Immunologic disease: Progress in wiping the slate clean
48
AURA June 4, 2016 Immunologic disease: Progress in wiping the slate clean Gregg J. Silverman, M.D. Professor of Medicine and Pathology Laboratory of B cell Immunobiology NYU School of Medicine
Transcript of Immunologic disease: Progress in wiping the slate clean

AURA June 4, 2016 Immunologic disease: Progress in wiping the slate clean
Gregg J. Silverman, M.D. Professor of Medicine and Pathology Laboratory of B cell Immunobiology NYU School of Medicine

Disclosures
• Dr. Silverman has been a consultant for Genentech, Roche, Pfizer, Onyx, BMS, Lilly, Crescendo, Quest Diagnostics
• Research support from RRF, Lupus Research Foundation, Alliance for Lupus Research and NIH-NIAID
• FDA approval will be mentioned when relevant
2

Copyright (©2009) from The Immune System, Third Edition by Parham. Reproduced by permission of Garland Science/Taylor & Francis Books, LLC.
Figure 1.9 The Immune System, Third Edition
Immune system is composed of two systems: Overlay of the adaptive immune provides advantages
Good memory provides host advantages But Bad memory can drive autoimmunity

Antigen receptor genes move during B- and T-cell differentiation
Somatic recombination generates an effectively limitless range of antigen receptors from a limited number of germline minigenes

Signal 1+ Signal 2 = activation
1
2
1
Signal 1 only = death/inactivation
Courtesy of M. Cancro, U Penn Signal 3 – molds the immune bias of the lymphocyte
The adaptive immune system continuously generates lymphocyte clones with randomly generated antigen receptors. How do we maintain immune tolerance in health?
Two signal hypothesis (Bretscher and Cohn) Science 1970 169(3950):1042-9.

Subset of MHC II genes (shared epitope) predisposes to RA autoantigen-specific T/B cell clonal expansions
Plenge RM et al. N Engl J Med. 2007;357(12):1199-1209.
Chromosome The grey horizontal line indicates SNPs that are significant at a genomewide level *SNPs plotted according to chromosomal location, with the log10 P values corrected with the use of genomic control.
SNPs, single nucleotide polymorphism; MHC, major histocompatibility complex; TRAF1, TNF signal transduction gene; C5, complement 5 gene.
6
Log 1
0 P V
alue
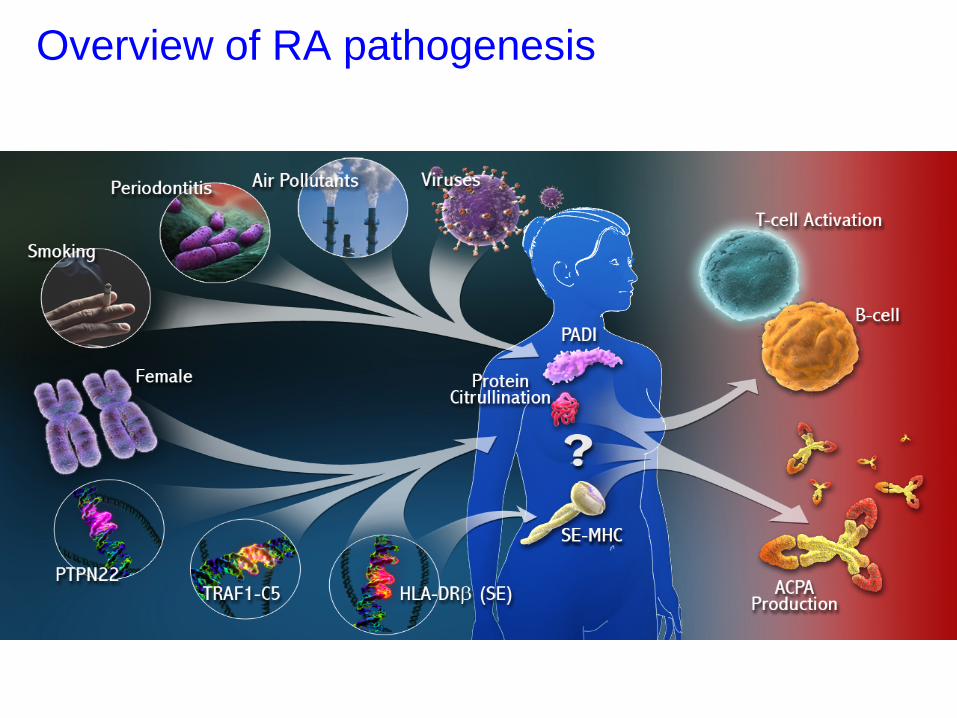
Overview of RA pathogenesis
7

Rheumatoid Arthritis: Hypothesis for Stages of Disease
Healthy
Pre-Clinical Phase
Autoimmune Early Synovitis
- Arthritis - Radiographic Changes
OVERT Rheumatoid Arthritis
- HLA-DRB1 (shared epitope)* - GWAS (PTPN22, others)
Genetics
- Smoking - Hormones - Bacteria* - Diet ?
Environmental Factors
Epitope Spreading + Titer Elevation
ACPA RF
Cytokines
Klareskog and others Courtesy of J. Scher Expanding repertoire of autoreactive lymphocytes

What is our interim progress in wiping the slate clean immune systems of patients with autoimmune disease?
Tabula rasa ? T cell
Plasma cell
B cell

Diverse approaches to eliminate B cells
Atacicept (TACI-Ig)
Rituximab (anti-CD20)
Belimumab/Tabalumab ( BAFF/BLyS)
Neutralizes both BAFF/BLyS and APRIL
CD19-1 (broadly reactive)
Autoreactive B cells
SLE RA
Other diseases
Stem Cell
Mature B cell
Transitional B cell
Pro/Pre B Cell
Immature B cell
Antigen stimulation
Memory Cell Antibody-producing plasma cells

B cell subsets in the blood
Jacobi, et al. Arthritis Rheum. 2010;62:201-10.
Unswitched memory Plasma cells plasmablasts Switched
memory
IgD+ IgD+CD10+ IgD- CD38++
CD27- naïve transitional/pre-naïve double negative, incl. CD27-memory
CD27+ pre-switched memory post-switched
memory
CD27++ plasma cells plasmablasts

CD27+ Memory B Cells
B C
ells
Time (months) RTX RTX
B cell depletion
B cell depletion
baseline regen- eration
1-2 3-4 5-6 regen- eration
1-2 3-4 5-6 0
25
20
15
10
5 A A A
A
Roll, et al. Arthritis Rheum. 2008;58:1566-75.
Clinical efficacy and B-cell regeneration in RA after Rituximab (RTX) treatment
A: P < 0.001 vs baseline. RTX approved for TNF IR RA

Naive B Cells
Perc
enta
ge
Time (months) RTX RTX
0 10 20 30 40 50 60 70 80 90
B cell depletion
B cell depletion
A
C
baseline regen- eration
1-2 3-4 5-6 regen- eration
1-2 3-4 5-6
B
A: P <.001 vs baseline; B: P <.05 vs baseline; C: P <.05 vs mos 5-6 after the first treatment.
Roll, et al. Arthritis Rheum. 2008;58:1566-75.
Clinical efficacy and B cell regeneration pattern in RA after RTX treatment

Synovial inflammation requires trafficking in the circulation between compartments
Silverman. Arthritis Rheum. 2006;54:2356-67.
TNF-α
Macrophage
Dendritic Cell
IFN-α
BAFF APRIL
TNF-α
Dendritic Cell
B Cells
B Cell T Cell TNF-α
IL-1
IFNγ
IL-1 TNF-α
IFNγ
IL-1 TNF-α IFNγ IL-1
Neutrophil
IL-1
B Cell
T Cell
Neutrophil
Synoviocytes
Bone marrow
Blood vessel
RTX: Accepted clinical paradigm for B cell-targeted therapy in RA
•Efficacy with safety •Associated with reduced circulating CD27+ memory B cells and increased naïve B cells
•Lower activated blood B cells •Lower activated blood T cells •Little or no effects on protective IgG antibodies
•Are these lessons to judge other agents?

16 Journal of Rheumatology 2014; 41; 824-828 FDA approved in RA

Anti-IL6R treatment causes decreases in switched and unswitched memory B cells
Roll, et al. Arthritis Rheum. 2011;63(5):1255-64.
In vivo effects of anti–Interleukin-6 Receptor inhibitor Tocilizumab at the B-cell level
Toculizumab approved in RA MTX IR
Overall memory B cells

Roll, et al. Arthritis Rheum. 2011;63(5):1255-64.
In vivo effects of anti–Interleukin-6 Receptor inhibitor Tocilizumab at the B-cell level
•Selective IL-6 blockade has focused and dramatic effects on B memory cells
•No significant effects on IgG levels, which is good for immune safety.
Tociluzimab Summary

Anti-TNF therapy in RA lowers levels of blood Memory B lymphocytes
• RA patients (n=45) on MTX (n=17), anti-TNF etanercept (n=11), or MTX/anti-TNF (n =17). Normal controls (n=22).
• Examined Peripheral Blood B cells by flow and cells from tonsillar biopsies.
• Etanercept increased peripheral blood naïve and transitional B cells while decreasing memory (both switched and unswitched).
• Immunohistochemistry of tonsil tissue revealed a decrease in follicular dendritic cell networks and germinal centers in etanercept treated populations
Anolik, et al. J Immunol. 2008;180(2):688-92.
*
Several TNFi approved for MTX IR RA

•RA may be associated with defects in B cell tolerance •Blockade of TNF mediated inflammation in RA can normalize some B cell associated defects of the cellular memory compartments
•TNF blockade can increase the proportion of transitional B cells and naïve B cells
•Can TNF blockade the frequency of anti-citrullinated self antigen memory B cells?
TNF Blockade Summary

In depth characterization of the anti-citrulline circulating B cells in RA patients
• Manuscript in preparation
22

Theoretical Pathway for Breaking Tolerance in RA
RF B cell Autoreactive
T Cells More
Autoreactive T Cells
Anti-citrulline B Cell
Citrullinated antigens
RF and anti-CCP antibodies lead to immune complexes, macrophage secretion of proinflammatory cytokines
Arginine-containing antigens
Anti-citrulline Plasma cell
PADI
Anti-CCP B cells capture any citrullinated protein, giving rise to expanded T-cell responses against self-antigens
T Cell
IgG anti-citrulline immune complexes are antigens for RF B cells
Adapted from: Niewold TB, et al. QJM. 2007;100(4):193-201.
24

IgG Anti-citrullinated Protein Antibodies (ACPAs)
•Production closely linked to SE-HLA Class II1
•~80-90% of ACPA-positive patients express SE2,3 •Multiple autoantibodies to multiple cit*-proteins
•fibrinogen, α-enolase, vimentin, others
•Moderately sensitive and highly specific for RA:
•45-80% and 96-100%, respectively4
•Rare in healthy individuals and in other conditions4
1. Källberg H et al. Am J Hum Genet. 2007;80:867–875. 2. Farragher TM et al. Arth Rheum. 2008;58(2):359-369. 3. Irigoyen P et al. Arth Rheum. 2005; 52(12):3813-3818. 4. Schellekens GA et al. Arthritis Rheum. 2000;43(1):155–163.
*cit=citrullinated

Citrullinated epitope IgG reactivity in CCP3-seropositive RA patients treated with TNF inhibitor + Methotrexate show similar epitope-specific ACPA patterns to patients treated with Methotrexate alone.
CCP3+ MTX
(n = 20)
CCP3+ TNFi/M
TX (n = 20)
CCP3-neg MTX
(n = 10)
Cit
hum
an
Fibr
inog
en
CC
P3
CitF
ilagg
rin c
fc-6
Cit
FibA
616
-35
Cit
FibB
36-
52
Cit
FibA
36-
50
Cit
Enol
ase
5-21
Cit
Vim
entin
59-
78
Cit
Vim
entin
419
-445
PC-B
SA
Teta
nus
Toxo
id
Anti-
hum
an Ig
G
BSA
(-)
Diverse serum IgG-ACPA in RA serum
A range of Cit-specific self antigens

Enumeration of ACPA IgG-secreting B cells in seropositive RA patient PBMC stimulated with CpG2006/IL-21/sCD40L.
RA CCP3Sero+ CCP3
RA CCP3Sero+ CQP3
Healthy CCP3
Healthy CQP3
CCP3 ASC/106P
BMC
CQP3 ASC/106P
BMC
Tetanus Toxoid
ASC/106PBMC
Total IgG ASC/106P
BMC
Spontaneous IgG
ASC/106PBMC
AVG RA CCP3sero+ (no biologic drug) (n=16) 41.3 +/- 0.5 1.9 +/- 0.6 71.1 +/- 2.6 30808.3 200.0 (n=15)
AVG RA CCP3sero+ (on biologic drug) (n=3) 12.5 +/- 0.8 0.8 +/- 1.2 52.5 +/-1.2 49166.7 320.8 (n=3)
AVG HC & RA seroneg (n=6) 2.8 +/- 3.0 3.2 +/- 2.7 65.4 +/- 1.2 42856.4 206.0 (n=5)

Healthy Rheumatoid Arthritis
Figure 4. Following whole PBMC stimulation, ACPA IgG-secreting B cells’ presence is restricted to CCP3-seropositive RA patients, while anti-Tetanus Toxoid secreting B cells are present in both healthy controls and RA patients.

B cell sorting and stimulation strategy to enumerate ACP secreting memory B cells
CD
27-A
PC
IgD-FITC
Stain PBMC on ice 30 min w/ FACS antibodies on ice, wash, perform sorting
CD40L cells
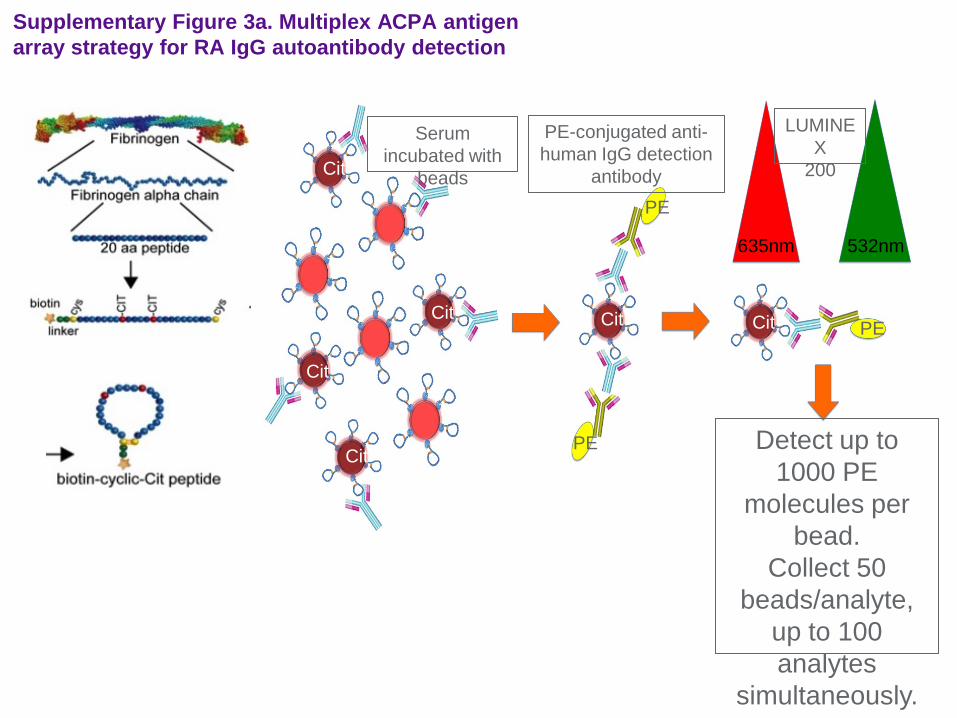
Supplementary Figure 3a. Multiplex ACPA antigen array strategy for RA IgG autoantibody detection
LUMINEX
200 Cit
Cit
Cit
Cit Cit Cit
PE
PE
PE
Serum incubated with
beads
PE-conjugated anti-human IgG detection
antibody
635nm 532nm
Detect up to 1000 PE
molecules per bead.
Collect 50 beads/analyte,
up to 100 analytes
simultaneously.

Upon stimulation, memory B cells in whole PBMC cultures sorted memory ACPA IgG with reactivity patterns that reiterate ACPA patterns in serum.
Serum IgG Induced memory IgG
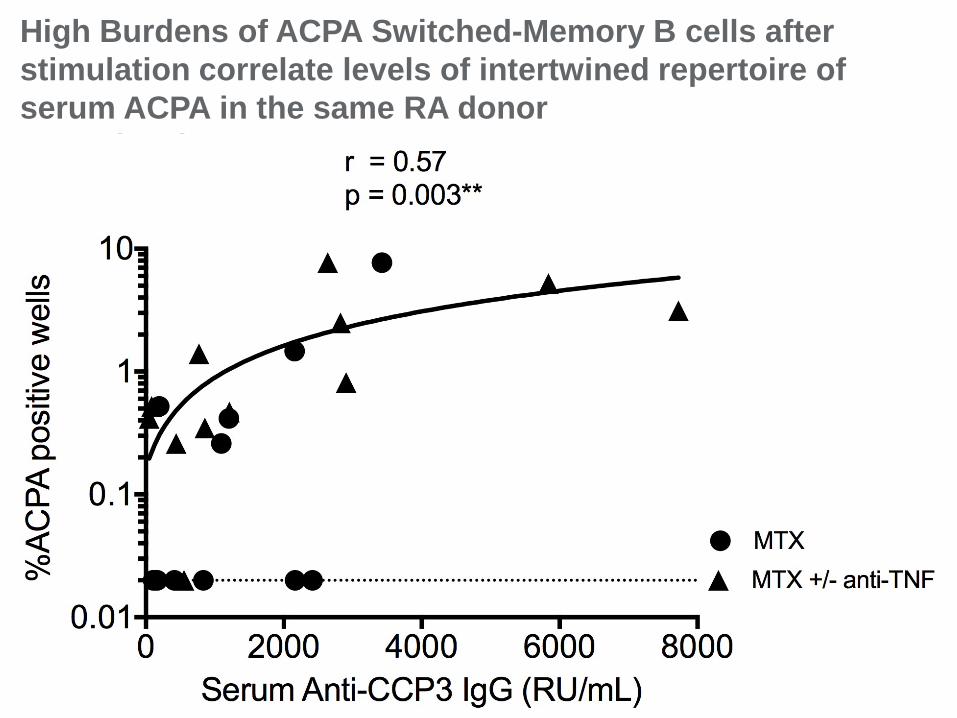
High Burdens of ACPA Switched-Memory B cells after stimulation correlate levels of intertwined repertoire of serum ACPA in the same RA donor ACPA levels.

High Burdens of blood ACPA Switched-Memory B cells are not uniformly abolished by treatment induced clinical remission, (or low disease activity). Levels of B cell memory do not correlate significantly with DAS28 Scores.
Our most commonly used therapies for RA do not eliminate the disease-associated memory B cell autoimmunity in the bloodstream
35
Conclusion

Targeting the BLyS/BAFF pathway: Atacicept and Belimumab/Tabalumab
BLyS APRIL
BAFF-R/BR3 TACI BCMA
Anti-BLyS TACI-Ig
• Atacicept: recomb fusion protein of the TACI* receptor and human IgG (not FDA approved)
• Belimumab: human monoclonal antibody which binds BLyS (approved in SLE only)
• *TACI: transmembrane activator and calcium modulator and cyclophilin-ligand interactor receptor Scapini, et al. Immunol Lett. 2008;116:1-6.
Ramanujam & Davidson. Arth Res Therapy. 2004;6:197-202.
Proteoglycan (syndecan-1)

Effects on blood B cell subsets Belimumab Phase II SLE trial
Wallace, et al Arthritis Rheum. 2009; 61(9): 1168–78.
Total B cells
Naive B cells
Activated B cells
Memory (CD27+) B cells
Decreases mature and plasma B cells but spares memory B cells and B-cell progenitors

Belimumab in RA: no significant clinical benefits in RA
•Human antibody to soluble BLyS
•Phase II, multicenter, double-blind, placebo- controlled, dose-ranging study in 283 patients with active moderate-to-severe RA 11 yr of disease DMARD IR 38% failed at least one TNF blocker significant but weak ACR20 response.
Cohen. J Rheumatol Suppl. 2006;77:12-7.
Atacicept – no benefit in RA Tabalumab-no benefit in RA
BAFF blockade may not have depleting effects on B cell memory
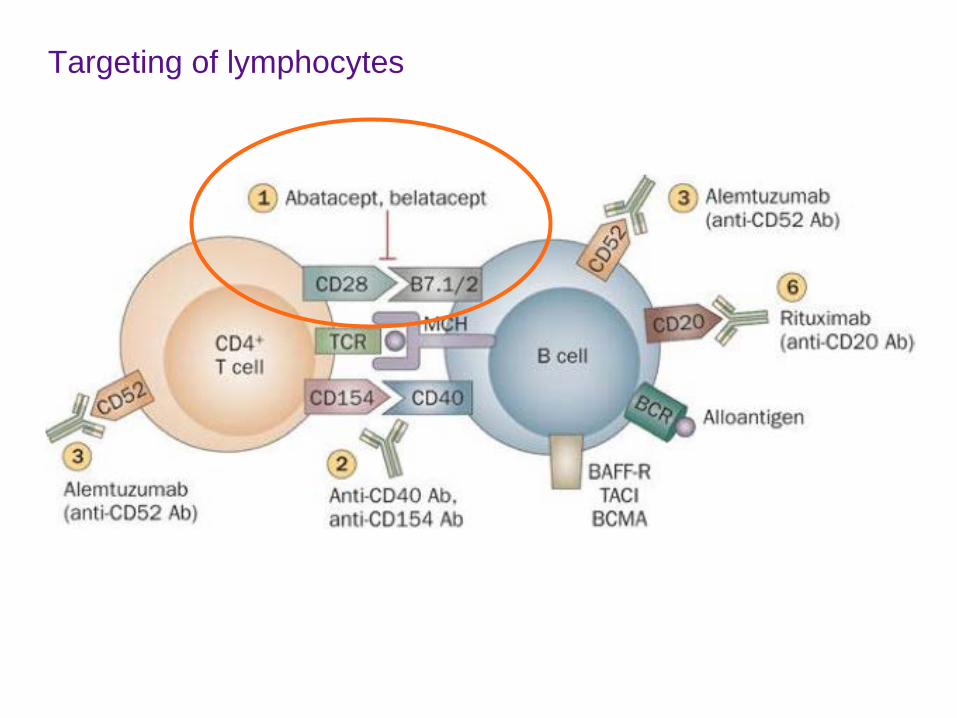
Targeting of lymphocytes

Abatacept in RA • ABA blocks T-cell co-stimulation, competing with CD28 for binding to CD80/CD86 signal required for full T-cell activation
• Open trial Bx/ reBx AB in RA pts (n=16) who failed TNFi
• 60% DAS28 responders after 4 months treatment.
• 15 pts with pre and 16 wk post bx
• Results: Small reduction in synovial cellular content, significant reduced only for B cells (CD20+ cells)
• Is ABA a B cell targeted agent?
Buch, et al. Ann Rheum Dis. 2009;68(7):1220.
approved for MTX IR RA
* CD20 sublining

Abatacept reduces levels of switched memory B cells, autoantibodies, and Immunoglobulins in RA.
Studies of 30 RA patients before and after ABA After 6 months of treatment, significant reductions of serum IgG, IgA, and IgM, with normalization of initially abnormal values. Significant reduction of IgG- and IgA-ACPA, & IgM-, IgA-, and IgG-RF Proportion of post-switch memory B cells significantly decreased.
Scarsi et al. J Rheumatol. 2014

CCP, cyclic citrullinated peptide; FLS, fibroblast-like synoviocyte; IFN, interferon; MMP, matrix metalloproteinase; RANKL, receptor activator of NF-κB ligand; RF, rheumatoid factor.
Osteoclast
TNF-α, IL-1, IL-6
T cell Plasma cell
Mφ Immune complexes Complement fixation Induce Mφ secretion of proinflammatory cytokines
B cell
RF, anti-CCP antibodies
TNF-α IL-1 IL-6
TNF-α IFN-γ IL-17 RANKL
FLS
MMPs Cathepsins
MMPs Cathepsins
Responsible for marginal erosions and bone loss
IL-1, IL-6, TNF-α IFN-γ
Abatacept (CTLA4-Ig)- blocks T Cell co-stimulation
APC (DC or Mφ)
Silverman & Boyle. Immunol Rev. 2008;223:175-85.

Window of Opportunity
• Clinical trials suggest that therapy initiated during (early) window of opportunity is more likely to lead to a sustained improvement.
• Based on limited current data, biologicals may increase the likelihood of persistent remission.
• Current data suggest medication-free remission is only ~3.6 to 22%. • Possible roles of disease duration, environment, and genetics should be investigated. • Reliable biomarkers (or imaging technology) are needed.
Nagy G, van Vollenhoven RF. Arthritis Res Ther. 2015;17:181.
Pre-disease Window of opportunity Progressive disease Time
Path
ogen
esis
Initiation of therapy
• Potential pathogenetic factors are present in many individuals (anti-CCP, RF)
Initiation of therapy
• Increased production of proinflammatory cytokines
• Synovitis • Osteoclast differentiation,
development of erosions Acce
lera
tion
due
to a
utoi
mm
unity
(fu
rther
loss
of t
oler
ance
) Initiation of therapy
• Lasting cytokine imbalance
• Synovial proliferation, chronic inflammation
• Structural damage Perm
anen
t au
toim
mun
ity
We need to understand the conditions that will re-establish tolerance during remission.

Concluding speculations •Diverse biologic agents that provide clinical benefits in RA can cause shifts but not normalize the memory B cell compartment.
•Common approaches suppress inflammation do not substantial the autoimmune state.
•This explains why halting therapy often leads to flare/recurrence.
•Drug-free “cure” of RA may require normalization of adaptive immune responses, with shift in B-cell subsets deletion of pathogenic autoimmune lymphocyte clones and long-lived plasma cells .
44

What is in the future?
•Combination therapies target B cells, T cells and plasma cells?
•Active induction of immune tolerance ? Cell based therapy (including stem cell infusions)
Apoptotic cell infusions for DC bias, i.e., extracorporeal photopheresis
Targeting immune checkpoints (e.g. PD-1)
45

etaphor for effective targeted therapy
1. Rheumatoid synovitis takes on an orderly structure with coordinated activities of cells and cytokines that drive pathogenesis
2. Not every cell type and soluble inflammatory factor is essential !
3. Targeted therapy may directly remove only one cell or cytokine from the process But this may cause disintegration of synovitis
Revised Metaphor circa 2015
B cells B cell Targeted Therapy
T cells
IL-6
TNFa
CD28
Osteoclasts Macrophages
Activated FLS
Com
plex
syn
oviti
s
Gregg Silverman, all Jenga rights reserved

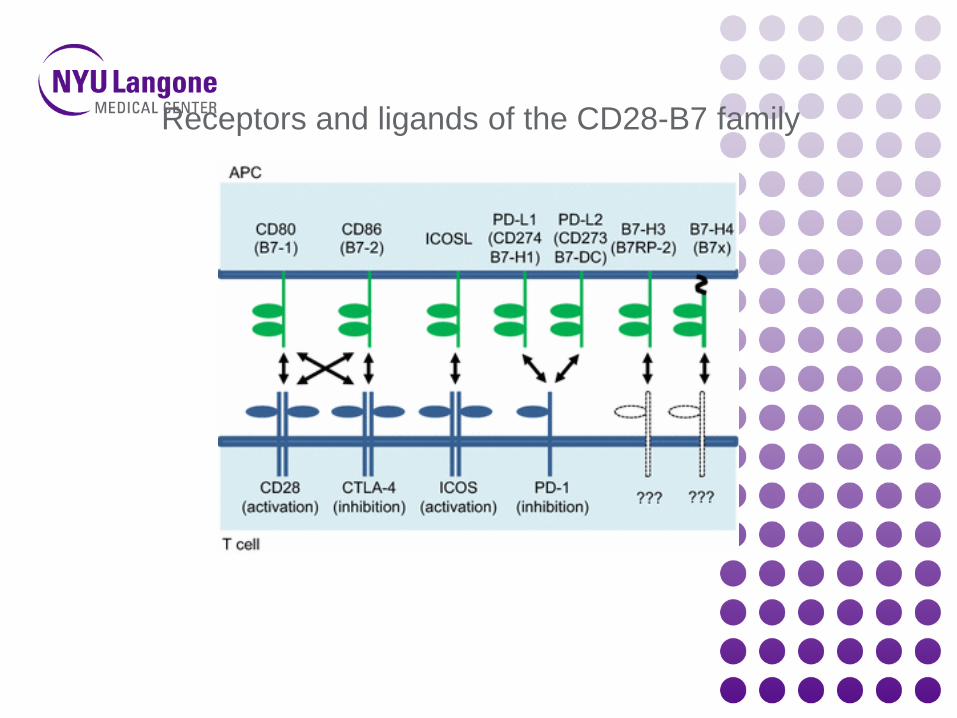
Receptors and ligands of the CD28-B7 family

Fig. 3 A molecular model for Programmed Death (PD)-1-mediated in
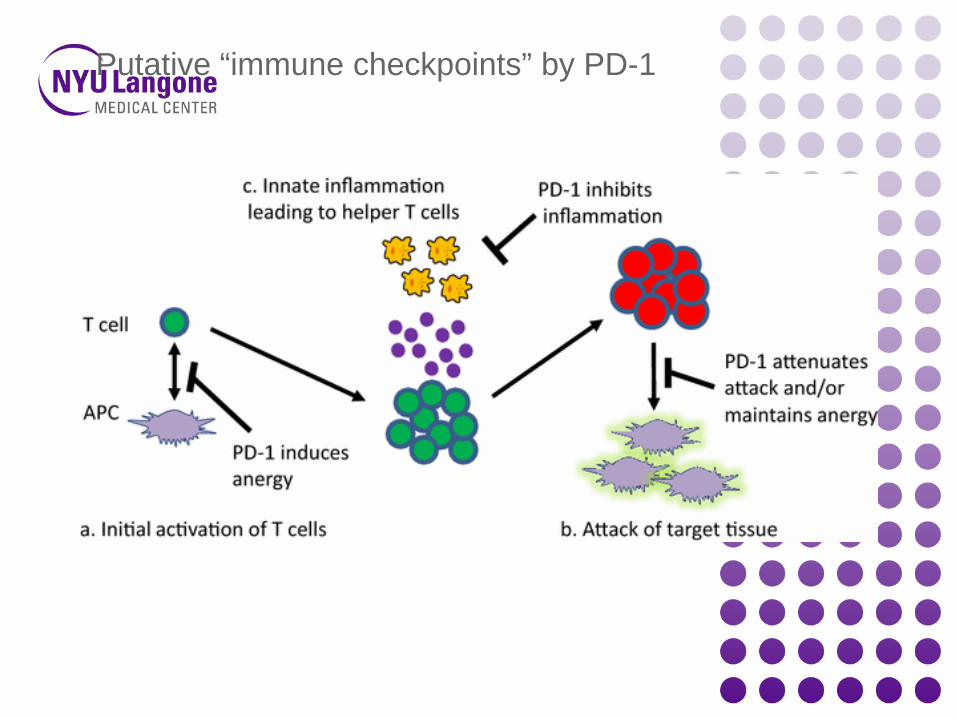
Putative “immune checkpoints” by PD-1