HCV-TARGET Hepatitis C Therapeutic Registry and...
106
-
Upload
nguyenhanh -
Category
Documents
-
view
220 -
download
6
Transcript of HCV-TARGET Hepatitis C Therapeutic Registry and...

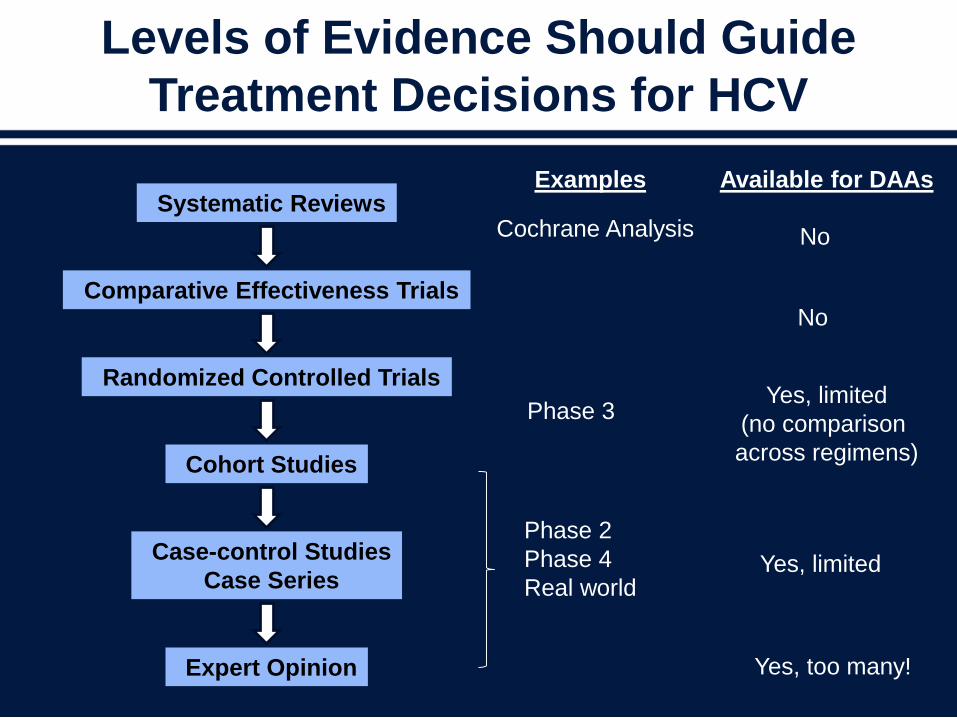
Levels of Evidence Should Guide
Treatment Decisions for HCV
Systematic Reviews
Randomized Controlled Trials
Cohort Studies
Case-control Studies
Case Series
Expert Opinion
Cochrane Analysis
Examples Available for DAAs
No
Phase 3
No
Phase 2
Phase 4
Real world
Yes, limited
(no comparison
across regimens)
Yes, limited
Yes, too many!
Comparative Effectiveness Trials

Gaps in Evidence
Need for Real-world Data
• Gaps in evidence
– Major evidence gaps around effectiveness of HCV therapies
eg, SOF + SMV enters guidelines and recent FDA approval based
on 167 patients from phase 2
Patient populations: women, blacks, older, comorbidities,
cirrhosis, active substance abuse or mental illness, prior DAA
failure, HIV, transplant, ESRD
Treatment harms/benefits (short-term and long-term), side effects
Impact of adherence and out-of-pocket costs
– Need to understand real-world effects of antiviral regimens
in a broader spectrum of patients
Real-world data often very different than predicted by phase 3
studies
The Benefits of Phase 4
• The benefits gained from postmarketing data
– We learn how drugs “behave” in the real world
Patients are more heterogeneous
Prescribers are more heterogeneous
Patients are not as carefully screened
Treatment is not as carefully monitored
– We broaden our knowledge of short- and long-term
benefits and risks
Trials are short; real life has no time limit
• Mission: to maintain an international registry of patients undergoing treatment with new therapies for HCV at both academic and community practices
• Study design: longitudinal, observational study
– Inclusion criteria: adult patients (≥18 years) prescribed any HCV treatment
• Specific aims
– Improve information of populations underrepresented in phase 3 trials
– Evaluate regimens used in clinical practice (approved and unapproved)
– Identify and remediate educational gaps and adverse event management
– Serve as a core for collaborative, translational studies
• Highlights
– Partnership: academia + industry + FDA
– >4700 patients enrolled to date
http://www.hcvtarget.org/
HCV-TARGET
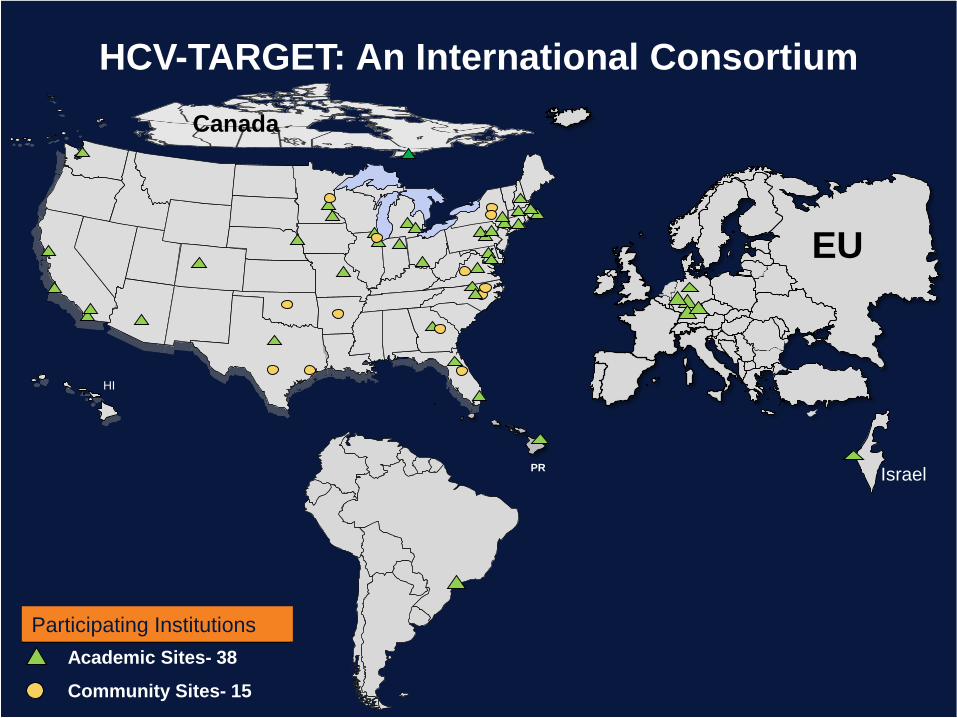
HCV-TARGET: An International Consortium
HI
Canada
PR
EU
IsraelSA
Academic Sites- 38
Community Sites- 15
Participating Institutions
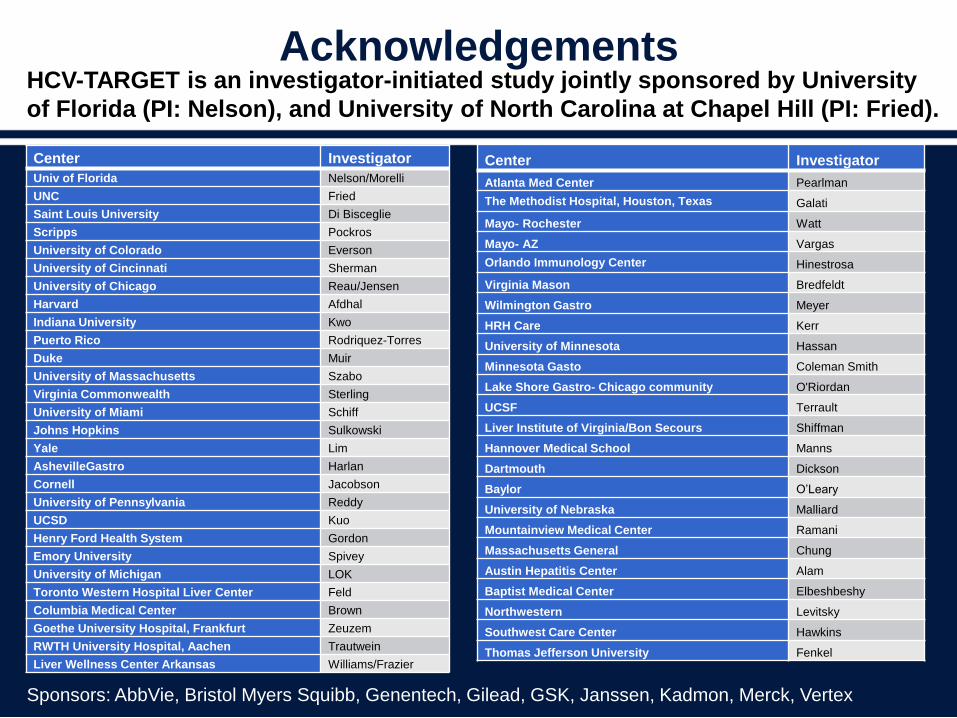
Acknowledgements
Center Investigator
Univ of Florida Nelson/Morelli
UNC Fried
Saint Louis University Di Bisceglie
Scripps Pockros
University of Colorado Everson
University of Cincinnati Sherman
University of Chicago Reau/Jensen
Harvard Afdhal
Indiana University Kwo
Puerto Rico Rodriquez-Torres
Duke Muir
University of Massachusetts Szabo
Virginia Commonwealth Sterling
University of Miami Schiff
Johns Hopkins Sulkowski
Yale Lim
AshevilleGastro Harlan
Cornell Jacobson
University of Pennsylvania Reddy
UCSD Kuo
Henry Ford Health System Gordon
Emory University Spivey
University of Michigan LOK
Toronto Western Hospital Liver Center Feld
Columbia Medical Center Brown
Goethe University Hospital, Frankfurt Zeuzem
RWTH University Hospital, Aachen Trautwein
Liver Wellness Center Arkansas Williams/Frazier
Center Investigator
Atlanta Med Center Pearlman
The Methodist Hospital, Houston, Texas Galati
Mayo- Rochester Watt
Mayo- AZ Vargas
Orlando Immunology Center Hinestrosa
Virginia Mason Bredfeldt
Wilmington Gastro Meyer
HRH Care Kerr
University of Minnesota Hassan
Minnesota Gasto Coleman Smith
Lake Shore Gastro- Chicago community O'Riordan
UCSF Terrault
Liver Institute of Virginia/Bon Secours Shiffman
Hannover Medical School Manns
Dartmouth Dickson
Baylor O’Leary
University of Nebraska Malliard
Mountainview Medical Center Ramani
Massachusetts General Chung
Austin Hepatitis Center Alam
Baptist Medical Center Elbeshbeshy
Northwestern Levitsky
Southwest Care Center Hawkins
Thomas Jefferson University Fenkel
Sponsors: AbbVie, Bristol Myers Squibb, Genentech, Gilead, GSK, Janssen, Kadmon, Merck, Vertex
HCV-TARGET is an investigator-initiated study jointly sponsored by University
of Florida (PI: Nelson), and University of North Carolina at Chapel Hill (PI: Fried).
HCV-TARGET: Real-world
Data Promising Real-world
Solutions
Mark Sulkowski, MD
Professor of Medicine
Johns Hopkins University School of Medicine
Medical Director, Viral Hepatitis Center
Divisions of Infectious Diseases and
Gastroenterology/Hepatology
Baltimore, Maryland USA
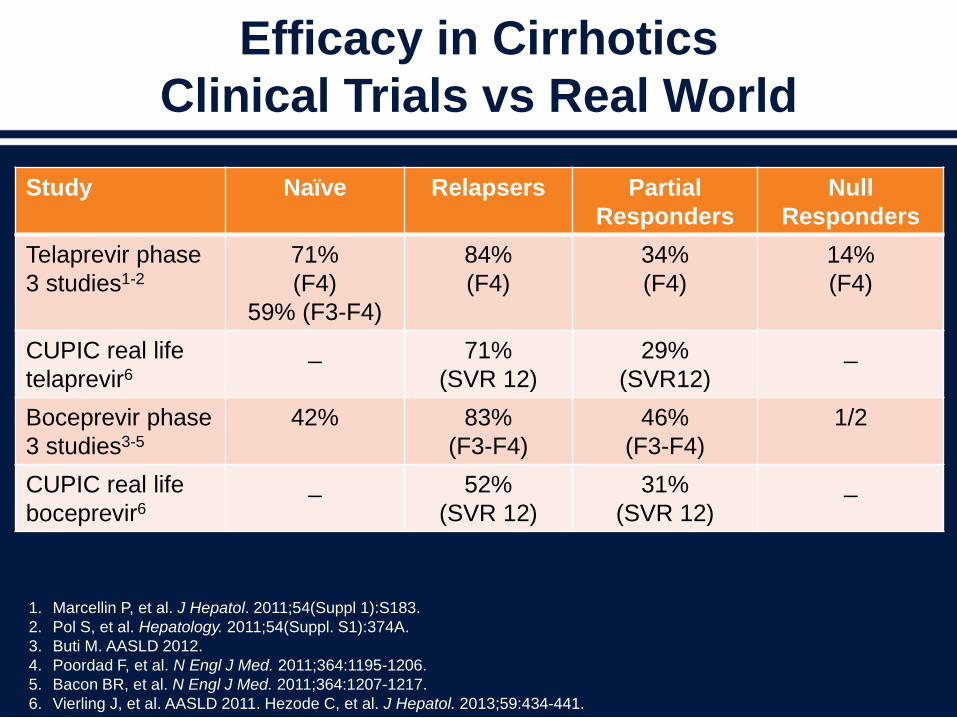
Efficacy in Cirrhotics
Clinical Trials vs Real World
Study Naïve Relapsers Partial
Responders
Null
Responders
Telaprevir phase
3 studies1-2
71%
(F4)
59% (F3-F4)
84%
(F4)
34%
(F4)
14%
(F4)
CUPIC real life
telaprevir6
_ 71%
(SVR 12)
29%
(SVR12)
_
Boceprevir phase
3 studies3-5
42% 83%
(F3-F4)
46%
(F3-F4)
1/2
CUPIC real life
boceprevir6
_ 52%
(SVR 12)
31%
(SVR 12)
_
1. Marcellin P, et al. J Hepatol. 2011;54(Suppl 1):S183.
2. Pol S, et al. Hepatology. 2011;54(Suppl. S1):374A.
3. Buti M. AASLD 2012.
4. Poordad F, et al. N Engl J Med. 2011;364:1195-1206.
5. Bacon BR, et al. N Engl J Med. 2011;364:1207-1217.
6. Vierling J, et al. AASLD 2011. Hezode C, et al. J Hepatol. 2013;59:434-441.
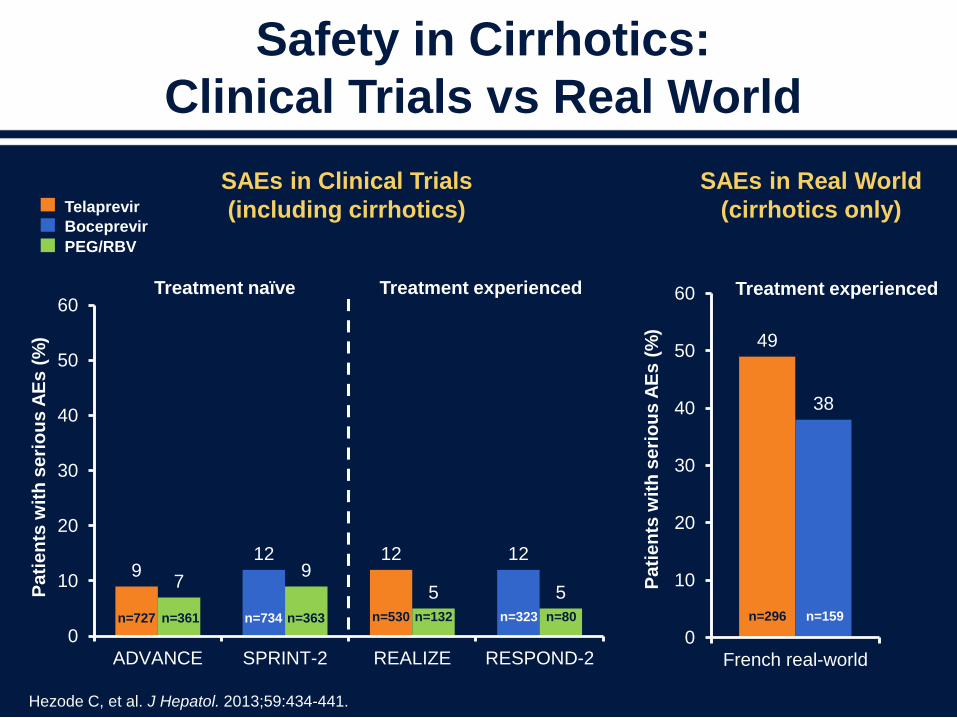
49
38
0
10
20
30
40
50
60
French real-worldP
ati
en
ts w
ith
se
rio
us
AE
s (
%)
912 12 12
79
5 5
0
10
20
30
40
50
60
ADVANCE SPRINT-2 REALIZE RESPOND-2
Pa
tie
nts
wit
h s
eri
ou
s A
Es
(%
)
n=530 n=323n=734n=727 n=159n=296
SAEs in Clinical Trials
(including cirrhotics)
SAEs in Real World
(cirrhotics only)
Treatment naïve Treatment experienced Treatment experienced
Telaprevir
Boceprevir
n=132 n=80n=363n=361
PEG/RBV
Safety in Cirrhotics:
Clinical Trials vs Real World
Hezode C, et al. J Hepatol. 2013;59:434-441.
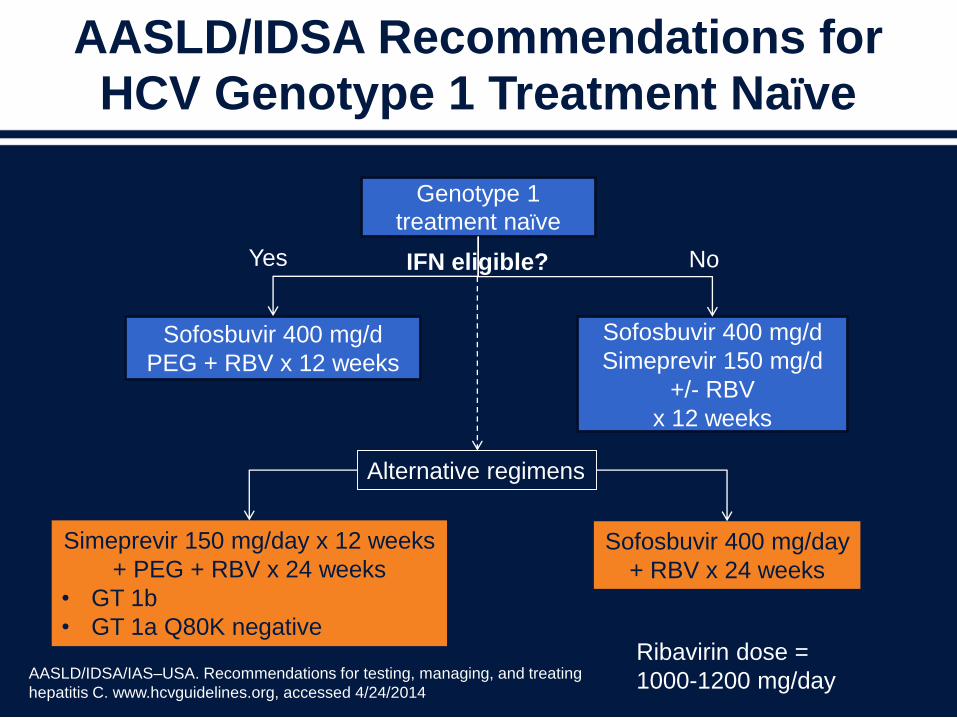
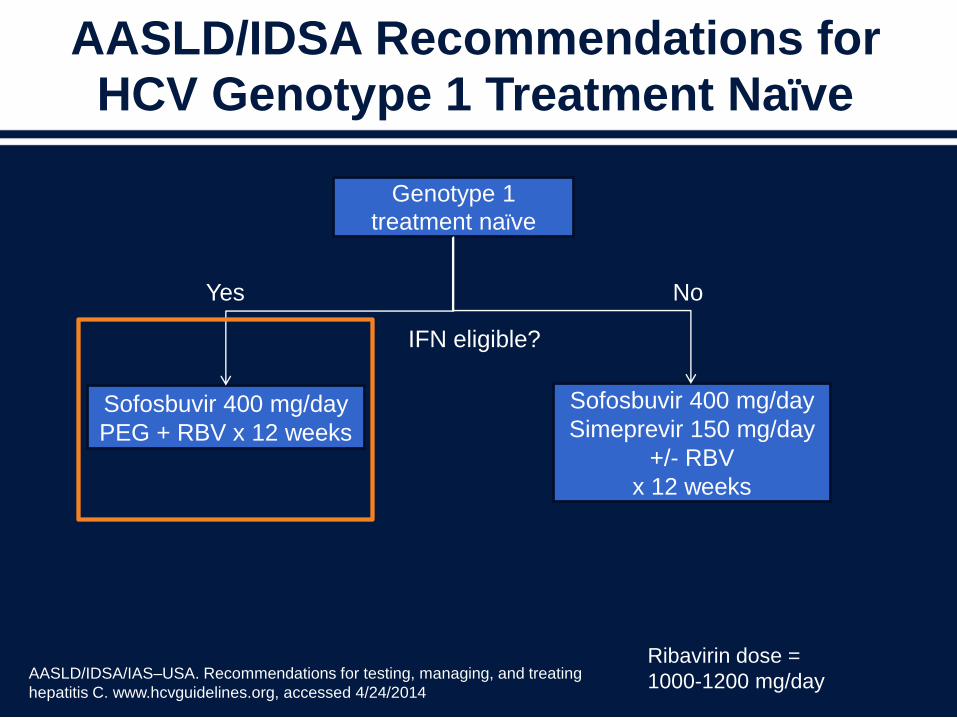
AASLD/IDSA Recommendations for HCV Genotype 1 Treatment Naïve
AASLD/IDSA/IAS–USA. Recommendations for testing, managing, and treating
hepatitis C. www.hcvguidelines.org, accessed 4/24/2014
Genotype 1
treatment naïve
Sofosbuvir 400 mg/d
PEG + RBV x 12 weeks
Sofosbuvir 400 mg/d
Simeprevir 150 mg/d
+/- RBV
x 12 weeks
IFN eligible?Yes No
Simeprevir 150 mg/day x 12 weeks
+ PEG + RBV x 24 weeks
• GT 1b
• GT 1a Q80K negative
Sofosbuvir 400 mg/day
+ RBV x 24 weeks
Alternative regimens
Ribavirin dose =
1000-1200 mg/day
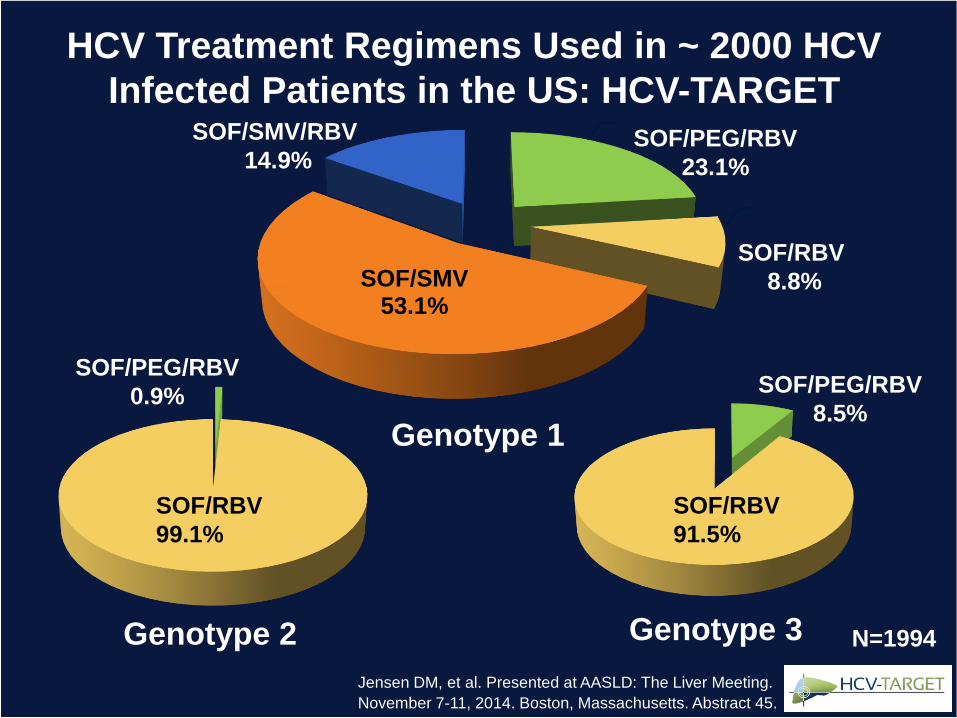
HCV Treatment Regimens Used in ~ 2000 HCV
Infected Patients in the US: HCV-TARGET
N=1994
SOF/SMV 53.1%
Genotype 2 Genotype 3
SOF/PEG/RBV
0.9%
SOF/RBV
99.1%
SOF/PEG/RBV
8.5%
SOF/RBV
91.5%
Genotype 1
SOF/SMV/RBV
14.9%SOF/PEG/RBV
23.1%
SOF/RBV
8.8%
Jensen DM, et al. Presented at AASLD: The Liver Meeting.
November 7-11, 2014. Boston, Massachusetts. Abstract 45.
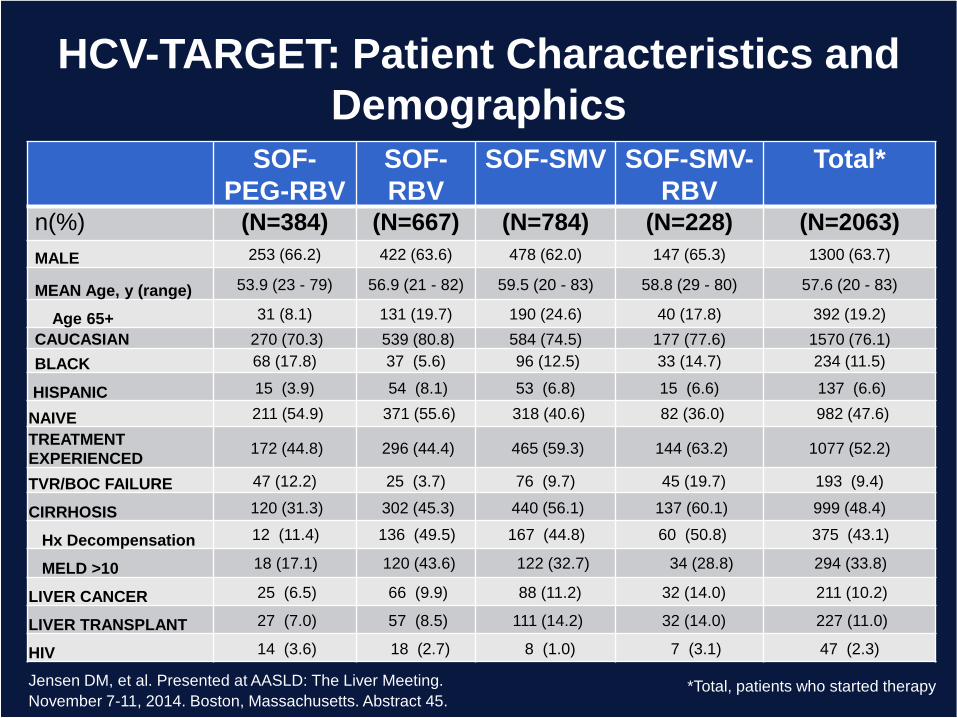
HCV-TARGET: Patient Characteristics and
DemographicsSOF-
PEG-RBV
SOF-
RBV
SOF-SMV SOF-SMV-
RBV
Total*
n(%) (N=384) (N=667) (N=784) (N=228) (N=2063)
MALE 253 (66.2) 422 (63.6) 478 (62.0) 147 (65.3) 1300 (63.7)
MEAN Age, y (range) 53.9 (23 - 79) 56.9 (21 - 82) 59.5 (20 - 83) 58.8 (29 - 80) 57.6 (20 - 83)
Age 65+ 31 (8.1) 131 (19.7) 190 (24.6) 40 (17.8) 392 (19.2)
CAUCASIAN 270 (70.3) 539 (80.8) 584 (74.5) 177 (77.6) 1570 (76.1)
BLACK 68 (17.8) 37 (5.6) 96 (12.5) 33 (14.7) 234 (11.5)
HISPANIC 15 (3.9) 54 (8.1) 53 (6.8) 15 (6.6) 137 (6.6)
NAIVE 211 (54.9) 371 (55.6) 318 (40.6) 82 (36.0) 982 (47.6)
TREATMENT
EXPERIENCED 172 (44.8) 296 (44.4) 465 (59.3) 144 (63.2) 1077 (52.2)
TVR/BOC FAILURE 47 (12.2) 25 (3.7) 76 (9.7) 45 (19.7) 193 (9.4)
CIRRHOSIS 120 (31.3) 302 (45.3) 440 (56.1) 137 (60.1) 999 (48.4)
Hx Decompensation 12 (11.4) 136 (49.5) 167 (44.8) 60 (50.8) 375 (43.1)
MELD >10 18 (17.1) 120 (43.6) 122 (32.7) 34 (28.8) 294 (33.8)
LIVER CANCER 25 (6.5) 66 (9.9) 88 (11.2) 32 (14.0) 211 (10.2)
LIVER TRANSPLANT 27 (7.0) 57 (8.5) 111 (14.2) 32 (14.0) 227 (11.0)
HIV 14 (3.6) 18 (2.7) 8 (1.0) 7 (3.1) 47 (2.3)
*Total, patients who started therapy Jensen DM, et al. Presented at AASLD: The Liver Meeting.
November 7-11, 2014. Boston, Massachusetts. Abstract 45.
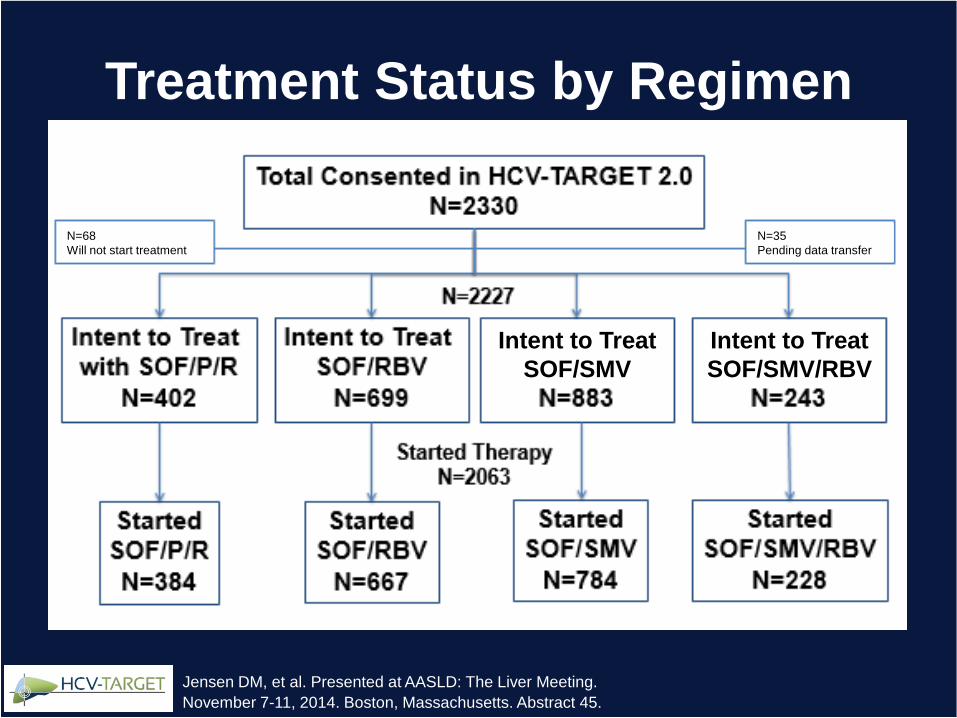
Treatment Status by Regimen
Jensen DM, et al. Presented at AASLD: The Liver Meeting.
November 7-11, 2014. Boston, Massachusetts. Abstract 45.
N=68
Will not start treatment
N=35
Pending data transfer
Intent to Treat
SOF/SMV
Intent to Treat
SOF/SMV/RBV
AASLD/IDSA Recommendations for HCV Genotype 1 Treatment Naïve
Genotype 1
treatment naïve
Sofosbuvir 400 mg/day
PEG + RBV x 12 weeks
Sofosbuvir 400 mg/day
Simeprevir 150 mg/day
+/- RBV
x 12 weeks
IFN eligible?
Yes No
Ribavirin dose =
1000-1200 mg/dayAASLD/IDSA/IAS–USA. Recommendations for testing, managing, and treating
hepatitis C. www.hcvguidelines.org, accessed 4/24/2014
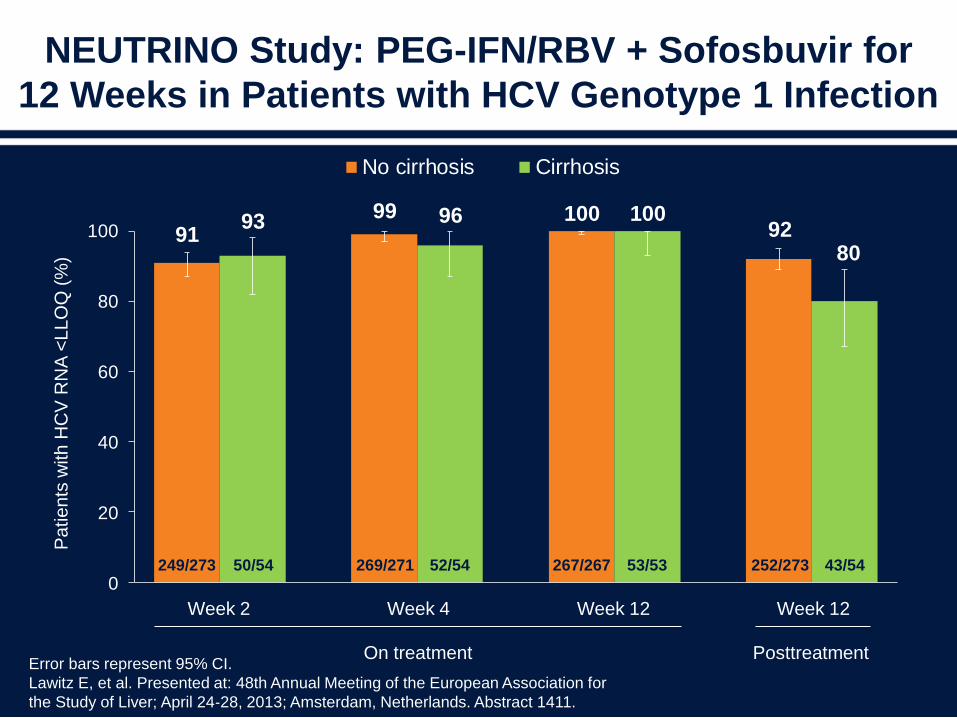
NEUTRINO Study: PEG-IFN/RBV + Sofosbuvir for
12 Weeks in Patients with HCV Genotype 1 Infection
Error bars represent 95% CI.
Lawitz E, et al. Presented at: 48th Annual Meeting of the European Association for
the Study of Liver; April 24‐28, 2013; Amsterdam, Netherlands. Abstract 1411.
9193
99 96 100 10092
80
0
20
40
60
80
100
No cirrhosis Cirrhosis
Posttreatment On treatment
Pa
tie
nts
with
HC
V R
NA
<LL
OQ
(%
)
50/54 52/54 53/53
Week 2 Week 4 Week 12 Week 12
43/54249/273 269/271 267/267 252/273
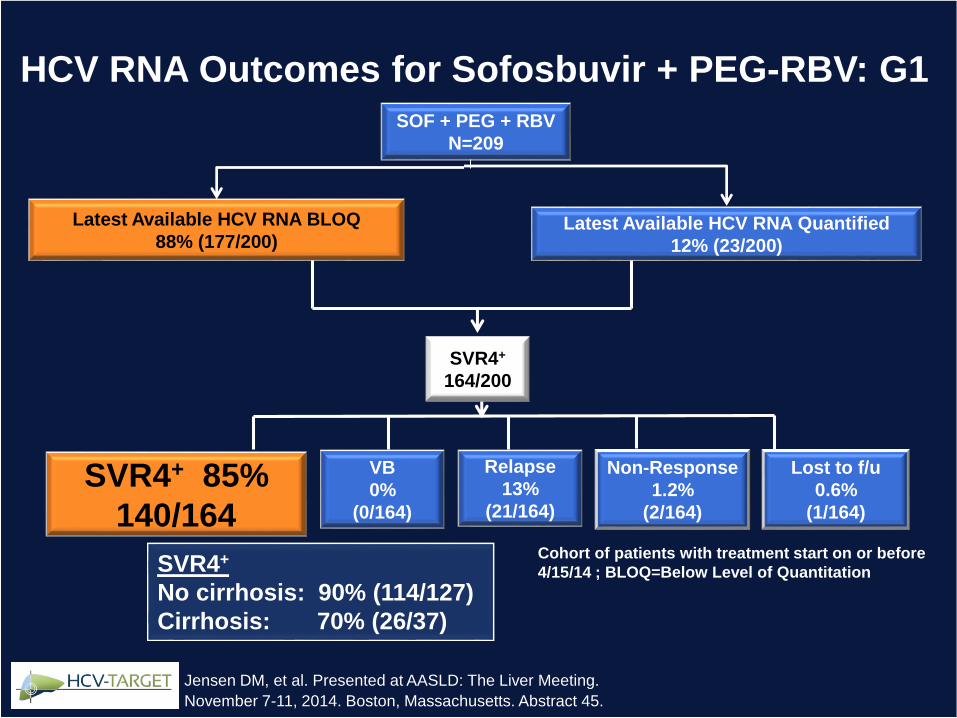
SOF + PEG + RBV
N=209
Latest Available HCV RNA BLOQ
88% (177/200)Latest Available HCV RNA Quantified
12% (23/200)
Cohort of patients with treatment start on or before
4/15/14 ; BLOQ=Below Level of Quantitation
HCV RNA Outcomes for Sofosbuvir + PEG-RBV: G1
VB
0%
(0/164)
Relapse
13%
(21/164)
SVR4+
164/200
SVR4+ 85%
140/164
Non-Response
1.2%
(2/164)
SVR4+
No cirrhosis: 90% (114/127)
Cirrhosis: 70% (26/37)
Lost to f/u
0.6%
(1/164)
Jensen DM, et al. Presented at AASLD: The Liver Meeting.
November 7-11, 2014. Boston, Massachusetts. Abstract 45.
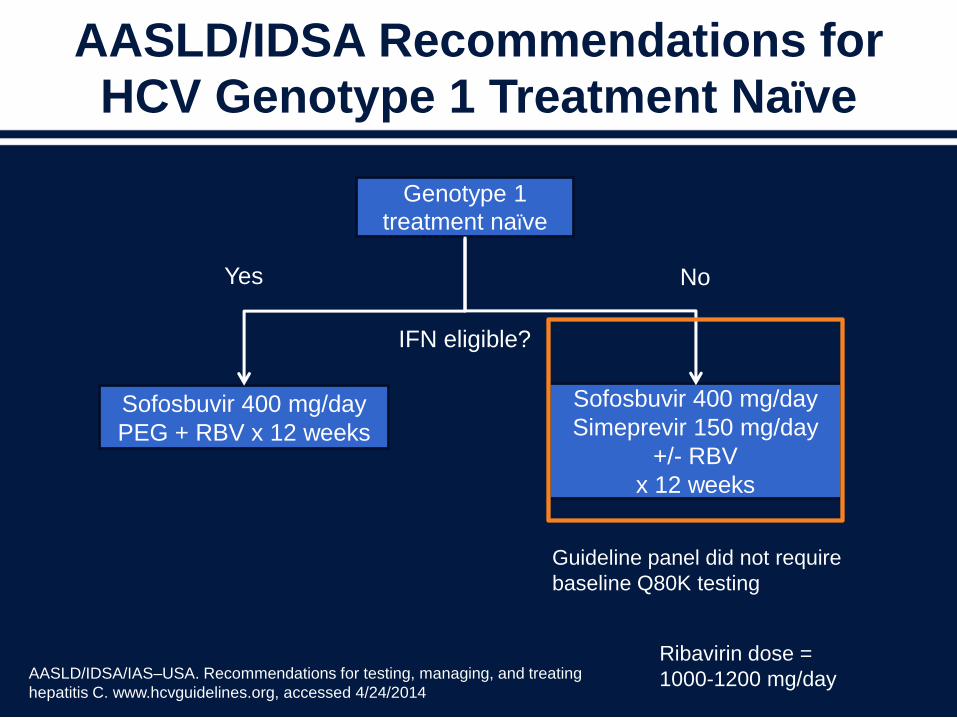
AASLD/IDSA Recommendations for HCV Genotype 1 Treatment Naïve
Genotype 1
treatment naïve
Sofosbuvir 400 mg/day
PEG + RBV x 12 weeks
Sofosbuvir 400 mg/day
Simeprevir 150 mg/day
+/- RBV
x 12 weeks
IFN eligible?
Yes No
Ribavirin dose =
1000-1200 mg/dayAASLD/IDSA/IAS–USA. Recommendations for testing, managing, and treating
hepatitis C. www.hcvguidelines.org, accessed 4/24/2014
Guideline panel did not require
baseline Q80K testing
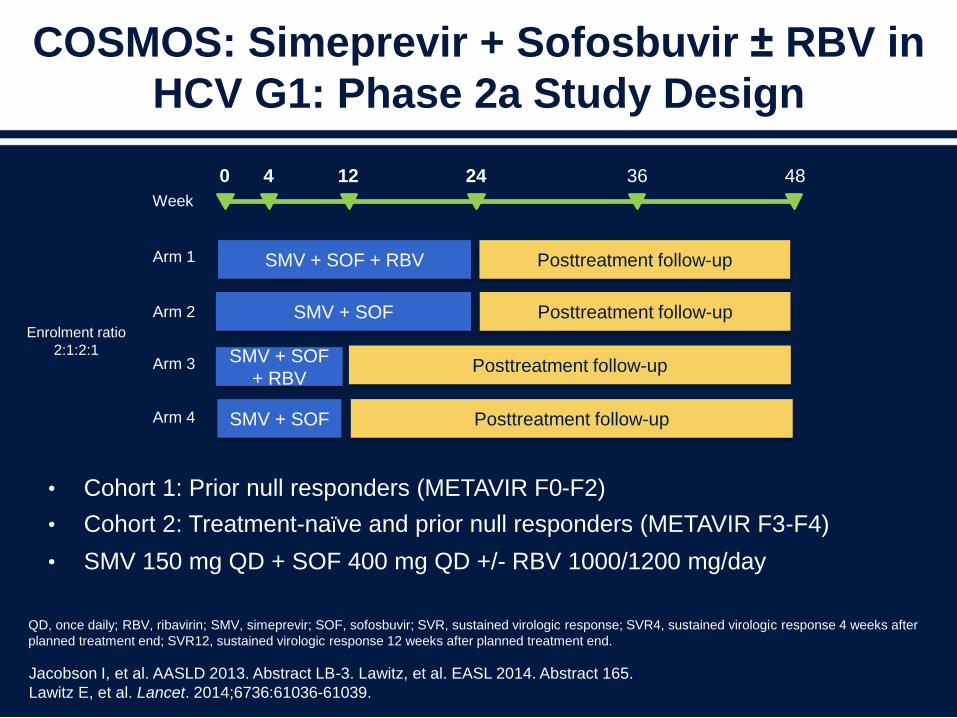
COSMOS: Simeprevir + Sofosbuvir ± RBV in
HCV G1: Phase 2a Study Design
• Cohort 1: Prior null responders (METAVIR F0-F2)
• Cohort 2: Treatment-naïve and prior null responders (METAVIR F3-F4)
• SMV 150 mg QD + SOF 400 mg QD +/- RBV 1000/1200 mg/day
Jacobson I, et al. AASLD 2013. Abstract LB-3. Lawitz, et al. EASL 2014. Abstract 165.
Lawitz E, et al. Lancet. 2014;6736:61036-61039.
QD, once daily; RBV, ribavirin; SMV, simeprevir; SOF, sofosbuvir; SVR, sustained virologic response; SVR4, sustained virologic response 4 weeks after
planned treatment end; SVR12, sustained virologic response 12 weeks after planned treatment end.
SMV + SOF + RBV Posttreatment follow-up
0 4 12 24 36 48
Arm 1
Week
SMV + SOF
SMV + SOF
+ RBV
SMV + SOF
Posttreatment follow-up
Posttreatment follow-up
Posttreatment follow-up
Arm 2
Arm 3
Arm 4
Enrolment ratio
2:1:2:1
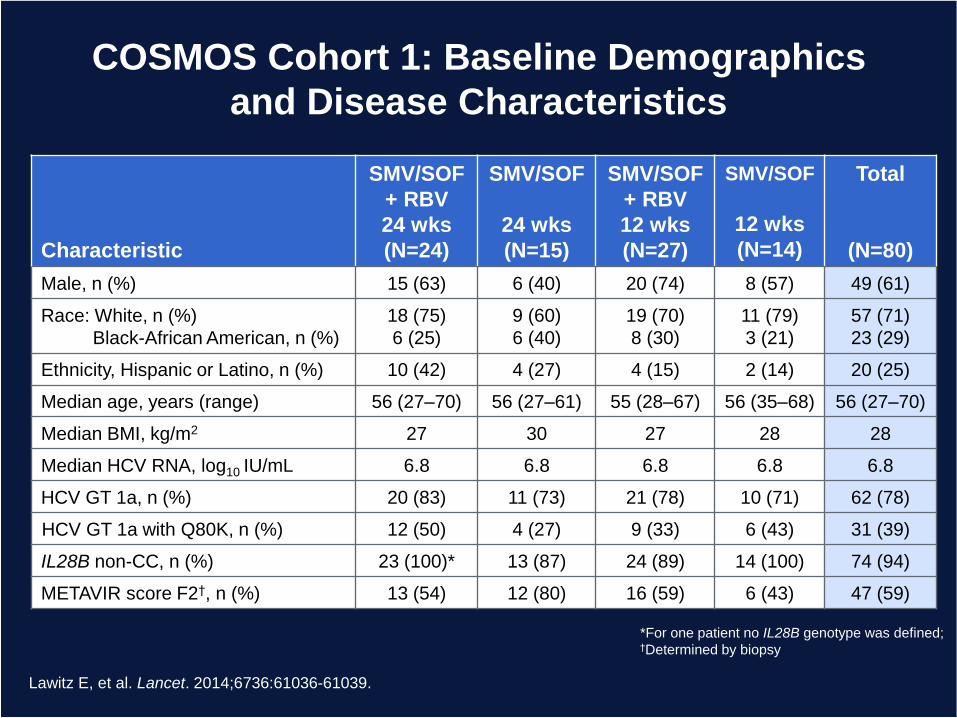
COSMOS Cohort 1: Baseline Demographics
and Disease Characteristics
Characteristic
SMV/SOF
+ RBV
24 wks
(N=24)
SMV/SOF
24 wks
(N=15)
SMV/SOF
+ RBV
12 wks
(N=27)
SMV/SOF
12 wks
(N=14)
Total
(N=80)
Male, n (%) 15 (63) 6 (40) 20 (74) 8 (57) 49 (61)
Race: White, n (%)
Black-African American, n (%)
18 (75)
6 (25)
9 (60)
6 (40)
19 (70)
8 (30)
11 (79)
3 (21)
57 (71)
23 (29)
Ethnicity, Hispanic or Latino, n (%) 10 (42) 4 (27) 4 (15) 2 (14) 20 (25)
Median age, years (range) 56 (27–70) 56 (27–61) 55 (28–67) 56 (35–68) 56 (27–70)
Median BMI, kg/m2 27 30 27 28 28
Median HCV RNA, log10 IU/mL 6.8 6.8 6.8 6.8 6.8
HCV GT 1a, n (%) 20 (83) 11 (73) 21 (78) 10 (71) 62 (78)
HCV GT 1a with Q80K, n (%) 12 (50) 4 (27) 9 (33) 6 (43) 31 (39)
IL28B non-CC, n (%) 23 (100)* 13 (87) 24 (89) 14 (100) 74 (94)
METAVIR score F2†, n (%) 13 (54) 12 (80) 16 (59) 6 (43) 47 (59)
*For one patient no IL28B genotype was defined;†Determined by biopsy
Lawitz E, et al. Lancet. 2014;6736:61036-61039.
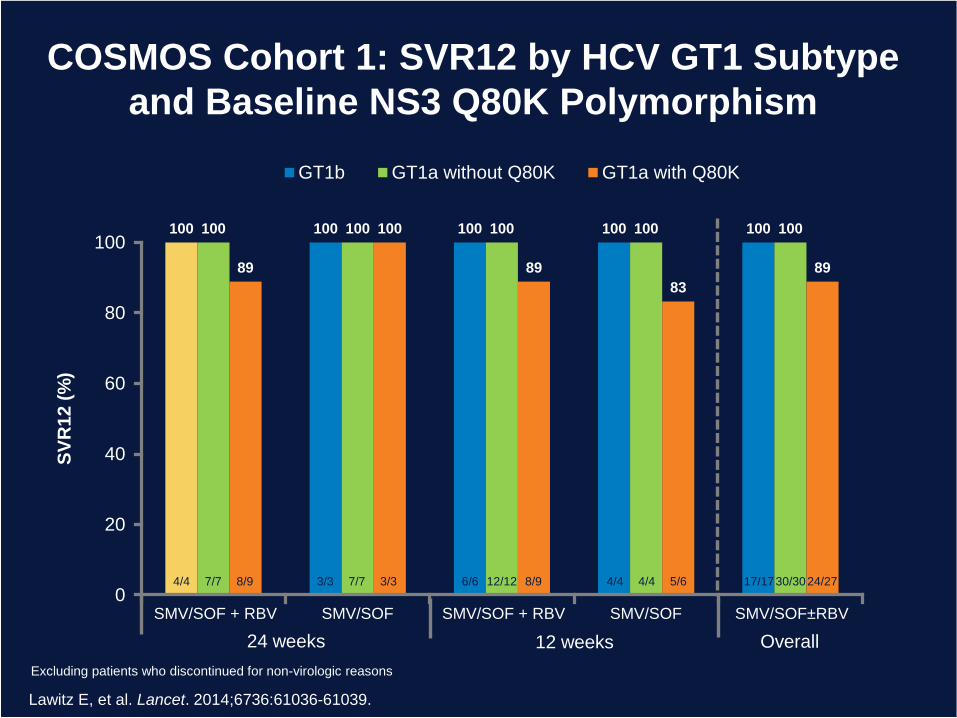
100 100 100 100 100100 100 100 100 100
89
100
89
83
89
0
20
40
60
80
100
GT1b GT1a without Q80K GT1a with Q80K
SMV/SOF±RBV
SV
R1
2 (
%)
SMV/SOF + RBV SMV/SOF + RBVSMV/SOF SMV/SOF
24 weeks 12 weeks Overall
4/4 7/7 8/9 3/3 7/7 3/3 6/6 12/12 8/9 4/4 4/4 5/6 17/1730/3024/27
Excluding patients who discontinued for non-virologic reasons
COSMOS Cohort 1: SVR12 by HCV GT1 Subtype
and Baseline NS3 Q80K Polymorphism
Lawitz E, et al. Lancet. 2014;6736:61036-61039.
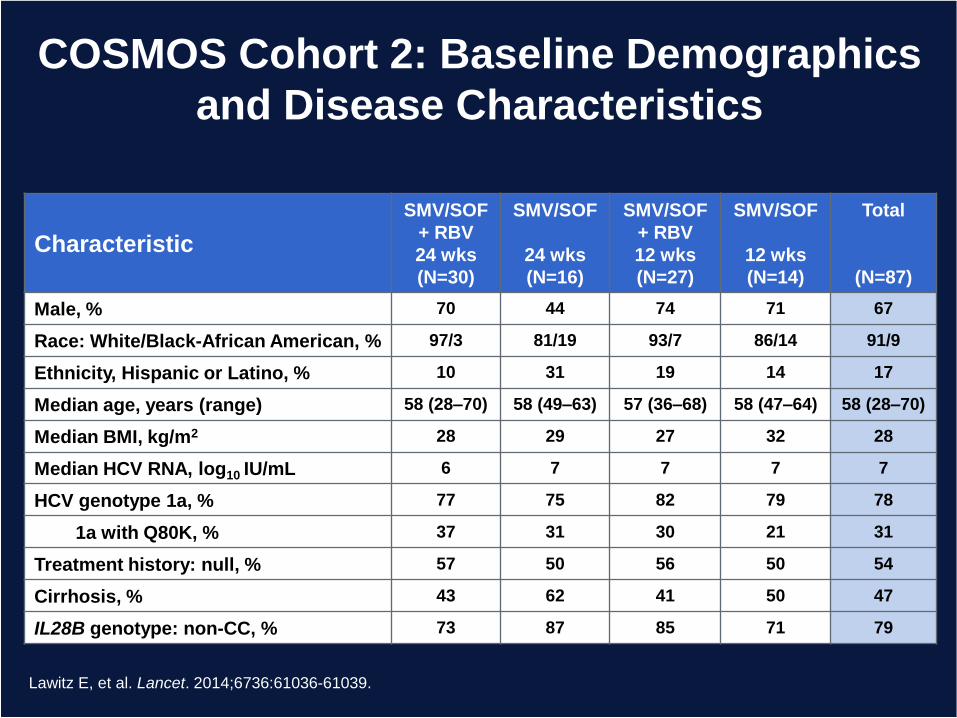
COSMOS Cohort 2: Baseline Demographics
and Disease Characteristics
Characteristic
SMV/SOF
+ RBV
24 wks
(N=30)
SMV/SOF
24 wks
(N=16)
SMV/SOF
+ RBV
12 wks
(N=27)
SMV/SOF
12 wks
(N=14)
Total
(N=87)
Male, % 70 44 74 71 67
Race: White/Black-African American, % 97/3 81/19 93/7 86/14 91/9
Ethnicity, Hispanic or Latino, % 10 31 19 14 17
Median age, years (range) 58 (28–70) 58 (49–63) 57 (36–68) 58 (47–64) 58 (28–70)
Median BMI, kg/m2 28 29 27 32 28
Median HCV RNA, log10 IU/mL 6 7 7 7 7
HCV genotype 1a, % 77 75 82 79 78
1a with Q80K, % 37 31 30 21 31
Treatment history: null, % 57 50 56 50 54
Cirrhosis, % 43 62 41 50 47
IL28B genotype: non-CC, % 73 87 85 71 79
Lawitz E, et al. Lancet. 2014;6736:61036-61039.
GT 1b
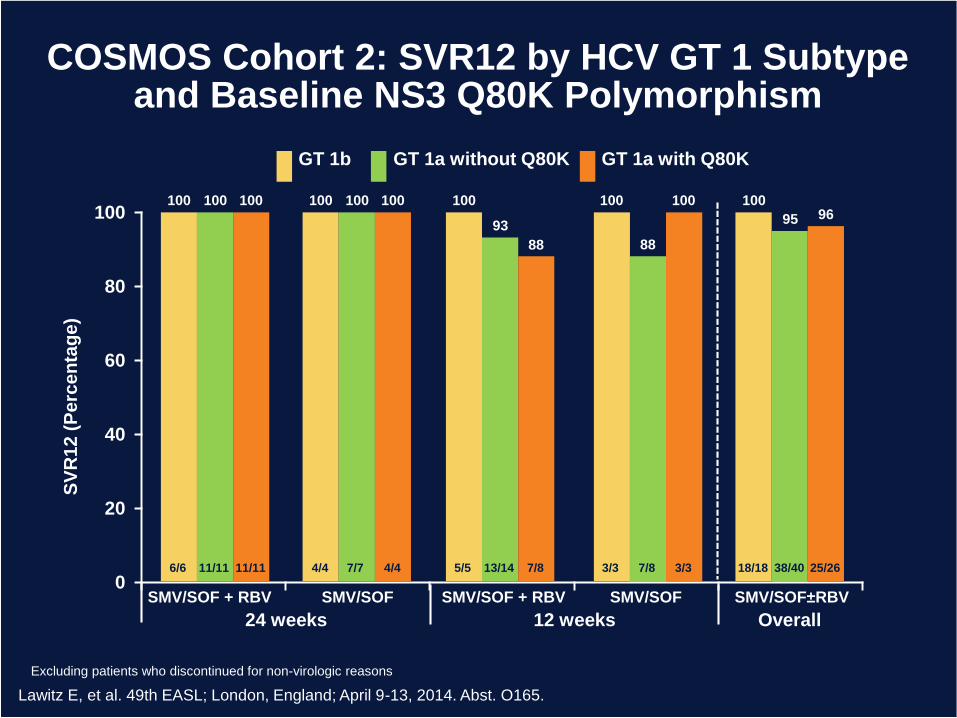
COSMOS Cohort 2: SVR12 by HCV GT 1 Subtype and Baseline NS3 Q80K Polymorphism
0
20
40
60
80
100
SMV/SOF±RBVSMV/SOF + RBV SMV/SOF + RBVSMV/SOF SMV/SOF
24 weeks 12 weeks Overall
Lawitz E, et al. 49th EASL; London, England; April 9-13, 2014. Abst. O165.
SV
R1
2 (
Pe
rce
nta
ge
)
GT 1a without Q80K
100 100
93
88
95
GT 1a with Q80K
100 100
88
10096
6/6 11/11 11/11 4/4 7/7 4/4 5/5 13/14 7/8 3/3 7/8 3/3 18/18 38/40 25/26
100 100 100 100 100
Excluding patients who discontinued for non-virologic reasons
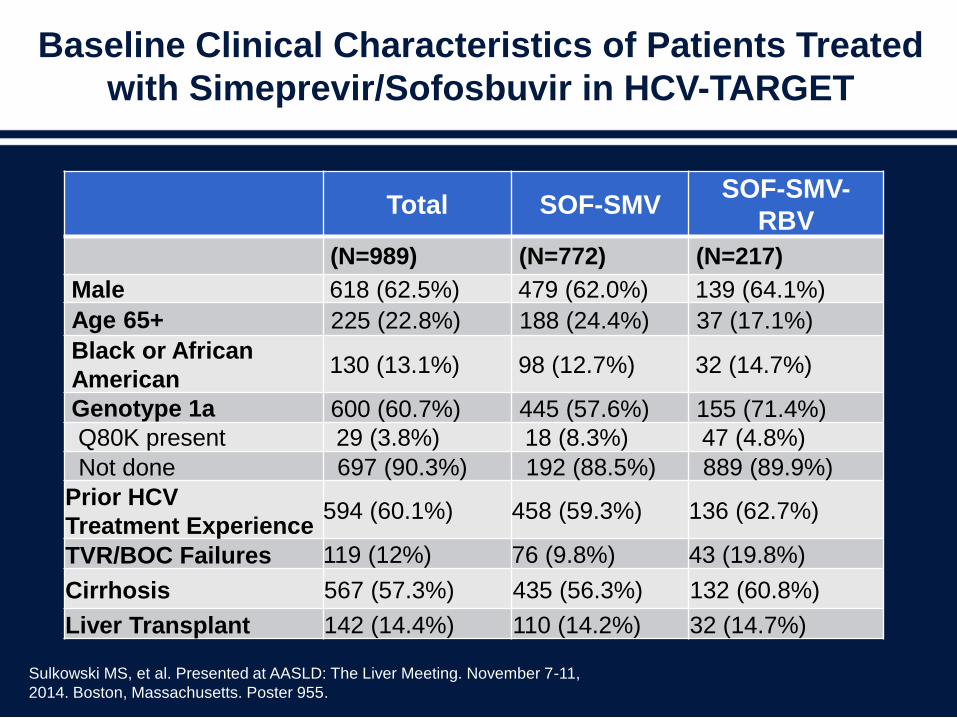
Baseline Clinical Characteristics of Patients Treated
with Simeprevir/Sofosbuvir in HCV-TARGET
Sulkowski MS, et al. Presented at AASLD: The Liver Meeting. November 7-11,
2014. Boston, Massachusetts. Poster 955.
Total SOF-SMVSOF-SMV-
RBV
(N=989) (N=772) (N=217)
Male 618 (62.5%) 479 (62.0%) 139 (64.1%)
Age 65+ 225 (22.8%) 188 (24.4%) 37 (17.1%)
Black or African
American130 (13.1%) 98 (12.7%) 32 (14.7%)
Genotype 1a 600 (60.7%) 445 (57.6%) 155 (71.4%)
Q80K present 29 (3.8%) 18 (8.3%) 47 (4.8%)
Not done 697 (90.3%) 192 (88.5%) 889 (89.9%)
Prior HCV
Treatment Experience594 (60.1%) 458 (59.3%) 136 (62.7%)
TVR/BOC Failures 119 (12%) 76 (9.8%) 43 (19.8%)
Cirrhosis 567 (57.3%) 435 (56.3%) 132 (60.8%)
Liver Transplant 142 (14.4%) 110 (14.2%) 32 (14.7%)
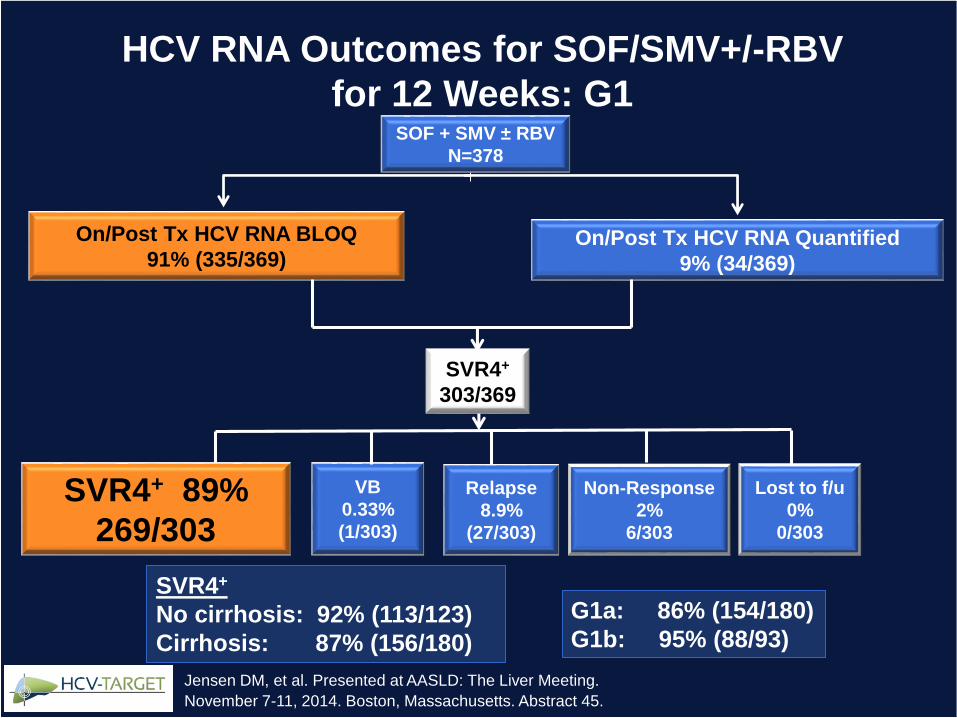
SOF + SMV ± RBV
N=378
On/Post Tx HCV RNA BLOQ
91% (335/369)On/Post Tx HCV RNA Quantified
9% (34/369)
VB
0.33%
(1/303)
Relapse
8.9%
(27/303)
SVR4+
303/369
SVR4+ 89%
269/303
Non-Response
2%
6/303
SVR4+
No cirrhosis: 92% (113/123)
Cirrhosis: 87% (156/180)
G1a: 86% (154/180)
G1b: 95% (88/93)
Lost to f/u
0%
0/303
HCV RNA Outcomes for SOF/SMV+/-RBV
for 12 Weeks: G1
Jensen DM, et al. Presented at AASLD: The Liver Meeting.
November 7-11, 2014. Boston, Massachusetts. Abstract 45.
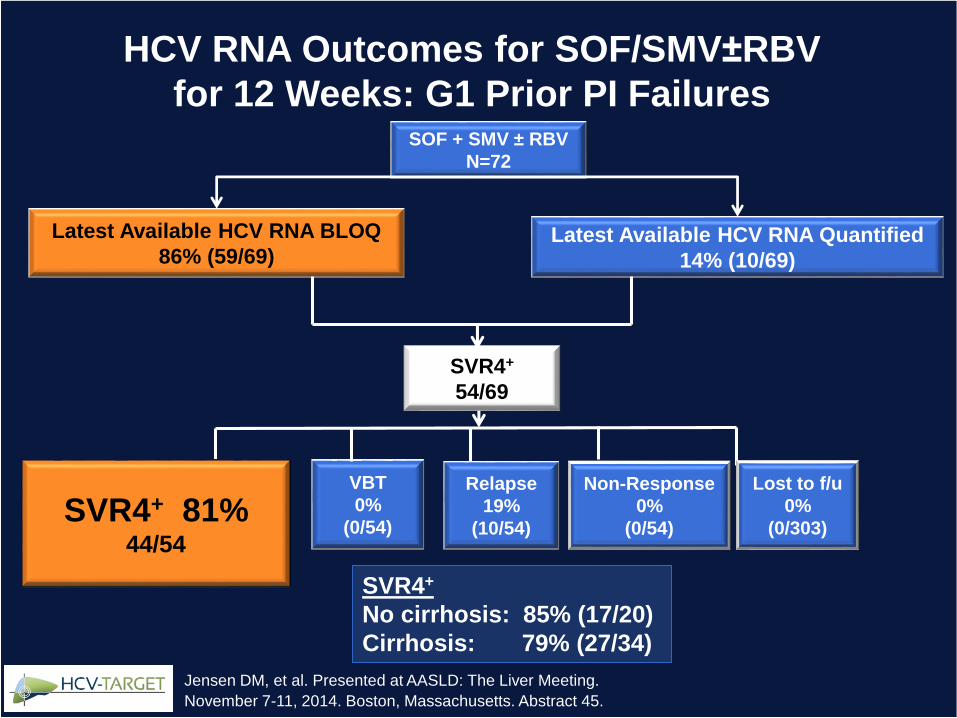
SOF + SMV ± RBV
N=72
Latest Available HCV RNA BLOQ
86% (59/69)Latest Available HCV RNA Quantified
14% (10/69)
VBT
0%
(0/54)
Relapse
19%
(10/54)
SVR4+
54/69
SVR4+ 81%44/54
Non-Response
0%
(0/54)
SVR4+
No cirrhosis: 85% (17/20)
Cirrhosis: 79% (27/34)
Lost to f/u
0%
(0/303)
Jensen DM, et al. Presented at AASLD: The Liver Meeting.
November 7-11, 2014. Boston, Massachusetts. Abstract 45.
HCV RNA Outcomes for SOF/SMV±RBV
for 12 Weeks: G1 Prior PI Failures
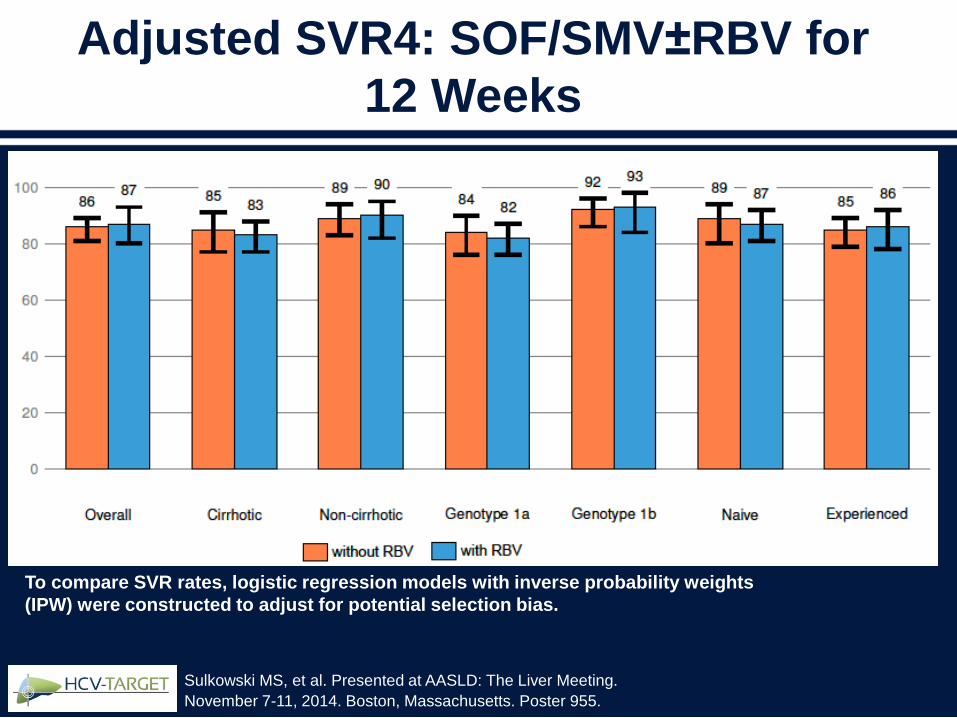
To compare SVR rates, logistic regression models with inverse probability weights
(IPW) were constructed to adjust for potential selection bias.
Adjusted SVR4: SOF/SMV±RBV for
12 Weeks
Sulkowski MS, et al. Presented at AASLD: The Liver Meeting.
November 7-11, 2014. Boston, Massachusetts. Poster 955.
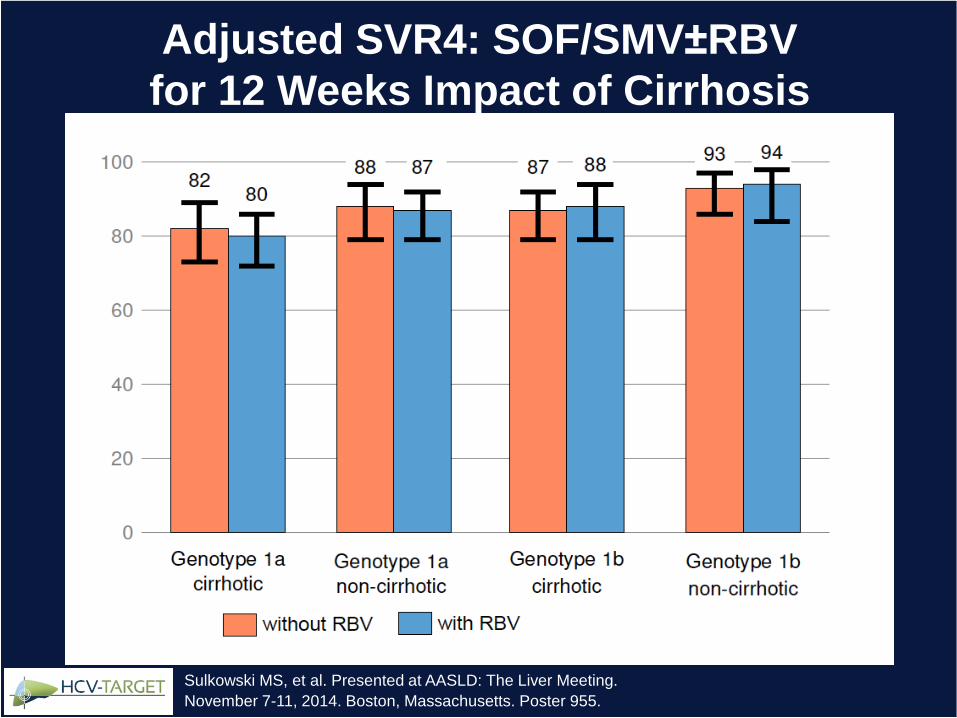
Sulkowski MS, et al. Presented at AASLD: The Liver Meeting.
November 7-11, 2014. Boston, Massachusetts. Poster 955.
Adjusted SVR4: SOF/SMV±RBV
for 12 Weeks Impact of Cirrhosis
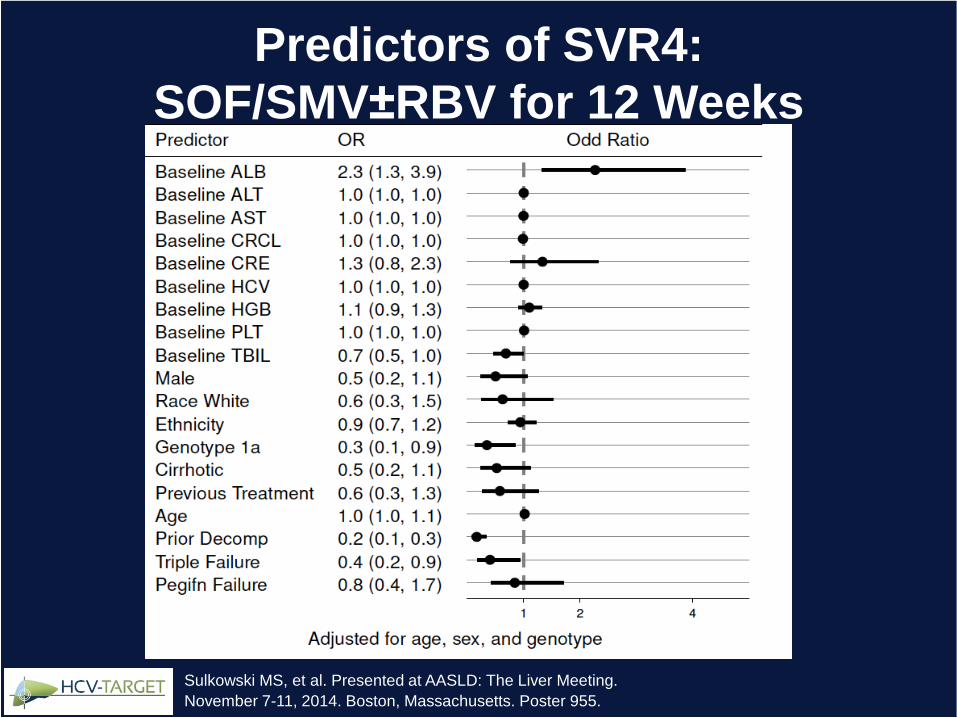
Predictors of SVR4:
SOF/SMV±RBV for 12 Weeks
Sulkowski MS, et al. Presented at AASLD: The Liver Meeting.
November 7-11, 2014. Boston, Massachusetts. Poster 955.
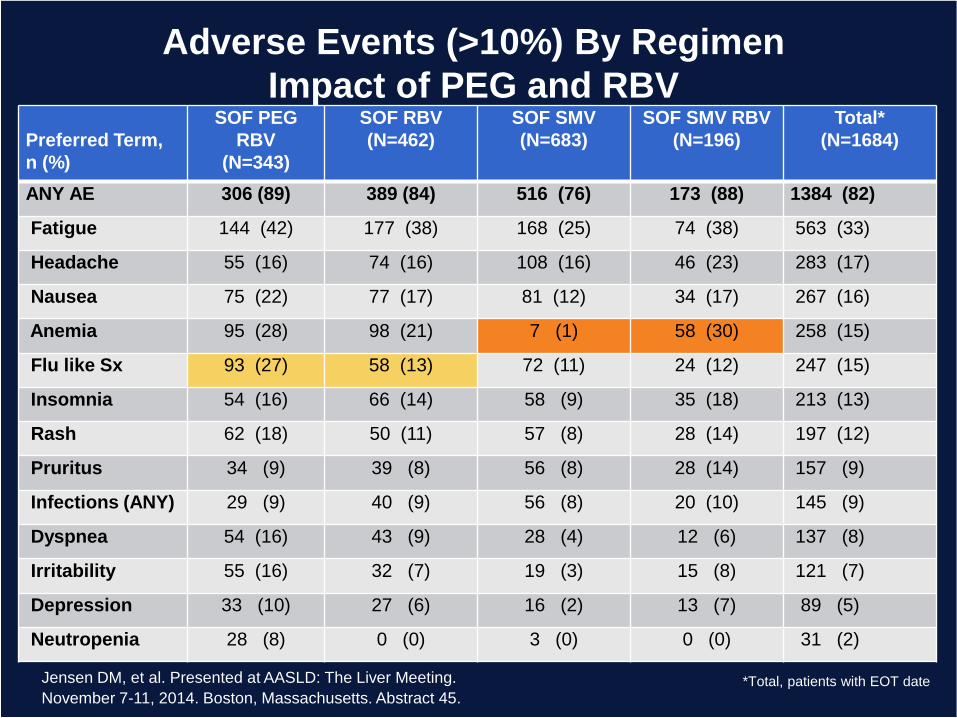
Adverse Events (>10%) By Regimen
Impact of PEG and RBV
*Total, patients with EOT date
Preferred Term,
n (%)
SOF PEG
RBV
(N=343)
SOF RBV
(N=462)
SOF SMV
(N=683)
SOF SMV RBV
(N=196)
Total*
(N=1684)
ANY AE 306 (89) 389 (84) 516 (76) 173 (88) 1384 (82)
Fatigue 144 (42) 177 (38) 168 (25) 74 (38) 563 (33)
Headache 55 (16) 74 (16) 108 (16) 46 (23) 283 (17)
Nausea 75 (22) 77 (17) 81 (12) 34 (17) 267 (16)
Anemia 95 (28) 98 (21) 7 (1) 58 (30) 258 (15)
Flu like Sx 93 (27) 58 (13) 72 (11) 24 (12) 247 (15)
Insomnia 54 (16) 66 (14) 58 (9) 35 (18) 213 (13)
Rash 62 (18) 50 (11) 57 (8) 28 (14) 197 (12)
Pruritus 34 (9) 39 (8) 56 (8) 28 (14) 157 (9)
Infections (ANY) 29 (9) 40 (9) 56 (8) 20 (10) 145 (9)
Dyspnea 54 (16) 43 (9) 28 (4) 12 (6) 137 (8)
Irritability 55 (16) 32 (7) 19 (3) 15 (8) 121 (7)
Depression 33 (10) 27 (6) 16 (2) 13 (7) 89 (5)
Neutropenia 28 (8) 0 (0) 3 (0) 0 (0) 31 (2)
Jensen DM, et al. Presented at AASLD: The Liver Meeting.
November 7-11, 2014. Boston, Massachusetts. Abstract 45.
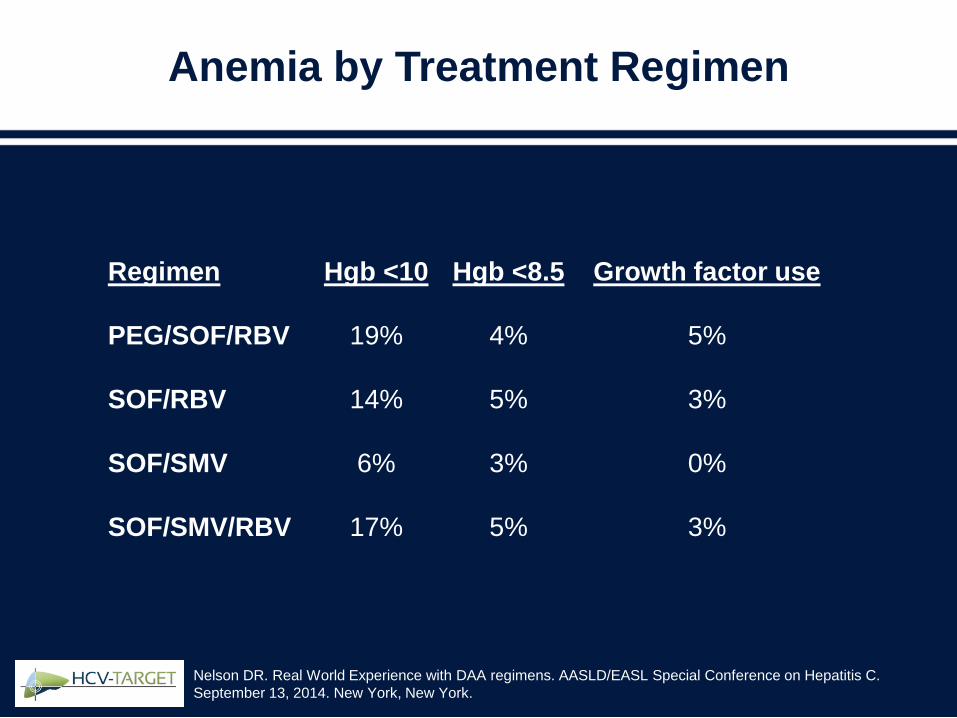
Anemia by Treatment Regimen
Regimen
PEG/SOF/RBV
SOF/RBV
SOF/SMV
SOF/SMV/RBV
Hgb <8.5
4%
5%
3%
5%
Growth factor use
5%
3%
0%
3%
Hgb <10
19%
14%
6%
17%
Nelson DR. Real World Experience with DAA regimens. AASLD/EASL Special Conference on Hepatitis C.
September 13, 2014. New York, New York.
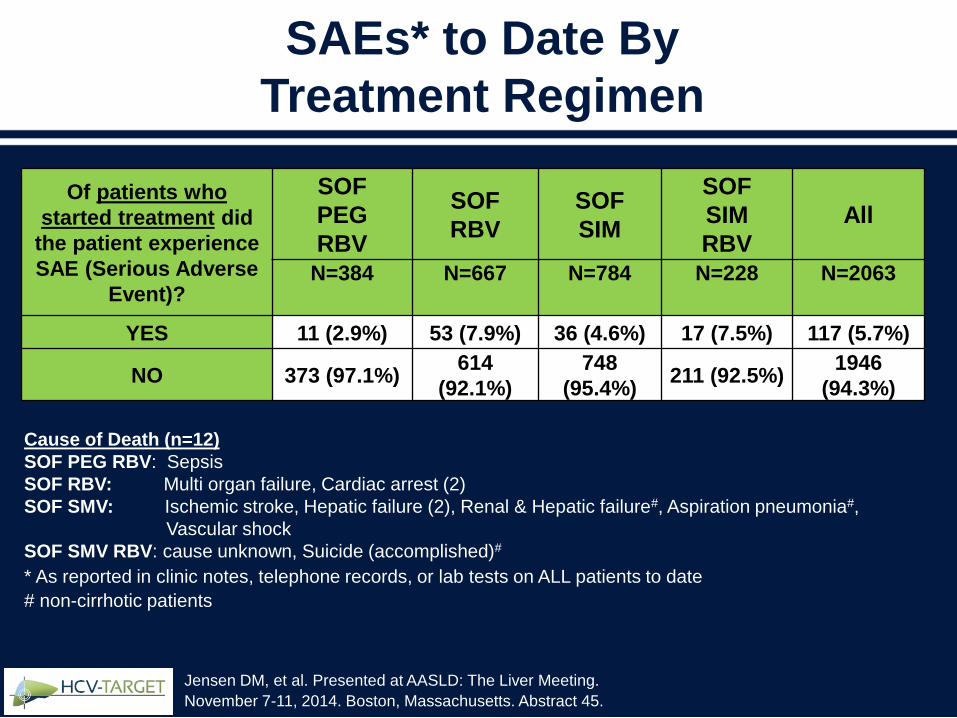
Of patients who
started treatment did
the patient experience
SAE (Serious Adverse
Event)?
SOF
PEG
RBV
SOF
RBV
SOF
SIM
SOF
SIM
RBV
All
N=384 N=667 N=784 N=228 N=2063
YES 11 (2.9%) 53 (7.9%) 36 (4.6%) 17 (7.5%) 117 (5.7%)
NO 373 (97.1%)614
(92.1%)
748
(95.4%)211 (92.5%)
1946
(94.3%)
Cause of Death (n=12)
SOF PEG RBV: Sepsis
SOF RBV: Multi organ failure, Cardiac arrest (2)
SOF SMV: Ischemic stroke, Hepatic failure (2), Renal & Hepatic failure#, Aspiration pneumonia#,
Vascular shock
SOF SMV RBV: cause unknown, Suicide (accomplished)#
* As reported in clinic notes, telephone records, or lab tests on ALL patients to date
# non-cirrhotic patients
SAEs* to Date By
Treatment Regimen
Jensen DM, et al. Presented at AASLD: The Liver Meeting.
November 7-11, 2014. Boston, Massachusetts. Abstract 45.
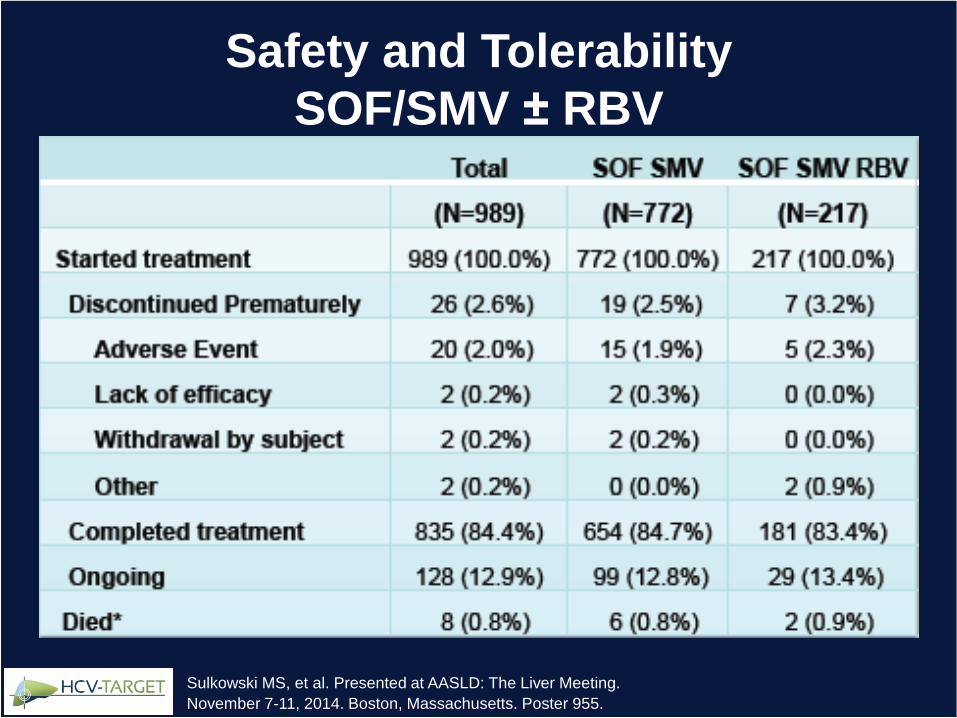
Safety and Tolerability
SOF/SMV ± RBV
Sulkowski MS, et al. Presented at AASLD: The Liver Meeting.
November 7-11, 2014. Boston, Massachusetts. Poster 955.
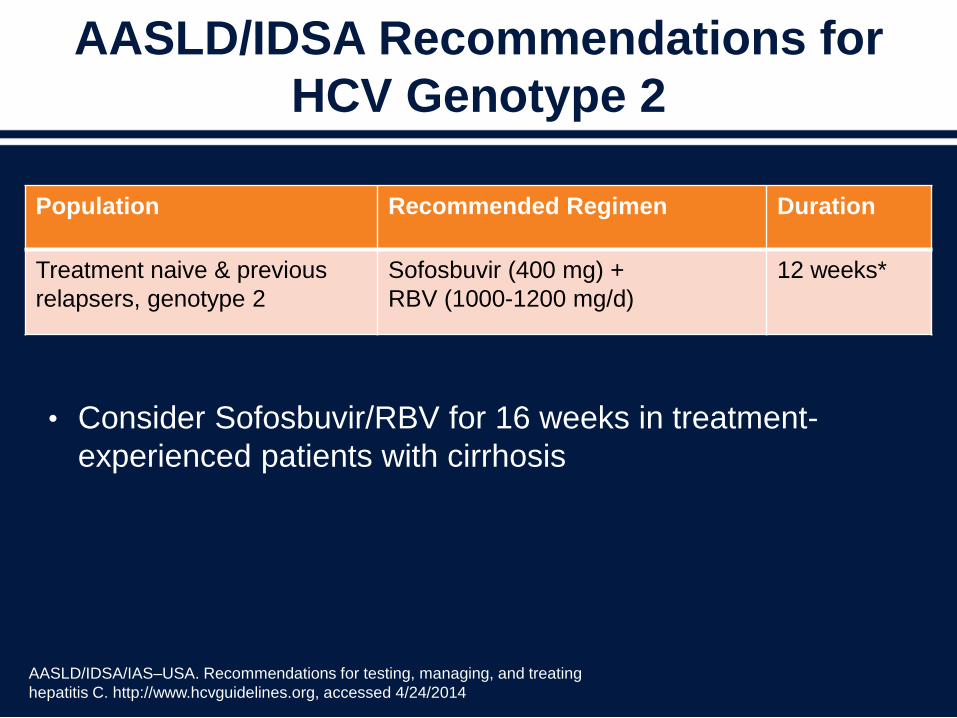
AASLD/IDSA Recommendations for
HCV Genotype 2
AASLD/IDSA/IAS–USA. Recommendations for testing, managing, and treating
hepatitis C. http://www.hcvguidelines.org, accessed 4/24/2014
• Consider Sofosbuvir/RBV for 16 weeks in treatment-
experienced patients with cirrhosis
Population Recommended Regimen Duration
Treatment naive & previous
relapsers, genotype 2
Sofosbuvir (400 mg) +
RBV (1000-1200 mg/d)
12 weeks*
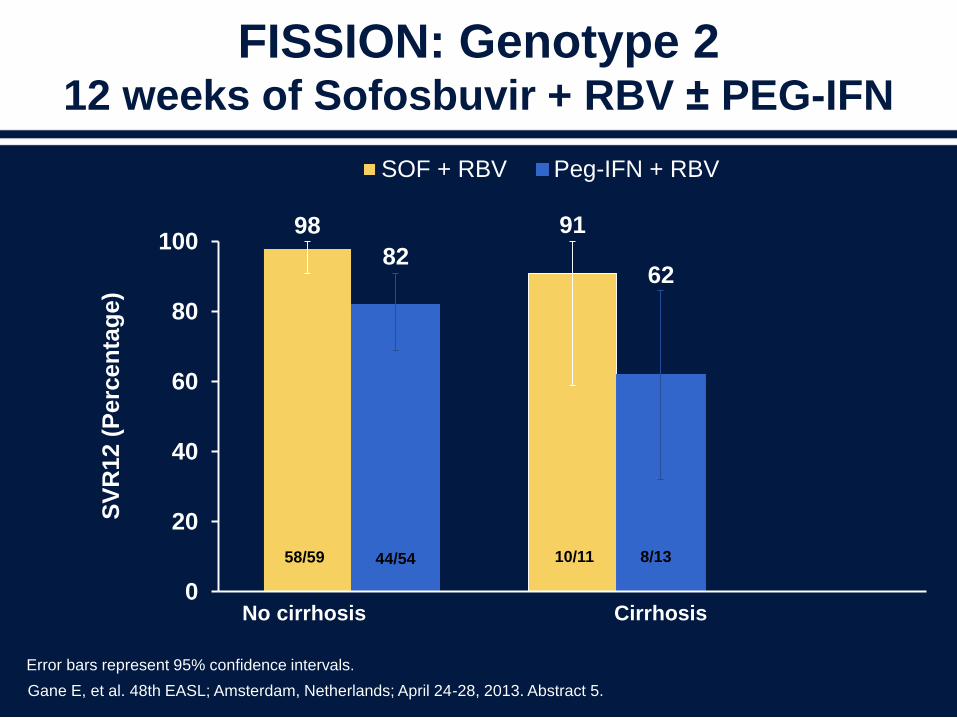
98
82
91
62
0
20
40
60
80
100
SOF + RBV Peg-IFN + RBV
SV
R12 (
Perc
en
tag
e)
No cirrhosis Cirrhosis
FISSION: Genotype 212 weeks of Sofosbuvir + RBV ± PEG-IFN
58/59 44/54 10/11 8/13
Gane E, et al. 48th EASL; Amsterdam, Netherlands; April 24-28, 2013. Abstract 5.
Error bars represent 95% confidence intervals.
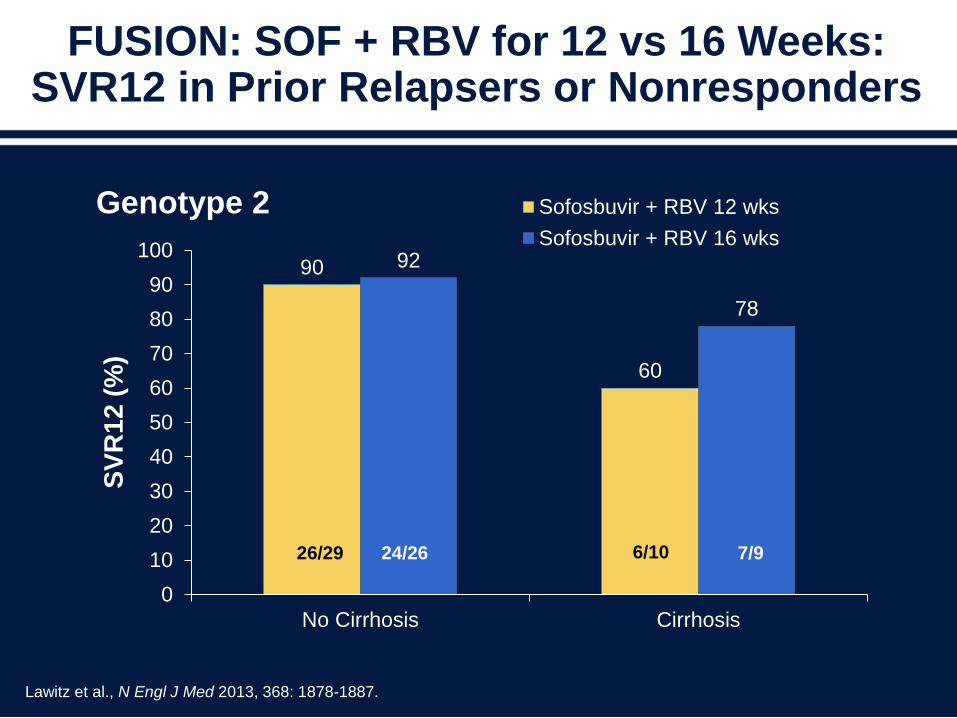
FUSION: SOF + RBV for 12 vs 16 Weeks: SVR12 in Prior Relapsers or Nonresponders
90
60
92
78
0
10
20
30
40
50
60
70
80
90
100
No Cirrhosis Cirrhosis
SV
R1
2 (
%)
Genotype 2 Sofosbuvir + RBV 12 wks
Sofosbuvir + RBV 16 wks
6/1026/29 7/924/26
Lawitz et al., N Engl J Med 2013, 368: 1878-1887.
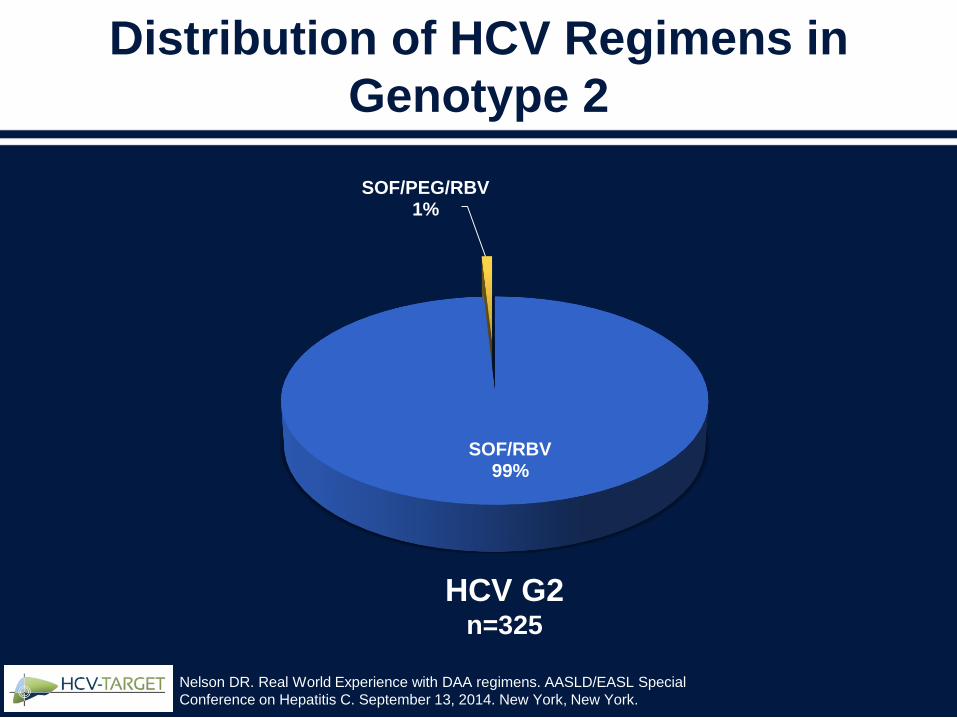
Distribution of HCV Regimens in
Genotype 2
SOF/RBV99%
SOF/PEG/RBV1%
HCV G2n=325
Nelson DR. Real World Experience with DAA regimens. AASLD/EASL Special
Conference on Hepatitis C. September 13, 2014. New York, New York.
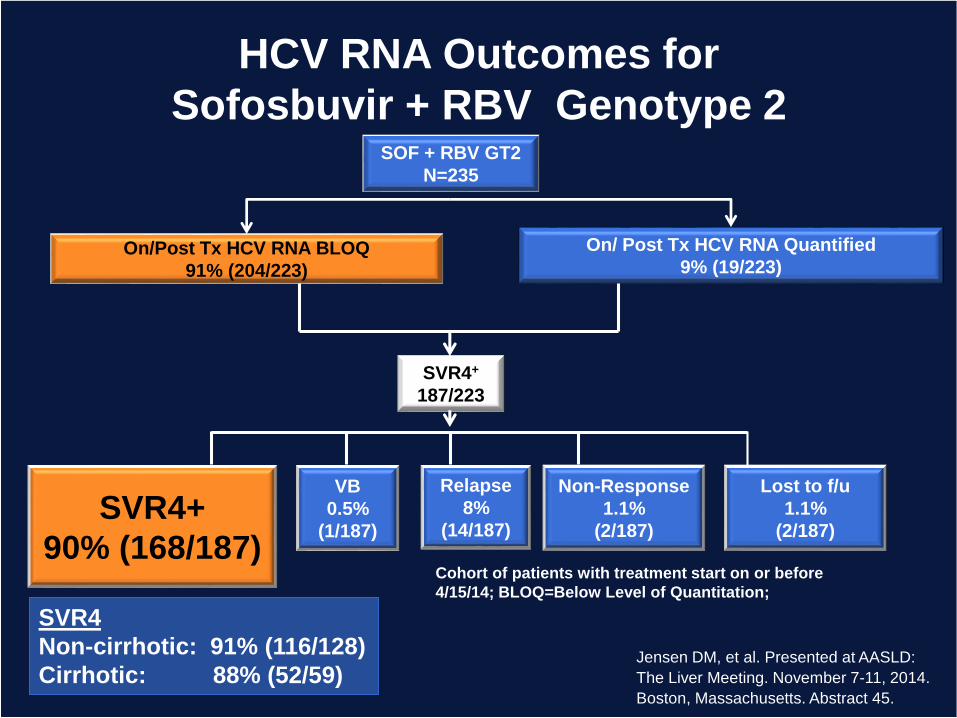
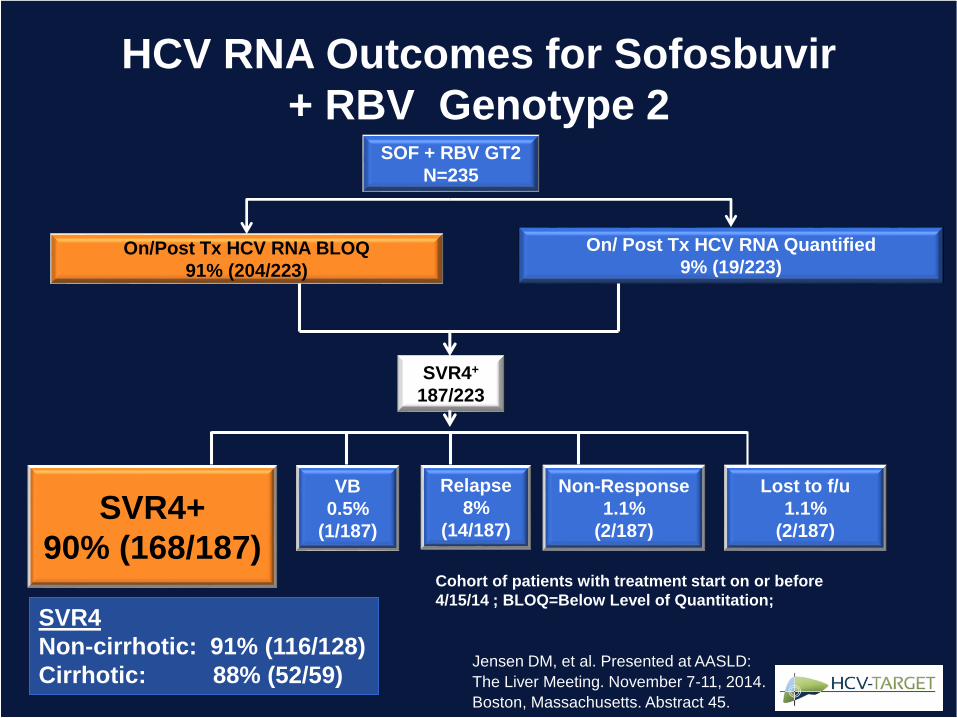
SOF + RBV GT2
N=235
On/Post Tx HCV RNA BLOQ
91% (204/223)
On/ Post Tx HCV RNA Quantified
9% (19/223)
Cohort of patients with treatment start on or before
4/15/14; BLOQ=Below Level of Quantitation;
VB
0.5%
(1/187)
Relapse
8%
(14/187)
SVR4+
187/223
SVR4+
90% (168/187)
Non-Response
1.1%
(2/187)
SVR4
Non-cirrhotic: 91% (116/128)
Cirrhotic: 88% (52/59)
Lost to f/u
1.1%
(2/187)
HCV RNA Outcomes for
Sofosbuvir + RBV Genotype 2
Jensen DM, et al. Presented at AASLD:
The Liver Meeting. November 7-11, 2014.
Boston, Massachusetts. Abstract 45.
HCV-TARGET
What Have We Learned So Far?
• HCV-TARGET is an ongoing study characterizing the use of
DAAs across a broad spectrum of clinical practices in North
America and Europe
• High percentage of “off-label” use of sofosbuvir and simeprevir
• Efficacy– Real-world data for new DAA regimens consistent with phase 2-3 trial
data to date…. Patients treated with SOF/Ledipasvir are currently being enrolled
• Viral issues:– Very low viral breakthrough rates
– Resistance testing is rarely obtained in clinical care
• Safety– Very low discontinuation and SAE rates
– AEs of all oral regimens much lower than those with PEG Lowest in RBV-free regimens
Jensen DM, et al. Presented at AASLD: The Liver Meeting.
November 7-11, 2014. Boston, Massachusetts. Abstract 45.
Real-World Outcomes:
Special Populations and
Management Issues
Nancy Reau, MD
Associate Professor of Medicine
University of Chicago School of Medicine
Chicago, IL
Objectives
• Evaluate efficacy in G1 populations
underrepresented in phase 3 clinical trials
– Cirrhosis
– African Americans
– Older age >65 years
– Posttransplant
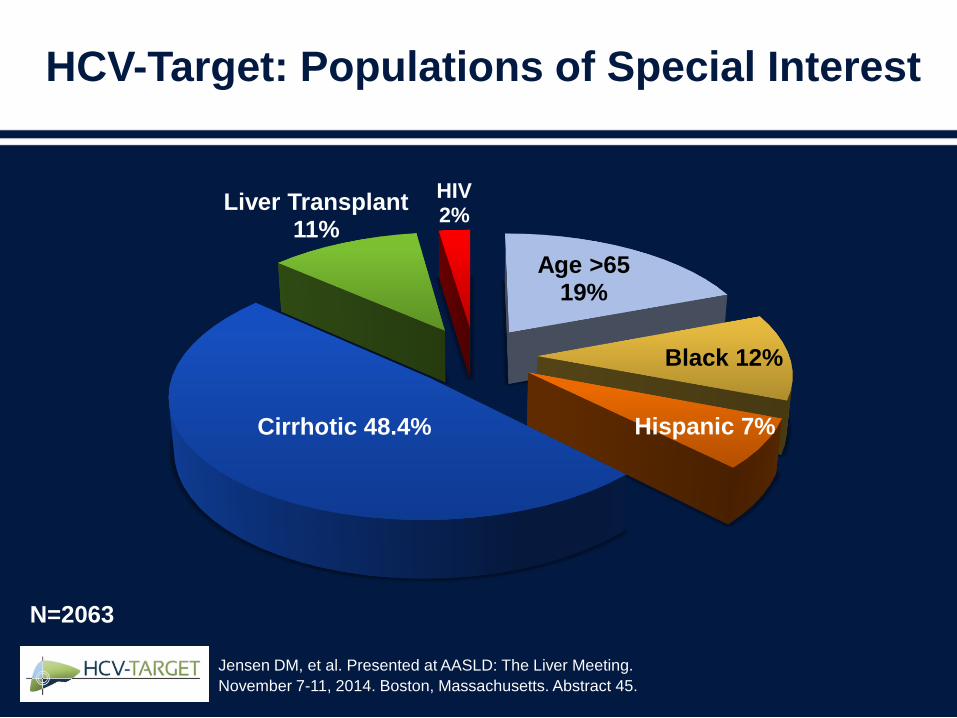
HCV-Target: Populations of Special Interest
Jensen DM, et al. Presented at AASLD: The Liver Meeting.
November 7-11, 2014. Boston, Massachusetts. Abstract 45.
Age >6519%
Black 12%
Hispanic 7%Cirrhotic 48.4%
Liver Transplant11%
HIV2%
N=2063
Underrepresented Populations
• Cirrhosis
• African Americans
• Age >65
• Transplant
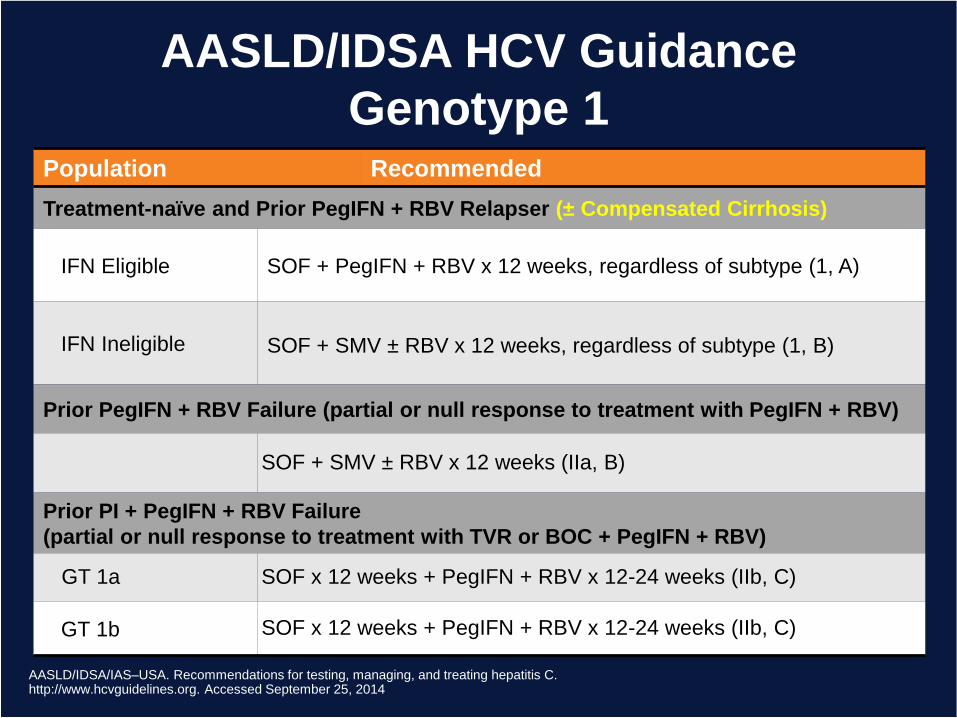
AASLD/IDSA HCV Guidance
Genotype 1
AASLD/IDSA/IAS–USA. Recommendations for testing, managing, and treating hepatitis C.http://www.hcvguidelines.org. Accessed September 25, 2014
Population Recommended
Treatment-naïve and Prior PegIFN + RBV Relapser (± Compensated Cirrhosis)
IFN Eligible SOF + PegIFN + RBV x 12 weeks, regardless of subtype (1, A)
IFN Ineligible SOF + SMV ± RBV x 12 weeks, regardless of subtype (1, B)
Prior PegIFN + RBV Failure (partial or null response to treatment with PegIFN + RBV)
SOF + SMV ± RBV x 12 weeks (IIa, B)
Prior PI + PegIFN + RBV Failure
(partial or null response to treatment with TVR or BOC + PegIFN + RBV)
GT 1a SOF x 12 weeks + PegIFN + RBV x 12-24 weeks (IIb, C)
GT 1b SOF x 12 weeks + PegIFN + RBV x 12-24 weeks (IIb, C)
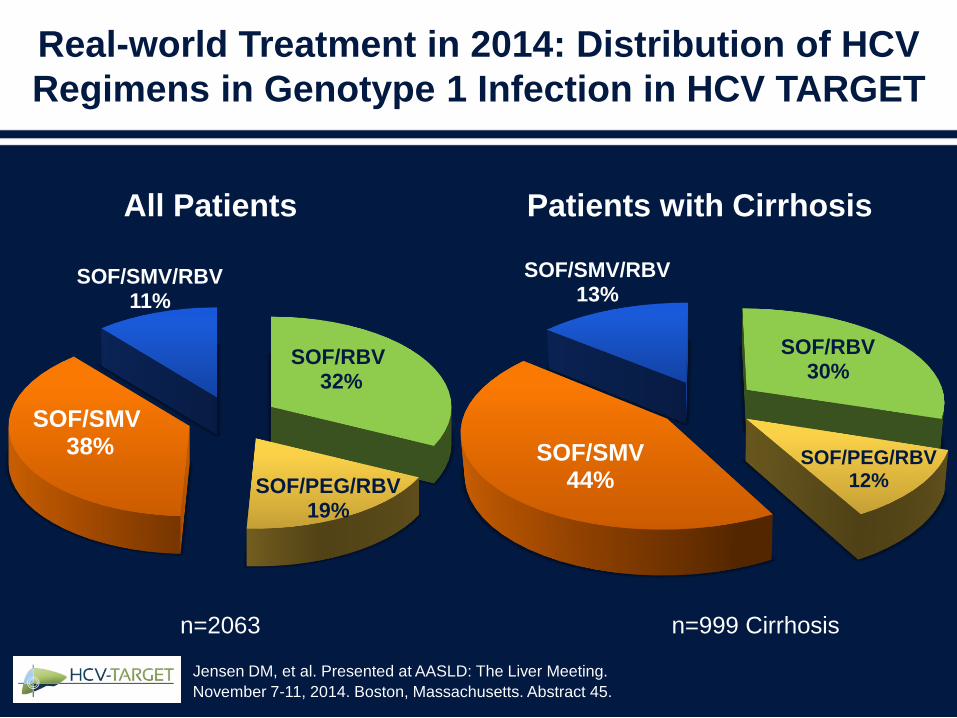
Real-world Treatment in 2014: Distribution of HCV
Regimens in Genotype 1 Infection in HCV TARGET
SOF/RBV32%
SOF/PEG/RBV 19%
SOF/SMV38%
SOF/SMV/RBV 11%
SOF/RBV30%
SOF/PEG/RBV12%
SOF/SMV44%
SOF/SMV/RBV13%
Patients with CirrhosisAll Patients
n=999 Cirrhosisn=2063
Jensen DM, et al. Presented at AASLD: The Liver Meeting.
November 7-11, 2014. Boston, Massachusetts. Abstract 45.

NEUTRINO (PEG+RBV+SOF for 12 weeks):
HCV G1/4 SVR Rates in Selected Subgroups
Lawitz E, et al. N Engl J Med. 2013,368:1878-1887.
9287
71
80
91
0
20
40
60
80
100
Multiple Factors*
SV
R12 (
%)
252/
273
47/
54
248/
27337/
52
43/
54
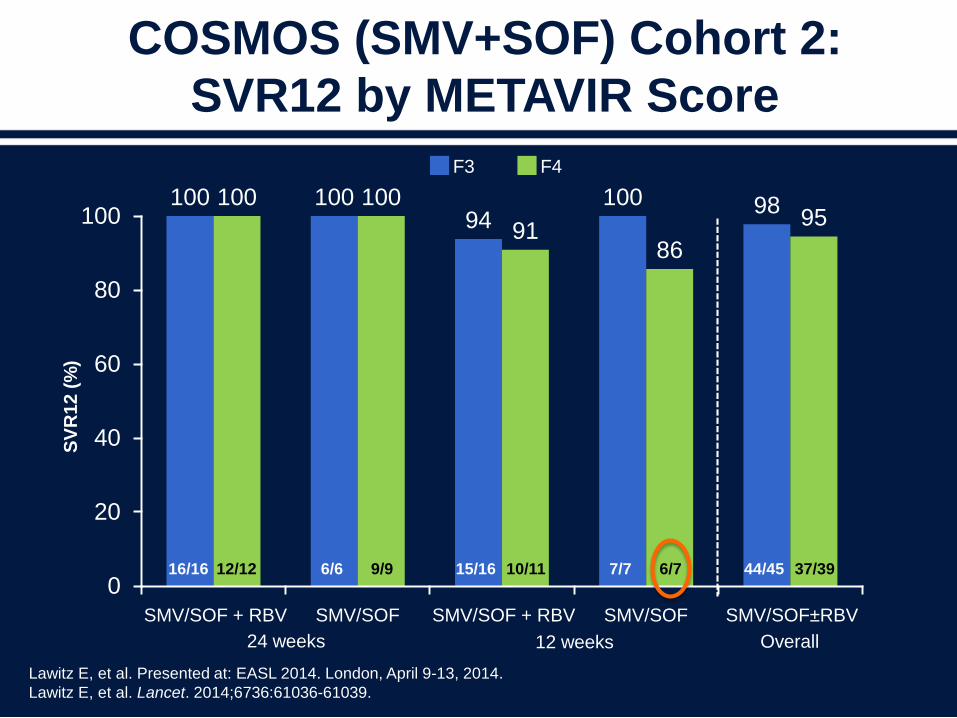
COSMOS (SMV+SOF) Cohort 2:
SVR12 by METAVIR Score
Lawitz E, et al. Presented at: EASL 2014. London, April 9-13, 2014.
Lawitz E, et al. Lancet. 2014;6736:61036-61039.
100 10094
100 98100 100
9186
95
0
20
40
60
80
100
SMV/SOF±RBV
SV
R1
2 (
%)
SMV/SOF + RBV SMV/SOF + RBVSMV/SOF SMV/SOF
24 weeks 12 weeks Overall
16/16 12/12 6/6 9/9 15/16 10/11 7/7 6/7 44/45 37/39
F3 F4
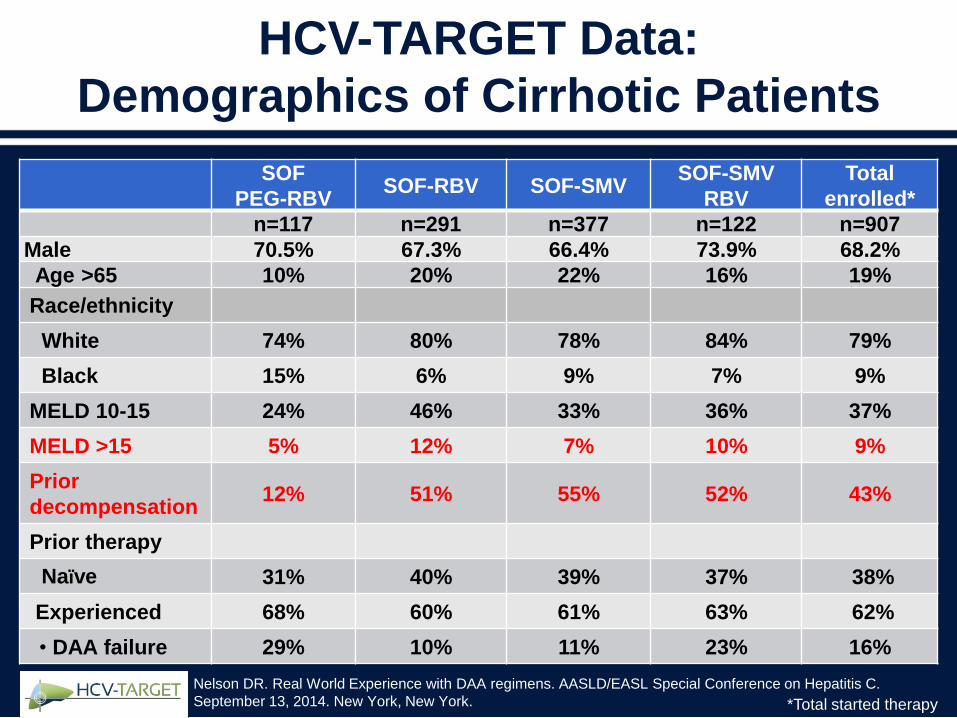
HCV-TARGET Data:
Demographics of Cirrhotic Patients
SOF
PEG-RBVSOF-RBV SOF-SMV
SOF-SMV
RBV
Total
enrolled*
n=117 n=291 n=377 n=122 n=907
Male 70.5% 67.3% 66.4% 73.9% 68.2%
Age >65 10% 20% 22% 16% 19%
Race/ethnicity
White 74% 80% 78% 84% 79%
Black 15% 6% 9% 7% 9%
MELD 10-15 24% 46% 33% 36% 37%
MELD >15 5% 12% 7% 10% 9%
Prior
decompensation12% 51% 55% 52% 43%
Prior therapy
Naïve 31% 40% 39% 37% 38%
Experienced 68% 60% 61% 63% 62%
• DAA failure 29% 10% 11% 23% 16%
*Total started therapy
Nelson DR. Real World Experience with DAA regimens. AASLD/EASL Special Conference on Hepatitis C.
September 13, 2014. New York, New York.
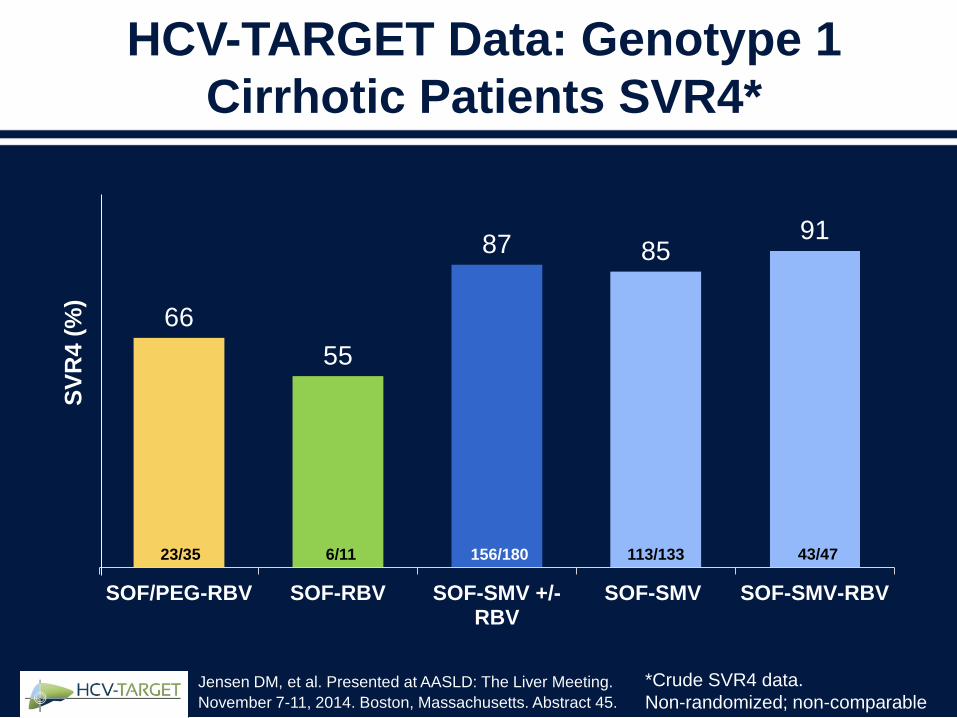
HCV-TARGET Data: Genotype 1
Cirrhotic Patients SVR4*
66
55
87 8591
SOF/PEG-RBV SOF-RBV SOF-SMV +/-RBV
SOF-SMV SOF-SMV-RBV
Jensen DM, et al. Presented at AASLD: The Liver Meeting.
November 7-11, 2014. Boston, Massachusetts. Abstract 45.
SV
R4 (
%)
23/35 6/11 156/180 113/133 43/47
*Crude SVR4 data.
Non-randomized; non-comparable
Underrepresented Populations
• Cirrhosis
• African Americans
• Age >65
• Transplant

NEUTRINO: SVR Rates in
Selected Subgroups
Lawitz E, et al. N Engl J Med. 2013,368:1878-1887.
9287
71
80
91
0
20
40
60
80
100
Multiple Factors
SV
R12 (
%)
252/
273
47/
54
248/
273
37/
52
43/
54
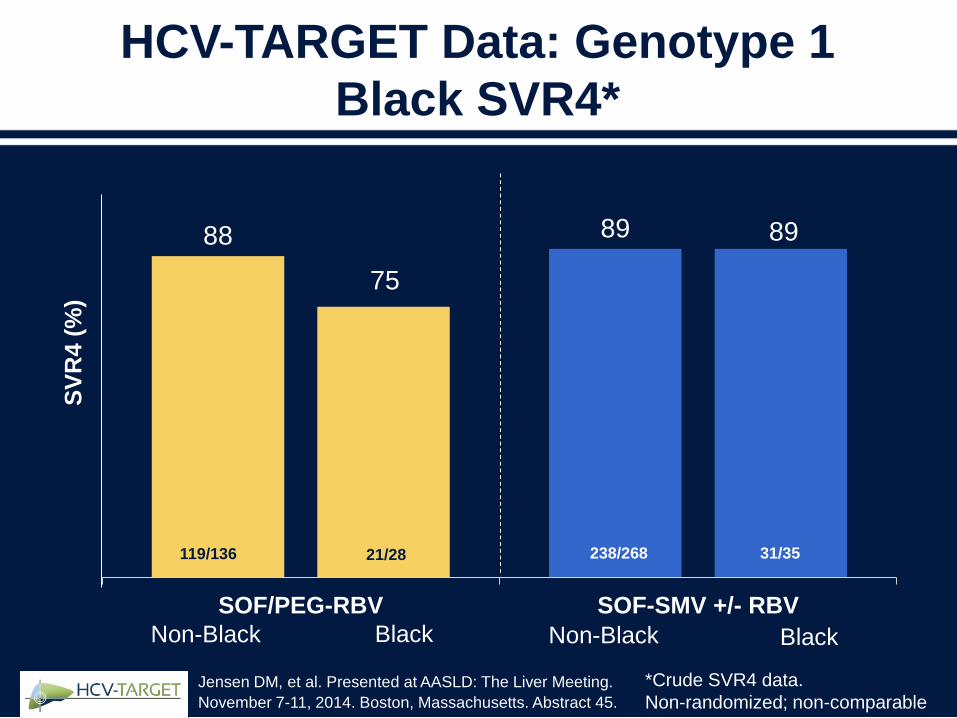
HCV-TARGET Data: Genotype 1
Black SVR4*
Jensen DM, et al. Presented at AASLD: The Liver Meeting.
November 7-11, 2014. Boston, Massachusetts. Abstract 45.
SV
R4 (
%)
BlackNon-Black BlackNon-Black
88 89
SOF/PEG-RBV SOF-SMV +/- RBV
75
119/136 21/28 238/268 31/35
*Crude SVR4 data.
Non-randomized; non-comparable
89
Underrepresented Populations
• Cirrhosis
• African Americans
• Age >65
• Transplant
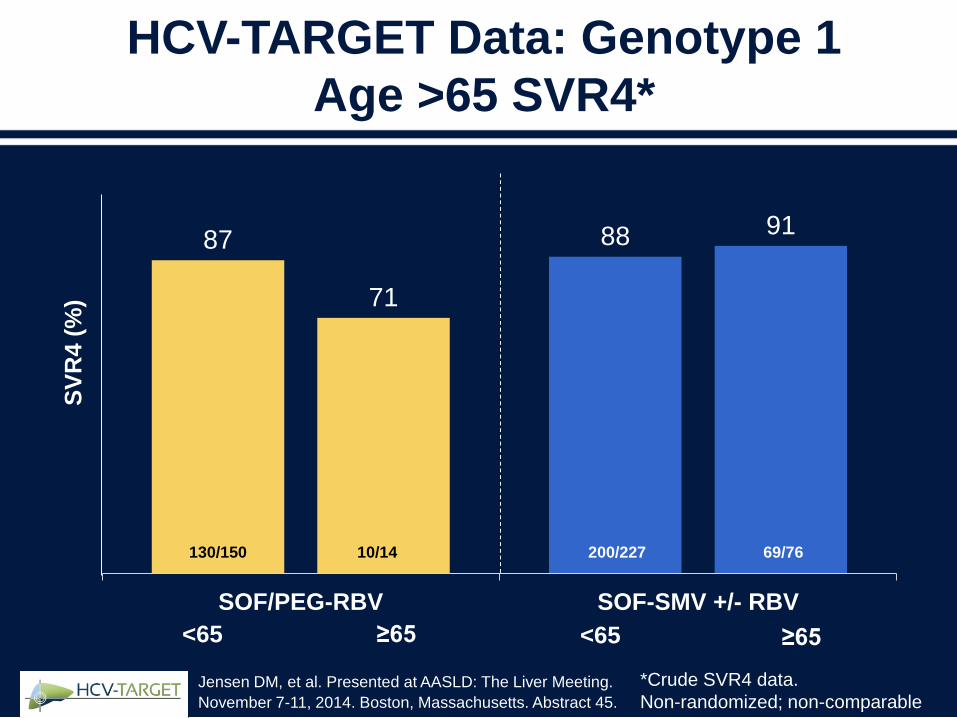
HCV-TARGET Data: Genotype 1
Age >65 SVR4*
Jensen DM, et al. Presented at AASLD: The Liver Meeting.
November 7-11, 2014. Boston, Massachusetts. Abstract 45.
87 88
71
91
SOF/PEG-RBV SOF-SMV +/- RBV
SV
R4 (
%)
130/150 10/14 200/227 69/76
≥65<65 ≥65<65
*Crude SVR4 data.
Non-randomized; non-comparable
Underrepresented Populations
• Cirrhosis
• African Americans
• Age >65
• Transplant
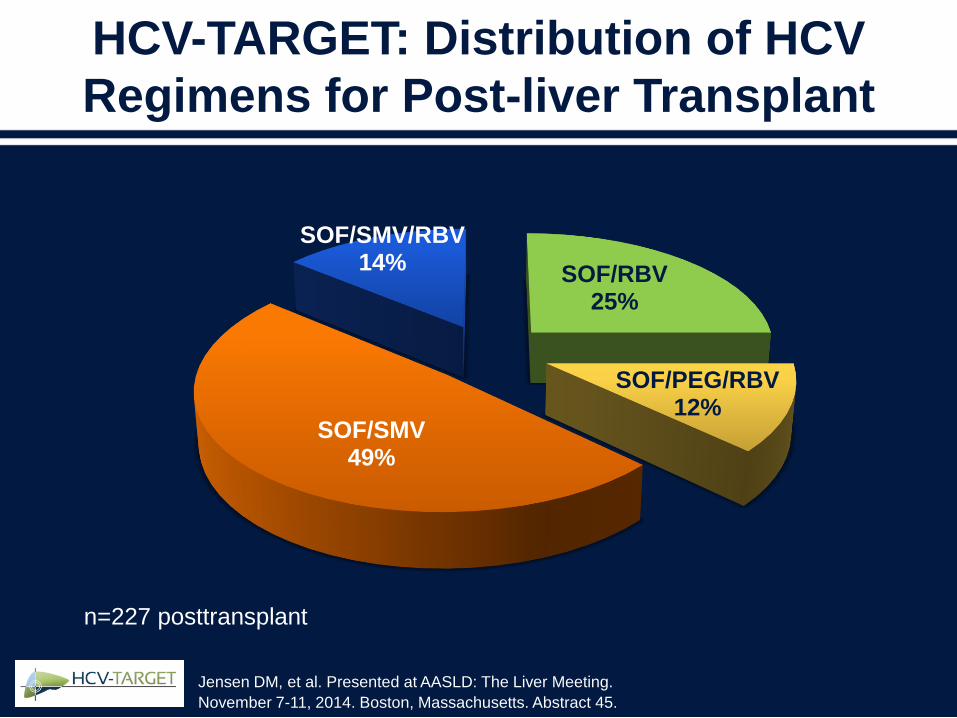
HCV-TARGET: Distribution of HCV
Regimens for Post-liver Transplant
n=227 posttransplant
SOF/RBV25%
SOF/PEG/RBV12%
SOF/SMV49%
SOF/SMV/RBV14%
Jensen DM, et al. Presented at AASLD: The Liver Meeting.
November 7-11, 2014. Boston, Massachusetts. Abstract 45.
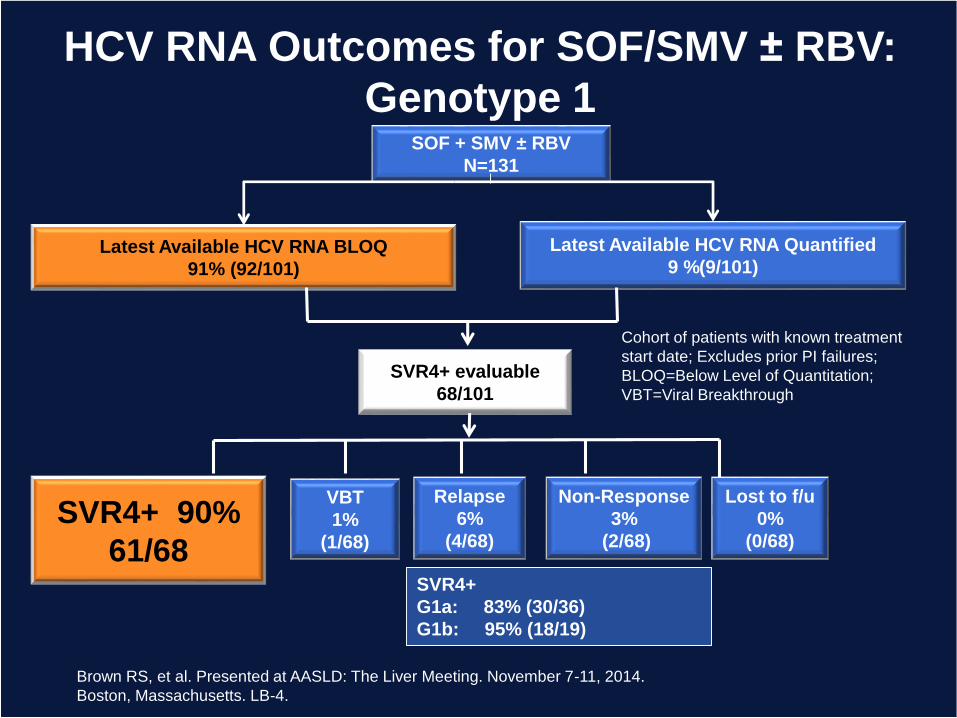
SOF + SMV ± RBV
N=131
Latest Available HCV RNA BLOQ
91% (92/101)
Latest Available HCV RNA Quantified
9 %(9/101)
Cohort of patients with known treatment
start date; Excludes prior PI failures;
BLOQ=Below Level of Quantitation;
VBT=Viral Breakthrough
HCV RNA Outcomes for SOF/SMV ± RBV:
Genotype 1
VBT
1%
(1/68)
Relapse
6%
(4/68)
SVR4+ evaluable
68/101
SVR4+ 90%
61/68
Non-Response
3%
(2/68)
Lost to f/u
0%
(0/68)
SVR4+
G1a: 83% (30/36)
G1b: 95% (18/19)
Brown RS, et al. Presented at AASLD: The Liver Meeting. November 7-11, 2014.
Boston, Massachusetts. LB-4.
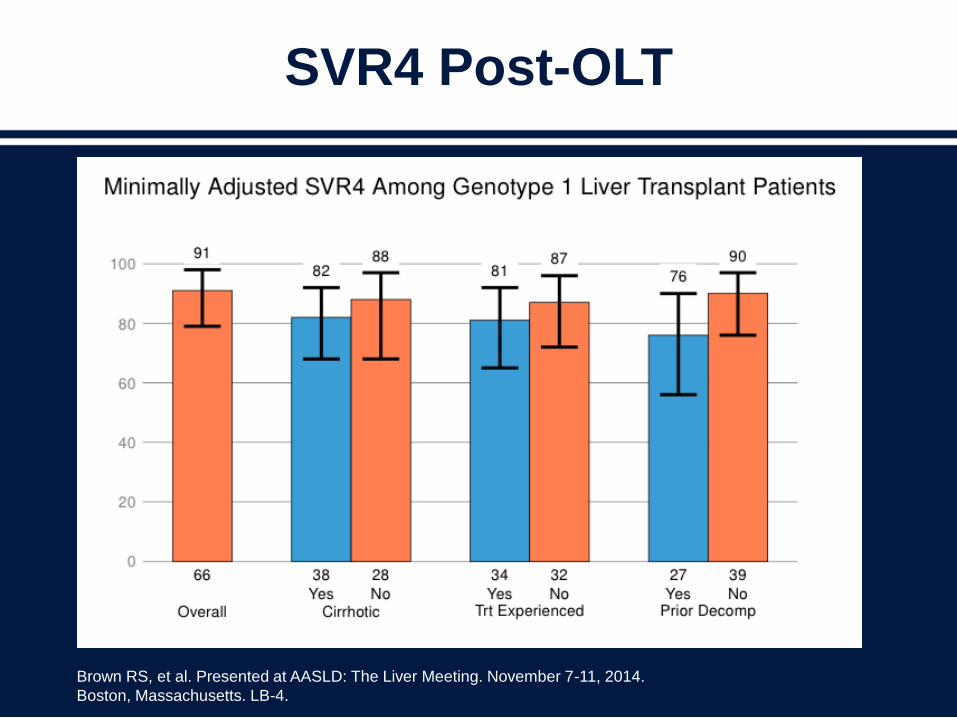
SVR4 Post-OLT
Brown RS, et al. Presented at AASLD: The Liver Meeting. November 7-11, 2014.
Boston, Massachusetts. LB-4.
Conclusions
• Most populations of special interest
received all-oral regimens
• Real-world data approximates clinical trial
data
• Special populations are no longer so
special
Treating Amid New
Guidelines and Options:
How to Decipher and
Apply to Practice
Ira M. Jacobson, MD
Weill Cornell Medical College
New York, New York USA
Many Considerations to Integrate
When Making Therapeutic Decisions
Clinical
judgmentGuidelines(“Guidance”)
Data
from
trials
Package
insert
CostThird
parties
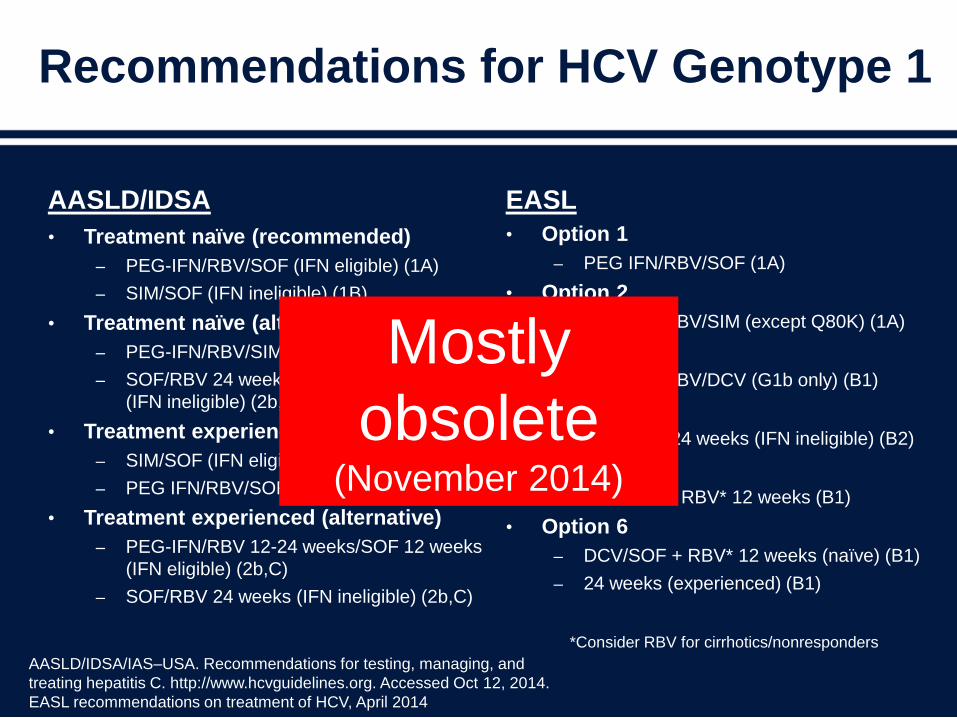
Recommendations for HCV Genotype 1
AASLD/IDSA
• Treatment naïve (recommended)
– PEG-IFN/RBV/SOF (IFN eligible) (1A)
– SIM/SOF (IFN ineligible) (1B)
• Treatment naïve (alternative)
– PEG-IFN/RBV/SIM (except Q80K) (2a, A)
– SOF/RBV 24 weeks
(IFN ineligible) (2b, B)
• Treatment experienced (recommended)
– SIM/SOF (IFN eligible or ineligible)(non-PI)
– PEG IFN/RBV/SOF (IFN eligible)(PI)
• Treatment experienced (alternative)
– PEG-IFN/RBV 12-24 weeks/SOF 12 weeks
(IFN eligible) (2b,C)
– SOF/RBV 24 weeks (IFN ineligible) (2b,C)
EASL
• Option 1
– PEG IFN/RBV/SOF (1A)
• Option 2
– PEG IFN/RBV/SIM (except Q80K) (1A)
• Option 3
– PEG IFN/RBV/DCV (G1b only) (B1)
• Option 4
– SOF/RBV 24 weeks (IFN ineligible) (B2)
• Option 5
– SIM/SOF + RBV* 12 weeks (B1)
• Option 6
– DCV/SOF + RBV* 12 weeks (naïve) (B1)
– 24 weeks (experienced) (B1)
AASLD/IDSA/IAS–USA. Recommendations for testing, managing, and
treating hepatitis C. http://www.hcvguidelines.org. Accessed Oct 12, 2014.
EASL recommendations on treatment of HCV, April 2014
*Consider RBV for cirrhotics/nonresponders
Mostly
obsolete (November 2014)
Proposition
There is no longer a role for interferon in
the treatment of HCV genotype 1.
What about ribavirin?
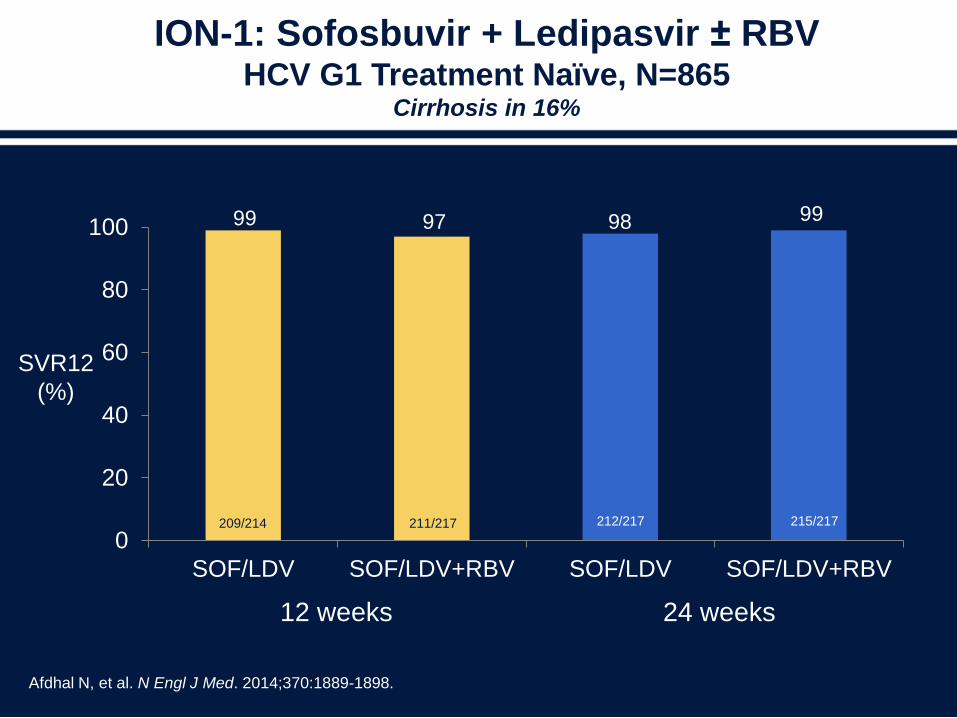
ION-1: Sofosbuvir + Ledipasvir ± RBVHCV G1 Treatment Naïve, N=865
Cirrhosis in 16%
0
20
40
60
80
100
SOF/LDV SOF/LDV+RBV SOF/LDV SOF/LDV+RBV
Afdhal N, et al. N Engl J Med. 2014;370:1889-1898.
12 weeks 24 weeks
SVR12
(%)
209/214 211/217 212/217 215/217
99 97 98 99
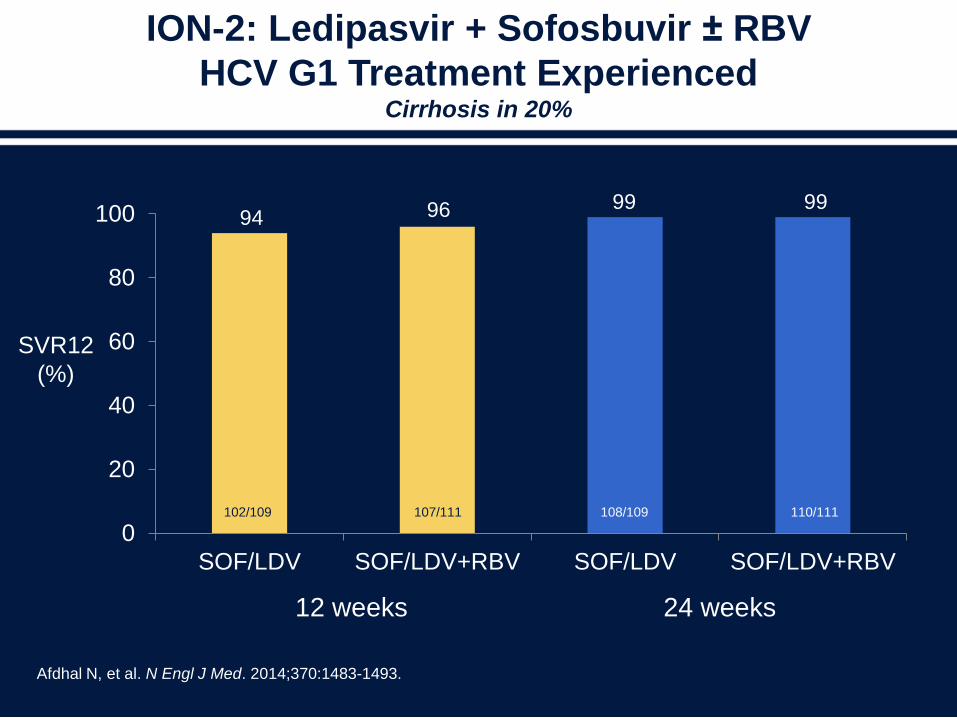
ION-2: Ledipasvir + Sofosbuvir ± RBV
HCV G1 Treatment ExperiencedCirrhosis in 20%
0
20
40
60
80
100
SOF/LDV SOF/LDV+RBV SOF/LDV SOF/LDV+RBV
Afdhal N, et al. N Engl J Med. 2014;370:1483-1493.
12 weeks 24 weeks
SVR12
(%)
102/109 107/111 108/109 110/111
94 96 99 99
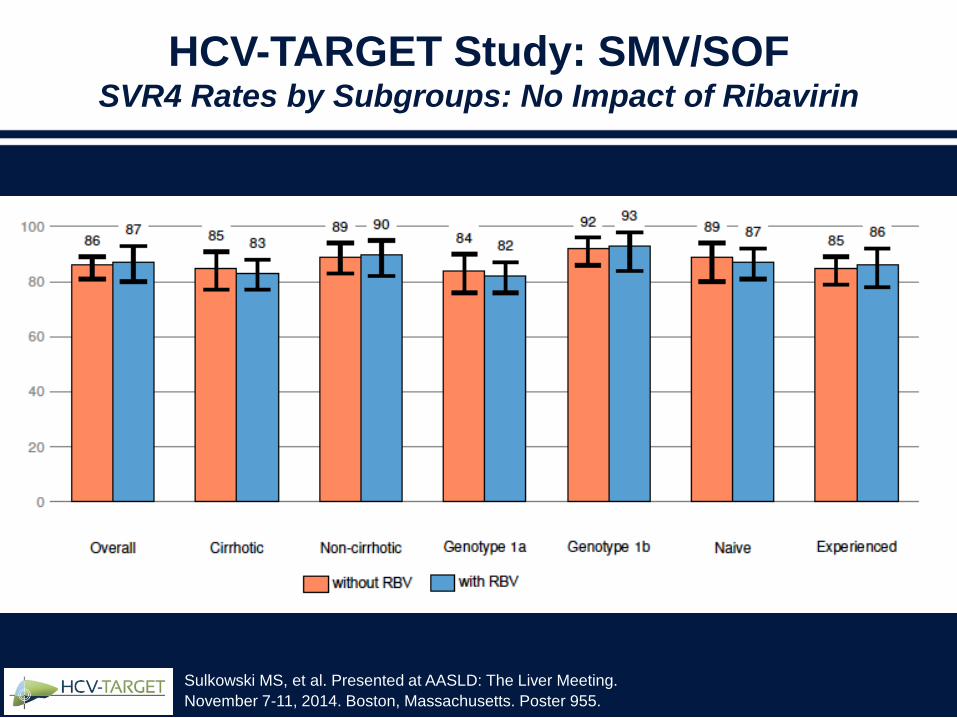
HCV-TARGET Study: SMV/SOFSVR4 Rates by Subgroups: No Impact of Ribavirin
Sulkowski MS, et al. Presented at AASLD: The Liver Meeting.
November 7-11, 2014. Boston, Massachusetts. Poster 955.
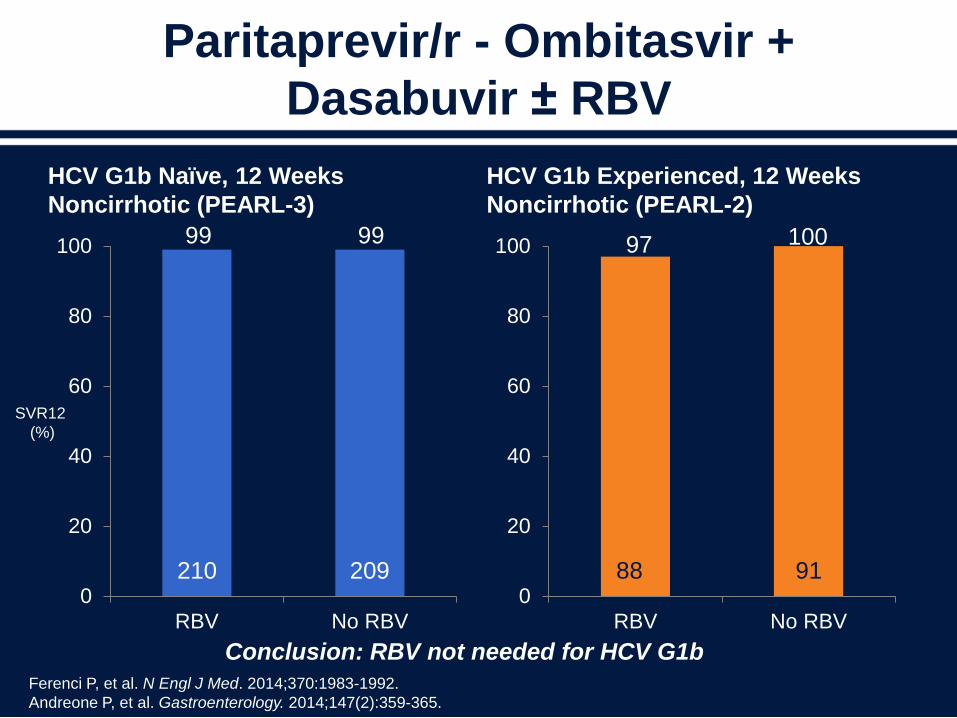
Paritaprevir/r - Ombitasvir +
Dasabuvir ± RBV
HCV G1b Naïve, 12 Weeks
Noncirrhotic (PEARL-3)
0
20
40
60
80
100
RBV No RBV
HCV G1b Experienced, 12 Weeks
Noncirrhotic (PEARL-2)
0
20
40
60
80
100
RBV No RBV
Ferenci P, et al. N Engl J Med. 2014;370:1983-1992.
Andreone P, et al. Gastroenterology. 2014;147(2):359-365.
210 209 88 91
99 99 97 100
Conclusion: RBV not needed for HCV G1b
SVR12
(%)
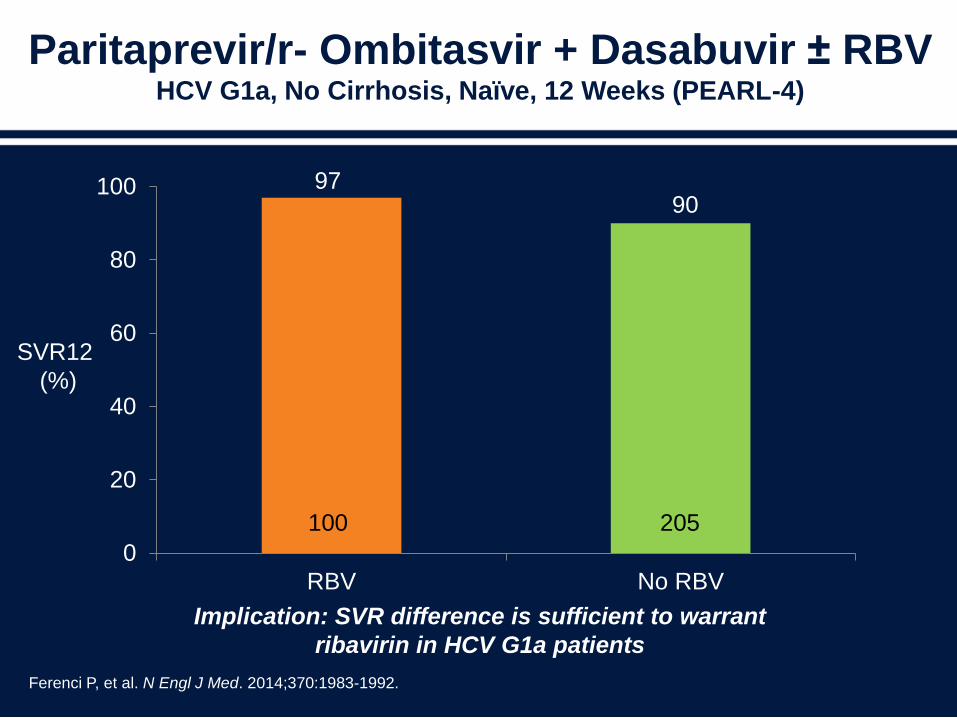
Paritaprevir/r- Ombitasvir + Dasabuvir ± RBVHCV G1a, No Cirrhosis, Naïve, 12 Weeks (PEARL-4)
0
20
40
60
80
100
RBV No RBV
Ferenci P, et al. N Engl J Med. 2014;370:1983-1992.
100 205
9790
Implication: SVR difference is sufficient to warrant
ribavirin in HCV G1a patients
SVR12
(%)

How Short Can We Make
Therapy With the First-wave
Regimens?
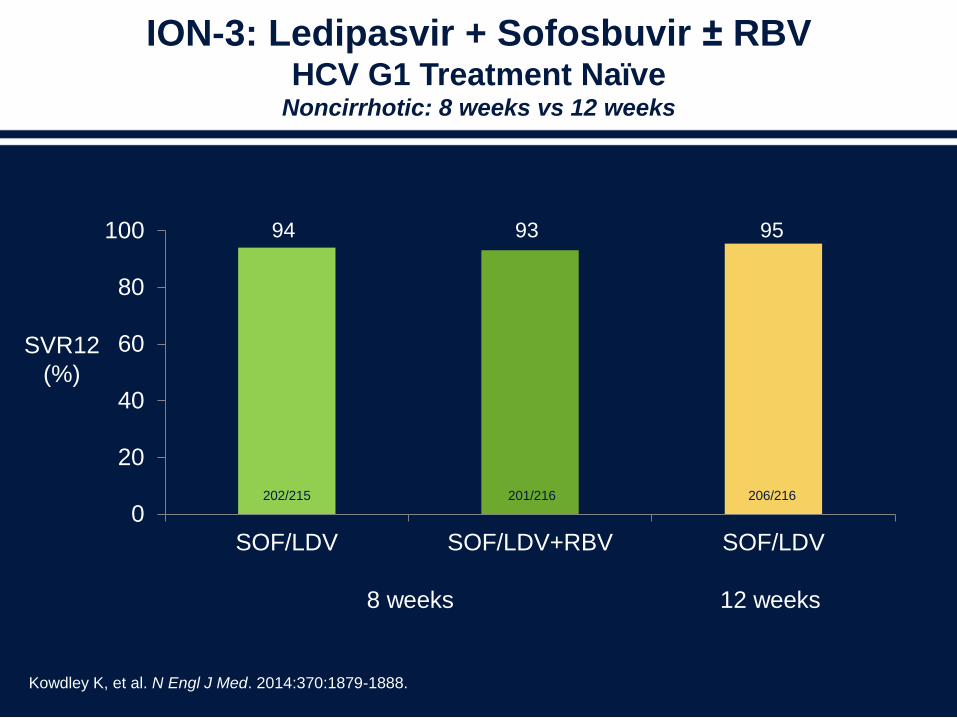
ION-3: Ledipasvir + Sofosbuvir ± RBVHCV G1 Treatment Naïve
Noncirrhotic: 8 weeks vs 12 weeks
0
20
40
60
80
100
SOF/LDV SOF/LDV+RBV SOF/LDV
Kowdley K, et al. N Engl J Med. 2014:370:1879-1888.
8 weeks 12 weeks
SVR12
(%)
202/215 201/216
94 93 95
206/216
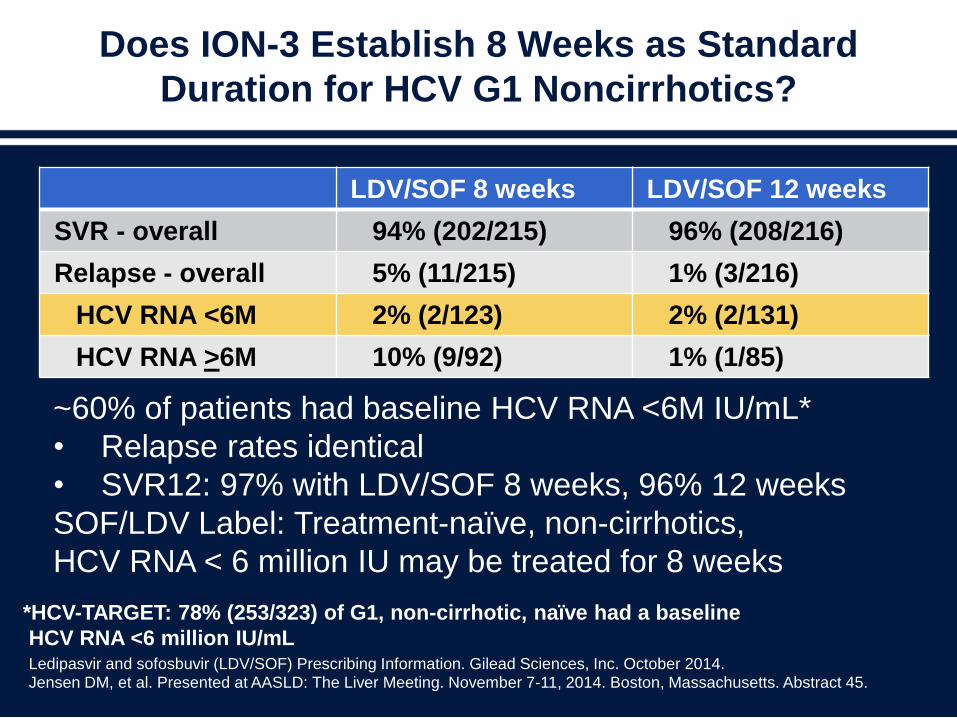
Does ION-3 Establish 8 Weeks as Standard
Duration for HCV G1 Noncirrhotics?
LDV/SOF 8 weeks LDV/SOF 12 weeks
SVR - overall 94% (202/215) 96% (208/216)
Relapse - overall 5% (11/215) 1% (3/216)
HCV RNA <6M 2% (2/123) 2% (2/131)
HCV RNA >6M 10% (9/92) 1% (1/85)
Ledipasvir and sofosbuvir (LDV/SOF) Prescribing Information. Gilead Sciences, Inc. October 2014. Jensen DM, et al. Presented at AASLD: The Liver Meeting. November 7-11, 2014. Boston, Massachusetts. Abstract 45.
~60% of patients had baseline HCV RNA <6M IU/mL*
• Relapse rates identical
• SVR12: 97% with LDV/SOF 8 weeks, 96% 12 weeks
SOF/LDV Label: Treatment-naïve, non-cirrhotics,
HCV RNA < 6 million IU may be treated for 8 weeks
*HCV-TARGET: 78% (253/323) of G1, non-cirrhotic, naïve had a baseline
HCV RNA <6 million IU/mL
How Long Should
Treatment-experienced
Cirrhotics Be Treated With the
First-wave DAA Regimens?
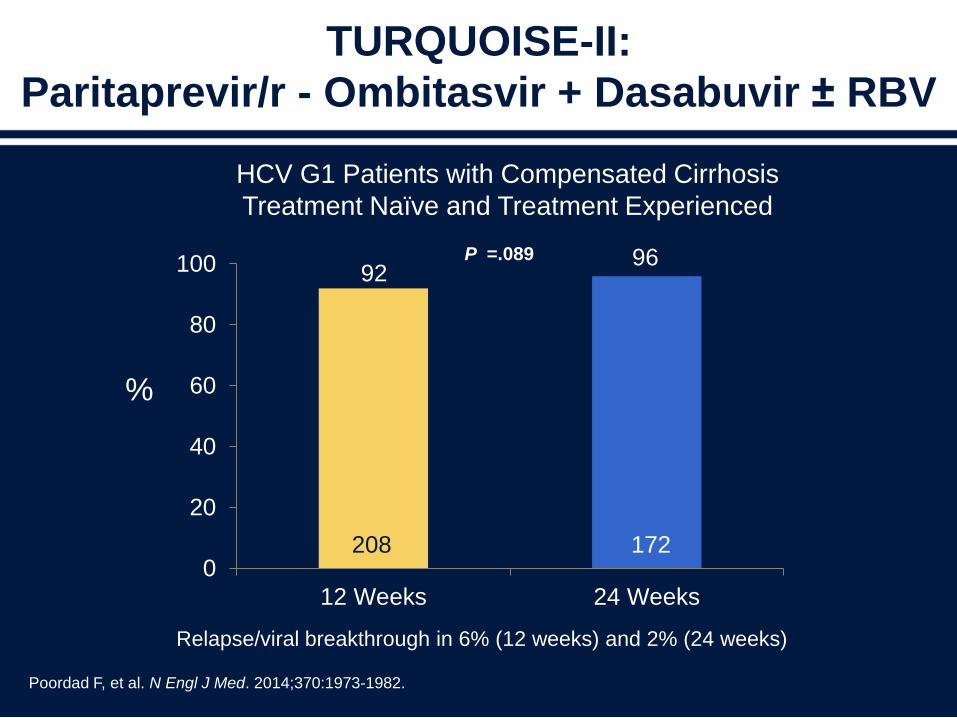
TURQUOISE-II:
Paritaprevir/r - Ombitasvir + Dasabuvir ± RBV
Poordad F, et al. N Engl J Med. 2014;370:1973-1982.
0
20
40
60
80
100
12 Weeks 24 Weeks
9296
208 172
Relapse/viral breakthrough in 6% (12 weeks) and 2% (24 weeks)
P =.089
HCV G1 Patients with Compensated Cirrhosis
Treatment Naïve and Treatment Experienced
%
Arm A: 12-week regimen
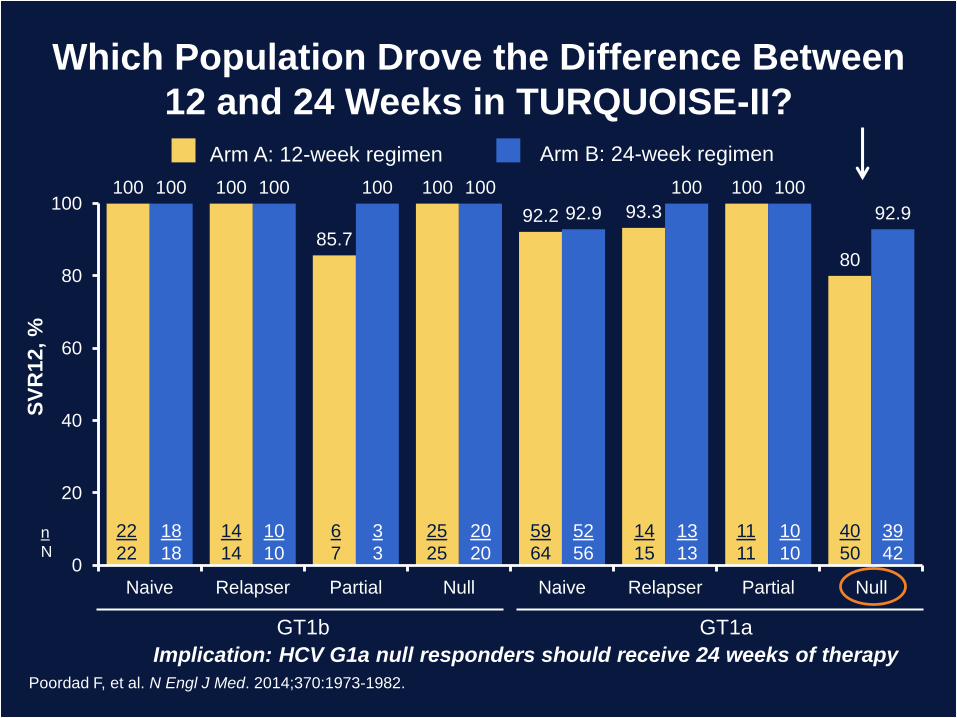
Which Population Drove the Difference Between
12 and 24 Weeks in TURQUOISE-II?
Poordad F, et al. N Engl J Med. 2014;370:1973-1982.
100 100
85.7
100
92.2 93.3
100
80
100 100 100 100
92.9
100 100
92.9
0
20
40
60
80
100
Naive Relapser Partial Null Naive Relapser Partial Null
SV
R12, %
Arm B: 24-week regimen
GT1b GT1a
n
N
22
22
18
18
14
14
10
10
6
7
3
3
25
25
20
20
59
64
52
56
14
15
13
13
11
11
10
10
40
50
39
42
Implication: HCV G1a null responders should receive 24 weeks of therapy
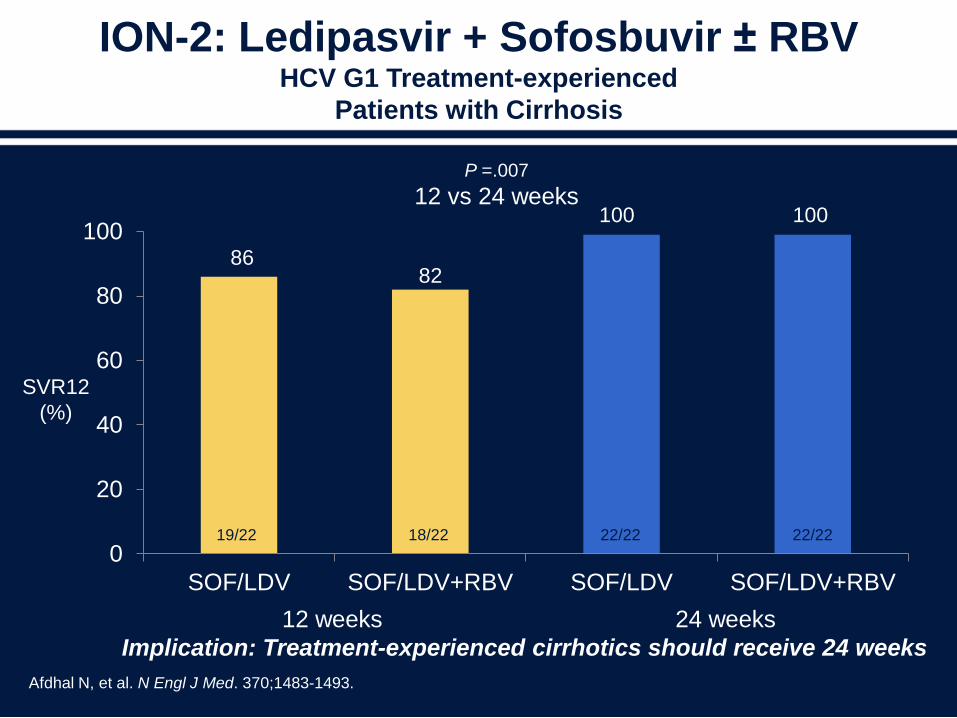
ION-2: Ledipasvir + Sofosbuvir ± RBV HCV G1 Treatment-experienced
Patients with Cirrhosis
0
20
40
60
80
100
SOF/LDV SOF/LDV+RBV SOF/LDV SOF/LDV+RBV
Afdhal N, et al. N Engl J Med. 370;1483-1493.
12 weeks 24 weeks
SVR12
(%)
8682
100 100
19/22 18/22 22/22 22/22
P =.007
12 vs 24 weeks
Implication: Treatment-experienced cirrhotics should receive 24 weeks
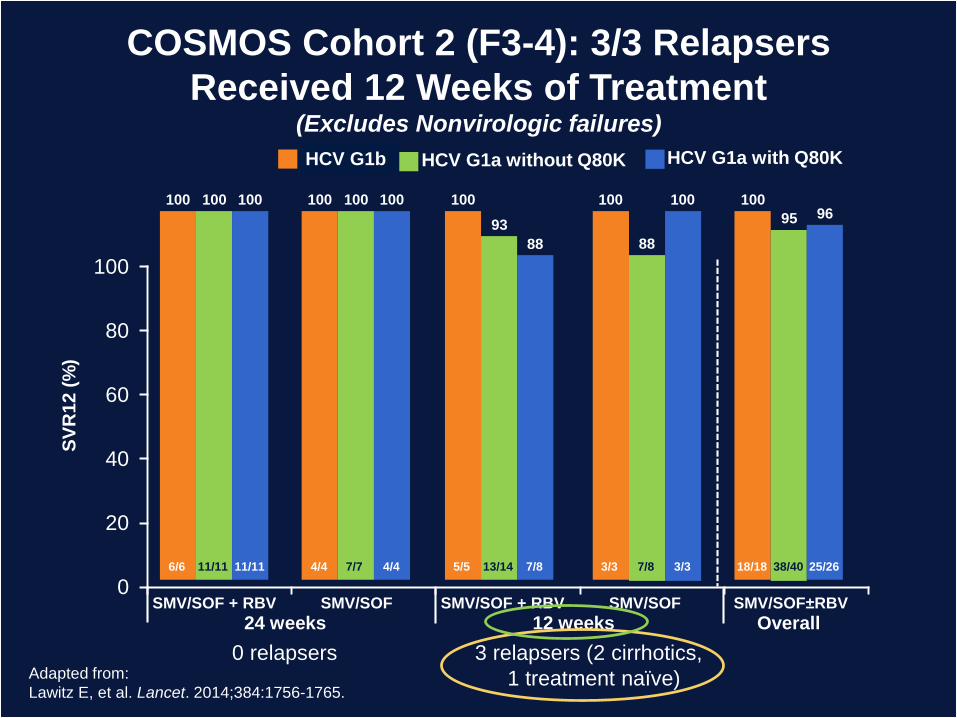
GT 1b
0
20
40
60
80
100
SMV/SOF±RBVSMV/SOF + RBV SMV/SOF + RBVSMV/SOF SMV/SOF
24 weeks 12 weeks Overall
SV
R1
2 (
%)
HCV G1a without Q80K
100 100
93
88
95
HCV G1a with Q80K
100 100
88
10096
6/6 11/11 11/11 4/4 7/7 4/4 5/5 13/14 7/8 3/3 7/8 3/3 18/18 38/40 25/26
100 100 100 100 100
COSMOS Cohort 2 (F3-4): 3/3 Relapsers
Received 12 Weeks of Treatment(Excludes Nonvirologic failures)
Adapted from:
Lawitz E, et al. Lancet. 2014;384:1756-1765.
0 relapsers 3 relapsers (2 cirrhotics,
1 treatment naïve)
HCV G1b
Q80K: Does It Matter When SMV
and SOF Are Used Together?
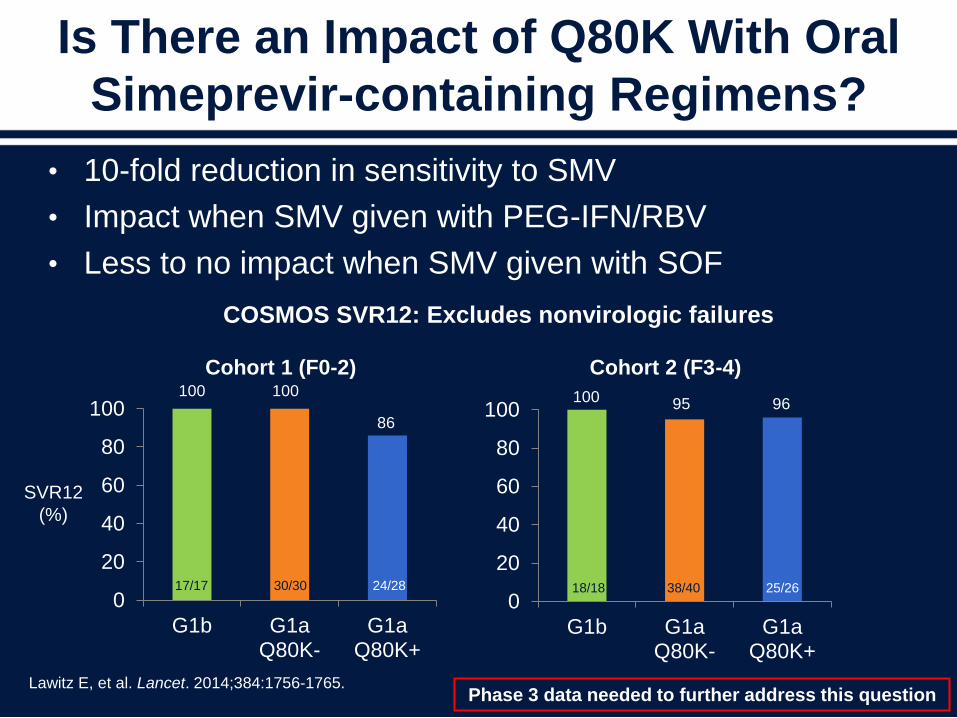
Is There an Impact of Q80K With Oral
Simeprevir-containing Regimens?
• 10-fold reduction in sensitivity to SMV
• Impact when SMV given with PEG-IFN/RBV
• Less to no impact when SMV given with SOF
Lawitz E, et al. Lancet. 2014;384:1756-1765.
0
20
40
60
80
100
G1b G1aQ80K-
G1aQ80K+
18/18 38/40 25/260
20
40
60
80
100
G1b G1aQ80K-
G1aQ80K+
COSMOS SVR12: Excludes nonvirologic failures
Cohort 1 (F0-2) Cohort 2 (F3-4)
17/17 30/30 24/28
100 95 96100 100
86
SVR12
(%)
Phase 3 data needed to further address this question
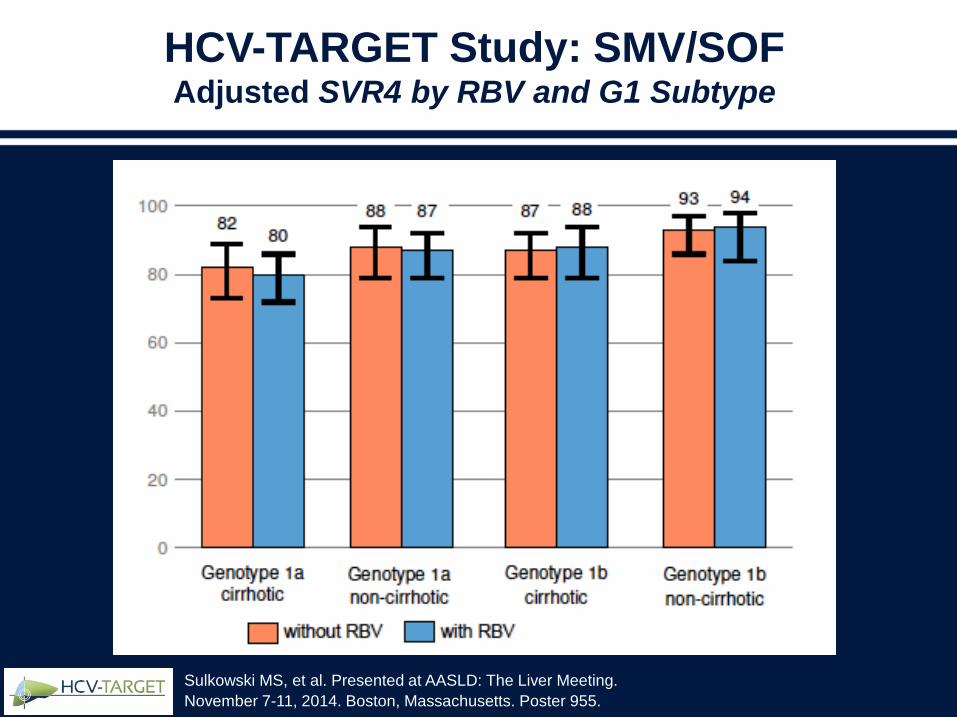
HCV-TARGET Study: SMV/SOFAdjusted SVR4 by RBV and G1 Subtype
Sulkowski MS, et al. Presented at AASLD: The Liver Meeting.
November 7-11, 2014. Boston, Massachusetts. Poster 955.
Treatment of
Protease Inhibitor Failures
Treatment of Protease
Inhibitor Failures
• Population sequencing is commercially available
– Detection limit 20% of viral population
– Negative sequencing assay may not identify
levels of RAVs sufficient to impair efficacy of
PI-containing regimens
• Non-PI regimens may be superior for this
population
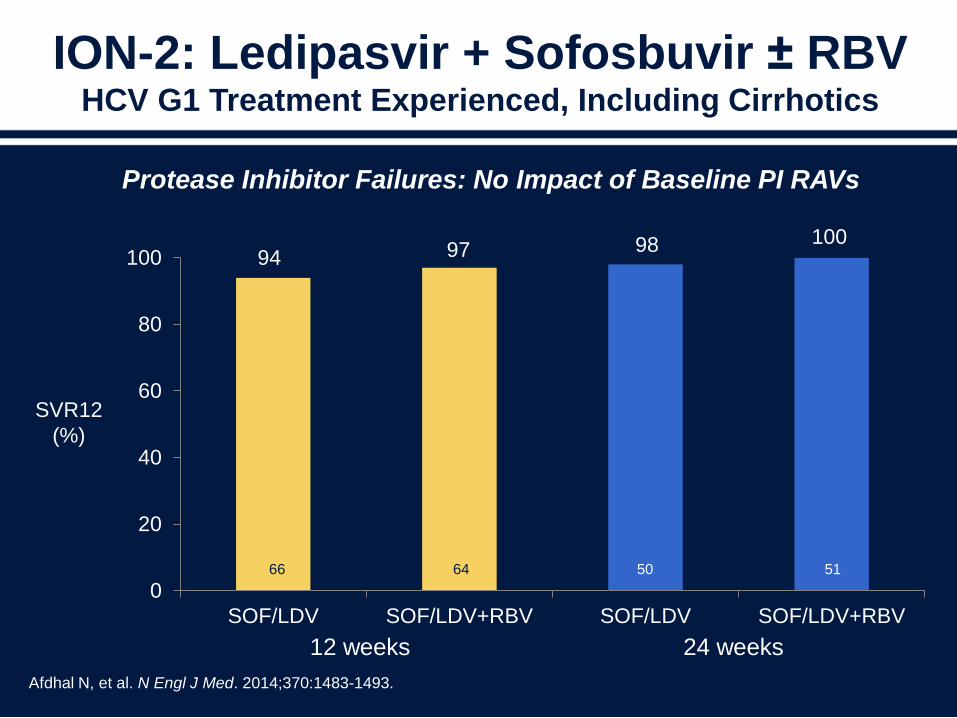
ION-2: Ledipasvir + Sofosbuvir ± RBV HCV G1 Treatment Experienced, Including Cirrhotics
0
20
40
60
80
100
SOF/LDV SOF/LDV+RBV SOF/LDV SOF/LDV+RBV
Afdhal N, et al. N Engl J Med. 2014;370:1483-1493.
12 weeks 24 weeks
SVR12
(%)
66 64 50 51
94 97 98 100
Protease Inhibitor Failures: No Impact of Baseline PI RAVs
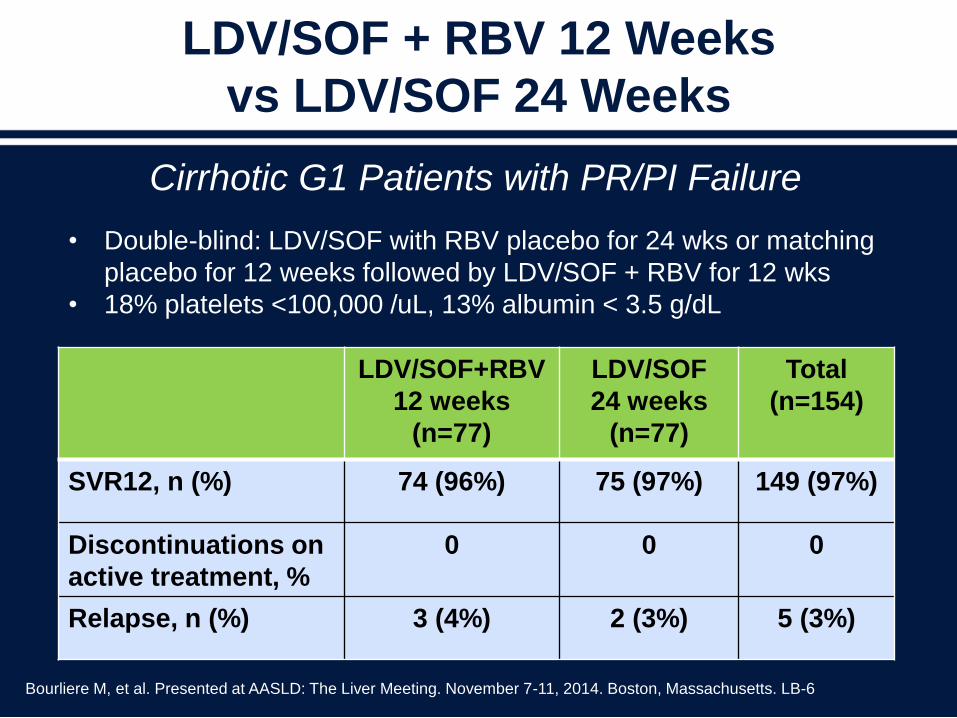
LDV/SOF + RBV 12 Weeks
vs LDV/SOF 24 Weeks
Cirrhotic G1 Patients with PR/PI Failure
Bourliere M, et al. Presented at AASLD: The Liver Meeting. November 7-11, 2014. Boston, Massachusetts. LB-6
• Double-blind: LDV/SOF with RBV placebo for 24 wks or matching
placebo for 12 weeks followed by LDV/SOF + RBV for 12 wks
• 18% platelets <100,000 /uL, 13% albumin < 3.5 g/dL
LDV/SOF+RBV
12 weeks
(n=77)
LDV/SOF
24 weeks
(n=77)
Total
(n=154)
SVR12, n (%) 74 (96%) 75 (97%) 149 (97%)
Discontinuations on
active treatment, %
0 0 0
Relapse, n (%) 3 (4%) 2 (3%) 5 (3%)

SVR12 for Treatment Experienced,
Genotypes 1, Prior Regimen
Intent to Treat Per Protocol
Dieterich D, et al. Presented at AASLD: The Liver Meeting. November 7-11, 2014. Boston, Massachusetts. Abstract 46.
TRIO Cohort
SVR12, % Prior PEG
+ RBV + PI
Failure
Prior PEG
+ RBV
Failure
SOF +
PEG/RBV73 67
SMV + SOF ±
RBV82 80
SVR12, % Prior PEG
+ RBV +
PI Failure
Prior PEG
+ RBV
Failure
SOF +
PEG/RBV78 73
SMV + SOF
± RBV87 86
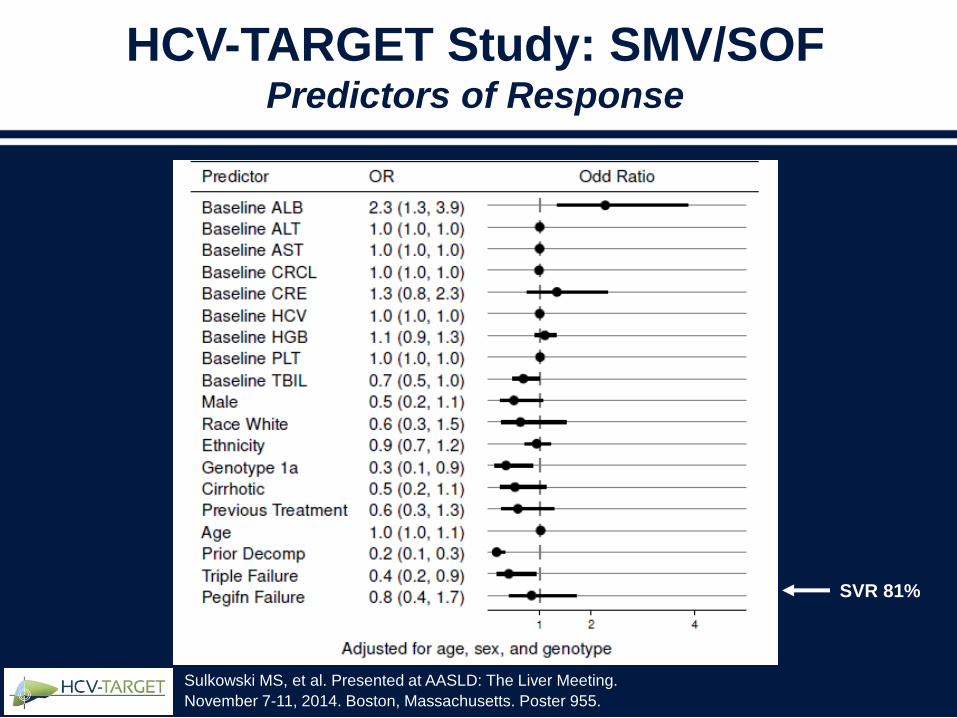
HCV-TARGET Study: SMV/SOFPredictors of Response
Sulkowski MS, et al. Presented at AASLD: The Liver Meeting.
November 7-11, 2014. Boston, Massachusetts. Poster 955.
SVR 81%
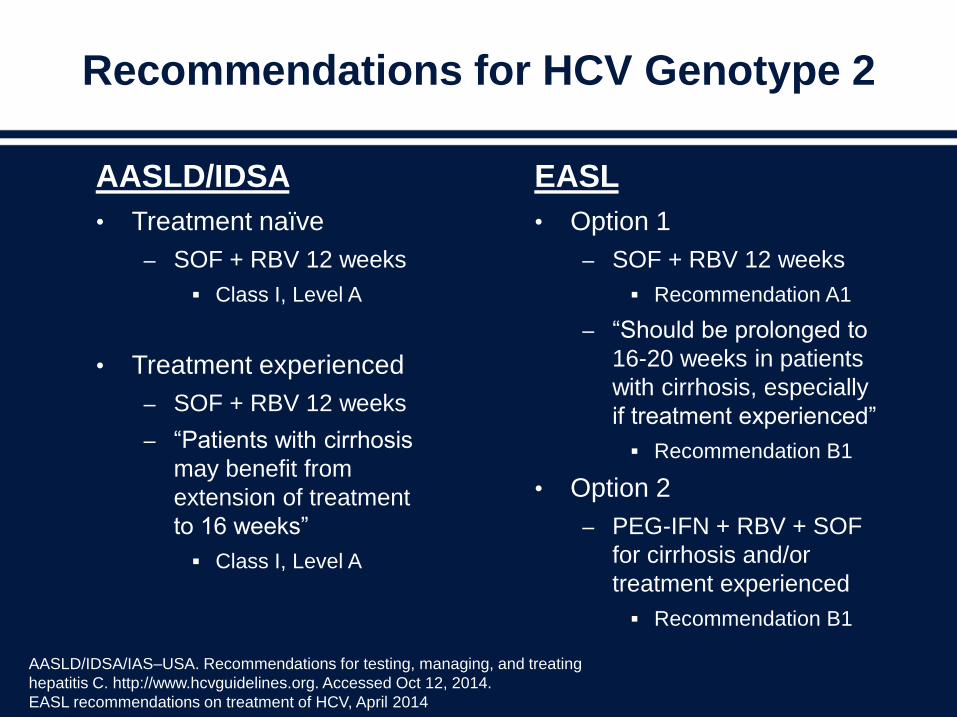
Recommendations for HCV Genotype 2
AASLD/IDSA
• Treatment naïve
– SOF + RBV 12 weeks
Class I, Level A
• Treatment experienced
– SOF + RBV 12 weeks
– “Patients with cirrhosis
may benefit from
extension of treatment
to 16 weeks”
Class I, Level A
EASL
• Option 1
– SOF + RBV 12 weeks
Recommendation A1
– “Should be prolonged to
16-20 weeks in patients
with cirrhosis, especially
if treatment experienced”
Recommendation B1
• Option 2
– PEG-IFN + RBV + SOF
for cirrhosis and/or
treatment experienced
Recommendation B1
AASLD/IDSA/IAS–USA. Recommendations for testing, managing, and treating
hepatitis C. http://www.hcvguidelines.org. Accessed Oct 12, 2014.
EASL recommendations on treatment of HCV, April 2014
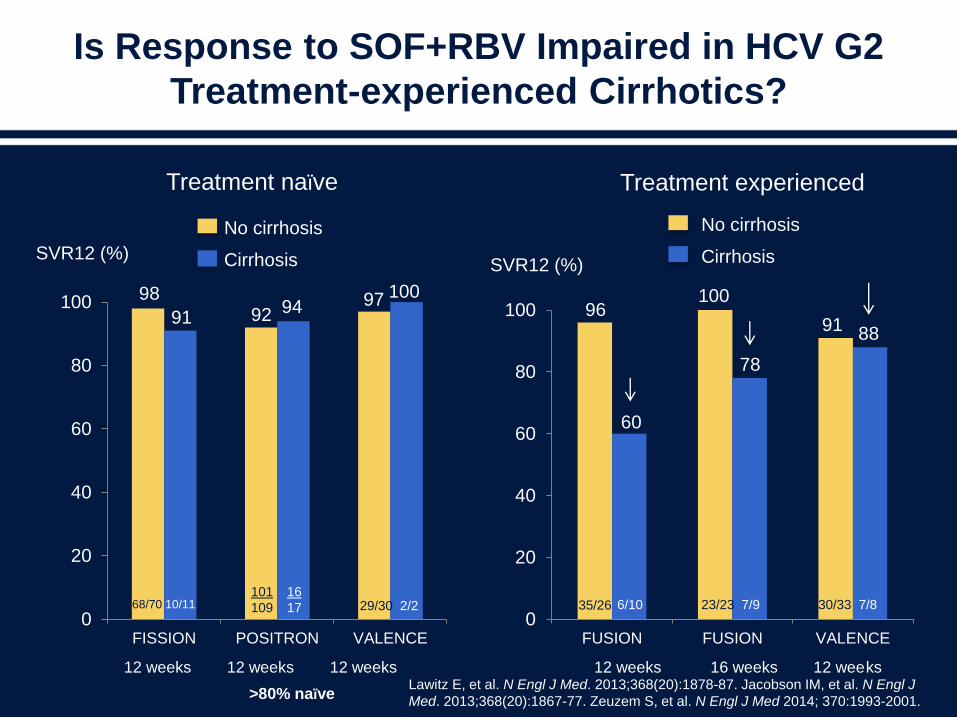
Is Response to SOF+RBV Impaired in HCV G2
Treatment-experienced Cirrhotics?
0
20
40
60
80
100
FISSION POSITRON VALENCE0
20
40
60
80
100
FUSION FUSION VALENCE
Treatment experienced
12 weeks 12 weeks 12 weeks 12 weeks 16 weeks 12 weeks
60
78
98
91 92 94 97 100
9196
100
6/10 23/23 7/9 30/33 7/829/30 2/268/70 10/11
>80% naïve
101
109
16
17 35/26
88
No cirrhosis
Cirrhosis
Treatment naïve
No cirrhosis
CirrhosisSVR12 (%)SVR12 (%)
Lawitz E, et al. N Engl J Med. 2013;368(20):1878-87. Jacobson IM, et al. N Engl J
Med. 2013;368(20):1867-77. Zeuzem S, et al. N Engl J Med 2014; 370:1993-2001.
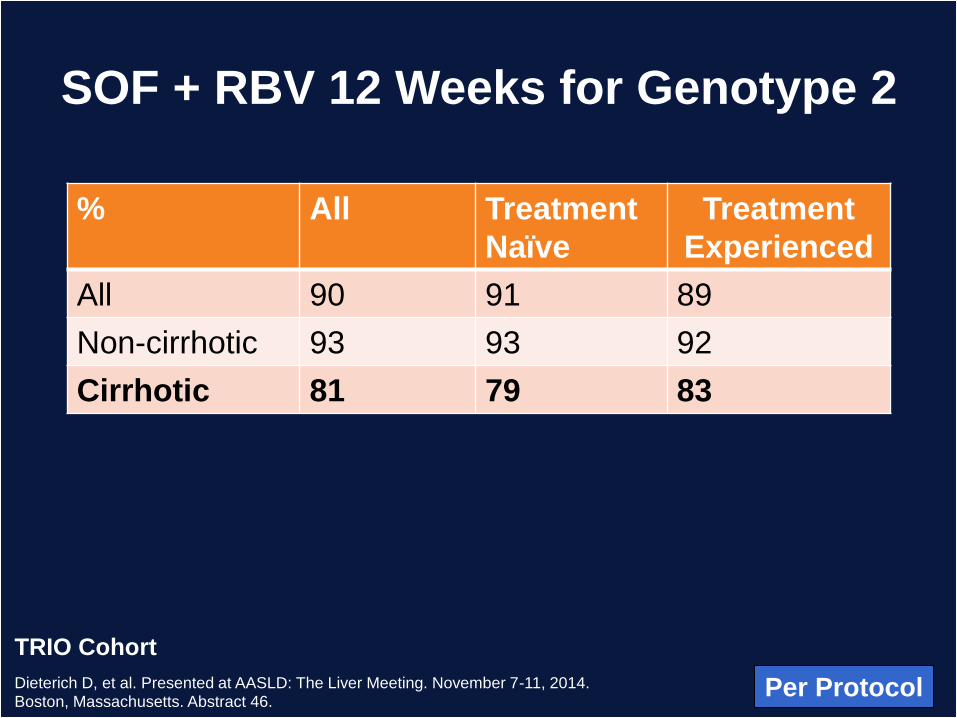
SOF + RBV 12 Weeks for Genotype 2
Per ProtocolDieterich D, et al. Presented at AASLD: The Liver Meeting. November 7-11, 2014. Boston, Massachusetts. Abstract 46.
TRIO Cohort
% All Treatment
Naïve
Treatment
Experienced
All 90 91 89
Non-cirrhotic 93 93 92
Cirrhotic 81 79 83
SOF + RBV GT2
N=235
On/Post Tx HCV RNA BLOQ
91% (204/223)
On/ Post Tx HCV RNA Quantified
9% (19/223)
Cohort of patients with treatment start on or before
4/15/14 ; BLOQ=Below Level of Quantitation;
VB
0.5%
(1/187)
Relapse
8%
(14/187)
SVR4+
187/223
SVR4+
90% (168/187)
Non-Response
1.1%
(2/187)
SVR4
Non-cirrhotic: 91% (116/128)
Cirrhotic: 88% (52/59)
Lost to f/u
1.1%
(2/187)
HCV RNA Outcomes for Sofosbuvir
+ RBV Genotype 2
Jensen DM, et al. Presented at AASLD:
The Liver Meeting. November 7-11, 2014.
Boston, Massachusetts. Abstract 45.
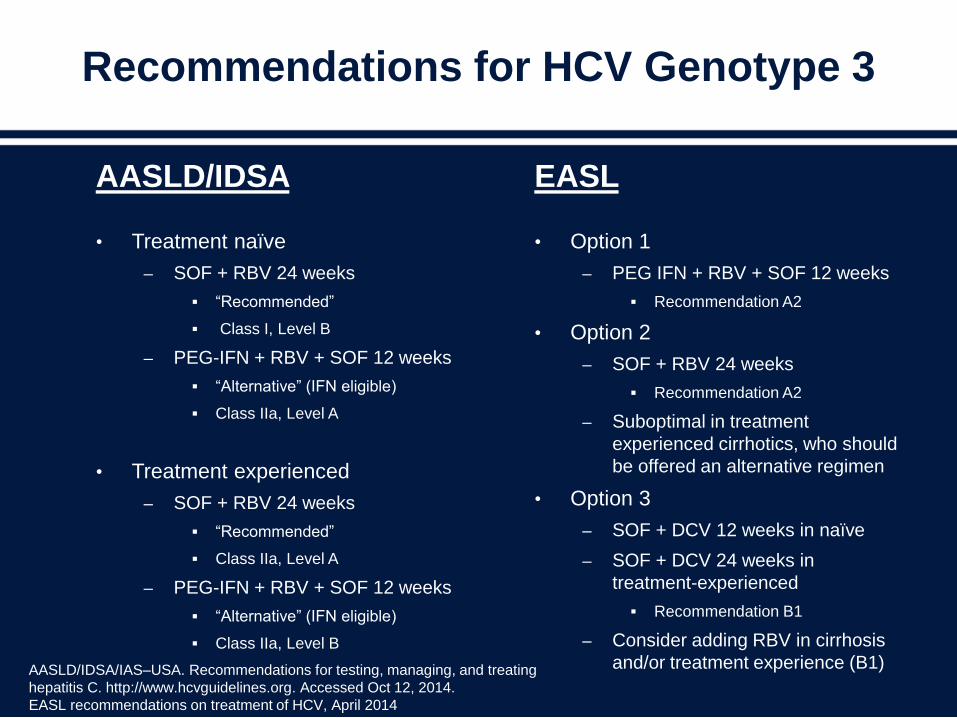
Recommendations for HCV Genotype 3
AASLD/IDSA
• Treatment naïve
– SOF + RBV 24 weeks
“Recommended”
Class I, Level B
– PEG-IFN + RBV + SOF 12 weeks
“Alternative” (IFN eligible)
Class IIa, Level A
• Treatment experienced
– SOF + RBV 24 weeks
“Recommended”
Class IIa, Level A
– PEG-IFN + RBV + SOF 12 weeks
“Alternative” (IFN eligible)
Class IIa, Level B
EASL
• Option 1
– PEG IFN + RBV + SOF 12 weeks
Recommendation A2
• Option 2
– SOF + RBV 24 weeks
Recommendation A2
– Suboptimal in treatment
experienced cirrhotics, who should
be offered an alternative regimen
• Option 3
– SOF + DCV 12 weeks in naïve
– SOF + DCV 24 weeks in
treatment-experienced
Recommendation B1
– Consider adding RBV in cirrhosis
and/or treatment experience (B1)AASLD/IDSA/IAS–USA. Recommendations for testing, managing, and treating
hepatitis C. http://www.hcvguidelines.org. Accessed Oct 12, 2014.
EASL recommendations on treatment of HCV, April 2014
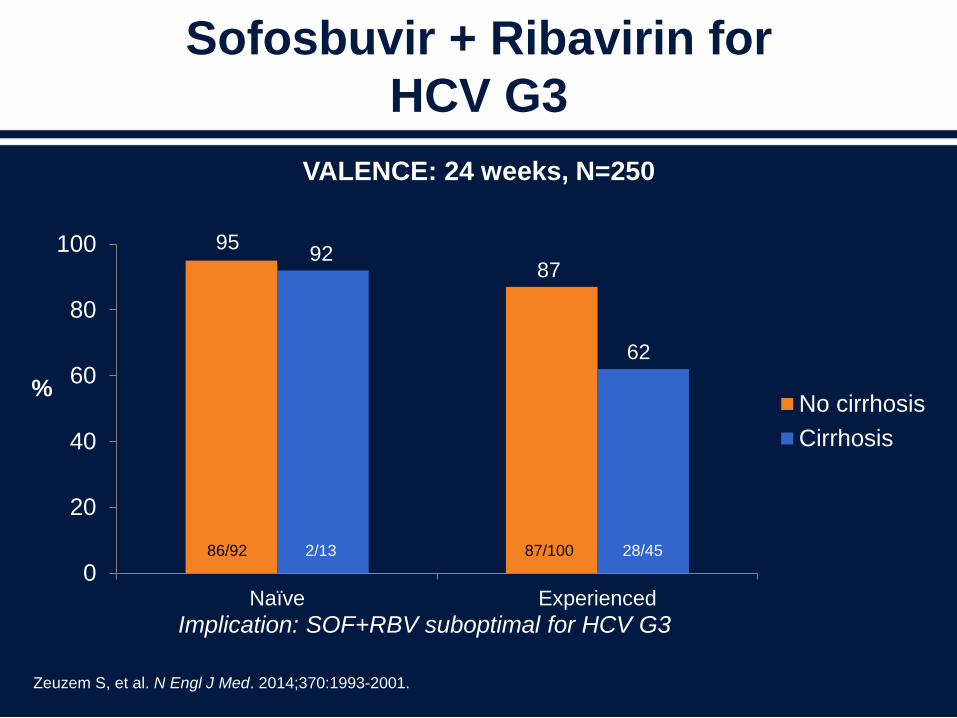
Sofosbuvir + Ribavirin for
HCV G3
0
20
40
60
80
100
Naïve Experienced
No cirrhosis
Cirrhosis
Zeuzem S, et al. N Engl J Med. 2014;370:1993-2001.
VALENCE: 24 weeks, N=250
9592
87
62
86/92 2/13 87/100 28/45
Implication: SOF+RBV suboptimal for HCV G3
%
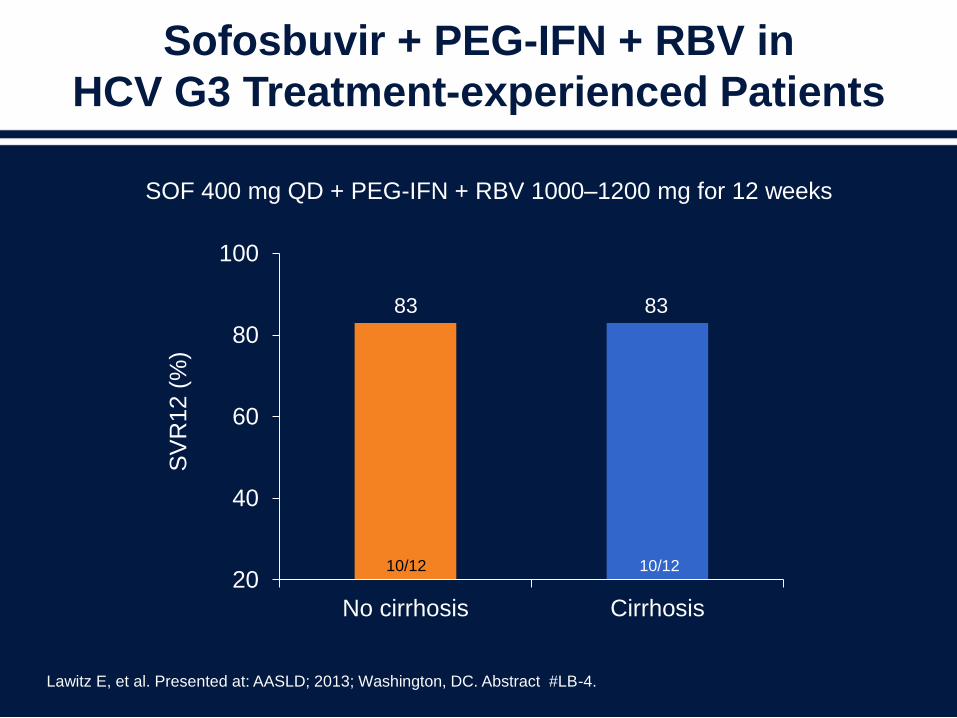
20
40
60
80
100
No cirrhosis Cirrhosis
SV
R12 (
%)
83
10/12
83
10/12
SOF 400 mg QD + PEG-IFN + RBV 1000–1200 mg for 12 weeks
Sofosbuvir + PEG-IFN + RBV in
HCV G3 Treatment-experienced Patients
Lawitz E, et al. Presented at: AASLD; 2013; Washington, DC. Abstract #LB-4.
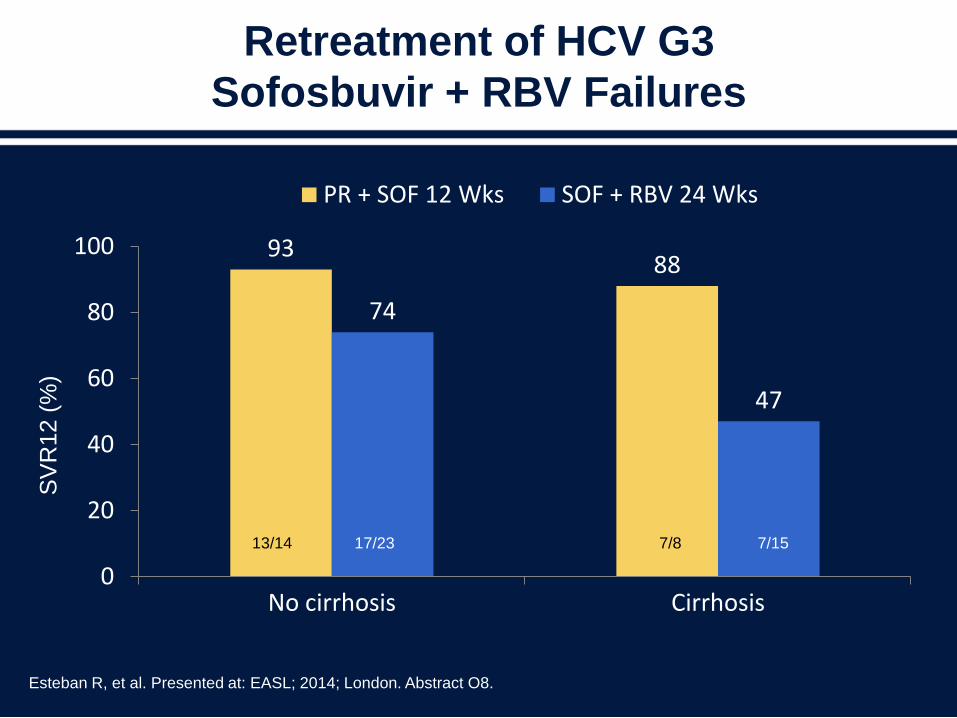
Retreatment of HCV G3
Sofosbuvir + RBV Failures
9388
74
47
0
20
40
60
80
100
No cirrhosis Cirrhosis
PR + SOF 12 Wks SOF + RBV 24 Wks
Esteban R, et al. Presented at: EASL; 2014; London. Abstract O8.
SV
R12 (
%)
13/14 17/23 7/8 7/15
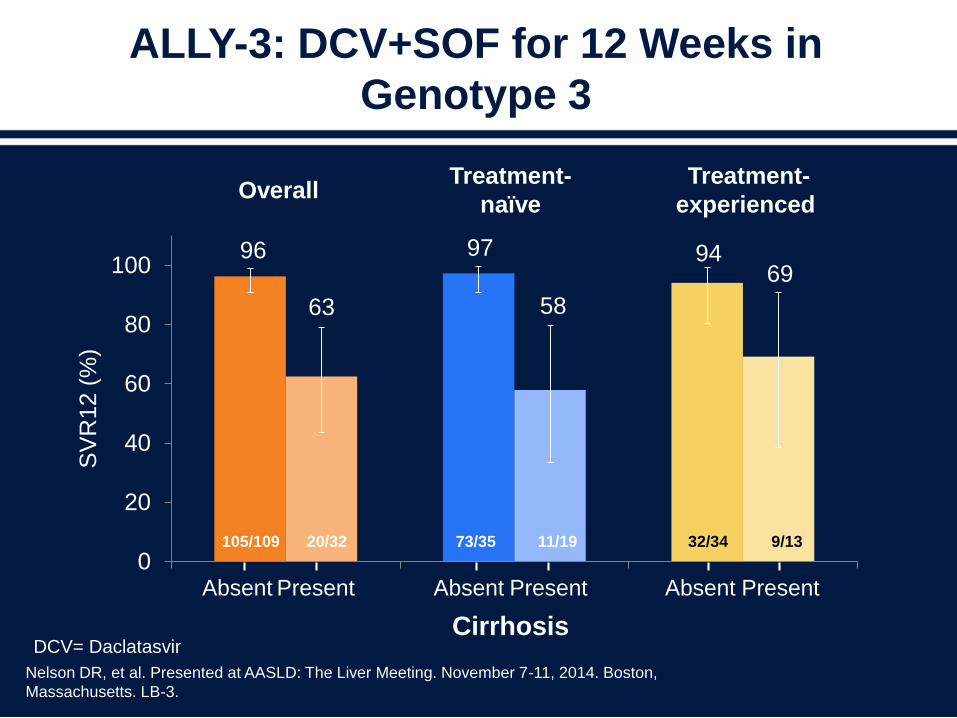
ALLY-3: DCV+SOF for 12 Weeks in
Genotype 3
96 97 94
63 58
69
0
20
40
60
80
100
SV
R12 (
%)
PresentAbsent PresentAbsent PresentAbsent
Treatment-
naïve
Treatment-
experiencedOverall
Cirrhosis
Nelson DR, et al. Presented at AASLD: The Liver Meeting. November 7-11, 2014. Boston,
Massachusetts. LB-3.
105/109 20/32 73/35 11/19 32/34 9/13
DCV= Daclatasvir
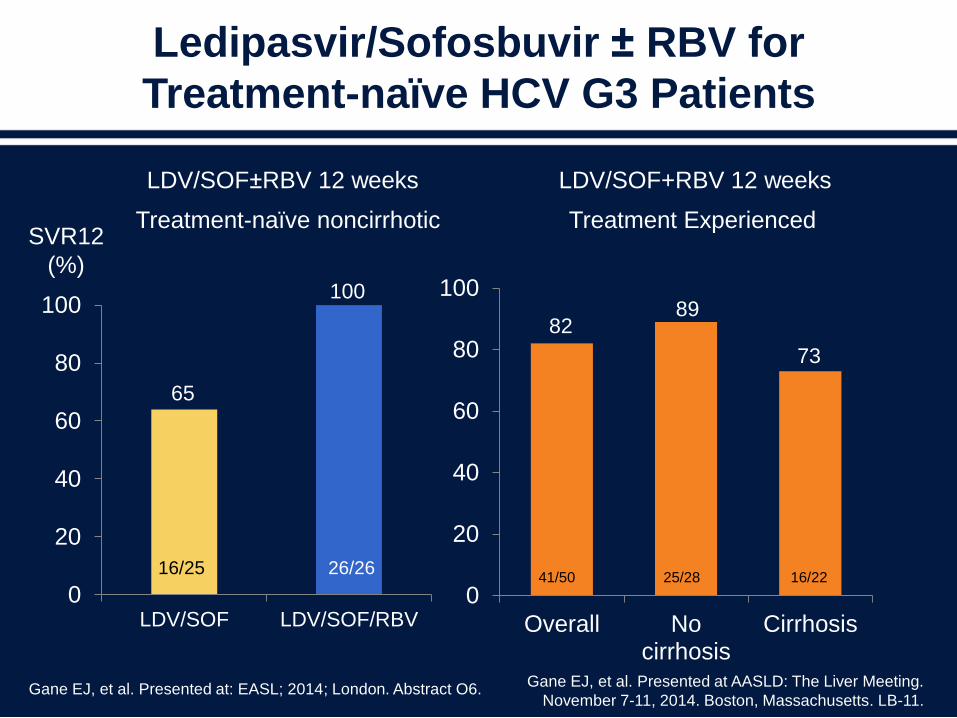
Ledipasvir/Sofosbuvir ± RBV for
Treatment-naïve HCV G3 Patients
0
20
40
60
80
100
LDV/SOF LDV/SOF/RBV
Gane EJ, et al. Presented at: EASL; 2014; London. Abstract O6.
65
16/25 26/26
SVR12
(%)
0
20
40
60
80
100
Overall Nocirrhosis
Cirrhosis
100
8289
73
LDV/SOF±RBV 12 weeks LDV/SOF+RBV 12 weeks
Treatment Experienced
41/50 25/28
Treatment-naïve noncirrhotic
Gane EJ, et al. Presented at AASLD: The Liver Meeting.
November 7-11, 2014. Boston, Massachusetts. LB-11.
16/22
Conclusions
• No more interferon for genotype 1, still a role for ribavirin
• Possible role for IFN as “placeholder” for genotype 3 pending
new DAAs to put into combination regimens
• Full disclosure to patients, e.g. risk of resistance if regimen fails
• Important considerations for treatment
– Correct regimen for patient’s genotype or subtype
– Appropriate duration of therapy (or unnecessarily prolonged)
– Need to assess degree of hepatic fibrosis pretreatment
– Education re: importance of compliance
– Attention to drug-drug interactions
– Monitoring during and after treatment especially for HCC in
patients with advanced fibrosis