HIV Update: Approaches to TB/HIV Integration
11
Approaches to TB/HIV Integration HIV Update No 9 February 2011
-
Upload
international-hivaids-alliance -
Category
Documents
-
view
220 -
download
1
description
This is one in a series of regular HIV updates from the Alliance. This update highlights opportunities and approaches for integration of TB and HIV at various levels, including the community level. It identifies key actions that are required for successful scale up of TB/HIV collaborative activities in high burden countries in line with the WHO interim policy.
Transcript of HIV Update: Approaches to TB/HIV Integration

Approaches to TB/HIV Integration
HIV Update No 9
February 2011

2
Introduction
Tuberculosis (TB) is the single most important threat to persons living with HIV. A total of 1.7 million
people died from TB in 2009, including 380,000 people living with HIV, equal to 4700 deaths per day.
Not only is TB the largest cause of death amongst persons living with HIV AIDS, but it also has
important implications related to drug interactions and toxicity when a person is on both TB and HIV
medications. The risk of developing active TB from latent tuberculosis infection is increased 100-fold
in the setting of HIV infection. Furthermore even after a diagnosis of TB has been made, persons on
TB treatment may experience clinical deterioration due to immune reconstitution (technically referred
to as TB IRIS i.e. immune reconstitution inflammatory syndrome).
We must acknowledge that there has been some good progress in TB control globally. The
percentage of people successfully treated reached the highest level at 86% in 2008. In addition, more
than 41 million people have been successfully treated and more than 6 million lives saved from TB in
the last five years alone. However, this is a small proportion compared to the estimated number of TB
infections that occur annually, a significant proportion of which goes unreported and untreated,
resulting in thousands of TB related deaths.
In addition, the global disease burden caused by multidrug resistant (MDR) TB, a form of TB which is
difficult and expensive to treat and which fails to respond to standard first line drugs, is increasing.
Current estimates indicate that there are more than 400,000 MDR cases occurring annually and
150,000 deaths from MDR TB. It is therefore clear that the global burden of TB is high and that this
burden is especially high amongst persons living with HIV who are particularly vulnerable to TB due to
their weak immunity. The global burden of TB disease has been accelerated by the co-existence of
the HIV epidemic.
Why integrate?
The need to integrate TB and HIV is both urgent and logical, mainly due to the close interaction
between TB and HIV as well as the increasing and compelling evidence of the benefits of effective
integration. HIV and TB have many common features in terms of disease burden, epidemiological
contexts and the recommended strategic activities for their control, which include prevention of spread
of infection, case finding as well as treatment.
Summary
Tuberculosis is the most important cause of death amongst persons living with HIV. Consequently,
integration of TB and HIV is important because of the close linkages between the two diseases.
Integration of TB and HIV can be achieved using several approaches for collaborative activities at
different levels. Additionally, successful integration of TB and HIV is the first step in ensuring that
both TB and HIV responses are fully integrated into the wider health system. Although a number of
programmatic, infrastructural and human resource challenges remain, with commitment of all
stakeholders, successful integration is possible and will facilitate the achievement of the health
Millennium Development Goals.

3
Also, and as noted above, TB has an important impact on people living with HIV. For instance, TB is
responsible for 23% of all HIV-related deaths in developing countries. Both TB and HIV control form
important indicators of Millennium Development Goal (MDG) number 6. The aim of MDG 6 is to
combat HIV, TB, Malaria and other infectious diseases. Consequently, addressing TB and HIV in an
integrated fashion is critical to achieving progress in this particular MDG.
In addition, there is strong evidence of benefits of TB HIV integration to both health systems (in terms
of improved cost efficiency and increased access to services) as well as clinical outcomes (in terms of
reduced deaths amongst HIV patients and greater cure rates amongst TB patients). Thus every effort
should be made to achieve some level of TB HIV integration.
It must however be noted that successful control of TB and HIV control depends on the presence of
effective health system functions e.g. vital registration, drug procurement, laboratories, human
resources, financing and so on. Consequently, integration of TB and HIV responses should also occur
within a wider agenda of integration of the two diseases i.e. HIV and TB, into the wider health system.
The World Health Organization and the Stop TB Partnership recommend collaborative activities
between TB and HIV at various levels, examples of which are alluded to in the following section.
What are the opportunities for integration?
HIV and TB can be integrated at various levels including global, national, sub-national (i.e. provincial
and district) facility as well as at the community level. TB integration into HIV programs can be
achieved through several approaches including advocacy, communication and social mobilization,
fostering partnerships, program planning and implementation as well as operational research.
1. National level
Scale up of TB and HIV collaborative activities may necessitate unification of the national TB and HIV
control programs (ideal but difficult), joint planning between the National TB and AIDS programs,
shared policies, strategies, training manuals etc. Emerging evidence shows that joint planning has
been done successfully in a number of high burden countries such as Kenya. In addition, cohort
analysis and Medical Information Systems should facilitate tracking of both the TB and HIV status of
patients. Providing basic TB and HIV training for all primary health workers, (including pre-service
training), is another critical step which ensures that every health worker is well versed with both TB
and HIV prevention and treatment skills. In order to facilitate integration at lower levels, patient flow in
facilities and referral pathways may need to be changed. In addition, regular TB and HIV registers
may need to be re-designed so that they capture TB screening, TB treatment and HIV testing etc,
depending on the context and availability of resources.
2. District and regional level
Further opportunities exist for integration of TB and HIV activities at the district level. District focal
persons (if in place) should be responsible for both TB and HIV service delivery, including
surveillance, monitoring and reporting rather than having two parallel and vertical systems for TB and
HIV.

4
In practical terms this means that the existing TB or HIV coordinators or focal persons would assume
responsibility for both TB and HIV programs at the district level. In addition, tremendous progress
could be achieved if the programmatic coordination, planning, budgeting and resource allocation
could be decentralised to the district level.
3. Health facility level
There are numerous opportunities for integration of both TB and HIV disease responses in order to
ensure optimal utilization of resources as well as minimize the impact of both diseases on health
outcomes. This integration can be achieved at the programming level and ultimately at the service
provision level. Among other collaborative activities, the following offer unique opportunities for
integration and have some overlap with WHO-recommended TB / HIV collaborative activities:
1. Testing all TB patients for HIV
Since HIV testing is a key entry point to care,
confidential counselling and testing for HIV should
be offered to every TB patient and if possible at
every TB service delivery point. TB patients should
also be included in post-test support mechanisms
such as psychosocial support clubs, group
therapies and so on.
2. Screening all HIV patients for TB
HIV patients are at increased risk of TB due to their weak immune status. The incidence of TB
disease is particularly high amongst people living with HIV as compared to HIV negative persons. For
this reason, persons living with HIV should be screened regularly for TB, using simple screening
procedures as recommended by the World Health Organization or national TB programs. These may
include screening patients for chronic cough, night sweats, weight loss, previous history of contact
with a person on treatment for pulmonary TB, tuberculin skin sensitivity testing and so on. Early
diagnosis and treatment reduces the burden of TB disease at the population level.
3. Providing antiretroviral therapy early in patients with TB
Antiretroviral Therapy (ART) has been shown to dramatically reduce the incidence of TB amongst
persons living with HIV. Current evidence suggests that ART reduces the incidence of TB disease by
up to 80-90%. This is a huge benefit which should be made available to every eligible person living
with HIV. The WHO now recommends starting treatment at higher CD4 counts of 350.

5
Isoniazid preventive therapy means
that a person without TB disease (but
who is at high risk) takes TB drugs
for a period of at least six months as
a preventive measure against
Tuberculosis.
This effectively means that a larger proportion of HIV patients
would benefit from a reduced risk of developing TB disease if
they started ART earlier in line with this particular
recommendation. Every eligible person living with HIV should
access antiretroviral drugs before their CD 4 count falls far
below 350.
4. Provision of Isoniazid Preventive Therapy for PLHIV
at high risk of TB
Isoniazid preventive therapy (IPT) increases the likelihood that a
HIV positive individual will remain free of TB disease.
Currently, the global uptake of IPT has been low, mainly due to
slow policy changes at national levels as well as the fear that
Isoniazid resistance could emerge as a result of widespread use
of IPT. The World Health Organization recommends provision of
IPT for 6 months to HIV persons at high risk of TB.
A recent trial conducted in Botswana by the US-based Centres
for Disease Control and Prevention showed that the residual
benefit of IPT can extend up to 36 months, and that this benefit
is largely restricted to persons with positive tuberculin tests.
Additional evidence shows that if ART is offered together with
IPT, it has an even greater protective benefit, meaning that
these two interventions can be combined to further reduce the
risk of TB disease amongst people living with HIV in settings
where there is high prevalence of both diseases.
5. Provision of Cotrimoxazole Prophylaxis Therapy to
HIV positive TB patients
Cotrimoxazole prophylaxis should be offered to persons living with HIV as per national guidelines,
including those on TB treatment. Cotrimoxazole is an important drug which reduces the risk of
opportunistic infections amongst persons living with HIV.
WHO Interim Policy on
Collaborative TB and HIV
Activities
A Establish mechanisms for
collaboration
A1 Joint coordination of TB HIV
at national regional, district and
local levels
A2 Surveillance of HIV amongst
TB patients
A3 Joint TB /HIV planning
A4 Monitoring & evaluation
B Decrease the burden of TB
in Persons living with HIV
B1 Intensified TB case finding
B2 IPT Implementation
B3 TB Infection control
C Decrease the burden of HIV
in tuberculosis patients
C1 Provide HIV testing and
counselling
C2 Introduce HIV prevention
C3 Cotrimoxazole prophylaxis
C4 HIV care and support

6
In such situations, close clinical monitoring is required due to possible drug toxicities. Cotrimozaxole
prophylaxis is protective against a wide range of other bacterial infections including Q fever,
pneumocystis jeroveci pneumonia, as well as protozoa infections such as malaria.
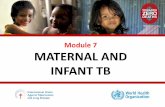
6. Physical proximity of TB and HIV service delivery points
Often, the linkages between HIV and TB can be improved by close physical proximity of TB and HIV
service provision points. However it is important to remember that infection control is critical in such
situations because of the increased vulnerability of HIV patients to TB. Clear patient flow and referral
pathways at the health facility can often be beneficial in ensuring that there are no missed
opportunities in TB case detection as well as HIV testing and counselling. This can be achieved
through a number of models as shown below, depending on health system factors and resource
contexts.
Model 1: Cross referrals
between HIV and TB service
points
Model 2: Partial integration e.g.
TB and HIV services in the
same facility or synchronised
same day appointments
Model 3: provision of TB and
HIV services under the same
roof or same provider
TB and HIV services are
separate and TB patients and
the co-infected seek HIV testing
services, HIV care and
treatment support outside of the
TB clinic. TB/HIV services are
linked by a referral system. This
is the most common model in
many settings
Partial integration is achieved
by deliberate effort by health
professionals to ensure that
services can be delivered on
the same day.
TB and HIV services
(Counselling and testing for
HIV, ART, TB screening and
treatment) are provided in the
same room by the same staff.
4. Community level
The number of persons living with HIV is gradually increasing, partly due to the fact that the
availability of ART has prolonged the lives of people living with HIV, as well as the continuing
occurrence of new infections. Community health or extension workers need to be trained in both HIV
and TB. They need to be equipped with tools and skills to advocate for both TB and HIV responses.
TB HIV TB HIV BOTH

7
Standardized short-course
anti-TB treatment is often
provided under direct and
supportive observation
(DOT) which helps to ensure
the right drugs are taken at
the right time for the full
duration of treatment.
Supportive observation can
be provided by the health
workers, designated family
members, community
resource persons or peers.
Intensified case finding, home based care, contact tracing, DOT follow up as well as defaulter tracing
for both ART and TB treatment should be performed by the same community health worker,
whenever possible. It is not necessary to have community health worker for TB and others for HIV. In
addition, support to patients on TB medications, Isoniazid Preventive Therapy, ART and
Cotrimoxazole Prophylaxis should be offered as an integrated package to both HIV and TB patients
including nutritional screening and support.
What is the Road map to achievement of MDG 6 TB and HIV indicators?
As the year 2015 approaches, every effort should be made to ensure that MDG 6 indicators including
a reduction in the burden of TB and HIV will be achieved. Integration of TB and HIV using several
approaches to include those suggested below offers a strategic roadmap towards this.
1. Advocacy communication and social mobilization
All stakeholders should scale up multi-disease advocacy
on TB and HIV. Civil society and treatment groups should
monitor their governments’ policies on TB and HIV
integration and advocate for change. Joint awareness-
raising for both TB and HIV including IEC materials and
campaigns are now urgently needed.
2. Program monitoring and evaluation and operational research
Joint program indicators for both TB and HIV should be emphasized and tracked consistently,
including program tools and registers which should track TB and HIV status, service uptake, retention
in care, adherence to treatment, Isoniazid Preventive Therapy and Cotrimoxazole Prophylaxis
Therapy. Monitoring and reporting TB treatment outcomes stratified according to HIV status especially
mortality as well as recording and reporting TB prevalence amongst HIV patients are valuable
indicators that could show the extent of integration in service provision. More collaborative operational
research and surveys are required to deal with emerging issues in HIV and TB. The important
message here is that programs should ensure that information on TB and HIV is systematically
collected, analysed and informs decision making at all levels.
3. Partnerships
Public-private partnerships continue to offer an additional platform through which private health
providers are sensitized about both TB and HIV prevention, care and treatment. Partnership with the
community has been shown to increases access and adherence to both TB and ART. Fostering
partnerships with other stakeholders including non-governmental organizations, government
institutions, pharmaceutical organizations and advocacy groups is important for successful
integration.

8
What are the key determinants of success?
Epidemiological context, including HIV and TB prevalence, malnutrition, social economic factors,
geographical setting (rural versus urban), poverty and gender may influence success of integration. In
addition, the health system architecture, service availability, service access, health financing and
policy are important determinants of extent of integration. There are important programmatic,
infrastructural, and staffing challenges in many developing countries which may need to be addressed
within the wider health system in-order to facilitate TB / HIV integration. However, with strong
commitment from the political leaders, civil society, treatment advocacy groups and the community,
successful integration of TB and HIV can be achieved.
Conclusions
There is urgent need to put into place rigorous measures to integrate TB and HIV response globally,
which can be achieved at various levels and using a number of approaches. A number of
programmatic, infrastructural, and human resource challenges must be addressed through
strengthening the health systems. Communities can play an important role in supporting the
integration of TB into HIV programs by tackling stigma and discrimination, offering support to people
living with HIV and TB and strengthening community-based referrals, linkages and service provision
of both TB and HIV.

9
Glossary of Terms and Abbreviations
1. AIDS: Acquired Immune Deficiency Syndrome
2. ART: Antiretroviral therapy which constitutes a combination of drugs from two or more classes
for HIV treatment
3. DOT: Directly observed therapy for Tuberculosis
4. HIV: Human immunodeficiency virus
5. IPT : Isoniazid preventive therapy is one of the key interventions recommended by WHO in
1998 to reduce the burden of TB in people living with HIV
6. MDG: Millennium development goals are eight international development goals that all 192
United Nations member states and at least 23 international organizations have agreed to
achieve by the year 2015.
7. MDR: Multi-drug resistant Tuberculosis is a particularly form of TB which is hard to treat which
is associated with resistance of Tuberculosis mycobacterium to multiply even in the presence of
TB drugs such as Rifampicin or Isoniazid.
8. PLHIV: People living with HIV
9. Q fever: Q fever is a zoonosis caused by Coxiella burnetii which can cause complications in
pregnancy.
10. TB : Tuberculosis, a contagious and airborne disease (mainly of the lungs) which is caused by
Tuberculosis mycobacterium
11. TB IRIS: Tuberculosis immune reconstitution inflammatory syndrome, which can lead to clinical
deterioration of a person on treatment for due to the improvement of the immune system.
12. WHO: World Health Organization

10
References and recommended readings:
1. WHO Interim policy on collaborative HIV TB activities. 2004. WHO Geneva. Available at
http://www.who.int/hiv/pub/tb/en/Printed_version_interim-policy_2004.pdf
2. STOP TB Partnership. 2008 Global Plan to stop TB 2006-2015. Progress report 2006-2008.
Available at
http://www.stoptb.org/assets/documents/global/plan/The_global_plan_progress_report1.pdf
3. Friedland G, Harries A, Coetzee D Implementation issues in tuberculosis/HIV program
collaboration and integration: 3 case studies. J Infect Dis. 2007 Aug 15;196 Suppl 1:S114-23.
4. Gandhi NR, Moll AP, Lalloo U, Pawinski R, Zeller K, Moodley P, Meyer E, Friedland G;
Tugela Ferry Care and Research (TFCaRes) Collaboration.Successful integration of
tuberculosis and HIV treatment in rural South Africa: the Sizonq'oba study. J Acquir Immune
Defic Syndr. 2009 Jan 1;50(1):37-43.
5. Wandwalo E Kapalata N, Tarimo E Corrigan CB Morkve O Collaboration between the national
tuberculosis programme and a non-governmental organisation in TB/HIV care at a district
level: experience from Tanzania. Afr Health Sci. 2004 Aug;4(2):109-14.
6. Harris JB, Hatwiinda SM, Randels KM, Chi BH, Kancheya NG, Jham MA, Samungole KV,
Tambatamba BC, Cantrell RA, Levy JW, Kimerling ME, Reid SE Early lessons from the
integration of tuberculosis and HIV services in primary care centers in Lusaka, Zambia. Int J
Tuberc Lung Dis. 2008 Jul;12(7):773-9.
7. Conseil A, Mounier-Jack S, Coker R Integration of health systems and priority health
interventions: a case study of the integration of HIV and TB control programmes into the
general health system in Vietnam. Health Policy Plan. 2010 Nov;25 Suppl 1:i32-36.
8. Maher D Re-thinking global health sector efforts for HIV and tuberculosis epidemic control:
promoting integration of programme activities within a strengthened health system. BMC
Public Health. 2010 Jul 5;10:394.
9. Carcopino X, Raoult D, Bretelle F, Boubli L, Stein A. Managing Q fever during pregnancy: the
benefits of long-term cotrimoxazole therapy. Clin Infect Di.s 2007 Sep 1;45(5):548-55. Epub
2007 Jul 17.

11
For further information please contact:
Gitau Mburu
Senior Advisor, HIV and Health Systems
e-mail address: [email protected]
Telephone:+44(0)1273 718929
International HIV/AIDS Alliance
(International secretariat)
Telephone: +44(0)1273 718900
Fax: +44(0)1273 718901
www.aidsalliance.org
Registered British charity number: 1038860