentation Required for Clinical Review
• History and physical and/or consultation notes including:
ο Patient's life expectancy (for chronic pain only)
ο Previous and current pain or spasticity medication trials (doses, schedules) including duration, and response(s) (as applicable)
ο Previous conservative treatment(s), duration, and response(s) including physical therapy and alternative therapies
ο Behavioral, psychological and social support assessment
ο Psychological evaluation and clearance (if applicable)
ο Reason for the procedure outlining why there are no further treatment options for the patient’s condition (e.g., spasticity, chronic pain)
ο Medication requested for the intrathecal infusion pump
• Pertinent physician progress notes
• Other pertinent multidisciplinary notes/reports: (e.g., psychological or psychiatric evaluation, physical therapy, multidisciplinary pain management)
• Make/Model of intrathecal implantable infusion device and FDA approved indications
Post Service
• Procedure report(s)
Medical Policy
21
Coding
This Policy relates only to the services or supplies described herein. Benefits may vary according to benefit design; therefore, contract language should be reviewed before applying the terms of the Policy. Inclusion or exclusion of a procedure, diagnosis or device code(s) does not constitute or imply member coverage or provider reimbursement.
MN/IE
The following service/procedure may be considered medically necessary in certain instances and investigational in others. Services may be medically necessary when policy criteria are met. Services are considered investigational when the policy criteria are not met or when the code describes application of a product in the position statement that is investigational.
Type Code Description
CPT®
36260 - 36262 Insertion of implantable intra-arterial infusion pump (e.g., for chemotherapy of liver)
36563 Insertion of tunneled centrally inserted central venous access device with subcutaneous pump
36576 Repair of central venous access device, with subcutaneous port or pump, central or peripheral insertion site
36583 Replacement, complete, of a tunneled centrally inserted central venous access device, with subcutaneous pump, through same venous access
36590 Removal of tunneled central venous access device, with subcutaneous port or pump, central or peripheral insertion
61215 Insertion of subcutaneous reservoir, pump or continuous infusion system for connection to ventricular catheter
62318
Injection(s), including indwelling catheter placement, continuous infusion or intermittent bolus, of diagnostic or therapeutic substance(s) (including anesthetic, antispasmodic, opioid, steroid, other solution), not including neurolytic substances, includes contrast for localization when performed, epidural or subarachnoid; cervical or thoracic
62319
Injection(s), including indwelling catheter placement, continuous infusion or intermittent bolus, of diagnostic or therapeutic substance(s) (including anesthetic, antispasmodic, opioid, steroid, other solution), not including neurolytic substances, includes contrast for localization when performed, epidural or subarachnoid; lumbar or sacral (caudal)
62350
Implantation, revision or repositioning of tunneled intrathecal or epidural catheter, for long-term medication administration via an external pump or implantable reservoir/infusion pump; without
Medical Policy
22
laminectomy
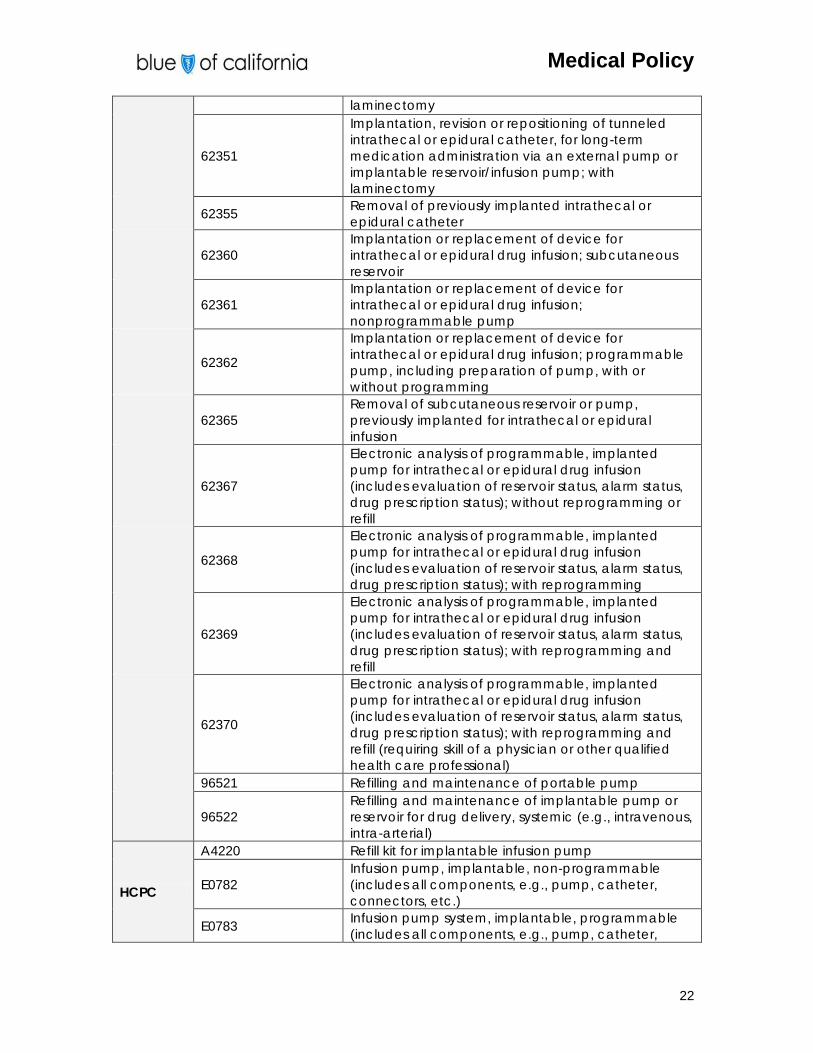
62351
Implantation, revision or repositioning of tunneled intrathecal or epidural catheter, for long-term medication administration via an external pump or implantable reservoir/infusion pump; with laminectomy
62355 Removal of previously implanted intrathecal or epidural catheter
62360 Implantation or replacement of device for intrathecal or epidural drug infusion; subcutaneous reservoir
62361 Implantation or replacement of device for intrathecal or epidural drug infusion; nonprogrammable pump
62362
Implantation or replacement of device for intrathecal or epidural drug infusion; programmable pump, including preparation of pump, with or without programming
62365 Removal of subcutaneous reservoir or pump, previously implanted for intrathecal or epidural infusion
62367
Electronic analysis of programmable, implanted pump for intrathecal or epidural drug infusion (includes evaluation of reservoir status, alarm status, drug prescription status); without reprogramming or refill
62368
Electronic analysis of programmable, implanted pump for intrathecal or epidural drug infusion (includes evaluation of reservoir status, alarm status, drug prescription status); with reprogramming
62369
Electronic analysis of programmable, implanted pump for intrathecal or epidural drug infusion (includes evaluation of reservoir status, alarm status, drug prescription status); with reprogramming and refill
62370
Electronic analysis of programmable, implanted pump for intrathecal or epidural drug infusion (includes evaluation of reservoir status, alarm status, drug prescription status); with reprogramming and refill (requiring skill of a physician or other qualified health care professional)
96521 Refilling and maintenance of portable pump
96522 Refilling and maintenance of implantable pump or reservoir for drug delivery, systemic (e.g., intravenous, intra-arterial)
HCPC
A4220 Refill kit for implantable infusion pump
E0782 Infusion pump, implantable, non-programmable (includes all components, e.g., pump, catheter, connectors, etc.)
E0783 Infusion pump system, implantable, programmable (includes all components, e.g., pump, catheter,
Medical Policy
23
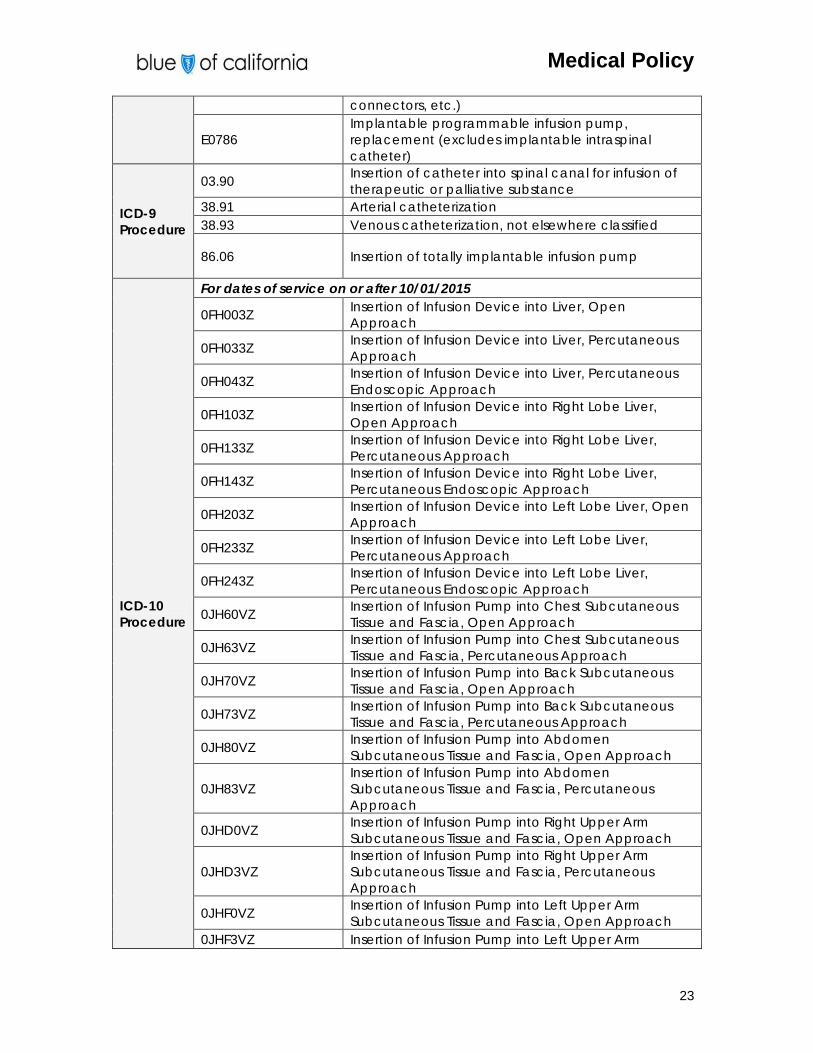
connectors, etc.)
E0786 Implantable programmable infusion pump, replacement (excludes implantable intraspinal catheter)
ICD-9 Procedure
03.90 Insertion of catheter into spinal canal for infusion of therapeutic or palliative substance
38.91 Arterial catheterization 38.93 Venous catheterization, not elsewhere classified
86.06 Insertion of totally implantable infusion pump
ICD-10 Procedure
For dates of service on or after 10/01/2015
0FH003Z Insertion of Infusion Device into Liver, Open Approach
0FH033Z Insertion of Infusion Device into Liver, Percutaneous Approach
0FH043Z Insertion of Infusion Device into Liver, Percutaneous Endoscopic Approach
0FH103Z Insertion of Infusion Device into Right Lobe Liver, Open Approach
0FH133Z Insertion of Infusion Device into Right Lobe Liver, Percutaneous Approach
0FH143Z Insertion of Infusion Device into Right Lobe Liver, Percutaneous Endoscopic Approach
0FH203Z Insertion of Infusion Device into Left Lobe Liver, Open Approach
0FH233Z Insertion of Infusion Device into Left Lobe Liver, Percutaneous Approach
0FH243Z Insertion of Infusion Device into Left Lobe Liver, Percutaneous Endoscopic Approach
0JH60VZ Insertion of Infusion Pump into Chest Subcutaneous Tissue and Fascia, Open Approach
0JH63VZ Insertion of Infusion Pump into Chest Subcutaneous Tissue and Fascia, Percutaneous Approach
0JH70VZ Insertion of Infusion Pump into Back Subcutaneous Tissue and Fascia, Open Approach
0JH73VZ Insertion of Infusion Pump into Back Subcutaneous Tissue and Fascia, Percutaneous Approach
0JH80VZ Insertion of Infusion Pump into Abdomen Subcutaneous Tissue and Fascia, Open Approach
0JH83VZ Insertion of Infusion Pump into Abdomen Subcutaneous Tissue and Fascia, Percutaneous Approach
0JHD0VZ Insertion of Infusion Pump into Right Upper Arm Subcutaneous Tissue and Fascia, Open Approach
0JHD3VZ Insertion of Infusion Pump into Right Upper Arm Subcutaneous Tissue and Fascia, Percutaneous Approach
0JHF0VZ Insertion of Infusion Pump into Left Upper Arm Subcutaneous Tissue and Fascia, Open Approach
0JHF3VZ Insertion of Infusion Pump into Left Upper Arm
Medical Policy
24
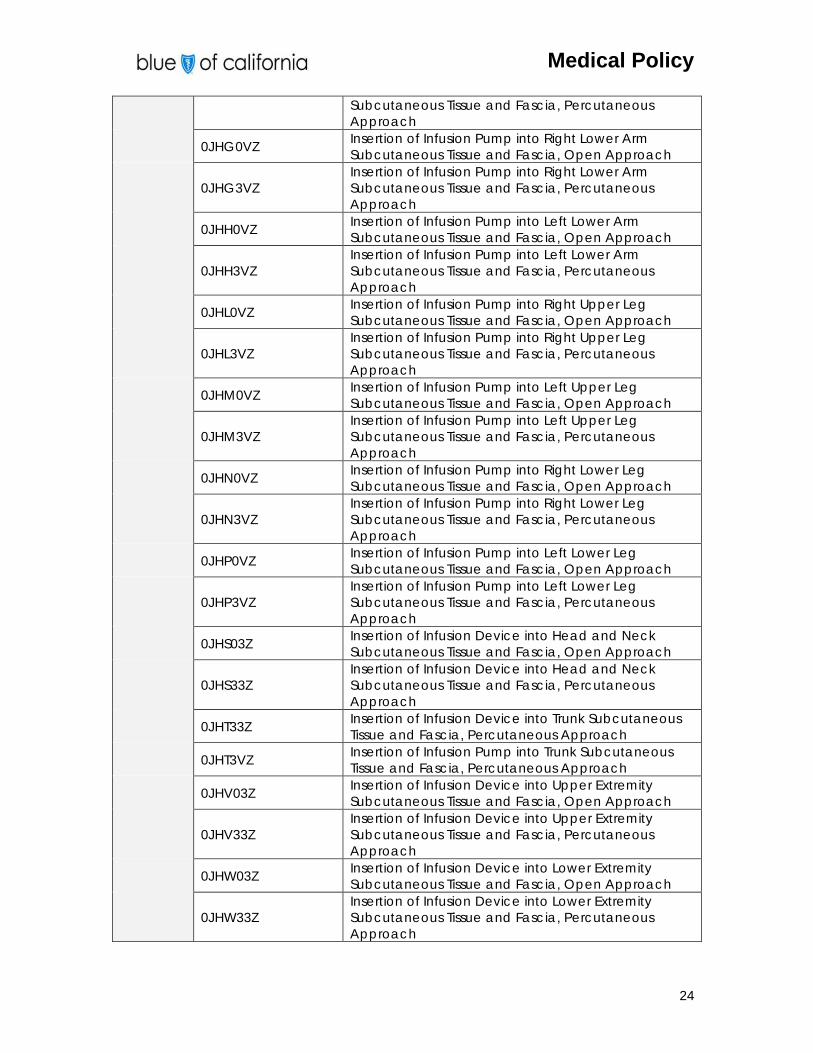
Subcutaneous Tissue and Fascia, Percutaneous Approach
0JHG0VZ Insertion of Infusion Pump into Right Lower Arm Subcutaneous Tissue and Fascia, Open Approach
0JHG3VZ Insertion of Infusion Pump into Right Lower Arm Subcutaneous Tissue and Fascia, Percutaneous Approach
0JHH0VZ Insertion of Infusion Pump into Left Lower Arm Subcutaneous Tissue and Fascia, Open Approach
0JHH3VZ Insertion of Infusion Pump into Left Lower Arm Subcutaneous Tissue and Fascia, Percutaneous Approach
0JHL0VZ Insertion of Infusion Pump into Right Upper Leg Subcutaneous Tissue and Fascia, Open Approach
0JHL3VZ Insertion of Infusion Pump into Right Upper Leg Subcutaneous Tissue and Fascia, Percutaneous Approach
0JHM0VZ Insertion of Infusion Pump into Left Upper Leg Subcutaneous Tissue and Fascia, Open Approach
0JHM3VZ Insertion of Infusion Pump into Left Upper Leg Subcutaneous Tissue and Fascia, Percutaneous Approach
0JHN0VZ Insertion of Infusion Pump into Right Lower Leg Subcutaneous Tissue and Fascia, Open Approach
0JHN3VZ Insertion of Infusion Pump into Right Lower Leg Subcutaneous Tissue and Fascia, Percutaneous Approach
0JHP0VZ Insertion of Infusion Pump into Left Lower Leg Subcutaneous Tissue and Fascia, Open Approach
0JHP3VZ Insertion of Infusion Pump into Left Lower Leg Subcutaneous Tissue and Fascia, Percutaneous Approach
0JHS03Z Insertion of Infusion Device into Head and Neck Subcutaneous Tissue and Fascia, Open Approach
0JHS33Z Insertion of Infusion Device into Head and Neck Subcutaneous Tissue and Fascia, Percutaneous Approach
0JHT33Z Insertion of Infusion Device into Trunk Subcutaneous Tissue and Fascia, Percutaneous Approach
0JHT3VZ Insertion of Infusion Pump into Trunk Subcutaneous Tissue and Fascia, Percutaneous Approach
0JHV03Z Insertion of Infusion Device into Upper Extremity Subcutaneous Tissue and Fascia, Open Approach
0JHV33Z Insertion of Infusion Device into Upper Extremity Subcutaneous Tissue and Fascia, Percutaneous Approach
0JHW03Z Insertion of Infusion Device into Lower Extremity Subcutaneous Tissue and Fascia, Open Approach
0JHW33Z Insertion of Infusion Device into Lower Extremity Subcutaneous Tissue and Fascia, Percutaneous Approach
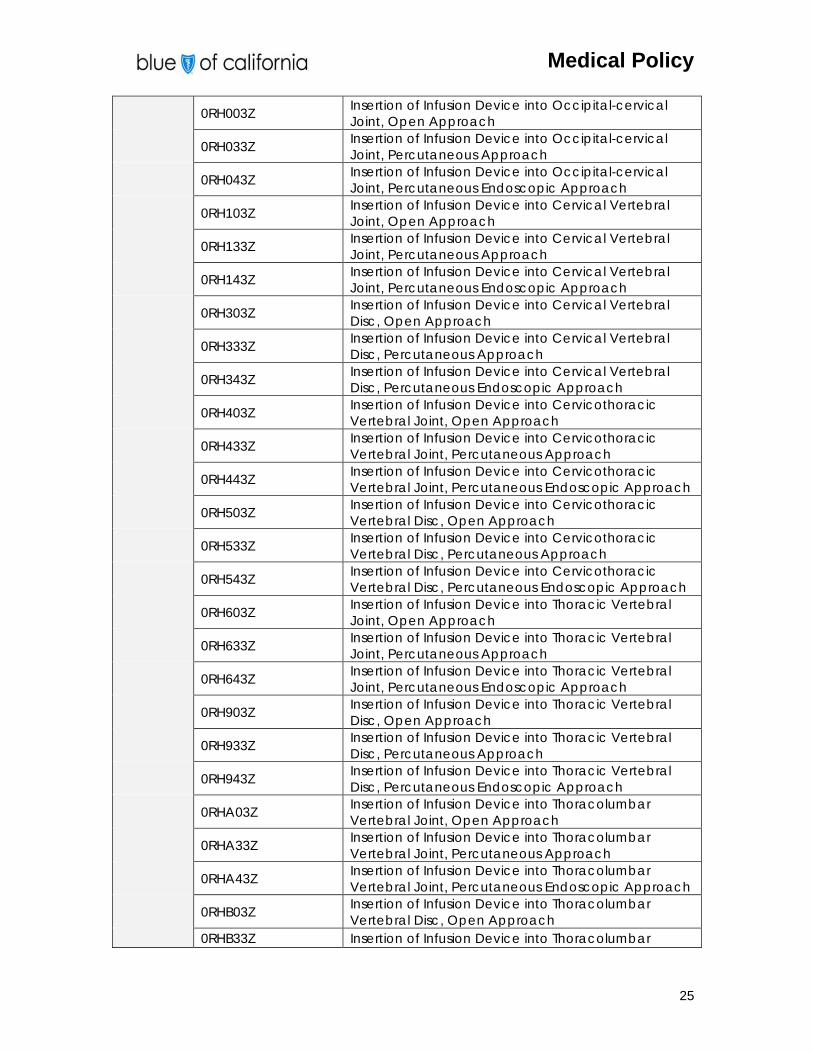
Medical Policy
25
0RH003Z Insertion of Infusion Device into Occipital-cervical Joint, Open Approach
0RH033Z Insertion of Infusion Device into Occipital-cervical Joint, Percutaneous Approach
0RH043Z Insertion of Infusion Device into Occipital-cervical Joint, Percutaneous Endoscopic Approach
0RH103Z Insertion of Infusion Device into Cervical Vertebral Joint, Open Approach
0RH133Z Insertion of Infusion Device into Cervical Vertebral Joint, Percutaneous Approach
0RH143Z Insertion of Infusion Device into Cervical Vertebral Joint, Percutaneous Endoscopic Approach
0RH303Z Insertion of Infusion Device into Cervical Vertebral Disc, Open Approach
0RH333Z Insertion of Infusion Device into Cervical Vertebral Disc, Percutaneous Approach
0RH343Z Insertion of Infusion Device into Cervical Vertebral Disc, Percutaneous Endoscopic Approach
0RH403Z Insertion of Infusion Device into Cervicothoracic Vertebral Joint, Open Approach
0RH433Z Insertion of Infusion Device into Cervicothoracic Vertebral Joint, Percutaneous Approach
0RH443Z Insertion of Infusion Device into Cervicothoracic Vertebral Joint, Percutaneous Endoscopic Approach
0RH503Z Insertion of Infusion Device into Cervicothoracic Vertebral Disc, Open Approach
0RH533Z Insertion of Infusion Device into Cervicothoracic Vertebral Disc, Percutaneous Approach
0RH543Z Insertion of Infusion Device into Cervicothoracic Vertebral Disc, Percutaneous Endoscopic Approach
0RH603Z Insertion of Infusion Device into Thoracic Vertebral Joint, Open Approach
0RH633Z Insertion of Infusion Device into Thoracic Vertebral Joint, Percutaneous Approach
0RH643Z Insertion of Infusion Device into Thoracic Vertebral Joint, Percutaneous Endoscopic Approach
0RH903Z Insertion of Infusion Device into Thoracic Vertebral Disc, Open Approach
0RH933Z Insertion of Infusion Device into Thoracic Vertebral Disc, Percutaneous Approach
0RH943Z Insertion of Infusion Device into Thoracic Vertebral Disc, Percutaneous Endoscopic Approach
0RHA03Z Insertion of Infusion Device into Thoracolumbar Vertebral Joint, Open Approach
0RHA33Z Insertion of Infusion Device into Thoracolumbar Vertebral Joint, Percutaneous Approach
0RHA43Z Insertion of Infusion Device into Thoracolumbar Vertebral Joint, Percutaneous Endoscopic Approach
0RHB03Z Insertion of Infusion Device into Thoracolumbar Vertebral Disc, Open Approach
0RHB33Z Insertion of Infusion Device into Thoracolumbar
Medical Policy
26
Vertebral Disc, Percutaneous Approach
0RHB43Z Insertion of Infusion Device into Thoracolumbar Vertebral Disc, Percutaneous Endoscopic Approach
0RHE03Z Insertion of Infusion Device into Right Sternoclavicular Joint, Open Approach
0RHE33Z Insertion of Infusion Device into Right Sternoclavicular Joint, Percutaneous Approach
0RHE43Z Insertion of Infusion Device into Right Sternoclavicular Joint, Percutaneous Endoscopic Approach
0RHF03Z Insertion of Infusion Device into Left Sternoclavicular Joint, Open Approach
0RHF33Z Insertion of Infusion Device into Left Sternoclavicular Joint, Percutaneous Approach
0RHF43Z Insertion of Infusion Device into Left Sternoclavicular Joint, Percutaneous Endoscopic Approach
0RHG03Z Insertion of Infusion Device into Right Acromioclavicular Joint, Open Approach
0RHG33Z Insertion of Infusion Device into Right Acromioclavicular Joint, Percutaneous Approach
0RHG43Z Insertion of Infusion Device into Right Acromioclavicular Joint, Percutaneous Endoscopic Approach
0RHH03Z Insertion of Infusion Device into Left Acromioclavicular Joint, Open Approach
0RHH33Z Insertion of Infusion Device into Left Acromioclavicular Joint, Percutaneous Approach
0RHH43Z Insertion of Infusion Device into Left Acromioclavicular Joint, Percutaneous Endoscopic Approach
0RHJ03Z Insertion of Infusion Device into Right Shoulder Joint, Open Approach
0RHJ33Z Insertion of Infusion Device into Right Shoulder Joint, Percutaneous Approach
0RHJ43Z Insertion of Infusion Device into Right Shoulder Joint, Percutaneous Endoscopic Approach
0RHK03Z Insertion of Infusion Device into Left Shoulder Joint, Open Approach
0RHK33Z Insertion of Infusion Device into Left Shoulder Joint, Percutaneous Approach
0RHK43Z Insertion of Infusion Device into Left Shoulder Joint, Percutaneous Endoscopic Approach
0RHL03Z Insertion of Infusion Device into Right Elbow Joint, Open Approach
0RHL33Z Insertion of Infusion Device into Right Elbow Joint, Percutaneous Approach
0RHL43Z Insertion of Infusion Device into Right Elbow Joint, Percutaneous Endoscopic Approach
0RHM03Z Insertion of Infusion Device into Left Elbow Joint, Open Approach
0RHM33Z Insertion of Infusion Device into Left Elbow Joint, Percutaneous Approach
Medical Policy
27
0RHM43Z Insertion of Infusion Device into Left Elbow Joint, Percutaneous Endoscopic Approach
0RHN03Z Insertion of Infusion Device into Right Wrist Joint, Open Approach
0RHN33Z Insertion of Infusion Device into Right Wrist Joint, Percutaneous Approach
0RHN43Z Insertion of Infusion Device into Right Wrist Joint, Percutaneous Endoscopic Approach
0RHP03Z Insertion of Infusion Device into Left Wrist Joint, Open Approach
0RHP33Z Insertion of Infusion Device into Left Wrist Joint, Percutaneous Approach
0RHP43Z Insertion of Infusion Device into Left Wrist Joint, Percutaneous Endoscopic Approach
0RHQ03Z Insertion of Infusion Device into Right Carpal Joint, Open Approach
0RHQ33Z Insertion of Infusion Device into Right Carpal Joint, Percutaneous Approach
0RHQ43Z Insertion of Infusion Device into Right Carpal Joint, Percutaneous Endoscopic Approach
0RHR03Z Insertion of Infusion Device into Left Carpal Joint, Open Approach
0RHR33Z Insertion of Infusion Device into Left Carpal Joint, Percutaneous Approach
0RHR43Z Insertion of Infusion Device into Left Carpal Joint, Percutaneous Endoscopic Approach
0RHS03Z Insertion of Infusion Device into Right Metacarpocarpal Joint, Open Approach
0RHS33Z Insertion of Infusion Device into Right Metacarpocarpal Joint, Percutaneous Approach
0RHS43Z Insertion of Infusion Device into Right Metacarpocarpal Joint, Percutaneous Endoscopic Approach
0RHT03Z Insertion of Infusion Device into Left Metacarpocarpal Joint, Open Approach
0RHT33Z Insertion of Infusion Device into Left Metacarpocarpal Joint, Percutaneous Approach
0RHT43Z Insertion of Infusion Device into Left Metacarpocarpal Joint, Percutaneous Endoscopic Approach
0RHU03Z Insertion of Infusion Device into Right Metacarpophalangeal Joint, Open Approach
0RHU33Z Insertion of Infusion Device into Right Metacarpophalangeal Joint, Percutaneous Approach
0RHU43Z Insertion of Infusion Device into Right Metacarpophalangeal Joint, Percutaneous Endoscopic Approach
0RHV03Z Insertion of Infusion Device into Left Metacarpophalangeal Joint, Open Approach
0RHV33Z Insertion of Infusion Device into Left
Medical Policy
28
Metacarpophalangeal Joint, Percutaneous Approach
0RHV43Z Insertion of Infusion Device into Left Metacarpophalangeal Joint, Percutaneous Endoscopic Approach
0RHW03Z Insertion of Infusion Device into Right Finger Phalangeal Joint, Open Approach
0RHW33Z Insertion of Infusion Device into Right Finger Phalangeal Joint, Percutaneous Approach
0RHW43Z Insertion of Infusion Device into Right Finger Phalangeal Joint, Percutaneous Endoscopic Approach
0RHX03Z Insertion of Infusion Device into Left Finger Phalangeal Joint, Open Approach
0RHX33Z Insertion of Infusion Device into Left Finger Phalangeal Joint, Percutaneous Approach
0RHX43Z Insertion of Infusion Device into Left Finger Phalangeal Joint, Percutaneous Endoscopic Approach
0SH003Z Insertion of Infusion Device into Lumbar Vertebral Joint, Open Approach
0SH033Z Insertion of Infusion Device into Lumbar Vertebral Joint, Percutaneous Approach
0SH043Z Insertion of Infusion Device into Lumbar Vertebral Joint, Percutaneous Endoscopic Approach
0SH203Z Insertion of Infusion Device into Lumbar Vertebral Disc, Open Approach
0SH233Z Insertion of Infusion Device into Lumbar Vertebral Disc, Percutaneous Approach
0SH243Z Insertion of Infusion Device into Lumbar Vertebral Disc, Percutaneous Endoscopic Approach
0SH303Z Insertion of Infusion Device into Lumbosacral Joint, Open Approach
0SH333Z Insertion of Infusion Device into Lumbosacral Joint, Percutaneous Approach
0SH343Z Insertion of Infusion Device into Lumbosacral Joint, Percutaneous Endoscopic Approach
0SH403Z Insertion of Infusion Device into Lumbosacral Disc, Open Approach
0SH433Z Insertion of Infusion Device into Lumbosacral Disc, Percutaneous Approach
0SH443Z Insertion of Infusion Device into Lumbosacral Disc, Percutaneous Endoscopic Approach
0SH503Z Insertion of Infusion Device into Sacrococcygeal Joint, Open Approach
0SH533Z Insertion of Infusion Device into Sacrococcygeal Joint, Percutaneous Approach
0SH543Z Insertion of Infusion Device into Sacrococcygeal Joint, Percutaneous Endoscopic Approach
0SH603Z Insertion of Infusion Device into Coccygeal Joint, Open Approach
Medical Policy
29
0SH633Z Insertion of Infusion Device into Coccygeal Joint, Percutaneous Approach
0SH643Z Insertion of Infusion Device into Coccygeal Joint, Percutaneous Endoscopic Approach
0SH703Z Insertion of Infusion Device into Right Sacroiliac Joint, Open Approach
0SH733Z Insertion of Infusion Device into Right Sacroiliac Joint, Percutaneous Approach
0SH743Z Insertion of Infusion Device into Right Sacroiliac Joint, Percutaneous Endoscopic Approach
0SH803Z Insertion of Infusion Device into Left Sacroiliac Joint, Open Approach
0SH833Z Insertion of Infusion Device into Left Sacroiliac Joint, Percutaneous Approach
0SH843Z Insertion of Infusion Device into Left Sacroiliac Joint, Percutaneous Endoscopic Approach
0SH903Z Insertion of Infusion Device into Right Hip Joint, Open Approach
0SH933Z Insertion of Infusion Device into Right Hip Joint, Percutaneous Approach
0SH943Z Insertion of Infusion Device into Right Hip Joint, Percutaneous Endoscopic Approach
0SHB03Z Insertion of Infusion Device into Left Hip Joint, Open Approach
0SHB33Z Insertion of Infusion Device into Left Hip Joint, Percutaneous Approach
0SHB43Z Insertion of Infusion Device into Left Hip Joint, Percutaneous Endoscopic Approach
0SHC03Z Insertion of Infusion Device into Right Knee Joint, Open Approach
0SHC33Z Insertion of Infusion Device into Right Knee Joint, Percutaneous Approach
0SHC43Z Insertion of Infusion Device into Right Knee Joint, Percutaneous Endoscopic Approach
0SHD03Z Insertion of Infusion Device into Left Knee Joint, Open Approach
0SHD33Z Insertion of Infusion Device into Left Knee Joint, Percutaneous Approach
0SHD43Z Insertion of Infusion Device into Left Knee Joint, Percutaneous Endoscopic Approach
0SHF03Z Insertion of Infusion Device into Right Ankle Joint, Open Approach
0SHF33Z Insertion of Infusion Device into Right Ankle Joint, Percutaneous Approach
0SHF43Z Insertion of Infusion Device into Right Ankle Joint, Percutaneous Endoscopic Approach
0SHG03Z Insertion of Infusion Device into Left Ankle Joint, Open Approach
OSHG33Z Insertion of Infusion Device into Left Ankle Joint, Percutaneous Approach
0SHG43Z Insertion of Infusion Device into Left Ankle Joint,
Medical Policy
30
Percutaneous Endoscopic Approach
0SHH03Z Insertion of Infusion Device into Right Tarsal Joint, Open Approach
0SHH33Z Insertion of Infusion Device into Right Tarsal Joint, Percutaneous Approach
0SHH43Z Insertion of Infusion Device into Right Tarsal Joint, Percutaneous Endoscopic Approach
0SHJ03Z Insertion of Infusion Device into Left Tarsal Joint, Open Approach
0SHJ33Z Insertion of Infusion Device into Left Tarsal Joint, Percutaneous Approach
0SHJ43Z Insertion of Infusion Device into Left Tarsal Joint, Percutaneous Endoscopic Approach
0SHK03Z Insertion of Infusion Device into Right Metatarsal-Tarsal Joint, Open Approach
0SHK33Z Insertion of Infusion Device into Right Metatarsal-Tarsal Joint, Percutaneous Approach
0SHK43Z Insertion of Infusion Device into Right Metatarsal-Tarsal Joint, Percutaneous Endoscopic Approach
0SHL03Z Insertion of Infusion Device into Left Metatarsal-Tarsal Joint, Open Approach
0SHL33Z Insertion of Infusion Device into Left Metatarsal-Tarsal Joint, Percutaneous Approach
0SHL43Z Insertion of Infusion Device into Left Metatarsal-Tarsal Joint, Percutaneous Endoscopic Approach
0SHM03Z Insertion of Infusion Device into Right Metatarsal-Phalangeal Joint, Open Approach
0SHM33Z Insertion of Infusion Device into Right Metatarsal-Phalangeal Joint, Percutaneous Approach
0SHM43Z Insertion of Infusion Device into Right Metatarsal-Phalangeal Joint, Percutaneous Endoscopic Approach
0SHN03Z Insertion of Infusion Device into Left Metatarsal-Phalangeal Joint, Open Approach
0SHN33Z Insertion of Infusion Device into Left Metatarsal-Phalangeal Joint, Percutaneous Approach
0SHN43Z Insertion of Infusion Device into Left Metatarsal-Phalangeal Joint, Percutaneous Endoscopic Approach
0SHP03Z Insertion of Infusion Device into Right Toe Phalangeal Joint, Open Approach
0SHP33Z Insertion of Infusion Device into Right Toe Phalangeal Joint, Percutaneous Approach
0SHP43Z Insertion of Infusion Device into Right Toe Phalangeal Joint, Percutaneous Endoscopic Approach
0SHQ03Z Insertion of Infusion Device into Left Toe Phalangeal Joint, Open Approach
0SHQ33Z Insertion of Infusion Device into Left Toe Phalangeal Joint, Percutaneous Approach
0SHQ43Z Insertion of Infusion Device into Left Toe Phalangeal Joint, Percutaneous Endoscopic Approach
Medical Policy
31
ICD-9 Diagnosis All Diagnoses
ICD-10 Diagnosis
For dates of service on or after 10/01/2015 All Diagnoses
Policy History
This section provides a chronological history of the activities, updates and changes that have occurred with this Medical Policy.
Effective Date Action Reason 3/5/2012 New Policy Adoption TRIAD
Healthcare Inc., Musculoskeletal Health Services Medical Policy
Medical Policy Committee
7/14/2014 Policy revision with position change
Medical Policy Committee
1/30/2015 Policy title change from Implantable Intrathecal Drug Delivery Systems Policy revision without position change
Medical Policy Committee
Definitions of Decision Determinations
Medically Necessary: A treatment, procedure or drug is medically necessary only when it has been established as safe and effective for the particular symptoms or diagnosis, is not investigational or experimental, is not being provided primarily for the convenience of the patient or the provider, and is provided at the most appropriate level to treat the condition.
Investigational/Experimental: A treatment, procedure or drug is investigational when it has not been recognized as safe and effective for use in treating the particular condition in accordance with generally accepted professional medical standards. This includes services where approval by the federal or state governmental is required prior to use, but has not yet been granted.
Split Evaluation: Blue Shield of California / Blue Shield of California Life & Health Insurance Company (Blue Shield) policy review can result in a Split Evaluation, where a treatment, procedure or drug will be considered to be investigational for certain indications or conditions, but will be deemed safe and effective for other indications or conditions, and therefore potentially medically necessary in those instances.
Prior Authorization Requirements
This service (or procedure) is considered medically necessary in certain instances and investigational in others (refer to policy for details).
For instances when the indication is medically necessary, clinical evidence is required to determine medical necessity.

Medical Policy
32
For instances when the indication is investigational, you may submit additional information to the Prior Authorization Department.
Within five days before the actual date of service, the Provider MUST confirm with Blue Shield that the member's health plan coverage is still in effect. Blue Shield reserves the right to revoke an authorization prior to services being rendered based on cancellation of the member's eligibility. Final determination of benefits will be made after review of the claim for limitations or exclusions.
Questions regarding the applicability of this policy should also be directed to the Prior Authorization Department. Please call 1-800-541-6652 or visit the Provider Portal www.blueshieldca.com/provider.
The materials provided to you are guidelines used by this plan to authorize, modify, or deny care for persons with similar illness or conditions. Specific care and treatment may vary depending on individual need and the benefits covered under your contract. These Policies are subject to change as new information becomes available.


















