Immunotherapy In Bladder Cancerd2qrtshcpf0x30.cloudfront.net/nodes/188/AUA Slides FINAL...
96
Transcript of Immunotherapy In Bladder Cancerd2qrtshcpf0x30.cloudfront.net/nodes/188/AUA Slides FINAL...


Agenda
Agenda Item Speaker
8:00-8:15 AM Welcome/Introductions/Pretest Dr. Kamat, Chair
8:15-8:25 AM Immunotherapy in Bladder Cancer: Basic Concepts Dr. Dreicer
8:25-9:05 AM Clinical Experience with Immunotherapy in Bladder Cancer
8:25-8:40 AM ICI in Advanced/Met Disease and Lessons Learned Dr. Bellmunt
8:40-8:50 AM Predictive Biomarkers for Checkpoint Blockade Therapy Dr. Dinney
8:50-9:05 AM Roundtable Discussion Dr. Dreicer (Moderator)
9:05-9:50 AM Practical Aspects of Immune Checkpoint Inhibitors
9:05-9:15 AM Safety Profile of ICIs: Early Recognition & Management Dr. Dreicer
9:15-9:25 AM Ways Urologists Can Adopt ICI into Clinical Practice: Med Onc Perspective Dr. Bellmunt
9:25-9:35 AM Ways Urologists Can Adopt ICI into Clinical Practice: Urologist’s Perspective Dr. Dinney
9:35-9:50 AM Roundtable Discussion Dr. Kamat (Moderator)
9:50-10:00 AM Concluding Remarks/Posttest Dr. Kamat, Chair

1. Describe the basic concepts of cancer immunotherapy, including immune checkpoint blockade, and rationale for its use in bladder cancer.
2. Appraise safety and efficacy of current and emerging cancer immunotherapy, including immune checkpoint inhibitors, in patients with locally advanced or metastatic bladder cancer.
3. Evaluate the role for biomarkers in locally advanced or metastatic bladder cancer when immune checkpoint inhibitors are used.
4. Identify practical strategies to prevent, anticipate, and manage immune-related adverse events in patients with locally advanced or metastatic bladder cancer in your urology practice.
Learning Objectives

Faculty

Faculty Disclosures
Joaquim Bellmunt, MD, PhD - has disclosed that he is a consultant for AstraZeneca, Genentech, and Merck and receives grant/research support from Novartis and Sanofi.
Colin P.N. Dinney, MD - has disclosed that he receives financial or material support from FKD Therapies.
Robert Dreicer, MD, MS, MACP, FASCO - has disclosed that he is a consultant for Asana, Astellas, AstraZeneca, Bristol-Myers Squibb, Eisai, Exelixis, Medivation, Roche, and Sanofi-Genzyme. He also receives grant/research support from Asana, Genentech, and Merck.
Ashish M. Kamat, MD, MBBS, FACS - has disclosed that he is a consultant for Abbott Molecular, Cepheid, Heat Biologics, Merck, Oncogenics, Photocure, Spectrum Pharmaceuticals, Telesta Therapeutics, and Theralase. He also receives grant/research support from FKD Therapies, Heat Biologics, Merck, and Photocure.

Agenda
Agenda Item Speaker
8:00-8:15 AM Welcome/Introductions/Pretest Dr. Kamat, Chair
8:15-8:25 AM Immunotherapy in Bladder Cancer: Basic Concepts Dr. Dreicer
8:25-9:05 AM Clinical Experience with Immunotherapy in Bladder Cancer
8:25-8:40 AM ICI in Advanced/Met Disease and Lessons Learned Dr. Bellmunt
8:40-8:50 AM Predictive Biomarkers for Checkpoint Blockade Therapy Dr. Dinney
8:50-9:05 AM Roundtable Discussion Dr. Dreicer (Moderator)
9:05-9:50 AM Practical Aspects of Immune Checkpoint Inhibitors
9:05-9:15 AM Safety Profile of ICIs: Early Recognition & Management Dr. Dreicer
9:15-9:25 AM Ways Urologists Can Adopt ICI into Clinical Practice: Med Onc Perspective Dr. Bellmunt
9:25-9:35 AM Ways Urologists Can Adopt ICI into Clinical Practice: Urologist’s Perspective Dr. Dinney
9:35-9:50 AM Roundtable Discussion Dr. Kamat (Moderator)
9:50-10:00 AM Concluding Remarks/Posttest Dr. Kamat, Chair

Robert Dreicer, MD, MS, MACP, FASCOHead, Medical Oncology Section
Deputy Director, University of Virginia Cancer Center
Co-Director Paul Mellon Urologic Oncology Center
Professor of Medicine and Urology
University of Virginia School of Medicine
Immunotherapy in Bladder Cancer

• Renal Cancer
– HD IL2 – FDA-approved
– Interferon alfa
• Prostate Cancer
– Sipuleucel T – first and only FDA-approved cancer vaccine
• Bladder Cancer
– BCG
– Avelumab, Atezolizumab, Durvalumab, Nivolumab: FDA-approved in advanced urothelial cancer and in cisplatin-ineligible cases (atezolizumab)
Immunomodulatory Therapeutics in GU Cancers
U.S. Food and Drug Administration

Funt SA, Rosenberg JE. Nat Rev Clin Oncol. 2017; Kamat AM, et al. Lancet. 2016.
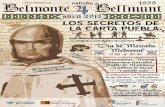
Bladder Cancer Therapeutic Landscape
T2-T4: Muscle-Invasive Bladder
Cancer (MIBC)
Radical cystectomy; <25% get adjuvant/
neoadjuvant (Gem/Cis)
First-Line Metastatic
Gem/Cis or MVAC are SOC in US; Gem/Carbo or Atezolizumab for
Cis-ineligible (50%)
Second-Line Metastatic
Avelumab, Atezolizumab,Durvalumab, Nivolumab
ORR 15%-19.6%mOS: 7.9-11.4 mo
Taxanes, gemcitabine,pemetrexed,
vinflunine (EU)ORR: 10%
mOS: 7-9 mo
10%-15%
10%-15%
70%-80%Ta/T1/Tis: Non‒Muscle-Invasive Bladder
Cancer (NMIBC)
TURBT/intravesical BCG
Normal Urothelium

Non–Muscle-Invasive Bladder Cancer: Bacillus Calmette-Guérin (BCG)
Initial response rates of approximately 70%
Functions via activation of immune system and induction of inflammatory response
Mechanism of action not completely understood
• BCG attaches to urothelial cells, followed by internalization
• Cells then upregulate MHC-II molecules and secrete cytokines, resulting in recruitment of immune cells, including lymphocytes, to tumor environment
BCG: gold standard in treatment of high-risk NMIBC
Kamat AM, et al. Lancet. 2016.

• Tumors must evolve mechanisms to locally evade and or disable the immune system.
• The goal of T-cell checkpoint blockade is to prohibit access of tumor cells to the “off switch” of the T-cell, restoring and maintaining tumor-specific immunity.
Why do tumors evade the immune response?

Mellman I, et al. Nature. 2011.
T-Cell Activation Represents a Balance of Activating and Inhibitory Factors
CD28
OX40
GITR
CD137
CD27
HVEM LAG-3
VISTA
BTLA
TIM-3
PD-1
CTLA-4
Agonistic antibodies
Blocking antibodies
T-cell stimulation
Activating Receptors
Inhibitory Receptors

Hayden EC. Nature. 2012.
Anti-PD-1/PD-L1: Unleash Cytotoxic CD8+ T-cells
PD-L1 binds PD-1, inhibiting T-cell response
A separate therapyuses antibodiesthat bind PD-L1on the tumour cell
PD-L1
Antibodies block inhibitory signal to PD-1
T-cell receptor recognizes tumour cell

Cancer Genome Atlas Research Network. Nature. 2014.
Expression Patterns Define Subsets of Bladder Cancer
mut/amp/fusionPapillary/squamous
Missing data
mRNA/miRNA/protein
Integrated Analysis of mRNA, miRNA and Protein Data
-2 0 2

Bladder Cancer Molecular Taxonomy: Summary from a Consensus Meeting
Kamat AM, et al. Lancet. 2016.
TCGA Cluster II corresponds to the MDACC p53-like subtype

Powles T, et al. Nature. 2014.
PD-L1 Expression in Metastatic Bladder Cancer
IHC Score(N = 205)
Tumor-Infiltrating Immune Cells, n (%)
Tumor Cells, n (%)
IHC 3 18 (9) 14 (7)
IHC 2 37 (18) 8 (4)
IHC 1 89 (43) 37 (18)
IHC 0 61 (30) 146 (71)
PD-L1 Positivity in UBC Tumors by IHC

Tumor Response With Atezolizumab Anti-PD-L1 Therapy in Metastatic Bladder Cancer
aPatients with CRs who had ≤100% reduction of target lesions due to lymph node target lesions; all lymph nodes returned to normal size per RECIST v1.1.
Max
imu
m S
LD R
ed
uct
ion
Fro
m B
ase
line,
%
100
90
80
70
60
50
40
30
20
10
0
-10
-20
-30
-40
-50
-60
-70
-80
-90
-100
IHC (IC) 0IHC (IC) 1IHC (IC) 2IHC (IC) 3IHC (IC) Unknown
a
a
Powles T, et al. Nature. 2014.

• Non-muscle invasive disease– Building upon BCG– Beyond BCG
• Locally advanced disease– Neoadjuvant/adjuvant
• Metastatic disease– Four agents approved– Phase III trial demonstrating survival compared to chemotherapy
• Combinatorial strategies – Extending the benefit to more patients
Immunotherapeutics in Bladder Cancer

Agenda
Agenda Item Speaker
8:00-8:15 AM Welcome/Introductions/Pretest Dr. Kamat, Chair
8:15-8:25 AM Immunotherapy in Bladder Cancer: Basic Concepts Dr. Dreicer
8:25-9:05 AM Clinical Experience with Immunotherapy in Bladder Cancer
8:25-8:40 AM ICIs in Advanced/Metastatic Disease and Lessons Learned Dr. Bellmunt
8:40-8:50 AM Predictive Biomarkers for Checkpoint Blockade Therapy Dr. Dinney
8:50-9:05 AM Roundtable Discussion Dr. Dreicer (Moderator)
9:05-9:50 AM Practical Aspects of Immune Checkpoint Inhibitors
9:05-9:15 AM Safety Profile of ICIs: Early Recognition & Management Dr. Dreicer
9:15-9:25 AM Ways Urologists Can Adopt ICI into Clinical Practice: Med Onc Perspective Dr. Bellmunt
9:25-9:35 AM Ways Urologists Can Adopt ICI into Clinical Practice: Urologist’s Perspective Dr. Dinney
9:35-9:50 AM Roundtable Discussion Dr. Kamat (Moderator)
9:50-10:00 AM Concluding Remarks/Posttest Dr. Kamat, Chair

Joaquim Bellmunt, MD PhDAssociate Professor of Medicine
Harvard Medical School
Dana-Farber Cancer Institute
Immune Checkpoint Inhibitors (ICIs)in Advanced/Metastatic Disease and
Lessons Learned from Other Malignancies

Overview of APPROVED Checkpoint Inhibitors in THE US, EU, and JAPAN*
US EU Japan
PD-1 PD-L1 CTLA-4 Combination
Nivolumab1-3 Pembrolizumab4-6 Atezolizumab7 Durvalumab11 Avelumab8 Ipilimumab9,10 Nivolumab + ipilimumab1,2
Manufacturer BMS Merck Roche/Genentech AstraZeneca EMD Serono BMS BMS
Line 1L+ 2L+ 3L+ 1L+ 2L+ 3L+ 1L+** 2L+ 2L+ 1L+ 2L+ 1L+ 1L+
mMelanoma
mNSCLC
aRCC
cHL
mSCCHN
mUC
mMCC
Treatment schedule
q2w q3w q3w q2w q2w q3w X4Nivo then ipiq3w X4, then
nivo q2w
Atezolizumab, avelumab, durvalumab, and tremelimumab are not currently approved in Europe (status as of 05/10/2017).
*As of May 10, 2017. Please refer to product labeling for approved indications for each tumor type. **For cisplatin-ineligible patients only
1L, first line; 2L, second line; 3L, third line; aRCC, advanced renal cell carcinoma; cHL, classical Hodgkin lymphoma; CTLA-4, cytotoxic T-lymphocyte antigen-4; DTC, differentiated thyroid cancer; EU, European Union; ipi, ipilimumab; IV, intravenous; mMCC, metastatic Merkel cell carcinoma; mMelanoma, metastatic melanoma; mNSCLC, metastatic non-small cell lung cancer; mRCC, metastatic renal cell carcinoma; mSCCHN, metastatic squamous cell carcinoma of the head and neck; mUC, metastatic urothelial carcinoma; nivo, nivolumab; PD-1, programmed death receptor-1; PD-L1, programmed death ligand 1; PO, orally; q2w, every 2 weeks; q3w, every 3 weeks.1Nivolumab U.S. Prescribing Information. 2Nivolumab EU Prescribing Information. 3Ono Pharmaceuticals, Japan [Press Release]. 4Pembrolizumab U.S. Prescribing Information. 5Pembrolizumab EU Prescribing Information. 6Merck, Japan [Press Release]. 7Atezolizumab U.S. Prescribing Information. 8Avelumab U.S. Prescribing Information. 9Ipilimumab U.S. Prescribing Information. 10Ipilimumab EU Prescribing Information. 11Durvalumab U.S. Prescribing Information

Pembrolizumab Updated Results and Biomarker Analysis from KEYNOTE-012
Overall Response Rate = 28% (8/33)
64% experienced a decrease in target lesions
–30% decrease
Ch
ange
Fro
m B
ase
line
in S
um
of
Lon
gest
D
iam
eter
of
Targ
et L
esio
n, %
Median OS (N = 29) 12.7 months (95% CI 5.7-NR)12m OS = 52.9%
Analysis cutoff date: March 23, 2015.
Plimack ER, et al. Lancet Oncol. 2017.

IMvigor210, CheckMate 275, STUDY 1108 and JAVELIN: Recent Investigational and Registrational Trials in Pretreated mUC*
Patient number
Study Arms
Key Inclusion Criteria
Primary Endpoints
PD-L1 expressionPD-L1+PD-L1-NE/unknown
*No head-to-head studies have been conducted and direct comparisons cannot be made between these studies. †265 patients were evaluated for efficacy. ‡191 locally advanced/mUC patients enrolled and received treatment; 103 patients were eligible for efficacy analysis..§241 mUC patients were evaluated for safety and 153 mUC patients were evaluated for efficacy.BOR, best overall response; ECOG, Eastern Cooperative Oncology Group performance score; IC, immune cell; NE, not evaluable; ORR, objective response rate; PD-L1, programmed death ligand 1; TC, tumor cell
1Loriot Y, et al. Poster presentation at ESMO 2016. 783P; 2Sharma P, et al. Lancet Oncol. 2017; 3Powles T, et al. Poster presentation at 2017 ASCO GU. 286. 4Patel M, et al. Poster presentation at 2017 ASCO GU. 330.
CheckMate 2752
NivolumabPhase 2
270†
Nivolumab 3 mg/kg IV q2w
• ≥1 Platinum-containing or ≤12 months of neoadjuvant/adjuvant treatment
• Tumor tissue for PD-L1 testing• ECOG PS 0-1
• ORR
1% cut-off on TC• 46%• 54%
Study 11083
DurvalumabPhase 1/2
191‡
Durvalumab10 mg/kg IV q2w
• Histologically confirmed solid tumors
Locally advanced or mUC cohort:• Had progressed, on were
ineligible for, or refused any number of prior therapies
• ECOG PS 0-1
• Safety• ORR
25% cut-off on TC or IC• 51.3%• 41.4%• 7.3%
IMvigor 2101
Atezolizumab Phase 2
310 (Cohort 2)
Atezolizumab 1200 mg IV q3w
Cohort 2:• ≥1 Platinum-containing or ≤12
months of neoadjuvant/adjuvant treatment
• Tumor tissue for PD-L1 testing• ECOG PS 0-1
• ORR
IC1/2/3 (1% cut-off on IC)• 67%• 33%
JAVELIN solid tumor4
AvelumabPhase 1
241§
Avelumab 10 mg/kg IV q2w
• Solid tumors
mUC cohort:• Had progressed on post-
platinum treatment or cisplatin-ineligible
• Unselected for PD-L1• ECOG PS 0-1
• BOR• Safety
5% cut-off on TC• 33.6%• 48.5%• 17.8%

Phase 1 Evaluation of Pembrolizumab, Avelumab, Atezolizumab and Durvalumab in Advanced UC Shows Robust Activity
PembrolizumabPlimack 2017 AtezolizumabPowles 2014
AvelumabApolo 2016 DurvalumabMassard 2016

Phase II Studies with PD1/PD-L1 INHIBITORSin Second Line and Beyond (Platinum Treated)

Rosenberg JE, et al. Lancet. 2016.

Outcome, %All
N=265
Confirmed ORR by BIRCa 19.6
95% CI 15.0–24.9
Median PFS in months (95% CI) 2.00 (1.87–2.63)
Median OS in months (95% CI) 8.74 (6.05–NR)
PD-L1 <1%n=143
PD-L1 ≥1%n=122
PD-L1<5%n=184
PD-L1 ≥5%n=81
16.1 23.8 15.8 28.4
10.5–23.1 16.5–32.3 10.8–21.8 18.9–39.5
1.87 (1.77–2.04)
3.55 (1.94–3.71)
5.95 (4.30–8.08)
11.30 (8.74–NR)
In 52 responders • Time to response: 1.9 months (1.6–5.9)• Duration of response: NR (7.4-NR)• Ongoing responders at time of response: 40/52 (77%)
Safety: no new safety profile compare to prior reports
aBIRC, blinded independent review committee
Phase II CheckMate 275 studyAntitumor Activity of Nivolumab
Sharma P, et al. Lancet Oncol. 2017.

Phase I/II Studies with PD1/PD-L1 InhibitorsFirst-Line
“Unfit” Patients

Balar AV, et al. Lancet. 2017.

Agent and Indication(s) Dosing Guideline
Avelumab (PD-L1–blocking antibody)• Locally advanced or metastatic urothelial carcinoma (mUC) with disease progression during or
following platinum-containing chemotherapy or disease progression within 12 months of neoadjuvant or adjuvant treatment with platinum-containing chemotherapy
10 mg/kg as an intravenous infusion over 60 minutes every 2 weeks.Premedicate for the first 4 infusions and subsequently as needed.
Atezolizumab (PD-L1–blocking antibody)• Locally advanced or metastatic urothelial carcinoma (mUC) with disease progression during or
following platinum-containing chemotherapy or disease progression within 12 months of neoadjuvant or adjuvant treatment with platinum-containing chemotherapy
• Locally advanced or mUC who are not eligible for cisplatin chemotherapy (initial treatment)
1200 mg IV every 3weeks; treat until disease progression or unacceptable toxicity. Infuse over 1 hr for initial infusion; if tolerated, subsequent infusions may be given over 30 mins.
Durvalumab (PD-L1–blocking antibody)
• Patients with locally advanced or metastatic urothelial carcinoma (mUC) who have disease progression during or following platinum-containing chemotherapy or disease progression within 12 months of neoadjuvant or adjuvant treatment with platinum-containing chemotherapy
10 mg/kg as an intravenous infusion over 60 minutes every 2 weeks.
Nivolumab (PD-1–blocking antibody)• Patients with locally advanced or metastatic urothelial carcinoma (mUC) who have disease
progression during or following platinum-containing chemotherapy or disease progression within 12 months of neoadjuvant or adjuvant treatment with platinum-containing chemotherapy
240 mg administered as an intravenous infusion over 60 minutes every 2 weeks until disease progression or unacceptable toxicity.
FDA-Approved Immune Checkpoint Inhibitors for Urothelial Carcinoma
FDA Prescribing Information.

Objective Response (by PD-L1 Subgroups)
N = 100
CPS <1%†
N = 33CPS ≥1% to <10%
N = 33CPS ≥10%
N = 30
n % (95% CI) n % (95% CI) n % (95% CI)
ORR ( 24%) 6 18% (7-36%) 5 15% (5-32%) 11 37% (20-56%)
Complete response 1 3% (0.1-16%) 0 – 4 13% (4-31%)
Partial response 5 15% (5-32%) 5 15% (5-32%) 7 23% (10-42%)
Stable disease 3 9% (2-24%) 5 15% (5-32%) 7 23% (10-42%)
Data cutoff date: June 1, 2016
†Excluding those with CPS unknown
• The PD-L1 high expression cut point was determined to be CPS ≥10% (PD-L1 positive tumor, immune cells) and enriched for response; this cut point will be validated in the remaining patients in the cohort (n = 274 additional patients)
• Median time to response: 2.0 months (range, 1.9-4.8) • Median duration of response : Not reached (range, 1.4+ to 9.8+ months)• Duration of response rate ≥6 months: 83%
*CPS = combined positive score for PD-L1–positive cells (tumor, immune cells)
KEYNOTE-052: Pembrolizumab1st-Line Therapy for Cisplatin-Ineligible
Balar, et al. Ann Oncol. 2016.

KEYNOTE-045 Study Design (NCT02256436)1
SECOND LINE Phase III
IMvigor211 Study Design (NCT02302807)2
Estimated timelines Estimated completion: Sept 2016 (Early termination)
Pembrolizumab
SOC:Paclitaxel,
Docetaxel or Vinflunine
Secondary end points
•ORR•Safety
Primary end points•OS•PFS
• Urothelial cancer
• Progression or recurrence of urothelial cancer following a first-line platinum-containing regimen.
• No more than 2 prior lines of systemic chemotherapy.
RandomizationN = 542 patients
1Bellmunt J, et al. N Engl J Med. 2017; 2Clinicaltrials.gov.
Estimated timelines Estimated completion: Nov 2017
Atezolizumab
SOC:Docetaxel,
Paclitaxel or Vinflunine
Secondary end points
•ORR•PFS•DOR•Safety
Primary end points
•OS • Urothelial cancer
• Progression or recurrence of urothelial cancer following a first-line platinum-containing regimen.
RandomizationN = 932 patients

Bellmunt J, et al. N Engl J Med. 2017.
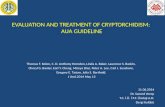
43.9%30.7%
KEYNOTE-045 Study (NCT02256436) Overall Survival: Total
Median (95% CI)10.3 mo (8.0-11.8) 7.4 mo (6.1-8.3)
270 226 194 169 147 131 87 54 27 13 4 0 0
272 232 171 138 109 89 55 27 14 3 0 0 0
No. at risk
Events, n HR (95% CI) P
Pembro 155 0.73 (0.59-0.91) 0.0022
Chemo 179

Bellmunt J, et al. N Engl J Med. 2017.
Confirmed Objective Response Rate
Assessed per RECIST v1.1 by blinded, independent central review.Data cutoff date: Sep 7, 2016.
No alpha allocated to the comparison of ORR in the CPS ≥10% population.
0
5
10
15
20
25
30
35
40
OR
R, %
(9
5%
CI) 21.1%
11.4%
Δ9.6%P = 0.0011
PR
CR
Total Population
0
5
10
15
20
25
30
35
40
OR
R, %
(9
5%
CI)
21.6%
6.7%
CPS ≥10% Population
7.0%
14.1%3.3%
8.1%
6.8%
14.9%
2.2%4.4%
Pembrolizumab(N = 270)
Chemotherapy(N = 272)
Pembrolizumab(N = 74)
Chemotherapy(N = 90)

0
5
10
15
20
25
30
Inci
de
nce
, %
Data cutoff date: Sep 7, 2016.
Pembrolizumab
1-2 3-5Grade
Bellmunt J, et al. N Engl J Med. 2017.
Treatment-Related AEs with Incidence ≥10%

0
5
10
15
20
25
30
Inci
de
nce
, %Treatment-Related AEs with Incidence ≥10%
Pembrolizumab
1-2 3-5Grade
Bellmunt J, et al. N Engl J Med. 2017.
Chemotherapy
Alopecia occurred in 37.6% of patients in the chemotherapy arm.Data cutoff date: Sep 7, 2016.

• The primary efficacy endpoint, overall survival, was to be tested in a successive fashion in study populations defined by PD-L1 expression.
• The first population tested was people with the highest levels of PD-L1 expression (IC2/3), followed by those with any level of PD-L1 expression (IC1/2/3), and followed by the overall study population (Intention-To-Treat; ITT).
• Statistical significance needed to be achieved in the IC2/3 population in order to evaluate the IC1/2/3 population for statistical significance, and similarly achieved in the IC1/2/3 population in order to evaluate the overall study population for statistical significance.

• Exciting times in the treatment of urothelial carcinoma
• Immunotherapy is a well tolerated and active treatment for our patients
• Many open questions remain with regards to understanding predicting factors
• Several other novel immunotherapies are in clinical development
– Checkpoint inhibitors
– Combinations
– Antibody drug conjugates
– Targeted agents
Immunotherapy in UC - Conclusions

Agenda
Agenda Item Speaker
8:00-8:15 AM Welcome/Introductions/Pretest Dr. Kamat, Chair
8:15-8:25 AM Immunotherapy in Bladder Cancer: Basic Concepts Dr. Dreicer
8:25-9:05 AM Clinical Experience with Immunotherapy in Bladder Cancer
8:25-8:40 AM ICI in Advanced/Met Disease and Lessons Learned Dr. Bellmunt
8:40-8:50 AM Predictive Biomarkers for Checkpoint Blockade Therapy Dr. Dinney
8:50-9:05 AM Roundtable Discussion Dr. Dreicer (Moderator)
9:05-9:50 AM Practical Aspects of Immune Checkpoint Inhibitors
9:05-9:15 AM Safety Profile of ICIs: Early Recognition & Management Dr. Dreicer
9:15-9:25 AM Ways Urologists Can Adopt ICI into Clinical Practice: Med Onc Perspective Dr. Bellmunt
9:25-9:35 AM Ways Urologists Can Adopt ICI into Clinical Practice: Urologist’s Perspective Dr. Dinney
9:35-9:50 AM Roundtable Discussion Dr. Kamat (Moderator)
9:50-10:00 AM Concluding Remarks/Posttest Dr. Kamat, Chair

Colin P.N. Dinney, MDDepartment of Urology
MD Anderson Cancer Center
Predictive Biomarkers for Checkpoint Blockade Therapy

• Tumors with high PD-L1 expression will be more susceptible to checkpoint blockade.
• Phase I trials with nivolumab (anti PD-1) and atezolizumab revealed 18-25% response rates.
• Nivolumab: 36% (9/25) with >5% tumor cell PD-L1 expression responded compared with 0/17 with neg. expression (Mouse anti human PDL-1 (clone 5H1)1
• Atezolizumab: highest response was in tumors with >10% TIL staining (Rabbit anti-human PD-L1 (clone SP142)2
• Different antibodies, different target tissue
Hypothesis
1Topalian SL, et al. N Engl J Med. 2012; 2Herbst RS, et al. Nature. 2014.

• Powles, et al. Nature. 2014. Phase I Atezolizumab
• Rosenberg, et al. Lancet. 2016. Phase II Atezolizumab
• Balar, et al. Lancet. 2017. Phase II Atezolizumab
• Massard, et al. J Clin Oncol. 2016. Phase I Durvalumab
• Sharma, et al. Lancet Oncol. 2016. Phase I/II Nivolumab
• Sharma, et al. Lancet Oncol. 2017. Phase I/II Nivolumab
• Plimack, et al. Lancet Oncol. 2017. Phase I Pembrolizumab
• Bellmunt, et al. N Engl J Med. 2017. Phase III Pembrolizumab
PD-L1 Expression as a Predictor of Checkpoint Blockade Sensitivity in UC
5/8 studies reported positive association with PD-L1 staining

Summary of the Results
Study AgentCompanion IHC
AntibodyThreshold for
PositivityTarget Cells
Assay Associated w/ Response?
Powles T, et al. Nature. 2014. Atezolizumab “Proprietary” 5% TILs Yes
Rosenberg JE, et al. Lancet. 2016. Atezolizumab SP142 5% TILs Yes
Balar AV, et al. Lancet. 2017. (platinum ineligible)
Atezolizumab SP142 5% TILs No
Massard C, et al. J Clin Oncol. 2017. Durvalumab SP263 25%TILs &
TCsYes
Sharma P, et al. Lancet Oncol. 2016. Nivolumab Dako 28-8 1% TCs No
Sharma P, et al. Lancet Oncol. 2017. Nivolumab Dako 28-8 1% TCs Yes
Plimack ER, et al. Lancet Oncol. 2017.
Pembrolizumab 22C3 1%TILs &
TCsTILs only
Bellmunt J, et al. N Engl J Med. 2017. (chemo vs immuno 2nd line)
Pembrolizumab 22C3 10%TILs &
TCsNo

Can PD-L1-negative Cells become PD-L1-positive?Adaptive Regulation of PD-L1 Expression
MPDL3280A
PD-L1CD8
Baseline
PD-L1CD8
On-Tx
Powderly, ASCO 2013.
Anti-PD-L1
T cells and tumor cells expressing PD-L1
Question: Instead of focusing so much attention on a single marker such as PD-L1, should we consider additional biomarkers such as T-cell subsets and tumor burden?
CD8 T-cells PD-L1 CD8 T-cells PD-L1

• PD-L1 expression associated with worse overall mortality after cystectomy for organ-confined disease (HR: 3.2).1
• No association with PD-L1 expression and post-cystectomy survival.2
• No association of PD-L1 TC staining with outcomes, but positive association of PD-L1 IC staining with improved survival in M1 patients.3
PD-L1 Expression As A Prognostic Biomarker In Bladder Cancer? The Jury is Still Out
1Boorjian SA, et al. Clin Cancer Res. 2008; 2Faraj SF, et al. Urology. 2015; 3Bellmunt J, et al. Ann Oncol. 2015.

• What cells are important? Tumor cells vs ICs?
• What is the appropriate threshold for positive staining?
• Which assays are more reliable? – “Blueprint project” – industry sponsored comparison of four companion
assays• SP142 is outlier with consistently lower scoring
• More inter-observer variability with IC with intraclass correlation coefficients 0.2 c/w 0.8 for TC
• 37% of patients had assay-dependent classification (one or more of 4 assays would reclassify response).
Why No Consistent Performance?
Hirsch FR, et al. J Thorac Oncol. 2017.

• PD-L1 “positivity” inconsistently enriches for clinical benefit
• For bladder cancer, there is currently no requirement for PD-L1 testing prior to checkpoint blockade therapy
• IHC is unreliable for measuring PD-L1 expression
• Mutational burden correlates with response
• Need to look beyond a single static biomarker
Bottom Line

Agenda
Agenda Item Speaker
8:00-8:15 AM Welcome/Introductions/Pretest Dr. Kamat, Chair
8:15-8:25 AM Immunotherapy in Bladder Cancer: Basic Concepts Dr. Dreicer
8:25-9:05 AM Clinical Experience with Immunotherapy in Bladder Cancer
8:25-8:40 AM ICI in Advanced/Met Disease and Lessons Learned Dr. Bellmunt
8:40-8:50 AM Predictive Biomarkers for Checkpoint Blockade Therapy Dr. Dinney
8:50-9:05 AM Roundtable Discussion Dr. Dreicer (Moderator)
9:05-9:50 AM Practical Aspects of Immune Checkpoint Inhibitors
9:05-9:15 AM Safety Profile of ICIs: Early Recognition & Management Dr. Dreicer
9:15-9:25 AM Ways Urologists Can Adopt ICI into Clinical Practice: Med Onc Perspective Dr. Bellmunt
9:25-9:35 AM Ways Urologists Can Adopt ICI into Clinical Practice: Urologist’s Perspective Dr. Dinney
9:35-9:50 AM Roundtable Discussion Dr. Kamat (Moderator)
9:50-10:00 AM Concluding Remarks/Posttest Dr. Kamat, Chair

1. What is the “sense” of the urologic community to the emergence of checkpoint inhibitor therapy in advanced disease and how may it help drive clinical trials in both non-muscle invasive and locally advanced disease?
2. Given the different PD-L1 assays and the results of trials to date, is there a role for routine PD-L1 testing in urothelial cancer?
3. What is the future for chemotherapy in bladder cancer?
4. Can you envision a role for cytoreductive surgery in metastatic urothelial cancer in the context of immunotherapy?
Roundtable Discussion 1

Agenda
Agenda Item Speaker
8:00-8:15 AM Welcome/Introductions/Pretest Dr. Kamat, Chair
8:15-8:25 AM Immunotherapy in Bladder Cancer: Basic Concepts Dr. Dreicer
8:25-9:05 AM Clinical Experience with Immunotherapy in Bladder Cancer
8:25-8:40 AM ICI in Advanced/Met Disease and Lessons Learned Dr. Bellmunt
8:40-8:50 AM Predictive Biomarkers for Checkpoint Blockade Therapy Dr. Dinney
8:50-9:05 AM Roundtable Discussion Dr. Dreicer (Moderator)
9:05-9:50 AM Practical Aspects of Immune Checkpoint Inhibitors
9:05-9:15 AM Safety Profile of ICIs: Early Recognition & Management Dr. Dreicer
9:15-9:25 AM Ways Urologists Can Adopt ICI into Clinical Practice: Med Onc Perspective Dr. Bellmunt
9:25-9:35 AM Ways Urologists Can Adopt ICI into Clinical Practice: Urologist’s Perspective Dr. Dinney
9:35-9:50 AM Roundtable Discussion Dr. Kamat (Moderator)
9:50-10:00 AM Concluding Remarks/Posttest Dr. Kamat, Chair

Robert Dreicer, MD, MS, MACP, FASCO
Safety Profile of Checkpoint Inhibitors: Early Recognition & Management Strategies

• Major side effects of immunotherapy are related to development of “autoimmunity”
• Immune-related adverse events, also known as “immune-mediated adverse events” (irAEs, imAEs), may occur in any organ system
• Certain events may be life threatening or fatal
• Prompt recognition of potentially severe irAEs improves outcomes
• Combining checkpoint inhibitors with agents such at CTLA4 inhibitors significantly increases irAEs
Toxicity of Immune Checkpoint Blockade

Teply BA and Lipson EJ. Oncology. 2014.
Immune-Related Adverse Events
GastrointestinalColitis/diarrhea
NeuromuscularPeripheral sensory
neuropathy
RespiratoryPneumonitis
HepaticAutoimmune hepatitis
ALT/AST increases
RenalNephritis
Renal failure
SkinMaculopapular rash
Pruritus
EndocrineHypophysitis
ThyroiditisType 1 diabetes

Avelumab Atezolizumab Durvalumab Nivolumab
Adverse Event, (%) All Grades Grades 3-4 All Grades Grades 3-4 All Grades Grades 3-4 All Grades Grades 3-4
Gen - Fatigue 41 7 52 6 39 6 46 7
Gen – Peripheral edema 17 0.4 18 1 15 2 13 0.4
Gen - Pyrexia 16 1 21 1 14 1 17 0.4
GI - Constipation 18 1 21 0.3 21 1 16 0.4
GI - Nausea 24 1 25 2 16 2 22 0.7
GI - Vomiting 14 1 17 1 - - 12 1.9
GI – Abdominal pain 19 2 17 4 14 3 13 1.5
GI – Diarrhea/colitis 18 2 18 1 13 1 17 2.6
Resp - Cough 14 0 14 0.3 10 0 18 0
Resp - Dyspnea 17 2 16 4 13 2 14 3.3
Skin - Rash 15 0.4 15 0.3 11 1 16 1.5
GU - UTI 21 5 22 9 15 4 17 7
GU - Hematuria - - 14 3 - - - -
Musculoskeletal pain 25 3 15 2 24 4 30 2.6
Reduced appetite 21 2 26 1 19 1 22 2.2
U.S. FDA Prescribing Information
Checkpoint Inhibitor Adverse Events(occurring in ≥10% of those with urothelial cancer that has progressed on platinum-containing regimen)

Adverse event Severity Dose modification
Colitis
Grade 2 diarrhea or colitis Withhold dose
Grade 3 diarrhea or colitisWithhold dose when administered as single agent
Grade 4 diarrhea or colitis Permanently discontinue
PneumonitisGrade 2 Withhold dose
Grade 3 or 4 Permanently discontinue
HepatitisAST or ALT >3 and up to 5x ULN or T bili >1.5 and up to 3x ULN Withhold dose
AST or ALT >5x ULN or T bili >3x ULN Permanently discontinue
NephritisSerum creatinine >1.5 and up to 6x ULN Withhold dose
Serum creatinine more than 6x ULN Permanently discontinue
Nivolumab Prescribing Information.
Nivolumab: Management of Selected AEs

Nivolumab Prescribing Information.
Nivolumab: Management of Selected AEs
Adverse event Severity Dose modification
Skin
Grade 3 rash or suspected Stevens-Johnson syndrome (SJS) or TEN
Withhold dose
Grade 4 rash or confirmed SJS or TEN Permanently discontinue
Other
Grade 3 AE1st occurrenceRecurrence of same grade 3 AE
Withhold dosePermanently discontinue
Life threatening or grade 4 AE Permanently discontinue
Requirement for prednisone or equivalent 10 mg daily for >12 weeks
Permanently discontinue
Persistent grade 2 or 3 AEs lasting12 weeks or longer
Permanently discontinue

• Anti-TNFα chimeric mAb (infliximab) → binds circulating TNFα
• Indications include ankylosing spondylitis, Crohn’s, psoriasis/psoriatic arthritis, rheumatoid arthritis, ulcerative colitis
• Dosing – Standard (rheumatologic conditions): 5 mg/kg IV at 0, 2, and 6 weeks,
then every 8 weeks maintenance– For irAEs, 5 mg/kg IV x 1 or 2 doses often sufficient to control
symptoms
Management Beyond Steroids
Naidoo J, et al. Ann Oncol. 2016; Infliximab Prescribing Information.

• No reliable means to predict who or when patients will develop irAEs
– History of autoimmunity exclusionary in clinical trials
– irAE may reflect nascent autoimmunity unmasked by checkpoint blockade
• Early diagnosis and aggressive systemic corticosteroids are key to prevent life-threatening consequences
• Biologics (TNFα antagonists) are highly effective in management of irAEs refractory to high-dose steroids or steroid-taper refractory
– Potential use as first-line treatment
Immune-Related Adverse Events

• Immune checkpoint inhibitor therapy is NOT chemotherapy
– Patient education, close follow-up MANDATORY
• Education of our colleagues (i.e. Hospital Medicine, Family Medicine, ER, and Internal Medicine docs) is critical
– Colitis
• Combination IO therapies have potential to improve outcomes, but with a potential price in toxicity
• Implications for an older patient population
Immune-Related Adverse Events: Caveats

Agenda
Agenda Item Speaker
8:00-8:15 AM Welcome/Introductions/Pretest Dr. Kamat, Chair
8:15-8:25 AM Immunotherapy in Bladder Cancer: Basic Concepts Dr. Dreicer
8:25-9:05 AM Clinical Experience with Immunotherapy in Bladder Cancer
8:25-8:40 AM ICI in Advanced/Met Disease and Lessons Learned Dr. Bellmunt
8:40-8:50 AM Predictive Biomarkers for Checkpoint Blockade Therapy Dr. Dinney
8:50-9:05 AM Roundtable Discussion Dr. Dreicer (Moderator)
9:05-9:50 AM Practical Aspects of Immune Checkpoint Inhibitors
9:05-9:15 AM Safety Profile of ICIs: Early Recognition & Management Dr. Dreicer
9:15-9:25 AM Ways Urologists Can Adopt ICI into Clinical Practice: Med Onc Perspective Dr. Bellmunt
9:25-9:35 AM Ways Urologists Can Adopt ICI into Clinical Practice: Urologist’s Perspective Dr. Dinney
9:35-9:50 AM Roundtable Discussion Dr. Kamat (Moderator)
9:50-10:00 AM Concluding Remarks/Posttest Dr. Kamat, Chair

Joaquim Bellmunt, MD
Ways Urologists Can Adopt ICI into Clinical Practice: Medical Oncologist’s Perspective

20161989 1993 1997 2001 2005 2009 2013
MVAC (Ph II)1
Paclitaxel (Ph II)2
Docetaxel (Ph II)4
Gemcitabine + Cisplatin (Ph III)5
HD-MVAC (Ph III)6
Gemcitabine + Paclitaxel (Ph II)7
Vinflunine (Ph III)9
Gemcitabine + Carboplatin / MCaVi (Ph III)11
Gemcitabine + Cisplatin + Paclitaxel (Ph III)12
Gemcitabine authorisation in UK
(Oct 26, '95)3Gemcitabine
EMA harmonisation (Sep 23, '08)8
Vinflunine EMA approval (Sep 21, '09)10
1Sternberg CN, et al. Cancer. 1989; 2Roth BJ, et al. J Clin Oncol. 1994; 3Eli Lilly. SmPC Gemzar® 01-Jul-2014 (www.medicined.org.uk); 4McCaffrey JA, et al. J Clin Oncol. 1997; 5Von der Maase H, et al. J Clin Oncol. 2000; 6Sternberg CN, et al. J Clin Oncol. 2001; 7Meluch AA, et al. J Clin Oncol. 2001; 8EMA. EMEA/CHMP/512295/2008; 24.09.2018 (www.ema.europa.eu); 9Bellmunt J, et al. J Clin Oncol. 2009; 10EMA. EMEA/H/C/000983; 2012 (www.ema.europa.eu); 11De Santis M, et al. J Clin Oncol. 2009; 12Bellmunt J, et al. J Clin Oncol. 2012.
Pu
blic
atio
nA
gen
cy A
ctio
n
Evolution of Systemic Therapy for Urothelial Cancer

2016 20171989 1993 1997 2001 2005 2009 2013
MVAC (Ph II)1
Paclitaxel (Ph II)2
Docetaxel (Ph II)4
Gemcitabine + Cisplatin (Ph III)5
HD-MVAC (Ph III)6
Gemcitabine + Paclitaxel (Ph II)7
Vinflunine (Ph III)9
Gemcitabine + Carboplatin / MCaVi (Ph III)11
Gemcitabine + Cisplatin + Paclitaxel (Ph III)12
Gemcitabine authorisation in UK
(Oct 26, '95)3Gemcitabine
EMA harmonisation (Sep 23, '08)8
Vinflunine EMA approval (Sep 21, '09)10
1Sternberg CN, et al. Cancer. 1989; 2Roth BJ, et al. J Clin Oncol. 1994; 3Eli Lilly. SmPC Gemzar® 01-Jul-2014 (www.medicined.org.uk); 4McCaffrey JA, et al. J Clin Oncol. 1997; 5Von der Maase H, et al. J Clin Oncol. 2000; 6Sternberg CN, et al. J Clin Oncol. 2001; 7Meluch AA, et al. J Clin Oncol. 2001; 8EMA. EMEA/CHMP/512295/2008; 24.09.2018 (www.ema.europa.eu); 9Bellmunt J, et al. J Clin Oncol. 2009; 10EMA. EMEA/H/C/000983; 2012 (www.ema.europa.eu); 11De Santis M, et al. J Clin Oncol. 2009; 12Bellmunt J, et al. J Clin Oncol. 2012; 13Rosenberg JE, et al. Lancet. 2016; 14Massard C et al. ASCO 2016: abstract #4502 and oral presentation; 15AstraZeneca. Press Release 17.02.2016 (access: www.astrazeneca.com); 16FDA. Press Release 18.05.2016 (access: www.fda.gov); 17Apolo AB, et al. J Clin Oncol. 2016; 18Galsky MD, et al. ESMO 2016: abstract #LBA31_PR; 19Balar A, et al. Ann Oncol. 2016.
Pu
blic
atio
nA
gen
cy A
ctio
nEvolution of Systemic Therapy for Urothelial Cancer
Nivolumab (Ph II)18
Pembrolizumab (Ph I/II)19
Durvalumab FDA breakthrough
designation (Feb 17, '16)15
Atezolizumab FDA approval
(May 18, '16)16
Atezolizumab (Ph II)13
Durvalumab (Ph I/II)14
Avelumab (Ph I)17
NivolumabFDA approval(Feb 2, 2017)
AtezolizumabFDA approval
1st line cis-inelig(Apr 16, 2017)
DurvalumabFDA approval(May 1, 2017)
AvelumabFDA approval(May 9, 2017)
PembroFDA approval (?June 2017?)

• Durability of responses
• Continued response or disease stabilization even off therapy
– Suggests induction of a tumour specific memory response
• Unconventional or delayed immune-mediated responses
• Overall tolerability as a monotherapy (good partner compound)
• Non-cumulative toxicities
Rationale to Use Anti-PD-1/L1 Further in GU: Distinct Features of PD-1/L1 Blockade
Motzer RJ, et al. J Clin Oncol. 2014; Amin A, et al. J Clin Oncol.2014; Topalian SL, et al. J Clin Oncol. 2014; Drake CG, et al. J Clin Oncol. 2013.

Safety Profile of IO Therapy in Patients With Advanced Bladder Cancer Differs from Systemic Chemotherapy1
Rash Pneumonitis Dyspnea
Colitis
Increased Aspartate Aminotransferase
Increased Alanine Aminotransferase
Adverse event monitoring and early identification of immune-mediated
adverse events is crucial to safe use of IO therapy2
Immune-related adverse reactions related to T-cell modulation may affect
various organ systems
Endocrinopathy(eg, thyroid dysfunction)
1Rosenberg JE, et al. Lancet. 2016; 2Helissey C, et al. J Geriatr Oncol. 2016.

• Effective management of severe irAEsbased on
– Early recognition: assess patients for signs/symptoms of enterocolitis, dermatitis, neuropathy, endocrinopathy, or hepatotoxicity at baseline and before each dose
– Frequent monitoring
– Use of corticosteroids (and/or other immunosuppressive therapies) combined with either delaying or discontinuing ipilimumab
• Experience from sites utilizing the following recommendations suggest that it minimizes morbidity and hospitalizations
Global Management of irAEs
• Screen patients for adverse events: Weekly call to pts for first 16 weeks
– Review checklist to assess key symptoms
– Reinforce importance of reporting any new or worsening symptom
• Monitor outpatients with ongoing AEs: minimum biweekly call
• For patients admitted to an outside hospital for AEs
– Frequent contact with admitting physician and subspecialist
– Provide guidance on detection and management of irAEs

NMIBC BCG refractory
MIBC Neoadjuvant:Cisplatin-eligible
MIBC Neoadjuvant:Cisplatin-ineligible
MIBC Adjuvant: Cisplatin-eligible
MIBC Adjuvant: Cisplatin refractor and cisplatin-ineligible
Metastatic Cisplatin-eligible Front-line
Metastatic Cisplatin-ineligible Front-line
Metastatic Maintenance after front-line
2nd line and beyond
Disease States Model For Immunotherapy
• Genomic inducers of response
– Somatic/germline profiling
– Neoantigen discovery
• Pathologic score to predict response
Adapted from Bellmunt J, et al. Cancer Treat Rev. 2017.

Where Do We Go from Here? Select Ongoing Trials in Bladder Cancer
Non-Muscle Invasive
KEYNOTE-057 (Ph 2): • Pembrolizumab in BCG
unresponsive NMIBC
NCT02792192 (Ph 1/2):• Atezolizumab ± BCG in high
risk NMIBC
Muscle Invasive
CheckMate 274 (Ph 3): • Nivolumab vs placebo
postsurgery MIBC
IMvigor 010 (Ph 3):• Atezolizumab vs observation
postsurgery PD-L1+ MIBC
DANUBE (Ph 3):• Durvalumab ± Tremelimumab
vs chemo Tx-naïve, unresectable, urothelial carcinoma
KEYNOTE-052 (Ph 2):• Pembrolizumab Tx-naïve,
cisplatin ineligible, locally advanced mUC
KEYNOTE-361 (Ph 3):• Pembrolizumab ± chemo vs
chemo in Tx-naïve advanced or mUC
IMvigor 130 (Ph 3):• Atezolizumab gem-cis vs gem-
cis in untreated advanced or mUC
Pretreated Metastatic
CheckMate 275 (Ph 2):• Nivolumab for locally
advanced or mUC after Pt failure
IMvigor 211 (Ph 3):• Atezolizumab vs chemo in
locally adv or mUC, after Pt failure
KEYNOTE-045 (Ph 3):• Pembrolizumab vs chemo in
locally adv or mUC, after Pt failure
JAVELIN Bladder 100 (Ph 3):• Avelumab as maintenance vs BSC for locally advanced mUC
Bellmunt J, et al. Cancer Treat Rev. 2017
Treatment NaïveMetastatic

The Future: Combinatorial Strategies
PD-1 Blockade
Immune Inhibitory Molecules
+
CTLA-4 AbLAG-3TIM3
Immune Stimulating Molecules
IL-2TLR agonistsCD-137 AbAnti-OX40
Targeted Therapies
VEGF TKIsmTOR inhibitorsVEGF AbHDAC inhibitors
Vaccines IMA901Dendritic cells
Chemotherapy
RadiationVanneman M and Dranoff G. Nat Rev Cancer. 2012.
Gemcitabine5-FU

MIBC, muscle-invasive bladder cancer1Amin MB, et al. Eur Urol. 2013; 2Hansel DE, et al. Eur Urol. 2013; 3Milowsky MI, et al. J Clin Oncol. 2016; 4Montironi R, et al. Arch Pathol Lab Med. 2016; 5NCCN Clinical Practice Guidelines in Oncology: Bladder Cancer V.2.2016.
Optimal Management of Advanced Bladder Cancer Requires a Multidisciplinary Approach1-5
Multidisciplinary Team
Medical Oncologist
OncologyNurse
Radiation Oncologist
Urologist
Pharmacist
• “Providing the best management for patients with bladder neoplasia relies on close cooperation and teamwork among urologists, oncologists, radiologists, and pathologists”
– 2nd International Consultation on Bladder Cancer1
• “Multidisciplinary input via tumor board discussions and/or directed consultations is critical to the optimal management of patients with MIBC and MBC”
– ASCO Clinical Practice Guideline Endorsement3

• Toxicity is mostly low grade and can be treated with supportive treatment.
• A concerted effort to educate the whole multidisciplinary team needs to take place and development of accessible algorithms to ensure minimized risk with toxicity.
• The key to successful management of checkpoint antibody toxicities is early diagnosis, high suspicion, excellent patient-provider communication, and rapid and aggressive use of corticosteroids and other immune suppressants for irAEs.
Conclusions

• The majority of both nivolumab and ipilimumab related AEs to date have been reversible and manageable by delaying study drug ±administration of corticosteroids; other immunosuppressants may also be needed.
• The following categories of AEs, requiring greater vigilance and early intervention: pulmonary, hepatic, renal, GI, endocrine, neurological, skin.
Conclusions

Agenda
Agenda Item Speaker
8:00-8:15 AM Welcome/Introductions/Pretest Dr. Kamat, Chair
8:15-8:25 AM Immunotherapy in Bladder Cancer: Basic Concepts Dr. Dreicer
8:25-9:05 AM Clinical Experience with Immunotherapy in Bladder Cancer
8:25-8:40 AM ICI in Advanced/Met Disease and Lessons Learned Dr. Bellmunt
8:40-8:50 AM Predictive Biomarkers for Checkpoint Blockade Therapy Dr. Dinney
8:50-9:05 AM Roundtable Discussion Dr. Dreicer (Moderator)
9:05-9:50 AM Practical Aspects of Immune Checkpoint Inhibitors
9:05-9:15 AM Safety Profile of ICIs: Early Recognition & Management Dr. Dreicer
9:15-9:25 AM Ways Urologists Can Adopt ICI into Clinical Practice: Med Onc Perspective Dr. Bellmunt
9:25-9:35 AM Ways Urologists Can Adopt ICI into Clinical Practice: Urologist’s Perspective Dr. Dinney
9:35-9:50 AM Roundtable Discussion Dr. Kamat (Moderator)
9:50-10:00 AM Concluding Remarks/Posttest Dr. Kamat, Chair

Colin P.N. Dinney, MD
Ways Urologists Can Adopt ICI into Clinical Practice: Urologist’s Perspective

• Unprecedented activity in the 2nd line metastatic setting
• Approved as 1st line therapy for platinum-ineligible metastatic disease
• Neoadjuvant and adjuvant trials ongoing
• Patient selection remains a challenge
Question: How do you identify platinum-eligible patients for chemotherapy or immunotherapy?
Immunotherapy for Locally Advanced and Metastatic UC

Immune Infiltration in MIBC
Cluster II Cluster IVCluster II Cluster IV
Basal TCGA Cluster IV tumors are enriched with lymphocytes
Choi adapted from TCGA

Bladder Cancer Molecular Taxonomy: Summary from a Consensus Meeting
Kamat AM, et al. Lancet. 2016.
TCGA Cluster II corresponds to the MDACC p53-like subtype

Subtype Specific Response to Chemotherapy
McConkey, et al. Eur Urol. 2016.
MDACC Discovery (P=0.018)
Choi, et al. Cancer Cell. 2014.

Lessons Learned from the IMvigor 210 Trial: Atezolizumab
• Basal tumors had the highest prevalence of immune infiltration.• Response was higher in the Luminal Cluster II (MDACC p53-like which is chemoresistant)• Non-overlapping sensitivity to chemo- and immunotherapy.
Rosenberg JE, et al. Lancet. 2016.

Ways Urologists Can Adopt ICI into Clinical PracticeWhat about NMIBC?

• Who should design and lead these trials?
• Which disease states?
• Which agents should be evaluated in this space?
• Does toxicity commensurate with disease lethality?
• Could checkpoint blockade inhibitors cause a delay or change in operative plan?
• How do you select the appropriate patients?
Questions for Checkpoint Blockade Inhibitor Therapy for NMIBC

• Single arm trials in BCG-unresponsive population
• BCG-failure group not a current approval strategy
• What about the BCG-intolerant patient?
• Randomized trials vs. BCG necessary for approval in the BCG-naïve population
• Does the progression rate and lethality of LG NMIBC justify extension to this indication?
• Anything short of a CR will be a treatment failure
Trial Design Considerations for Checkpoint Blockade in NMIBC

• Is it safe?
• Are checkpoint blockade biomarkers expressed by BCG naïve and unresponsive NMIBC?
• Does this matter?
• How effective are these agents?
• We don’t have much information yet
• Answers to some of these questions on the way
What Do We Know about Checkpoint Blockade Inhibitors in NMIBC So Far?

Immune-Mediated Adverse Events (imAEs)
• Pneumonitis
• Colitis
• Hypophysitis
• Dermatitis
• Hepatitis

Checkpoint biomarkers are expressed at relatively low levels
in untreated NMIBCs.
Checkpoint Blockade Biomarker Expressionin BCG Naive NMIBC

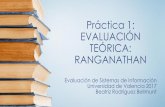
PD-L1 Expression Following BCG
Inman et al, Cancer 2007Inman BA, et al. Cancer. 2007.
UC demonstrating absence of PD-L1 staining (20x) UC demonstrating marked membranous PD-L1 staining (20x)
PD-L1+ BCG granuloma in recurrent UC (2.5x) PD-L1+ BCG granuloma in recurrent UC (40x)

PD-L1 Expression by Bladder Cancer
Bellmunt J, et al. Ann Oncol. 2015.
PD-L1 expression did not correlate with BCG exposure

Surveillance for 18 months
BCG unresponsive Ta/T1/Tis (TURBT)
MP
DL3
28
0A
cystocytol
MP
DL3
28
0A
MP
DL3
28
0A
MP
DL3
28
0A
cystobiopsy cytol
MP
DL3
28
0A
MP
DL3
28
0A
Phase II Trial of Atezolizumab (PD-L1) in BCG-Unresponsive NMIBC
MP
DL3
28
0A
MPDL3280Amaintenance
q3wks for 9 cyclesM
PD
L32
80
A
RFS @ 18months
q3 weeksCR @
21 weeks*(=6 months post TURBT)
q3 weeks9 weeks*
•Registration within 6 weeks of TURBT•Start therapy within 5 days of registration
* time is relative to first dose of MPDL3280A
Clinicaltrials.gov: NCT02844816.

Pembrolizumab (PD-1) for BCG-Unresponsive NMIBC
Patients with BCG-unresponsive
HR NMIBC
CystoscopyMonth 3
(q3m)
CystoscopyMonth 6 Cystoscopy
Month 24
Imaging Month 6
(q6m)
Imaging Month 24
Primary Endpoint: CR/DFSUp to 2 year of treatment with 1 year of post-treatment follow-up
Pembrolizumab 200 mg IV solution for infusion
… …Pembrolizumab (q3w)
Clinicaltrials.gov: NCT02625961.

BCG Unresponsive
NMIBCN=15
Month0 3 6 9 12 15 18 21 24
Legend
PD-1 or PD-L1 antibodyQ 2 weeks
rAd-IFN/Syn3 day 0 and day 1 Month 3
Primary End Point: Safety as per NCI CTCAE version 4.0
Secondary End Points:1. Rate of recurrent or progressive cancer at 24 months 2. Rate of patients able to tolerate ≥2 doses of rAd-IFN/Syn33. Tolerance as per AUASS
Correlative Studies: Urinary/blood: cytokines, DNA, mRNA, miRNA Q28 days x 6 Tissue biopsy at study entry and on progression: TIL characteristics IHC/Flow, cytokines, DNA, mRNA, miRNA
Combination Therapy Will be the KeySUO CTC rAd-Interferon (IFN)/Syn3 + Nivolumab
Proposed SUO CTC

• Decision should be data driven
• Early efficacy and tolerability will be available from ongoing trials
• Toxicity profile in the metastatic setting suggests that these agents can be delivered by urologists
• Comfort with delivering systemic therapy depends on training and support
• Cost/reimbursement and loss of technical fees will play a factor
• Availability of BCG
Checkpoint Blockade vs Intravesical Therapy?

• Role in locally advanced disease
• Patient selection is the key
• NMIBC is in a wait-and-see period
• Results from ongoing trials eagerly anticipated
• Support clinical trials and get smarter
Summary

Do you want to give up NMIBC as well?

Agenda
Agenda Item Speaker
8:00-8:15 AM Welcome/Introductions/Pretest Dr. Kamat, Chair
8:15-8:25 AM Immunotherapy in Bladder Cancer: Basic Concepts Dr. Dreicer
8:25-9:05 AM Clinical Experience with Immunotherapy in Bladder Cancer
8:25-8:40 AM ICI in Advanced/Met Disease and Lessons Learned Dr. Bellmunt
8:40-8:50 AM Predictive Biomarkers for Checkpoint Blockade Therapy Dr. Dinney
8:50-9:05 AM Roundtable Discussion Dr. Dreicer (Moderator)
9:05-9:50 AM Practical Aspects of Immune Checkpoint Inhibitors
9:05-9:15 AM Safety Profile of ICIs: Early Recognition & Management Dr. Dreicer
9:15-9:25 AM Ways Urologists Can Adopt ICI into Clinical Practice: Med Onc Perspective Dr. Bellmunt
9:25-9:35 AM Ways Urologists Can Adopt ICI into Clinical Practice: Urologist’s Perspective Dr. Dinney
9:35-9:50 AM Roundtable Discussion Dr. Kamat (Moderator)
9:50-10:00 AM Concluding Remarks/Posttest Dr. Kamat, Chair

1. Are there any differences in the safety profile of the various PD-L1 and PD-1 inhibitors or can they be considered one “class”?
2. What are the challenges in imAE identification and management, especially for those not accustomed to administering chemotherapy?
3. What are the most challenging imAEs to treat and why? Which potential imAEs are most likely to guide your patient selection? Given urologists’ knowledge of UC patients, which of the presented imAEs could present particular challenges?
4. What practical points would you make to a busy urological practice looking to incorporate IO agents into their practice—say for MIBC/NMIBC?
Roundtable Discussion 2