Imagistic and histopathologic concordances in … · in degenerative lesions of intervertebral...
6
Rom J Morphol Embryol 2011, 52(1 Suppl):327–332 ORIGINAL PAPER Imagistic and histopathologic concordances in degenerative lesions of intervertebral disks MARIANA CEVEI 1) , ELENA ROŞCA 2) , L. LIVIU 1) , GABRIELA MUŢIU 3) , DORINA STOICĂNESCU 4) , LILIANA VASILE 5) 1) Department of Rehabilitation 2) Department of Pathology 3) Department of Histology Faculty of Medicine and Pharmacy, University of Oradea 4) Department of Medical Genetics 5) Department of Histology “Victor Babeş” University of Medicine and Pharmacy, Timisoara Abstract Lumbar disk lesions in 47 cases were initially diagnosed using MRI investigation, then, after surgery, biological and histopathological aspects of intervertebral disks were revealed. Pieces from intervertebral disks were used for electron microscopy studies in order to determine collagen in the components of the intervertebral disk. The aim of the present study was to highlight the correspondence between the MRI aspect in cases with clinically manifest lumbar hernia, staged according to MRI Modic classification, and the histopathological aspect in patients with surgical interventions on the intervertebral disks. 4/5 of the analyzed disks had advanced forms of degenerescence of the intervertebral disks: hyalinized disk cartilage ± intradiskal calcification or ossification zones, chronic inflammatory infiltrate at the disk cartilage level. Electron microscopy studies made on disk fragments obtained by discectomy revealed quantitative and qualitative changes of all types of collagen at the level of the three anatomical structures of the intervertebral disks, which correspond to the MRI changes. Keywords: intervertebral disk, magnetic resonance imaging, histopathology. Introduction The development of molecular biology facilitated a better understanding of the processes that lead to the degenerative disease of intervertebral disks. Numerous studies aiming to identify the causes and risk factors for this degenerative disorder have been performed [1]. It is now known that degenerative disk disorder is strongly linked to genetic factors, recent research indicating that heredity has a dominant role in disk degeneration and explains about 74% of the variance in adult populations. Studies regarding genetic influences are performed since 1998 and many genes associated with disk degeneration have been confirmed, such as the genes that code for collagen I, collagen IX (COL9A2 and COL9A3), collagen XI (COL11A2), IL-1, IL-6, aggrecan, vitamin D receptor, MMP-3, VDR and CILP. For some of these, gene-gene, gene-environment or gene-age interactions may exist [2]. Recent advances have led to further understanding of the complexity of disk degenerative disease and allowed development of new treatments, targeting the biochemical pathways involved in the degenerative cascade. Gene therapy has also shown much promise as a powerful tool in the treatment of intervertebral disk degeneration. Other new targets for gene therapy have also been identified, such as TGF-beta1, TIMP-1, and LMP-1 [3]. Some studies revealed that occupational factors, such as whole-body vibration, have an additive effect to genetic risk factors increasing the likelihood of having the disorder. Of the independent genetic markers, IL1A–889T allele had the strongest association with intervertebral disk disease [4]. Additional studies, including linkage analyses and whole genome scanning in different populations and whole range of ages will improve understanding the influence of genes on disk degeneration [2]. Activity restriction in cases with lumbar disk hernia represents a solid argument that pleads for deepening studies regarding the biology of the intervertebral disk, leading to early diagnosis and effective treatment according to biological staging correlated to the stage of the disorder, which is offered by magnetic resonance imaging (MRI) investigation [5]. Classifications of lumbar spine degeneration by imaging methods were first provided by Modic MT [6]. In that study, Modic MT followed up, using magnetic resonance, the evolution of patients submitted to treatment for disk conditions with chemopapain, classifying these changes as grade I, II or III. Type I MRI changes consist of vertebral bodies parallel with the vertebral plateau of degenerated disk that shows hyposignal on ponderate images in T1 and hyperintensity in T2. There is no radiological correspondent. R J M E Romanian Journal of Morphology & Embryology http://www.rjme.ro/
Transcript of Imagistic and histopathologic concordances in … · in degenerative lesions of intervertebral...

Rom J Morphol Embryol 2011, 52(1 Suppl):327–332
OORRIIGGIINNAALL PPAAPPEERR
Imagistic and histopathologic concordances in degenerative lesions of intervertebral
disks MARIANA CEVEI1), ELENA ROŞCA2), L. LIVIU1), GABRIELA MUŢIU3),
DORINA STOICĂNESCU4), LILIANA VASILE5)
1)Department of Rehabilitation 2)Department of Pathology 3)Department of Histology
Faculty of Medicine and Pharmacy, University of Oradea 4)Department of Medical Genetics
5)Department of Histology “Victor Babeş” University of Medicine and Pharmacy, Timisoara
Abstract Lumbar disk lesions in 47 cases were initially diagnosed using MRI investigation, then, after surgery, biological and histopathological aspects of intervertebral disks were revealed. Pieces from intervertebral disks were used for electron microscopy studies in order to determine collagen in the components of the intervertebral disk. The aim of the present study was to highlight the correspondence between the MRI aspect in cases with clinically manifest lumbar hernia, staged according to MRI Modic classification, and the histopathological aspect in patients with surgical interventions on the intervertebral disks. 4/5 of the analyzed disks had advanced forms of degenerescence of the intervertebral disks: hyalinized disk cartilage ± intradiskal calcification or ossification zones, chronic inflammatory infiltrate at the disk cartilage level. Electron microscopy studies made on disk fragments obtained by discectomy revealed quantitative and qualitative changes of all types of collagen at the level of the three anatomical structures of the intervertebral disks, which correspond to the MRI changes. Keywords: intervertebral disk, magnetic resonance imaging, histopathology.
Introduction
The development of molecular biology facilitated a better understanding of the processes that lead to the degenerative disease of intervertebral disks. Numerous studies aiming to identify the causes and risk factors for this degenerative disorder have been performed [1]. It is now known that degenerative disk disorder is strongly linked to genetic factors, recent research indicating that heredity has a dominant role in disk degeneration and explains about 74% of the variance in adult populations. Studies regarding genetic influences are performed since 1998 and many genes associated with disk degeneration have been confirmed, such as the genes that code for collagen I, collagen IX (COL9A2 and COL9A3), collagen XI (COL11A2), IL-1, IL-6, aggrecan, vitamin D receptor, MMP-3, VDR and CILP. For some of these, gene-gene, gene-environment or gene-age interactions may exist [2]. Recent advances have led to further understanding of the complexity of disk degenerative disease and allowed development of new treatments, targeting the biochemical pathways involved in the degenerative cascade. Gene therapy has also shown much promise as a powerful tool in the treatment of intervertebral disk degeneration. Other new targets for gene therapy have also been identified, such as TGF-beta1, TIMP-1, and LMP-1 [3]. Some studies
revealed that occupational factors, such as whole-body vibration, have an additive effect to genetic risk factors increasing the likelihood of having the disorder. Of the independent genetic markers, IL1A–889T allele had the strongest association with intervertebral disk disease [4]. Additional studies, including linkage analyses and whole genome scanning in different populations and whole range of ages will improve understanding the influence of genes on disk degeneration [2].
Activity restriction in cases with lumbar disk hernia represents a solid argument that pleads for deepening studies regarding the biology of the intervertebral disk, leading to early diagnosis and effective treatment according to biological staging correlated to the stage of the disorder, which is offered by magnetic resonance imaging (MRI) investigation [5]. Classifications of lumbar spine degeneration by imaging methods were first provided by Modic MT [6]. In that study, Modic MT followed up, using magnetic resonance, the evolution of patients submitted to treatment for disk conditions with chemopapain, classifying these changes as grade I, II or III. Type I MRI changes consist of vertebral bodies parallel with the vertebral plateau of degenerated disk that shows hyposignal on ponderate images in T1 and hyperintensity in T2. There is no radiological correspondent.
R J M ERomanian Journal of
Morphology & Embryologyhttp://www.rjme.ro/

Mariana Cevei et al.
328
Type II MRI changes consist of increased intensity of the signal on ponderate images in T1 and an iso-intense signal or slightly hyperintense in T2 images and represent the imagistic expression of disk lesions consisting of annular protrusion and relatively recent incipient disk hernia. They do not have a radiological correspondent.
MRI investigations revealing type III changes, show decreasing intensity of the signal on ponderate images both in T1 and T2, being correlated on usual planar radiographic images with extensive bone sclerosis. They are associated with disk hernia, disk extrusion, free disk fragment, lesions of the posterior vertebral ligament [7].
From the biological point of view, the intervertebral disk is characterized by the presence of collagen (its quantity increases with age), water, condroitin sulphates in complexes of non-fibrillar proteins, hyaluronic acid and keratosulphates [8]. Disk composition changes during development, growth, ageing and degeneration and this influences the response of the disk to changes in mechanical stress [9, 10].
The aim of the present study was to highlight the correspondence between the aspect of MRI in cases with clinically manifest lumbar hernia, staged according to MRI Modic classification, and the histopathological aspect in patients with surgical interventions on the intervertebral disks.
Materials and Methods
The study was performed on a group of 47 cases with discectomy for lumbar disk hernia, selected from the patients admitted in the Medical Rehabilitation Clinical Hospital Băile Felix, with the diagnosis of low back pain accompanied or not by radiculopathy due to lumbar hernia, between January 2008 and September 2008. All the patients were investigated by MRI before surgery. We used MRI Modic classification, which categorizes disk lesions in three classes, according to their severity. Forty-seven intervertebral disks were taken from patients operated in the Neurosurgery Department of Oradea Clinical County Hospital.
Lumbar disk lesions were initially diagnosed using MRI investigation, then, after surgery, biological and histopathological aspects of the intervertebral disks were revealed. Fragments from intervertebral disks were used for electron microscopy studies in order to determine collagen in the components of the inter-vertebral disk. They were studied using both transmission electron microscopy and scanning electron microscopy, but fragments from the 47 disks were also examined by column and paper adsorption chroma-tography methods. Electron microscopy studies aimed to analyze the collagen types from intervertebral disks obtained by discectomy. These assessments were performed in order to reveal quantitative or qualitative changes of six types of collagen (I, II, III, V, VI, IX) in nucleus pulposus, annulus fibrosus and cartilaginous end-plates from the intervertebral disk. For the histo-pathological examination, specimens were paraffin-embedded and stained with Hematoxylin–Eosin. Photos of the slides were made with Polaroid XIO type. Different types of collagen were determined using
electron microscopy studies, by measuring distinct chains and total mass of collagen fiber chains.
Results
Patients’ age varied between 22 and 54 years, with a mean of 48.8 years. Distribution of genders was: 31 males (65%) with a mean age of 45.3 years and 16 females (35%), with a mean age of 39.6 years.
Localization of disk hernia established by MRI investigation revealed: L3 level – two cases (4.3%), L4 level – 30 cases (63%), L5 level – 15 cases (32.6%).
Type I MRI Modic changes were found in four (8.5%) samples, type II changes were identified in five (10.63%) samples and type III MRI Modic changes in 38 (80.8%) samples.
Intervertebral disk degeneration is revealed by chondrocyte lesions in the fibrous cartilage: various stages of altered nuclear structure, cytoplasmic vacuola-tion. Cells disappear from lacunae. Intercellular cartila-genous matrix, depending upon cell alterations, suffers degradation processes: loss of tinctoriality, fiber lysis, calcification. The cartilaginous channel contains connective tissue with many neoformation vessels, hemorrhagic suffusions and rich PMN infiltration, lympho-monocytes and macrophages. Chondrocytes show alterations of the nucleus (pyknosis) and of the cytoplasm (vacuolization). The matrix is eosinophilic, poor in fibers. Some chondrocytes are deeply altered and disappeared from lacunae.
Histopathological changes noticed in the early forms of degenerescence of the intervertebral disk have been identified in five samples (10.63%) (Figure 1):
▪ myxoid degenerescence of the disk cartilage, with chondroblasts and chondrocytes;
▪ hyalinisation and areas of interfibrillar edema on the fibrous disk tissue.
Figure 1 – Fibrous cartilage (territorial matrix), inter-territorial with fibrous aspect and small isogenic groups or isolated chondrocytes (AA–PAS, ×40).
Histopathological changes – second phase of dege-neration – moderate forms of degenerescence of the intervertebral disk (Figure 2), identified in 13 (27.65%) cases were:
▪ cartilaginous tissue with chondrocytes in lacunae, papillary aspect and hemorrhagic areas;
▪ chondroblasts and chondrocytes associated with areas of myxoid degenerescence.

Imagistic and histopathologic concordances in degenerative lesions of intervertebral disks
329
Figure 2 – Cartilaginous matrix with isolated or degenerated chondrocytes disappeared from lacunae, fibrillar disorganization, although maintained in oblique plans to each other. Matrix territories retain metachromasy of the fibers at AT pH 5 (×40).
Histopathological changes – type III, in advanced forms of degenerescence of the intervertebral disk, (Figure 3), seen in 29 cases (57.44%), were:
▪ myxoid degenerescence and intradiskal calcifica-tions;
▪ hyalinized disk cartilage with intradiskal calcifica-tion areas and the presence of young cells – fibroblasts and chondroblasts;
▪ cartilaginous tissue with areas of fibrosis and chronic inflammatory infiltrate.
Figure 3 – Fibrous cartilage with multiple fissures, with extensive areas of dystrophic calcification and disappearance of the chondrocytes from lacunae (HE stain, ×40).
Column and paper-adsorption chromatography analysis together with electron microscopy examination of the 47 fragments of intervertebral disks revealed quantitative and qualitative changes of the three anato-mical structures. Data obtained were corroborated with the results of the MRI investigation.
Electron microscopy studies performed on inter-vertebral disk fragments obtained by discectomy revealed qualitative and quantitative changes of all types of collagen in all three anatomical structures of intervertebral disks, which correspond to MRI changes.
The dominant morphological characteristic of the injured chondrocyte from the degenerated intervertebral disk in electron microscopy is the presence of numerous complex lipid vacuoles of unequal sizes, all over the cytoplasm, with a tendency to unification. In many degenerated chondrocytes the autophagic phenomenon includes large cytoplasmic territories or the aspect of residual bodies (autophagosomes) with abundant undigested granular material. On the surface of many chondrocytes there are mixed expansions like microvilli or long digitiforme ones as micro-folds in contact with a
reduced intercellular matrix. The sub-plasma membrane is seen in some chondrocytes as fine, granular electrono-dense material, representing either a secretion or endo-cytated product. Territorial cartilage matrix from hernia-ted intervertebral disk reveals in electron microscopy collagen fibers of unequal thickness, sectioned in various incidences and showing a disordered arrangement.
In six cases (12.76%) the following aspects of the intervertebral disk were encountered (Figure 4):
▪ absence/minimal increase of collagen I and II in nucleus pulposus;
▪ increase with a slight change of collagen I, II, III, IV in annulus fibrosus;
▪ absence of collagen I and presence of collagen II in the cartilaginous end-plates.
Figure 4 – Type I and II collagen fibers (TEM).
These cases correspond to the four patients (66.6%) with MRI changes type I and to two patients with MRI changes type II and also to the five cases (83%) with histopathological changes type I and one with type II.
In seven cases (14.89%), electron microscopy revealed the following aspects (Figure 5):
▪ increase of collagen III in nucleus pulposus; ▪ moderate presence of collagen V and increase of
collagen III in annulus fibrosus; ▪ presence of collagen III, V, VI in cartilaginous
end-plates.
Figure 5 – Fragment from intervertebral disk studied by scanning electron microscopy revealing type II changes.
Disk lesions of these cases corresponded to type II MRI changes in five cases (71.4%) and type II histo-pathological changes for all cases.
Mariana Cevei et al.
330
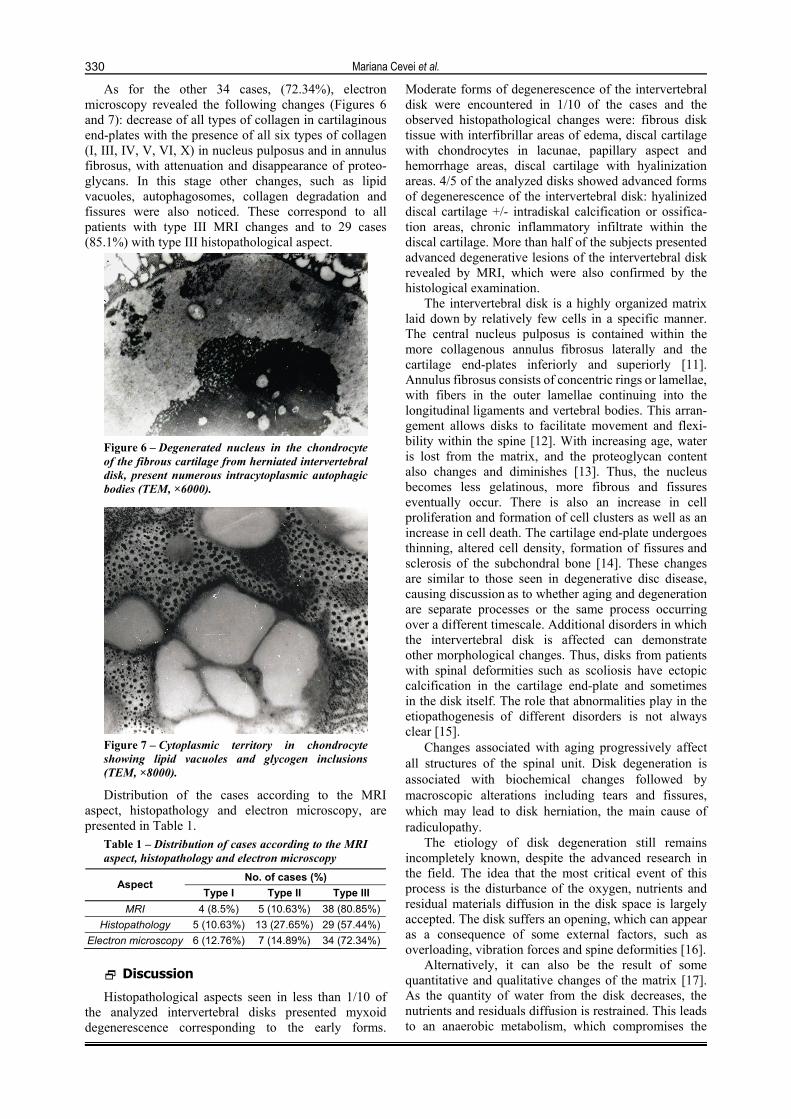
As for the other 34 cases, (72.34%), electron microscopy revealed the following changes (Figures 6 and 7): decrease of all types of collagen in cartilaginous end-plates with the presence of all six types of collagen (I, III, IV, V, VI, X) in nucleus pulposus and in annulus fibrosus, with attenuation and disappearance of proteo-glycans. In this stage other changes, such as lipid vacuoles, autophagosomes, collagen degradation and fissures were also noticed. These correspond to all patients with type III MRI changes and to 29 cases (85.1%) with type III histopathological aspect.
Figure 6 – Degenerated nucleus in the chondrocyte of the fibrous cartilage from herniated intervertebral disk, present numerous intracytoplasmic autophagic bodies (TEM, ×6000).
Figure 7 – Cytoplasmic territory in chondrocyte showing lipid vacuoles and glycogen inclusions (TEM, ×8000).
Distribution of the cases according to the MRI aspect, histopathology and electron microscopy, are presented in Table 1.
Table 1 – Distribution of cases according to the MRI aspect, histopathology and electron microscopy
No. of cases (%) Aspect Type I Type II Type III
MRI 4 (8.5%) 5 (10.63%) 38 (80.85%) Histopathology 5 (10.63%) 13 (27.65%) 29 (57.44%)
Electron microscopy 6 (12.76%) 7 (14.89%) 34 (72.34%)
Discussion
Histopathological aspects seen in less than 1/10 of the analyzed intervertebral disks presented myxoid degenerescence corresponding to the early forms.
Moderate forms of degenerescence of the intervertebral disk were encountered in 1/10 of the cases and the observed histopathological changes were: fibrous disk tissue with interfibrillar areas of edema, discal cartilage with chondrocytes in lacunae, papillary aspect and hemorrhage areas, discal cartilage with hyalinization areas. 4/5 of the analyzed disks showed advanced forms of degenerescence of the intervertebral disk: hyalinized discal cartilage +/- intradiskal calcification or ossifica-tion areas, chronic inflammatory infiltrate within the discal cartilage. More than half of the subjects presented advanced degenerative lesions of the intervertebral disk revealed by MRI, which were also confirmed by the histological examination.
The intervertebral disk is a highly organized matrix laid down by relatively few cells in a specific manner. The central nucleus pulposus is contained within the more collagenous annulus fibrosus laterally and the cartilage end-plates inferiorly and superiorly [11]. Annulus fibrosus consists of concentric rings or lamellae, with fibers in the outer lamellae continuing into the longitudinal ligaments and vertebral bodies. This arran-gement allows disks to facilitate movement and flexi-bility within the spine [12]. With increasing age, water is lost from the matrix, and the proteoglycan content also changes and diminishes [13]. Thus, the nucleus becomes less gelatinous, more fibrous and fissures eventually occur. There is also an increase in cell proliferation and formation of cell clusters as well as an increase in cell death. The cartilage end-plate undergoes thinning, altered cell density, formation of fissures and sclerosis of the subchondral bone [14]. These changes are similar to those seen in degenerative disc disease, causing discussion as to whether aging and degeneration are separate processes or the same process occurring over a different timescale. Additional disorders in which the intervertebral disk is affected can demonstrate other morphological changes. Thus, disks from patients with spinal deformities such as scoliosis have ectopic calcification in the cartilage end-plate and sometimes in the disk itself. The role that abnormalities play in the etiopathogenesis of different disorders is not always clear [15].
Changes associated with aging progressively affect all structures of the spinal unit. Disk degeneration is associated with biochemical changes followed by macroscopic alterations including tears and fissures, which may lead to disk herniation, the main cause of radiculopathy.
The etiology of disk degeneration still remains incompletely known, despite the advanced research in the field. The idea that the most critical event of this process is the disturbance of the oxygen, nutrients and residual materials diffusion in the disk space is largely accepted. The disk suffers an opening, which can appear as a consequence of some external factors, such as overloading, vibration forces and spine deformities [16].
Alternatively, it can also be the result of some quantitative and qualitative changes of the matrix [17]. As the quantity of water from the disk decreases, the nutrients and residuals diffusion is restrained. This leads to an anaerobic metabolism, which compromises the

Imagistic and histopathologic concordances in degenerative lesions of intervertebral disks
331
viability of the cell. Then the cellular density in the disk decreases and, consequently, the synthesis and mainte-nance of the matrix are affected. The synthesis of the matrix macromolecules decreases, which results in the diminishing of the quantity of water in the disk [18, 19].
The matrices differ significantly in their relative amounts of the structural macromolecules. Proteoglycan and water concentration decrease with aging [20]. Gruber HE and Hanley EN Jr [21] pioneered the study of apoptosis in disk degeneration in 1998. They quantified the incidence of apoptotic cell death in the annulus and compared its quantity between the tissues from the diseased subjects and normal control. Their findings revealed that there is a high incidence of apoptosis in the intervertebral disk. In their other study, they even reported that insulin-like growth factor-1 (IGF-1) and platelet-derived growth factor (PDGF) had anti-apoptotic effects on human intervertebral disk cells in vitro [22]. Since Gruber’s report, the estimated degree of apoptosis has been considered and reflected as a scale of disk degeneration by several authors [16].
The herniated disks are characterized by global decrease of mucopolysaccharides and increase of collagen in parallel with the clinical evolution of the case [18, 19]. The consistency of the changes found on the gross structure of the disc and on magnetic resonance is significant, implying the great reliability of the images found [23–25].
Electron microscopy studies revealed concordant results with magnetic resonance and histopathological images [26, 27]. As a result of the clinical, MRI, histo-pathological and biochemical data analysis of the 47 cases, we developed a clinical-imaging staging of the intervertebral disk lesions and a correspondent biological staging.
The imaging staging offered by the MRI had as a reference point the classification made by Modic (types I, II, III). Data from several studies, which aimed to follow-up Modic changes, revealed that these changes are dynamic markers of the normal age-related degenerative process of the lumbar spine, their prevalence increasing with age. In time, these lesions can convert from one type to another, mixed-type changes also being described, probably representing
intermediate stages during conversion. Type 1 changes seem to be inflammatory in origin and strongly
associated with active low back symptoms, reflecting a state of active degeneration and biomechanical instability of the lumbar spine. Type 2 changes are less clearly associated with low back pain, seemingly indicating a more biomechanically stable state. The exact nature and pathogenetic significance of type 3 changes still remain largely unknown [28–31].
Conclusions
A biological staging corresponds to the imaging staging of intervertebral disk lesions.
Electronic microscopy studies made on disk fragments obtained by discectomy revealed quantitative and qualitative changes of all types of collagen the three anatomical structures of intervertebral disk that correspond to the MRI changes.
The obtained concordances give us hope for an early diagnosis of disk hernias, by associating data obtained from cell biology of the intervertebral disk with the images provided by MRI.
These correlations are very important from the practical point of view, because the predictive values allow the approximation with a high degree of proba-bility of future results (“disease outcome”) in patients with lumbar disk hernia.
References [1] PATEL KP, SANDY JD, AKEDA K, MIYAMOTO K, CHUJO T,
AN HS, MASUDA K, Aggrecanases and aggrecanase-generated fragments in the human intervertebral disc at early and advanced stages of disc degeneration, Spine (Phil Pa 1976), 2007, 32(23):2596–2603.
[2] KALICHMAN L, HUNTER DJ, The genetics of intervertebral disc degeneration. Associated genes, Joint Bone Spine, 2008, 75(4):388–396.
[3] HUBERT MG, VADALA G, SOWA G, STUDER RK, KANG JD, Gene therapy for the treatment of degenerative disk disease, J Am Acad Orthop Surg, 2008, 16(6):312–319.
[4] VIRTANEN IM, KARPPINEN J, TAIMELA S, OTT J, BARRAL S, KAIKKONEN K, HEIKKILÄ O, MUTANEN P, NOPONEN N, MÄNNIKKÖ M, TERVONEN O, NATRI A, ALA-KOKKO L, Occupational and genetic risk factors associated with intervertebral disc disease, Spine (Phil Pa 1976), 2007, 32(10):1129–1134.
[5] FROST H, LAMB SE, DOLL HA, CARVER PT, STEWART- BROWN S, Randomised controlled trial of physiotherapy compared with advice for low back pain, BMJ, 2004, 329(7468):708.
[6] MODIC MT, Modic type 1 and type 2 changes, J Neurosurg Spine, 2007, 6(2):150–151; discussion 151.
[7] WICHMAN HJ, Discography: over 50 years of controversy, WMJ, 2007, 106(1):27–29.
[8] CZERVIONKE LF, HAUGHTON VM, Degenerative disease of the spine. In: ATLAS SW (ed), Magnetic resonance imaging of the brain and spine, Lippincott–Raven Publisher, Philadelphia, 2002, 1633–1714.
[9] LEE JH, CHUNG CK, KIM HJ, Disparity between MR imaging and histochemical grading in human intervertebral disc degeneration, J Korean Neurosurg Soc, 2006, 39(6):432–437.
[10] GRUBER HE, INGRAM JA, DAVIS DE, HANLEY EN, Increased cell senescence is associated with decreased cell prolife-ration in vivo in the degenerating human annulus, Spine J, 2009, 9(3):210–215.
[11] VERNON-ROBERTS B, MOORE RJ, FRASER RD, The natural history of age-related disc degeneration: the influence of age and pathology on cell populations in the L4–L5 disc, Spine (Phila Pa 1976), 2008, 33(25):2767–2773.
[12] VAN GOETHEM JWM, VAN DEN HAUWE L, PARIZEL PM, Degenerative disc disease. In: VAN GOETHEM JWM, VAN DEN HAUWE L, PARIZEL PM (eds), Spinal imaging, Springer-Verlag, Berlin–Heidelberg, 2007, 127–156.
[13] JINKINS JR, Acquired degenerative changes of the inter-vertebral segments at and suprajacent to the lumbosacral junction. A radioanatomic analysis of the nondiscal structures of the spinal column and perispinal soft tissues, Eur J Radiol, 2004, 50(2):134–158.
[14] HASSELBLATT M, MAINTZ D, GOLL T, WILDFÖRSTER U, SCHUL C, PAULUS W, Frequency of unexpected and important histopathological findings in routine intervertebral disc surgery, J Neurosurg Spine, 2006, 4(1):20–23.
[15] ROBERTS S, EVANS H, TRIVEDI J, MENAGE J, Histology and pathology of the human intervertebral disc, J Bone Joint Surg Am, 2006, 88(Suppl 2):10–14.
[16] PUERTAS EB, YAMASHITA H, DE OLIVEIRA VM, DE SOUZA PS, Classification of intervertebral disc degeneration by magnetic resonance, Acta Ortop Bras, 2009, 17(1):46–49.
[17] LEUNG VY, CHAN WC, HUNG SC, CHEUNG KM, CHAN D, Matrix remodeling during intervertebral disc growth and degeneration detected by multichromatic FAST staining, J Histochem Cytochem, 2009, 57(3):249–256.

Mariana Cevei et al.
332
[18] ROH JS, TENG AL, YOO JU, DAVIS J, FUREY C, BOHLMANN HH, Degenerative disorders of the lumbar and cervical spine, Orthop Clin North Am, 2005, 36(3):255–262.
[19] GALLUCCI M, PUGLIELLI E, SPLENDIANI A, PISTOIA F, SPACCA G, Degenerative disorders of the spine, Eur Radiol, 2005, 15(3):591–598.
[20] BENNEKER LM, HEINI PF, ANDERSON SE, ALINI M, ITO K, Correlation of radiographic and MRI parameters to morpho-logical and biochemical assessment of intervertebral disc degeneration, Eur Spine J, 2005, 14(1):27–35.
[21] GRUBER HE, HANLEY EN JR, Analysis of aging and degeneration of human intervertebral disc. Comparison of surgical specimens with normal controls, Spine (Phil Pa 1976), 1998, 23(7):751–757.
[22] GRUBER HE, HOELSCHER GL, INGRAM JA, BETHEA S, HANLEY EN, IGF-1 rescues human intervertebral annulus cells from in vitro stress-induced premature senescence, Growth Factors, 2008, 26(4):220–225.
[23] BEATTIE P, MEYERS SP, STRATFORD P, MILLARD RW, HOLLENBERG GM, Associations between patient report of symptoms and anatomic impairment visible on lumbar magnetic resonance imaging, Spine (Phil Pa 1976), 2000, 25(7):819–828.
[24] MITRA D, CASSAR-PULLICINO VN, MCCALL IW, Longitudinal study of vertebral type-1 end-plate changes on MR of the lumbar spine, Eur Radiol, 2004, 14(9):1574–1581.
[25] PANDE KC, KHURJEKAR K, KANIKDALEY V, Correlation of low back pain to a high-intensity zone of the lumbar disc in Indian patients, J Orthop Surg (Hong Kong), 2009, 17(2):190–193.
[26] WU AS, FOURNEY DR, Incidence of unusual and clinically significant histopathological findings in routine discectomy, J Neurosurg Spine, 2006, 5(5):410–413.
[27] CHRISTE A, LÄUBLI R, GUZMAN R, BERLEMANN U, MOORE RJ, SCHROTH G, VOCK P, LÖVBLAD KO, Degeneration of the cervical disc: histology compared with radiography and magnetic resonance imaging, Neuroradiology, 2005, 47(10):721–729.
[28] ESPOSITO P, PINHEIRO-FRANCO JL, FROELICH S, MAITROT D, Predictive value of MRI vertebral end-plate signal changes (Modic) on outcome of surgically treated degenerative disc disease. Results of a cohort study including 60 patients, Neurochirurgie, 2006, 52(4):315–322.
[29] KUISMA M, KARPPINEN J, NIINIMÄKI J, OJALA R, HAAPEA M, HELIÖVAARA M, KORPELAINEN R, TAIMELA S, NATRI A, TERVONEN O, Modic changes in endplates of lumbar vertebral bodies: prevalence and association with low back and sciatic pain among middle-aged male worker, Spine (Phil Pa 1976), 2007, 32(10):1116–1122.
[30] ALBERT HB, MANNICHE C, Modic changes following lumbar disc herniation, Eur Spine J, 2007, 16(7):977–982.
[31] RAHME R, MOUSSA R, The Modic vertebral endplate and marrow changes: pathologic significance and relation to low back pain and segmental instability of the lumbar spine, AJNR Am J Neuroradiol, 2008, 29(5):838–842.
Corresponding author Mariana Cevei, Associate Professor, MD, PhD, Faculty of Medicine and Pharmacy, University of Oradea, Medical Rehabilitation Clinical Hospital Felix Spa, 417500 Felix, Romania; Phone +40723–281 865, e-mail: [email protected] Received: November 3rd, 2010
Accepted: December 18th, 2010